 Alan R. Schroeder
Alan R. Schroeder Thomas B. Newman
Thomas B. Newman Sabine Girod3
Sabine Girod3- 1Department of Pediatrics, Stanford University School of Medicine, Stanford, CA, United States
- 2Departments of Epidemiology and Biostatistics and Pediatrics, San Francisco School of Medicine, University of California, San Francisco, San Francisco, CA, United States
- 3Department of Surgery (Plastic and Reconstructive Surgery), Stanford University School of Medicine, Stanford, CA, United States
- 4Department of Epidemiology and Biostatistics, San Francisco School of Medicine, University of California, San Francisco, San Francisco, CA, United States
- 5Facultad de Odontología, Universidad Mayor, Santiago, Chile
Objective: To determine the cumulative incidence and predictors of third molar (3M, “wisdom teeth”) extractions in the United States.
Methods: We retrospectively analyzed a US private dental insurance claims database to create a Kaplan-Meier curve for the cumulative incidence of 3M extractions and used Cox proportional hazards to assess associations between sex, geographic region, and extractions.
Results: Between 2007 and 2016, by age 25, ~80% of patients underwent ≥1 tooth extraction and an estimated 50% of patients underwent ≥1 3M extraction. Factors associated with 3M extractions included female sex (adjusted hazard ratio [aHR] 1.08, 95% CI 1.07–1.08) and residence in the West (aHR 1.82, 95% CI 1.81–1.85) or South (aHR 1.5, 95% CI 1.49–1.51) geographic regions as compared to the Northeast.
Conclusion: 3M extractions are likely the most common surgery performed in US adolescents and young adults. Significant geographic variation suggests that elucidation of the indications for this common procedure is a public health priority.
Introduction
Third molar (3M, “wisdom teeth”) extractions are common in the United States (US). However, the benefit of this procedure for asymptomatic molars remains controversial (1, 2). Although a limited number of investigations have described the frequency of 3M extractions in the US, these studies have largely been focused on narrow geographic regions and only cover up to the year 2011 (3, 4). As our understanding of the risks and benefits of this procedure continues to evolve, updated frequency estimates are needed to better delineate the overall impact on the population. Similarly, better understanding of patterns of utilization could help to inform future quality improvement initiatives and/or clinical trials. Using a national dental insurance claims database, we estimated the cumulative incidence of third molar extractions in the United States and describe procedural variation by sex and geographic region.
Methods
Design and Data Source
We used a retrospective cohort design to analyze the cumulative incidence of 3M extractions by age 60 years among US patients in the IBM MarketScan® Dental Database. This database provides insurance claims information for a large sample of privately insured patients and can be linked to the IBM MarketScan® Commercial Database. All information is de-identified.
Study Population and Variables
We included all patients under 60 years of age enrolled at any time between January 1, 2007, and December 31, 2016. We began by identifying tooth extractions using Current Dental Terminology (CDT) codes D7140 (“extraction, erupted tooth or exposed root”), D7220 (“removal of impacted tooth—soft tissue”), D7230 (“removal of impacted tooth—partially bony”), D7240 (“removal of impacted tooth—completely bony”), D7241 (“removal of impacted tooth—completely bony, with unusual surgical complications”), D7250 (“removal of residual roots”), and D7251 (“Coronectomy—intentional partial tooth removal”). 3Ms can be precisely identified when tooth numbers 1, 16, 17, and 32 are attached to the procedure codes. However, specification of the tooth number was inconsistent in the dataset. Therefore, we opted to present the cumulative incidence curves using several approaches: (1) any extraction, defined as having at least one tooth extraction, regardless of tooth number; (2) documented 3M extractions, defined as having at least one extraction specifically numbered as a 3M; and (3) an aggregate of known 3M extractions plus imputed missing data on tooth number (see statistical section below).
We examined associations of the procedure with sex and geographic region. Although other demographic variables such as ethnicity and socioeconomic status might influence the frequency of the procedure, in order to preserve privacy and de-identification, the Marketscan database does not contain this information.
Statistical Analysis
We present cumulative extraction incidence using Kaplan-Meier curves and use Cox proportional hazards to examine the influence of sex and geographic region. For the cumulative incidence plot, we used data from the dental enrollment dataset and dental claims dataset. Because of the high number of missing tooth numbers, we imputed whether the extractions corresponded to 3M's using Classification and Regression Tree (CART) from the Multivariate Imputation by Chain Equation (MICE) package in R (R Core Team 2020) (5). In this method, a number of bootstrap samples are drawn from the observed data with replacement. From each bootstrap sample, a CART model is fitted to impute the missing data (i.e., 3M extraction). As a result, MICE creates a number of imputed datasets, each one using a different CART model. In this analysis, we used MICE to create a total of ten imputed datasets. For each imputed dataset, we calculated a cumulative incidence curve. Afterward, we computed the mean cumulative incidence curve. Because of computational constraints posed by the size of the datasets, for the imputations we created a subset of 265,050 randomly selected claims, which corresponds to ~1% of the total number of claims. We used the dataset without imputations (i.e., only those observations with documented tooth number) to compute cumulative incidence curves for known 3M extractions and any tooth extraction, as previously defined.
To evaluate which variables are more influential in the CART models used to impute 3M extractions, we created another CART model, but this time using all the observations with documented tooth number. In that model, the variables used to predict 3M extractions are procedure code, age at service, age at coverage start, and number of teeth ever extracted.
Finally, Cox proportional hazards were calculated in STATA (version 14, College Station, TX) for documented (i.e., not imputed) 3M extractions using the full dataset. We conducted all the analyses in 2020.
Results
Among 26,482,180 million subjects in the dental claims dataset at any point during the study period, there were 9,945,392 extractions in 3,530,405 subjects (13.3% of subjects who were enrolled at any point): 1,280,923 (12.9%) were specifically for 3M's, 1,801,264 (18.1%) were for extractions of a non-3M, and 6,863,205 (69%) were for extractions with a missing tooth number. Approximately 50% of patients are estimated to undergo at least one 3M extraction by age 25 (Figure 1). Factors associated with 3M extractions included female sex (adjusted hazard ratio [aHR] 1.08, 95% CI 1.07–1.08) and residence in the West (aHR 1.82, 95% CI 1.81–1.85) or South (aHR 1.5, 95% CI 1.49–1.51) compared with the Northeast (Table 1).
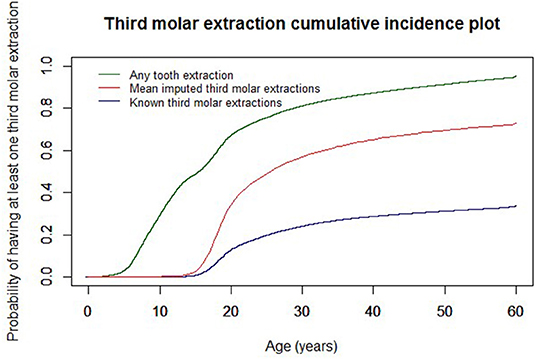
Figure 1. Cumulative incidence plot of third molar extractions.
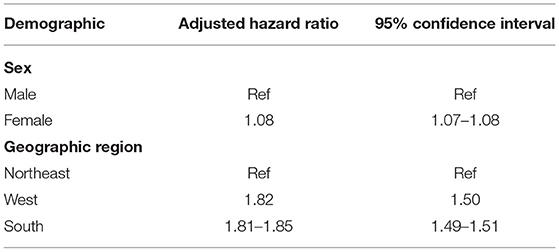
Table 1. Demographic variables significantly associated with third molar extractions in the US.
Discussion
Our findings demonstrate that tooth extractions are commonly performed in the US, occurring in ~80% of privately insured adults by the age of 25 years. From our Kaplan-Meier curve (Figure 1), we estimate that about half of adults undergo at least one 3M extraction by the age of 25 years and about 70% by age 60. Third molar extractions are performed slightly more commonly in females. We also observed substantial geographic variation, with the procedure performed more commonly in the West and South compared with the Northeast, a finding that has not previously been noted in published literature to our knowledge.
The literature on 3M extraction frequency is sparse and has been limited by reliance on surgeon surveys (1) and narrow geographic focus (3, 4). Our incidence estimates are similar to findings from a prospective study in the Pacific Northwest from 2009 to 10 which reported that prophylactic removal was recommended for 59% of 16–22 year-old patients (3). According to a study questionnaire, the most commonly cited justification for 3M removal by participating dentists was “to prevent future problems.” Approximately 39% of subjects ultimately underwent at least one extraction during the study period (6), a proportion that is close to the percentage of patients in that age group estimated to have undergone at least one extraction in our study.
A claims data investigation from the Michigan area revealed that 44% of 13–21 year-old patients underwent at least one 3M extraction, with 80.4% of those patients having all four 3Ms removed (4). There was striking variability in procedural frequency across practices, with under 10% of patients undergoing the procedure in 7% of practices and 60% or more of patients undergoing the procedure in ~15% of practices. While reasons for this variation are unclear, unwarranted regional variations in health care delivery have been proposed as a sign of overtreatment (7).
Controversy persists regarding the indications for prophylactic 3M removal. A recently updated Cochrane Review concluded that there is insufficient evidence to determine whether asymptomatic 3Ms should be removed or retained (2), and the American Public Health Association has published recommendations against routine removal (8). On the other hand, the American Association of Oral and Maxillofacial Surgeons statement advocates for surgical management of diseased 3Ms and 3Ms at “high risk of developing disease” (9).
We noted substantial geographic variation in procedural frequency, with 3M extractions occurring more commonly in the West or South compared to the Northeast. Coupled with the findings from Eklund et al. (4) surrounding variation between practices, this level of unwarranted variation may suggest that overtreatment is occurring (7). Our findings should be validated through future investigations and further explored to understand the roots of the geographic differences.
Third molar extractions can cause harm due to possible opioid exposure (10), and the procedure has associated surgical and anesthetic risks. Additionally, prophylactic antibiotics have side effects and can lead to antimicrobial resistance. Our data on the cumulative incidence of the procedure is a necessary first step as we strive to better understand the overall risk:benefit profile of this common procedure from a public health perspective.
The main limitation of this study is the high proportion of missing tooth numbers accompanying extraction claims, which led us to impute missing data. However, missing tooth numbers are unlikely to explain the geographic variation we observed. Moreover, the concordance of our findings with data from older, regional studies suggests that our estimates may be reasonably accurate. Additionally, other unmeasured demographic or clinical factors not included in our analysis may explain procedural variation.
Conclusion
Based on our estimates, 3M extractions are likely the most common surgery performed on US adolescents and young adults. Given the uncertain risk:benefit profile and the observed significant geographic variation, further elucidation of the indications for this common procedure is a public health priority.
Data Availability Statement
The datasets presented in this article are not readily available because the commercial claims dataset was purchased by Stanford. Requests to access the datasets should be directed to the company directly (Marketscan).
Ethics Statement
The studies involving human participants were reviewed and approved by Stanford Institutional Review Board (waived). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Friedman JW. The prophylactic extraction of third molars: a public health hazard. Am J Public Health. (2007) 97:1554–9. doi: 10.2105/AJPH.2006.100271
2. Ghaeminia H, Nienhuijs ME, Toedtling V, Perry J, Tummers M, Hoppenreijs TJ„ et al. Surgical removal versus retention for the management of asymptomatic disease-free impacted wisdom teeth. Cochrane Database Syst Rev. (2020) 5:CD003879. doi: 10.1002/14651858.CD003879.pub5
3. Cunha-Cruz J, Rothen M, Spiekerman C, Drangsholt M, McClellan L, Huang GJ, et al. Recommendations for third molar removal: a practice-based cohort study. Am J Public Health. (2014) 104:735–43. doi: 10.2105/AJPH.2013.301652
4. Eklund SA, Pittman JL. Third-molar removal patterns in an insured population. J Am Dent Assoc. (2001) 132:469–75. doi: 10.14219/jada.archive.2001.0209
5. van Buuren S, Groothius-Oudshoorn K. Mice: multivariate imputation by chained equations in R. J Stat Softw. (2011) 45:1–67. doi: 10.18637/jss.v045.i03
6. Huang GJ, Cunha-Cruz J, Rothen M, et al. A prospective study of clinical outcomes related to third molar removal or retention. Am J Public Health. (2014) 104:728–34. doi: 10.2105/AJPH.2013.301649
7. Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care. Ann Intern Med. (2003) 138:273–87. doi: 10.7326/0003-4819-138-4-200302180-00006
8. American Public Health Association. Opposition of Prophylactic Removal of Third Molars (Wisdom Teeth). Available online at: https://apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2014/07/24/14/29/opposition-to-prophylactic-removal-of-third-molars-wisdom-teeth (accessed June 13, 2020).
9. American Association of Oral Maxillofacial Surgeons. Management of Third Molar Teeth. Available online at: https://www.aaoms.org/docs/govt_affairs/advocacy_white_papers/management_third_molar_white_paper.pdf (accessed June 13, 2020).
Keywords: third molar, extraction, epidemiology, children, insurance claims
Citation: Schroeder AR, Newman TB, Girod S, Hashemi S and Häberle AD (2022) Estimated Cumulative Incidence of Wisdom Tooth Extractions in Privately Insured US Patients. Front. Dent. Med. 3:937165. doi: 10.3389/fdmed.2022.937165
Received: 05 May 2022; Accepted: 16 June 2022;
Published: 08 July 2022.
Edited by:
Jayakumar Jayaraman, Virginia Commonwealth University, United StatesReviewed by:
Resmi Raju, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NIH), United StatesTaibah Albaker, Virginia Commonwealth University, United States
Copyright © 2022 Schroeder, Newman, Girod, Hashemi and Häberle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alan R. Schroeder, YXNjaHJvZUBzdGFuZm9yZC5lZHU=