 Silvia Cruchet1
Silvia Cruchet1 Sandra Hirsch1
Sandra Hirsch1 Diana Villa-López2Mucio Moreno-Portillo2Juan C. Palomo2Ana T. Abreu-Abreu3Juan M. Abdo-Francis4
Diana Villa-López2Mucio Moreno-Portillo2Juan C. Palomo2Ana T. Abreu-Abreu3Juan M. Abdo-Francis4 Carlos Jiménez-Gutiérrez2Martin Rojano2
Carlos Jiménez-Gutiérrez2Martin Rojano2 Gabriel López-Velázquez5
Gabriel López-Velázquez5 Pedro Gutiérrez-Castrellón6*
Pedro Gutiérrez-Castrellón6*- 1Instituto de Nutrición y Tecnología de los Alimentos (INTA), Universidad de Chile, Santiago de Chile, Chile
- 2Gastroenterology Department, Hospital General Dr. Manuel Gea González, Mexico City, Mexico
- 3Gastroenterology Department, Hospital Ángeles Pedregal, Mexico City, Mexico
- 4Gastroenterology Department, Hospital Ángeles Acoxpa, Mexico City, Mexico
- 5Laboratorio de Biomoléculas y Salud Infantil, Instituto Nacional de Pediatría, Mexico City, Mexico
- 6Traslational Research Division, International Scientific Council for Probiotics, Mexico City, Mexico
Background: Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder in adults. Systematic reviews with meta-analyses have demonstrated the efficacy and safety of probiotics in improving symptoms of IBS.
Aim: The aim of the study was to demonstrate the efficacy and safety of Limosilactobacillus reuteri (L. reuteri) DSM 17938 combined with L. reuteri ATCC PTA 6475 regarding improving the symptoms associated with IBS in adults.
Methods: A randomized, double-blind, placebo-controlled clinical trial was conducted in 140 adults aged 18 years to 65 years with a diagnosis of IBS (based on the Rome IV criteria). After 2 weeks of washout, subjects were randomized to receive either 2 × 108 colony-forming units (CFUs) of L. reuteri DSM 17938 combined with L. reuteri ATCC PTA 6475 plus standard of care or placebo plus standard of care for 14 weeks, followed by a post-intervention period of 2 additional weeks. Changes in gastrointestinal symptoms (as measured with the GSRS-IBS), stool pattern (as measured with the Bristol scale), quality of life, depression and anxiety, frequency of adverse events, and fecal calprotectin concentrations were evaluated.
Results: In total, 70 subjects were allocated to receive L. reuteri and 70 were allocated to receive placebo. During the pre-randomization phase, no differences were observed between the groups in terms of IBS-associated symptoms and stool consistency. Starting at week 6 of the intervention, subjects in group L. reuteri showed a significant improvement in IBS-associated symptoms (p < 0.01). A significant improvement was also observed in fecal calprotectin concentration in the L. reuteri group at the end of interventions (30.2 ± 11.8 mg/g of stool in the L. reuteri group and 41.6 mg/g ± 10.7 mg/g in the placebo group; p = 0.019). The frequency of adverse events was similar between groups.
Conclusions: A twice-a-day intervention for 14 weeks is safe and effective, reduces the symptoms associated with IBS in adults aged 18 years to 65 years, improves stool consistency, and reduces symptoms associated with anxiety after 6 weeks.
Background
Irritable bowel syndrome (IBS) is the most common functional gastrointestinal disorder in adults. It is characterized by chronic abdominal pain and changes in bowel habits without an identifiable organic cause. Its prevalence is approximately 10%–15% (1–5). Annually, IBS accounts for approximately 3.1 million outpatient medical visits in the United States, with a cost exceeding $20 billion (6, 7). It is most common in women and in people aged between 20 years and 40 years (8).
IBS is characterized clinically by chronic abdominal pain of variable intensity and periodic exacerbations, changes in stool form (diarrhea, constipation, or both), and the sensation of incomplete evacuation, even when the rectum is empty, among other characteristics. It can be associated with various extraintestinal symptoms, such as altered sexual function, dysmenorrhea, dyspareunia, and increased urinary frequency and urgency (8, 9). Its pathogenesis is complex, and various intestinal motor function alterations, a prolonged gastrointestinal transit time, an exaggerated motor response, the hyperexcitability of various receptors on the intestinal wall to stimuli, such as histamine, nitric oxide, and proteases, and changes in intestinal microbiota profiles, among other factors, have been described as generators of the syndrome (9).
Its definition has changed over time. The ROME IV criteria describe four subtypes: IBS with predominant constipation (i.e., hard or lumpy stools in ≥ 25% of evacuations or soft or watery in < 25% of evacuations), IBS with predominant diarrhea (i.e., watery or soft stools in ≥ 25% of evacuations/hard or lumpy stools in < 5% of evacuations), mixed IBS (i.e., hard or lumpy stools in ≥ 25% of evacuations/watery stools in ≥ 25% of evacuations), and undetermined IBS (10–12).
From a therapeutic point of view, modifying dietary habits represents one of the most frequently used treatments (13). Increasing fiber intake represents one of the most common dietary modifications. Considering the changes observed in the intestinal microbiota profiles in these patients, the beneficial effects of fiber may reflect the increase in the production of short-chain fatty acids and their actions as prebiotics (14). Another dietary alternative is the low-FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet, which continues to generate controversies (15–24).
Considering the changes that have been observed for several years in the intestinal microbiota profiles in the subjects with IBS, the coadjuvant role of probiotics in controlling gastrointestinal symptoms was analyzed. In 2015, a systematic review was published in which 24 clinical trials were included, with 1,793 subjects. A significant improvement in abdominal pain (RR 1.96, 95% CI 1.14 to 3.36; p = 0.01), an improvement in the global symptoms scale score (RR 2.4, 95% CI 1.13 to 5.21; p = 0.02), and a specific effect on abdominal distension, pain, inflammation, and flatulence (SMD −2.57, 95% CI −13.05 to −0.92) were observed (25).
Recently, a meta-analysis on the impact of the administration of probiotics in adults with IBS was published. A total of 35 clinical trials were included in the study, with more than 3,452 subjects; the results indicated that, compared with placebo, probiotics reduced the incidence of persistent symptoms (RR 0.79, 95% CI 0.70 to 0.89; p 0.0001) and improved global symptoms and the abdominal pain score (SMD –0.25, 95% CI –0.36 to –0.14; p = 0.00001), abdominal distension score (SMD −0.15, 95% CI −0.27 to −0.03; p = 0.01), and flatulence score (SMD −0.20, 95% CI −0.35 to −0.05; p = 0.01), without conclusively establishing the predominance of any particular type of probiotic (26).
Limosilactobacillus reuteri DSM 17938 and L. reuteri ATCC PTA 6475 are two strains of L. reuteri species, with specific modes of action as identified in vitro and in animal models, showing clear anti-inflammatory potential as well as intestinal epithelial integrity and gut homeostasis capabilities. Both strains showed tolerance to gastric juice and no viability reduction after simulated gastric transit over 180 min (27). L. reuteri ATCC PTA 6475 showed higher adhesion capacity to epithelial cell lines and a mucus layer in vitro than L. reuteri DSM 17938 (27, 28). L. reuteri DSM 17938 has been shown to improve epithelial barrier function by increasing the expression of tight junction proteins and dramatically increasing enterocyte migration and proliferation in the neonatal mouse intestine (29). Interestingly, L. reuteri ATCC PTA 6475 has been shown to support gastrointestinal homeostasis by inducing histamine responses that suppress the development of inflammation-associated colon cancer in mice (30), while L. reuteri DSM 17938 showed strong antipathogenic activity through the induction of reuterin in vitro (31). Moreover, while L. reuteri ATCC PTA 6475 supports important gut–brain signaling pathways by inducing oxytocin in an autism spectrum disorder mouse model (32), L. reuteri DSM 17938 has been shown to reduce TRPV1 pain receptor signaling in mice (33). Given the mechanisms induced by these two L. reuteri strains, we decided to explore their effect in the context of IBS. The primary endpoint of this trial was to evaluate the efficacy of administering L. reuteri DSM 17938 and L. reuteri ATCC PTA 6475 for a total of 14 weeks on the global clinical improvements in gastrointestinal symptoms, evaluated using the GSRS-IBS. Second, we evaluated the effects of the intervention on the consistency of bowel movements, quality of life, depression and anxiety scores, fecal calprotectin levels, and frequency of potentially related adverse events.
Materials and methods
This was a randomized, double-blind, multi-center clinical trial with two parallel treatment arms that was approved by the Research Committee and Research Ethics Committee of the Institute of Nutrition and Food Technology, Chile, and by the Research and Research Ethics Committees of Dr. Manuel Gea González General Hospital, Mexico (approval number 04–17–2018); the study is registered at clinicaltrials.gov as NCT04037826. A total of 140 adults aged 18 years to 65 years of either sex with a body mass index of ≤ 3 kg/m2 and a diagnosis of IBS based on the Rome IV criteria (i.e., recurrent abdominal pain, on average at least once per week in the last 3 months, related to defecation, associated with a change in the frequency of stools, and/or associated with a change in the appearance of bowel movements) were included; the participants were identified at the gastroenterology departments of the aforementioned institutions between 27 March 2018 and 22 August 2019, with completion of follow-up occurring in December 2019. Subjects with relevant systemic, organic, or metabolic diseases other than IBS; subjects with a recent history of previous major abdominal surgery; and subjects who had consumed antibiotics, proton pump inhibitors, H2 antagonists, or probiotics for at least 48 continuous hours in the 2 weeks before the baseline evaluation were excluded from the study. Considering the results published in 2016 by Yan Zhang et al. (34) in which an improvement in the global score of the IBS symptom severity scale (GSRS-IBS) was identified in 700 patients with IBS assigned to the probiotic group, compared with 575 patients with IBS included in the control group (53.3% vs. 27.7%), with an alpha error of 5%, a power of 80%, and a potential loss to follow-up of 20%, the minimum sample size was calculated as 70 subjects per treatment arm, for a total of 140 subjects in the study. Once the selection criteria were met, the subjects who signed an informed consent form were invited to participate in a 2-week pre-randomization evaluation period; the frequency and intensity of their gastrointestinal manifestations were evaluated using the gastrointestinal symptoms rating scale specific to IBS (GSRS-IBS) (35). The subjects were standardized in two sessions to use GSRS-IBS by sub-investigators. Before the recruited subjects started to fill the GSRS-IBS daily report form, they were requested to practice on a dummy version until they understand and do not have mistakes. After that they were allowed to fill the daily report form. The characteristics of their bowel movements were evaluated using the Bristol scale, the quality-of-life score was evaluated using IBS QoL Score (36), and depression and anxiety by the Goldberg Scale (37). FODMAPs and concomitant medications received during the period were also evaluated. The eating pattern was evaluated by requesting subjects to report in the diary report form 2 days during the week and 1 day during the weekend for the frequency and number of foods. Once the 2-week pre-randomization period was completed, the subjects were given an appointment for a new evaluation. For those subjects who met the IBS criteria, randomization was carried out to blindly determine who received L. reuteri ‘Gastrus’ (L. reuteri DSM 17938 and L. reuteri ATCC PTA 6475; BioGaia, Stockholm, Sweden), which contained a minimum of 2 × 108 CFU, one chewable tablet twice daily, for a minimum total daily dose of 4 × 108 CFU/day for 14 weeks, or placebo at the same frequency and for the same time interval. The placebo product was of identical composition except that it lacked bacteria. The study product was kept refrigerated (2°C–8°C) during the study period. To maintain adherence, subjects received a phone call every week to evaluate follow-up and reinforce the use of the investigational product. On every in-place visit, the investigator reinforced the importance of continuing to take the products.
The allocation of interventions was completely blinded for both the researcher and the participant. The sponsor carried out centralized randomization and the codes were kept safe by the non-blinded pharmacist until the end of the trial. Before the start of the interventions, and in addition to the clinical scales, a baseline sample of fecal matter was obtained to measure fecal calprotectin concentrations. During the 14-week intervention period, the GSRS-IBS, the Bristol scale, the quality-of-life scale, and the depression and anxiety scale were administered weekly. A second fecal sample was obtained at the end of the intervention to evaluate changes in fecal calprotectin values. Because of the high prevalence of lactose intolerance in Chile, a lactose intolerance test was made for Chilean subjects, to eliminate lactose intolerance as a cause of some of the abdominal complaints.
At the end of the intervention period and 14-week follow-up, the subject was asked to remain in the study for an additional 2 weeks, without intervention, to evaluate the potential changes in the GSRS-IBS, Bristol scale, quality-of-life, and depression and anxiety scores.
Throughout the intervention phase and for the additional 2-week surveillance phase, the feeding pattern, adherence to treatment, use of other concomitant medications, and frequency and severity of adverse events were evaluated. The subjects reported in the diary potential adverse events, and the principal investigators classified them as related or unrelated to the intervention. The diary report form (DRF) reported the type and amount of food consumed, the use of any medication during their participation in the study, and any adverse events. The journal included written instructions for filling out the forms. The information reported by subjects on the DRF was transcribed manually by investigators on a case report form (CRF) for further analysis. To ensure compliance with respect to the completion of the journal and follow-up visits, the study staff made periodic telephone calls to the study subjects to remind them of upcoming visits and to ensure that they fully understood the necessary instructions for correctly filling out the journal. All the collected information is presented using descriptive statistics, including the number of observations, missing observations, minimum value, median, maximum value, mean, and standard deviation. The p-values and the calculation of the 95% confidence intervals for the GSRS-IBS were performed as two-tailed tests. The changes in the GSRS-IBS and Bristol scores were analyzed using a generalized linear model for repeated measures. A one-way analysis of variance (ANOVA) was used to compare depression and anxiety scores and fecal calprotectin levels between groups. The changes in quality-of-life scores across time were analyzed using generalized linear models. For each hypothesis test, a p-value < 0.05 was considered significant. SPSS version 25 for Mac (IBM Corporation, Armonk, NY, USA) was used for all statistical analyses.
Results
A total of 210 potential subjects were screened to participate in the study. A total of 140 patients were selected to be randomized to either the L. reuteri group (n = 70) or the placebo group (n = 70). In total, 20 subjects were recruited in Chile (10 in the L. reuteri group and 10 in the placebo group) and 120 in México (60 in the L. reuteri group and 60 in the placebo group). The causes of screening failure are included in the Consolidated Standards of Reporting Trials (CONSORT) flowchart. At the second visit, five Chilean patients withdrew because they were not willing to fill out the questionnaires or come to the control sessions due to a lack of time. (Figure 1: CONSORT flowchart for the study.).
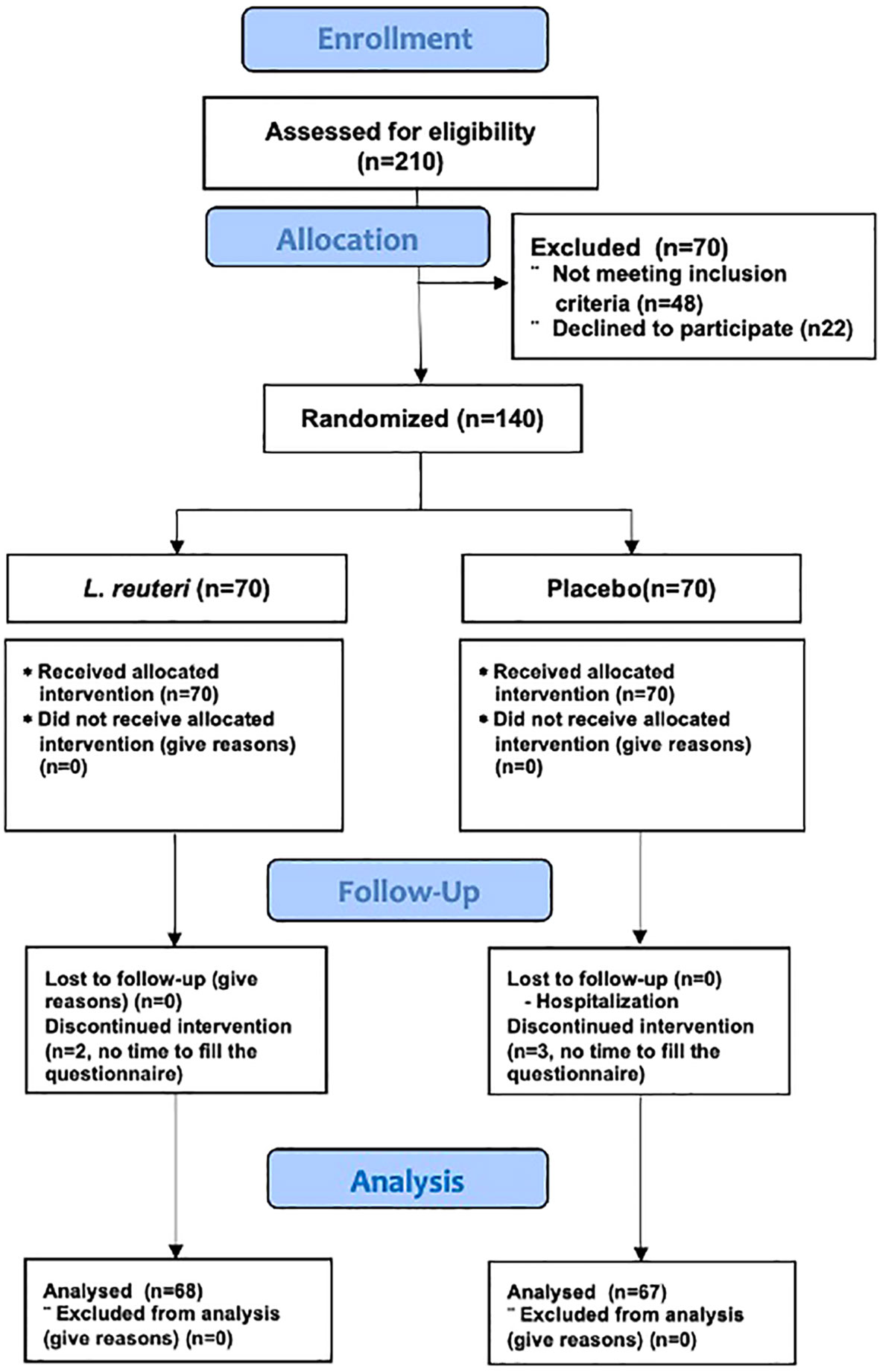
Figure 1 CONSORT Flow Diagram.
Because the analysis by subgroups (Chilean cohort vs. Mexican cohort) did not show any significant differences (see Supplementary Material), we present the main results as a global cohort, comparing 68 subjects allocated to the L. reuteri group and 67 to the control group.
The age of the subjects was 39.4 years ± 9.98 years in the L. reuteri group and 40.2 years ± 11.1 years in the placebo group (p = NS). Most of the recruited subjects were female (82% in the L. reuteri group and 78% in the placebo group; p = NS). Ingestion of FODMAPs before recruitment was reported as low, at 85% and 80% in the L. reuteri and placebo groups, respectively (p = NS). Except for greater smoking, a greater frequency of physical activity, and higher levels of calprotectin in the L. reuteri group at admission, no significant differences were found (Table 1).
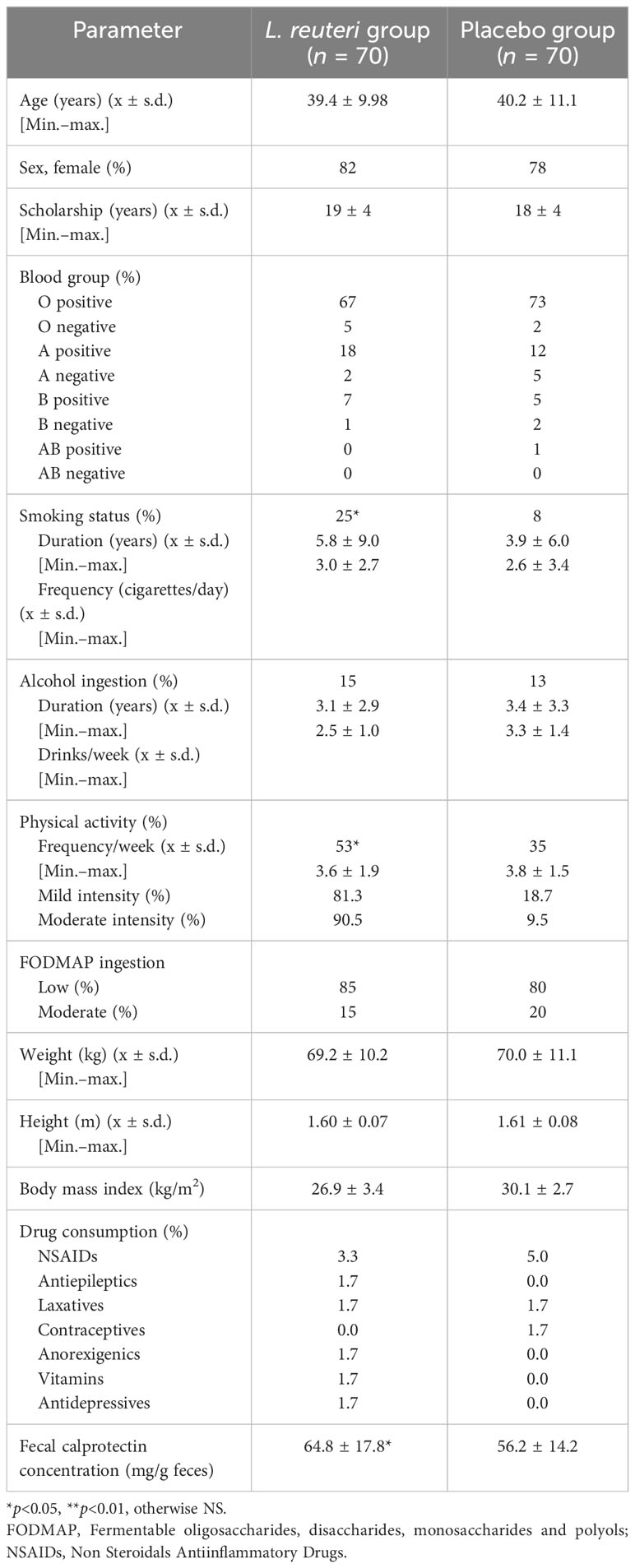
Table 1 Base information at recruitment.
During the pre-randomization phase, no differences were observed in the GSRS-IBS (47.8 ± 8.4 in the L. reuteri group and 48.3 ± 9.8 in the placebo group; p = 0.74), Bristol scale (3.5 ± 1.17 in the L. reuteri group and 3.7 ± 0.97 in the placebo group; p = 0.24), quality-of-life (100 ± 18.7 in the L. reuteri group and 99 ± 17.8 in the placebo group), anxiety (5.9 ± 2.81 in the L. reuteri group and 6.6 ± 2.34 in the placebo group), or depression scores (2.8 ± 1.83 in the L. reuteri group and 2.9 ± 2.13 in the placebo group) (see appendix for Supplementary Material Tables S1, 2). During the intervention phase, the adjusted model showed a clear improvement in the severity of IBS-related symptoms observed in the L. reuteri group, starting from week 6 (18.86 ± 5.47 vs. 20.93 ± 5.55, 95% CI −3.91 to −0.23; p < 0.05) and maintained to the end of the 14-week intervention (7.94 ± 6.96 vs. 11.71 ± 6.54, 95% CI −6.03 to −1.51; p < 0.001) (Figure 2A, Supplementary Table S3). To handle the risk of mass significance for multiple measurements, we measured the area under the curve (AUC) for the GSRS-IBS score, as calculated by the means of the trapezoid formula and by three time periods, and showed that there was a statistically significant difference between the groups from the screening of participants, which was more pronounced from week 6 of the intervention onward (Figure 2B, Supplementary Table S4).
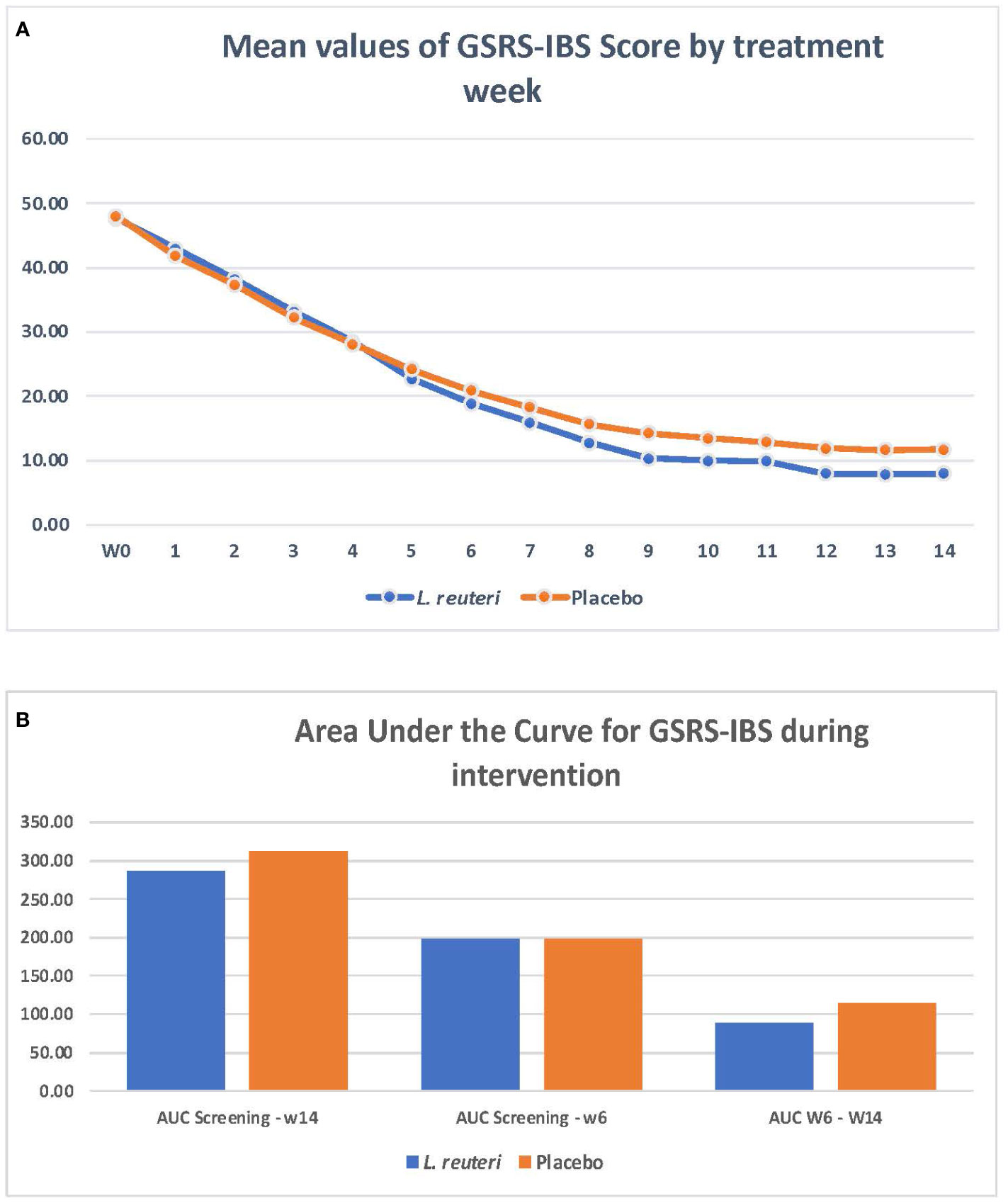
Figure 2 Limosilactobacillus reuteri DSM 17938 + ATCC PTA 6475 and improvement on irritable bowel syndrome symptoms.
The main improvement of IBS symptoms was related to abdominal pain, pain relieved by a bowel action, bloating, passing gas, and visible distension, which was reduced and was significantly better in the L. reuteri group than in the placebo group (Table 2) Stool consistency, as evaluated by the Bristol scale, did not show significant differences between groups. (Figure 3) As an exploratory analysis, we divided the samples by the type of IBS, identifying 23 constipated types, 33 predominantly diarrheic types, and 84 mixed types. Except for a significant improvement on the Bristol scale for diarrheic types in the first 8 weeks in favor of L. reuteri, we did not observe significant differences that could have been produced by the small sample size of the subgroups (Supplementary Figures 4, 5).

Table 2 Evolution of IBS symptoms during the intervention (as based on GSRS-IBS score).
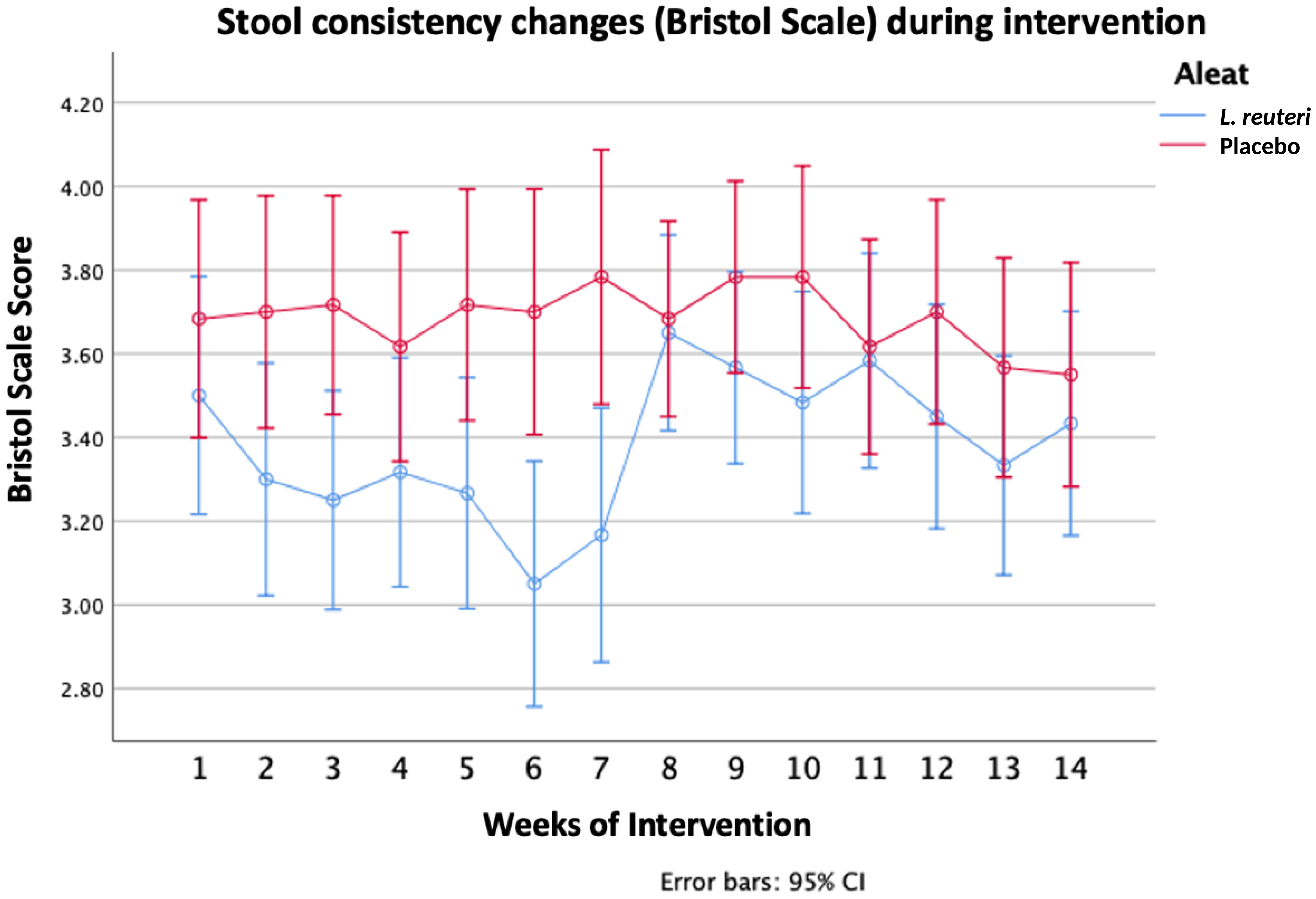
Figure 3 Stool consistency changes (Bristol Scale) during intervention.
A significant improvement was observed at the end of the 14 weeks of treatment in the L. reuteri group regarding the quality-of-life score and anxiety levels, with a trend toward improving anxiety (Table 3).
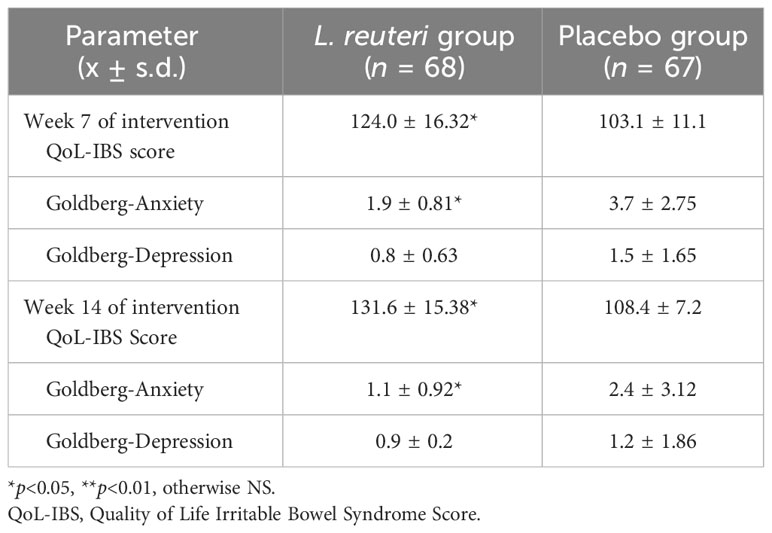
Table 3 Quality of life, anxiety, and depression scores in the treatment phase (14 weeks).
Fecal calprotectin values in the L. reuteri group were significantly lower at the end of 14 weeks of treatment than in those in the placebo group (30.2 mg/g ± 11.8 mg/g of stool vs. 41.6 mg/g ± 10.7 mg/g of stool; p = 0.019). Regarding the safety of the interventions, no significant differences were observed in the frequency of adverse events reported in the first 30 min after ingesting products under research during the intervention period (Table 4). Data related to lactose intolerance did not modify the effect of the intervention, so we do not present it here.
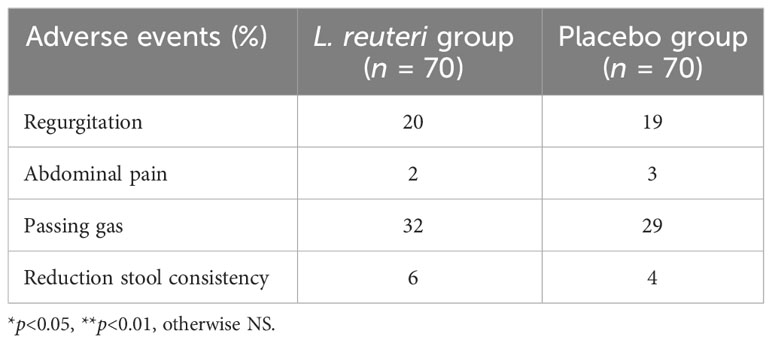
Table 4 Frequency of adverse events during the treatment phase (14 weeks).
At the end of the intervention period, the subjects were under surveillance for 2 additional weeks to evaluate the evolution of IBS symptoms and changes on the Bristol, quality-of-life, anxiety, and depression scale scores. The changes observed during the intervention phase were maintained during this post-treatment period (Table 5).
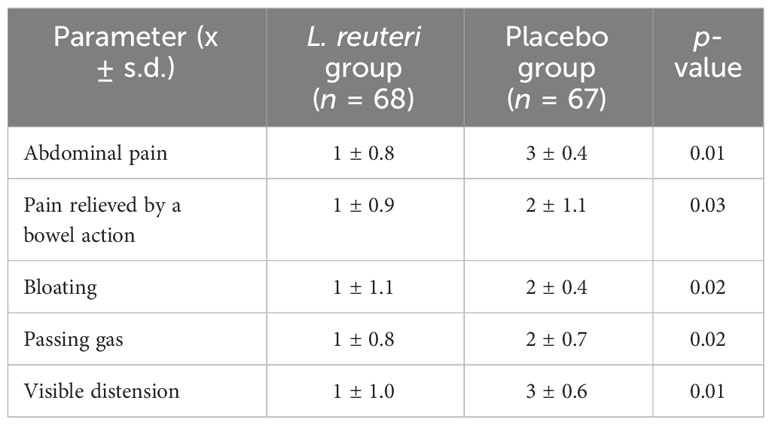
Table 5 GSRS-IBS evaluation (post-treatment observational phase).
Discussion and conclusions
IBS represents one of the most common brain–gut–microbiome interaction disorders, with significant symptoms and a significant deterioration in quality of life; it is therefore associated with a significant economic impact due to frequent episodes of symptomatology and, thus, increased work absenteeism. Although its exact causes are unknown, altered visceral hypersensitivity (38, 39), chronic immune activation with the development of low-grade inflammation (40–43), and changes in the alpha and beta diversity of the intestinal microbiome have been described (44–47).
In this sense, probiotics have shown different impacts through modulating hypersensitivity, reducing low-grade inflammation, and modifying alpha or beta diversity in the intestinal microbiome (48–57). The different strains of Lactobacillus have been shown to reduce pro-inflammatory tumor necrosis factor alpha (TNF-α) production in peripheral blood mononuclear cells in healthy subjects. A combination of Lactobacillus strains has been shown to reduce pro-inflammatory cytokines in the digestive tract of subjects with neuroinflammation (48–50).
Some Bifidobacteria have been reported to enhance the immune responsivity of mucosal surfaces and have shown promising benefits for healthy adults (51). Other strains of Bifidobacterium also decrease lipopolysaccharide (LPS) concentrations, which may reduce inflammatory cytokine production (52) and reduce cytokine- and T-cell-mediated inflammation (53). These effects are likely to improve the intestinal barrier and immune function and may also have a role in alleviating functional gastrointestinal disorders such as IBS (54).
Lactobacillus strains modulate visceral hypersensation and alleviate visceral pain in some animal models, increasing enterocyte opioid and cannabinoid receptor expression and reducing the activity of sodium channels (55, 56). Studies on healthy mice with modified microbiota secondary to the use of antibiotics showed inhibition of VH associated with inflammation after administration of Lactobacillus, a clear anti-inflammatory response, and inhibition of afferent pain pathways (57).
Concerning strain specificity and dose-specific effects of probiotics on IBS, although in 2018, a certain differential effect was demonstrated in terms of the potency of Lactobacillus species and Bifidobacteria with respect to improving IBS symptoms (58), the reality is that, to date, it has not been possible to demonstrate the significant effect of a particular strain at a specific dose and with a determined frequency. For example, in 2018, an analysis of the efficacy of VSL3 in subjects with IBS did not find sufficient evidence to demonstrate significant efficacy regarding controlling symptoms in subjects with IBS (59).
Protecting intestinal epithelial integrity in IBS patients is crucial to avoid mucosal damage and increased permeability. We combined two L. reuteri probiotic strains with specific and complementary effects at the intestinal mucosa, previously established in vitro and in vivo. L. reuteri ATCC PTA 6475 has been shown to bind to intestinal mucus in vitro as well as to normalize tight junction protein expression in IPEC-2 monolayers infected by enterotoxigenic Escherichia coli (ETEC) (60). L. reuteri DSM 17938 is a well-established probiotic strain that has been shown to stimulate enterocyte migration and microbial diversity in the neonatal mouse intestine (29). Moreover, L. reuteri ATCC PTA 6475 and L. reuteri DSM 17938 have been shown to significantly reduce ETEC-induced IL-6 and TNF-α secretion in IPEC-2 cells, providing evidence for a potential mucosal anti-inflammatory effect in animals and humans (60). The scientific rationale for combining these two strains was to identify the potential synergistic effects of the combination.
In this study, we demonstrated that the use of L. reuteri DSM 17938 and L. reuteri ATCC PTA 6475 significantly reduces the clinical symptoms associated with IBS when evaluated using the GSRS-IBS score. Subjects treated with the combination of probiotics showed an 80% vs. 43% reduction in the frequency and severity of symptoms starting from week 6 of the intervention. Even when we calculated the 95% CIs for the differences between the L. reuteri and the placebo interventions, we identified these significant differences, which supports the significance of the effect. Improvements in symptoms were predominantly observed in abdominal pain, pain relieved by a bowel action, bloating and visible distension (which started to improve on week 5 of treatment), and passing gas improvement (starting on week 10). This effect is aligned with previous evidence for L. reuteri in subjects with Helicobacter pylori infections or functional abdominal pain, in which abdominal pain and bloating reduction were significantly reduced (61–65). This is consistent with the evidence previously cited in animal models in which these two strains modulated low-grade inflammation, increased tight junction proteins, and reduced visceral hypersensitivity. One interesting result regarding the efficacy observed in the cohort of subjects treated with probiotics is that this effect remained during the 2-week observation period after the treatment was stopped. The impact of intervention on the immune and anti-inflammatory effects of the use of L. reuteri had been previously observed by our group in children treated with L. reuteri DSM 17938, in which the effects persisted 12 weeks after intervention (66).
The quality-of-life and anxiety scores also significantly improved in subjects treated with L. reuteri. A significant reduction in the frequency and severity of IBS-related symptoms, mainly abdominal pain, bloating, and distension, seems to be the more logical explanation for the improvement of these two parameters. Recently, a systematic review with meta-analysis has shown that probiotics significantly reduce anxiety in adults, as evaluated by the State–Trait Anxiety Inventory (STAI) (MD, −6.88, 95% CI −12.35 to −1.41; p = 0.01; I2 = 24%) (67). A growing body of evidence suggests that probiotics can modulate gut–brain interactions by regulating neurotransmitters and proteins critical for the neural excitatory–inhibitory balance, mood, cognitive functions, and memory processes (68–70). Although the pathways involved are not completely understood, they might be associated with the brain tissue’s susceptibility to changes in the inflammatory process and oxidative stress status (71, 72).
Finally, in terms of safety, potential adverse events evaluated in the first 30 min after subjects received the intervention did not show significant differences between the probiotics group and the placebo group, which is aligned with previous evidence that shows the safety and tolerability of these two strains of L. reuteri in toddlers, children, and adults.
The main strengths of our study are, first, the size of the sample; second, the strategy used to establish an objective monitoring period and apply validated scales over a period of 2 weeks to ensure compliance with the Rome IV criteria; third, double-blinding with an extended follow-up period of 14 weeks to identify the onset of effects and evaluate the continuity of effects across time; and, finally, the establishment of a follow-up period of 2 weeks, without intervention, to evaluate residual anti-inflammatory effects.
Among the main limitations is the inability to perform, given the sample size, a stratified analysis based on the type of IBS to evaluate a differential impact (perhaps with a greater effect among individuals with predominant constipation). The second major limitation is the lack of an analysis of the patients’ baseline and final microbiota profile to establish a correlation between the clinical changes observed and potential changes in the alpha and beta diversity of the populations of fecal microbiota.
The evidence identified in the present study, the first of its kind to demonstrate the efficacy of this combination of L. reuteri strains, indicates that the strains are safe and effective adjuvants for the management of gastrointestinal symptoms in adults with IBS and improve the quality of life and associated symptoms of anxiety in these patients.
This line of research should be continued to provide additional support to the results obtained herein. If possible, the interventions should be randomized within each IBS subtype, and changes in the microbiota profile and their association with pro-/anti-inflammatory biomarkers should be evaluated in at least one subsample of subjects in each stratum.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comite de Investigación y Comite de Ética de la Investigación. Hospital General Dr Manuel Gea González. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SC: Supervision, Writing – review & editing, Project administration. SH: Methodology, Validation, Writing – review & editing, Project administration. DV-L: Writing – review & editing, Investigation. JP: Investigation, Writing – review & editing. MM-P: Supervision, Writing – review & editing. AA-A: Writing – review & editing, Investigation. JA-F: Investigation, Writing – review & editing. CJ-G: Formal Analysis, Methodology, Writing – review & editing. MR: Conceptualization, Investigation, Writing – review & editing. GL-V: Formal Analysis, Investigation, Writing – review & editing. PG-C: Conceptualization, Methodology, Project administration, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Biogaia Sweden partially funded the activities conducted during this trial, support investigators with active product and placebo and cost of publication.
Acknowledgments
We would like to thank Mikael Åström, M.Sc., Ph.L., for his help and contribution to the statistical analysis of the data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and the final decision to publish.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fgstr.2023.1296048/full#supplementary-material
References
1. Talley NJ, Zinsmeister AR, Van Dyke C, Melton MJ III. Epidemiology of colonic symptoms and the irritable bowel syndrome. Gastroenterology (1991) 101:927–34. doi: 10.1016/0016-5085(91)90717-Y
2. Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci (1993) 38:1569–80. doi: 10.1007/BF01303162
3. Hungin AP, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: An international survey of 40,000 subjects. Aliment Pharmacol Ther (2003) 17:643–50. doi: 10.1046/j.1365-2036.2003.01456.x
4. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin Gastroenterol Hepatol (2012) 10:712–721 e4. doi: 10.1016/j.cgh.2012.02.029
5. Chey WD, Kurlander J, Eswaran S. Irritable bowel syndrome: A clinical review. JAMA (2015) 313:949–58. doi: 10.1001/jama.2015.0954
6. Everhart JE, Ruhl CE. Burden of digestive diseases in the United States part I: Overall and upper gastrointestinal diseases. Gastroenterology (2009) 136:376–86. doi: 10.1053/j.gastro.2008.12.015
7. Agarwal N, Spiegel BM. The effect of irritable bowel syndrome on health-related quality of life and health care expenditures. Gastroenterol Clin North Am (2011) 40:11–9. doi: 10.1016/j.gtc.2010.12.013
8. Gibson PR, Varney J, Malakar S, Muir JG. Food components and irritable bowel syndrome. Gastroenterology (2015) 148:1158–1174 e4. doi: 10.1053/j.gastro.2015.02.005
9. Saha L. Irritable bowel syndrome: Pathogenesis, diagnosis, treatment, and evidence-based medicine. World J Gastroenterol (2014) 20:6759–73. doi: 10.3748/wjg.v20.i22.6759
10. Desipio J, Friedenberg FK, Korimilli A, Richter JE, Parkman HP, Fisher RS. High-resolution solid-state manometry of the antropyloroduodenal region. Neurogastroenterol Motil (2007) 19:188–95. doi: 10.1111/j.1365-2982.2006.00866.x
11. Friedenberg FK. Tonic and phasic pyloric activity in response to CCK-octapeptide. Dig Dis Sci (2008) 53:905–11. doi: 10.1007/s10620-008-0214-1
12. Malik A, Lukaszewski K, Caroline D, Parkman H. A retrospective review of enteroclysis in patients with obscure gastrointestinal bleeding and chronic abdominal pain of undetermined etiology. Dig Dis Sci (2005) 50:649–55. doi: 10.1007/s10620-005-2551-7
13. Latulippe ME, Skoog SM. Fructose malabsorption and intolerance: Effects of fructose with and without simultaneous glucose ingestion. Crit Rev Food Sci Nutr (2011) 51:583–92. doi: 10.1080/10408398.2011.566646
14. Lacy BE. The science, evidence, and practice of dietary interventions in irritable bowel syndrome. Clin Gastroenterol Hepatol (2015) 13:1899–906. doi: 10.1016/j.cgh.2015.02.043
15. Fedewa A, Rao SS. Dietary fructose intolerance, fructan intolerance and FODMAPs. Curr Gastroenterol Rep (2014) 16:370. doi: 10.1007/s11894-013-0370-0
16. Barrett JS, Gearry RB, Muir JG, Irving PM, Rose R, Rosella O, et al. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther (2010) 31:874–82. doi: 10.1111/j.1365-2036.2010.04237.x
17. Kim Y, Park SC, Wolf BW, Hertzler SR. Combination of erythritol and fructose increases gastrointestinal symptoms in healthy adults. Nutr Res (2011) 31:836–41. doi: 10.1016/j.nutres.2011.09.025
18. Komericki P, Akkilic-Materna M, Strimitzer T, Weyermair K, Hammer HF, Aberer W. Oral xylose isomerase decreases breath hydrogen excretion and improves gastrointestinal symptoms in fructose malabsorption—A double-blind, placebo-controlled study. Aliment Pharmacol Ther (2012) 36:980–7. doi: 10.1111/apt.12057
20. Marcason W. What is the FODMAP diet? J Acad Nutr Diet (2012) 112:1696. doi: 10.1016/j.jand.2012.08.005
21. Klein AV, Kiat H. The mechanisms underlying fructose-induced hypertension: A review. J Hypertens (2015) 33:912–20. doi: 10.1097/HJH.0000000000000551
22. El-Salhy M, Gundersen D. Diet in irritable bowel syndrome. Nutr J (2015) 14:36. doi: 10.1186/s12937-015-0022-3
23. Atkinson W, Sheldon TA, Shaath N, Whorwell PJ. Food elimination based on IgG antibodies in irritable bowel syndrome: A randomised controlled trial. Gut (2004) 53:1459–64. doi: 10.1136/gut.2003.037697
24. Austin GL, Dalton CB, Hu Y, Morris CB, Hankins J, Weinland SR, et al. A very low-carbohydrate diet improves symptoms and quality of life in diarrhea-predominant irritable bowel syndrome. Clin Gastroenterol Hepatol (2009) 7:706–708 e1. doi: 10.1016/j.cgh.2009.02.023
25. Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol (2015) 21(10):3072–84. doi: 10.3748/wjg.v21.i10.3072
26. Niu H-L, Xiao J-Y. The efficacy and safety of probiotics in patients with irritable bowel syndrome: Evidence based on 35 randomized controlled trials. Int J Surg (2020) 75:116–27. doi: 10.1016/j.ijsu.2020.01.142
27. Jensen H, Grimmer S, Naterstad K, Axelsson L. In vitro testing of commercial and potential probiotic lactic acid bacteria. Int J Food Microbiol (2012) 153(1-2):216–22. doi: 10.1016/j.ijfoodmicro.2011.11.020
28. Walsham AD, MacKenzie DA, Cook V, Wemyss-Holden S, Hews CL, Juge N, et al. Lactobacillus reuteri Inhibition of Enteropathogenic Escherichia coli Adherence to Human Intestinal Epithelium. Front Microbiol (2016) 7:244. doi: 10.3389/fmicb.2016.00244
29. Preidis GA, Saulnier DM, Blutt SE, Mistretta T-A, Riehle KP, Major AM, et al. Probiotics stimulate enterocyte migration and microbial diversity in the neonatal mouse intestine. FASEB J (2012) 26:1960–9. doi: 10.1096/fj.10-177980
30. Shi Z, Fultz RS, Engevik MA, Gao C, Hall A, Major A, et al. Distinct roles of histamine H1- and H2-receptor signaling pathways in inflammation-associated colonic tumorigenesis. Am J Physiol Gastrointest Liver Physiol (2019) 316:G205–16. doi: 10.1152/ajpgi.00212.2018
31. Jones SE, Versalovic J. Probiotic Lactobacillus reuteri biofilms produce antimicrobial and anti-inflammatory factors. BMC Microbiol (2009) 9:35. doi: 10.1186/1471-2180-9-35
32. Buffington SA, Di Prisco GV, Auchtung TA, Ajami NJ, Petrosino JF, Costa-Mattioli M. Microbial reconstitution reverses maternal diet-induced social and synaptic deficits in offspring. Cell (2016) 165:1762–75. doi: 10.1016/j.cell.2016.06.001
33. Perez-Burgos A, Wang L, McVey Neufeld KA, Mao YK, Ahmadzai M, Janssen LJ, et al. The TRPV1 channel in rodents is a major target for antinociceptive effect of the probiotic Lactobacillus reuteri DSM 17938. J Physiol (2015) 593(17):3943–57. doi: 10.1113/JP270229
34. Zhang Y, Li L, Guo C, Mu D, Feng B, Zuo X, et al. Effects of probiotic type, dose and treatment duration on irritable bowel syndrome diagnosed by Rome III criteria: a meta-analysis. BMC Gastroenterol (2016) 16:62. doi: 10.1186/s12876-016-0470
35. Wiklund IK, Fullerton S, Hawkey CJ, Jones RH, Longstreth GF, Mayer EA, et al. An irritable bowel syndrome-specific symptom questionnaire: development and validation. Scand J Gastroenterol (2003) 38:947–54. doi: 10.1080/00365520310004209
36. Andrae DA, Patrick DL, Drossman DA. Covington PS Evaluation of the Irritable Bowel Syndrome Quality of Life (IBS-QOL) questionnaire in diarrheal-predominant irritable bowel syndrome patients. Health Qual Life Outcomes (2013) 11:208. doi: 10.1186/1477-7525-11-208
37. Campillo-Serrano C, Caraveo Anduaga J, Medina-Mora ME, Martinez-Lanz P. Inter-clinician reliability of the Mexican version of Goldberg's "Standardized Psychiatric Interview". Acta Psiquiatr Psicol Am Lat (1981) 27:44–53.
38. Mertz H, Morgan V, Tanner G, Pickens D, Price R, Shyr Y, et al. Regional cerebral activation in irritable bowel syndrome and control subjects with painful and nonpainful rectal distention. Gastroenterology (2000) 118(5):842–8. doi: 10.1016/S0016-5085(00)70170-3
39. Sloots CE, Felt-Bersma RJ. Rectal sensorimotor characteristics in female patients with idiopathic constipation with or without paradoxical sphincter contraction. Neuro Gastroenterol Motil (2003) 15(2):187–93. doi: 10.1046/j.1365-2982.2003.00392.x
40. Ford AC, Talley NJ. Mucosal inflammation as a potential etiological factor in irritable bowel syndrome: a systematic review. J Gastroenterol (2011) 46(4):421–31. doi: 10.1007/s00535-011-0379-9
41. Macsharry J, O'Mahony L, Fanning A, Bairead E, Sherlock G, Tiesman J, et al. Mucosal cytokine imbalance in irritable bowel syndrome. Scand J Gastroenterol (2008) 43(12):1467–76. doi: 10.1080/00365520802276127
42. Piche T, Saint-Paul MC, Dainese R, Marine-Barjoan E, Iannelli A, Montoya ML, et al. Mast cells and cellularity of the colonic mucosa correlated with fatigue and depression in irritable bowel syndrome. Gut (2008) 57(4):468–73. doi: 10.1136/gut.2007.127068
43. Törnblom H, Lindberg G, Nyberg B, Veress B. Full-thickness biopsy of the jejunum reveals inflammation and enteric neuropathy in irritable bowel syndrome. Gastroenterology (2002) 123(6):1972–9. doi: 10.1053/gast.2002.37059
44. Attaluri A, Jackson M, Valestin J, Rao SS. Methanogenic flora is associated with altered colonic transit but not stool characteristics in constipation without IBS. Am J Gastroenterol (2010) 105(6):1407–11. doi: 10.1038/ajg.2009.655
45. Kassinen A, Krogius-Kurikka L, Mäkivuokko H, Rinttilä T, Paulin L, Corander J, et al. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology (2007) 133(1):24–33. doi: 10.1053/j.gastro.2007.04.005
46. Pittayanon R, Lau JT, Yuan Y, Leontiadis GI, Tse F, Surette M, et al. Gut microbiota in patients with irritable bowel syndrome-a systematic review. Gastroenterology (2019) 157:97–108. doi: 10.1053/j.gastro.2019.03.049
47. Lo Presti A, Zorzi F, Del Chierico F, Altomare A, Cocca S, Avola A, et al. Fecal and mucosal microbiota profiling in irritable bowel syndrome and inflammatory bowel disease. Front Microbiol (2019) 10(1655):1–14. doi: 10.3389/fmicb.2019.01655
48. Kekkonen RA, Lummela N, Karjalainen H, Latvala S, Tynkkynen S, Jrvenp S, et al. Probiotic intervention has strain-specific anti-inflammatory effects in healthy adults. World J Gastroenterol (2008) 14:2029–36. doi: 10.1017/s0022029903006034
49. Schultz M, Linde HJ, Lehn N, Zimmermann K, Grossmann J, Falk W, et al. Immunomodulatory consequences of oral administration of Lactobacillus rhamnosus strain GG in healthy volunteers. J Dairy Res (2003) 70:165–73. doi: 10.3748/wjg.14.2029
50. Lavasani S, Dzhambazov B, Nouri M, Fak F, Buske S, Molin G, et al. A novel probiotic mixture exerts a therapeutic efect on experimental autoimmune encephalomyelitis mediated by IL-10 producing regulatory T cells. PloS One (2010) 5:e9009. doi: 10.1371/journal.pone.0009009
51. West NP, Horn PL, Pyne DB, Gebski VJ, Lahtinen SJ, Fricker PA, et al. Probiotic supplementation for respiratory and gastrointestinal illness symptoms in healthy physically active individuals. Clin Nutr (2014) 33:581–7. doi: 10.1016/j.clnu.2013.10.002
52. Rodes L, Khan A, Paul A, Coussa-Charley M, Marinescu D, Tomaro-Duchesneau C, et al. Effect of probiotics Lactobacillus and Bifidobacterium on gut-derived lipopolysaccharides and inflammatory cytokines: An in vitro study using a human colonic microbiota model. J Microbiol Biotechnol (2013) 23:518–26. doi: 10.4014/jmb.1205.05018
53. O’Mahony C, Scully P, O’Mahony D, Murphy S, O’Brien F, Lyons A, et al. Commensal-induced regulatory T cells mediate protection against pathogen-stimulated NF-kappaB activation. PloS Pathog (2008) 4:e1000112. doi: 10.1371/journal.ppat.1000112
54. Rajilic-Stojanovic M, Biagi E, Heilig HG, Kajander K, Kekkonen RA, Tims S, et al. Global and deep molecular analysis of microbiota signatures in fecal samples from patients with irritable bowel syndrome. Gastroenterology (2011) 141:1792–801. doi: 10.1053/j.gastro.2011.07.043
55. Verd EF, Berck P, Bergonzelli GE, Huang X-X, Blennerhasset P, Rochat F, et al. Lactobacillus paracasei normalizes muscle hypercontractility in a murine model of postinfective gut dysfunction. Gastroenterology (2004) 127:826–37. doi: 10.1053/j.gastro.2004.06.007
56. Wang B, Mao Y, Diorio C, Wang L, Huizinga JD, Bienenstock J, et al. Lactobacillus reuteriingestion and IKCachannel blockade have similar effects on rat colon motility and myenteric neurones. Neurogastroenterol Motil (2009) 22:98–e33.
57. Verdu EF, Bercik P, Verma-Gandhu M, Huang X-X, Blennerhassett P, Jackson W, et al. Specific probiotic therapy attenuates antibiotic induced visceral hypersensitivity in mice. Gut (2006) 55:182–90. doi: 10.1136/gut.2005.066100
58. Ford AC, Harris LA, Lacy BE, Quigley EMM, Moayyedi P. Systematic review with meta-analysis: the efficacy of prebiotics, probiotics, synbiotics and antibiotics in irritable bowel syndrome. Aliment Pharmacol Ther (2018) 48(10):1044–60. doi: 10.1111/apt.15001
59. Connell M, Shin A, James-Stevenson T, Xu H, Imperiale TF, Herron J. Systematic review and meta-analysis: Efficacy of patented probiotic, VSL#3, in irritable bowel syndrome. Neurogastroenterol Motil (2018) 30(12):e13427. doi: 10.1111/nmo.13427
60. Karimi S, Jonsson H, Lundh T, Roos S. Lactobacillus reuteri strains protect epithelial barrier integrity of IPEC-J2 monolayers from the detrimental effect of enterotoxigenic Escherichia coli. Physiol Rep (2018) 6(2):e13514. doi: 10.14814/phy2.13514
61. Francavilla R, Polimeno L, DemiChina A, Maurogiovanni G, Principi B, Scaccianoce G, et al. Lactobacillus reuteri strain combination in Helicobacter pylori infection: a randomized, double-blind, placebo-controlled study. J Clin Gastroenterol (2014) 48:407–13. doi: 10.1097/MCG.0000000000000007
62. Romano C, Ferrau' V, Cavataio F, Iacono G, Spina M, Lionetti E, et al. Lactobacillus reuteri in children with functional abdominal pain (FAP). Paediatr Child Health (2014) 50:E68–71. doi: 10.1111/j.1440-1754.2010.01797.x
63. Weizman Z, Abu-Abed J, Binsztok M. Lactobacillus reuteri DSM 17938 for the management of functional abdominal pain in childhood: A randomized, double-blind, placebo-controlled trial. .J Pediatr (2016) 174:160–4. doi: 10.1016/j.jpeds.2016.04.003
64. Jadrešin O, Hojsak I, Mišak Z, Kekez AJ, Trbojević T, Ivković L, et al. Lactobacillus reuteri DSM 17938 in the treatment of functional abdominal pain in children: RCT study. .J Pediatr Gastroenterol Nutr (2017) 64:925–9. doi: 10.1097/MPG.0000000000001478
65. Jadrešin O, Sila S, Trivić I, Mišak Z, Kolaček S, Hojsak I. Lactobacillus reuteri DSM 17938 is effective in the treatment of functional abdominal pain in children: Results of the double-blind randomized study. .Clin Nutr (2020) 39:3645–51. doi: 10.1016/j.clnu.2020.04.019
66. Gutierrez-Castrellon P, Lopez-Velazquez G, Diaz-Garcia L, Jimenez-Gutierrez C, Mancilla-Ramirez J, Estevez-Jimenez J, et al. Diarrhea in preschool children and Lactobacillus reuteri: a randomized controlled trial. Pediatrics. (2014) 133:e904–9. doi: 10.1542/peds.2013-0652
67. El Dib R, Periyasamy AG, de Barros JL, França CG, Senefonte FL, Vesentini G, et al. Kapoor AProbiotics for the treatment of depression and anxiety: A systematic review and meta-analysis of randomized controlled trials. Clin Nutr ESPEN (2021) 45:75–90. doi: 10.1016/j.clnesp.2021.07.027
68. Allen AP, Hutch W, Borre YE, Kennedy PJ, Temko A, Boylan G, et al. Bifidobacterium longum 1714 as a translational psychobiotic: modulation of stress, electrophysiology and neurocognition in healthy volunteers. Transl Psychiatry (2016) 6:e939–9. doi: 10.1038/tp.2016.191
69. Bercik P, Verdu EF, Foster JA, Macri J, Potter M, Huang X, et al. Chronic gastrointestinal inflammation induces anxiety-like behavior and alters central nervous system biochemistry in mice. Gastroenterology (2010) 139:2102e2112.e1. doi: 10.1053/j.gastro.2010.06.063
70. Cheng L-H, Liu Y-W, Wu C-C, Wang S, Tsai Y-C. Psychobiotics in mental health, neurodegenerative and neurodevelopmental disorders. J Food Drug Anal (2019) 27:632e48. doi: 10.1016/j.jfda.2019.01.002
71. D'Mello C, Swain MG. Immune-to-brain communication pathways in inflammation-associated sickness and depression. Curr topics Behav Neurosci (2017) 31:73–94. doi: 10.1007/7854_2016_37
Keywords: L. reuteri DSM 17938, L. reuteri ATCC PTA 6475, irritable bowel syndrome, adults, randomized controlled (clinical) trial
Citation: Cruchet S, Hirsch S, Villa-López D, Moreno-Portillo M, Palomo JC, Abreu-Abreu AT, Abdo-Francis JM, Jiménez-Gutiérrez C, Rojano M, López-Velázquez G and Gutiérrez-Castrellón P (2024) Limosilactobacillus reuteri DSM 17938 and ATCC PTA 6475 for the treatment of moderate to severe irritable bowel syndrome in adults: a randomized controlled trial. Front. Gastroenterol. 2:1296048. doi: 10.3389/fgstr.2023.1296048
Received: 18 September 2023; Accepted: 28 November 2023;
Published: 04 January 2024.
Edited by:
Michele Di Stefano, IRCCS S.Matteo Hospital Foundation, ItalyReviewed by:
Enrico Stefano Corazziari, Humanitas Research Hospital, ItalyFabio Pace, Bolognini Hospital, Italy
Copyright © 2024 Cruchet, Hirsch, Villa-López, Moreno-Portillo, Palomo, Abreu-Abreu, Abdo-Francis, Jiménez-Gutiérrez, Rojano, López-Velázquez and Gutiérrez-Castrellón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro Gutiérrez-Castrellón, aW5wY29jaHJhbmVAZ21haWwuY29t