
 John Lee2
John Lee2
- 1 Department of Neurology, Stritch School of Medicine, Loyola University Chicago, Maywood, IL, USA
- 2 Department of Pathology, Stritch School of Medicine, Loyola University Chicago, Maywood, IL, USA
A 54-year-old woman presented to the emergency room with 3 months of slurred speech, language problems, and right hemiparesis. Initial impression based on history, exam, and imaging was brain abscess vs. primary or metastatic neoplasm. Brain biopsy of the lesion and pathologic specimens were obtained. Below is a description of her presentation, hospital course, imaging, and pathology, as well as a short discussion of the final diagnosis.
A 54-year-old right handed woman presented to the emergency department with complaints of slurred speech and right foot heaviness. She first noticed the symptoms 3 weeks earlier, and associated it with fatigue. However, the symptoms progressed, and she eventually also noticed difficulty thinking of the “right words to say.” She stated that she sometimes forgot words, as if she had trouble “getting them out.” By the time of presentation her right foot was very “heavy”; if she did not lift her leg high enough she would stumble. She had no headaches, nausea, vomiting, fevers, night sweats, visual, or sensory complaints.
She had a past medical history of depression, but no hypertension, hyperlipidemia, or diabetes. She was married, and had smoked 1/2 packs of cigarettes per day for the past 5 years. She drank a glass of wine per day and did not use any illicit substances. In the 3-years she had been out of the country two times – to Guatemala and Belize. Her family history was remarkable for a mother with an atrial myxoma, father with renal cell cancer and spinal malignancies, and a brother with a spindle cell tumor of the left arm. There was no family history of cardiovascular disease. Review of systems was unremarkable.
Blood pressure and other vital signs were normal. General physical examination was unremarkable. Neurologic examination was remarkable for slurred impaired fluency and repetition, with preserved comprehension, reading, and writing. She had a right lower facial droop, right pronator drift, and mild right hemiparesis. Muscle stretch reflexes were brisk and symmetric. Plantar responses were flexor. She had decreased dexterity on the right and an unsteady gait, with slight circumduction of her right leg.
Laboratory testing showed normal blood indices (normal white blood cell differential), and a normal metabolic profile. Chest radiograph was unremarkable. Cranial computerized tomography (CT) showed a low density mass with peripheral high attenuation rim within the left frontal lobe with adjacent vasogenic edema and trace midline shift (Figure 1).
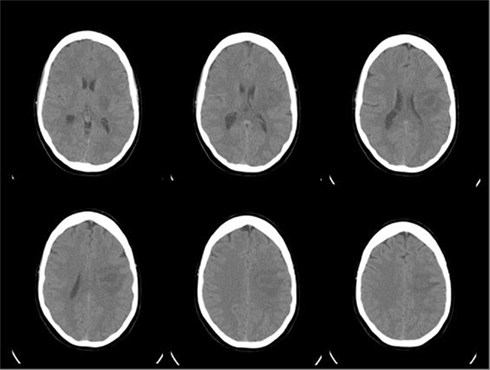
Figure 1. Non-contrast cranial CT upon presentation.
Magnetic resonance imaging (MRI) of her brain showed a 3.1-cm × 2.3-cm × 1.9-cm rim-enhancing left posterior frontal intra-axial mass that mildly restricted diffusion in the periphery and did not have a hemorrhagic component (Figure 2). Differential diagnosis of the lesion based on history, exam, and imaging included subacute/chronic infectious, neoplastic (primary brain vs. metastatic), and demyelinating processes. Empiric antibiotics and dexamethasone were started for initial concern of abscess and mild mass effect. Stereotactic brain biopsy of the lesion in the left frontal lobe was obtained.
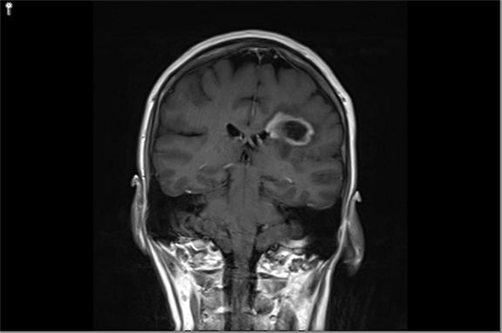
Figure 2. Coronal post-gadolinium T1-weighted MRI shows a mass in the subcortical left frontoparietal region abutting into the left lateral ventricle with associated peripheral ring-like enhancement.
Pathology
Discussion
Histology sections revealed brain parenchyma with evidence of demyelination, perivascular lymphocytic infiltrates, macrophages, reactive gliosis, and relative preservation of axons; consistent with a demyelinating process. There were no cells to suggest neoplastic atypia. Gram, Grocott methenamine silver (GMS), AFB, and SV40 stains were negative for microorganisms. A diagnosis of tumefactive multiple sclerosis (MS) was made based on her clinical history and imaging with the pathologic diagnosis (Figures 3–6).
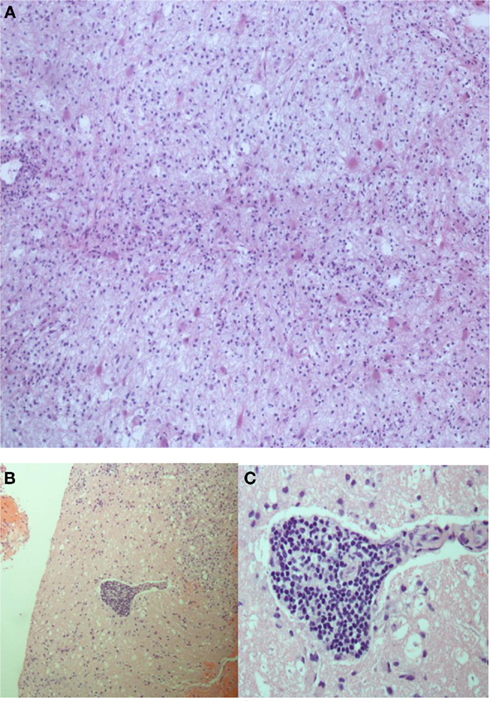
Figure 3. H and E staining shows brain parenchyma with focal lymphocytic infiltrates, numerous macrophages and reactive gliosis (A) and perivascular lymphocytic infiltrates (B,C).
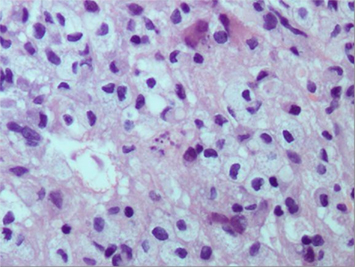
Figure 4. H and E staining remarkable for astrocytes with fragmented nuclear inclusions (Creutzfeldt-Peters cells) and numerous lipid-laden macrophages.
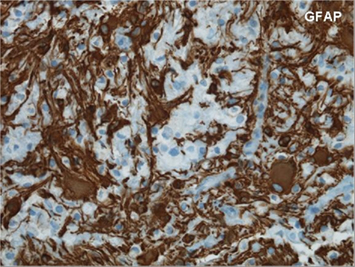
Figure 5. Glial fibrillary acidic protein staining shows relative a reactive gliosis pattern.
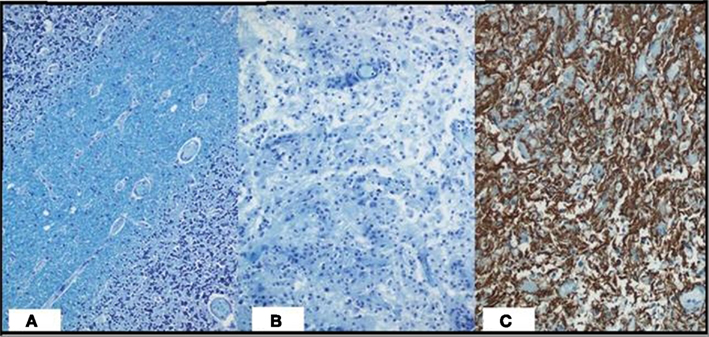
Figure 6. Luxol fast blue [control (A), patient (B)] shows relative destruction and loss of myelin with neurofilament staining (C) showing relative axonal preservation.
Tumefactive MS is a rare variant of MS characterized by the presence of large demyelinating plaques (>2 cm) on MRI (Pittock et al., 2005). Other atypical imaging features include mass effect, edema, and/or post-gadolinium enhancement (Lucchinetti et al., 2008). Potential gadolinium-enhancing patterns of tumefactive MS include ring (closed-ring most common), heterogeneous (punctuate and nodular), patchy and diffuse, cotton-ball, and homogeneous (Lucchinetti et al., 2008). Patients may present with a variety of clinical manifestations depending on the size and location of the lesion. Acute aphasia may be a common presentation, as in our patient, and is not necessarily indicative of a poor prognosis (Lacour et al., 2004).
Radiologically, the lesions may mimic neoplasms, and are typically supratentorial (Hu and Lucchinetti, 2009). Pathology reveals hypercellular confluent demyelinating lesions with inflammatory infiltrates, dominated by myelin-laden macrophages. There is relative axonal preservation. Creutzfeldt-Peters cells (Figure 4), astrocytes with fragmented nuclear inclusions, are present and may be confused with mitotic cells seen in glioblastoma (Hu and Lucchinetti, 2009). Most patients with initial presentation of tumefactive MS go on to develop a relapsing-remitting type MS. There are, however, rare reports of relapsing-remitting MS of the tumefactive type (Selkirk and Shi, 2005). Tumefactive lesions can also be associated with spontaneous intracranial hemorrhage. Magnetic resonance spectroscopy (mRS) generally shows decreased N-acetylaspartate (NAA)/creatinine (Cr) ratio, an increased choline (Cho)/Cr ratio, and presence of glutamate/glutamine or lactate peaks. These findings, however, are observed in various disease conditions (including neoplasia) and thus are not helpful in differentiating large tumefactive lesions from neoplasms (Kiriyama et al., 2010). Moreover, the imaging characteristics on mRS are not seen in all tumefactive demyelinating lesions, and thus biopsy is sometimes essential to diagnose patients presenting with tumefactive demyelination and no history of demyelinating disease (Kiriyama et al., 2010).
Acute exacerbations of tumefactive MS are treated with high-dose intravenous steroids and plasma exchange (Nilsson et al., 2009). In cases of malignant cerebral edema, hemicraniectomy has been recommended and can be a life-saving measure (Gormley and Zajicek, 2006; Nilsson et al., 2009). Immunomodulating agents may be necessary with a relapsing-remitting course or with progressive tumefactive demyelination despite above measures. In addition to traditional medications used to treat relapsing-remitting MS, case studies have shown favorable outcomes using Rituximab (Leussink et al., 2008), Mitoxantrone (Jeffery et al., 2004), Alemtuzumab (Gormley and Zajicek, 2006), and stem cell transplantation (Kimiskidis et al., 2007) in treating tumefactive demyelinating lesions.
Our patient was started on methylprednisolone with marked improvement of her weakness and language difficulty. Post-operative course was complicated by lower extremity deep vein thrombosis (DVT) and pulmonary embolism treated with warfarin for 6 months. After treatment with steroids and anticoagulation a lumbar puncture was done, and was unremarkable [cerebrospinal fluid oligoclonal bands negative (Hu and Lucchinetti, 2009), IgG index normal (0.62)].
Several months later she complained of increased fatigue, right arm and thigh swelling, and worsening dexterity of her right hand. Repeat imaging was remarkable for a discrete, contiguous enhancing hyperintense lesion just posterior to the previous one (Figure 7).
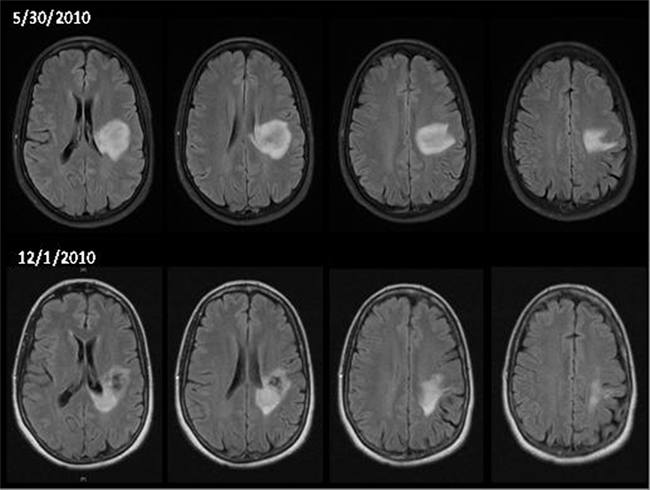
Figure 7. Comparison of brain MRI at presentation (May 30, 2010) and follow-up (December 1, 2010) showing a discrete contiguous lesion just posterior to the previous one.
She was readmitted for plasmapheresis and discharged on oral prednisone and Rituximab for relapsing-remitting tumefactive MS. On recent follow-up, approximately 1 year after initial presentation, she was noted to have a residual mild motor aphasia and spastic right hemiparesis. She has had no further clinical relapses to date.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Gormley, K. M., and Zajicek, J. P. (2006). “Alemtuzumab and craniotomy for severe acute demyelinating illness,” in 16th Meeting of the European Neurological Society, Plymouth.
Hu, W., and Lucchinetti, C. F. (2009). The pathological spectrum of CNS inflammatory demyelinating diseases. Semin. Immunopathol. 31, 439–453.
Jeffery, D. R., Lefkowitz, D. S., and Crittenden, J. P. (2004). Treatment of Marburg variant multiple sclerosis with mitoxantrone. J. Neuroimaging 14, 58–62.
Kimiskidis, V. K., Sakellari, I., and Tsimourtou, V. (2007). Autologous stem-cell transplantation in malignant multiple sclerosis: a case with a favorable long-term outcome. Mult. Scler. 14, 278.
Kiriyama, T., Kataoka, H., Taoka, T., Tonomura, Y., Terashima, M., Morkawa, M., Tanizawa, E., Kawahara, M., Furiya, Y., Sugie, K., Kichikawa, K., and Ueno, S. (2010). Characteristic neuroimaging in patients with tumefactive demyelinating lesions exceeding 30mm. J. Neuroimaging 21, e69–e77.
Lacour, A., de Seze, J., Revenco, E., Lebrun, C., Masmoudi, K., Vidry, E., Rumbach, L., Chatel, M., Verier, A., and Vermersch, P. (2004). Acute aphasia in multiple sclerosis: a multicenter study of 22 patients. Neurology 62, 974–977.
Leussink, V. I., Lehmann, H. C., Meyer, Z. H. G., Hartung, H. P., Stuve, O., and Kieseier, B. C. (2008). Rituximab induces clinical stabilization in a patient with fulminate multiple sclerosis not responding to natalizumab: evidence for disease heterogeneity. J. Neurol. 255, 1436.
Lucchinetti, C. F., Gavrilova, R. H., Metz, I., Parisi, J. E., Scheithauer, B. W., Weigand, S., Thomsen, K., Mandrekar, J., Altintas, A., Erickson, B. J., Konig, F., Giannini, C., Lassmann, H., Linbo, L., Pittock, S. J., and Bruk, W. (2008). Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis. Brain 131, 1759–1777.
Nilsson, P., Larsson, E. M., Kahlon, B., Nordstrom, C. H., and Norrving, B. (2009). Tumefactive demyelinating disease treated with decompressive craniotomy. Eur. J. Neurol. 16, 639–642.
Pittock, A. J., McClelland, R. L., Achenbach, S. J., Konig, F., Bitsch, A., Bruck, W., Lassmann, H., Parisi, J. E., Scheithauer, B. W., Rodriguez, M., Weinshenker, B. G., and Lucchinetti, C. F. (2005). Clinical course, pathological correlations, and outcome of biopsy proved inflammatory demyelinating disease. J. Neurol. Neurosurg. Psychiatr. 76, 1693–1697.
Keywords: hemiparesis, slurred speech, diagnosis
Citation: Venizelos A, Lee J and Biller J (2011) Language impairment and right hemiparesis in a 54-year-old woman. Front. Neur. 2:40. doi: 10.3389/fneur.2011.00040
Received: 10 May 2011;
Paper pending published: 22 May 2011;
Accepted: 08 June 2011;
Published online: 01 July 2011.
Edited by:
Osvaldo Fustinoni, Universidad de Buenos Aires, ArgentinaReviewed by:
Luciano A. Sposato, INECO Foundation, ArgentinaGustavo Saposnik, St. Michael’s Hospital – University of Toronto, Canada
Copyright: © 2011 Venizelos, Lee and Biller. This is an open-access article subject to a non-exclusive license between the authors and Frontiers Media SA, which permits use, distribution and reproduction in other forums, provided the original authors and source are credited and other Frontiers conditions are complied with.
*Correspondence: José Biller, Department of Neurology, Stritch School of Medicine, Loyola University Chicago, Building 105, Room 2700, 2160 South 1st Avenue, Maywood, IL 60153, USA. e-mail:amJpbGxlckBsdW1jLmVkdQ==