 Rebecca Brandon1,2Yannan Jiang3,4
Rebecca Brandon1,2Yannan Jiang3,4 Rui Qian Yeu1,2Ry Tweedie-Cullen1,2Kate Smallman5Glenn Doherty6Kerry A. Macaskill-Smith7Rebekah J. Doran7Penny Clark7
Rui Qian Yeu1,2Ry Tweedie-Cullen1,2Kate Smallman5Glenn Doherty6Kerry A. Macaskill-Smith7Rebekah J. Doran7Penny Clark7 Allan Moffitt8
Allan Moffitt8 Troy Merry2,9Norma Nehren10Frances King11Jennie Harré Hindmarsh11
Troy Merry2,9Norma Nehren10Frances King11Jennie Harré Hindmarsh11 Megan Patricia Leask2,12,13
Megan Patricia Leask2,12,13 Tony R. Merriman2,12,13
Tony R. Merriman2,12,13 Brandon Orr-Walker14Peter R. Shepherd2,15Ryan Paul2,16
Brandon Orr-Walker14Peter R. Shepherd2,15Ryan Paul2,16 Rinki Murphy1,2*
Rinki Murphy1,2*- 1Department of Medicine, Faculty of Medical and Health Sciences, The University of Auckland, Auckland, New Zealand
- 2Maurice Wilkins Centre for Molecular Biodiscovery, Auckland, New Zealand
- 3Department of Statistics, Faculty of Sciences, The University of Auckland, Auckland, New Zealand
- 4National Institute for Health Innovation, School of Population Health, The University of Auckland, Auckland, New Zealand
- 5Diabetes Foundation Aotearoa, Auckland, New Zealand
- 6Tongan Health Society, Auckland, New Zealand
- 7Ventures/Pinnacle Incorporated, Hamilton, New Zealand
- 8Procare Primary Health Organisation, Auckland, New Zealand
- 9Discipline of Nutrition, University of Auckland, Auckland, New Zealand
- 10Te Hiku Hauora, Northland District Health Board, Kaitaia, New Zealand
- 11Ngāti Porou Hauora, Tairāwhiti, New Zealand
- 12Department of Biochemistry, University of Otago, Dunedin, New Zealand
- 13Division of Clinical Immunology and Rheumatology, University of Alabama at Birmingham, Birmingham, AL, United States
- 14Middlemore Clinical Trials, Auckland, New Zealand
- 15Department of Molecular Medicine and Pathology, School of Medical Sciences, The University of Auckland, Auckland, New Zealand
- 16Department of Medicine, University of Waikato, Waikato, New Zealand
Background: Understanding which group of patients with type 2 diabetes will have the most glucose lowering response to certain medications (which target different aspects of glucose metabolism) is the first step in precision medicine.
Aims: We hypothesized that people with type 2 diabetes who generally have high insulin resistance, such as people of Māori/Pacific ethnicity, and those with obesity and/or hypertriglyceridemia (OHTG), would have greater glucose-lowering by pioglitazone (an insulin sensitizer) versus vildagliptin (an insulin secretagogue).
Methods: A randomised, open-label, two-period crossover trial was conducted in New Zealand. Adults with type 2 diabetes, HbA1c>58mmol/mol (>7.5%), received 16 weeks of either pioglitazone (30mg) or vildagliptin (50mg) daily, then switched to the other medication over for another 16 weeks of treatment. Differences in HbA1c were tested for interaction with ethnicity or OHTG, controlling for baseline HbA1c using linear mixed models. Secondary outcomes included weight, blood pressure, side-effects and diabetes treatment satisfaction.
Results: 346 participants were randomised (55% Māori/Pacific) between February 2019 to March 2020. HbA1c after pioglitazone was lower than after vildagliptin (mean difference -4.9mmol/mol [0.5%]; 95% CI -6.3, -3.5; p<0.0001). Primary intention-to-treat analysis showed no significant interaction effect by Māori/Pacific vs other ethnicity (1.5mmol/mol [0.1%], 95% CI -0.8, 3.7), and per-protocol analysis (-1.2mmol/mol [0.1%], 95% CI -4.1, 1.7). An interaction effect (-4.7mmol/mol [0.5%], 95% CI -8.1, -1.4) was found by OHTG status. Both treatments generated similar treatment satisfaction scores, although there was greater weight gain and greater improvement in lipids and liver enzymes after pioglitazone than vildagliptin.
Conclusions: Comparative glucose-lowering by pioglitazone and vildagliptin is not different between Māori/Pacific people compared with other New Zealand ethnic groups. Presence of OHTG predicts greater glucose lowering by pioglitazone than vildagliptin.
Clinical trial registration: www.anzctr.org.au, identifier (ACTRN12618001907235).
Introduction
The epidemic of type 2 diabetes (T2D) is of significant concern due to increased morbidity, mortality, and health care costs. Current treatment guidelines recommend early use of sodium glucose transport protein 2 inhibitors (SGLT2i) and glucagon like peptide 1 receptor agonists (GLP1RA) for those with high cardiovascular risk, heart failure or renal disease (1). In the remainder, metformin, followed by a range of other medications are recommended for glucose lowering on a sequential, additive basis, influenced by cost, side effect profiles, and average treatment effects from clinical trials (1). Consideration of personal characteristics such as comorbidities, and circumstances such as food security, financial stability, alongside setting an appropriate target HbA1c for individuals is part of individualising treatment of T2D. Identifying subgroups or strata of patients with similar characteristics who respond better to one type of glucose-lowering therapy over another, and/or have altered risk of treatment-specific side effects, has been termed stratification of treatment response, which represents the first step towards precision medicine for T2D (2).
The glucose lowering response to non-insulin therapies that target discrete aspects of glucose metabolism is, extremely variable between individuals with T2D. Knowledge of which medications are likely to be most effective for individuals with T2D is important to minimise cost, side effects and periods of hyperglycaemia associated with initiating an ineffective medication. In the absence of knowledge about which subgroups of people with T2D respond better to a particular medication, relatively low glucose lowering response to certain treatments may be inappropriately attributed to non-adherence. There is emerging evidence for stratification of glucose lowering response to certain medications for T2D by baseline characteristics, such as ethnicity, obesity and triglyceride levels.
Ethnicity as a marker for differential medication responsiveness has been investigated as a simple tool for therapeutic stratification of T2D medications. Both SGLT2i and dipeptidyl peptidase 4 inhibitor (DPP4i) have been reported to be more effective in lowering HbA1c in people of Asian compared with European ethnicity (3). Metformin may be more effective in African Americans with younger onset T2D compared to Americans of European ethnicity (4). Alpha-glucosidase inhibitors appear to work better in South East Asians than Europeans (5).
It is unclear whether differences in treatment response by ethnicity are due to biological differences in underlying T2D aetiology, or whether ethnicity serves as a proxy for residual confounders such as level of glycaemia, concomitant diabetes therapies, dietary factors, medication adherence or other health inequities. Biological differences in underlying T2D aetiology using routinely assessed clinical markers of insulin resistance, such as obesity and/or high triglycerides (OHTG), have been shown to predict less glucose-lowering to DPP4i (6), which amplifies glucose-stimulated beta cell insulin secretion through the endogenous incretin pathway. Those with obesity have been reported to have greater glucose-lowering with thiazolidinediones (6, 7), which act to improve insulin sensitivity and lipid metabolism by stimulating the nuclear receptor peroxisome proliferator-activated receptor gamma (PPARG).
Māori are the indigenous people of Aotearoa, New Zealand and share common Polynesian ancestry with Pacific peoples. Obesity and elevated triglyceride levels are prevalent in people of Māori and Pacific ethnicities (8, 9). There are disparities in diabetes outcomes for Māori and Pacific peoples (10), hence research into biological and other factors underlying these disparities are needed. To date glucose lowering response to different medications in people of Māori or Pacific ethnicity with T2D has not been studied. In this T2D medication, Which One is Right Here (WORTH) trial, we tested the potential stratification of comparative glycaemic response to pioglitazone (thiazolidinedione) and vildagliptin (DPP4i), by Māori or Pacific ethnicity and by OHTG status.
Materials and methods
Participant eligibility
Patients with T2D for >1 year, who had been on stable doses of metformin and/or sulfonylurea for >3 months were eligible to participate if they were aged 18–80 years inclusive, had HbA1c > 58 mmol/mol [> 7.5%] and < 111 mmol/mol [<12.3%], had never been on DPP4i or thiazolidinedione, had no insulin use, had no active infection requiring antibiotics, had no contraindication to either trial medication, and were able to give written informed consent. These eligibility criteria were modified to enable those on stable doses of two other types of oral glucose-lowering medications to participate in this trial (acarbose or dapagliflozin) as dual therapy with either metformin or sulfonylurea. Recruitment targeted 40% of participants being of Māori and/or Pacific ethnicity.
Settings and location
The trial participants were recruited at nine sites across urban (Auckland and Waikato) and rural settings (Te Tai Tokerau (Northland) and Te Tairāwhiti (East Coast of the North Island) in NZ.
Trial design
We conducted an investigator-initiated, multi-centre, open-label, two-treatment (pioglitazone 30mg once daily [P], vildagliptin 50mg once daily [V]), two-period (16-weeks each), randomised, crossover trial. There was no washout period between medications because medication withdrawal could have caused detrimental rebound hyperglycaemia and this was deemed unnecessary due to neither of the two medications having a continuing glucose lowering effect beyond 4 weeks. The primary outcome of HbA1c measurement, which reflects glycaemia over the preceding 8-12 weeks, would therefore reflect results only from the last medication during the 16-week treatment period, without any carry over effect from the first medication. The strength of the PV/VP crossover design is that both interventions were evaluated for each participant, which allows comparison at the individual rather than group level alone (11). In addition, participants could express preferences by comparing their experiences of both interventions which is not possible in a parallel group design. The trial protocol was approved by the NZ Health and Disability Ethics Committee, and has been published (12). All participants gave written informed consent.
Outcome and baseline measures
The primary outcome measure was HbA1c after each 16-week treatment period. The primary analysis was to test stratification in HbA1c response by Māori or Pacific ethnicity and the pre-specific secondary analysis was to test stratification in HbA1c response by OHTG status. To minimise confounding by adherence or treatment change, protocol adherence was considered to be those who on assessment had >75% adherence to the trial medication based on pill counts, had not commenced any additional glucose-lowering therapies since the baseline eligibility visit, and had not stopped any baseline glucose-lowering medication. HbA1c data were considered invalid if they were obtained more than 7 days after completing the study medication phase. Secondary outcome measures included body weight, blood pressure (BP), frequency of side effects, and Diabetes Treatment Satisfaction Questionnaire (DTSQ) (13) total scores, change in scores, and patient preference for either medication at the end of each treatment period. Serious adverse events (AEs) were collected throughout the trial period.
Self-reported ethnicity was recorded at the baseline visit. Participants were asked to tick all of the following categories that applied: Māori, Pacific, NZ European, Other European, Indian, Other Asian, Other (asked to specify). Prioritised ethnicity classification as Māori or Pacific was defined if either of these ethnicities were ticked or specified in “Other”. Diabetes diagnosis date, current and past diabetes medications, co-morbidities and other medications were verified by medical records. Fasting blood tests were performed to assess HbA1c, glucose, lipids, renal, liver function at baseline and were repeated at the end of each treatment period. OHTG was defined by the presence of BMI ≥30kg/m2 and/or high triglycerides ≥2.3mmol/L. Fasting C-peptide, diabetes autoantibodies and blood for genetic analysis were taken at baseline. All biochemical analyses were performed at local diagnostic laboratories with validated and accredited assays. The 3-screen islet cell autoantibody Enzyme-Linked Immunosorbent Assay (ELISA) kit (RSR limited, Cardiff, UK) was used for combined quantitative determination of glutamic acid decarboxylase (GAD), islet tyrosine phosphatase-2 (IA-2) and zinc transporter8 (ZnT8) autoantibodies in human serum. All samples testing above the assay concentration threshold of 20u/mL were tested again using separate ELISA assays for each autoantibody (Anti-GAD and Anti-IA2, Euroimmun AG, Lübeck, Germany; ZnT8, ElisaRSR, Cardiff, UK).
Randomisation
Eligible participants were randomised 1:1 to one of the two sequences (VP or PV) by a central trial pharmacist using a secure trial database. The randomised study medication was couriered to the participant’s nominated address by the central trial pharmacy. Randomisation lists were prepared by the trial statistician, using permuted block randomisation with variable block sizes (2 or 4) and stratified by recruiting region and self-reported ethnicity (Māori and Pacific vs non-Māori/non-Pacific, including New Zealand European, other European, Indian, Asian, and other groups). This was an open-label trial, where both participants and research staff were aware of the treatment sequences [VP/PV] after randomisation.
Statistical analysis
We aimed to recruit a total of 300 participants, with a target sample size of 40% Māori and Pacific people. This sample size would provide 80% power at 5% significance level to detect a minimal effect size of 0.35 standard deviation (SD) between Māori and Pacific vs non-Māori/non-Pacific groups on the difference in HbA1c between two test medications, allowing for 10% loss to follow up. Full details were reported in the published trial protocol (12).
All randomised participants were included in the primary outcome analysis, following the intention to treat (ITT) principle. Missing HbA1c data after each treatment were imputed using the baseline value or any lab data collected post-baseline before the scheduled assessment window. Per protocol (PP), analysis was also performed on the primary outcome, including only those participants who provided complete outcome data with no major protocol violations. All outcomes were assessed using valid visit data collected within the scheduled assessment window. No imputation was considered on secondary outcomes. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Baseline demographic and clinical characteristics of all randomised participants were summarised overall and by ethnicity. Continuous variables were presented as mean and SD. Categorical variables were presented in frequencies and percentages. Whether the difference in achieved HbA1c for the two medications was different between Māori and Pacific vs non-Māori/non-Pacific participants was tested using a linear mixed model with both fixed and random effects. The fixed effects included the baseline outcome value, period, medication class, patient group and its interaction with the medication. The random effect included patients as the cluster. The model-adjusted mean difference between two medications was estimated for each patient group, and the interaction effect between medications and patient groups was estimated with a 95% confidence interval (CI). Similar regression analyses were conducted to test the medication response with other patient groups of interest, including OHTG status (high BMI ≥30kg/m2 and/or high triglycerides ≥2.3mmol/L vs BMI <30kg/m2 and triglycerides <2.3mmol/L). As a secondary analysis, the overall treatment effect was compared between the two medications without the interaction with patient group term and potential carryover effect was tested. Generalised linear regression was used on other secondary outcomes collected at the end of the trial, including patient medication preference and DTSQ change score. Statistical tests were two-sided at 5% significance level. The CONSORT 2010 statement extension for randomised crossover trials was followed (14).
Results
Participant flow
A total of 346 participants who completed eligibility screening between February 2019 and March 2020, were randomised to VP or PV sequence (173 each). Of these, valid HbA1c data were obtained in 261 participants after vildagliptin and 237 participants after pioglitazone, with 203 participants completing both assessments (Figure 1). The large proportion of invalid HbA1c data was due to pandemic related delays in obtaining timely blood tests within 7 days of completing the study medication phase. There were 16 participants who withdrew during pioglitazone treatment and 15 who withdrew during vildagliptin treatment.
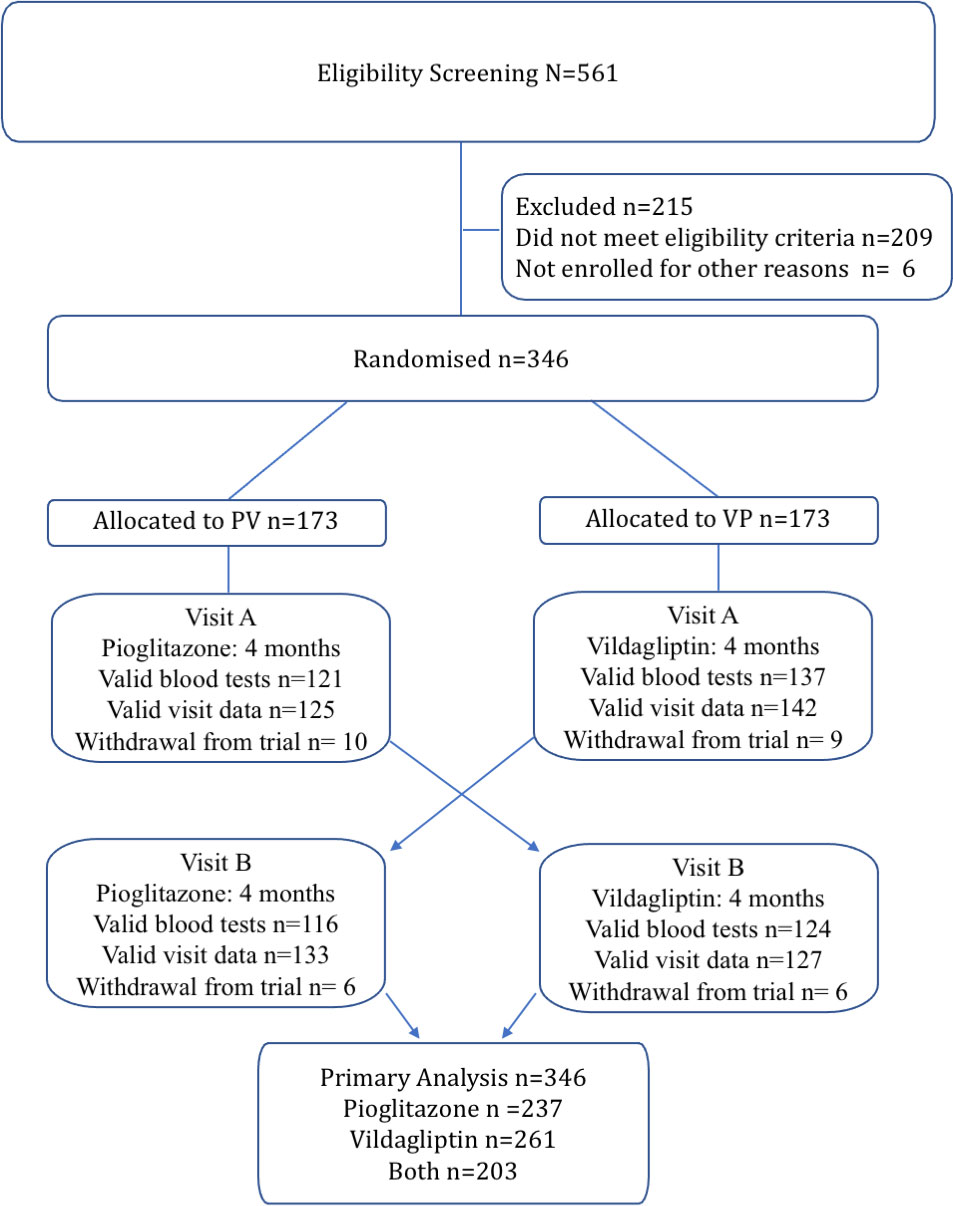
Figure 1 Flow diagram of the study participants included in this analysis.
Baseline data
The mean (SD) for age was 57.5 (10.9) years, HbA1c 75 (12) mmol/mol), [9% 1.1)], diabetes duration 9 (6) years; 41% of participants were women, 55% were Māori and/or Pacific (Table 1). Of all trial participants, 78 (23%) were Māori, 111 (32%) were Pacific people, 90 (26%) were NZ European, 67 (26%) were from other ethnic groups. There was no difference in characteristics by sequence PV vs VP. OHTG was present in 88% of Māori and Pacific participants. (Table 2). Nine participants tested positive in the triple autoantibody screening assay, verified as only GAD, (Supplementary Table 1). All had preserved fasting C-peptide (320-1983pmol/L), and were included in the analyses.
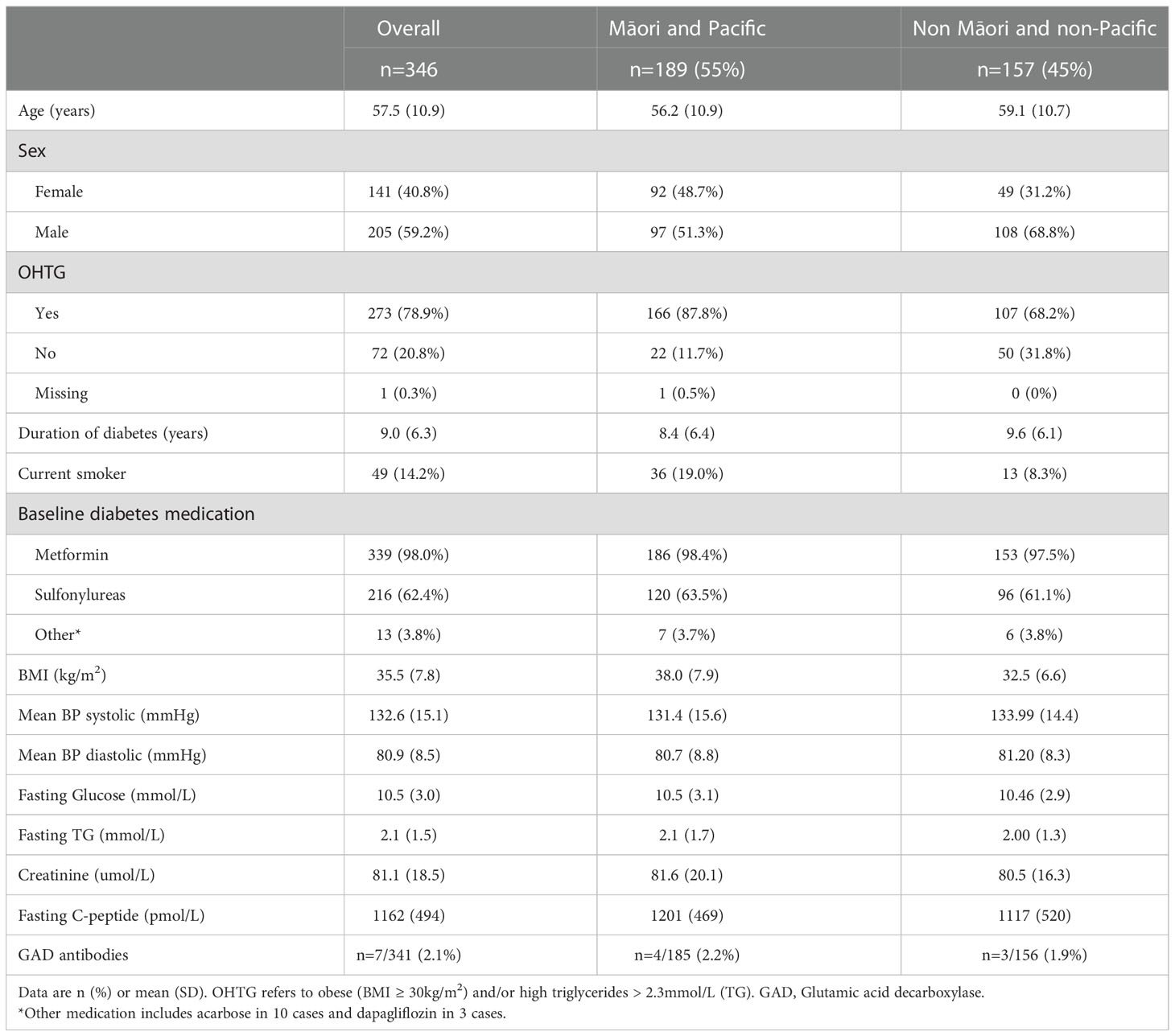
Table 1 Baseline demographics and clinical characteristics.
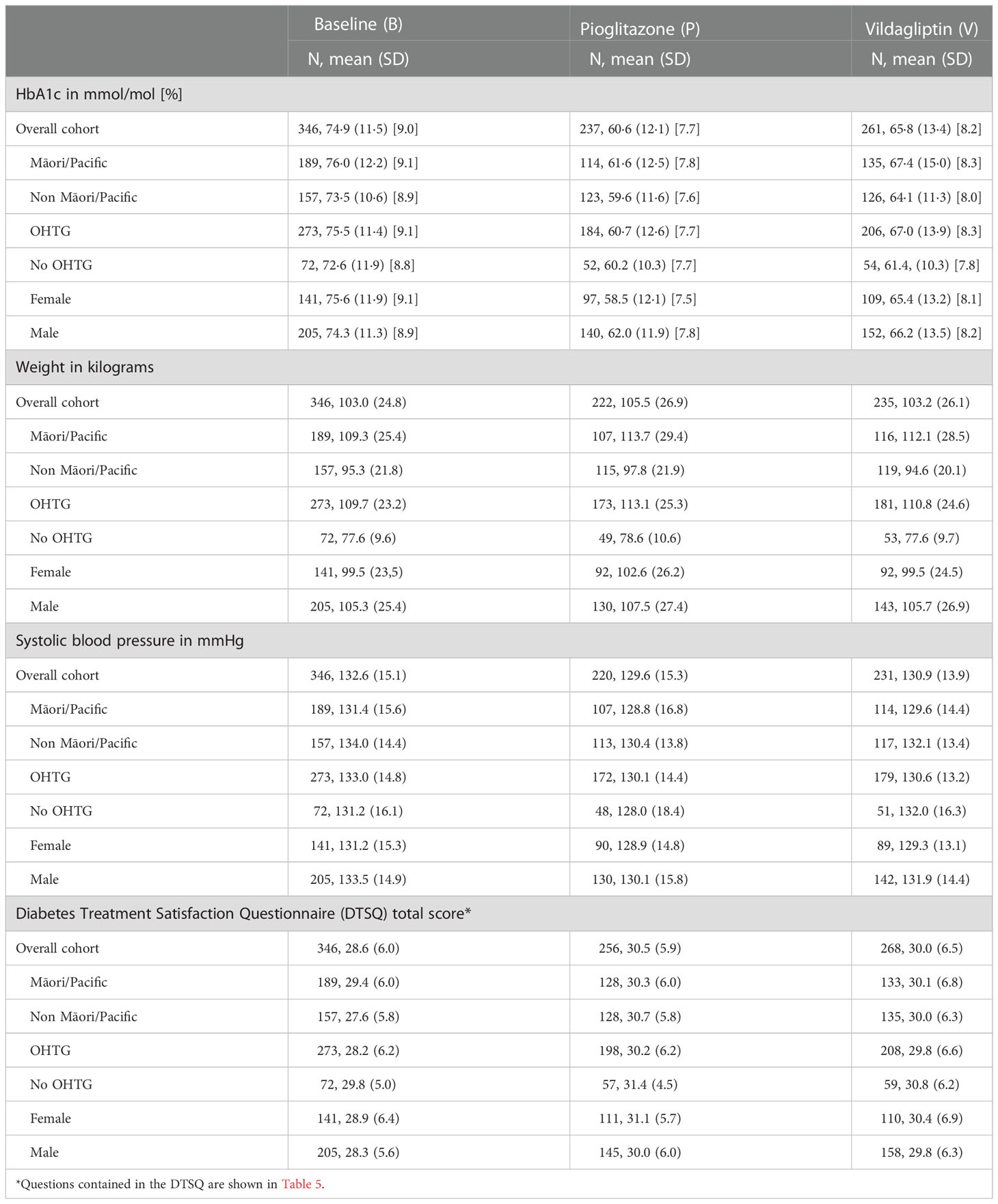
Table 2 Descriptive data at baseline and after each treatment.
Outcomes
Overall, a greater mean decrease in HbA1c was observed after pioglitazone than after vildagliptin treatment (adjusted mean difference -4.9mmol/mol [-0.5%], 95%CI -6.3, -3.5; p < 0.0001) (Table 3). No carry-over effect was found (p=0.94). The primary ITT analysis showed no interaction effect in HbA1c response between treatments (pioglitazone vs vildagliptin) by ethnicity (Māori and Pacific -2.1mmol/mol [0.19%] vs non-Māori/non-Pacific -3.6 mmol/mol [0.33%]; interaction effect 1.5mmol/mol [0.14%], 95%CI -0.8, 3.7, p= 0.2). This was consistent with the PP analysis (Māori and Pacific -6.1mmol/mol [0.56%] vs non-Māori/non-Pacific -4.9mmol/mol [0.45%]; interaction effect -1.2mmol/mol [0.11%], 95%CI -4.1, 1.7, p=0.40); and the analysis of all valid data (Māori and Pacific -5.4mmol/mol [0.5%] vs non-Māori/non-Pacific -4.4mmol/mol [0.4%], interaction effect -1.1mmol/mol [0.1%], 95%CI -3.8, 1.7; p=0.4) (Table 4).
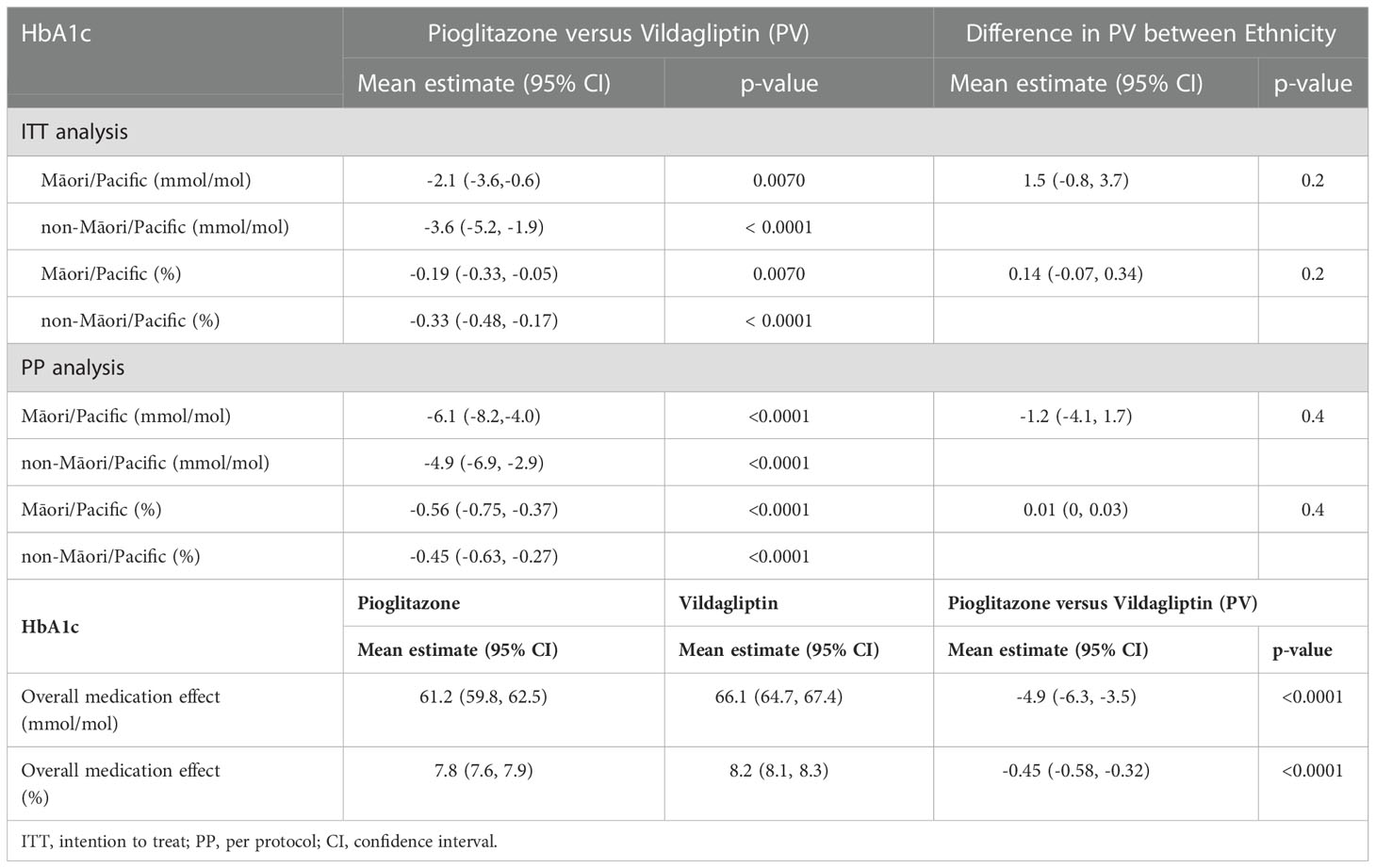
Table 3 The estimated medication effects on HbA1c and its interaction with ethnicity (primary outcome analysis).
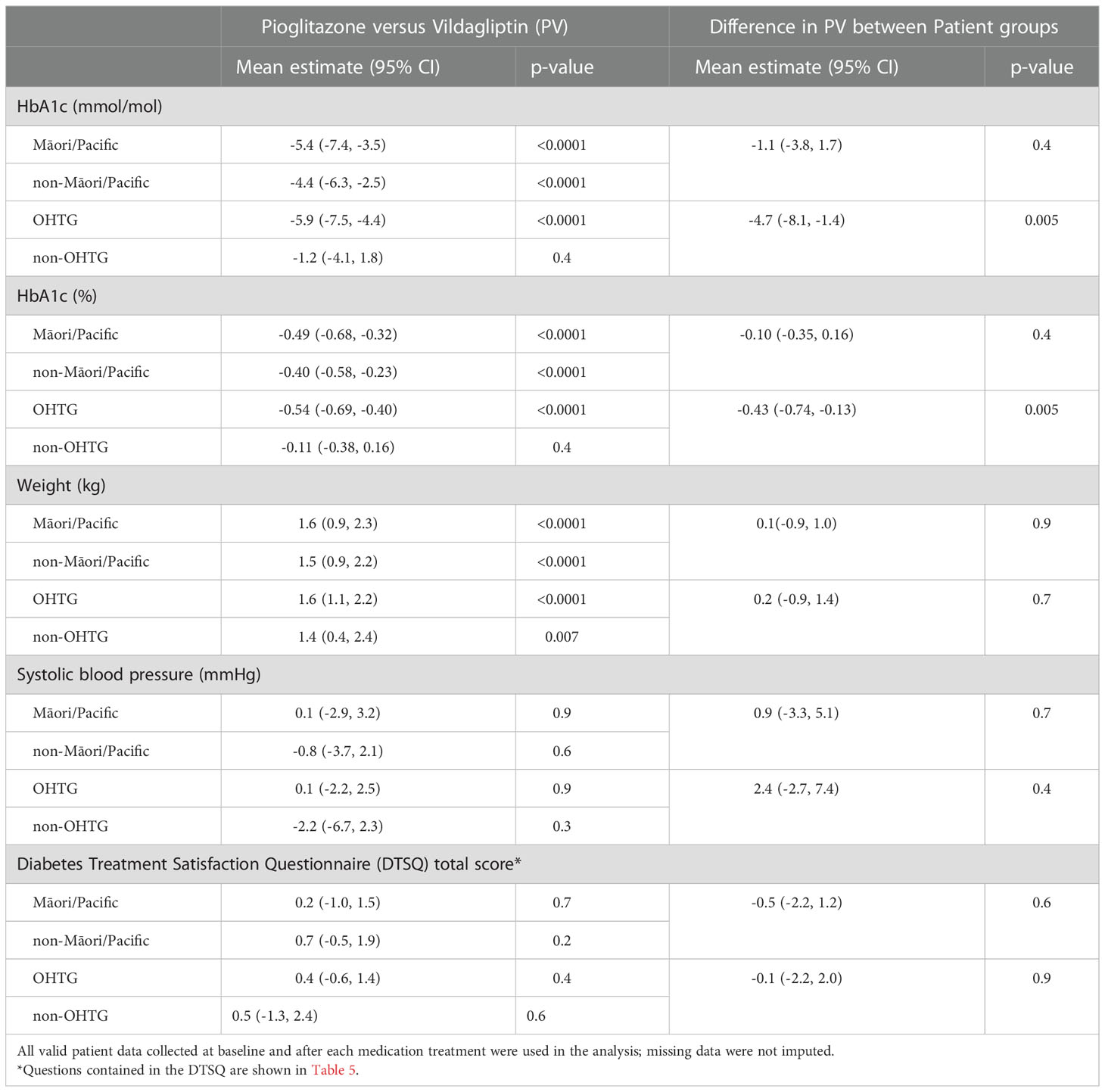
Table 4 The estimated medication effects on patient outcomes and its interaction with patient groups.
A treatment difference in HbA1c response was observed in participants with OHTG (-5.9mmol/mol [0.54%]) compared with those without OHTG (-1.2mmol/mol [0.11%]), with an estimated interaction effect of -4.7mmol/mol [0.43%], 95%CI -8.1, -1.4, p=0.005 (Table 4).
Mean weight after pioglitazone was higher than after vildagliptin treatment, with an adjusted mean difference of 1.6kg (95%CI [1.1, 2.0]; p<0.0001). There was no interaction in weight change response to pioglitazone versus vildagliptin by ethnicity or OHTG status (Table 4). BP and DTSQ did not differ by treatment group in the overall analysis, by ethnicity, or OHTG status (Tables 4, 5). There was no significant carryover effect detected for weight (p=0.66). There were 27 (7.8%) participants reporting new or worsening pedal edema after pioglitazone and 15 (4.3%) after vildagliptin (Chi-square p=0.06).
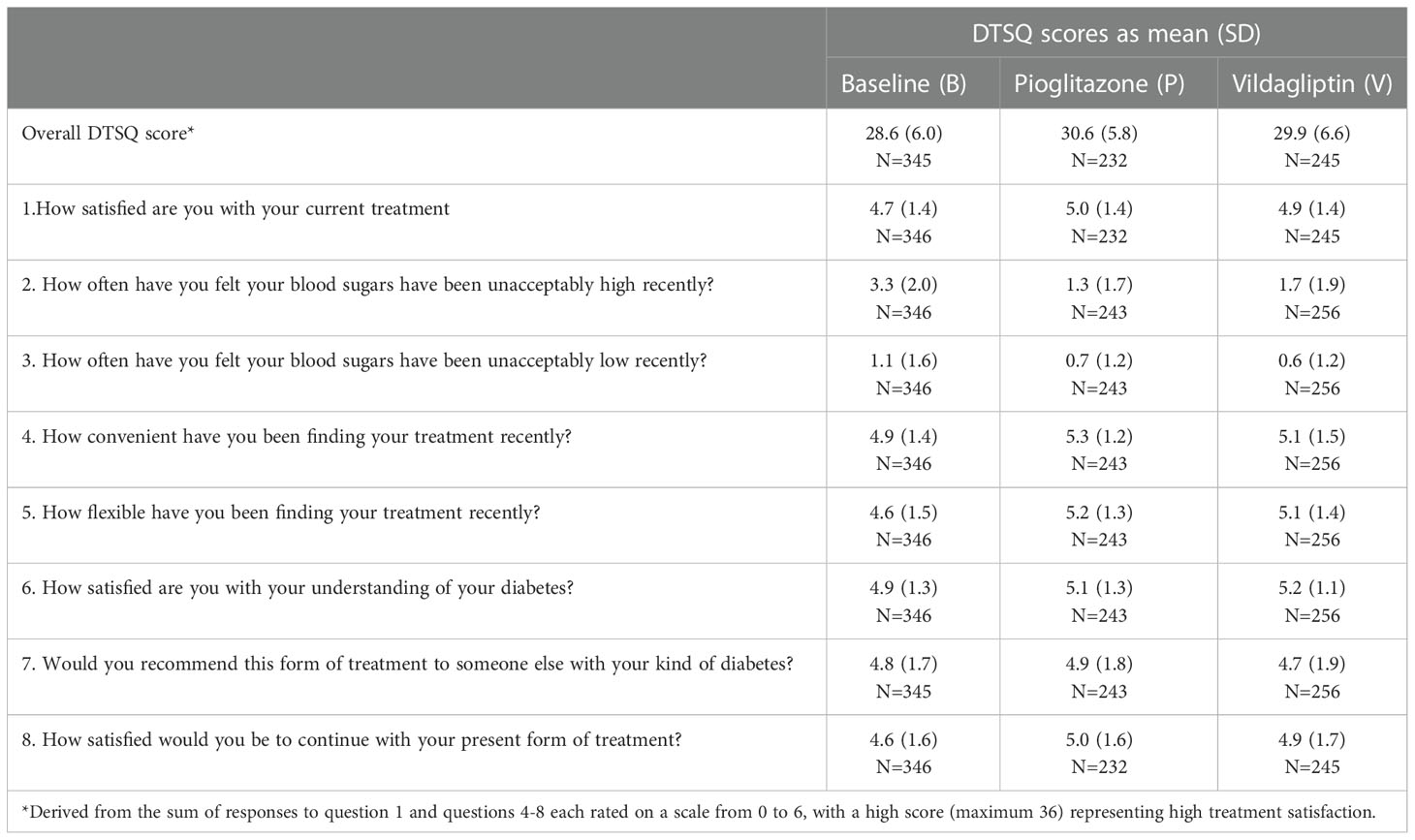
Table 5 DTSQ scores at baseline and after each treatment.
Hepatic enzymes, alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT) were lower after pioglitazone but remained unchanged after vildagliptin (difference p<0.0001). The difference in hepatic enzymes after pioglitazone vs vildagliptin, did not differ significantly by Māori and Pacific ethnicity or OHTG. Triglycerides reduced after pioglitazone compared with after vildagliptin (mean difference -0.3mmol/L, p<0.0001), with no interaction by ethnicity or OHTG grouping. HDL-C increased more after pioglitazone than after vildagliptin (+0.1mmol/L, p<0.0001).
At the final trial visit, 257 participants indicated their preferred medication: 98 (38%) preferred pioglitazone, 87 (34%) preferred vildagliptin, and 72 (28%) indicated either no preference (n=62) or neither (n=10). No differences in medication preference were found by ethnicity, or OHTG strata after adjusting for their treatment sequence (PV or VP), the change in HbA1c, weight and DTSQ score between two treatments.
There were 15 serious adverse events: 3 deaths (2 strokes and 1 myocardial infarction) and 12 hospitalisations. None were deemed to be due to the trial medication by an independent data safety monitoring committee.
Discussion
This multicentre, two-way, randomised crossover trial showed that the glucose-lowering response to pioglitazone relative to vildagliptin was not different between people of Māori or Pacific ethnicity and other New Zealand ethnicities. However, there was a significant interaction in relative glucose-lowering by OHTG status, with 4.7mmol/mol greater reduction in HbA1c by pioglitazone relative to vildagliptin among those with OHTG. Those without OHTG had similar glucose lowering to each medication. Importantly, both treatments generated similar treatment satisfaction scores although there was greater weight gain and greater improvement in lipids and liver enzymes after pioglitazone than vildagliptin. No severe adverse events were directly related to these treatments.
While people of Māori or Pacific ethnicity had higher prevalence of OHTG, such ethnicity grouping did not predict altered glucose lowering response to pioglitazone versus vildagliptin. Within Māori and Pacific populations, there is genetic heterogeneity in risk and aetiology of T2D. A genetic variant (rs373863828, p.Arg457Gln) in the CREBRF gene, specifically found in approximately 25% people of Māori and Pacific ancestry, is associated with increased body mass index (15, 16) yet 40% lower odds of T2D (15, 16), due to enhanced insulin secretion capacity (17). Testing whether CREBRF gene variant status has utility in predicting stratified glucose lowering responses to T2D medications among people of Māori and Pacific ethnicity is currently underway (12). OHTG status has been reported to predict lower glucose response in studies with European participants (6).
In contrast to rosiglitazone, which is no longer used due to its associated increased risk of myocardial infarction and overall mortality (18), pioglitazone has demonstrable cardiovascular benefits (19, 20). This is thought to be partly due to its favourable impact on lipids (21, 22), which was also observed in this trial. In addition, our finding of improvement in liver enzymes with pioglitazone treatment is consistent with its reported benefits in non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Whilst the weight gain with pioglitazone has been highlighted as a caution for its use, our data suggests the weight gain was mild and did not reduce patient satisfaction.
The lack of interaction of reduction in liver enzymes or lipids after pioglitazone with baseline OHTG is interesting. One explanation is that the glucose lowering action of pioglitazone is mediated by ligand binding to nuclear receptor PPARG which are most abundant in adipocytes and hence greater in people with obesity (23). In contrast, the liver enzyme or lipid lowering action of pioglitazone may be mediated by other pathways that are not directly correlated with baseline OHTG status such as PPAR alpha expression (24).
Comparative medication glucose response data from this crossover study design provides evidence-based understanding of how patients would respond if they were to switch from one medication to another. While this is something that happens frequently in diabetes care, there is very limited clinical data about how patients’ glycaemic control changes when this happens or which medication they prefer. In addition, several consensus reports describe that when making treatment decisions for patients with type 2 diabetes it is important to consider not only the efficacy and safety of each medication, but also patient preference. This open-label cross-over study provides the added value of patient preference outcomes between pioglitazone and vildagliptin in the real-world setting. The protocol for a three-way crossover study including a DPP4 inhibitor, thiazolidinedione and a SGLT2 inhibitor has been described, which will provide further information on stratification of glucose response to three diabetes medications by routine clinical features ascertained at baseline (25).
A key limitation of this trial was the low follow up rate resulting in only 203 participants with valid HbA1c data after both treatments. Some of this related to difficulties encountered during the pandemic in obtaining a timely HbA1c result at the end of each study medication treatment phase and in conducting in person assessments. This is unlikely to have introduced any retention bias as each person contributed their own comparative data for both medications. Furthermore, the analysis was conducted with and without imputation on the primary analysis population, to test the robustness of the findings. Secondly, the open-label nature of the trial was selected for lower cost and complexity, which may have introduced observer and participant bias, but increased external validity. Thirdly, the crossover trial design might have led to the inappropriate estimation of the risk of weight gain with each medication, although the sensitivity analysis showed no significant carryover effect. The crossover design was selected as the best method to test differential glucose-lowering responses using HbA1c as the primary outcome measure between two diabetes medications in different patient subgroups (11). A longer treatment duration of each period could have mitigated against the slow onset and offset of each medication in absence of wash-out period. However, the 16-week consecutive treatment period was considered the most efficient study design.
It is well recognised that overall glucose lowering effects of pioglitazone are typically greater than vildagliptin. The important finding of this study is that a superior glucose-lowering response to pioglitazone versus vildagliptin is observed mainly in those with OHTG. Whilst OHTG is more prevalent in those of Māori and Pacific ethnicity, the glucose-lowering response was not significantly different by such ethnicity group in a multi-ethnic New Zealand population. This has several clinical implications. Firstly, these findings suggest that ethnicity is not a sufficient proxy for stratified medicine for pioglitazone and vildagliptin in T2D. Rather, clinical markers of insulin resistance that are routinely available in clinical practice such as BMI and triglyceride levels are able to predict whether superior glucose lowering response to pioglitazone relative to vildagliptin is expected. The recent progress in better defining novel T2D subtypes based on underpinning disease mechanisms such as age at diabetes diagnosis, GAD antibodies, C-peptide and genetic factors need to be explored for their utility in predicting other stratified glucose lowering responses (26). However, the use of non-routine biomarkers are less easily adopted in clinical practice. Secondly, the participant satisfaction data suggests people are generally not troubled by the small weight increase from pioglitazone so this medication is best selected for those with OHTG to maximise risk vs benefits. Finally, T2D treatment guidelines could include consideration of OHTG to inform treatment selection between vildagliptin and pioglitazone. Including a more prominent role for pioglitazone over vildagliptin in the presence of OHTG would be reasonable since this medication produces much greater glucose lowering in this subgroup. This is a robust finding that has now been replicated in a non-European population. Pioglitazone treatment selection will need to be considered in the context of other common indications for this medication such as fatty liver or dyslipidaemia, and relatively uncommon contraindications such as heart failure, osteoporosis and macular oedema, as part of individualised care based on patient characteristics.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by NZ Health and Disability Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RM designed the trial. YJ was responsible for the statistical analysis of the data. TRM was responsible for the genetic analysis plan. ML designed the population-specific genetic variant panel. TM assisted with genetic analysis of the data. RM and PRS obtained funding. RB, RY, RT-C, KS, GD, KAM, RD, PC, AM, NN, FK, JH, BO-W, and RP were responsible for trial implementation and data acquisition. RB and RM wrote the first draft of this manuscript and RM handled the revisions. All authors reviewed the manuscript and approved the final version for submission.
Funding
This study received funding from Health Research Council Programme Grant 18-1681, Middlemore clinical trial research grant and Maurice Wilkins Centre for Molecular Biodiscovery. The trial’s funders had no role in trial design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to all the data in the trial and had final responsibility for the decision to submit for publication.
Acknowledgments
We are grateful to all the participants who took part in this study. We acknowledge Yiping Zou and Stacey Ruru for assisting with the data collection for this trial. We are grateful for the helpful input from John Baker in the planning of this trial; pharmacist Dale Griffiths and the team from zoom pharmacy who dispensed and couriered trial medication to participants; Chris McKinlay and the study database design and support team. We are grateful to Manish Khanolkar and Geoff Braatvedt for providing adjudication for serious adverse events in this trial. We thank the trial staff at each site, particularly Hinemoa McLelland (Research Nurse) for Ngāti Porou Hauora site; Mele Vaka (Research Nurse) from Tongan Health Society; Melissa Peterson (Research Nurse) from Te Hiku Hauora; Gillian Stonelake (Research GP) for Waikato; Diane Caveney and Liz Walker (Research Nurses) from Middlemore Clinical Trials; Trish Harry (Research Co-ordinator) from Diabetes Foundation Aotearoa. We acknowledge Riku Takei for assistance with the PC analysis.
Conflict of interest
Authors RP and RM have received speaking honoraria from Lilly, Boehringer Ingelheim, Astra Zeneca, Sanofi, Novo Nordisk, also Novartis (RM) and Inova pharmaceuticals (RP). RP is a member of the Lilly, Novo Nordisk and Dexcom New Zealand advisory boards. Authors KAM, RD, PC were employed by Ventures/Pinnacle Incorporated, a primary health care organisation which has no relevant commercial or financial relationships.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.1091421/full#supplementary-material
References
1. American Diabetes Association. Pharmacologic approaches to glycemic treatment. Diabetes Care (2021) 44:S111–24. doi: 10.2337/dc21-S009
2. Chung WK, Erion K, Florez JC, Hattersley AT, Hivert M-F, Lee CG, et al. Precision medicine in diabetes: A consensus report from the American diabetes association (ADA) and the European association for the study of diabetes (EASD). Diabetes Care (2020) 43:1617–35. doi: 10.2337/dci20-0022
3. Gan S, Dawed AY, Donnelly LA, Nair ATN, Palmer CAN, Mohan V, et al. Efficacy of modern diabetes treatments DPP-4i, SGLT-2i, and GLP-1RA in white and Asian patients with diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Care (2020) 43:1948–57. doi: 10.2337/dc19-2419
4. Williams LK, Padhukasahasram B, Ahmedani BK, Peterson EL, Wells KE, Gonzalez Burchard E, et al. Differing effects of metformin on glycemic control by race-ethnicity. J Clin Endocrinol Metab (2014) 99:3160–8. doi: 10.1210/jc.2014-1539
5. Weng J, Soegondo S, Schnell O, Sheu WH-H, Grzeszczak W, Watada H, et al. Efficacy of acarbose in different geographical regions of the world: Analysis of a real-life database. Diabetes Metab Res Rev (2015) 31:155–67. doi: 10.1002/dmrr.2576
6. Dennis JM, Shields BM, Hill AV, Knight BA, McDonald TJ, Rodgers LR, et al. Precision medicine in type 2 diabetes: Clinical markers of insulin resistance are associated with altered short- and long-term glycemic response to DPP-4 inhibitor therapy. Diabetes Care (2018) 41:705–12. doi: 10.2337/dc17-1827
7. Dennis JM, Henley WE, Weedon MN, Lonergan M, Rodgers LR, Jones AG, et al. Sex and BMI alter the benefits and risks of sulfonylureas and thiazolidinediones in type 2 diabetes: A framework for evaluating stratification using routine clinical and individual trial data. Diabetes Care (2018) 41:1844–53. doi: 10.2337/dc18-0344
8. Gentles D, Metcalf P, Dyall L, Scragg R, Sundborn G, Schaaf D, et al. Serum lipid levels for a multicultural population in Auckland, new Zealand: results from the diabetes heart and health survey (DHAH) 2002-2003. N Z Med J (2007) 120:U2800.
9. Ministry of Health. Annual data explorer 2020/2021: New Zealand health survey (2021). Available at: https://minhealthnz.shinyapps.io/nz-health-survey-2020-21-annual-data-explorer/.
10. Yu D, Zhao Z, Osuagwu UL, Pickering K, Baker J, Cutfield R, et al. Ethnic differences in mortality and hospital admission rates between māori, pacific, and European new Zealanders with type 2 diabetes between 1994 and 2018: A retrospective, population-based, longitudinal cohort study. Lancet Glob Health (2021) 9:e209–17. doi: 10.1016/S2214-109X(20)30412-5
11. Lonergan M, Senn SJ, McNamee C, Daly AK, Sutton R, Hattersley A, et al. Defining drug response for stratified medicine. Drug Discovery Today (2017) 22:173–9. doi: 10.1016/j.drudis.2016.10.016
12. Yeu RQ, Brandon R, Jiang Y, Griffiths D, Smallman K, Moffitt A, et al. Randomised cross-over trial of vildagliptin and pioglitazone as add-on therapy in patients with type 2 diabetes: Predicting which one is right here (WORTH) study protocol. BMJ Open (2020) 10:e036518. doi: 10.1136/bmjopen-2019-036518
13. Bradley C, Speight J. Patient perceptions of diabetes and diabetes therapy: Assessing quality of life. Diabetes Metab Res Rev (2002) 18(Suppl 3):S64–69. doi: 10.1002/dmrr.279
14. Dwan K, Li T, Altman DG, Elbourne D. CONSORT 2010 statement: Extension to randomised crossover trials. BMJ (2019) 366:l4378. doi: 10.1136/bmj.l4378
15. Minster RL, Hawley NL, Su C-T, Sun G, Kershaw EE, Cheng H, et al. A thrifty variant in CREBRF strongly influences body mass index in samoans. Nat Genet (2016) 48:1049–54. doi: 10.1038/ng.3620
16. Krishnan M, Major TJ, Topless RK, Dewes O, Yu L, Thompson JMD, et al. Discordant association of the CREBRF rs373863828 a allele with increased BMI and protection from type 2 diabetes in Maori and pacific (Polynesian) people living in Aotearoa/New Zealand. Diabetologia (2018) 61:1603–13. doi: 10.1007/s00125-018-4623-1
17. Burden HJ, Adams S, Kulatea B, Wright-McNaughton M, Sword D, Ormsbee JJ, et al. The CREBRF diabetes-protective rs373863828-a allele is associated with enhanced early insulin release in men of māori and pacific ancestry. Diabetologia (2021) 64:2779–89. doi: 10.1007/s00125-021-5552-x
18. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med (2007) 356:2457–71. doi: 10.1056/NEJMoa072761
19. Dormandy JA, Charbonnel B, Eckland DJA, Erdmann E, Massi-Benedetii M, Moules IK, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive study (PROspective pioglitAzone clinical trial in macroVascular events): A randomised controlled trial. Lancet (2005) 366:1279–89. doi: 10.1016/S0140-6736(05)67528-9
20. Erdmann E, Dormandy JA, Charbonnel B, Massi-Benedetti M, Moules IK, Skene AM, et al. The effect of pioglitazone on recurrent myocardial infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction: Results from the PROactive (PROactive 05) study. J Am Coll Cardiol (2007) 49:1772–80. doi: 10.1016/j.jacc.2006.12.048
21. Deeg MA, Buse JB, Goldberg RB, Kendall DM, Zagar AJ, Jacober SJ, et al. Pioglitazone and rosiglitazone have different effects on serum lipoprotein particle concentrations and sizes in patients with type 2 diabetes and dyslipidemia. Diabetes Care (2007) 30:2458–64. doi: 10.2337/dc06-1903
22. Schernthaner G, Chilton RJ. Cardiovascular risk and thiazolidinediones–what do meta-analyses really tell us? Diabetes Obes Metab (2010) 12:1023–35. doi: 10.1111/j.1463-1326.2010.01262.x
23. Spiegelman BM. PPAR-gamma: Adipogenic regulator and thiazoledinedione receptor. Diabetes (1998) 47:507–14. doi: 10.2337/diabetes.46.4.507
24. Orasanu G, Ziouzenkova O, Devchand PR, Nehra V, Hamdy O, Horton ES, et al. The PPARG agonist pioglitazone represses inflammation in a PPARG alpha-dependent manner: in vitro and in vivo in mice. J Am Coll Cardiol (2008) 52:869–81. doi: 10.1016/j.jacc.2008.04.055
25. Angwin C, Jenkinson C, Jones A, Jennison C, Henley W, Farmer A, et al. TriMaster: Randomised double-blind crossover study of a DPP4 inhibitor, SGLT2 inhibitor and thiazoleidinedione as second-line or third-line therapy in patients with type 2 diabetes who have suboptimal glycemic control on metformin treatment with or without a sulfonylurea – a MASTERMIND study protocol. BMJ Open (2020) 10:e04278. doi: 10.1136/bmjopen-2020-042784
Keywords: dipeptidyl peptidase inhibitor, Māori, Pacific, pioglitazone, precision medicine, stratified drug response, thiazolidinedione, obesity
Citation: Brandon R, Jiang Y, Yeu RQ, Tweedie-Cullen R, Smallman K, Doherty G, Macaskill-Smith KA, Doran RJ, Clark P, Moffitt A, Merry T, Nehren N, King F, Hindmarsh JH, Leask MP, Merriman TR, Orr-Walker B, Shepherd PR, Paul R and Murphy R (2023) Stratified glucose-lowering response to vildagliptin and pioglitazone by obesity and hypertriglyceridemia in a randomized crossover trial. Front. Endocrinol. 13:1091421. doi: 10.3389/fendo.2022.1091421
Received: 07 November 2022; Accepted: 02 December 2022;
Published: 09 January 2023.
Edited by:
Pranav Kumar Prabhakar, Lovely Professional University, IndiaReviewed by:
Gopal L. Khatik, National Institute of Pharmaceutical Education and Research, IndiaEwan Pearson, University of Dundee, United Kingdom
Copyright © 2023 Brandon, Jiang, Yeu, Tweedie-Cullen, Smallman, Doherty, Macaskill-Smith, Doran, Clark, Moffitt, Merry, Nehren, King, Hindmarsh, Leask, Merriman, Orr-Walker, Shepherd, Paul and Murphy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rinki Murphy, r.murphy@auckland.ac.nz