 Wendy Mouradian
Wendy Mouradian Janice Lee3
Janice Lee3 Martha Somerman
Martha Somerman- 1School of Dentistry, University of Washington, Seattle, WA, United States
- 2The Santa Fe Group, New York, NY, United States
- 3National Institute of Dental and Craniofacial Research, National Institutes of Health, Bethesda, MD, United States
- 4Independent Researcher, New York, NY, United States
- 5National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, Bethesda, MD, United States
The past decade has seen marked increases in research findings identifying oral-systemic links. Yet, much of dental research remains poorly integrated with mainstream biomedical research. The historic separation of dentistry from medicine has led to siloed approaches in education, research and practice, ultimately depriving patients, providers, and policy makers of findings that could benefit overall health and well-being. These omissions amount to lost opportunities for risk assessment, diagnosis, early intervention and prevention of disease, increasing cost and contributing to a fragmented and inefficient healthcare delivery system. This perspective provides examples where fostering interprofessional research collaborations has advanced scientific understanding and yielded clinical benefits. In contrast are examples where failure to include dental research findings has limited progress and led to adverse health outcomes. The impetus to overcome the dental-medical research divide gains further urgency today in light of the coronavirus pandemic where contributions that dental research can make to understanding the pathophysiology of the SARS-CoV-2 virus and in diagnosing and preventing infection are described. Eliminating the research divide will require collaborative and trans-disciplinary research to ensure incorporation of dental research findings in broad areas of biomedical research. Enhanced communication, including interoperable dental/medical electronic health records and educational efforts will be needed so that the public, health care providers, researchers, professional schools, organizations, and policymakers can fully utilize oral health scientific information to meet the overall health needs of the public.
Introduction
Biomedical research grew dramatically after World War II with the generation of new antibiotics, the unraveling of the genetic code, the birth of molecular biology, and the first successful organ transplants, among major milestones. The National Institutes of Health (NIH) expanded accordingly, but in ways reflecting traditional clinical specialties that divide the body into disparate organs and systems, a division that perpetuates the sharp divide between dentistry and medicine. But the very discoveries and technologies that are rapidly transforming our understanding of life and life processes demand we put the body back together again (Table 1). For example, we know that a gene associated with a particular organ can manifest in other organs, or turn other genes on or off, and we know that a drug targeted to a particular pathogen can wreak havoc elsewhere in the body. But what is also now clear is that the body is even more extensively and deeply connected than had been thought. The coronavirus pandemic is a case in point. A member of a family of viruses typically associated with respiratory symptoms, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is responsible for the coronavirus disease 2019 (COVID-19), can result in fatigue, loss of smell and taste, gastrointestinal problems, cognitive deficits, depression, life-threatening pneumonia, neurological disorders and symptoms that can persist in some individuals long after initial infection (15–18). Yet the mouth and oral health considerations continue to be treated as a class by themselves, separate from the rest of the body, ignored and omitted from research studies large and small. This gap results in missed opportunities to reveal important oral-systemic interactions or explain how other parts of the body regulate functions in the mouth. This perspective provides examples of the consequences resulting from the lack of integration and the benefits gained when oral-systemic integration is in place. This is a perspective, not a review, but we provide additional references to a few scientific papers and reviews within the last 6 years, which expand on the examples provided here (19–27).
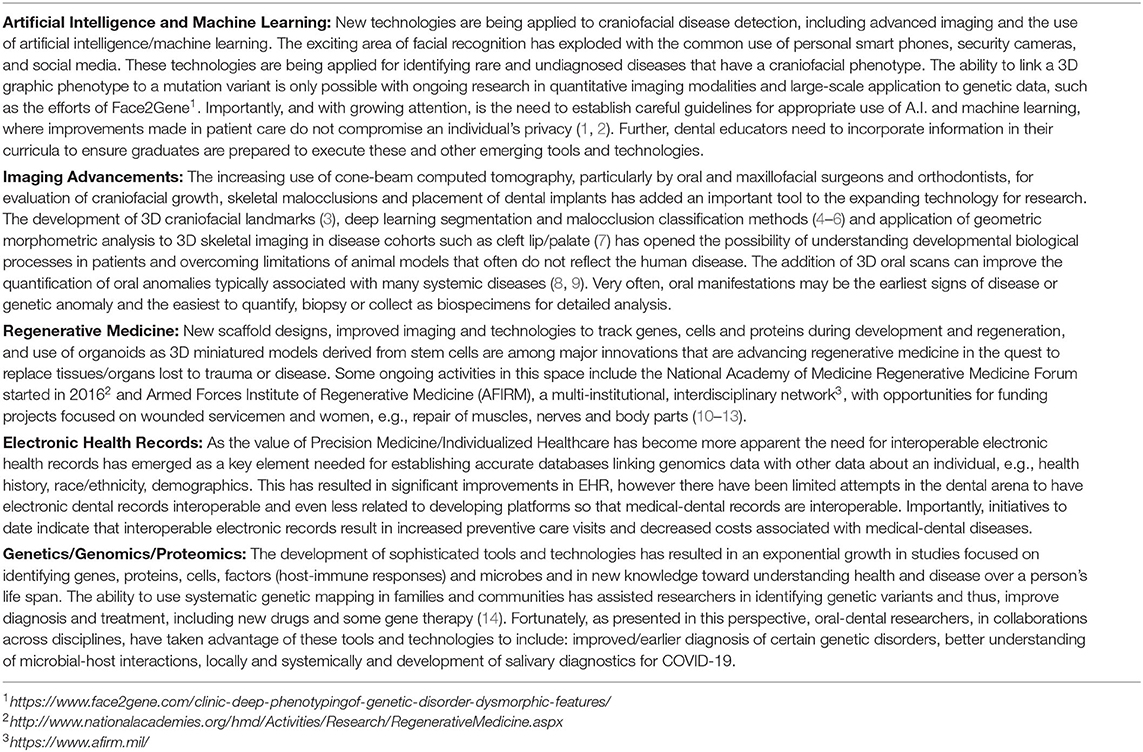
Table 1. Tools and technologies informing clinical practice and oral health outcomes.
The Failure to Connect
Not Really All Parts of Us, but Getting Close
The goal of this innovative Precision Medicine initiative, launched by the NIH in 2015, named All of Us, is to build one of the most diverse health databases in history by inviting one million Americans, 18 and older, of all backgrounds, to voluntarily submit biologic samples and personal information to enable investigators to learn how biology, lifestyle and environment affect health (28). Participants are asked to answer surveys; they can submit data from wearable measuring devices and allow researchers access to their electronic health records (29). Early on, to get the program going, they were not able to include dental questions in the survey. More recently, two dental questions were added i.e., have you seen a dentist in the last 12 months and do you have access to dental care, with plans to include a more comprehensive oral-dental history, plus collecting salivary samples within the coming year, behind schedule due to the pandemic. We are optimistic that oral-dental health data will be included within the context of total health. On another positive note, UK Biobank now includes collecting salivary samples along with an oral health survey (30).
Incompatible EHRs
The goal of integrated oral and overall health data from All of Us is exacerbated by the general lack of interoperability between medical and dental electronic health records making it difficult to obtain an individual's inclusive dental and medical history. Exclusion of oral health data can delay diagnoses and treatment by missing characteristic oral signs of particular conditions, syndromes and diseases, with repercussions on overall health over the lifetime. Establishing a fully integrated dental-medical electronic health record must be a priority to ensure research advances provide optimal clinical care and guidance (28, 29). We recognize the current siloed approaches are on both the medical and dental side. Many dental communities have not fully embraced interprofessional models of teaching and clinical practice, favoring the technical aspects of dentistry. We need buy-in from all healthcare teams to be successful in delivering the concepts discussed in this perspective.
Childhood Caries Risk
Failure to include oral health in other large genomic-phenomic studies also limits understanding of oral conditions directly. For example, childhood dental caries remains the number one chronic disease in children, more prevalent than asthma (30). This state of affairs is amplified by health disparities that disproportionately affect poorer groups, minorities and other underserved and vulnerable populations who lack access to care (31). While some progress has been made toward identifying genetic contributions to periodontal disease and caries (2), failure to include oral health research in large-scale genomic-phenomic initiatives of gene-environment interactions impedes mechanistic understanding of caries risk in children.
Oral Health in Aging
Biological aging is considered a normal physiological process known to be influenced by an individual's risk to include, but not limited to, hormonal changes, chronic inflammatory diseases, diet (nutrition/sugar intake/alcohol), and smoking. There is increasing evidence that periodontal disease, as a chronic infection with persistent inflammation locally and systemically, may contribute to unhealthy aging (32–35). The increasing evidence that severity of periodontal disease has a negative effect on telomere length, where decrease in telomere length is a measure of biological aging, highlights the importance of including oral health status as part of determination of one's total health across a life span (36). Another area needing attention relates to salivary flow with aging. Studies have demonstrated that even though there is some decrease in salivation and a change in salivary composition with aging, it is adequate in healthy aging individuals (37, 38). However, the onset of systemic diseases and the addition of many commonly used drugs as well as radiation therapies can irritate oral tissues and directly cause xerostomia, raising the risk of caries. Yet, how many providers recognize these risks or ask their patients if their various therapies or drug regimens have had any effects on their oral/dental tissues? The inclusion of oral health in aging research is critical to better serve older individuals and develop therapies to preserve oral health.
The Need for Dental Scientists in Clinical Trials
The knowledge dental scientists bring to characteristics of oral tissues can provide valuable clues in diagnosing systemic diseases as well as predicting and elucidating the impact of new therapies on the oral cavity. Recent examples of clinical trials conducted without input from dental scientists illustrate the delays in diagnosis and potential harms in patient outcomes.
Dental Phenotypes
Individuals with genetic mutations often exhibit specific dental phenotypes (observable traits), which may be seen on oral examination. For example, individuals with hypophosphatasia (HPP), caused by mutations in the alkaline phosphatase gene, often have defects in the formation of tooth root cementum, dentin and enamel. Yet clinical trials using alkaline phosphatase enzyme replacement therapy for HPP failed to include an examination of participants' teeth (39). The effects of such therapies on the teeth are just now being analyzed. Several other disorders where oral tissues are now included in the research study have resulted in recognition of substantial oral tissue phenotypes that can lead to more rapid and earlier diagnosis and treatment (8, 40–42).
New Immuno-Cancer Treatments
Other examples of dental contributions to clinical studies and trials are related to broader effects of new therapies on oral tissues. For example, many drugs may affect salivary gland function, alter tooth color, affect mucosal function or cause oral lesions—at times so severe that patients must discontinue therapy. As a result, new drug treatments for a variety of serious disorders require the involvement of oral health scientists as key members of the research team at the outset. The development of immune checkpoint inhibitors (ICI) to treat cancers has identified the concerning side effect of profound xerostomia after a few weeks or months of treatment (43). While this has encouraged research on how ICI disrupts salivary gland function, it underscores why inclusion of dentist scientists is critical.
Osteonecrosis of the Jaw
Without dental-medical integration the oral side effects of new therapies can take years to fathom. This was the case for medication-related osteonecrosis of the jaw (44). It has now been established that anti-resorptive drugs used not only to treat osteoporosis but also some cancers, can result in severe jaw problems as well as other anomalies of bone metabolism. The research confirming cause and effect was the result of intense cross collaboration between dental and non-dental researchers including animal studies, case reports and patient records. It is currently part of clinical endocrinology guidelines to consult a dentist when initiating these therapies, especially cancer therapies (45). Similar best clinical practices include obtaining early dental consultation prior to the initiation of head and neck radiation therapy (for oral cancers). This integration of dental with medical care has lowered the risk of the devastating side effect of osteoradionecrosis of the jaw and improved the quality of life for patients undergoing radiation therapy.
Hospital Acquired Pneumonia
Hospital acquired pneumonia (HAP) accounts for 25 percent of all hospital-acquired infections (46) and presents a serious risk for patients hospitalized with COVID-19 (47). Studies conducted in a veterans' hospital setting have supplied evidence that non-ventilator-associated HAP was reduced significantly by providing standard oral health care (48), improving patient outcomes while lowering costs of care. This study has been expanded to include eight VA hospitals with plans for national VA deployment. While substantial evidence exists that oral health care is a modifiable risk factor for HAP and other infectious diseases, it has not been adopted universally (49, 50).
Human Papillomavirus Virus (HPV) Vaccine
This is an example where dental patient evaluation was omitted in clinical trials to evaluate the effectiveness of HPV vaccines. HPV vaccines are now recognized for their potential to prevent HPV-related oropharyngeal cancers, which have risen dramatically in recent years, especially in younger-aged groups (51). It took collaborative research efforts to reveal that this sexually transmitted disease can cause devastating manifestation in the oral cavity, and to increase research support to better understand the biologic implications of HPV +/− oral cancers. Since research has shown that some individuals are more likely to seek dental care (including for cosmetic reasons) compared with medical care, dental professionals need appropriate training so they can counsel their patients appropriately and even administer HPV and other vaccines, including COVID-19 (52). In fact, several states have approved providing vaccines in the dental setting, a view supported by the American Dental Association (53, 54).
Gains When Dental Scientists Are Part of the Team
Several areas of research are benefiting from new broad-based initiatives, cross-collaborations and multidisciplinary teamwork, specifically: microbiology, salivary studies, and craniofacial anomalies.
The Human Microbiome
From the initial discoveries that dental caries and periodontal disease were associated with specific bacterial species, oral health scientists have analyzed the complex microbial communities lining oral and dental surfaces in what were called biofilms. These complex microbial communities continue to be explored for relationships with many other diseases, including malignancies (55–57). With availability of newer tools and technologies researchers have expanded their horizons beyond mapping the human genome with its 20,000 genes to explore the much larger domain of the human microbiome, including previously uncultivable microbes. The Human Microbiome Project (HMP) was launched by NIH in 2007 (58) to map the human microbiome, choosing five sites: mouth, nasal, skin, gastrointestinal and urogenital tract. It is a stunning example of the information that can be gleaned when the dental domain is included in transdisciplinary research projects (59). One of the HMP outcomes has been a deeper awareness that microbes have a major influence on the host in health and disease, a story which is just beginning to unfold (60–68). As far as the mouth is concerned, it is a domain where oral scientists have been pioneers (69).
The immune-microbiome complex has become an area of intense investigation comparing the effects of a healthy vs. a diseased microbiome on the host-immune response. Intriguingly, Klebsiella can induce an inflammatory response in the gut, but not in the oral mucosa (60), while Fusobacterium nucleatum, an oral bacterium associated with severe periodontal disease, is linked to colon cancer (70). Porphyromonas gingivalis, a keystone pathogen in chronic periodontal disease, has been identified in amyloid plaques of individuals with Alzheimer's disease (71, 72).
The Periodontitis-Diabetes Story
The observation that patients with uncontrolled diabetes often have severe periodontitis inspired yet another major success story of the payoff when dental and non-dental researchers work together. Initial observations among the Pima tribe (73, 74) led to a focus on host-immune-microbial interactions and the key observation that in cases of uncontrolled diabetes, oral tissues, along with other tissues in the body, exhibit a hyperinflammatory response to local insults, such as infection or trauma. Addressing the hyperinflammatory issues early proved to be effective in managing, and in some cases preventing, the periodontal disease consequences of diabetes. Provision of non-surgical treatment has been associated with reductions in metabolic markers of dysglycemia, primarily glycated hemoglobin (75–77). Further, analyses of insurance databases have suggested that the provision of non-surgical periodontal treatment to persons with diabetes is associated with improved health outcomes, including reduced utilization and costs (78–80). So persuasive have been the findings from these studies that a number of U.S. insurance companies now offer additional dental care for their diabetic clients as a way to forestall more serious complications and hospitalizations. The establishment of the diabetes-periodontitis connection has important implications for addressing health disparities. Diabetes and obesity (a risk factor for diabetes) disproportionately occur in poor and minority groups. If they lack access to dental care, the impact of the two diseases will be more severe.
Salivary Diagnostics
The attractiveness of using saliva, known to contain, among other things, viral pathogens, shed cellular material (including genetic), and circulating antibodies, coupled with ease of sampling, has resulted in research targeted at detecting specific diseases or disorders and some success in the commercial development of diagnostic kits for this purpose. However, as saliva is a diluted exudate compared with blood, the amount of a given biomarker in saliva may be inadequate to detect with current tools and technologies Advanced technologies may improve that situation and indeed the advent of the coronavirus pandemic has already led to the development of safe and effective salivary test kits to detect SARS-CoV-2 in an individual (81). Symptomatic and asymptomatic spread of this virus is likely from saliva droplets and respiratory fluids (82, 83). Additionally, saliva may serve as a better source for detection of oral conditions such as oral pharyngeal HPV cancer than currently used blood tests and may be an ideal source for a “liquid biopsy” for point of care application (84–87).
Craniofacial Conditions
One of the best examples of comprehensive, collaborative care that includes dental specialists in a multidisciplinary setting is the craniofacial anomalies team. The American Cleft Palate-Craniofacial Association (ACPA) recognizes craniofacial teams who meet standards based on parameters of care that have been shown through research to provide optimal care for children with cleft lip and palate or other craniofacial anomalies. Dental specialists are integral to these teams with a direct impact on improved quality and outcomes of treatment. Several areas of research have advanced the care of children with congenital craniofacial anomalies and the understanding of disease processes leading to potential novel therapeutics for ectodermal dysplasia (88–90), promising intrauterine therapies to rescue cleft palate in mouse models (91–95), and better understanding of post-natal craniofacial development in patients with cleft lip and palate (7).
The Pandemic and Dental Research
While the dental community has long implemented safe practices of infection control and personalized protective equipment (PPE) resulting in very low infection rates among dentists during the pandemic (96), the potential for engaging the dental community in enhanced testing and sampling technologies is huge. Through the simple act of touching a dental mirror to the inside cheek of a patient, a dentist can be the “point of contact” for sampling saliva as a diagnostic fluid. Additionally, biosensors incorporated in a dental mirror or toothbrush can record vital signs, including temperature fluctuations and oxygen saturation, which could detect the early presence of disease in a community. Realtime data collection from such smart tools can protect the US population by predicting early hotspots of disease, as noted by Kinsa smart thermometers during the early phase of the SARS-CoV-2 pandemic1.
Conclusions: A Call to Action for Researchers, Educators and Clinicians
The goal of this perspective is to increase awareness of these issues and to activate researchers, healthcare providers, economists, policy drivers, advocacy groups and the communities we serve, locally and globally, to advance collaborations across all disciplines/communities. We cannot afford to ignore data from the dental, oral and craniofacial part of the body. A few suggested action items are presented in Table 2.
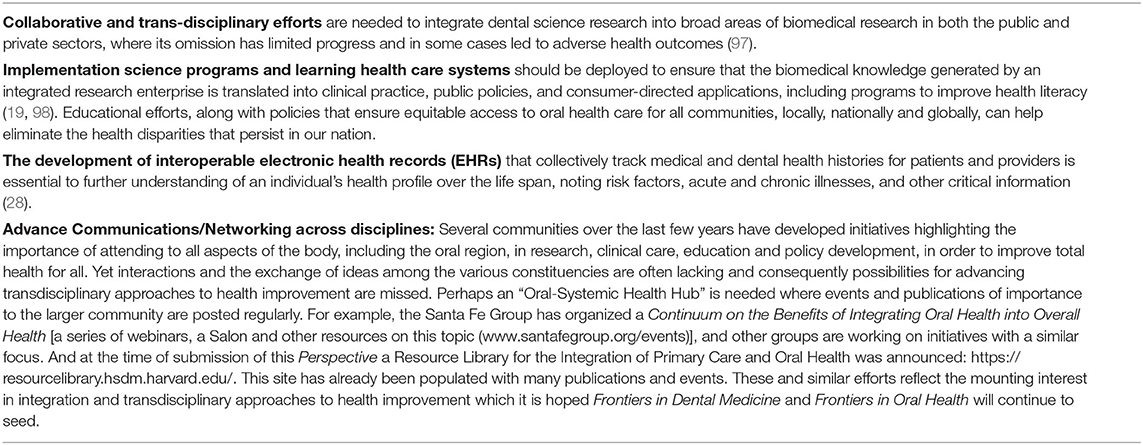
Table 2. Approaches toward achieving integration of oral health within the context of total health.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
This study was supported by the NIDCR/NIH and the Santa Fe Group.
Conflict of Interest
JW declares that she is a paid contractor, as a scientific writer and editor, for the Santa Fe Group.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Special thanks are extended to the FDEM staff and to the Santa Fe Group.
Footnotes
References
1. Bender EM, McMillan-Major A, and Shmitchell S. On the dangers of stochastic parrots: can language models be too big? In: FAccT '21: Proceedings of the 2021 ACM Conference on Fairness, Accountability, and Transparency. (2021). p. 610–23. doi: 10.1145/3442188.3445922
2. Matheny M, Thadaney Israni S, Ahmed M, and Whicher D editors. Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. NAM Special Publication. Washington, DC: National Academy of Medicine (2019). Available online at: https://nam.edu/artificial-intelligence-special-publication/
3. Liberton DK, Verma P, Contratto A, and Lee JS. Development and validation of novel three-dimensional craniofacial landmarks on cone-beam computed tomography scans. J Craniofac Surg. (2019) 30:e611–15. doi: 10.1097/SCS.0000000000005627
4. Torosdagli N, Liberton DK, Verma P, Sincan M, Lee JS, and Bagci U. Deep geodesic learning for segmentation and anatomical landmarking. IEEE Trans Med Imaging. (2019) 38:919–31. doi: 10.1109/TMI.2018.2875814
5. Kim, Misra D, Rodriguez L, Gill M, Liberton DK, Almpani K, et al. Malocclusion classification on 3d cone-beam CT craniofacial images using multi-channel deep learning models. Annu Int Conf IEEE Eng Med Biol Soc. (2020) 2020:1294–8. doi: 10.1109/EMBC44109.2020.9176672
6. Misra DG, Lee MJS, and Antani S. Segmentation of anterior tissues in craniofacial cone-beam CT images. In: IEEE 33rd International Symposium on Computer-Based Medical Systems. (2020). p. 71–6. doi: 10.1109/CBMS49503.2020.00021
7. Liberton DK, Verma P, Almpani K, Fung PW, Mishra R, Oberoi S, et al. Craniofacial analysis may indicate co-occurrence of skeletal malocclusions and associated risks in development of cleft lip and palate. J Dev Biol. (2020) 8:2. doi: 10.3390/jdb8010002
8. Jani P, Nguyen QC, Almpani K, Keyvanfar C, Mishra R, Liberton D, et al. Severity of oro-dental anomalies in Loeys-Dietz syndrome segregates by gene mutation. J Med Genet. (2020) 57:699–707. doi: 10.1136/jmedgenet-2019-106678
9. Daich Varela M, Jani P, Zein WM, D'Souza P, Wolfe L, Chisholm J, et al. The peroxisomal disorder spectrum and Heimler syndrome: deep phenotyping and review of the literature. Am J Med Genet C Semin Med Genet. (2020) 184:618–30. doi: 10.1002/ajmg.c.31823
10. Liu J, Kim YS, Richardson CE, Tom A, Ramakrishnan C, Birey F, et al. Genetically targeted chemical assembly of functional materials in living cells, tissues, and animals. Science. (2020) 367:1372–6. doi: 10.1126/science.aay4866
11. Lumelsky N, O'Hayre M, Chander P, Shum L, and Somerman MJ. Autotherapies: enhancing endogenous healing and regeneration. Trends Mol Med. (2018) 24:919–30. doi: 10.1016/j.molmed.2018.08.004
12. Nagai K, Ideguchi H, Kajikawa T, Li X, Chavakis T, Cheng J, et al. An injectable hydrogel-formulated inhibitor of prolyl-4-hydroxylase promotes T regulatory cell recruitment and enhances alveolar bone regeneration during resolution of experimental periodontitis. FASEB J. (2020) 34:13726–40. doi: 10.1096/fj.202001248R
13. Kim J, Koo BK, and Knoblich JA. Human organoids: model systems for human biology and medicine. Nat Rev Mol Cell Biol. (2020) 21:571–84. doi: 10.1038/s41580-020-0259-3
14. Collins FS, Doudna JA, Lander ES, and Rotimi CN. Human molecular genetics and genomics - important advances and exciting possibilities. N Engl J Med. (2021) 384:1–4. doi: 10.1056/NEJMp2030694
15. Gupta A, Madhavan MV, Sehgal K, Nair N, Mahajan S, Sehrawat TS, et al. Extrapulmonary manifestations of COVID-19. Nat Med. (2020) 26:1017–32. doi: 10.1038/s41591-020-0968-3
16. da Rosa Mesquita R, Francelino Silva Junior LC, Santos Santana FM, Farias de Oliveira T, Campos Alcântara R, Monteiro Arnozo G, et al. Clinical manifestations of COVID-19 in the general population: systematic review. Wien Klin Wochenschr. (2020) 133:377–82. doi: 10.1007/s00508-020-01760-4
17. Pierron D, Pereda-Loth V, Mantel M, Moranges M, Bignon E, Alva O, et al. Smell and taste changes are early indicators of the COVID-19 pandemic and political decision effectiveness. Nat Commun. (2020) 11:5152. doi: 10.1038/s41467-020-18963-y
18. Coke CJ, Davison B, Fields N, Fletcher J, Rollings J, Roberson L, et al. SARS-CoV-2 infection and oral health: therapeutic opportunities and challenges. J Clin Med. (2021) 10:156. doi: 10.3390/jcm10010156
19. Chambers DA, Feero WG, and Khoury MJ. Convergence of implementation science, precision medicine, and the learning health care system: a new model for biomedical research. JAMA. (2016) 315:1941–2. doi: 10.1001/jama.2016.3867
20. Wang CJ, and McCauley LK. Osteoporosis and periodontitis. Curr Osteoporos Rep. (2016) 14:284–91. doi: 10.1007/s11914-016-0330-3
21. Siddiqi, Zafar S, Sharma A, and Quaranta A. Diabetes mellitus and periodontal disease: the call for interprofessional education and interprofessional collaborative care - A systematic review of the literature. J Interprof Care. (2020) 1–9. doi: 10.1080/13561820.2020.1825354
22. Kitamoto S, Nagao-Kitamoto H, Jiao Y, Gillilland MG 3rd, Hayashi A, Imai J, et al. The intermucosal connection between the mouth and gut in commensal pathobiont-driven colitis. Cell. (2020) 182:447–62 e14. doi: 10.1016/j.cell.2020.05.048
23. Kleinstein SE, Nelson KE, and Freire M. Inflammatory networks linking oral microbiome with systemic health and disease. J Dent Res. (2020) 99:1131–9. doi: 10.1177/0022034520926126
24. Dioguardi M, Crincoli V, Laino L, Alovisi M, Sovereto D, Mastrangelo F, et al. The role of periodontitis and periodontal bacteria in the onset and progression of Alzheimer's disease: a systematic review. J Clin Med. (2020) 9:495. doi: 10.3390/jcm9020495
25. Ling MR, Chapple IL, and Matthews JB. Peripheral blood neutrophil cytokine hyper-reactivity in chronic periodontitis. Innate Immun. (2015) 21:714–25. doi: 10.1177/1753425915589387
26. Delbove T, Gueyffier F, Juillard L, Kalbacher E, Maucort-Boulch D, Nony P, et al. Effect of periodontal treatment on the glomerular filtration rate, reduction of inflammatory markers and mortality in patients with chronic kidney disease: a systematic review. PLoS One. (2021) 16:e0245619. doi: 10.1371/journal.pone.0245619
27. Nguyen QC, Duverger O, Mishra R, Mitnik GL, Jani P, Frischmeyer-Guerrerio PA, et al. Oral health-related quality of life in Loeys-Dietz syndrome, a rare connective tissue disorder: an observational cohort study. Orphanet J Rare Dis. (2019) 14:291. doi: 10.1186/s13023-019-1250-y
28. Mosen DM, Banegas MP, Dickerson JF, Fellows JL, Brooks NB, Pihlstrom DJ, et al. Examining the association of medical-dental integration with closure of medical care gaps among the elderly population. J Am Dent Assoc. (2021) 152:302–8. doi: 10.1016/j.adaj.2020.12.010
29. Tenuta LMA, Canady C, Eber RM, and Johnson L. Agreement in medications reported in medical and dental electronic health records. JDR Clin Trans Res. (2021). doi: 10.1177/23800844211004525. [Epub ahead of print].
30. Benjamin RM. Oral health: the silent epidemic. Public Health Rep. (2010) 125:158–9. doi: 10.1177/003335491012500202
31. Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Borgnakke WS, et al. Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J Periodontol. (2015) 86:611–22. doi: 10.1902/jop.2015.140520
32. Sen S, Redd K, Trivedi T, Moss K, Alonso A, Soliman EZ, et al. Periodontal disease, atrial fibrillation and stroke. Am Heart J. (2021) 235:36–43. doi: 10.1016/j.ahj.2021.01.009
33. Romandini M, Baima G, Antonoglou G, Bueno J, Figuero E, and Sanz M. Periodontitis, edentulism, and risk of mortality: a systematic review with meta-analyses. J Dent Res. (2021) 100:37–49. doi: 10.1177/0022034520952401
34. Monsarrat P, Blaizot A, Kemoun P, Ravaud P, Nabet C, Sixou M, et al. Clinical research activity in periodontal medicine: a systematic mapping of trial registers. J Clin Periodontol. (2016) 43:390–400. doi: 10.1111/jcpe.12534
35. Van Dyke TE, Kholy KE, Ishai A, R.Takx AP, Mezue K, Abohashem SM, et al. Inflammation of the periodontium associates with risk of future cardiovascular events. J Periodontol. (2021) 92:348–58. doi: 10.1002/JPER.19-0441
36. Nguyen LM, Chon JJ, Kim EE, Cheng JC, and Ebersole JL. Biological aging and periodontal disease: analysis of NHANES. (2001-2002). JDR Clin Trans Res. (2021). doi: 10.1177/2380084421995812. [Epub ahead of print].
37. Baum BJ. Salivary gland fluid secretion during aging. J Am Geriatr Soc. (1989) 37:453–8. doi: 10.1111/j.1532-5415.1989.tb02644.x
38. Ship JA, Pillemer SR, and Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc. (2002) 50:535–43. doi: 10.1046/j.1532-5415.2002.50123.x
39. Whyte MP. Hypophosphatasia - aetiology, nosology, pathogenesis, diagnosis and treatment. Nat Rev Endocrinol. (2016) 12:233–46. doi: 10.1038/nrendo.2016.14
40. Thumbigere-Math V, Alqadi A, Chalmers NI, Chavez MB, Chu EY, Collins MT, et al. Hypercementosis associated with ENPP1 mutations and GACI. J Dent Res. (2018) 97:432–41. doi: 10.1177/0022034517744773
41. Chavez MB, Kramer K, Chu EY, Thumbigere-Math V, and Foster BL. Insights into dental mineralization from three heritable mineralization disorders. J Struct Biol. (2020) 212:107597. doi: 10.1016/j.jsb.2020.107597
42. Lee AE, Chu EY, Gardner PJ, Duverger O, Saikali A, Wang SK, et al. A cross-sectional cohort study of the effects of FGF23 deficiency and hyperphosphatemia on dental structures in hyperphosphatemic familial tumor calcinosis. JBMR Plus. (2021) 5:e10470. doi: 10.1002/jbm4.10470
43. Warner BM, Baer AN, Lipson EJ, Allen C, Hinrichs C, Rajan A, et al. Sicca syndrome associated with immune checkpoint inhibitor therapy. Oncologist. (2019) 24:1259–69. doi: 10.1634/theoncologist.2018-0823
44. Wan JT, Sheeley DM, Somerman MJ, and Lee JS. Mitigating osteonecrosis of the jaw (ONJ) through preventive dental care and understanding of risk factors. Bone Res. (2020) 8:14. doi: 10.1038/s41413-020-0088-1
45. Foster BL, Nociti FH Jr, and Somerman MJ. The rachitic tooth. Endocr Rev. (2014) 35:1–34. doi: 10.1210/er.2013-1009
46. Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. (2014) 370:1198–208. doi: 10.1056/NEJMoa1306801
47. Botros N, Iyer P, and Ojcius DM. Is there an association between oral health and severity of COVID-19 complications? Biomed J. (2020) 43:325–7. doi: 10.1016/j.bj.2020.05.016
48. Munro S, and Baker D. Reducing missed oral care opportunities to prevent non-ventilator associated hospital acquired pneumonia at the department of veterans affairs. Appl Nurs Res. (2018) 44:48–53. doi: 10.1016/j.apnr.2018.09.004
49. Kaneoka, Pisegna JM, Miloro KV, Lo M, Saito H, Riquelme LF, et al. Prevention of healthcare-associated pneumonia with oral care in individuals without mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Infect Control Hosp Epidemiol. (2015) 36:899–906. doi: 10.1017/ice.2015.77
50. Baker D, and Quinn B. Hospital acquired pneumonia prevention initiative-2: incidence of nonventilator hospital-acquired pneumonia in the United States. Am J Infect Control. (2018) 46:2–7. doi: 10.1016/j.ajic.2017.08.036
51. Gillison ML, Chaturvedi AK, Anderson WF, and Fakhry C. Epidemiology of human papillomavirus-positive head and neck squamous cell carcinoma. J Clin Oncol. (2015) 33:3235–42. doi: 10.1200/JCO.2015.61.6995
52. Strauss SM, Alfano MC, Shelley D, and Fulmer T. Identifying unaddressed systemic health conditions at dental visits: patients who visited dental practices but not general health care providers in 2008. Am J Public Health. (2012) 102:253–5. doi: 10.2105/AJPH.2011.300420
53. Villa, Chmieliauskaite M, and Patton LL. Including vaccinations in the scope of dental practice: the time has come. J Am Dent Assoc. (2021) 152:184–6. doi: 10.1016/j.adaj.2020.09.025
54. Wright JT. COVID-19 vaccination: science, politics and public health. J Am Dent Assoc. (2021) 152:181–3. doi: 10.1016/j.adaj.2021.01.009
55. F.Teles RF, Alawi F, Castilho RM, and Wang Y. Association or causation? Exploring the oral microbiome and cancer links. J Dent Res. (2020) 99:1411–24. doi: 10.1177/0022034520945242
56. Bornigen D, Ren B, Pickard R, Li J, Ozer E, Hartmann EM, et al. Alterations in oral bacterial communities are associated with risk factors for oral and oropharyngeal cancer. Sci Rep. (2017) 7:17686. doi: 10.1038/s41598-017-17795-z
57. Kitamoto S, Nagao-Kitamoto H, Hein R, Schmidt TM, and Kamada N. The bacterial connection between the oral cavity and the gut diseases. J Dent Res. (2020) 99:1021–9. doi: 10.1177/0022034520924633
58. Turnbaugh PJ, Ley RE, Hamady M, Fraser-Liggett CM, Knight R, and Gordon JI. The human microbiome project. Nature. (2007) 449:804–10. doi: 10.1038/nature06244
59. Gevers D, Knight R, Petrosino JF, Huang K, McGuire AL, Birren BW, et al. The human microbiome project: a community resource for the healthy human microbiome. PLoS Biol. (2012) 10:e1001377. doi: 10.1371/journal.pbio.1001377
60. Atarashi K, Suda W, Luo C, Kawaguchi T, Motoo I, Narushima S, et al. Ectopic colonization of oral bacteria in the intestine drives TH1 cell induction and inflammation. Science. (2017) 358:359–65. doi: 10.1126/science.aan4526
61. Tsukasaki M, Komatsu N, Nagashima K, Nitta T, Pluemsakunthai W, Shukunami C, et al. Host defense against oral microbiota by bone-damaging T cells. Nat Commun. (2018) 9:701. doi: 10.1038/s41467-018-03147-6
62. Willis JR, and Gabaldon T. The human oral microbiome in health and disease: from sequences to ecosystems. Microorganisms. (2020) 8:308. doi: 10.3390/microorganisms8020308
63. Genco RJ, and Sanz M. Clinical and public health implications of periodontal and systemic diseases: an overview. Periodontol 2000. (2020) 83:7–13. doi: 10.1111/prd.12344
64. Aquino-Martinez R, and Hernandez-Vigueras S. Severe COVID-19 lung infection in older people and periodontitis. J Clin Med. (2021) 10:279. doi: 10.3390/jcm10020279
65. Paul O, Arora P, Mayer M, and Chatterjee S. Inflammation in periodontal disease: possible link to vascular disease. Front Physiol. (2020) 11:609614. doi: 10.3389/fphys.2020.609614
66. Chung M, Zhao N, Meier R, Koestler DC, Wu G, de Castillo E, et al. Comparisons of oral, intestinal, and pancreatic bacterial microbiomes in patients with pancreatic cancer and other gastrointestinal diseases. J Oral Microbiol. (2021) 13:1887680. doi: 10.1080/20002297.2021.1887680
67. Helenius-Hietala J, Suominen AL, Ruokonen H, Knuuttila M, Puukka P, Jula A, et al. Periodontitis is associated with incident chronic liver disease-A population-based cohort study. Liver Int. (2019) 39:583–91. doi: 10.1111/liv.13985
68. Acharya, and Bajaj JS. Gut microbiota and complications of liver disease. Gastroenterol Clin North Am. (2017) 46:155–69. doi: 10.1016/j.gtc.2016.09.013
69. Hajishengallis G, and Chavakis T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat Rev Immunol. (2021). doi: 10.1038/s41577-020-00488-6
70. Mima K, Nishihara R, Qian ZR, Cao Y, Sukawa Y, Nowak JA, et al. Fusobacterium nucleatum in colorectal carcinoma tissue and patient prognosis. Gut. (2016) 65:1973–80. doi: 10.1136/gutjnl-2015-310101
71. Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, Konradi A, et al. Porphyromonas gingivalis in Alzheimer's disease brains: evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. (2019) 5:eaau3333. doi: 10.1126/sciadv.aau3333
72. Costa MJF, de Araújo IDT, da Rocha Alves L, da Silva RL, Dos Santos Calderon P, Borges BCD, et al. Relationship of Porphyromonas gingivalis and Alzheimer's disease: a systematic review of pre-clinical studies. Clin Oral Investig. (2021) 25:797–806. doi: 10.1007/s00784-020-03764-w
73. Shlossman M, Knowler WC, Pettitt DJ, and Genco RJ. Type 2 diabetes mellitus and periodontal disease. J Am Dent Assoc. (1990) 121:532–6. doi: 10.14219/jada.archive.1990.0211
74. Nelson RG, Shlossman M, Budding LM, Pettitt DJ, Saad MF, Genco RJ, et al. Periodontal disease and NIDDM in Pima Indians. Diabetes Care. (1990) 13:836–40. doi: 10.2337/diacare.13.8.836
75. D'Aiuto F, Gkranias N, Bhowruth D, Khan T, Orlandi M, Suvan J, et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: a 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. (2018) 6:954–65. doi: 10.1016/S2213-8587(18)30038-X
76. Cao R, Li Q, Wu Q, Yao M, Chen Y, and Zhou H. Effect of non-surgical periodontal therapy on glycemic control of type 2 diabetes mellitus: a systematic review and Bayesian network meta-analysis. BMC Oral Health. (2019) 19:176. doi: 10.1186/s12903-019-0829-y
77. Baeza M, Morales A, Cisterna C, Cavalla F, Jara G, Isamitt Y, et al. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. J Appl Oral Sci. (2020) 28:e20190248. doi: 10.1590/1678-7757-2019-0248
78. Nasseh K, Vujicic M, and Glick M. The relationship between periodontal interventions and healthcare costs and utilization. Evidence from an Integrated Dental, Medical, and Pharmacy Commercial Claims Database. Health Econ. (2017) 26:519–27. doi: 10.1002/hec.3316
79. Smits KPJ, Listl S, Plachokova AS, Van der Galien O, and Kalmus O. Effect of periodontal treatment on diabetes-related healthcare costs: a retrospective study. BMJ Open Diabetes Res Care. (2020) 8:e001666. doi: 10.1136/bmjdrc-2020-001666
80. Alfano MC. The economic impact of periodontal inflammation. In: Glick M, editor. The Oral-Systemic Health Connection, 2nd ed. Batavia, IL: Quintessence Publishing Co, Inc. p. 358–69.
81. Wyllie AL, Fournier J, Casanovas-Massana A, Campbell M, Tokuyama M, Vijayakumar P, et al. Saliva or nasopharyngeal swab specimens for detection of SARS-CoV-2. N Engl J Med. (2020) 383:1283–6. doi: 10.1056/NEJMc2016359
82. Fernandes LL, Pacheco VB, Borges L, Athwal HK, de Paula Eduardo F, Bezinelli L, et al. Saliva in the diagnosis of COVID-19: a review and new research directions. J Dent Res. (2020) 99:1435–43. doi: 10.1177/0022034520960070
83. Huang N, Perez P, Kato T, Mikami Y, Okuda K, Gilmore RC, et al. SARS-CoV-2 infection of the oral cavity and saliva. Nat Med. (2021) 27:892–903. doi: 10.1038/s41591-021-01296-8
84. Tang KD, Baeten K, Kenny L, Frazer IH, Scheper G, and Punyadeera C. Unlocking the potential of saliva-based test to detect HPV-16-driven oropharyngeal cancer. Cancers. (2019) 11:473. doi: 10.3390/cancers11040473
85. Ahn SM, Chan JY, Zhang Z, Wang H, Khan Z, Bishop JA, et al. Saliva and plasma quantitative polymerase chain reaction-based detection and surveillance of human papillomavirus-related head and neck cancer. JAMA Otolaryngol Head Neck Surg. (2014) 140:846–54. doi: 10.1001/jamaoto.2014.1338
86. Fakhry, Blackford AL, Neuner G, Xiao W, Jiang B, Agrawal A, et al. Association of oral human papillomavirus DNA persistence with cancer progression after primary treatment for oral cavity and oropharyngeal squamous cell carcinoma. JAMA Oncol. (2019) 5:985–92. doi: 10.1001/jamaoncol.2019.0439
87. Aro K, Wei F, Wong DT, and Tu M. Saliva liquid biopsy for point-of-care applications. Front Public Health. (2017) 5:77. doi: 10.3389/fpubh.2017.00077
88. Margolis CA, Schneider P, Huttner K, Kirby N, Houser TP, Wildman L, et al. Prenatal treatment of X-linked hypohidrotic ectodermal dysplasia using recombinant ectodysplasin in a canine model. J Pharmacol Exp Ther. (2019) 370:806–13. doi: 10.1124/jpet.118.256040
89. Schneider H, Faschingbauer F, Schuepbach-Mallepell S, Korber I, Wohlfart S, Dick A, et al. Prenatal correction of X-linked hypohidrotic ectodermal dysplasia. N Engl J Med. (2018) 378:1604–10. doi: 10.1056/NEJMoa1714322
90. Marchegiani S, Davis T, Tessadori F, van Haaften G, Brancati F, Hoischen A, et al. Recurrent Mutations in the Basic Domain of TWIST2 Cause Ablepharon Macrostomia and Barber-Say Syndromes. Am J Hum Genet. (2015) 97:99–110. doi: 10.1016/j.ajhg.2015.05.017
91. Jia S, Zhou J, Wee Y, Mikkola ML, Schneider P, and D'Souza RN. Anti-EDAR agonist antibody therapy resolves palate defects in Pax9(-/-) mice. J Dent Res. (2017) 96:1282–9. doi: 10.1177/0022034517726073
92. Jia S, Zhou J, and D'Souza RN. Pax9's dual roles in modulating Wnt signaling during murine palatogenesis. Dev Dyn. (2020) 249:1274–84. doi: 10.1002/dvdy.189
93. Jia S, Zhou J, Fanelli C, Wee Y, Bonds J, Schneider P, et al. Small-molecule Wnt agonists correct cleft palates in Pax9 mutant mice in utero. Development. (2017) 144:3819–3828. doi: 10.1242/dev.157750
94. Oliver JD, Turner EC, Halpern LR, Jia S, Schneider P, and D'Souza RN. Molecular diagnostics and in utero therapeutics for orofacial clefts. J Dent Res. (2020) 99:1221–7. doi: 10.1177/0022034520936245
95. Oliver JD, Jia S, Halpern LR, Graham EM, Turner EC, Colombo JS, et al. Innovative molecular and cellular therapeutics in cleft palate tissue engineering. Tissue Eng Part B Rev. (2020). doi: 10.1089/ten.teb.2020.0181
96. Estrich CG, Mikkelsen M, Morrissey R, Geisinger ML, Ioannidou E, Vujicic M, et al. Estimating COVID-19 prevalence and infection control practices among US dentists. J Am Dent Assoc. (2020) 151:815–24. doi: 10.1016/j.adaj.2020.09.005
97. Somerman MJ, and Mouradian WE. Integrating oral and systemic health: innovations in transdisciplinary science, health care and policy. Front Dent Med. (2020) 1:599214. doi: 10.3389/fdmed.2020.599214
Keywords: medical-dental integration, oral-systemic research, clinical trials, interoperable electronic health records, microbiome
Citation: Mouradian W, Lee J, Wilentz J and Somerman M (2021) A Perspective: Integrating Dental and Medical Research Improves Overall Health. Front. Dent. Med. 2:699575. doi: 10.3389/fdmed.2021.699575
Received: 23 April 2021; Accepted: 17 May 2021;
Published: 22 June 2021.
Edited by:
Man-Kyo Chung, University of Maryland, Baltimore, United StatesReviewed by:
Mark Reynolds, University of Maryland, Baltimore, United StatesJeffrey Ebersole, University of Nevada, Las Vegas, United States
Copyright © 2021 Mouradian, Lee, Wilentz and Somerman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martha Somerman, bWFydGhhLnNvbWVybWFuQG5paC5nb3Y=