 Jakub S. Gąsior1*
Jakub S. Gąsior1* Marcel Młyńczak2*
Marcel Młyńczak2* Craig A. Williams3
Craig A. Williams3 Aleksandra Popłonyk4
Aleksandra Popłonyk4 Daria Kowalska4
Daria Kowalska4 Paulina Giezek4
Paulina Giezek4 Bożena Werner1
Bożena Werner1
- 1Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Warsaw, Poland
- 2Faculty of Mechatronics, Institute of Metrology and Biomedical Engineering, Warsaw University of Technology, Warsaw, Poland
- 3Public Health and Sports Sciences Department, Children’s Health and Exercise Research Centre, Faculty of Health and Life Sciences, University of Exeter Medical School, University of Exeter, Exeter, United Kingdom
- 4Department of Physiotherapy, Medical University of Warsaw, Warsaw, Poland
The interventions aimed at improving the levels of physical activity (PA) in children and adolescents diagnosed with heart disease did not produce the expected outcomes. Safe participation in sport activities proposed based on actual recommendations could be a solution to promote PA in this population. The aims of this study were to discover a causal diagram of sport participation in children and youth with heart disease and establish the factors that affect and are affected thereof through the use of questionnaires. Furthermore, the study aims to qualitatively assess the reliability of the constructed diagram in comparison with existing medical knowledge. The Greedy Fast Causal Inference method was employed to conduct a data-driven search of the directed acyclic graph that represents the causal relationships within the provided observational data. This causal discovery was performed using the Tetrad software. The analysis involved a cohort of 121 Caucasian patients (50 females) diagnosed with heart disease. The age range of the patients included in the study was 8–17 years. The study findings indicate that the participants engaged in sports presented significantly higher values of health-related quality of life (QoL) and motives for participating in physical and leisure activities. Age appears to be a cause of sport participation. Sport participation appears to be a cause of participation in physical education classes, which in turn appears to be a cause of higher enjoyment. Higher enjoyment appears to be a cause of other motives for participating in physical and leisure activities, as well as a higher score in terms of physical health. The causal diagram provided a graphical representation of the causal relationship between sport participation and better QoL with potential confounders for children and adolescents with heart disease that nearly coincided with the existing literature. Clinical trials should be designed to validate clinical utility of the presented causal diagram.
1. Introduction
Since the recommendations for physical activity (PA), recreational sport, and exercise training in pediatric patients with congenital heart disease (ConHD) were published a decade ago (1), a number of studies have assessed the PA level and the reported associations between higher PA levels and better health-related outcomes in this population (2–5). Interestingly, discrepant results exist regarding the differences in PA level between children with ConHD and healthy peers (6–8). The authors of a review on PA modification in youth with ConHD published in 2021 presented that 50% of the analyzed studies showed a lack of significant differences in PA levels between patients and age-matched healthy peers (6). Comparable PA levels of children with ConHD to normal children, however, higher than previously reported by others, were recently observed by authors from Belgium, who speculated that this could be attributed to their policy of motivating and encouraging children to participate in sports (9). Indeed, sport is one of the best investments for promoting PA (10), as it provides medical and psychosocial benefits for children and adolescents (11, 12). Sport participation could be a solution to promote PA in children and youth with ConHD as interventions aimed at improving PA levels in this population did not produce the expected outcomes (13–16). Nevertheless, despite the existence of published evidence- and practice-based guidelines for pediatric cardiac rehabilitation programs (17), as well as recommendations for exercise (18) and examination procedures that aim to ensure safe participation in sports for each individual with ConHD (1, 19–23), and positive consequences of sports participation in this group (24–26), recent studies continue to report instances where patients experience a lack of PA promotion and/or restriction on sport participation by physicians (27–30). In addition, parental overprotection, children's low self-efficacy and fear to exercise, lack of adequate information on PA clearance of the physical education teachers are listed as factors that limit sport participation in youth with ConHD (6, 14, 31).
Reviewing the barriers and facilitators contributing to children sports participation is important (32, 33), so that healthcare providers and parents may be able to enhance and promote sport activities in children with ConHD (26, 29, 34–36). Therefore, we aim to evaluate relationships (particularly in the causal sense) that can be discovered from the questionnaire responses regarding various factors. This can be accomplished using data-driven causal discovery methods, which are intended to search the causal structure [so-called directed causal diagrams, directed acyclic graph (DAG)] from observational data (37, 38). The aims of this pilot study are to discover a causal diagram of sport participation in children and adolescents with heart disease and establish the factors that affect and are affected thereof through the use of questionnaires (treated as observational data). Furthermore, the study aims to qualitatively assess the reliability of the constructed diagram in comparison with existing medical knowledge (addressed in the Discussion).
2. Method
2.1. Study design and population
The present study is reported in accordance with STROBE guidelines (39). The observational prospective study was conducted from January 2022 to January 2023. The study included a cohort of 121 patients, aged from 8 to 18 years, who voluntarily participated in the study during their routine pediatric follow-up visit. The study eliminated children with (a) impairments that hindered their ability to understand and/or respond to the items in the questionnaires, (b) non-cardiac diseases that prevented them from sport participation, and (c) without confirmed diagnosis. All the interviewed children completed the questionnaires under the supervision of one parent or legal guardian. This study is a part of the research project on assessment of determinants of PA levels in pediatric patients with heart disease.
2.2. Questionnaire
The team prepared a questionnaire consisting of closed-ended questions pertaining to demographic data (age, sex, place of residence, number of siblings), clinical cardiac diagnosis (ConHD, cardiac arrhythmia, cardiomyopathy, myocarditis), sport participation status of the patient (actual and before diagnosis with additional information such as type, duration, and frequency of the sport and duration of training session), patient's additional activities with potential influence on participation in sport activities (transport to school, participation in domestic chores, physical education classes, out-of-school additional activities, and spending free time: preferred place and companionship), parental education and sport participation status, and sleep disturbances. Table 1 presents all the data that were collected using the questionnaire.
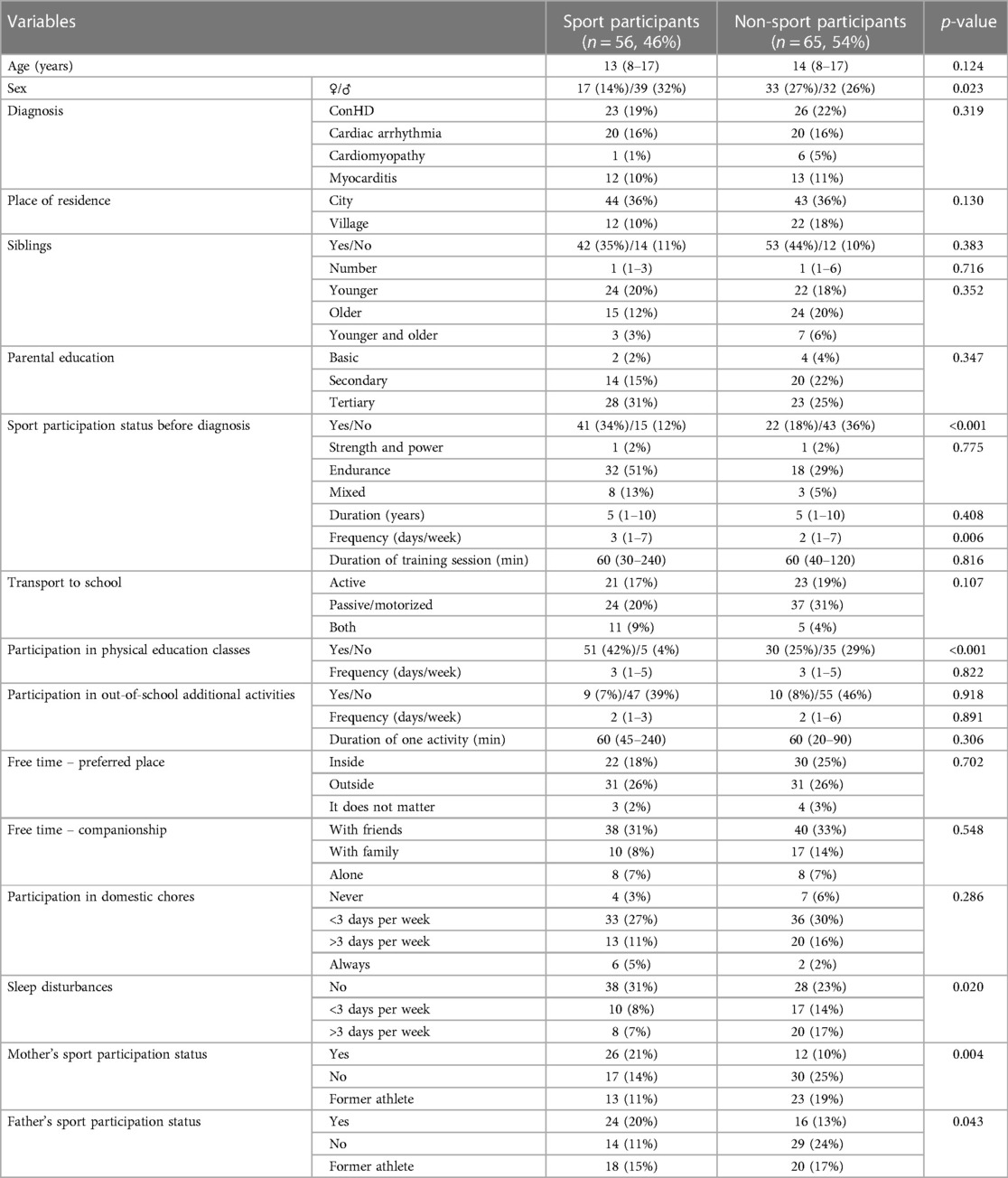
Table 1. Differences between the sport participants and non-sport participants groups.
2.3. Pediatric Quality of Life Inventory 4.0 Core Scales
The Health-related quality of life (HRQoL) was assessed using a Polish version of the Pediatric Quality of Life Inventory 4.0 (PedsQL™) Generic Core Scales questionnaire—a self-report version for children (8–12 years) and adolescents (13–18 years). The questionnaire consists of 23 items in four scales that assess the physical functioning, emotional functioning, social functioning, and school functioning. The items were scored on a 5-point Likert scale from 1 “Never a problem” to 5 “Almost always a problem.” The participants were asked how much of a problem each item has been during the past month. A higher score represented a better HRQoL (40).
2.4. Physical Activity and Leisure Motivation Scale—Youth
The Physical Activity and Leisure Motivation Scale—Youth (PALMS-Y) consists of 28 items with seven subscales (mastery, enjoyment, psychological condition, physical condition, appearance, affiliation, and competition/ego) measuring different types of motives for participating in physical and leisure activities. Each subscale consists of four items. The response format for all of the items is a 5-point Likert scale rated from 1 “Strongly disagree” to 5 “Strongly agree,” higher scores reflect the participant's experience of a higher level of that motive for participating in physical and leisure activities (41).
2.5. Statistics
The data-driven search of the DAG (causal discovery) was performed using the Greedy Fast Causal Inference (GFCI) technique for continuous variables. The GFCI approach is a combination of and improvement upon two algorithms:
• Fast Causal Inference (FCI) (42), which begins with a complete undirected graph.
• Fast Greedy Equivalence Search (FGES) (43), which starts with an empty graph, and adds iteratively needed edges, and then eliminates unnecessary ones in a graph.
The GFCI method uses the latter one (FGES) to find a “supergraph” (the skeleton of connections), and then the former (FCI) is utilized to prune the “supergraph” to find the final orientations (44).
This method can assess whether the relation is direct and whether there are any latent confounders between the two variables being analyzed.
The whole analysis was performed using Tetrad 6.5.3 software (45). The input data were the table with rows corresponding to the study participants and columns with various variables recorded from the questionnaire (as listed in subsequent lines in Tables 1, 2). All variables were stored as numeric values (so that the technique for continuous variable can be utilized), and the table was prepared in a way that no information regarding the column names and their respective meanings was provided for the analysis, and the order of the data columns and rows did not play any role.
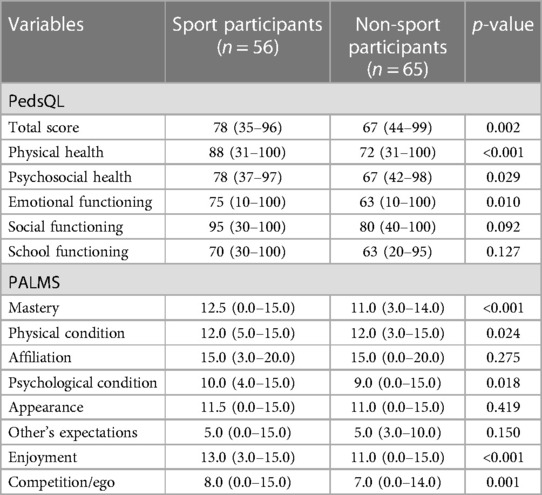
Table 2. Differences in PedsQL and PALMS between the sport participants and non-sport participants groups.
Then, we used default settings for the GFCI method:
• Cutoff for p-value (0.01).
• Penalty discount (2).
• Faithfulness assumed.
• Unlimited length for any discriminating path.
• The complete FCI rule set was not used.
• No bootstraps.
• Ensemble method: highest.
As a result, the output graph was created, and hidden column names were back uncovered in order to produce Figure 1.
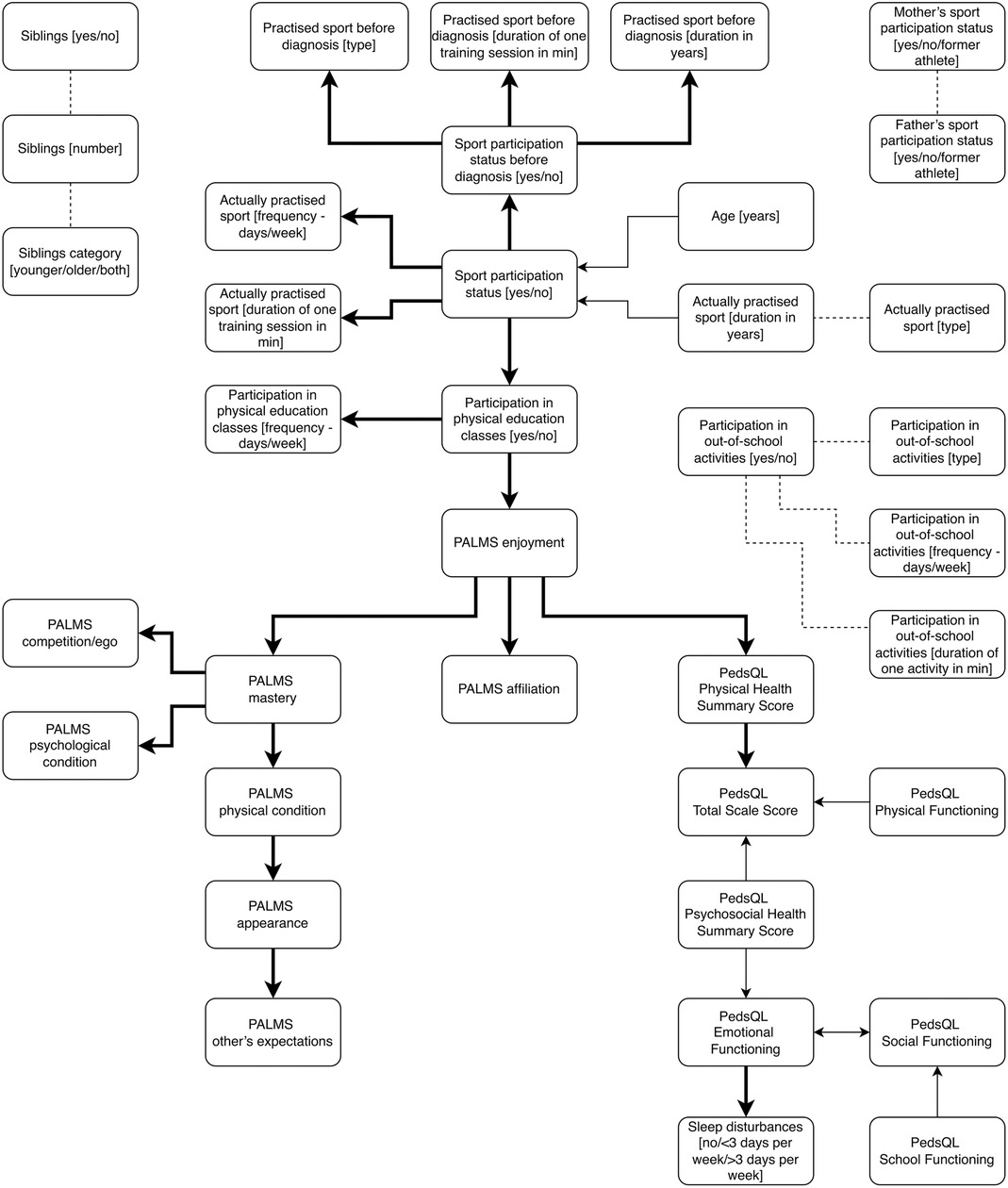
Figure 1. The causal diagram presenting the relationships between the variables collected using the questionnaires. The thickened and solid arrow from one variable to another means the former appears to be the direct cause of the latter, and there is no latent confounder between them. A thin and solid arrow means either the input variable is a cause of the output one or there is an unmeasured confounder. The thin and dashed line represents the case in which one of the following holds: first variable is a cause of another, the opposite relationship, there is an unmeasured confounder, both the first relation with the unmeasured confounder, or both the second relation with the unmeasured confounder.
The Shapiro–Wilk test was used to test the data distribution for normality. The U-Mann–Whitney non-parametric test was utilized to compare the medians of the two groups (unpaired case). The χ2 test was used to compare the frequencies between groups. The level of statistical significance was set at p < 0.05 (STATISTICA 13, StatSoft Inc., Tulsa, OK, USA).
3. Results
There were 121 completed questionnaires received from Caucasian patients (n = 50 females) diagnosed with heart disease with a median age of 13 years (range: 8–17). The descriptive statistics of all data that were collected from the questionnaires are presented in Table 1. Table 2 presents the PedsQL and PALMS scores. There were 56 (46%) sport participants and 65 (54%) non-sport participants. A total of 22 (18%) patients had stopped their participation in sport due to their diagnosis. Among the groups of sport participants and non-sport participants, there were five and 25 patients, respectively, who had medical exemptions from participating in physical education classes.
The study found that sport participants had a higher proportion of boys (p < 0.05) and children who engaged in sports prior to diagnosis (p < 0.001), who participated in physical education classes (p < 0.001), with a lower number of nights with sleep disturbances (p < 0.05), and parents that participated in sport activities (p < 0.05) than the non-sport participants. Sport participants practiced endurance sports (n = 45), strength and power sports (n = 4), and mixed sports (n = 7). They practiced a sport with a median of three times per week (range: 1–7). In addition, the median duration of one training session was 60 min (range: 30–240). The reasons for participation in sport were as follows: because I like it/it is my passion (n = 41), to take care of the health and body (n = 29), to spend time with friends (n = 26), to relieve emotions or stress (n = 16), to spend time with parents (n = 12), and because my parents encourage me (n = 2).
Sport participants presented significantly higher values of HRQoL in total score, physical health, psychosocial health, and emotional functioning. In addition, they exhibited significantly higher values in PALMS-Y subscales: mastery, physical condition, psychological condition, enjoyment, and competition/ego (see Table 2).
Figure 1 presents the causal diagram as a result from the GFCI method, estimated in a data-driven scenario. From the perspective of the study subject, some relationships should be particularly indicated:
(i) Age appears to be a cause of sport participation in pediatric patients with heart disease. Sport participants were younger.
(ii) Sport participation appears to be a cause of participation in sport activities prior to diagnosis and participation in physical education classes—this appears to be a cause of higher intrinsic motive—enjoyment.
(iii) Higher patients’ enjoyment appears to be a cause of higher affiliation and mastery motives but also higher physical health score.
(iv) Both higher physical and psychosocial health scores appear to be causes of better HRQoL (total PedsQL score).
(v) Higher psychosocial health score appears to be a cause of higher emotional functioning.
(vi) Lower emotional functioning appears to be a cause of sleep disturbances.
The variables included in the questionnaire that were found to be causally unrelated with other variables were sex, diagnosis, place of residence, parental education, reasons for participation in sport, place and/or companionship for spending free time, transport to school, and participation in domestic chores.
4. Discussion
In this pilot study, the idea was to discover the causal diagram of factors that may affect and be affected by sport participation in children and adolescents with heart disease and to assess the reliability of the diagram by comparing it with the existing literature. Based on the diagram, sport participation appears to be a cause of participation in physical education classes, and this practice appears to be a cause of higher enjoyment. Higher patients’ enjoyment appears to be a cause of other motives for participating in physical and leisure activities, as well as a higher physical health score. Importantly, emotional functioning appears to be a cause of sleep disturbances. Among the analyzed variables, only age appears to be a cause of sport participation, however, with unmeasured confounder(s). It is worth mentioning that other factors that may influence on the likelihood of sport participation in pediatric patients with heart disease such as sex, diagnosis, or parents’ sport participation status were found to be causally unrelated with the sport participation status of the patients. The heterogeneity of the group may have impacted these results.
The GFCI method employed in our study successfully identified a graph of sport participation in pediatric patients with heart disease that nearly coincided with the existing literature. There are several original studies on sport participation in pediatric patients with ConHD, mostly assessing its association with QoL. The correlation between beliefs in self-efficacy and involvement in sport and PA was shown to be stronger in adolescents than the severity of the disease (46). Higher self-efficacy, male gender, and participation in physical education classes were associated with a higher likelihood of engagement in PA (34). Patients who exercised more often (school classes or fitness centers) were more likely to participate in leisure or competitive sports (25). Participation in sports was associated with improved exercise capacity, emotional, psychological, and social wellbeing, and generally with a higher QoL (47, 48). An improvement in health status has been observed after a 3-day multi-sports camp (49). Participating in recreational sport encouraged patients to be more intrinsically motivated to engage in PA—patients emphasized their enjoyment of PA as a primary source of motivation (26). The findings from existing literature suggest the occurrence of closed-loop interaction between higher self-efficacy and/or higher intrinsic motivation and higher involvement in sport and PA in pediatric patients with ConHD. Understanding the patient's motivation for PA or sport can be helpful to a clinician or a physical therapist in order to stimulate participation in PA and/or identify suitable forms of activity. To assess an individual's goal-oriented motivation, the Physical Activity and Leisure Motivation Scale was developed (41). The scale measures eight types of motivation—enjoyment and mastery factors, significantly higher in group of sport participants in our study, can be considered as intrinsic motivation, while the other six factors describe extrinsic motivation based on the self-determination theory (50).
There is an urgent need for global action aimed at decreasing levels of insufficient activity in both healthy children and pediatric patients with chronic conditions and disability (51). Proposed interventions aimed at improving PA levels in children and youth with ConHD did not produce the expected outcomes (13–16). Learning causal diagram discovered a priori with longitudinal data providing extensive prior knowledge may be a helpful technique in establishing the kind and dose of sport activities as a potential solution for promoting PA in this population.
Causal diagrams based on observational data have been utilized in Alzheimer's pathophysiology (52). The authors constructed a “gold-standard” causal structure graph based on the existing literature. Then, they applied three algorithms to discover this causal structure from observational data. FGES, the method used in the presented study, managed to (almost perfectly) recover the “gold-standard” graph. In addition, the authors provided a detailed guideline on how causal discovery algorithm can be applied to discover high-quality causal relationships (52). Recently (2023), Huie et al. (53) discussed chronic low back pain as a “Big Data” problem and identified how data-driven method that uses artificial intelligence and high dimensional datasets (constraint-based: FCI and score-based: FGES algorithms) to identify causal structures may help better understand causal factors for low back pain, guide clinical practice, and improve outcomes.
The causal diagram was presented as solely the data-driven output of the GFCI method, without supplementing it with any specific medical knowledge or experience-based intuition. It seemed that some relations had not been “detected” by a method (we were aware of such a possibility prospectively), even if simple comparisons (presented in Table 1) are found as significant. Perhaps, these relationships may be further emphasized with a similar analysis conducted on a larger population. As with all studies, there are a number of limitations to consider. These include the limited dataset used for identifying DAG (no sensitivity analysis could be conducted), heterogeneity of a small study group, and the failure to differentiate between different types of sports, i.e., competitive or recreational/leisure. The inclusion of participants across a wide age range in the study group should be also considered as a study limitation—drop out from sports is increasing with increasing age during childhood and adolescence (54). The directed edges in the discovered DAG are being interpreted causally. Accordingly, the edge Age → Sport participation status in the graph can be interpreted as age causally influences the sport participation status in pediatric patients with heart disease. The results of the direct comparison showed that sport participants were younger; however, as this relation is not separated in the DAG, it does not inform regarding the extent to which a change in age would causally affect sport participation status.
One advantage of conducting this pilot study is that it will pave the way for future research involving a larger population of pediatric patients with heart disease and will include more factors that have the potential to affect and/or might be a consequence of sport participation, such as PA level, obesity status, cardio-respiratory function, health-related physical fitness, cardiac module of PedsQL, and parental support. Then the objective would be to: (i) identify the appropriate set of variables to minimize bias due to potential confounding associations and (ii) to generate hypotheses to be tested (as interventions in the causal sense) in future trials.
5. Conclusion
In conclusion, causal diagram provided a graphical representation of the causal relationship between sport participation and better QoL with potential confounders for children and adolescents with heart disease that nearly coincided with the existing knowledge. However, it is important to exercise caution in interpreting these findings, as there are certain limitations that have been mentioned. Clinical trials should be designed to validate the clinical utility of the presented causal diagram. The optimal dose of PA (55) and promotion strategies still remain a challenge. Pediatric cardiologists should propose appropriate sport activities for children and adolescents with heart disease as a strategy for promoting active lifestyles to improve QoL.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bioethical Committee of the Medical University of Warsaw (AKBE/95/2021). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
Conceptualization: JG and MM; formal analysis: JG and MM; investigation: JG, AP, DK, and PG; writing – original draft: JG, MM, AP, DK, and PG; writing – review & editing: CW and BW. All authors contributed to the article and approved the submitted version.
Funding
This research was partly supported by a statutory grant to the Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Poland (grant number: 10/Z/GW/N/21).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Takken T, Giardini A, Reybrouck T, Gewillig M, Hövels-Gürich HH, Longmuir PE, et al. Recommendations for physical activity, recreation sport, and exercise training in paediatric patients with congenital heart disease: a report from the exercise, basic & translational research section of the European Association of Cardiovascular Prevention and Rehabilitation, the European Congenital Heart and Lung Exercise Group, and the Association for European Paediatric Cardiology. Eur J Prev Cardiol. (2012) 19(5):1034–65. doi: 10.1177/1741826711420000
2. Lopez JR, Voss C, Kuan MTY, Hemphill NM, Sandor GGS, Harris KC. Physical activity is associated with better vascular function in children and adolescents with congenital heart disease. Can J Cardiol. (2020) 36(9):1474–81. doi: 10.1016/j.cjca.2019.12.019
3. Härtel JA, Herberg U, Jung T, Winkler C, Breuer J, Müller N. Physical activity and heart rate monitoring in Fontan patients—should we recommend activities in higher intensities? PLoS One. (2020) 15(1):e0228255. doi: 10.1371/journal.pone.0228255
4. Brudy L, Meyer M, Oberhoffer R, Ewert P, Müller J. Move more—be happier? Physical activity and health-related quality of life in children with congenital heart disease. Am Heart J. (2021) 241:68–73. doi: 10.1016/j.ahj.2021.07.004
5. Callegari A, Faeth K, Pfammatter C, Jung R, Berger F, Burkhardt B, et al. Physical activity in Fontan patients relates to quality of life and sleep quality. Front Cardiovasc Med. (2022) 9:915810. doi: 10.3389/fcvm.2022.915810
6. van Deutekom AW, Lewandowski AJ. Physical activity modification in youth with congenital heart disease: a comprehensive narrative review. Pediatr Res. (2021) 89(7):1650–8. doi: 10.1038/s41390-020-01194-8
7. Brudy L, Meyer M, Garcia-Cuenllas L, Oberhoffer R, Hager A, Ewert P, et al. Objective physical activity assessment in clinical congenital heart disease research: a systematic review on study quality, methodology, and outcomes. Cardiology. (2021) 146(2):240–52. doi: 10.1159/000512186
8. Acosta-Dighero R, Torres-Castro R, Rodríguez-Núñez I, Rosales-Fuentes J, Vilaró J, Fregonezi G, et al. Physical activity assessments in children with congenital heart disease: a systematic review. Acta Paediatr. (2020) 109(12):2479–90. doi: 10.1111/apa.15478
9. Zaqout M, Vandekerckhove K, De Wolf D, Panzer J, Bové T, François K, et al. Determinants of physical fitness in children with repaired congenital heart disease. Pediatr Cardiol. (2021) 42(4):857–65. doi: 10.1007/s00246-021-02551-y
10. Lee JE, Pope Z, Gao Z. The role of youth sports in promoting children’s physical activity and preventing pediatric obesity: a systematic review. Behav Med. (2018) 44(1):62–76. doi: 10.1080/08964289.2016.1193462
11. Logan K, Cuff S, Council on Sports Medicine and Fitness. Organized sports for children, preadolescents, and adolescents. Pediatrics. (2019):e20190997. doi: 10.1542/peds.2019-0997
12. Ostrzyżek-Przeździecka K, Panczyk M, Bronikowski M, Gąsior JS, Feleszko W. Association of low physical activity with higher respiratory tract infections frequency among pre-school children. Pediatr Res. (2023) 94(2):594–602. doi: 10.1038/s41390-022-02436-7
13. Klausen SH, Andersen LL, Søndergaard L, Jakobsen JC, Zoffmann V, Dideriksen K, et al. Effects of eHealth physical activity encouragement in adolescents with complex congenital heart disease: the PReVaiL randomized clinical trial. Int J Cardiol. (2016) 221:1100–6. doi: 10.1016/j.ijcard.2016.07.092
14. Caterini JE, Campisi ES, Cifra B. Physical activity promotion in pediatric congenital heart disease: are we running late? Can J Cardiol. (2020) 36(9):1406–16. doi: 10.1016/j.cjca.2020.07.003
15. Williams CA, Wadey C, Pieles G, Stuart G, Taylor RS, Long L. Physical activity interventions for people with congenital heart disease. Cochrane Database Syst Rev. (2020) 10(10):CD013400. doi: 10.1002/14651858.CD013400.pub2
16. Lin PJ, Fanjiang YY, Wang JK, Lu CW, Lin KC, Cheong IM, et al. Long-term effectiveness of an mHealth-tailored physical activity intervention in youth with congenital heart disease: a randomized controlled trial. J Adv Nurs. (2021) 77(8):3494–506. doi: 10.1111/jan.14924
17. Tran D, Maiorana A, Ayer J, Lubans DR, Davis GM, Celermajer DS, et al. Recommendations for exercise in adolescents and adults with congenital heart disease. Prog Cardiovasc Dis. (2020) 63(3):350–66. doi: 10.1016/j.pcad.2020.03.002
18. Tikkanen AU, Vova J, Holman L, Chrisman M, Clarkson K, Santiago R, et al. Core components of a rehabilitation program in pediatric cardiac disease. Front Pediatr. (2023) 11:1104794. doi: 10.3389/fped.2023.1104794
19. Budts W, Pieles GE, Roos-Hesselink JW, de la Garza MS, D’Ascenzi F, Giannakoulas G, et al. Recommendations for participation in competitive sport in adolescent and adult athletes with congenital heart disease (CHD): position statement of the sports cardiology & exercise section of the European Association of Preventive Cardiology (EAPC), the European Society of Cardiology (ESC) working group on adult congenital heart disease and the sports cardiology, physical activity and prevention working group of the Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. (2020) 41(43):4191–9. doi: 10.1093/eurheartj/ehaa501
20. Cantinotti M, Giordano R, Assanta N, Murzi B, Melo M, Franchi E, et al. Strengths, limitations, and geographical discrepancies in the eligibility criteria for sport participation in young patients with congenital heart disease. Clin J Sport Med. (2018) 28(6):540–60. doi: 10.1097/JSM.0000000000000474
21. Hirth A, Reybrouck T, Bjarnason-Wehrens B, Lawrenz W, Hoffmann A. Recommendations for participation in competitive and leisure sports in patients with congenital heart disease: a consensus document. Eur J Cardiovasc Prev Rehabil. (2006) 13(3):293–9. doi: 10.1097/01.hjr.0000220574.22195.d6
22. Maron BJ, Chaitman BR, Ackerman MJ, Bayés de Luna A, Corrado D, Crosson JE, et al. Recommendations for physical activity and recreational sports participation for young patients with genetic cardiovascular diseases. Circulation. (2004) 109(22):2807–16. doi: 10.1161/01.CIR.0000128363.85581.E1
23. Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. (2021) 42(1):17–96. doi: 10.1093/eurheartj/ehaa605
24. Voss C, Duncombe SL, Dean PH, de Souza AM, Harris KC. Physical activity and sedentary behavior in children with congenital heart disease. J Am Heart Assoc. (2017) 6(3):e004665. doi: 10.1161/JAHA.116.004665
25. Rato J, Sousa A, Cordeiro S, Mendes M, Anjos R. Sports practice predicts better functional capacity in children and adults with Fontan circulation. Int J Cardiol. (2020) 306:67–72. doi: 10.1016/j.ijcard.2019.11.116
26. Blais AZ, Lougheed J, Yaraskavitch J, Adamo KB, Longmuir PE. “I really like playing games together”: understanding what influences children with congenital heart disease to participate in physical activity. Child Care Health Dev. (2020) 46(4):457–67. doi: 10.1111/cch.12754
27. Williams CA, Gowing L, Horn R, Stuart AG. A survey of exercise advice and recommendations in United Kingdom paediatric cardiac clinics. Cardiol Young. (2017) 27(5):951–6. doi: 10.1017/S1047951116002729
28. Siaplaouras J, Niessner C, Helm PC, Jahn A, Flemming M, Urschitz MS, et al. Physical activity among children with congenital heart defects in Germany: a nationwide survey. Front Pediatr. (2020) 8:170. doi: 10.3389/fped.2020.00170
29. Longmuir PE, Corey M, McCrindle BW. Interactions with home and health environments discourage physical activity: reports from children with complex congenital heart disease and their parents. Int J Environ Res Public Health. (2021) 18(9):4903. doi: 10.3390/ijerph18094903
30. Blanchard J, McCrindle BW, Longmuir PE. The impact of physical activity restrictions on health-related fitness in children with congenital heart disease. Int J Environ Res Public Health. (2022) 19(8):4426. doi: 10.3390/ijerph19084426
31. Moola F, Faulkner GE, Kirsh JA, Kilburn J. Physical activity and sport participation in youth with congenital heart disease: perceptions of children and parents. Adapt Phys Activ Q. (2008) 25(1):49–70. doi: 10.1123/apaq.25.1.49
32. Somerset S, Hoare DJ. Barriers to voluntary participation in sport for children: a systematic review. BMC Pediatr. (2018) 18(1):47. doi: 10.1186/s12887-018-1014-1
33. Carbone PS, Smith PJ, Lewis C, LeBlanc C. Promoting the participation of children and adolescents with disabilities in sports, recreation, and physical activity. Pediatrics. (2021) 148(6):e2021054664. doi: 10.1542/peds.2021-054664
34. Kwon SJ, Choi EK, Lee KH, Im YM. Factors influencing physical activity in adolescents with complex congenital heart disease. Child Health Nurs Res. (2019) 25(3):262–72. doi: 10.4094/chnr.2019.25.3.262
35. Majnemer A, Rohlicek C, Dahan-Oliel N, Sahakian S, Mazer B, Maltais DB, et al. Participation in leisure activities in adolescents with congenital heart defects. Dev Med Child Neurol. (2020) 62(8):946–53. doi: 10.1111/dmcn.14422
36. Bay A, Lämås K, Berghammer M, Sandberg C, Johansson B. Enablers and barriers for being physically active: experiences from adults with congenital heart disease. Eur J Cardiovasc Nurs. (2021) 20(2):276–84. doi: 10.1177/1474515120963314
37. Ramanan N, Natarajan S. Causal learning from predictive modeling for observational data. Front Big Data. (2020) 3:535976. doi: 10.3389/fdata.2020.535976
38. Glymour C, Zhang K, Spirtes P. Review of causal discovery methods based on graphical models. Front Genet. (2019) 10:524. doi: 10.3389/fgene.2019.00524
39. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. (2007) 4(10):e296. doi: 10.1371/journal.pmed.0040296
40. Varni JW, Burwinkle TM, Seid M, Skarr D. The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambul Pediatr. (2003) 3(6):329–41. doi: 10.1367/1539-4409(2003)003%3C0329:tpaapp%3E2.0.co;2
41. Kueh YC, Abdullah N, Kuan G, Morris T, Naing NN. Testing measurement and factor structure invariance of the physical activity and leisure motivation scale for youth across gender. Front Psychol. (2018) 9:1096. doi: 10.3389/fpsyg.2018.01096
42. Spirtes P, Glymour C, Scheines R. Causation, prediction, and search. New York: Springer-Verlag (1993). Lecture Notes in Statistics.
43. Ramsey J, Glymour M, Sanchez-Romero R, Glymour C. A million variables and more: the fast greedy equivalence search algorithm for learning high-dimensional graphical causal models, with an application to functional magnetic resonance images. Int J Data Sci Anal. (2017) 3(2):121–9. doi: 10.1007/s41060-016-0032-z
44. Ogarrio JM, Spirtes P, Ramsey J. A hybrid causal search algorithm for latent variable models. JMLR Workshop Conf Proc. (2016) 52:368–79.28239434
45. Ramsey JD, Zhang K, Glymour M, Romero RS, Huang B, Ebert-Uphoff I, et al. Tetrad—a toolbox for causal discovery. Proceedings of the 8th international workshop in climate informatics (2018).
46. Bar-Mor G, Bar-Tal Y, Krulik T, Zeevi B. Self-efficacy and physical activity in adolescents with trivial, mild, or moderate congenital cardiac malformations. Cardiol Young. (2000) 10(6):561–6. doi: 10.1017/s1047951100008829
47. Knowles RL, Day T, Wade A, Bull C, Wren C, Dezateux C, et al. Patient-reported quality of life outcomes for children with serious congenital heart defects. Arch Dis Child. (2014) 99(5):413–9. doi: 10.1136/archdischild-2013-305130
48. Dean PN, Gillespie CW, Greene EA, Pearson GD, Robb AS, Berul CI, et al. Sports participation and quality of life in adolescents and young adults with congenital heart disease. Congenit Heart Dis. (2015) 10(2):169–79. doi: 10.1111/chd.12221
49. Moons P, Barrea C, Suys B, Ovaert C, Boshoff D, Eyskens B, et al. Improved perceived health status persists three months after a special sports camp for children with congenital heart disease. Eur J Pediatr. (2006) 165(11):767–72. doi: 10.1007/s00431-006-0171-7
50. Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. (2012) 9:78. doi: 10.1186/1479-5868-9-78
51. Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. (2020) 4(1):23–35. doi: 10.1016/S2352-4642(19)30323-2
52. Shen X, Ma S, Vemuri P, Simon G, Alzheimer’s Disease Neuroimaging Initiative. Challenges and opportunities with causal discovery algorithms: application to Alzheimer’s pathophysiology. Sci Rep. (2020) 10(1):2975. doi: 10.1038/s41598-020-59669-x
53. Huie JR, Vashisht R, Galivanche A, Hadjadj C, Morshed S, Butte AJ, et al. Toward a causal model of chronic back pain: challenges and opportunities. Front Comput Neurosci. (2023) 16:1017412. doi: 10.3389/fncom.2022.1017412
54. Vella SA, Schweickle MJ, Sutcliffe JT. Prevalence of drop-out from organised extracurricular sports and associations with body fat percentage during childhood and adolescence. BMJ Open Sport Exerc Med. (2020) 6(1):e000751. doi: 10.1136/bmjsem-2020-000751
Keywords: causal diagram, sport, children, adolescents, heart disease, heart defects, pediatric patients
Citation: Gąsior JS, Młyńczak M, Williams CA, Popłonyk A, Kowalska D, Giezek P and Werner B (2023) The discovery of a data-driven causal diagram of sport participation in children and adolescents with heart disease: a pilot study. Front. Cardiovasc. Med. 10:1247122. doi: 10.3389/fcvm.2023.1247122
Received: 25 June 2023; Accepted: 6 November 2023;
Published: 21 November 2023.
Edited by:
Inga Voges, University Medical Center Schleswig-Holstein, GermanyReviewed by:
Gottfried Greve, University of Bergen, NorwayLee Pyles, West Virginia University, United States
© 2023 Gąsior, Młyńczak, Williams, Popłonyk, Kowalska, Giezek and Werner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jakub S. Gąsior amFrdWIuZ2FzaW9yQHd1bS5lZHUucGw= Marcel Młyńczak bWFyY2VsLm1seW5jemFrQHB3LmVkdS5wbA==