 Renato Ferreira-da-Silva1,2*†
Renato Ferreira-da-Silva1,2*† Mariana Lobo2†
Mariana Lobo2† Ana Rafaela Abreu1†Juliana Pereira-Macedo1†Beatriz Mós1Carolina Ameijeiras Rodriguez1,2†Inês Mariana Lourenço1,3†Isabel Vieira1Jorge Junqueira Polónia1,4†Luís Gouveia1,2Lurdes Silva1
Ana Rafaela Abreu1†Juliana Pereira-Macedo1†Beatriz Mós1Carolina Ameijeiras Rodriguez1,2†Inês Mariana Lourenço1,3†Isabel Vieira1Jorge Junqueira Polónia1,4†Luís Gouveia1,2Lurdes Silva1 Manuela Morato5†Manuela Pinto6†Mario Forrester1†Marta Pereira7Nuno Rodrigues8Tayanny Biase1†Inês Ribeiro1,2†
Manuela Morato5†Manuela Pinto6†Mario Forrester1†Marta Pereira7Nuno Rodrigues8Tayanny Biase1†Inês Ribeiro1,2†- 1Porto Pharmacovigilance Centre, Faculty of Medicine of the University of Porto, Porto, Portugal
- 2RISE-Health, Department of Community Medicine, Information and Health Decision Sciences, Faculty of Medicine of the University of Porto, Porto, Portugal
- 3RISE-Health, Department of Surgery and Physiology, Faculty of Medicine, University of Porto, Porto, Portugal
- 4RISE-Health, Department of Medicine, Faculty of Medicine of the University of Porto, Porto, Portugal
- 5LAQV@REQUIMTE, Laboratory of Pharmacology, Department of Drug Sciences, Faculty of Pharmacy of the University of Porto, Porto, Portugal
- 6Local Health Unit of São João, E.P.E., Porto, Portugal
- 7Local Health Unit of Santo António, E.P.E., Porto, Portugal
- 8Local Health Unit of Vila Nova de Gaia/Espinho, E.P.E., Porto, Portugal
Background: Upadacitinib is an oral Janus kinase 1 (JAK1) selective inhibitor approved for the treatment of rheumatoid arthritis (RA) and other immune-mediated inflammatory diseases. Concerns have emerged regarding a potential increased risk of venous thromboembolism (VTE) with JAK inhibitors (JAKi), though real-world evidence remains limited.
Objective: To assess the post-marketing safety profile of upadacitinib in relation to VTE using global pharmacovigilance data.
Methods: We conducted a disproportionality analysis using Individual Case Safety Reports (ICSRs) from VigiBase, accessed via VigiLyze, including all reports up to February 20, 2025. Upadacitinib was compared with: (i) all other medicines; (ii) other second-line advanced RA therapies (bDMARDs and tsDMARDs); and (iii) other JAKi (baricitinib, tofacitinib, filgotinib). Reporting Odds Ratios (ROR) and Information Components (IC), with 95% confidence intervals, were calculated.
Results: Descriptive analyses identified 678 VTE cases with upadacitinib, predominantly affecting women (68.1%), with a median age of 63 years. Most were classified as serious (91.2%), although fatal outcomes were less frequent than with comparators. In disproportionality analyses, upadacitinib showed a significant signal versus all medicines (ROR: 2.08; IC: 1.04) and versus other second-line therapies (ROR: 1.40; IC: 0.41), but not versus other JAKi (ROR: 0.98; IC: –0.04). In 2023, disproportionality declined, particularly relative to other JAKi (ROR: 0.57; IC: –0.38).
Conclusion: Upadacitinib-related VTE cases display distinct clinical characteristics. These findings support continued pharmacovigilance and the need for robust real-world studies to clarify absolute and comparative risks, inform regulation, and guide personalised therapeutic strategies in RA.
Highlights
• Upadacitinib was associated with a higher-than-expected reporting of venous thromboembolism (VTE) compared with all medicines in VigiBase, other second-line therapies, and other JAK inhibitors (JAKi) for rheumatoid arthritis, suggesting a potential safety signal warranting monitoring in clinical practice.
• Within the JAKi class, upadacitinib showed a nuanced safety profile, with fewer reports of deep vein thrombosis but higher reports of pulmonary thrombosis compared with other JAKi, suggesting event-type-specific differences in VTE risk.
• Age-stratified analyses revealed that upadacitinib had higher VTE reporting in nearly all age groups compared to other JAKi, except in patients aged 18–44 years, highlighting the need for age-specific risk assessment when prescribing upadacitinib.
• In 2023, the disproportionality signal for VTE with upadacitinib attenuated compared to previous years and to other JAKi, potentially reflecting evolving prescribing practices, patient selection, and the impact of regulatory risk minimization measures.
• Despite a higher proportion of serious classifications, upadacitinib-related VTE cases had a lower proportion of fatal outcomes compared to other JAKi and therapies, underscoring the complexity of assessing severity and outcomes in spontaneous reporting data.
Introduction
The Janus kinase (JAK) family includes four intracellular non-receptor tyrosine kinases: JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2) (1). Among them, JAK1 stands out for its ability to form heterodimers with the other three JAKs, playing a critical role in signaling pathways. JAK1 dysregulation is strongly associated with inflammation and severe autoimmune conditions (2), which has led to a growing interest from researchers in studying JAK1 inhibitors as therapeutic agents. One such inhibitor, upadacitinib, is an oral drug that selectively targets JAK1 by reversibly inhibiting its signaling pathway. After several studies, a robust safety profile between its risk and benefit was demonstrated concerning its administration in several diseases compared to placebo, offering a more tailored approach to managing immune-mediated conditions (3, 4). Upadacitinib was initially approved by regulatory agencies, including the Food and Drug Administration (FDA) (5) and the European Medicines Agency (EMA) (6), in 2019 for treating rheumatoid arthritis (RA). Therapeutic strategies for RA typically involve disease-modifying antirheumatic drugs (DMARDs), which comprise biologic agents (bDMARDs) and targeted synthetic agents (tsDMARDs), the latter including JAK inhibitors (JAKi), all aimed at controlling inflammation and halting disease progression (7, 8). Since then, its therapeutic indications have been expanded to include other chronic inflammatory diseases, such as dermatological and gastrointestinal conditions, including moderately to severely active Crohn’s disease (9), and more recently, giant cell arteritis (10). Notably, the FDA approved upadacitinib as the first oral treatment option for Crohn’s disease in patients with inadequate response or intolerance to tumor necrosis factor (TNF) blockers, highlighting its growing role in addressing unmet clinical needs across multiple inflammatory conditions (11, 12).
Despite the efficacy of JAK1 inhibitors to treat inflammatory and immune-mediated diseases, some concerns have been pointed out relating to their use, especially the increased risk of major adverse cardiovascular events (MACE), malignancy, mortality or occurrence of venous thromboembolic events (VTE) (13). In fact, in two studies carried out by the ORAL Surveillance trial (14, 15), with 4,362 included patients (1,455 receiving tofacitinib) and a median follow-up of 4.0 years, one of the JAKi, tofacitinib, was associated with an increase in MACE, cancer, VTE, pulmonary embolism and death. Opportunistic infections, such as herpes zoster or tuberculosis, were also associated with tofacitinib (14). Moreover, according to a study by Gouverneur et al. (16), which included 5,870 patients, 93.7% of whom were diagnosed with RA and treated with JAKi (tofacitinib and baricitinib), a total of 92 thromboembolic events were recorded. Of these, 41.3% were VTE, with a slight trend toward an increased risk, particularly in patients with pre-existing cardiovascular risk factors, such as hypertension and a history of smoking. After reviewing these results, the FDA warned about the risks of MACE, malignancies, and VTE with tofacitinib, restricting JAKi use to patients unresponsive to TNF inhibitors (TNFis). Based on comparable evidence, these restrictions were later extended to baricitinib and upadacitinib. Consequently, guidelines recommend a cautious approach when prescribing JAKi to patients at risk of thrombosis (17).
A recent trial involving 4,298 patients treated with upadacitinib across different indications found similar rates of MACE and VTE to those observed with other biologic treatments for RA, psoriatic arthritis, or ankylosing spondylitis, suggesting that upadacitinib does not entail increased risk compared to other therapies (18). From another perspective, a post hoc analysis pooling safety data from six phase III trials evaluated 3,209 patients treated with upadacitinib 15 mg daily (alone or in combination with methotrexate), adalimumab, or methotrexate monotherapy. The rates of MACE and VTE were higher among RA patients with increased cardiovascular risk but remained comparable across treatment groups. However, significantly increased rates of serious opportunistic infections and non-melanoma skin cancer were observed in upadacitinib-treated patients compared with comparators (19). In contrast, a systematic review and meta-analysis conducted by Partalidou et al. 20), which included 23 studies, found no statistically significant differences in the occurrence of MACE or DVT between JAKi and TNFi in patients with RA, highlighting the need for more conclusive evidence regarding the cardiovascular safety of JAKi.
Therefore, the present study aimed to address the ongoing controversy and evidence gaps regarding the safety profile of upadacitinib, particularly its potential association with VTE. Using post-marketing data from VigiBase, we conducted a disproportionality analysis to detect potential safety signals. The analysis was structured across three comparative levels: (i) a global comparison with all other medicines; (ii) a focused comparison with other second-line advanced therapies for RA, including both bDMARDs and tsDMARDs, as defined in the Portuguese clinical guidelines; and (iii) a targeted comparison with other JAKi. The aim was to explore the safety of upadacitinib both in a broad pharmacovigilance context and within its originally approved indication (RA), using a multilevel approach to provide insight into its risk profile across general and condition-specific settings.
Materials and methods
Source of data
This study is based on Individual Case Safety Reports (ICSRs) extracted from VigiBase, the World Health Organization (WHO) global database of ICSRs. Managed by the Uppsala Monitoring Centre (UMC), VigiBase compiles pharmacovigilance data from over 150 national drug regulatory authorities worldwide (21). The database is linked to standardized medical and drug classifications, including MedDRA (Medical Dictionary for Regulatory Activities) and WHODrug (WHO’s medicinal product dictionary), ensuring consistency in case coding, retrieval, and analysis. Reports in VigiBase originate from spontaneous reporting systems and regulatory submissions, which may vary in completeness and causality assessment, but collectively serve as a critical resource for global pharmacovigilance and signal detection.
Study design and case selection
This study is a retrospective pharmacovigilance analysis evaluating the reporting pattern of VTE associated with upadacitinib in VigiBase. All ICSRs recorded up to February 20, 2025, were considered to define upadacitinib suspected cases (exposed cases) and several comparative groups (non-exposed cases), with no restrictions applied based on reporting country, patient demographics (age, gender), or report type. The study focused on VTE, identified using the Standardized MedDRA Query (SMQ) Narrow for “Embolic and thrombotic events, venous” (SMQ code: 20000084), which encompasses 102 Preferred Terms (PTs) related to venous thromboembolism. To minimize potential biases associated with spontaneous reporting, automated and manual verification excluded duplicate records and reports with incomplete case information.
We assessed the safety profile of upadacitinib for VTE by conducting a disproportionality analysis using post-marketing data from VigiBase, accessed via VigiLyze. The analysis was structured across three comparative levels. First, upadacitinib was compared with all other medicines in the database. Second, we restricted the comparison to other second-line advanced therapies for RA, as defined by the Portuguese National Pharmacy and Therapeutics Committee, including both bDMARDs (abatacept, rituximab, tocilizumab) and tsDMARDs, all of which are JAKi (baricitinib, tofacitinib, filgotinib). Third, we compared upadacitinib specifically with other tsDMARDs (i.e., JAKi: baricitinib, tofacitinib, filgotinib). These three comparator levels allowed for a multilevel evaluation of the safety profile of upadacitinib, both broadly and in relation to therapeutically and mechanistically similar agents.
Data analysis and signal detection
A descriptive statistical analysis was initially carried out on the demographic and clinical characteristics of cases, including age, sex, country of primary source (grouped according to WHO geographic regions), year of VigiBase initial date, number of drugs per case (categorized as 1, 2–4, or ≥ 5 drugs reported), reported RA indication, number of AE per case, seriousness status and criteria, and fatal outcomes.
A disproportionality analysis was performed using two established signal detection methods for all drugs with at least three reports of the target AE: Reporting Odds Ratio (ROR) and Information Component (IC). Both methods were applied to each combination of the target drug (upadacitinib) and target AE (VTE) to identify potential safety signals. The ROR was calculated with a 95% confidence interval (95% CI), and a signal was considered statistically significant when the lower bound of the 95% CI exceeded 1, indicating a higher-than-expected reporting rate of VTE associated with upadacitinib relative to the comparator drugs. Based on a Bayesian statistical approach, the IC was also calculated with a 95% CI, and a signal was considered statistically significant when the lower bound of the CI 95% exceeded 0. Given that ROR is widely used but sensitive to sample size variations, potentially leading to false positives with low report counts, IC was used as a complementary approach to adjust for background reporting rates and reduce spurious associations (Supplementary Tables 1, 2).
To investigate potential patterns and predictors of disproportionality, subgroup analyses were conducted across several predefined categories (e.g., MedDRA PT, sex, age group, year of report, RA indication, Supplementary Table 3, and number of co-medicated drugs). These analyses aimed to characterize how the disproportionality of VTE reporting associated with upadacitinib may vary across relevant patient or reporting characteristics, which may represent potential confounding factors related to VTE occurrence and help discuss possible false-positive and false-negative findings.
This study was conducted using anonymized ICSRs from a spontaneous reporting database, and therefore, ethical approval and patient consent were not required. All analyses complied with international pharmacovigilance and pharmacoepidemiology standards, including those outlined by the WHO and the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) Guide on Methodological Standards in Pharmacoepidemiology (22). The study followed the REporting of A Disproportionality Analysis for DrUg Safety Signal Detection Using Individual Case Safety Reports in PharmacoVigilance (READUS-PV) guideline, ensuring methodological rigor in safety signal detection and adherence to pharmacovigilance best practices (23).
All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria). Disproportionality analysis was implemented using the function “da” of the “pvda” package.1
Results
Descriptive analysis
At the time of extraction, VigiBase included a total of 41,285,626 ICSRs, of which 552,319 (1.34%) were associated with at least one second-line therapy agent for RA under study. Among these, 228,997 ICSRs (41%) involved at least one JAKi, whether or not it included upadacitinib. Specifically, 62,257 ICSRs (27% of JAKi-related reports) identified upadacitinib as a suspected or interacting drug. Most cases involving upadacitinib were reported in 2023 (24,139; 39%), showing a temporal distribution similar to that of JAKi-related ICSRs and ICSRs involving any second-line therapy anti-RA drug (Figure 1 and Table 1).
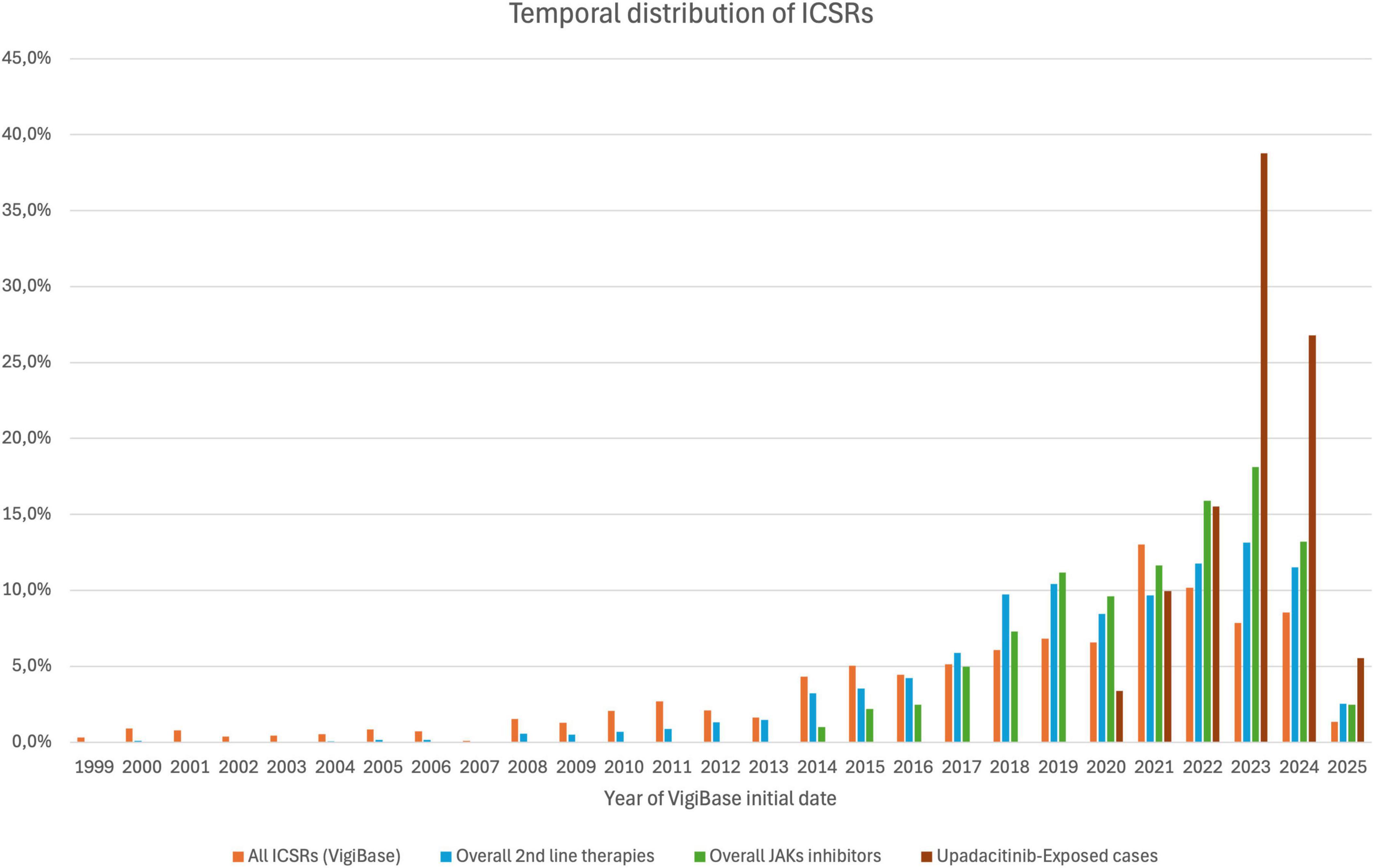
Figure 1. Temporal distribution of Individual Case Safety Reports (ICSRs) across different drug categories in VigiBase from 1999 to 2025. Each bar represents the proportion of ICSRs per year involving: any drug in VigiBase (orange), second-line therapies for rheumatoid arthritis (blue), JAK inhibitors (green), and upadacitinib (brown). Reports include any type of adverse event. Reporting begins later for drug classes authorized after 1999.
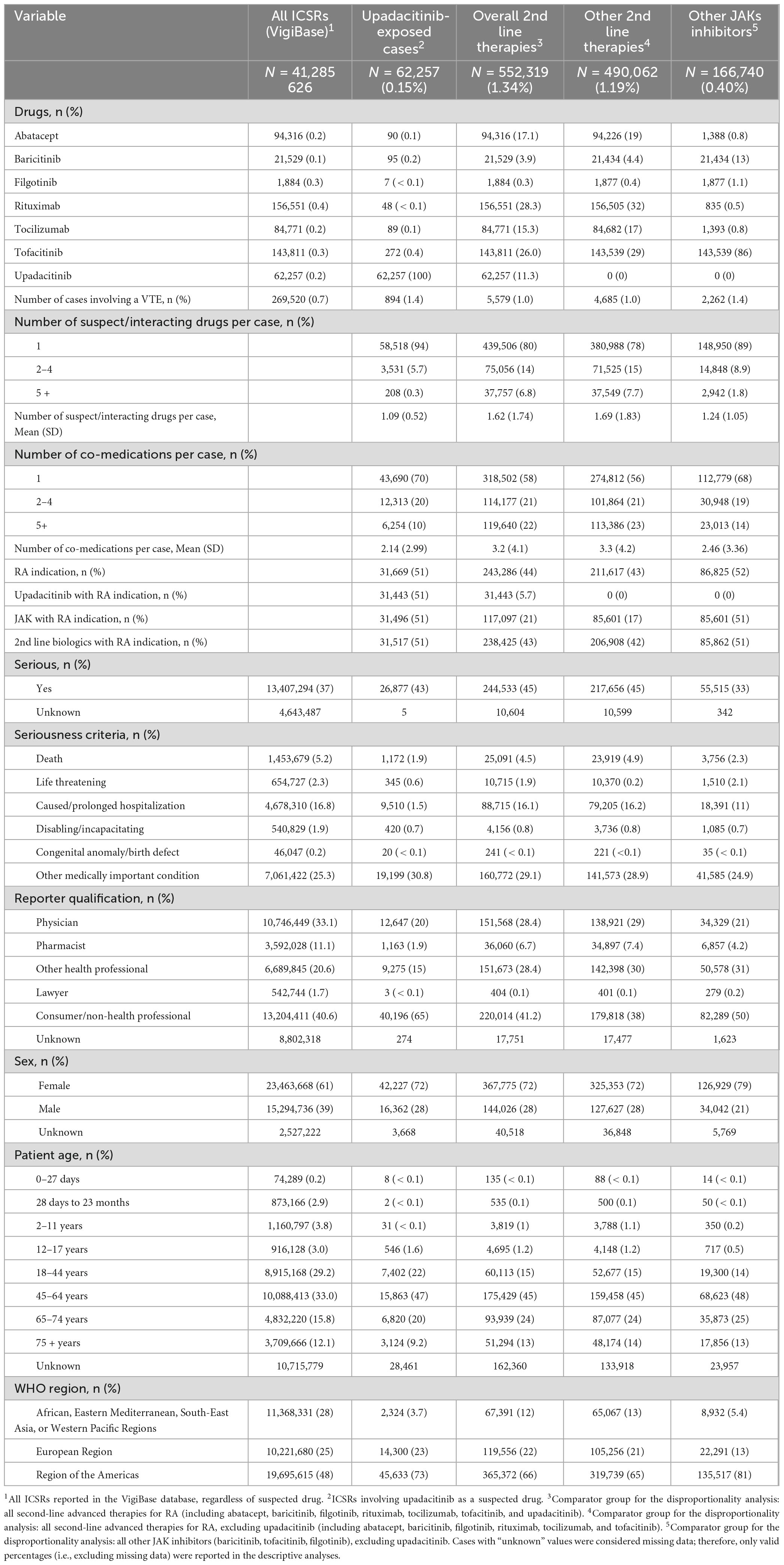
Table 1. Characteristics of individual case safety reports (ICSRs) recorded in VigiBase, grouped by upadacitinib exposure and comparator groups.
We identified 894 ICSRs in VigiBase in which upadacitinib was associated with a VTE, corresponding to 1.4% of ICSRs where upadacitinib was a suspected or interacting drug (exposed cases). This represents a similar prevalence of VTEs when compared with other JAKi-related ICSRs (2,262; 1.4%) but larger relative to other second-line therapies (4,684; 1.0%) and any other drugs (268,626; 0.7%).
Among alternative second-line therapies for RA management, the most reported in VigiBase were rituximab (156,505; 32%), tofacitinib (143,539; 29%), abatacept (94,226; 19%) and tocilizumab (84,682; 17%). Tofacitinib (143 539; 86%) was the most common JAKi reported among non-exposed cases within JAKi-related ICSRs. Most ICSRs documented only one suspected/interacting drug, regardless of the sample of cases considered. However, non-exposed groups tended to have a higher number of drugs per report. Just over half of the JAKi cases reported upadacitinib for a RA indication (upadacitinib: 31,443; 51%; other JAKi: 85,601; 51%), whereas the proportion of cases reporting other second-line therapies for an RA indication was lower (206,908; 42%). Upadacitinib (26,877; 43%) and other therapies (217,656; 45%) ICSRs were more frequently classified as serious when compared to ICSRs associated with other JAKi (55,515; 33%). However, the proportion of deaths in upadacitinib-related ICSRs (1,172; 4.4%) was the lowest among all groups, compared to other JAKi (3,756; 6.8%) and other therapies (23,919; 11%). This was also below the overall death proportion reported in VigiBase (1,453,679; 5.2%).
Most AE suspected to be related to a JAKi were reported by consumers or non-health professionals (upadacitinib: 40,196; 65%, other JAKi: 82,289; 50%). In contrast, reports associated with other second-line therapies were more evenly distributed, with physicians (138,921; 29%) and other health professionals (142,398; 30%) contributing substantially, indicating that reporting was not concentrated among consumers in these cases.
Compared to the overall ICSR dataset at VigiBase, reports involving a suspected or interacting second-line therapies for RA, whether a JAKi or not, were more frequently observed in women and patients aged over 44 years. While most ICSRs originated from the Region of the Americas (48%), a disproportionate number of reports involving upadacitinib (73%) came from this region.
Disproportionality analysis
Upadacitinib was associated with a disproportionately higher reporting of VTE compared to all drugs in VigiBase (IC: 1.14 [1.04, 1.23]; ROR: 2.22 [2.08, 2.37]), as well as when explicitly compared to other second-line therapies used for RA (IC: 0.51 [0.41, 0.60]; ROR: 1.51 [1.40, 1.62]). However, when compared to other JAKi, upadacitinib demonstrates an overall comparable VTE risk (IC: 0.06 [−0.04, 0.15]; ROR: 1.06 [0.98, 1.15]). Notably, it is associated with significantly fewer VTE reports than baricitinib (IC: −0.60 [−0.69, −0.51]; ROR: 0.32 [0.29, 0.35]), but substantially more than tofacitinib (IC: 0.43 [0.34, 0.53]; ROR: 1.60 [1.47, 1.74]) (Table 2).
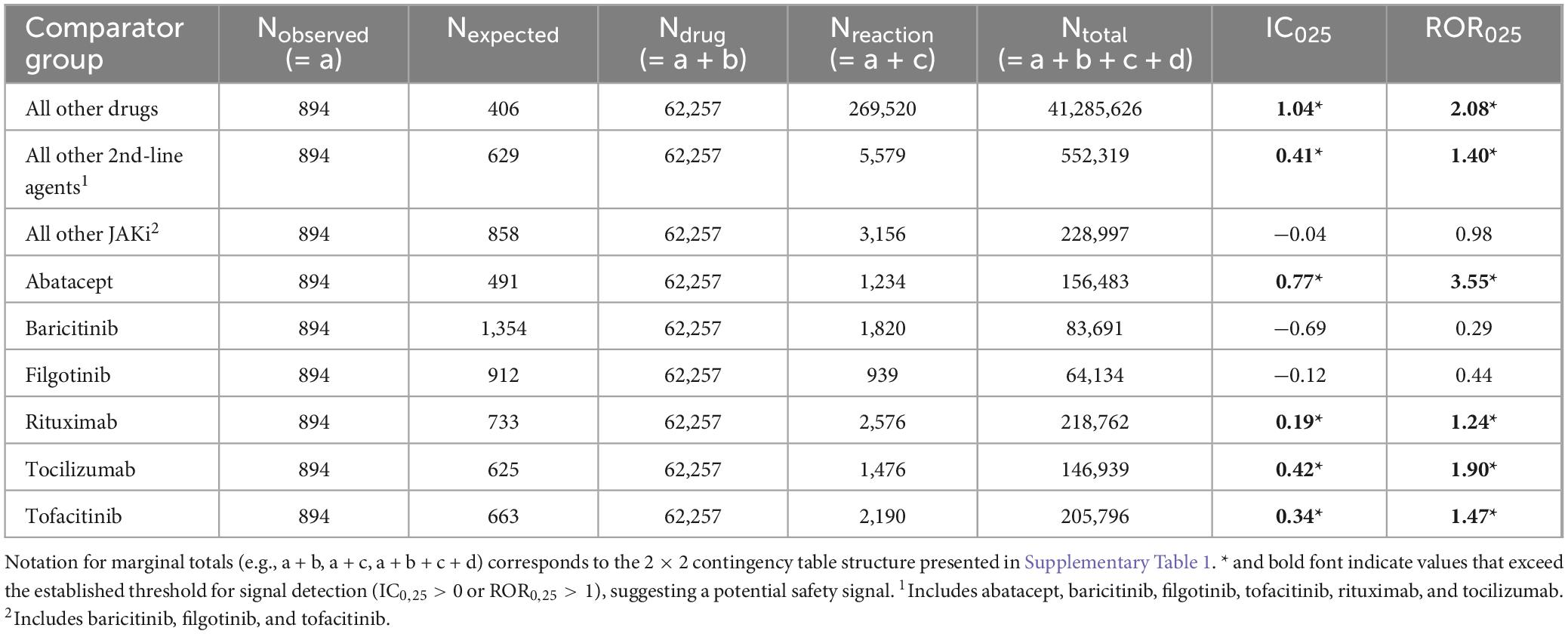
Table 2. Disproportionality analysis of venous thromboembolism (VTE) associated with upadacitinib, comparing it to different drug groups using reporting odds ratio (ROR) and information component (IC).
Analysis by reaction
Despite an overall disproportionately higher reporting of VTE compared to other second-line therapies, this pattern varied when specific AE were considered (Figure 2A). Among the most reported PT terms (i.e., Pulmonary thrombosis, Pulmonary embolism, Deep vein thrombosis), upadacitinib showed an increased risk of pulmonary embolism (n = 420, IC: 0.4 [0.25, 0.53]; ROR: 1.37 [1.24, 1.52]) and pulmonary thrombosis (n = 160, IC: 1.62 [1.38, 1.83]; ROR: 4.21 [3.47, 5.10]), but no significantly different risk associated with deep vein thrombosis (DVT) (n = 219, IC: 0.03 [−0.16, 0.22]; ROR: 1.03 [0.89, 1.18]). Against other JAKi, upadacitinib was significantly less reported as being associated with deep vein thrombosis (IC: −0.37 [-0.57, −0.18]; ROR: 0.71 [0.61, 0.83]) and borderline significantly less pulmonary embolism (IC: −0.13 [−0.27, 0]; ROR: 0.88 [0.78, 0.99]), yet remained disproportionately more associated with pulmonary thrombosis (IC: 0.82 [0.59, 1.03]; ROR: 2.48 [2.00, 3.08]) (Figure 2B).
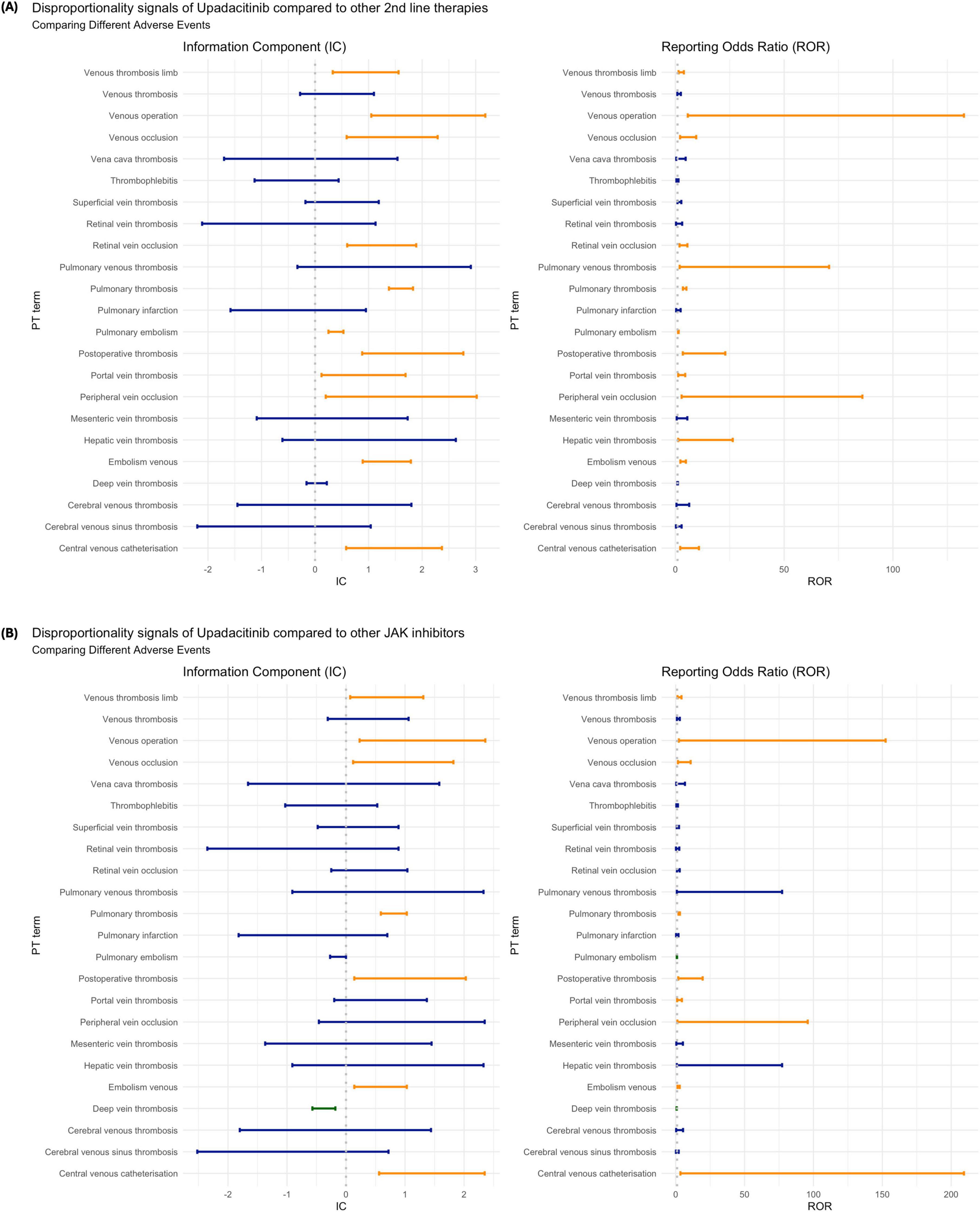
Figure 2. Disproportionality analysis of venous thromboembolism (VTE) associated with upadacitinib by Preferred Term (PT): (A) compared to other second-line therapies for rheumatoid arthritis; and (B) compared to other JAK inhibitors. Estimates are shown using the Information Component (IC) and Reporting Odds Ratio (ROR), each with 95% confidence intervals. Orange bars indicate statistically significant signals (IC0,25 > 0 or ROR0,25 > 1); blue bars indicate non-significant findings; green bars indicate inverse disproportionality (lower-than-expected reporting).
Disproportionate signal analysis by other variables of interest
Our results indicate no significant differences in VTE reporting trends across genders, regardless of the drug comparator group. Similarly, no notable variation was observed across age groups when upadacitinib was compared to other second-line therapies (Figure 3A). However, compared to other JAKi, nearly all age groups exhibited a disproportionately higher reporting of VTE associated with upadacitinib, contrasting with the overall findings that suggested no distinct safety profile. The only exception was among patients aged 18–44 years, for whom the reporting of upadacitinib-associated VTE did not reach statistical significance (IC: 0.27 [–0.02, 0.54]; ROR: 1.32 [1.04, 1.68]) (Figure 3B).
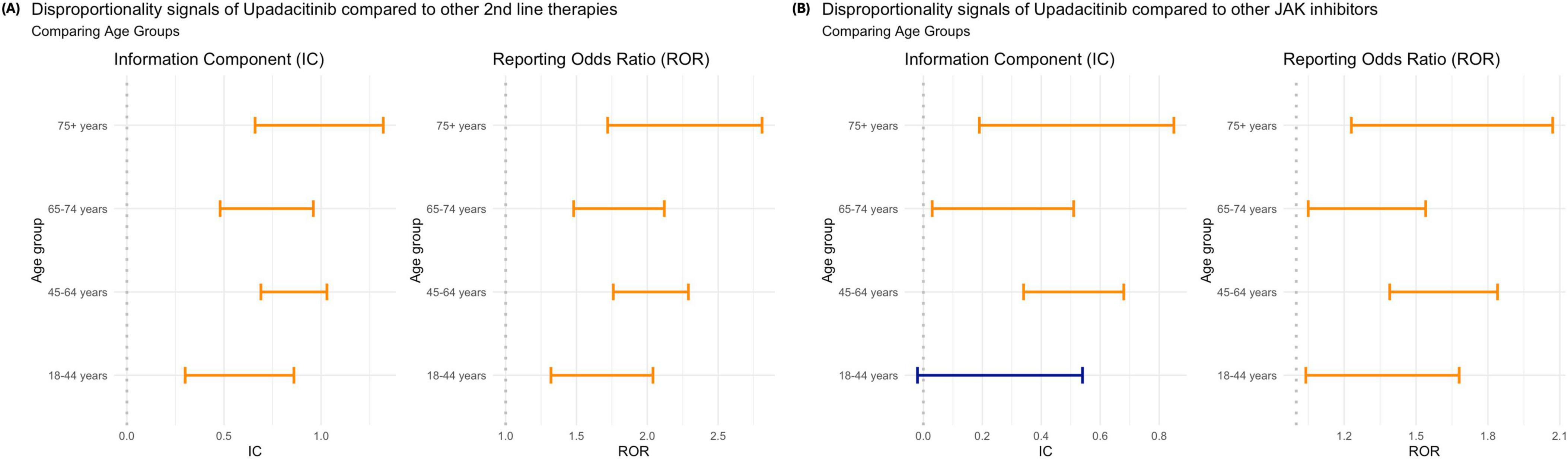
Figure 3. Disproportionality analysis of venous thromboembolism (VTE) associated with upadacitinib by age group: (A) compared to other second-line therapies for rheumatoid arthritis; and (B) compared to other JAK inhibitors. Estimates are shown using the Information Component (IC) and Reporting Odds Ratio (ROR), each with 95% confidence intervals. Orange bars indicate statistically significant signals (IC0,25 > 0 or ROR0,25 > 1; blue bars indicate non-significant findings.
In 2023, upadacitinib demonstrated a more favorable reporting pattern compared to other years. During this period, it was not associated with a significantly increased risk of VTE relative to other second-line therapies (IC: 0.05 [–0.14, 0.23]; ROR: 1.05 [0.90, 1.23]). Furthermore, it showed a significantly lower disproportionality in VTE reporting compared to other JAKi (IC: –0.38 [–0.58, –0.21]; ROR: 0.57 [0.48, 0.68]). In all other years, the safety profile of upadacitinib remained consistent with the overall findings observed across the entire study period (Figure 4).
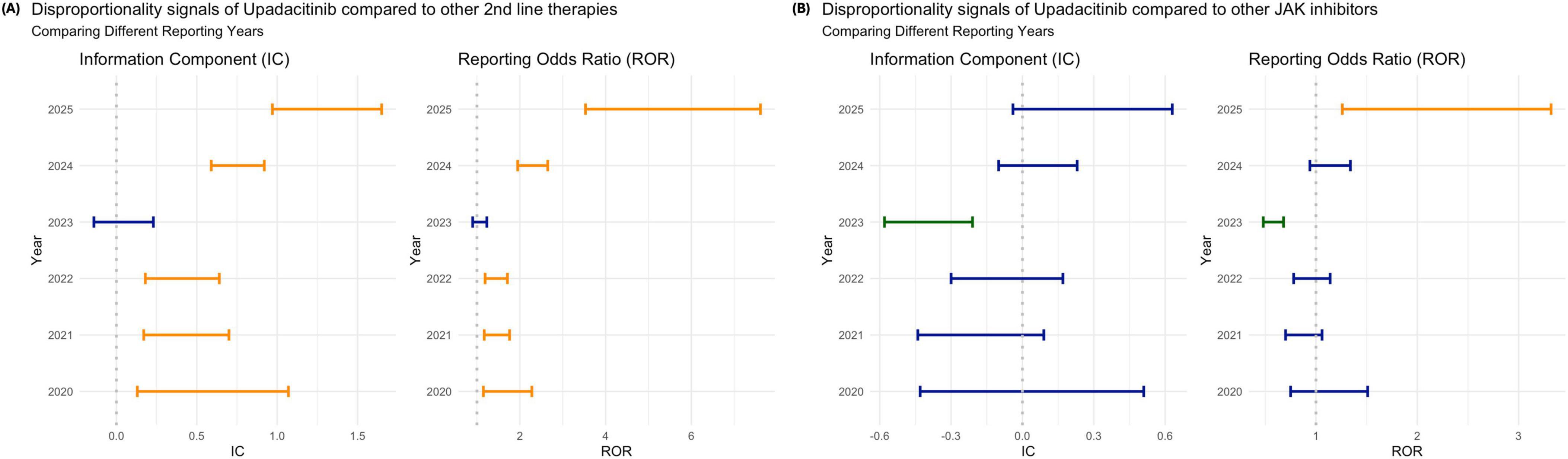
Figure 4. Disproportionality analysis of venous thromboembolism (VTE) associated with upadacitinib by reporting year: (A) compared to other second-line therapies for rheumatoid arthritis; and (B) compared to other JAK inhibitors. Estimates are shown using the Information Component (IC) and Reporting Odds Ratio (ROR), each with 95% confidence intervals. Orange bars indicate statistically significant signals (IC0,25 > 0 or ROR0,25 > 1; blue bars indicate non-significant findings; green bars indicate inverse disproportionality (lower-than-expected reporting).
When stratified by sex, the disproportionality analysis showed that, compared to other second-line therapies, upadacitinib was consistently associated with higher reporting of VTE in both male and female patients, with statistically significant disproportionality signals observed for men (IC: 0.50 [0.39, 0.60]; ROR: 1.54 [1.42, 1.68]) and women (IC: 0.55 [0.44, 0.65]; ROR: 1.50 [1.39, 1.63]) (Figure 5A). In contrast, when compared to other JAKi, no significant variation was observed between sexes, with both IC and ROR values close to the null (Figure 5B).
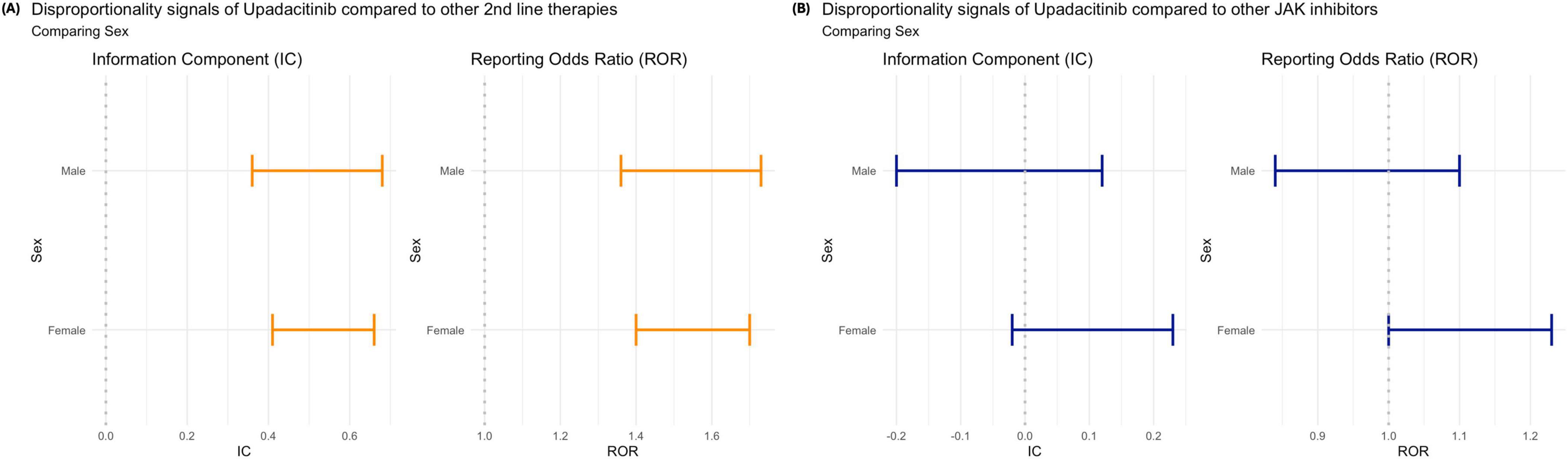
Figure 5. Disproportionality analysis of venous thromboembolism (VTE) associated with upadacitinib by patient sex: (A) compared to other second-line therapies for rheumatoid arthritis; and (B) compared to other JAK inhibitors. Estimates are shown using the Information Component (IC) and Reporting Odds Ratio (ROR), each with 95% confidence intervals. Orange bars indicate statistically significant signals (IC0,25 > 0 or ROR0,25 > 1; blue bars indicate non-significant findings.
Subgroup analysis by the number of suspected or interacting drugs reinforced the disproportional signal of VTE occurrence associated with upadacitinib compared with other second-line therapies, as cases involving a single suspected or interacting drug remained statistically significant. When restricting the analysis to JAKi or other second-line therapies reported for an RA indication, the results were consistent with the overall findings: upadacitinib was associated with a disproportionately higher reporting of VTE compared with other second-line therapies, whereas, when compared with other JAKi, upadacitinib showed a comparable VTE reporting pattern (Supplementary Figures 1, 2).
Discussion
To our knowledge, this is the first study to evaluate the global safety profile of upadacitinib in relation to VTE, using worldwide spontaneous ARD reports data from VigiBase, without temporal restrictions, through a structured multi-level disproportionality analysis of ICSR data to ensure comprehensive signal detection. The results indicate that upadacitinib is associated with a higher-than-expected reporting of VTE compared not only to all other drugs in VigiBase but also to other second-line therapies commonly used for RA, among which rituximab and tocilizumab showed a comparatively safer profile. Within the JAKi class, while the overall reporting pattern for upadacitinib was similar to other JAK inhibitors as a group, notable differences emerged at the individual drug level: upadacitinib was associated with fewer VTE reports than baricitinib but more than tofacitinib.
Importantly, the first-level comparison against all other medicines should be interpreted strictly as a global signal-screening step with limited clinical interpretability. Patients receiving upadacitinib typically have systemic inflammatory diseases with intrinsically elevated VTE risk – meta-analyses estimate ∼1.5–2.0-fold higher VTE risk in RA and ∼2–3-fold in IBD versus the general population – so indication-related confounding is expected at this level (24–26). Consistent with regulatory practices, disproportionality screening is an accepted first step in routine signal management but remains hypothesis-generating and requires contextualization with more specific comparators (27). Our second- and third-level analyses (advanced RA therapies and other JAKi) were designed precisely to mitigate this limitation and provide findings of greater clinical relevance. Notably, when the analysis was restricted to reports explicitly referring to RA, the results remained consistent with the overall findings, reinforcing the robustness of the observed disproportionality signal.
Mechanistically, Janus kinase/signal transducers and activators of transcription (JAK/STAT) signaling is intertwined with pathways of coagulation and immune-driven thrombosis. The JAK/STAT pathway plays a role in platelet production and activation, linking it to thrombosis pathophysiology (28). Inhibiting JAKs can simultaneously affect multiple cytokine networks—some that normally promote clot formation and others that protect against it. For example, blocking certain JAK-dependent cytokines that have anti-inflammatory and anti-thrombotic effects (such as IL-10 or type I interferons) might remove a protective brake on thrombosis, even if the drug also suppresses pro-thrombotic inflammatory signals (29). It has been hypothesized that selectively inhibiting one JAK isoform may upset the balance between pro- and anti-thrombotic signaling cascades, which could contribute to a prothrombotic tendency in susceptible patients (29). However, the precise biological mechanism by which JAKi might promote VTE remains uncertain, underscoring the need for further mechanistic studies (30). Understanding these drug-specific effects on coagulation pathways will be important to clarify why thrombotic events occur in some JAKi-treated patients and whether certain agents in this class carry lower thrombotic risk than others.
Notably, among biologics, rituximab and tocilizumab showed a comparatively safer VTE reporting profile, aligning with evidence that TNFα or IL-6 inhibitors may carry lower thrombotic risk (31). Within the JAK inhibitor class, upadacitinib’s overall reporting pattern was similar to the class as a whole, but important differences emerged at the individual drug level. Upadacitinib was associated with fewer VTE reports than baricitinib but more than tofacitinib, in line with recent pharmacovigilance analyses showing VTE, stroke, and ischemic heart disease events were more frequently reported with upadacitinib and baricitinib than with tofacitinib (32). This heterogeneity underscores that JAKi should not be viewed as a homogeneous group in terms of safety profile. Differences in JAK selectivity may partly explain the observed VTE reporting patterns. Baricitinib inhibits JAK1 and JAK2 and is uniquely associated with transient increases in platelet counts, possibly through JAK2-mediated thrombopoietin signaling, which could theoretically elevate thrombotic risk. In contrast, tofacitinib (JAK1/3) and upadacitinib (JAK1-selective) are generally associated with reductions in platelet counts (33, 34). Our data align with previous findings, indicating fewer VTE reports for upadacitinib than for baricitinib, but more than for tofacitinib. These differences highlight that JAK inhibitors should not be considered a homogeneous class when evaluating benefit–risk profiles. Despite its more selective mechanism, the disproportionality signal observed for upadacitinib suggests that its VTE risk cannot be disregarded. While this does not establish causality (35), it reinforces the need for ongoing monitoring and further investigation.
Another noteworthy observation was that upadacitinib-related VTE cases showed a lower proportion of fatal outcomes compared with other JAK inhibitors and second-line therapies. While this finding should be interpreted cautiously, several explanations may be considered. Differences in baseline patient characteristics, such as younger age or fewer comorbidities among upadacitinib users, could partly account for this pattern, as younger populations generally present lower VTE-related mortality risk. For instance, in a large Swedish cohort, patients with VTE and no comorbidities (Charlson Comorbidity Index = 0) had < 1% mortality at 3 months, whereas those with multimorbidity clusters (e.g., cardiometabolic or digestive diseases) showed markedly elevated VTE risks (adjusted ORs 3.44 and 4.35, respectively) (36). Previous pharmacovigilance data further support this interpretation: fatal ADRs represent just over 1% of all global reports, although not specific to VTE, and are disproportionately concentrated among older patients with comorbidities (37). Importantly, VTE-specific data indicate that case fatality differs substantially by event type, with 30-day mortality rates around 7–11% for pulmonary embolism compared with < 3% for isolated DVT (38, 39). These differences suggest that both patient characteristics and the relative distribution of PE versus DVT events may influence the observed lower fatality proportion in upadacitinib-related reports. Although causality cannot be established, this signal warrants further investigation in large, controlled real-world studies with adjustment for baseline thrombotic risk factors.
Therapeutic decision-making might be influenced in patients with a higher baseline VTE risk, such as those with a history of thrombosis, obesity, certain comorbidities, female sex, or prolonged immobility, by favoring treatments with a more favorable thrombotic profile when possible (31). Differences in AE reporting across disease states may also play a role. Upadacitinib is approved for multiple immune-mediated inflammatory conditions, including RA, axial spondyloarthritis (both radiographic and non-radiographic forms), psoriatic arthritis, giant cell arteritis, atopic dermatitis, and, more recently, inflammatory bowel disease (40–42). These indications differ in baseline thrombotic risk and patient profiles. For example, RA confers a twofold increased VTE risk compared to the general population, and active IBD is associated with an even higher risk (43). Such factors may influence reporting patterns and should be considered when interpreting upadacitinib’s safety signals. Furthermore, our subgroup findings indicate that stronger disproportionality signals were observed in cases with multiple concomitant drugs, suggesting that polypharmacy or combined immunosuppressive therapy—common in RA treatment—may contribute to the increased thrombotic risk reported with upadacitinib. This observation reinforces that the present data predominantly reflect RA treatment contexts, where co-administration of methotrexate, corticosteroids, or biologics is frequent. In contrast, in dermatological indications such as atopic dermatitis or alopecia areata, where JAK inhibitors are typically used as monotherapy and concomitant systemic immunosuppression is not allowed, the observed VTE disproportionality should not be directly extrapolated (13). These differences in therapeutic context and baseline thrombotic risk warrant careful consideration when generalizing safety signals across indications.
Interestingly, when upadacitinib was compared to the JAK inhibitor class overall (treating all JAKi as a single group), no significant disproportionality signal for VTE was detected in our analysis. However, as noted above, relevant differences emerged when comparing individual drugs, highlighting that the JAK inhibitor class is not monolithic in its risk profile. These findings reinforce that clinicians should avoid treating the JAKi group as homogeneous in clinical decision-making and instead consider the safety nuances of each agent. Consistent with this, regulators have extended findings from the ORAL Surveillance trial, which showed increased rates of serious cardiovascular events and VTE with tofacitinib in high-risk RA patients, to the entire JAK inhibitor class (14). Those results prompted the FDA and EMA to extend class-wide warnings to other JAKi, including upadacitinib, even though direct comparative evidence for the newer agents remains limited (44, 45). In fact, the FDA in 2021 required updated boxed warnings for upadacitinib and baricitinib, considering that they share mechanisms with tofacitinib and “may have similar risks,” and now recommends using JAKi only in patients who have an inadequate response to TNF blockers, with careful consideration of individual risk factors.
Real-world evidence on upadacitinib’s thromboembolic risk is still emerging. Several recent studies have investigated the link between JAKi and VTE risk. For example, a large multi-database study across 14 data sources in the USA, Europe, and Japan (post-marketing surveillance) showed a significantly elevated VTE incidence for baricitinib compared to TNF inhibitors (incidence rate ratio ≈1.51, 95% CI 1.10–2.08) (46). Data for upadacitinib in such studies remain scarce, as it is a newer agent, but so far, it has not demonstrated a clear signal in those settings. Notably, a French nationwide cohort study of RA patients initiating JAKi (primarily tofacitinib or baricitinib) versus adalimumab found no statistically significant increase in VTE risk (HR≈1.1, 95% CI 0.7–1.6), including among older patients with cardiovascular risk factors, providing some reassurance (47). However, VTE events are relatively rare, and such observational studies may lack power or have confounding by indication (as patients on JAKi might have had more severe disease activity, which itself heightens thrombotic risk). Therefore, the absence of a signal in some studies should be interpreted with caution. On balance, our disproportionality findings together with existing evidence suggest that the potential VTE risk with upadacitinib (and JAKi in general) should not be overlooked, especially in vulnerable populations, even as more data are needed for definitive conclusions.
When stratified by age, upadacitinib was associated with a significantly higher disproportionality signal for VTE across all age groups when compared to other JAKi, except in the cohort aged 18–44 years, where the signal was borderline. In contrast, this age-related pattern was not observed when comparing upadacitinib to non-JAKi therapies, suggesting that age-related variations in thrombotic risk may be more pertinent within the JAKi. These observations resonate with clinical insights from the literature (14–16). Rajasimhan et al. (48) noted that patients over 50 years of age—especially those with prior VTE or cardiovascular risk factors—are at higher risk of thromboembolic events under JAKi therapy. This aligns with safety warnings highlighting increased risk in this age group. Notably, the EMA recommends that tofacitinib should only be used in patients aged over 65 years when no suitable alternatives are available. Similarly, the ORAL Surveillance trial identified age as a key risk modifier, with those over 65 experiencing higher rates of major adverse cardiovascular events and VTE on tofacitinib (14). Consistent with this, regulatory authorities have issued specific warnings for older patients. Both the FDA and EMA now caution that JAKi should be used with particular care in individuals over 65 or those with other cardiovascular or malignancy risk factors, and recommend that such patients be treated with JAKi only if no suitable alternatives are available (44, 45). With the aging of society and the increasing number of elderly patients with chronic inflammatory diseases who may be candidates for JAKi, these findings are highly relevant. Elderly patients are inherently at increased risk for thrombosis (including DVT and pulmonary embolism) (49), as well as infections such as sepsis (50) and herpes zoster due to age-related frailty and comorbidities (51). Our results reinforce that upadacitinib (like other JAKi) should be used with great caution in older patients, especially during prolonged treatments. In practice, this means prescribers should thoroughly screen for cardiovascular and thrombotic risk factors and perform risk stratification before initiating a JAKi. Patients with multiple risk factors might be better managed with alternative therapies when possible (52). Taken together with existing evidence, these pharmacovigilance findings provide additional insights to help prescribers make informed treatment decisions for patients with an elevated baseline risk of thromboembolic events. In such cases, choosing a JAKi with a more favorable VTE risk–benefit profile, or considering a non-JAK therapy, may be advisable.
We also observed that reports involving the use of these agents are more frequent in women than in men. This discrepancy may be related to the epidemiology of the disease as well as to clinical and social factors. RA exhibits a markedly higher prevalence in women, with an estimated female-to-male ratio of approximately 3:1. Consequently, a greater proportion of women receive advanced therapies, including biologic agents, which is reflected in the higher number of associated safety reports (53, 54). Women present immunological particularities, more X chromosomes and differences in the hormonal influence on the immune system, which not only affect susceptibility to disease but also the response to biological treatments (53, 55). Our stratified analyses by event type and time yielded additional insights. DVT was less frequently associated with upadacitinib compared to other JAKi, whereas pulmonary embolism (or “pulmonary thrombosis”) showed a relatively higher reporting frequency with upadacitinib. In fact, among the most commonly reported specific VTE event terms for upadacitinib, pulmonary embolism signals were prominent and had narrower confidence intervals, suggesting a more robust signal. The reason for this disproportionality in event types is not entirely clear. One possibility is that pulmonary emboli, being acute and clinically serious events, are more likely to be recognized and reported in the context of a newer drug like upadacitinib, whereas milder DVT events might be underreported or not immediately linked to the drug. It is notable that in the ORAL Surveillance trial and other analyses, the excess risk observed with JAKi was largely driven by pulmonary embolism events (14). High-dose tofacitinib, for example, was associated with a dose-dependent increase in pulmonary embolism risk (up to sixfold at 10 mg BID) compared to TNF blockers, even though differences in simple DVT were less pronounced (31). A plausible explanation is that JAKi may precipitate central or severe thrombotic events such as pulmonary embolism in susceptible patients, possibly through complex interactions between systemic inflammation, endothelial dysfunction, and coagulation pathways that are modulated by JAK-STAT signaling. Inflammation itself is a recognized risk factor for thrombosis in RA, and JAKi, while reducing pro-inflammatory cytokines, may also interfere with protective cytokines that regulate vascular homeostasis, potentially shifting the hemostatic balance toward thrombosis in certain contexts (56). However, the precise biological mechanisms underlying this potential prothrombotic tendency remain uncertain, warranting further mechanistic and clinical investigation. Meanwhile, clinicians should remain vigilant for early signs of pulmonary embolism (e.g., acute dyspnea, pleuritic chest pain, unexplained tachycardia) in patients receiving upadacitinib, given the importance of prompt detection and intervention in improving outcomes.
Additionally, we also observed that in 2023, upadacitinib showed a more favorable disproportionality profile (i.e., a lower reporting ratio for VTE) compared to other JAKi, coinciding with the highest volume of upadacitinib-related reports. This trend could reflect broader use of upadacitinib across indications and regions, as well as shifts in reporting patterns. Upadacitinib’s usage expanded significantly in 2022–2023, with approvals for atopic dermatitis and Crohn’s disease, leading to a large increase in the number of treated patients and ICSRs submitted (35). These new indications also change the user population, introducing patients with different baseline VTE risks, which may contribute to the observed signal attenuation. As upadacitinib’s patient exposure has grown, AE may now represent a smaller share of total reports, diluting disproportionality signals. Additionally, post-2021 prescribing became more selective, with JAKi increasingly avoided in high VTE-risk patients, possibly lowering VTE incidence in 2023 compared to earlier periods or to drugs like baricitinib. Given that the therapeutic indication is often missing in ICSRs, future studies, including time-series analyses aligned with approval dates for new indications, could help clarify evolving safety patterns. Continued monitoring will be needed to determine if this favorable trend for upadacitinib persists with broader use.
Overall, our findings underscore the need for further targeted research to clarify the VTE risk associated with upadacitinib and other JAKi. Large-scale real-world cohort or active surveillance studies with appropriate comparators and baseline risk adjustment are warranted to quantify absolute and relative VTE risks. For instance, a multi-database study found that baricitinib users had a ∼50% higher incidence of VTE compared to TNF inhibitors (IRR = 1.51; 95% CI 1.10–2.08) (31), while systematic reviews of RCTs report an increased odds of VTE with JAKi, reaching OR2.17 (95% CI 1.16–4.05) in analyses restricted to trials with ≥ 12 months follow-up (30). It remains uncertain whether the observed signals are driven primarily by pharmacologic effects – given that JAKi can interfere with platelet activation and endothelial function – or by patient characteristics such as age, comorbid cardiovascular risks, and disease activity, or a combination of both (57).
Limitations
The present study has several limitations that should be considered when interpreting the findings. Using VigiBase, a spontaneous reporting system, precludes the estimation of the true incidence or prevalence of VTE among patients exposed to upadacitinib and other JAKi, as underreporting, differential reporting by country and healthcare setting, and potential stimulated reporting following regulatory alerts or media coverage can introduce bias and affect signal detection sensitivity (58). Disproportionality analysis is a well-established tool for early signal detection, but it is inherently hypothesis-generating and can never serve as a confirmatory method. Its results cannot establish causality and are limited by the quality and completeness of ICSRs, which often lack detailed data on disease severity, indication, treatment duration, dosage, baseline thrombotic risk factors, patient comorbidities, and concomitant medications such as corticosteroids or NSAIDs, all of which may modulate VTE risk (59). The timing of VTE occurrence relative to drug initiation is frequently missing, complicating temporal association assessments. In addition, we could not stratify our analysis by therapeutic indication (e.g., RA, atopic dermatitis, Crohn’s disease), despite evidence that underlying disease activity and inflammation may influence thrombotic risk profiles across conditions for which upadacitinib is prescribed. This limitation results from the frequent absence of therapeutic indication in ICSRs within VigiBase, which prevented reliable allocation of cases to specific clinical contexts. Consequently, our findings may be subject to indication bias, as patients receiving upadacitinib for different conditions may present heterogeneous baseline risks for VTE. We explicitly acknowledge this and emphasize that our multilevel comparator design (including RA-specific comparators) was intended to mitigate, though not completely eliminate, this potential source of bias. Differences in healthcare systems, pharmacovigilance infrastructure, and prescribing practices across the over 140 countries contributing to VigiBase can also affect reporting patterns, and while our analysis included all available data without temporal restrictions to maximize sensitivity, changes in prescribing patterns and regulatory risk minimization measures in recent years, such as the 2022 EMA recommendations for JAKi, may have influenced reporting rates over time, potentially attenuating disproportionality signals. Additionally, the comparator groups used (all drugs, second-line therapies for RA, and other JAKi) provided a multi-level perspective but residual confounding is likely, as we could not adjust for baseline thrombotic risk factors and comorbidities, which may differ between treatment groups and substantially influence VTE risk. This limitation restricts causal inference, and our results should be interpreted strictly as hypothesis-generating signals rather than evidence of a definitive causal relationship. Despite these limitations, the use of VigiBase enables global, real-world monitoring of rare but serious AE such as VTE across diverse populations, supporting pharmacovigilance efforts and generating hypotheses for targeted active surveillance and comparative cohort studies that can better delineate the absolute and relative risks associated with upadacitinib and other JAKi to guide safer and personalized prescribing strategies.
Conclusion
This global real-world pharmacovigilance study provides important insight into the safety profile of upadacitinib, particularly its potential association with thromboembolic events, and highlights nuances within the JAKi class that are relevant for clinical decision-making. These findings, together with prior evidence, may assist prescribers in stratifying thromboembolic risk and selecting appropriate treatment for patients with RA and other immune-mediated conditions, balancing effectiveness with individual safety considerations. Future research should prioritize robust, long-term comparative pharmacoepidemiological studies using real-world cohorts to better clarify absolute and relative risks, establish causal relationships, and inform the development of practical risk stratification tools for clinical use. Ongoing pharmacovigilance will remain crucial to optimize the safe use of JAKi and to support evidence-informed, individualized treatment decisions that adapt to emerging safety data.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: VigiBase.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
RF-d-S: Formal analysis, Writing – original draft, Software, Visualization, Resources, Conceptualization, Project administration, Data curation, Methodology, Writing – review & editing, Supervision, Validation, Investigation. ML: Writing – original draft, Data curation, Writing – review & editing, Methodology, Conceptualization, Software, Formal analysis. AA: Writing – original draft, Visualization, Validation, Investigation, Writing – review & editing. JP-M: Writing – original draft, Validation, Visualization, Investigation, Writing – review & editing. BM: Writing – original draft, Investigation, Writing – review & editing, Visualization, Validation. CR: Writing – original draft, Visualization, Validation, Investigation, Writing – review & editing. IL: Writing – original draft, Visualization, Investigation, Validation, Writing – review & editing. IV: Validation, Writing – review & editing, Writing – original draft, Visualization, Investigation. JP: Writing – original draft, Visualization, Investigation, Writing – review & editing, Validation. LG: Writing – original draft, Investigation, Visualization, Validation, Writing – review & editing. LS: Validation, Writing – review & editing, Writing – original draft, Investigation, Visualization. MM: Writing – review & editing, Investigation, Visualization, Writing – original draft, Validation. MPi: Visualization, Writing – original draft, Validation, Investigation, Writing – review & editing. MF: Visualization, Validation, Writing – review & editing, Investigation, Writing – original draft. MPe: Writing – original draft, Visualization, Investigation, Validation, Writing – review & editing. NR: Writing – original draft, Visualization, Validation, Writing – review & editing, Investigation. TB: Validation, Visualization, Writing – original draft, Writing – review & editing, Investigation. IR: Investigation, Conceptualization, Validation, Methodology, Writing – review & editing, Supervision, Visualization, Writing – original draft.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by the project Sistema de VIGilância de Medicamentos e Dispositivos Médicos com Inteligência Artificial (VIGIA), co-funded by the European Union through the European Regional Development Fund (FEDER), under the Portugal 2030 Programme (COMPETE2030-FEDER-02045600).
Acknowledgments
We thank the WHO Collaborating Centre for International Drug Monitoring and the Uppsala Monitoring Centre for the development and maintenance of VigiBase, which enabled this research. The information does not represent the views of the WHO or UMC. The authors complied with all conditions of use of VigiBase data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1683751/full#supplementary-material
Footnotes
References
1. Schwartz DM, Bonelli M, Gadina M, O’Shea JJ. Type I/II cytokines, JAKs, and new strategies for treating autoimmune diseases. Nat Rev Rheumatol. (2016) 12:25–36. doi: 10.1038/nrrheum.2015.167
2. Tanaka Y, Luo Y, O’Shea JJ, Nakayamada S. Janus kinase-targeting therapies in rheumatology: a mechanisms-based approach. Nat Rev Rheumatol. (2022) 18:133–45. doi: 10.1038/s41584-021-00726-8
3. Burr NE, Gracie DJ, Black CJ, Ford AC. Efficacy of biological therapies and small molecules in moderate to severe ulcerative colitis: systematic review and network meta-analysis. Gut. (2022) doi: 10.1136/gutjnl-2021-326390. [Online ahead of print].
4. Burmester GR, Mysler E, Taylor PC, et al. POS0639 Benefit–risk analysis of upadacitinib versus adalimumab in patients with rheumatoid arthritis and higher or lower risk of cardiovascular disease. Ann Rheum Dis. (2024) 83:770–1. doi: 10.1136/annrheumdis-2024-eular.1416
5. U.S. Food and Drug Administration. Drug Trials Snapshots: Rinvoq [Internet]. Silver Spring, MD: FDA (2019).
7. Sepriano A, Kerschbaumer A, Bergstra SA, Smolen JS, van der Heijde D, Caporali R, et al. Safety of synthetic and biological DMARDs: a systematic literature review informing the 2022 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis. (2023) 82:107–18. doi: 10.1136/ard-2022-223357
8. Benjamin O, Goyal A, Lappin SL. Disease-Modifying Antirheumatic Drugs (DMARD). Treasure Island, FL: StatPearls Publishing (2023).
9. Mohamed MF, Bhatnagar S, Parmentier JM, Nakasato P, Wung P. Upadacitinib: mechanism of action, clinical, and translational science. Clin Transl Sci. (2024) 17:e13688. doi: 10.1111/cts.13688
10. Blockmans D, Penn SK, Setty AR, Schmidt WA, Rubbert-Roth A, Hauge EM, et al. A phase 3 trial of upadacitinib for giant-cell arteritis. N Engl J Med. (2025) 392:2013–24. doi: 10.1056/NEJMoa2413449
11. Dignass A, Esters P, Flauaus C. Upadacitinib in Crohn’s disease. Expert Opin Pharmacother. (2024) 25:359–70. doi: 10.1080/14656566.2024.2333964
12. U.S. Food and Drug Administration. FDA Approves First Oral Treatment for Moderately to Severely Active Crohn’s Disease [Internet]. Silver Spring, MD: FDA (2023).
13. Elmariah SB, Smith JS, Merola JF. JAK in the [Black] Box: a dermatology perspective on systemic JAK inhibitor safety. Am J Clin Dermatol. (2022) 23:427–31. doi: 10.1007/s40257-022-00701-3
14. Ytterberg SR, Bhatt DL, Mikuls TR, Koch GG, Fleischmann R, Rivas JL, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. (2022) 386:316–26. doi: 10.1056/NEJMoa2109927
15. Charles-Schoeman C, Fleischmann R, Mysler E, Greenwald M, Ytterberg SR, Koch GG, et al. Risk of venous thromboembolism with tofacitinib versus tumor necrosis factor inhibitors in cardiovascular risk-enriched rheumatoid arthritis patients. Arthritis Rheumatol. (2024) 76:1218–29. doi: 10.1002/art.42846
16. Gouverneur A, Avouac J, Prati C, Cracowski JL, Schaeverbeke T, Pariente A, et al. JAK inhibitors and risk of major cardiovascular events or venous thromboembolism: a self-controlled case series study. Eur J Clin Pharmacol. (2022) 78:1981–90. doi: 10.1007/s00228-022-03402-2
17. Wlassits R, Müller M, Fenzl KH, Lamprecht T, Erlacher L. JAK-. Inhibitors - a story of success and adverse events. Open Access Rheumatol. (2024) 16:43–53. doi: 10.2147/OARRR.S436637
18. Charles-Schoeman C, Choy E, McInnes IB, Mysler E, Nash P, Yamaoka K, et al. MACE and VTE across upadacitinib clinical trial programmes in rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis. RMD Open. (2023) 9:e003392. doi: 10.1136/rmdopen-2023-003392
19. Fleischmann R, Curtis JR, Charles-Schoeman C, Mysler E, Yamaoka K, Richez C, et al. Safety profile of upadacitinib in patients at risk of cardiovascular disease: integrated post hoc analysis of the SELECT phase III rheumatoid arthritis clinical programme. Ann Rheum Dis. (2023) 82:1130–41. doi: 10.1136/ard-2023-223916
20. Partalidou S, Patoulias D, Deuteraiou K, Avgerou P, Kitas G, Tzitiridou-Chatzopoulou M, et al. Risk of major adverse cardiovascular events and venous thromboembolism with JAK inhibitors versus TNF inhibitors in rheumatoid arthritis patients: a systematic review and meta-analysis. Mediterr J Rheumatol. (2024) 35(Suppl 1):10–9. doi: 10.31138/mjr.171023.rof
21. World Health Organization [WHO] The WHO Programme for International Drug Monitoring. Geneva: WHO (1968).
22. European Medicines Agency Guide on Methodological Standards in Pharmacoepidemiology (Revision 8). EMA/95098/2010. Amsterdam: EMA (2020).
23. Fusaroli M, Salvo F, Begaud B, AlShammari TM, Bate A, Battini V, et al. The Reporting of a disproportionality analysis for drug safety signal detection using individual case safety reports in PharmacoVigilance (READUS-PV): explanation and Elaboration. Drug Saf. (2024) 47:585–99. doi: 10.1007/s40264-024-01423-7
24. Molander V, Bower H, Frisell T, Askling J. Risk of venous thromboembolism in rheumatoid arthritis, and its association with disease activity: a nationwide cohort study from Sweden. Ann Rheum Dis. (2021) 80:169–75. doi: 10.1136/annrheumdis-2020-218419
25. Kim SC, Schneeweiss S, Liu J, Solomon DH. Risk of venous thromboembolism in patients with rheumatoid arthritis. Arthritis Care Res. (2013) 65:1600–7. doi: 10.1002/acr.22039
26. Arvanitakis KD, Arvanitaki AD, Karkos CD, Zintzaras EA, Germanidis GS. The risk of venous thromboembolic events in patients with inflammatory bowel disease: a systematic review and meta-analysis. Ann Gastroenterol. (2021) 34:680–90. doi: 10.20524/aog.2021.0631
27. Cutroneo PM, Sartori D, Tuccori M, Crisafulli S, Battini V, Carnovale C, et al. Conducting and interpreting disproportionality analyses derived from spontaneous reporting systems. Front Drug Saf Regul. (2023) 3:1323057. doi: 10.3389/fdsfr.2023.1323057
28. Miyakawa Y, Oda A, Druker BJ, Miyazaki H, Handa M, Ohashi H, et al. Thrombopoietin induces tyrosine phosphorylation of Stat3 and Stat5 in human blood platelets. Blood. (1996) 87:439–46. doi: 10.1182/blood.V87.2.439.bloodjournal872439
29. Kotyla PJ, Engelmann M, Giemza-Stokłosa J, Wnuk B, Islam MA. Thromboembolic Adverse Drug Reactions in Janus Kinase (JAK) Inhibitors: does the Inhibitor Specificity Play a Role? Int J Mol Sci. (2021) 22:2449. doi: 10.3390/ijms22052449
30. Ingrassia JP, Maqsood MH, Gelfand JM, Weber BN, Bangalore S, Lo Sicco KI, et al. Cardiovascular and venous thromboembolic risk with JAK inhibitors in immune-mediated inflammatory skin diseases: a systematic review and meta-analysis. JAMA Dermatol. (2024) 160:28–36. doi: 10.1001/jamadermatol.2023.4090
31. Zhang J, Li W, Gong M, Gu Y, Zhang H, Dong B, et al. Risk of venous thromboembolism with janus kinase inhibitors in inflammatory immune diseases: a systematic review and meta-analysis. Front Pharmacol. (2023) 14:1189389. doi: 10.3389/fphar.2023.1189389
32. Goldman A, Galper BL, Druyan A, Grossman C, Sharif K, Shechtman L, et al. Adverse cardiovascular events in rheumatoid arthritis patients treated with JAK inhibitors: an analysis of postmarketing spontaneous safety reports. Semin Arthritis Rheum. (2024) 67:152461. doi: 10.1016/j.semarthrit.2024.152461
33. Harigai M, Honda S. Selectivity of Janus kinase inhibitors in rheumatoid arthritis and other immune-mediated inflammatory diseases: is expectation the root of all headache? Drugs. (2020) 80:1183–201. doi: 10.1007/s40265-020-01349-1
34. Bonelli M, Kerschbaumer A, Kastrati K, Ghoreschi K, Gadina M, Heinz LX, et al. Selectivity, efficacy and safety of JAKinibs: new evidence for a still evolving story. Ann Rheum Dis. (2024) 83:139–60. doi: 10.1136/ard-2023-223850
35. Martinez de la Torre A, Clausen AB, Burden AM, Weiler S. Fracture-related safety reporting of JAK inhibitors: an analysis from the WHO Global VigiBase. Drug Saf. (2025) 48:191–201. doi: 10.1007/s40264-024-01490-w
36. Zöller B, Connors JM. Multimorbidity, comorbidity, frailty, and venous thromboembolism. Haematologica. (2024) 109:3852–9. doi: 10.3324/haematol.2023.284579
37. Montastruc JL, Lafaurie M, de Canecaude C, Durrieu G, Sommet A, Montastruc F, et al. Fatal adverse drug reactions: a worldwide perspective in the World Health Organization pharmacovigilance database. Br J Clin Pharmacol. (2021) 87:4334–40. doi: 10.1111/bcp.14851
38. Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrøm J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost. (2007) 5:692–9. doi: 10.1111/j.1538-7836.2007.02450.x
39. Dubois-Silva Á, Barbagelata-López C, Piñeiro-Parga P, López-Jiménez L, Riera-Mestre A, Schellong S, et al. Deep vein thrombosis symptoms and 30-day mortality in acute pulmonary embolism. Eur J Intern Med. (2023) 108:43–51. doi: 10.1016/j.ejim.2022.11.007
40. Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol. (2019) 123:144–51. doi: 10.1016/j.anai.2019.04.020
41. Figus FA, Piga M, Azzolin I, McConnell R, Iagnocco A. Rheumatoid arthritis: extra-articular manifestations and comorbidities. Autoimmun Rev. (2021) 20:102776. doi: 10.1016/j.autrev.2021.102776
42. Rosenbaum J, Chandran V. Management of comorbidities in ankylosing spondylitis. Am J Med Sci. (2012) 343:364–6. doi: 10.1097/MAJ.0b013e3182514059
43. Matta F, Singala R, Yaekoub AY, Najjar R, Stein PD. Risk of venous thromboembolism with rheumatoid arthritis. Thromb Haemost. (2009) 101:134–8. doi: 10.1160/TH08-08-0551
44. U.S. Food and Drug Administration. FDA Requires Warnings about Increased Risk of Serious Heart-Related Events, Cancer, Blood Clots, and Death for JAK Inhibitors that Treat Certain Chronic Inflammatory Conditions [Internet]. Silver Spring, MD: FDA (2021).
45. European Medicines Agency. EMA Recommends Measures to Minimise Risk of Serious Side Effects with Janus Kinase Inhibitors for Chronic Inflammatory Disorders [Internet]. Amsterdam: EMA (2022).
46. Salinas CA, Louder A, Polinski J, Zhang TC, Bower H, Phillips S, et al. Evaluation of VTE, MACE, and Serious infections among patients with RA treated with baricitinib compared to TNFi: a multi-database study of patients in routine care using disease registries and claims databases. Rheumatol Ther. (2023) 10:201–23. doi: 10.1007/s40744-022-00505-1
47. Hoisnard L, Pina Vegas L, Dray-Spira R, Weill A, Zureik M, Sbidian E. Risk of major adverse cardiovascular and venous thromboembolism events in patients with rheumatoid arthritis exposed to JAK inhibitors versus adalimumab: a nationwide cohort study. Ann Rheum Dis. (2023) 82:182–8. doi: 10.1136/ard-2022-222824
48. Rajasimhan S, Pamuk O, Katz JD. Safety of janus kinase inhibitors in older patients: a focus on the thromboembolic risk. Drugs Aging. (2020) 37:551–8. doi: 10.1007/s40266-020-00775-w
49. Di Nisio M, van Es N, Büller HR. Deep vein thrombosis and pulmonary embolism. Lancet. (2016) 388:3060–73. doi: 10.1016/S0140-6736(16)30514-1
50. Kotfis K, Wittebole X, Jaschinski U, Solé-Violán J, Kashyap R, Leone M, et al. A worldwide perspective of sepsis epidemiology and survival according to age: observational data from the ICON audit. J Crit Care. (2019) 51:122–32. doi: 10.1016/j.jcrc.2019.02.015
51. Kawai K, Yawn BP, Wollan P, Harpaz R. Increasing incidence of herpes zoster over a 60-year period from a population-based study. Clin Infect Dis. (2016) 63:221–6. doi: 10.1093/cid/ciw296
52. Di Napoli R, Richez C, Scavone C, Singier A, Demourgues M, Mascolo A, et al. Major adverse cardiovascular events related to JAK inhibitors: a disproportionality analysis using the WHO Global Individual Case Safety Database. Drug Saf. (2025) 48:943–52. doi: 10.1007/s40264-025-01535-8
53. Carmona L, Aurrecoechea E, García de Yébenes MJ. Tailoring rheumatoid arthritis treatment through a sex and gender lens. J Clin Med. (2023) 13:55. doi: 10.3390/jcm13010055
54. Vela-Casasempere P, Otero-Varela L, Gómez Sabater S, Caño Alameda R, Campos Fernández C, Calvo-Gutiérrez J, et al. Gender differences in clinical and prescribing characteristics of biologic and targeted synthetic drugs in naïve patients with rheumatoid arthritis: data from BIOBADASER III registry. Arthritis Res Ther. (2025) 27:103. doi: 10.1186/s13075-025-03571-2
55. Koc GH, Looijen AEM, van der Horst-Bruinsma IE, de Jong PHP. Sex differences in rheumatoid arthritis: new insights from clinical and patient-reported outcome perspectives. J Rheumatol. (2025) 52:553–62. doi: 10.3899/jrheum.2024-1258
56. Mori S, Ogata F, Tsunoda R. Risk of venous thromboembolism associated with Janus kinase inhibitors for rheumatoid arthritis: case presentation and literature review. Clin Rheumatol. (2021) 40:4457–71. doi: 10.1007/s10067-021-05911-4
57. Shah JT, Shah KT, Femia AN, Lo Sicco KI, Merola JF, Weber B, et al. Cardiovascular risk management in patients treated with janus kinase inhibitors. J Cardiovasc Pharmacol. (2024) 83:392–402. doi: 10.1097/FJC.0000000000001470
58. Bate A, Evans SJ. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol Drug Saf. (2009) 18:427–36. doi: 10.1002/pds.1742
Keywords: Janus kinase inhibitors, venous thromboembolism, pharmacovigilance, drug-related side effects and adverse reactions, rheumatoid arthritis, adverse drug reaction reporting systems
Citation: Ferreira-da-Silva R, Lobo M, Abreu AR, Pereira-Macedo J, Mós B, Rodriguez CA, Lourenço IM, Vieira I, Polónia JJ, Gouveia L, Silva L, Morato M, Pinto M, Forrester M, Pereira M, Rodrigues N, Biase T and Ribeiro I (2025) Post-marketing surveillance of upadacitinib: multilevel analysis of venous thromboembolism reporting in global data and rheumatoid arthritis. Front. Med. 12:1683751. doi: 10.3389/fmed.2025.1683751
Received: 11 August 2025; Accepted: 29 October 2025;
Published: 01 December 2025.
Edited by:
Bojing Shao, Oklahoma Medical Research Foundation, United StatesReviewed by:
Sun Changbo, Ningbo Traditional Chinese Medicine Hospital, ChinaEmi Sato, Fukuoka University, Japan
Copyright © 2025 Ferreira-da-Silva, Lobo, Abreu, Pereira-Macedo, Mós, Rodriguez, Lourenço, Vieira, Polónia, Gouveia, Silva, Morato, Pinto, Forrester, Pereira, Rodrigues, Biase and Ribeiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renato Ferreira-da-Silva, cnNpbHZhQG1lZC51cC5wdA==
†ORCID: Renato Ferreira-da-Silva, orcid.org/0000-0001-6517-6021; Mariana Lobo, orcid.org/0000-0003-3890-7735; Ana Rafaela Abreu, orcid.org/0009-0006-5574-8050; Juliana Pereira-Macedo, orcid.org/0000-0001-9271-0277; Carolina Ameijeiras Rodriguez, orcid.org/0000-0001-8817-7772; Inês Mariana Lourenço, orcid.org/0000-0003-0752-0802; Jorge Junqueira Polónia, orcid.org/0000-0002-0133-7217; Manuela Morato, orcid.org/0000-0002-9509-0613; Manuela Pinto, orcid.org/0009-0008-8759-1486; Mario Forrester, orcid.org/0000-0003-3966-7841; Tayanny Biase, orcid.org/0000-0003-2133-2621; Inês Ribeiro, orcid.org/0000-0002-3442-8158