 Carlos Collado Macián1
Carlos Collado Macián1 David Pujol Pocull1
David Pujol Pocull1 Fernando Dominguez1,2
Fernando Dominguez1,2 Juan Carlos López-Azor1
Juan Carlos López-Azor1 Pablo Garcia-Pavia1,2,3
Pablo Garcia-Pavia1,2,3 Julio Nuñez2,4
Julio Nuñez2,4 Marta Cobo Marcos1,2*
Marta Cobo Marcos1,2*
- 1Department of Cardiology, Hospital Universitario Puerta de Hierro Majadahonda, (IDIPHISA), Madrid, Spain
- 2Centro de Investigación Biomédica en Red en Enfermedades Cardiovasculares (CIBERCV), Madrid, Spain
- 3Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain
- 4Department of Cardiology, Hospital Clínico Universitario de Valencia, INCLIVA, Universidad de Valencia, Valencia, Spain
Background: Management of patients with refractory congestion, is one of the most important challenges in the field of heart failure (HF). Diuretic therapy remains the most widely used therapy to achieve euvolemia. However, some patients experience fluid overload despite the use of high-dose diuretics and new strategies to overcome diuretic resistance are needed.
Case Summary: We report an 85 years-old male patient admitted for decompensated HF with persistent tissue fluid overload (peripheral edema) for more than two weeks despite high dose of intravenous furosemide with the combination of other diuretics. At this point, we performed leg venous compression using elastic bandages for three days. After 72 h, edema disappeared, and additional weight loss was achieved (1 kg/day). No side effects were observed and the patient was discharged home euvolemic.
Conclusion: Venous leg compression may be an alternative therapy in patients with persistent tissue fluid overload resistant to diuretics.
Introduction
Fluid overload is frequent in patients with HF. A sustained increase in intravascular hydrostatic pressure and vascular permeability make fluid overload shift towards the interstitium, leading to extravascular fluid overload (1, 2). Most diuretics reduce intravascular congestion; however, hypotension and worsening renal function may limit the efficacy of diuretic therapy (3), so new strategies to overcome diuretic resistance are needed.
Case report
We present the case of an 85-year-old male who attended our emergency department with shortness of breath. The patient had a medical history of hypertension, dyslipidemia, obesity, chronic kidney disease, chronic obstructive pulmonary disease, ischemic heart disease, and atrial fibrillation. He presented his first episode of HF with preserved ejection fraction (HFpEF) two years earlier. At that moment, screening of amyloidosis was performed, and no secondary etiologies of HFpEF were found.
His treatment included amiloride/hydrochlorothiazide 5/50 mg/24 h, furosemide 120 mg/24 h, and dapagliflozin 10 mg/24 h.
On physical examination, he presented jugular venous distension, bilateral pulmonary crackles and bilateral edema above the knees. He was hemodynamically stable, showing a blood pressure of 140/60 mmHg, a heart rate of 71 beats per minute, and an oxygen saturation of 93% without oxygen therapy. At the moment of admission, his weight was 112 kg.
Blood tests showed elevated NT-proBNP (926 pg/ml) and worsening kidney function: creatinine 2.15 mg/dl (estimated glomerular filtration rate: 27.1 ml/min/1.73 m2, previous value 45.5 ml/min/1.73 m2). Chest x-ray revealed mild bilateral pleural effusion.
Echocardiography confirmed mild global hypertrophy of the left ventricle, preserved ejection fraction, diastolic dysfunction grade II, severe dilated left atrium, without pulmonary hypertension. The inferior vena cava was enlarged (21 mm), and lung B-lines were found in 6/8 fields.
Electrocardiogram revealed atrial fibrillation at 90 beats per minute and right bundle branch block.
The patient was admitted with the diagnosis of decompensated HF, and diuretic treatment was initiated following the 2021 ESC Heart Failure Guidelines (4).
Therapeutic intervention
An intravenous bolus of 120 mg furosemide (same dose taken orally at home) was administered.
The initial diuretic response was partially adequate (diuretic rate, 133 ml/h; urinary sodium, 56 mEq/L). However, congestion signs persisted, and the goal of 3,000 ml of diuresis per day was not achieved. Therefore, the furosemide dose was increased to 200 mg/12 h, and a sequential nephron blockade with chlorthalidone (50 mg/24 h) and dapagliflozin was implemented.
Despite this diuretic scalation, diuretic response didn't improve (Figure 1), so we decided to administer a combination of intravenous furosemide with hypertonic saline solution (Table 1) to improve tissue congestion. Subsequently, the patient presented a progressive increase in daily diuresis rate (>3,000 ccs every 24 h), an improvement in kidney function (creatinine 1.8 mg/dl), and a weight loss of 1–2 kg per day (8 kg on day 11).
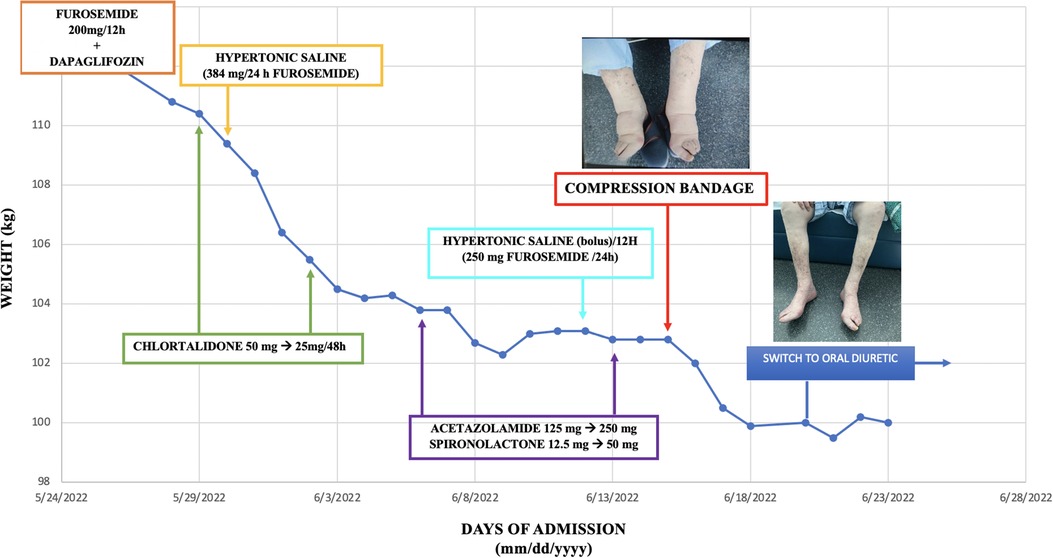
Figure 1. Timeline evolution of patient weight depending on the treatment administered. This timeline shows the different diuretics used during the patient's admission and their influence on weight loss. On day 20, the edema in the lower limbs was still evident; therefore, venous leg compression therapy was started for 72 h. When the bandages were removed, euvolemia was achieved, which allowed the change to oral diuretics and the patient's discharge.
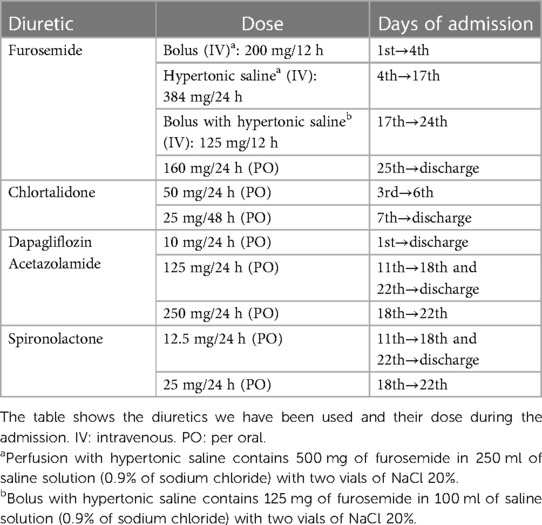
Table 1. Diuretics and their dose used in the admission.
Despite this, the patient persisted with edema up to the knee; therefore, two new classes of diuretics (acetazolamide and spironolactone) were added, without a significant improvement in diuretic response. On day 20, the patient persisted with signs of tissue congestion and signs of intravascular depletion (IVC diameter from 20 mm on admission to 14 mm, which collapses >50%).
Therefore, we decided to apply crepe bandages to the lower limbs from the feet to the knees. The initial bandage was removed after 24 h, and a new one was placed.
After 72 h of combined diuretic and leg venous compression (LVC), the patient lost 3 kg of weight, the edema resolved, and the kidney function improved. A slight increase in NT-proBNP and in the IVC diameter (from 14 to 17 mm after 24 h) was observed as an indirect sign of intravascular repletion. After achieving euvolemia, we could switch to oral therapy and discharge the patient. After six months of follow-up in our HF multidisciplinary program, the patient is asymptomatic, with no further decompensations.
Discussion
In this case, LVC was a helpful strategy for overcoming diuretic resistance in a patient with predominant tissue fluid overload and absence of intravascular congestion.
Multiparametric evaluation of congestion to quantify and phenotype congestion may lead to a more effective tailored approach.
Compression therapy in patients with HF has traditionally been considered a contraindication due to the hypothesis that increased cardiac preload may lead to worsening pulmonary congestion (5–7).
These hemodynamic changes have been analyzed in different studies. Derreppe et al. observed a significant increase in right atrial and pulmonary pressure after venous leg compression. Thirty minutes after withdrawing compression therapy, these parameters returned to baseline values (8).
In a study conducted by Wilputte et al., an increase in right blood pressure was observed with a transient deterioration in ventricular function secondary to an increase in preload and afterload in patients with NYHA III-IV HF (9).
Interestingly, a recent study evaluated the effect of 72 h-venous LVC according to IVC diameter in 20 subjects with ambulatory congestive HF (10). When basal IVC was <21 mm, a significant increase in the diameter of the IVC was observed in the group treated with LVC (approximately 2 mm), and this intravascular filling was associated with greater decongestion (increased natriuresis, weight loss, and peripheral edema). These results were not observed in the group with an initial vena cava diameter >21 mm.
Likewise, we observed a 3-mm increase in the diameter of the IVC after starting LVC. This was accompanied by an increase in diuresis rate and a slight increase in NT-proBNP levels.
Conclusion
Refractory congestion, particularly when tissue fluid overload predominates, is a complex scenario in which diuretic treatment may not be able to achieve euvolemia. In our case, LVC, together with the use of diuretics, allowed the patient to reach a state of euvolemia. This therapy could have an increasing role in the management of patients with evidence of extravascular/tissue fluid overload but without intravascular overload.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
DP, FD and MCM actively participated in the management of the patient during admission, as well as in the search for new strategies for the management of refractory congestion. JN taught us the usefulness of the compression bandage of lower limbs and its hemodynamic implications. PP and JA helped us in researching the topic and in preparing the case well to be presented in a journal. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. de la Espriella R, Santas E, Zegri Reiriz I, Górriz JL, Cobo Marcos M, Núñez J. Quantification and treatment of congestion in heart failure: a clinical and pathophysiological overview. Nefrologia. (2022) 42(2):145–62. doi: 10.1016/J.NEFROE.2021.04.00
2. de la Espriella R, Cobo M, Santas E, Verbrugge FH, Fudim M, Girerd N, et al. Assessment of filling pressures and fluid overload in heart failure: an updated perspective. Rev Esp Cardiol (Engl Ed). (2023) 76(1):47–57. doi: 10.1016/J.REC.2022.07.009
3. ter Maaten J, Valente M, Damman K, Hillege H, Navis G, Voors A. Diuretic response in acute heart failure-pathophysiology, evaluation, and therapy. Nat Rev Cardiol. (2015) 12:184–92. doi: 10.1038/nrcardio.2014.215
4. McDonagh TA, Metra M, Adamo M, Baumbach A, Böhm M, Burri H, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42(36):3599–726. doi: 10.1093/EURHEARTJ/EHAB368
5. Andriessen A, Apelqvist J, Mosti G, Partsch H, Gonska C, Abel M. Compression therapy for venous leg ulcers: risk factors for adverse events and complications, contraindications – a review of present guidelines. J Eur Acad Dermatol Venereol. (2017) 31(9):1562–8. doi: 10.1111/JDV.14390
6. Urbanek T, Juśko M, Kuczmik WB. Compression therapy for leg oedema in patients with heart failure. ESC Heart Failure. (2020) 7(5):2012. doi: 10.1002/EHF2.12848
7. Bain RJI, Tan LB, Murray RG, Davies MK, Littler WA. Central haemodynamic changes during lower body positive pressure in patients with congestive cardiac failure. Cardiovasc Res. (1989) 23(10):833–7. doi: 10.1093/CVR/23.10.833
8. Dereppe H, Hoylaerts M, Renard M, Leduc O, Bernard R, Leduc A. Hemodynamic impact of pressotherapy. J Mal Vasc. (1990) 15(3):267–9.2212870
9. Wilputte F, Renard M, Venner JP, Strapart J. Hemodynamic response to multilayered bandages dressed on a lower limb of patients with heart failure. Eur J Lym. (2005) 15:1–4.
Keywords: heart failure and transplantation diuretic resistance, edema, heart failure, venous leg compression, lower limb compression bandaging
Citation: Collado Macián C, Pujol Pocull D, Dominguez F, López-Azor JC, Garcia-Pavia P, Nuñez J and Cobo Marcos M (2023) Case report: Alternative approach for management of refractory volume overload in heart failure: usefulness of venous leg compression. Front. Cardiovasc. Med. 10:1230980. doi: 10.3389/fcvm.2023.1230980
Received: 30 May 2023; Accepted: 15 September 2023;
Published: 29 September 2023.
Edited by:
Francesco Gentile, Institute of Life Sciences, Sant'Anna School of Advanced Studies, ItalyReviewed by:
Gennady G. Taradin, Rostov State Medical University, RussiaJuan Betuel Ivey-Miranda, Mexican Social Security Institute (IMSS), Mexico
© 2023 Collado Macián, Pujol Pocull, Dominguez, López-Azor, Garcia-Pavia, Nuñez and Cobo Marcos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Cobo Marcos bWFydGFjb2JvbWFyY29zQGhvdG1haWwuY29t