 Judit Majnik
Judit Majnik Noémi Császár-Nagy
Noémi Császár-Nagy Georgina Böcskei2
Georgina Böcskei2- 1Department of Rheumatology and Clinical Immunology, Semmelweis University, Budapest, Hungary
- 2Hospital of the Hospitaller Order of Saint John of God, Budapest, Hungary
- 3Department of Public Management and Information Technology, Faculty of Science of Public Governance and Administration, National University of Public Service, Budapest, Hungary
- 4Department of Internal Medicine and Oncology, Semmelweis University, Budapest, Hungary
- 5Heart and Vascular Center, Semmelweis University, Budapest, Hungary
- 6Department of Genetics, Cell- and Immunobiology, Semmelweis University, Budapest, Hungary
Although the management of rheumatoid arthritis (RA) has improved remarkably with new pharmacological therapies, there is still a significant part of patients not reaching treatment goals. Difficult-to-treat RA (D2TRA) is a complex entity involving several factors apart from persistent inflammation, thereafter requiring a holistic management approach. As pharmacological treatment options are often limited in D2TRA, the need for non-pharmacological treatments (NPT) is even more pronounced. The mechanism of action of non-pharmacological treatments is not well investigated, NPTs seem to have a complex, holistic effect including the immune, neural and endocrine system, which can have a significant additive benefit together with targeted pharmacotherapies in the treatment of D2TRA. In this review we summarize the current knowledge on different NPT in rheumatoid arthritis, and we propose a NPT plan to follow when managing D2TRA patients.
Introduction
Targeted therapies have revolutionized the treatment of rheumatoid arthritis (RA), and disease remission and prevention of joint destruction has become a realistic goal. Before the widespread use of the new pharmacological therapies, non-pharmacological interventions had a more pronounced role in RA treatment, but in the last decades investigations in this field are less frequent.
The EULAR recommendations and the ACR guideline for the management of RA are focusing on pharmacological therapies based on synthetic and biological DMARDs (1, 2), but several EULAR recommendations include elements regarding different non-pharmacological therapeutic alternatives partly applicable in RA patients (3–6). In 2021 a EULAR Task Force published the definition of difficult-to-treat rheumatoid arthritis (D2TRA) consisting of three main points: (1) failure of at least two biological or targeted synthetic DMARDS; (2) presence of active/progressive disease; and (3) problematic management perceived by the rheumatologist or the patient (7).
In addition to new medications, the problematic management of D2TRA is highlighting the need for additional therapeutic strategies for reaching treatment goals and attaining a better quality of life in RA. In all RA patients but even more pronounced in D2TRA, drug-intolerance or inefficacy, pain, work disability, psychological and social complications raise our increasing attention to non-pharmacological therapies targeting several of these multiple disease aspects (Figure 1). Pharmacological and non-pharmacological therapies have an additional, synergistic effect in the treatment of RA and D2TRA, and non-pharmacological interventions can support the success of pharmacological therapies. The EULAR points to consider for the management of D2TRA (8, 9) include elements concerning non-pharmacological interventions, which have an increasingly recognized role in D2TRA.
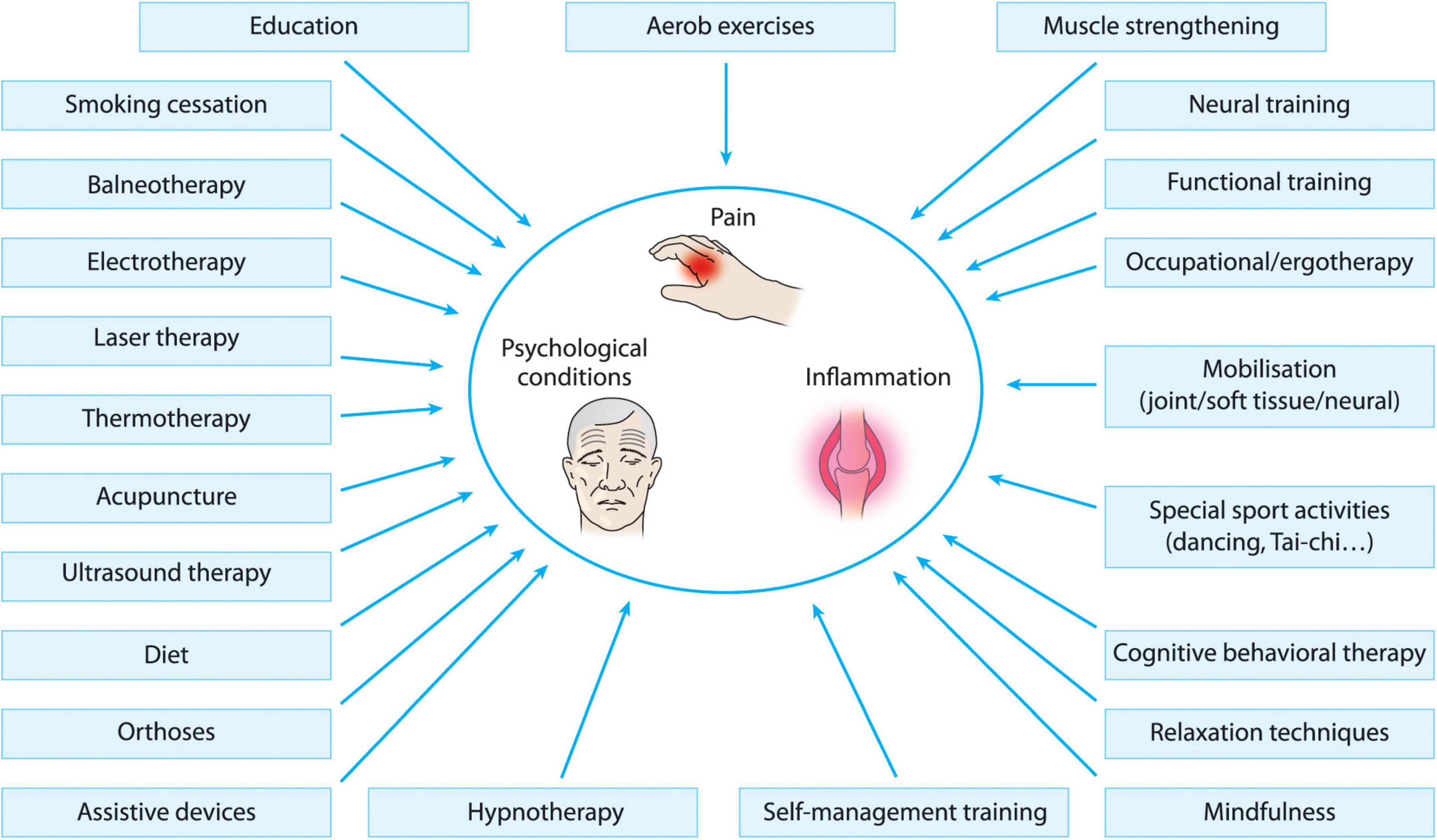
Figure 1. Different non-pharmacological treatment options in D2TRA.
The aim of this review is to summarize the recent knowledge about different non-pharmacological interventions in RA, to appoint those that could be of specific interest in D2TRA, and to suggest a practical structure of non-pharmacological treatment approach in D2TRA. The literature regarding non-pharmacological interventions is wide, however studies focusing on D2TRA, due to the recent establishment of D2TRA criteria are yet lacking. Data obtained in other groups of RA patients with established, active disease, long-lasting symptoms can be applied partly on D2TRA patients, and this review is focusing on these study results. In the literature search, under established RA we meant patients with clinical symptoms duration greater than 2 years (when defined in the study), and excluded studies about early RA or non-differentiated arthritis, under active disease we meant elevated DAS28 score (>3.2) or pain level (>40% on VAS) or elevated number of swollen or tender joints, and under long-lasting symptoms mainly pain, disability or functional limitations and comorbidities e.g., depression. The detailed summary of the reviewed literature is available in Supplementary Tables 1–3.
Exercise therapy
The positive effect of physical activity (PA) in inflammatory rheumatic diseases is well documented (4), and a 2019 review on different non-pharmacological treatment modalities in RA concluded that only exercise/physical activity interventions appeared to be effective in reducing the global impact of disease and quality of life (10). Exercise training programs seem to have the greatest benefit in those RA patients who are older, more inflamed and less fit (11), characteristics applicable to many D2TRA patients, thus emphasizing the role of exercise therapy in this patient group.
Rheumatoid arthritis patients with more active disease are prone to be physically less active and have more sedentary lifestyle (12), which also highlight the importance of maintaining physical activity in D2TRA. For RA patients with high disease activity, high rate of disability and long-standing disease, a person-centered, individualized exercise program can be helpful in improving self-efficacy and physical activity on the long term (13).
Summary of RCTs, Cochrane reviews and meta-analyses is presented in Supplementary Table 1. The aim of exercise interventions in RA are multiple including increase of endurance, agility, increase of muscle strength and mass, decrease of joint/soft tissue pain and swelling, improvement of musculoskeletal function, decrease of cardiovascular risk, improvement of self-efficacy and quality of life. There is much evidence, although mostly of low or moderate quality about the positive effect of dynamic, aerobic exercise programs, muscle strengthening exercises in RA patients on pain, function, fatigue, quality of life (14–18), and some data about positive effect on DAS28 score and inflammatory markers (ESR) (19). The benefits of Yoga or Tai-Chi in RA are uncertain or of low evidence (20–22). Regarding mobilization and neural techniques in RA there are also some trials, mainly showing an effect on pain (23, 24). As high load resistance training is not always feasible in active RA patients, low load or non-resistance training (25) or water-based exercises (26, 27) appear to be good alternatives.
Physical activity is important not only for musculoskeletal symptoms of RA, but also for several comorbidities, which may be more predominant in the D2TRA group. Physically inactive RA patients have significantly worse CVD risk profile (28), and high CVD risk RA patients may get substantial benefits from a physical activity program (29). Upper- and lower extremity strengthening exercise programs improved not only muscle strength but also mental health domain scores (30), and walking-based physical activity showed improvements in sleep duration and sleep quality in RA (31), although the latter studies were conducted in less active RA patients, thus further investigations are needed to clarify this impact in active, D2TRA patients.
It is a central question of all exercise programs how to achieve long-term persistency. This question points toward both educational and psychological techniques, showing the integrity of non-pharmacological treatment modalities. The transition from supervised to independent exercise and the long-term sustainment of physical activity can be supported by personal motivation interventions (32) and internet based techniques (33, 34). Several studies examined different home exercise programs. A SLR on home-based PA interventions in autoimmune rheumatic diseases including RA patients showed improved quality of life and functional capacity, reduced pain and disease activity similar to center-based interventions (35). Adherence and efficacy in home exercise programs can be improved with special strategies including education, self-management and training sessions (17). The importance of home-based programs has become even more emphasized due to the restrictions of COVID pandemic, and physical activity programs are showed to have positive effect on mental state and better vitality in RA (36).
Psychological interventions
In RA, the prevalence of different psychological problems like anxiety and depression is high (37), and even more pronounced in D2TRA (38). Depression was found to be 2–3 times more common in RA patients (39), it is considered as one of the most common comorbidity of RA (40) with common points in cytokine pattern (41), and there seems to be a bidirectional relationship between pain and depression (42).
Several psychological interventions have been studied in the treatment of RA (Supplementary Table 2). The main techniques are (1) education techniques (self-management training, coping skills training, modular behavioral education, patient education), (2) stress management and basic psychotherapies (relaxation techniques, counseling, supportive therapy, mindfulness, self-regulation therapy), (3) specific psychotherapies like cognitive-behavioral therapy (CBT), emotional disclosure (ED), hypnotherapy.
Education and self-management programs are widely used and accepted methods in RA (3, 5, 32, 43, 44), and even internet-based self-management programs have proved to be beneficial (45, 46). Mindfulness-based techniques are easy to perform, do not necessarily need the intervention of a psychotherapist, and are shown to have several beneficial effect on pain-related catastrophizing, fatigue, morning disability (47), pain and even DAS28-CRP score (48). Mindfulness-based group interventions were also shown to be effective on RA self-efficacy, pain, fatigue and overall well-being (49). Cognitive behavioral therapy was examined in RA patients in several study settings, it ameliorated pain, fatigue, function, tender joint count, self-efficacy (44, 50–53), and even internet-based therapy resulted in long persistent improvement of quality of life or tender joint count (46, 54, 55). Emotional disclosure has shown some positive effect in RA, but mostly mixed results have been found, this method seems to be less effective and needs special caution (51, 56).
Physiotherapy and balneotherapy
Among non-pharmacological treatment options in RA several physiotherapy and balneotherapy modalities have been studied. There are some positive results with laser acupuncture (57), underwater ultrasound (US) therapy (58, 59), transelectrical nerve stimulation (TENS) (60), transcutan stimulation of the cervical vagal nerve (61) and neuromuscular electrical stimulation (62–64). Cryotherapy has been studied in several groups of RA patients, both whole body cryostimulation and local cryotherapy had positive effects on clinical and laboratory parameters (65–67), and can be combined with physical activity with good effect on pain and disease activity (68).
Balneotherapy is widely used in musculoskeletal diseases and the effect in RA has been studied with some positive results, although mainly before the widespread use of biological therapies, thereafter the results should be interpreted with caution in D2TRA. Most positive effects were found with radon containing spa (69, 70), and sulphur spa therapy (71). Several studies about dead sea mud therapies have been published with positive results (72–74).
Dietary interventions
Different diets and nutritional supplements have been studied in inflammatory rheumatic diseases including RA. Mediterranean diet, especially when combined with physical exercise showed some effect on quality of life (75–77), although some results were obtained in RA patients with lower disease activity. Vitamin D supplementation is beneficial in patients with RA, with positive effects on disease activity (78) and comorbidities e.g., osteoporosis. Fish oil supplements and herbal therapies like gamma-linolenic acid containing seeds or Tripterygium wilfordii (thunder god vine—caution with potential toxic side effects) showed some beneficial clinical effects (79, 80), and there are some data about the potential benefits of probiotic supplementation in RA (81). Obesity can be a contributing factor in D2TRA, and case series, retrospective and pilot studies point toward the beneficial effect of weight loss on disease activity, physical functioning, eating behaviors and pain in RA (82–84). Nevertheless caution is needed with weight loss interventions, as lower BMI has been showed to be associated with increased mortality in RA (85, 86), which emphasizes the importance of personalized dietary programs.
Other non-pharmacological therapies
Several other non-pharmacological treatment options have been studied in RA patients, but evidence is scarce. Acupuncture showed some benefit on RA activity (87–91), and occupational therapy improved functional and work-related outcomes (92). Although smoking is a known risk factor for RA and for more aggressive disease and smokers are likely to respond less to some but not all TNF antagonists (93, 94), data are scarce about the effect of smoking cessation on disease activity (95). Orthoses and assistive devices are occasionally used by RA patients with some evidence of beneficial effect (96–98), but hand splints can even diminish grip strength (97) thus caution and personalized use is required.
Although out of the scope of this review, several surgical interventions should be mentioned among non-pharmacological therapies in RA (synovectomy with open or arthroscopic surgery or radiosynovectomy with intraarticular isotope injections, reconstructive surgery of ligaments, tendons, joint replacement/endoprosthesis intervention), all of them might be beneficial in D2TRA patients with joint destructions and disabilities. Another important issue is the access of social aid for D2TRA patients, and health care professionals have a role in helping with access to patient organizations, disability benefits, community support.
Proposed non-pharmacological treatment strategy in D2TRA
Based on the evidence found in the literature, we elaborated a NPT approach for D2TRA patients. We suggest that every D2TRA patient should receive an individualized non-pharmacological therapy (NPT) program (Figure 2). The two basic elements are a regular psychologic/educational help and a regular help in sustained physical training including aerobic and strengthening exercises. For this purpose, in parallel with the rheumatologist’s examination, every D2TRA patient should undergo a detailed examination by a psychologist and a physiotherapist, and reassessment should take place every 3/6 months until the patient meets the criteria of remission or low disease activity.
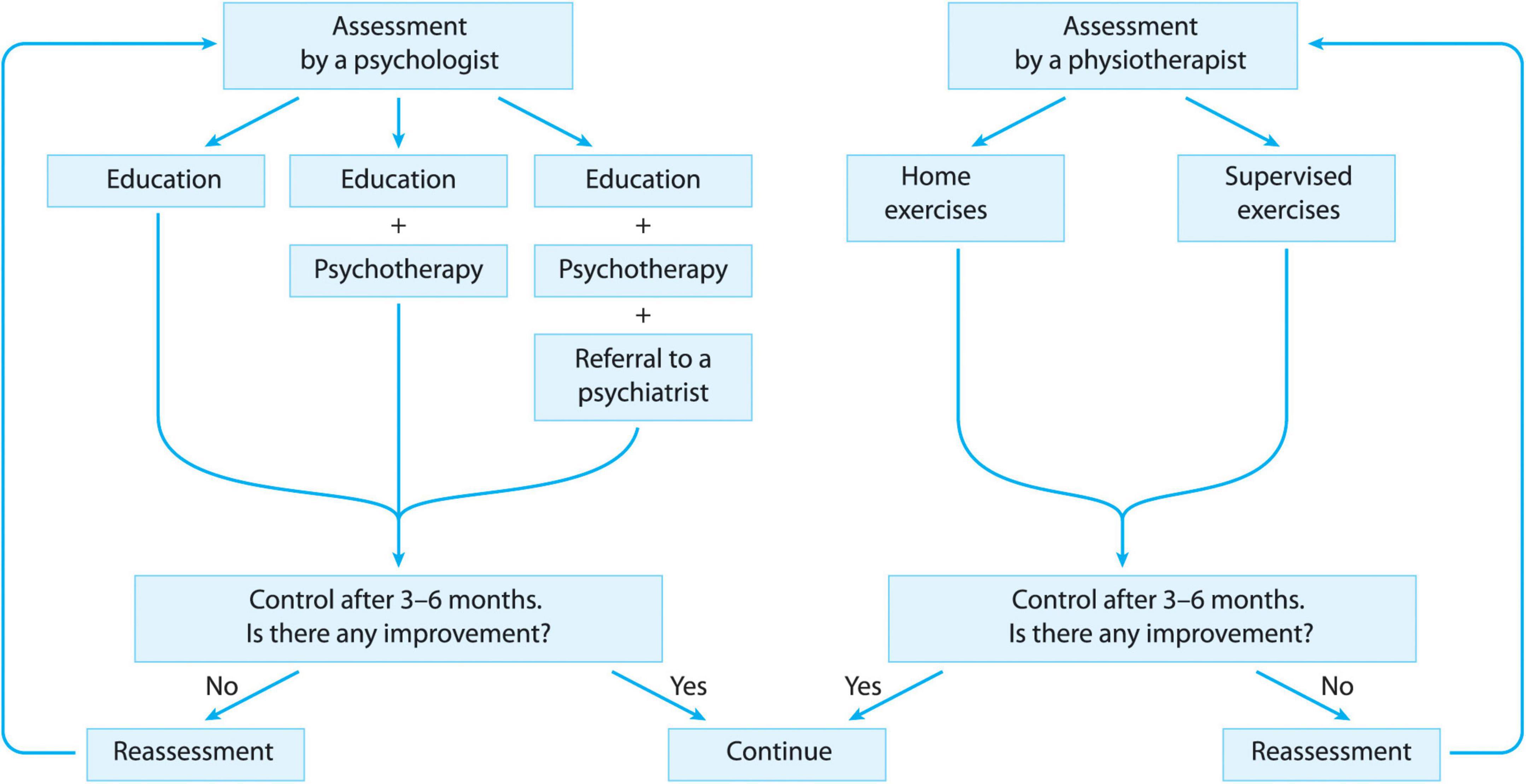
Figure 2. Proposed structure of non-pharmacological treatment in D2TRA.
According to the psychologist’s decision, every D2TRA patient can be enrolled in one of the following three intervention categories. No 1: Patients not in need of psychiatric examination or psychotherapy should receive regular educational sessions helping compliance and lifestyle changes. These educational sessions can be held individually or in groups, in the organization of the medical system or of patient organizations, by any health care worker (medical doctor, psychologist, nurse etc.) who is trained in this field. No 2: Patients in need of psychotherapy (e.g., for relaxation, coping strategies etc.) should be offered a psychotherapeutic intervention according to the psychologist’s decision (e.g., CBT, mindfulness) apart from the educational sessions, held by a psychologist. No 3: For those D2TRA patients where according to the psychologist’s judgment a psychotherapy is not sufficient (e.g., depression, fibromyalgia) an examination by a psychiatrist and pharmacotherapy when needed should be offered apart from the psychotherapy and the educational sessions.
According to the physiotherapist’s judgment, every D2TRA patient can be enrolled in one of the following two intervention categories. No 1: Independent regular aerobic and strengthening exercises at home for patients who do not need any supervision or help according to the physiotherapist. A digital or written material for the structuration of these exercises, and the writing of an exercise diary until the next reassessment is suggested in this group of patients. No 2: Regular supervised aerobic and strengthening exercise sessions should be offered to those patients, who need supervision due to compliance problems, disabilities, joint destructions, comorbidities etc.
Additionally to the above mentioned two elements, other NPT options can be offered to D2TRA patients, according to the decision of the rheumatologist/psychologist/physiotherapist/rehabilitation specialist/orthopedist. These NPT options can be additional exercise therapies (e.g., mobilization techniques, special trainings like dance, yoga), physiotherapies (e.g., US, laser, TENS, cryotherapy), balneotherapy, assistive devices, ergotherapy/occupational therapy.
Discussion
With the new biological and targeted therapies, complete remission has become an attainable goal in rheumatoid arthritis, nevertheless a part of RA patients are still not meeting treatment goals according to treat to target principles, and can be defined as difficult-to-treat RA. The different non-pharmacological therapies (NPT) cover a wide range of interventions, including many exercise modalities, psychological interventions, physio- and balneotherapy, dietary interventions, education etc. NPTs with their complex action can have a synergistic, additive effect with targeted pharmacological therapies, which is highly needed in D2TRA patients, where pharmacological treatment options are often limited. In this review we are summarizing the literature about NPT in RA focusing on patient groups with high probability of D2TRA. A limitation is that the term D2TRA is fairly new, and some studies about NPT were conducted before the widespread use of biological therapies, or patients in many studies were not selected according to the DMARD use, thus trials focusing definitely on D2TRA are yet lacking. This review is also meant to raise attention to this important issue.
We are suggesting that simultaneously with pharmacotherapy, a complex non-pharmacological treatment program should be offered to all D2TRA patients, including regular assessment by a psychologist and a physiotherapist in parallel with the rheumatologist’s investigations, and obligatory and optional NPT elements. Our NPT proposal is focusing on point 9 of the EULAR points to consider in D2TRA (8), which emphasizes the possibility of non-pharmacological interventions to optimize management, and it also has common elements with some other points of the EULAR point to consider: These are the possibility of misdiagnosis or coexistence of mimicking diseases (point 1), importance of shared decision-making (point 4), appropriate education and support (point 10) and the offering of self-management programs, education and psychological interventions (point 10). We are suggesting that following this NPT plan, D2TRA patients can be helped in reaching a better quality of life, better self-management and attainment of treatment goals. Additionally, as treatment options are often limited in D2TRA patients, and non-pharmacological interventions are generally shown to be safe and well tolerated, there is an unmet need for further investigation about different NPT in D2TRA, to clarify their impact on inflammation, cytokine patterns, the neuro-hormono-immunological system, and further clinical studies are needed in the future to optimize the non-pharmacological treatment options in D2TRA, promoting the holistic, personalized treatment approach of this complex disease.
Author contributions
JM and GN contributed to conception and design of the study. JM, NC-N, GB, TB, and GN did the literature search and wrote the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This work was supported by grants from the National Scientific Research Program OTKA K-131479, the Rheuma Tolerance for Cure H2020 777357, and with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development, and Innovation Fund, financed under the TKP2021-EGA/TKP2021-NVA/ TKP2021-NKTA funding scheme.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.991677/full#supplementary-material
Supplementary Table 1 | Summary of literature for exercise therapy in D2TRA.
Supplementary Table 2 | Summary of literature for psychological interventions in D2TRA.
Supplementary Table 3 | Summary of literature for physiotherapy, balneotherapy and other non-pharmacological interventions in D2TRA.
References
1. Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. (2020) 79:685–99.
2. Fraenkel L, Bathon JM, England BR, St Clair EW, Arayssi T, Carandang K, et al. 2021 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res. (2021) 73:924–39.
3. Zangi HA, Ndosi M, Adams J, Andersen L, Bode C, Boström C, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. (2015) 74:954–62. doi: 10.1136/annrheumdis-2014-206807
4. Osthoff A-KR, Niedermann K, Braun J, Adams J, Brodin N, Dagfinrud H, et al. 2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. Ann Rheum Dis. (2018) 77:1251–60. doi: 10.1136/annrheumdis-2018-213585
5. Nikiphorou E, Santos EJF, Marques A, Böhm P, Bijlsma JW, Daien CI, et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann Rheum Dis. (2021) 80:1278–85. doi: 10.1136/annrheumdis-2021-220249
6. Combe B, Landewe R, Daien CI, Hua C, Aletaha D, Álvaro-Gracia JM, et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann Rheum Dis. (2017) 76:948–59. doi: 10.1136/annrheumdis-2016-210602
7. Nagy G, Roodenrijs NM, Welsing PM, Kedves M, Hamar A, van der Goes MC, et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. (2021) 80:31–5. doi: 10.1136/annrheumdis-2020-217344
8. Nagy G, Roodenrijs NMT, Welsing PMJ, Kedves M, Hamar A, van der Goes MC, et al. EULAR points to consider for the management of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. (2022) 81:20–33. doi: 10.1136/annrheumdis-2021-220973
9. Roodenrijs NMT, Hamar A, Kedves M, Nagy G, van Laar JM, van der Heijde D, et al. Pharmacological and non-pharmacological therapeutic strategies in difficult-to-treat rheumatoid arthritis: a systematic literature review informing the EULAR recommendations for the management of difficult-to-treat rheumatoid arthritis. RMD Open. (2021) 7:e001512. doi: 10.1136/rmdopen-2020-001512
10. Santos EJF, Duarte C, Marques A, Cardoso D, Apóstolo J, da Silva JAP, et al. Effectiveness of non-pharmacological and non-surgical interventions for rheumatoid arthritis: an umbrella review. JBI Database Syst Rev Implement Rep. (2019) 17:1494–531. doi: 10.11124/JBISRIR-D-18-00020
11. Andonian BJ, Johannemann A, Hubal MJ, Pober DM, Koss A, Kraus WE, et al. Altered skeletal muscle metabolic pathways, age, systemic inflammation, and low cardiorespiratory fitness associate with improvements in disease activity following high-intensity interval training in persons with rheumatoid arthritis. Arthritis Res Ther. (2021) 23:187. doi: 10.1186/s13075-021-02570-3
12. Summers G, Booth A, Brooke-Wavell K, Barami T, Clemes S. Physical activity and sedentary behavior in women with rheumatoid arthritis: a comparison of patients with low and high disease activity and healthy controls. Open Access Rheumatol. (2019) 11:133–42. doi: 10.2147/OARRR.S203511
13. Feldthusen C, Dean E, Forsblad-d’Elia H, Mannerkorpi K. Effects of person-centered physical therapy on fatigue-related variables in persons with rheumatoid arthritis: a randomized controlled trial. Arch Phys Med Rehabil. (2016) 97:26–36. doi: 10.1016/j.apmr.2015.09.022
14. Hurkmans E, van der Giesen FJ, Vliet Vlieland TP, Schoones J, Van den Ende ECHM. Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis. Cochrane Database Syst Rev. (2009) 2009:CD006853. doi: 10.1002/14651858.CD006853.pub2
15. Hurkmans EJ, van den Berg MH, Ronday KH, Peeters AJ, le Cessie S, Vlieland TPMV. Maintenance of physical activity after Internet-based physical activity interventions in patients with rheumatoid arthritis. Rheumatology. (2010) 49:167–72. doi: 10.1093/rheumatology/kep285
16. Sobue Y, Kojima T, Ito H, Nishida K, Matsushita I, Kaneko Y, et al. Does exercise therapy improve patient-reported outcomes in rheumatoid arthritis? A systematic review and meta-analysis for the update of the 2020 JCR guidelines for the management of rheumatoid arthritis. Mod Rheumatol. (2022) 32:96–104. doi: 10.1080/14397595.2021.1886653
17. Manning VL, Hurley MV, Scott DL, Coker B, Choy E, Bearne LM. Education, self-management, and upper extremity exercise training in people with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res. (2014) 66:217–27. doi: 10.1002/acr.22102
18. Cramp F, Hewlett S, Almeida C, Kirwan JR, Choy EHS, Chalder T, et al. Non-pharmacological interventions for fatigue in rheumatoid arthritis. Cochrane Database Syst Rev. (2013) CD008322. doi: 10.1002/14651858.CD008322.pub2
19. Wen Z, Chai Y. Effectiveness of resistance exercises in the treatment of rheumatoid arthritis: a meta-analysis. Medicine. (2021) 100:e25019. doi: 10.1097/MD.0000000000025019
20. Mudano AS, Tugwell P, Wells GA, Singh JA. Tai Chi for rheumatoid arthritis. Cochrane Database Syst Rev. (2019) 9:CD004849. doi: 10.1002/14651858.CD004849.pub2
21. Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for rheumatic diseases: a systematic review. Rheumatology. (2013) 52:2025–30. doi: 10.1093/rheumatology/ket264
22. Ye X, Chen Z, Shen Z, Chen G, Xu X. Yoga for treating rheumatoid arthritis: a systematic review and meta-analysis. Front Med. (2020) 7:586665. doi: 10.3389/fmed.2020.586665
23. Lau YN, Ng J, Lee SY, Li LC, Kwan CM, Fan SM, et al. A brief report on the clinical trial on neural mobilization exercise for joint pain in patients with rheumatoid arthritis. Z Rheumatol. (2019) 78:474–8. doi: 10.1007/s00393-018-0521-7
24. Romanowski MW, Špiritović M, Romanowski W, Straburzyńska-Lupa A. Manual therapy (postisometric relaxation and joint mobilization) in knee pain and function experienced by patients with rheumatoid arthritis: a randomized clinical pilot study. Evid Based Complement Alternat Med. (2020) 2020:1452579. doi: 10.1155/2020/1452579
25. Liao C-D, Chen H-C, Huang S-W, Liou T-H. Exercise therapy for sarcopenia in rheumatoid arthritis: a meta-analysis and meta-regression of randomized controlled trials. Clin Rehabil. (2021) 36:145–57. doi: 10.1177/02692155211035539
26. Eversden L, Maggs F, Nightingale P, Jobanputra P. A pragmatic randomised controlled trial of hydrotherapy and land exercises on overall well being and quality of life in rheumatoid arthritis. BMC Musculoskelet Disord. (2007) 8:23. doi: 10.1186/1471-2474-8-23
27. Siqueira US, Orsini Valente LG, de Mello MT, Szejnfeld VL, Pinheiro MM. Effectiveness of aquatic exercises in women with rheumatoid arthritis: a randomized, controlled, 16-week intervention—the hydRA trial. Am J Phys Med Rehabil. (2017) 96:167. doi: 10.1097/PHM.0000000000000564
28. Metsios GS, Stavropoulos-Kalinoglou A, Panoulas VF, Wilson M, Nevill AM, Koutedakis Y, et al. Association of physical inactivity with increased cardiovascular risk in patients with rheumatoid arthritis. Eur J Cardiovasc Prev Rehabil. (2009) 16:188–94. doi: 10.1097/HJR.0b013e3283271ceb
29. Hupin D, Sarajlic P, Venkateshvaran A, Fridén C, Nordgren B, Opava CH, et al. Cardiovascular autonomic function changes and predictors during a 2-year physical activity program in rheumatoid arthritis: a PARA 2010 substudy. Front Med. (2021) 8:788243. doi: 10.3389/fmed.2021.788243
30. Sul B, Lee KB, Joo YB, Hong BY, Kim J-S, Kim K-J, et al. Twelve weeks of strengthening exercise for patients with rheumatoid arthritis: a prospective intervention study. J Clin Med Res. (2020) 9:2792. doi: 10.3390/jcm9092792
31. McKenna SG, Donnelly A, Esbensen BA, Comber L, Ng WL, Anjum AM, et al. The feasibility of an exercise intervention to improve sleep (time, quality and disturbance) in people with rheumatoid arthritis: a pilot RCT. Rheumatol Int. (2021) 41:297–310. doi: 10.1007/s00296-020-04760-9
32. Knittle K, De Gucht V, Hurkmans E, Peeters A, Ronday K, Maes S, et al. Targeting motivation and self-regulation to increase physical activity among patients with rheumatoid arthritis: a randomised controlled trial. Clin Rheumatol. (2015) 34:231–8. doi: 10.1007/s10067-013-2425-x
33. Hurkmans EJ, Maes S, de Gucht V, Knittle K, Peeters AJ, Ronday HK, et al. Motivation as a determinant of physical activity in patients with rheumatoid arthritis. Arthritis Care Res (Hoboken). (2010) 62:371–7. doi: 10.1002/acr.20106
34. Srikesavan C, Williamson E, Thompson JY, Cranston T, Swales C, Lamb SE. The online version of an evidence-based hand exercise program for people with rheumatoid arthritis: a mixed-method, proof-of-concept study. J Hand Ther. (2020) S0894–1130(20)30190–3. doi: 10.1016/j.jht.2020.10.011 [Epub ahead of print].
35. Sieczkowska SM, Smaira FI, Mazzolani BC, Gualano B, Roschel H, Peçanha T. Efficacy of home-based physical activity interventions in patients with autoimmune rheumatic diseases: a systematic review and meta-analysis. Semin Arthritis Rheum. (2021) 51:576–87. doi: 10.1016/j.semarthrit.2021.04.004
36. Brady SM, Fenton SAM, Metsios GS, Bosworth A, Duda JL, Kitas GD, et al. Different types of physical activity are positively associated with indicators of mental health and psychological wellbeing in rheumatoid arthritis during COVID-19. Rheumatol Int. (2021) 41:335–44. doi: 10.1007/s00296-020-04751-w
37. Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis. Rheumatology. (2013) 52:2136–48. doi: 10.1093/rheumatology/ket169
38. Roodenrijs NMT, van der Goes MC, Welsing PMJ, Tekstra J, Lafeber FPJG, Jacobs JWG, et al. Difficult-to-treat rheumatoid arthritis: contributing factors and burden of disease. Rheumatology. (2021) 60:3778–88. doi: 10.1093/rheumatology/keaa860
39. Kim SY, Chanyang M, Oh DJ, Choi HG. Association between depression and rheumatoid arthritis: two longitudinal follow-up studies using a national sample cohort. Rheumatology. (2020) 59:1889–97. doi: 10.1093/rheumatology/kez559
40. Fakra E, Marotte H. Rheumatoid arthritis and depression. Joint Bone Spine. (2021) 88:105200. doi: 10.1016/j.jbspin.2021.105200
41. Davies R, Williams J, Sime K, Jin H-S, Thompson C, Jordan L, et al. The role of interleukin-6 trans-signalling on cardiovascular dysfunction in inflammatory arthritis. Rheumatology. (2021) 60:2852–61. doi: 10.1093/rheumatology/keaa725
42. Harth M, Nielson WR. Pain and affective distress in arthritis: relationship to immunity and inflammation. Expert Rev Clin Immunol. (2019) 15:541–52. doi: 10.1080/1744666X.2019.1573675
43. Anvar N, Matlabi H, Safaiyan A, Allahverdipour H, Kolahi S. Effectiveness of self-management program on arthritis symptoms among older women: a randomized controlled trial study. Health Care Women Int. (2018) 39:1326–39. doi: 10.1080/07399332.2018.1438438
44. El Miedany Y, El Gaafary M, El Arousy N, Ahmed I, Youssef S, Palmer D. Arthritis education: the integration of patient-reported outcome measures and patient self-management. Clin Exp Rheumatol. (2012) 30:899–904.
45. Lorig KR, Ritter PL, Laurent DD, Plant K. The internet-based arthritis self-management program: a one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Rheum. (2008) 59:1009–17. doi: 10.1002/art.23817
46. Shigaki CL, Smarr KL, Siva C, Ge B, Musser D, Johnson R. RAHelp: an online intervention for individuals with rheumatoid arthritis. Arthritis Care Res. (2013) 65:1573–81. doi: 10.1002/acr.22042
47. Davis MC, Zautra AJ, Wolf LD, Tennen H, Yeung EW. Mindfulness and cognitive-behavioral interventions for chronic pain: differential effects on daily pain reactivity and stress reactivity. J Consult Clin Psychol. (2015) 83:24–35. doi: 10.1037/a0038200
48. Fogarty FA, Booth RJ, Gamble GD, Dalbeth N, Consedine NS. The effect of mindfulness-based stress reduction on disease activity in people with rheumatoid arthritis: a randomised controlled trial. Ann Rheum Dis. (2015) 74:472–4. doi: 10.1136/annrheumdis-2014-205946
49. Zangi HA, Mowinckel P, Finset A, Eriksson LR. A mindfulness-based group intervention to reduce psychological distress and fatigue in patients with inflammatory rheumatic joint diseases: a randomised controlled. Ann Rheum Dis. (2012) 71:911–7.
50. Hewlett S, Almeida C, Ambler N, Blair PS, Choy EH, Dures E, et al. Reducing arthritis fatigue impact: two-year randomised controlled trial of cognitive behavioural approaches by rheumatology teams (RAFT). Ann Rheum Dis. (2019) 78:465–72.
51. Lumley MA, Keefe FJ, Mosley-Williams A, Rice JR, McKee D, Waters SJ, et al. The effects of written emotional disclosure and coping skills training in rheumatoid arthritis: a randomized clinical trial. J Consult Clin Psychol. (2014) 82:644–58. doi: 10.1037/a0036958
52. Sharpe L, Schrieber L. A blind randomized controlled trial of cognitive versus behavioral versus cognitive-behavioral therapy for patients with rheumatoid arthritis. Psychother Psychosom. (2012) 81:145–52. doi: 10.1159/000332334
53. Zautra AJ, Davis MC, Reich JW, Nicassario P, Tennen H, Finan P, et al. Comparison of cognitive behavioral and mindfulness meditation interventions on adaptation to rheumatoid arthritis for patients with and without history of recurrent depression. J Consult Clin Psychol. (2008) 76:408–21. doi: 10.1037/0022-006X.76.3.408
54. Ferwerda M, van Beugen S, van Middendorp H, Visser H, Vonkeman H, Creemers M, et al. Tailored, therapist-guided internet-based cognitive behavioral therapy compared to care as usual for patients with rheumatoid arthritis: economic evaluation of a randomized controlled trial. J Med Internet Res. (2018) 20:e260. doi: 10.2196/jmir.9997
55. Terpstra JA, van der Vaart R, Ding HJ, Kloppenburg M, Evers AWM. Guided internet-based cognitive-behavioral therapy for patients with rheumatic conditions: a systematic review. Internet Interv. (2021) 26:100444. doi: 10.1016/j.invent.2021.100444
56. Keefe FJ, Anderson T, Lumley M, Caldwell D, Stainbrook D, Mckee D, et al. A randomized, controlled trial of emotional disclosure in rheumatoid arthritis: can clinician assistance enhance the effects? Pain. (2008) 137:164–72. doi: 10.1016/j.pain.2007.08.031
57. Attia AMM, Ibrahim FAA, Abd El-Latif NA, Aziz SW, Elwan AM, Abdel Aziz AAA, et al. Therapeutic antioxidant and anti-inflammatory effects of laser acupuncture on patients with rheumatoid arthritis. Lasers Surg Med. (2016) 48:490–7. doi: 10.1002/lsm.22487
58. Casimiro L, Brosseau L, Robinson V, Milne S, Judd M, Well G, et al. Therapeutic ultrasound for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. (2002) CD003787. doi: 10.1002/14651858.CD003787
59. Király M, Varga Z, Szanyó F, Kiss R, Hodosi K, Bender T. Effects of underwater ultrasound therapy on pain, inflammation, hand function and quality of life in patients with rheumatoid arthritis - a randomized controlled trial. Braz J Phys Ther. (2017) 21:199–205. doi: 10.1016/j.bjpt.2017.04.002
60. Brosseau L, Judd MG, Marchand S, Robinson VA, Tugwell P, Wells G, et al. Transcutaneous electrical nerve stimulation (TENS) for the treatment of rheumatoid arthritis in the hand. Cochrane Database Syst Rev. (2003) CD004377. doi: 10.1002/14651858.CD004377
61. Drewes AM, Brock C, Rasmussen SE, Møller HJ, Brock B, Deleuran BW, et al. Short-term transcutaneous non-invasive vagus nerve stimulation may reduce disease activity and pro-inflammatory cytokines in rheumatoid arthritis: results of a pilot study. Scand J Rheumatol. (2021) 50:20–7. doi: 10.1080/03009742.2020.1764617
62. Almeida GJ, Khoja SS, Piva SR. Dose-response relationship between neuromuscular electrical stimulation and muscle function in people with rheumatoid arthritis. Phys Ther. (2019) 99:1167–76. doi: 10.1093/ptj/pzz079
63. Piva SR, Khoja SS, Toledo FGS, Chester-Wasko M, Fitzgerald GK, Goodpaster BH, et al. Neuromuscular electrical stimulation compared to volitional exercise for improving muscle function in rheumatoid arthritis: a randomized pilot study. Arthritis Care Res. (2019) 71:352–61. doi: 10.1002/acr.23602
64. Pelland L, Brosseau L, Casimiro L, Welch V, Tugwell P, Wells GA. Electrical stimulation for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. (2002). Available online at: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003687/full (accessed January 9, 2022).
65. Gizińska M, Rutkowski R, Romanowski W, Lewandowski J, Straburzyńska-Lupa A. Effects of whole-body cryotherapy in comparison with other physical modalities used with kinesitherapy in rheumatoid arthritis. Biomed Res Int. (2015) 2015:409174. doi: 10.1155/2015/409174
66. Hirvonen H, Kautiainen H, Moilanen E, Mikkelsson M, Leirisalo-Repo M. The effect of cryotherapy on total antioxidative capacity in patients with active seropositive rheumatoid arthritis. Rheumatol Int. (2017) 37:1481–7. doi: 10.1007/s00296-017-3771-9
67. Jastrząbek R, Straburzyńska-Lupa A, Rutkowski R, Romanowski W. Effects of different local cryotherapies on systemic levels of TNF-α, IL-6, and clinical parameters in active rheumatoid arthritis. Rheumatol Int. (2013) 33:2053–60. doi: 10.1007/s00296-013-2692-5
68. Peres D, Sagawa Y Jr, Dugué B, Domenech SC, Tordi N, Prati C. The practice of physical activity and cryotherapy in rheumatoid arthritis: systematic review. Eur J Phys Rehabil Med. (2017) 53:775–87. doi: 10.23736/S1973-9087.16.04534-2
69. Franke A, Reiner L, Pratzel HG, Franke T, Resch KL. Long-term efficacy of radon spa therapy in rheumatoid arthritis–a randomized, sham-controlled study and follow-up. Rheumatology. (2000) 39:894–902. doi: 10.1093/rheumatology/39.8.894
70. Annegret F, Thomas F. Long-term benefits of radon spa therapy in rheumatic diseases: results of the randomised, multi-centre IMuRa trial. Rheumatol Int. (2013) 33:2839–50. doi: 10.1007/s00296-013-2819-8
71. Santos I, Cantista P, Vasconcelos C, Amado J. Balneotherapy and rheumatoid arthritis: a randomized control trial. Isr Med Assoc J. (2016) 18:474–8.
72. Sukenik S, Buskila D, Neumann L, Kleiner-Baumgarten A, Zimlichman S, Horowitz J. Sulphur bath and mud pack treatment for rheumatoid arthritis at the Dead Sea area. Ann Rheum Dis. (1990) 49:99–102. doi: 10.1136/ard.49.2.99
73. Sukenik S, Buskila D, Neumann L, Kleiner-Baumgarten A. Mud pack therapy in rheumatoid arthritis. Clin Rheumatol. (1992) 11:243–7. doi: 10.1007/BF02207966
74. Codish S, Abu-Shakra M, Flusser D, Friger M, Sukenik S. Mud compress therapy for the hands of patients with rheumatoid arthritis. Rheumatol Int. (2005) 25:49–54. doi: 10.1007/s00296-003-0402-4
75. Hagen KB, Byfuglien MG, Falzon L, Olsen SU, Smedslund G. Dietary interventions for rheumatoid arthritis. Cochrane Database Syst Rev. (2009) CD006400. doi: 10.1002/14651858.CD006400.pub2
76. García-Morales JM, Lozada-Mellado M, Hinojosa-Azaola A, Llorente L, Ogata-Medel M, Pineda-Juárez JA, et al. Effect of a dynamic exercise program in combination with mediterranean diet on quality of life in women with rheumatoid arthritis. J Clin Rheumatol. (2020) 26(7 Suppl. 2):S116–22. doi: 10.1097/RHU.0000000000001064
77. Pineda-Juárez JA, Lozada-Mellado M, Hinojosa-Azaola A, García-Morales JM, Ogata-Medel M, Llorente L, et al. Changes in hand grip strength and body weight after a dynamic exercise program and Mediterranean diet in women with rheumatoid arthritis: a randomized clinical trial. Physiother Theory Pract. (2020) 38:504–12. doi: 10.1080/09593985.2020.1777605
78. Guan Y, Hao Y, Guan Y, Bu H, Wang H. The effect of vitamin d supplementation on rheumatoid arthritis patients: a systematic review and meta-analysis. Front Med. (2020) 7:596007. doi: 10.3389/fmed.2020.596007
79. Akbar U, Yang M, Kurian D, Mohan C. Omega-3 fatty acids in rheumatic diseases: a critical review. J Clin Rheumatol. (2017) 23:330–9. doi: 10.1097/RHU.0000000000000563
80. Cameron M, Gagnier JJ, Chrubasik S. Herbal therapy for treating rheumatoid arthritis. Cochrane Database Syst Rev. (2011) CD002948. doi: 10.1002/14651858.CD002948.pub2
81. Guerreiro CS, Calado Â, Sousa J, Fonseca JE. Diet, microbiota, and gut permeability-the unknown triad in rheumatoid arthritis. Front Med. (2018) 5:349. doi: 10.3389/fmed.2018.00349
82. Weijers JM, Müskens WD, van Riel PLCM. Effect of significant weight loss on disease activity: reason to implement this non-pharmaceutical intervention in daily clinical practice. RMD Open. (2021) 7:e001498. doi: 10.1136/rmdopen-2020-001498
83. Kreps DJ, Halperin F, Desai SP, Zhang ZZ, Losina E, Olson AT, et al. Association of weight loss with improved disease activity in patients with rheumatoid arthritis: a retrospective analysis using electronic medical record data. Int J Clin Rheumtol. (2018) 13:1–10. doi: 10.4172/1758-4272.1000154
84. Somers TJ, Blumenthal JA, Dorfman CS, Huffman KM, Edmond SN, Miller SN, et al. Effects of a weight and pain management program in patients with rheumatoid arthritis with obesity: a randomized controlled pilot investigation. J Clin Rheumatol. (2022) 28:7–13. doi: 10.1097/RHU.0000000000001793
85. England BR, Baker JF, Sayles H, Michaud K, Caplan L, Davis LA, et al. Body mass index, weight loss, and cause-specific mortality in rheumatoid arthritis. Arthritis Care Res. (2018) 70:11–8. doi: 10.1002/acr.23258
86. Baker JF, Billig E, Michaud K, Ibrahim S, Caplan L, Cannon GW, et al. Weight loss, the obesity paradox, and the risk of death in rheumatoid arthritis. Arthritis Rheumatol. (2015) 67:1711–7. doi: 10.1002/art.39136
87. Tam L-S, Leung P-C, Li TK, Zhang L, Li EK. Acupuncture in the treatment of rheumatoid arthritis: a double-blind controlled pilot study. BMC Complement Altern Med. (2007) 7:35. doi: 10.1186/1472-6882-7-35
88. Lee MS, Shin B-C, Ernst E. Acupuncture for rheumatoid arthritis: a systematic review. Rheumatology. (2008) 47:1747–53. doi: 10.1093/rheumatology/ken330
89. Casimiro L, Barnsley L, Brosseau L, Milne S, Robinson VA, Tugwell P, et al. Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. (2005) CD003788. doi: 10.1002/14651858.CD003788.pub2
90. Sato M, Inubushi M, Shiga T, Hirata K, Okamoto S, Kamibayashi T, et al. Therapeutic effects of acupuncture in patients with rheumatoid arthritis: a prospective study using (18)F-FDG-PET. Ann Nucl Med. (2009) 23:311–6. doi: 10.1007/s12149-009-0238-4
91. Seca S, Patrício M, Kirch S, Franconi G, Cabrita AS, Greten HJ. Effectiveness of acupuncture on pain, functional disability, and quality of life in rheumatoid arthritis of the hand: results of a double-blind randomized clinical trial. J Altern Complement Med. (2019) 25:86–97. doi: 10.1089/acm.2018.0297
92. Macedo AM, Oakley SP, Panayi GS, Kirkham BW. Functional and work outcomes improve in patients with rheumatoid arthritis who receive targeted, comprehensive occupational therapy. Arthritis Rheum. (2009) 61:1522–30. doi: 10.1002/art.24563
93. Abhishek A, Butt S, Gadsby K, Zhang W, Deighton CM. Anti-TNF-α agents are less effective for the treatment of rheumatoid arthritis in current smokers. J Clin Rheumatol. (2010) 16:15. doi: 10.1097/RHU.0b013e3181ca4a2a
94. Szekanecz Z, Koncz Á, Dunkel J, Vencovský J, Cimdora Collaborators. Cigarette smoking and clinical response to certolizumab pegol treatment in Hungarian, Czech, and Slovak patients with rheumatoid arthritis: 104-week data from the CIMDORA prospective, non-interventional study. Clin Exp Rheumatol. (2019) 37:1010–8.
95. Roelsgaard IK, Esbensen BA, Østergaard M, Rollefstad S, Semb AG, Christensen R, et al. Smoking cessation intervention for reducing disease activity in chronic autoimmune inflammatory joint diseases. Cochrane Database Syst Rev. (2019) 9:CD012958. doi: 10.1002/14651858.CD012958.pub2
96. Tuntland H, Kjeken I, Nordheim LV, Falzon L, Jamtvedt G, Hagen KB. Assistive technology for rheumatoid arthritis. Cochrane Database Syst Rev. (2009) CD006729. doi: 10.1002/14651858.CD006729.pub2
97. Egan M, Brosseau L, Farmer M, Ouimet MA, Rees S, Wells G, et al. Splints/orthoses in the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. (2001) 2001:CD004018. doi: 10.1002/14651858.CD004018
Keywords: difficult-to-treat, rheumatoid arthritis, non-pharmacological, treatment, exercise, psychotherapy, physiotherapy
Citation: Majnik J, Császár-Nagy N, Böcskei G, Bender T and Nagy G (2022) Non-pharmacological treatment in difficult-to-treat rheumatoid arthritis. Front. Med. 9:991677. doi: 10.3389/fmed.2022.991677
Received: 11 July 2022; Accepted: 01 August 2022;
Published: 29 August 2022.
Edited by:
Alberto Lo Gullo, Garibaldi Hospital, ItalyReviewed by:
Pedro Santos-Moreno, Biomab IPS - Center for Rheumatoid Arthritis, ColombiaCopyright © 2022 Majnik, Császár-Nagy, Böcskei, Bender and Nagy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Judit Majnik, bWFqbmlrLmp1ZGl0QG1lZC5zZW1tZWx3ZWlzLXVuaXYuaHU=