 Isaac Almendros1,2,3
Isaac Almendros1,2,3 Miguel Ángel Martínez-García4
Miguel Ángel Martínez-García4 Francisco Campos-Rodríguez5
Francisco Campos-Rodríguez5 Erica Riveiro-Falkenbach6José L. Rodríguez-Peralto6Eduardo Nagore7Antonio Martorell-Calatayud8Luis Hernández Blasco9,10Jose Bañuls Roca9,10Eusebi Chiner Vives11
Erica Riveiro-Falkenbach6José L. Rodríguez-Peralto6Eduardo Nagore7Antonio Martorell-Calatayud8Luis Hernández Blasco9,10Jose Bañuls Roca9,10Eusebi Chiner Vives11 Alicia Sánchez-de-la-Torre2,12Jorge Abad-Capa2,13Josep Maria Montserrat2,14Amalia Pérez-Gil15
Alicia Sánchez-de-la-Torre2,12Jorge Abad-Capa2,13Josep Maria Montserrat2,14Amalia Pérez-Gil15 Valentín Cabriada-Nuño16Irene Cano-Pumarega17Jaime Corral-Peñafiel2,18Trinidad Diaz-Cambriles19
Valentín Cabriada-Nuño16Irene Cano-Pumarega17Jaime Corral-Peñafiel2,18Trinidad Diaz-Cambriles19 Olga Mediano2,20Joan Dalmau-Arias21
Olga Mediano2,20Joan Dalmau-Arias21 Ramon Farré1,2,3
Ramon Farré1,2,3 David Gozal22* On Behalf of the Spanish Sleep Network
David Gozal22* On Behalf of the Spanish Sleep Network
- 1Unitat de Biofísica i Bioenginyeria, Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona, Barcelona, Spain
- 2Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Madrid, Spain
- 3Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
- 4Respiratory Department, Hospital Universitario y Politécnico la Fe, Valencia, Spain
- 5Respiratory Department, Hospital Universitario de Valme, Seville, Spain
- 6Pathology Department, Medical School, Universidad Complutense, Instituto i + 12, Hospital Universitario 12 de Octubre, CIBERONC, Madrid, Spain
- 7Dermatology Department, Instituto Valenciano de Oncología, Valencia, Spain
- 8Dermatology Department, Hospital de Manises, Valencia, Spain
- 9Respiratory Department, ISABIAL, Hospital Gral, Univ. Alicante, Alicante, Spain
- 10Departamento Medicina Clinica, Univ. Miguel Hernandez, Elche, Spain
- 11Respiratory Department, Hospital san Juan de Alicante, Alicante, Spain
- 12Respiratory Department, Group of Translational Research in Respiratory Medicine, Hospital Universitari Arnau de Vilanova and Santa Maria, IRBLleida, Lleida, Spain
- 13Respiratory Department, Hospital Germans Trias i Pujol, Centro de investigacion Biomedica, Madrid, Spain
- 14Respiratory Department, Hospital Clinic-IDIBAPS, Barcelona, Spain
- 15Dermatology Department, Hospital de Valme, Seville, Spain
- 16Respiratory Department, Hospital Universitario Cruces, Bilbao, Spain
- 17Respiratory Department, Hospital Universitario de Getafe, Madrid, Spain
- 18Respiratory Department, Hospital Universitario S. Pedro Alcántara, Cáceres, Spain
- 19Respiratory Department, Hospital 12 de Octubre, Madrid, Spain
- 20Respiratory Department, Hospital Universitario de Guadalajara, CIBER de enfermedades respiratorias, Madrid, Spain
- 21Dermatology Department, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 22Department of Pediatrics, Pritzker School of Medicine, Biological Sciences Division, The University of Chicago, Chicago, IL, United States
Epidemiological associations linking between obstructive sleep apnea and poorer solid malignant tumor outcomes have recently emerged. Putative pathways proposed to explain that these associations have included enhanced hypoxia inducible factor (HIF)-1α and vascular endothelial growth factor (VEGF) cell expression in the tumor and altered immune functions via intermittent hypoxia (IH). Here, we examined relationships between HIF-1α and VEGF expression and nocturnal IH in cutaneous melanoma (CM) tumor samples. Prospectively recruited patients with CM tumor samples were included and underwent overnight polygraphy. General clinical features, apnea–hypopnea index (AHI), desaturation index (DI4%), and CM characteristics were recorded. Histochemical assessments of VEGF and HIF-1α were performed, and the percentage of positive cells (0, <25, 25–50, 51–75, >75%) was blindly tabulated for VEGF expression, and as 0, 0–5.9, 6.0–10.0, >10.0% for HIF-1α expression, respectively. Cases with HIF-1α expression >6% (high expression) were compared with those <6%, and VEGF expression >75% of cells was compared with those with <75%. 376 patients were included. High expression of VEGF and HIF-1α were seen in 88.8 and 4.2% of samples, respectively. High expression of VEGF was only associated with increasing age. However, high expression of HIF-1α was significantly associated with age, Breslow index, AHI, and DI4%. Logistic regression showed that DI4% [OR 1.03 (95% CI: 1.01–1.06)] and Breslow index [OR 1.28 (95% CI: 1.18–1.46)], but not AHI, remained independently associated with the presence of high HIF-1α expression. Thus, IH emerges as an independent risk factor for higher HIF-1α expression in CM tumors and is inferentially linked to worse clinical CM prognostic indicators.
Introduction
Cutaneous melanoma (CM) is a very aggressive type of skin cancer that is not only fraught with a high mortality rate, but is also a cancer type whose incidence has continued to increase over the last several decades (1). In an effort to identify tumors with more aggressive properties, several investigators have postulated that the high proliferative rates of CM could induce the presence of episodic intra-tumoral hypoxia, which in turn could foster alterations in melanoma malignant cells to promote invasion and metastasis, as well as resistance to chemotherapy (2–4).
Since intermittent hypoxia (IH)-induced alterations in tumor malignancy are driven, at least in part, by the transcriptional activity of hypoxia inducible factor-1α (HIF-1α) pathways (5–7), it is not surprising that many of the HIF-1α genes that are involved in regulation of cellular bioenergetics, angiogenesis, and expansion of the vascular supply network exhibit increased expression within rapidly proliferating tumors and are, therefore, considered as potentially viable reporters of CM aggressiveness and poor outcomes (8, 9). In addition, one of the major genes regulated by HIF-1α transcriptional activity is vascular endothelial growth factor (VEGF), a major regulator of the number of capillaries within a tissue (10, 11) and is also active in a vasculogenic mimicry capacity (12). Studies exploring the expression HIF-1α and VEGF in CM have, however, resulted in somewhat inconsistent results, with a propensity of the findings supporting the concept that increased expression of HIF-1α and VEGF in CM is associated with tumor staging as well as with other prognostic indicators (13–21).
Obstructive sleep apnea (OSA) is a highly prevalent disorder characterized by the presence of increased upper airway collapsibility during sleep that leads to either upper airway collapse or restricted airflow and consequent periodic hypoxia and hypercapnia events, usually terminated by arousal and restoration of airflow (22–24). The cyclical hypoxic events that characterize OSA have been implicated in a vast array of OSA-associated morbidities involving cardiovascular, metabolic, and cognitive systems (25–27). In recent years, potential associations between OSA and cancer have been reported and primarily ascribed to the effects of IH on tumor biology (28–31). In addition, both experimental and clinical evidence has indicated that CM is one of the more susceptible tumors to the IH patterns that characterize OSA (32–34).
Based on aforementioned considerations, we hypothesized that semiquantitative assessments of HIF-1α and VEGF immunoreactivity in excised CM tumors may be associated with typical severity measures of OSA. Hence, the objective of the present study was to analyze potential associations between the expression of HIF-1α and VEGF and measures of respiratory disturbance during sleep in a large prospective series of patients suffering from CM.
Materials and Methods
Design, Setting, and Patients
We conducted a prospective, multicenter study in 29 Spanish University Hospitals. Consecutive patients diagnosed with CM by the dermatology or oncology departments were eligible for inclusion in this study. Patients were excluded if they had melanoma of an unknown primary cause, melanoma in mucosa or melanomas “in situ,” respiratory failure, heart failure grades III–IV NYHA, pregnancy, or a prior diagnosis of SDB or CPAP treatment. The study was approved by the Ethical Committee of each participating center, and all patients signed the informed consent.
Procedures
All tumors were surgically resected and subjected to clinical staging. In addition to standard pathologic assessment in each center to establish the diagnosis of CM, all the specimens were re-evaluated in a melanoma reference center by an expert pathology panel whose members were blinded to any of the immunostaining findings. For each tumor, the following pathologic features were assessed by the panel: Breslow tumor thickness (in millimeter, and categorized as ≤1.00, 1.01–2.00, 2.01–4.00, and >4.00), ulceration (presence vs. absence), tumor mitotic rate (according to “hot spot” method and categorized in: >5 vs. ≤5 mitoses/mm2), and regression (presence vs. absence). Furthermore, the following clinical characteristics were also documented: tumor location (head/neck, upper extremities, trunk, lower extremities, acral), age at diagnosis, sex, body mass index (BMI, kg/m2), skin phototype, and stage at diagnosis [localized (I–II), loco-regional disease (III), and distant metastasis (IV)] by the treating dermatologists and institutional pathologists. In addition, the staging of each tumor was confirmed by a multi-institutional tumor board that was unaware of the immunohistological findings described below. Other markers of melanoma aggressiveness, namely, the presence of ulceration and regression in biopsy tissue, histologic subtypes of melanoma, presence of metastasis, and the invasion of sentinel lymph nodes were also documented.
Immunohistochemistry
Immunohistochemistry was performed on 4-μm-thick sections of formalin-fixed, paraffin-embedded melanoma samples. Immunostaining was performed on a Leica Bond-III stainer (Leica Biosystems, Newcastle, UK) using the Leica Bond Polymer Refine Kit (Leica Biosystems). Melanoma samples were stained with a 1:2 dilution of anti-VEGF prediluted antibody (ab27620, Abcam, Cambridge, UK) and with a 1:100 dilution of anti-HIF-1α antibody (ab51608, Abcam). The staining results were independently analyzed by two expert pathologists who were blinded to the staging and clinical features of the subjects. VEGF-specific staining was scored taking into account both the percentage of positive cells (0, <25, 25–50, 51–75, >75%) and expression intensity (low, moderate, or high) (Figure 1). HIF-1α-specific nuclear staining was scored taking into account the percentage of positive cells (0, 0–5, 6–10, >10%) as well as the expression intensity (low, moderate, or high) (Figure 1). After the blind scoring of immunohistochemical stains in each tumor was completed, the data were tabulated, and are presented accordingly.
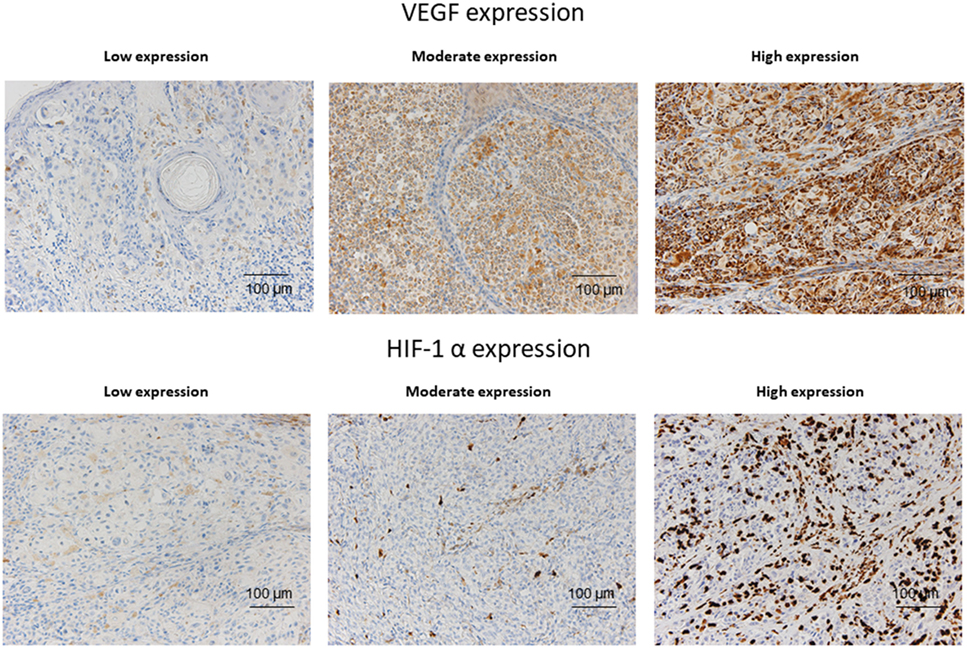
Figure 1. Representative examples of VEGF and HIF-1α expression according to expression levels (low, medium, and high) in melanoma sections.
Sleep Study
All patients included in the study underwent a diagnostic sleep study by means of respiratory polygraphy, using a device validated against polysomnography (Embletta Gold in 37% of the patients and Alice PDX in 63% of patients) both validated against PSG, and following the Spanish Society of Pneumology and Thoracic Surgery Guidelines for OSA diagnosis and treatment. The time span between the initial appointment for suspicion of melanoma and the sleep study was always lower than 6 months. Every sleep study was manually scored by skilled staff. All the studies included continuous recording of the oro-nasal flow and pressure, respiratory movements, and oxyhemoglobin saturation (SpO2). Apnea was defined as complete cessation of oro-nasal flow for ≥10 s and was classified as either obstructive or central, based on the presence or absence of respiratory efforts. Hypopnea was defined as a 30–90% reduction in oro-nasal flow for ≥10 s followed by a ≥3% decrease in SpO2, while Tsat90 was defined as the percentage of recording time with SpO2 <90%. The recording time, desaturation indices at 4% and the mean baseline nocturnal, baseline daytime, and minimum nocturnal saturation were also recorded. Those tests in which the patients claimed to sleep less than 4 h, or in which there were less than 5 h of nocturnal recording, were repeated.
Statistical Analysis
The SPSS 20.0 statistical package (Chicago, IL, USA) was used for all analyses. The data were expressed by using the mean and SD, or the median and the interquartile range for quantitative variables, according to whether or not they followed a normal distribution. The qualitative and dichotomic variables were expressed as the absolute value and the percentage with respect to the total. For analyses purposes, histochemical assessments of HIF-1α and VEGF expression variables were dichotomized: HIF-1α expression >6% (high expression) was compared with those samples with <6%, and VEGF expression >75% of cells was compared with those with <75%.
The comparison between these two groups’ baseline variables was made with the Student’s t-test for independent means or the Mann–Whitney test, according to the distribution of the quantitative variables, while the chi-square test was used to compare the two percentages. The factors independently related to the presence of a high HIF-1α or VEGF expressions were determined by introducing into two multivariate logistical regression analyses those variables which, in the opinion of the researchers, could have clinical importance. Odds ratios with 95% confidence intervals were calculated for each molecule expression. Although a two-tailed p-value of <0.05 was initially considered as indicative of statistical significance, Bonferroni test was used to correct p-values for multiple comparisons as appropriate.
Results
Baseline Characteristics
Of 476 eligible patients, 443 were prospectively recruited and provided informed consent to participate in this study and finally, 376 subjects had biopsy tissues available for analysis. The baseline clinical and tumor characteristics are depicted in Table 1, and the sleep-related symptoms and sleep test variables are shown in Table 2. The patients had a mean age of 56.4 (15.1) years (52.9% males), BMI of 27.3 (4.6) kg/m2, apnea–hypopnea index (AHI) of 14.9 (16.5) event/h, and DI4% of 10.2 (13.7) desaturations/h. Regarding the melanoma tumor, the mean Breslow index was 1.70 (2.5) mm, the most common anatomical site was the body (41.8%), and only four patients had distant metastasis at the time of the diagnosis.
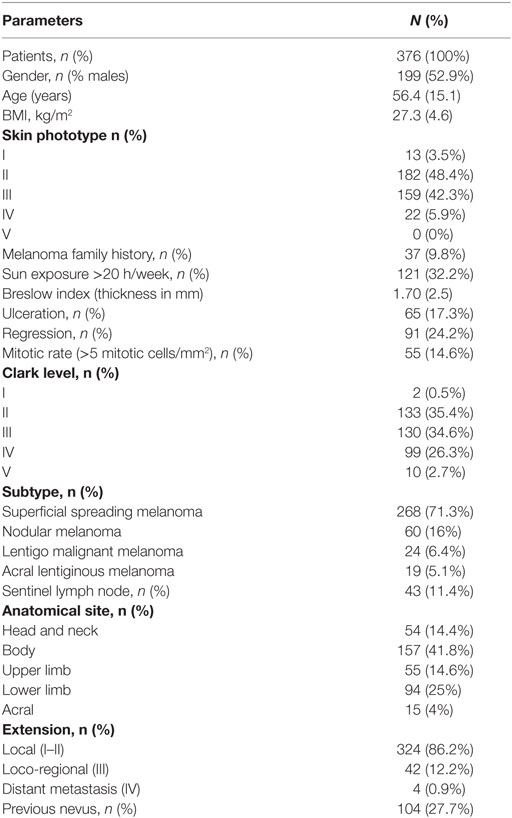
Table 1. Patient and cutaneous melanoma characteristics (n = 376).
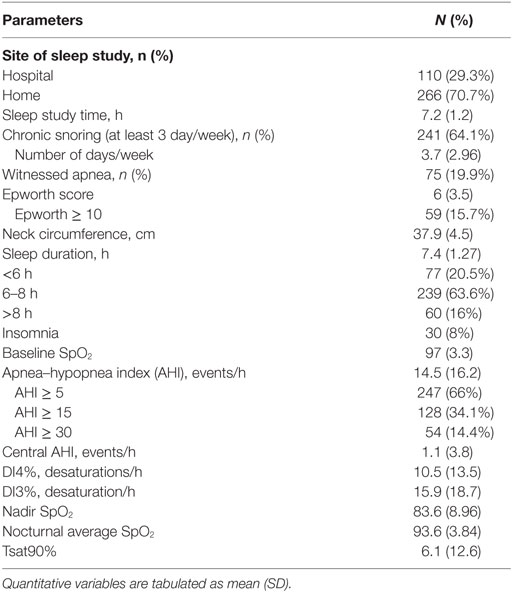
Table 2. Sleep characteristics and other comorbidities.
VEGF and HIF-1α Expression
The vast majority of melanoma samples presented high VEGF expression (333 patients, 88.8%), and non-high HIF-1α expression (360 patients, 95.7%). Only two samples (0.5%) presented no VEGF expression, and only 16 samples (4.2%) presented high HIF-1α expression, with only five patients presenting HIF-1α expression in more than 10% of cells. 6 (1.6%), 12 (3.4%), and 24 (6.4%) samples presented VEGF expression in less than 25%, between 25 and 50%, and between 51 and 75% of cells, respectively.
Univariate Analysis
Those patients with CM and high VEGF expression were most frequently females and showed significantly less mitotic index (Table 3), higher AHI value (nearly statistically significant), and lower Tsat90 (Table 4).
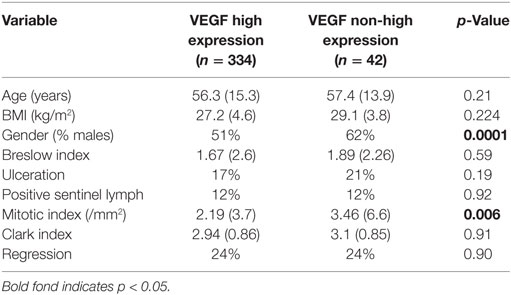
Table 3. Comparisons between expression of vascular endothelial growth factor (VEGF) and general characteristics and aggressiveness markers of melanoma.
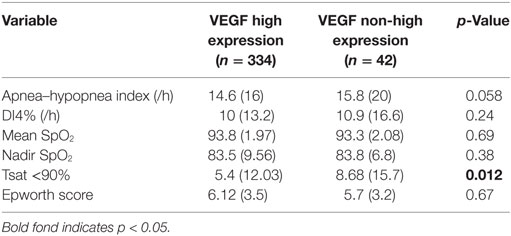
Table 4. Comparisons between expression groups of vascular endothelial growth factor (VEGF) regarding sleep-disordered breathing variables and intermittent/continuous hypoxia indicators.
On the other hand, those patients with CM and high HIF-1α expression showed significantly more CM aggressiveness markers, including increased mitotic index, higher Breslow index, the presence of ulceration and proportion of positive sentinel nodes (Table 5), and greater SDB severity regarding their corresponding DI4% (near statistically significant association: p = 0.08) and nadir SpO2 values (Table 6).
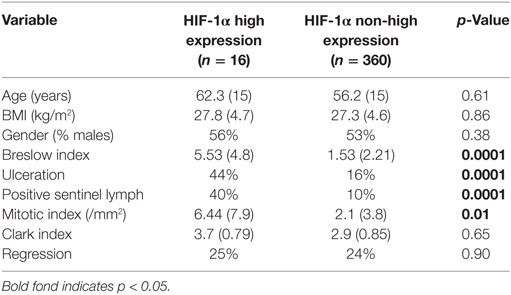
Table 5. Comparisons between the groups with high and low expression of hypoxia inducible factor (HIF)-1α regarding their general characteristics and aggressiveness markers of melanoma.
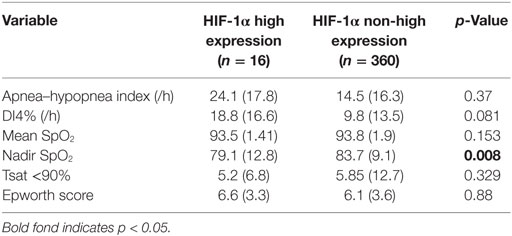
Table 6. Comparisons between the groups with high and low expression of hypoxia inducible factor (HIF)-1α in relation to sleep-disordered breathing variables and intermittent/continuous hypoxia indicators.
Multivariate Analysis: Logistic Regressions
To explore which variables were independently associated with high VEGF expression, four variables were introduced in the stepwise logistic regression: gender, AHI, Tsat90%, and mitotic index. However, none of these variables were significantly associated with VEGF expression (Table 7).
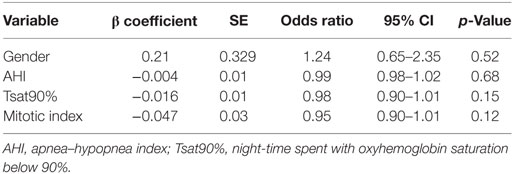
Table 7. Logistic regression analysis illustrating the lack of independent relationships between VEGF expression and melanoma aggressiveness, gender, and sleep study variables.
A similar analysis was conducted for HIF-1α expression. In this case, the two variables introduced into the logistic regression analysis were the Breslow index, which was the best marker of melanoma aggressiveness, and the DI4% as a marker of IH. Table 8 shows that both variables were independently associated with higher expression of HIF-1α.
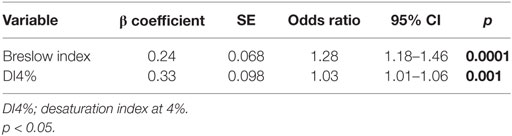
Table 8. Logistic regression analysis showing the independent relationships between the Breslow index and DI4% values and the presence of high expression levels of hypoxia inducible factor-1α in cutaneous melanoma tumors.
Discussion
This study shows that levels of HIF-1α expression in CM are independently associated with indicators of episodic hypoxia as derived from nocturnal polygraphic recordings in a large prospectively recruited cohort of CM patients. However, contrary to the significant associations between the patterns of HIF-1α expression and the severity of sleep-disordered breathing, VEGF expression was high in the vast majority of CM lesions, and did not manifest any significant relationship with polygraphically derived measurements, suggesting the absence of co-linearity between HIF-1α and VEGF expression in CM.
Before we discuss the potential implications of our findings, several methodological points deserve mention. First, this is the first prospective study concurrently evaluating one type of cancer, namely CM, and the presence of sleep-disordered breathing. Indeed, most of the existing literature to date has relied on retrospective databases, or alternatively, due to cohort size limitations, has not investigated a specific type of malignancy (28, 30, 35–41). The current study overcomes this major limitation, even if the methodological approach for assessment of sleep-disordered breathing consisted of overnight polygraphy rather than polysomnography, such that the role of disrupted sleep cannot be deduced (42). Of note, the prevalence of OSA and the distribution of severity categories of OSA in this cohort were similar to that reported in other population-based studies (43, 44), further attesting to the overall absence of bias in patient recruitment, which as indicated was guided by the diagnosis of CM. Second, to minimize any potential bias, we ascertained that there would be complete separation in the processing of the polygraphy scoring and the classification of the aggressiveness CM markers by the various expert panels. Finally, we implemented highly stringent and blinded HIF-1α and VEGF immunohistochemistry staining and cell counting procedures. However, we opted for a straightforward assessment of the expression of HIF-1α and VEGF to establish the potential validity of the a priori assumption, i.e., OSA is associated with increased hypoxia-related markers in CM tumors. In light of the current findings, future exploration of the major cell lineage subsets in which the presence of OSA induces the increased expression of HIF-1α would be of potential interest to the understanding of the dynamic underpinnings regulating tumor growth and metastatic potential. We should also remark that the number of CM patients with very high expression of HIF-1α was small (n = 16) and reflects the quartile-based categorical stratification approach undertaken here, as dictated by statistical considerations. Indeed, expansion of the number of staining intensity categories such as to offer more refined analyses would have required a much large cohort size to achieve adequate statistical power.
Indeed, previous work has indicated that HIF-1α plays pathophysiological roles in some of the previously identified morbid consequences of the disease. For example, the IH of OSA has been shown to contribute to liver fibrosis via recruitment of HIF-1α signaling (45). Similarly, targeting HIF-1α-related pathways may attenuate cardiovascular and metabolic consequences of IH (46–50). Thus, it is reasonable to assume that increased HIF-1α expression in the context of sleep-disordered breathing in our cohort would lead to increased HIF-1α expression in tissues in general and more specifically in the CM lesions, where its transcriptional activity could have fostered increased proliferation and other aggressiveness indicators (14–16). In contrast, the absence of any significant association between VEGF expression in the CM sections and correlates of nocturnal hypoxemia was surprising. Indeed, previous studies have shown that circulating levels of VEGF are increased in OSA (51–54), suggesting that similar patterns may be present in tissues. However, the presence of an unfavorable balance between VEGF and endothelial and vascular factors that may promote vascular injury has been suggested in OSA and could reduce the efficacy of the VEGF pro-angiogenic activity (55). Alternatively, chronic IH may attenuate rather promote the transcription of HIF-1α at the promoter level of its gene targets as recently shown (50), such that the major driver for increased VEGF expression in the tumors could be the intrinsic intra-tumoral hypoxia rather than the IH of OSA. Under such circumstances, it is also possible that the increased VEGF expression may not necessarily reflect the severity of OSA or of intra-tumoral hypoxia, and may be driven by alternative transcriptional regulators such as HIF-2 (21). Notwithstanding, the presence of independent associations between a prognostic indicator of CM (i.e., Breslow index), and a measure of OSA severity (i.e., DI4%) as explaining the variance in HIF-1α expression abundance suggest that the presence of OSA and its severity may contribute to the malignant characteristics of CM, and play a deleterious role in the outcomes of this highly prevalent tumor.
Conclusion
In a large multicenter cohort of patients being diagnosed with CM, the expression of HIF-1α in the tumoral lesions is independently associated with nocturnal IH measures of sleep disordered breathing severity. These findings provide additional support to the evolving epidemiological and biological evidence whereby sleep apnea may play a deleterious role in cancer outcomes.
Other Members of the Spanish Sleep Network
Elidia Molina Herrera, Rosa M. García Martín, Pathology Department. Hospital 12 de octubre, Madrid, Spain; Maria Niveiro de Jaime, Pathology Department, ISABIAL, Hospital Gral, Univ. Alicante, Alicante, Spain, Departamento Medicina Clínica. Univ. Miguel Hernandez, Elche, Spain; Sara Moreno, Dermatology Department, Hospital Universitario Arnau de Vilanova, University of Lleida, IRBLleida, Lleida, Spain; Ferran Barbé Ilia, Respiratory Department, Group of Translational Research in Respiratory Medicine, Hospital Universitari Arnau de Vilanova and Santa Maria, IRBLleida, Lleida, Catalonia, Spain, Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Madrid, Spain; Manuel Sánchez de la Torre, Respiratory Department, Group of Translational Research in Respiratory Medicine, Hospital Universitari Arnau de Vilanova and Santa Maria, IRBLleida, Lleida, Catalonia, Spain, Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Madrid, Spain; Esther de Eusebio, Dermatology Department, Hospital Universitario de Guadalajara, Spain; Pedro Landete, Pneumology Service, Hospital la Princesa, Madrid, Spain; Manuel Moragón Gordon, Dermatology Department, Hospital Universitario, San Juan de Alicante, Spain; Eva Arias, Respiratory Department, Hospital 12 de Octubre, Madrid, Spain; Fernando Masa, Respiratory Department, Hospital Universitario S. Pedro Alcántara, Cáceres, Spain, Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Madrid, Spain; Carlos González Herrada, Dermatology Department, Hospital Universitario de Getafe, Madrid, Spain; Cristina Carrera, Dermatology Department, Hospital Clinic-IDIBAPS, Barcelona, Spain; Aida Muñoz Ferrer, Respiratory Department, Hospital Germans Trials y Pujol, Barcelona, Spain; Aram Boada, Dermatology Department, Hospital Germans Trials y Pujol, Barcelona, Spain; Ana Fortuna, Mercé Mayos, Respiratory Department, Hospital Santa Creu i Sant Pau, Barcelona, Spain; Jesús Gardeazabal García, Dermatology Department, Hospital Universitario Cruces, Bilbao, Spain.
Ethics Statement
The study was approved by the human ethics committees at the various participating sites, and written informed consent was obtained from each participant in accordance with the Declaration of Helsinki. The following human subject committtes provided approval for the study: Central Ethics Committee: Comité ético de investigación biomédica of Hospital Politécnico y Universitario La Fe de Valencia. Protocol # Cod 2012/1048 (includes subjects recruited at the hospitals La Fe, Manises y Instituto Valenciano de Oncologia). Comité ético de investigación clínica (CEIC) del Hospital Clinic de Barcelona. Protocol # 25042013. Comité ético de investigación clínica del Hospital General de Alicante. Agencia Valenciana de Salud. Protocol # 2013/030. Comité ético de investigación clínica del Hospital San Juan de Alicante. Agencia Valenciana de Salud. Código 12/304. Comité ético de investigación clínica y ensayos clínicos de Getafe. Protocol # A03-13. Comité ético de investigación clínica y ensayos clínicos de Guadalajara (SESCAM). Protocol # 19032013. Comitè d’Etica de la investigaciò del Hospital Germans Trials i Pujol. Protocol # PI13-074. Comitè d’Etica de la investigaciò del Hospital Santa Creu i Sant Pau. No protocol #. Comitè d’Etica de la investigaciò (CEIC) del Hospital Arnau de Vilanova de Lleida. Protocol # CEIC-1154. Comité ético de investigación clínica y ensayos clínicos de la Comunidad autónoma del País Vasco. Protocol # PI2014046. Informe del Comité local de ensatos clínicos. Valme. Protocol # 301012. Comité ético de investigación clínica y ensayos clínicos de Cáceres. No protocol #.
Author Contributions
IA, MM-G, FC-R, and DG participated in the conceptual framework of the project; MM-G., FC-R, ER-F, JR-P, EN, AM-C, LH-B, JR, EV, AS-T, JA-C, JM, AP-G, VC-N, IC-P, JC-P, TD-C, OM, and JD-A recruited patients and collected data and/or samples; MM-G, DG, IA, MM-G, FC-R, and RF interpreted data and drafted the manuscript. All authors approved the final version of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling Editor is currently co-organizing a Research Topic with one of the authors IA and confirms the absence of any other collaboration.
Funding
IA is supported by SEPAR (086/2014 and 595/2017). MM-G is supported by the Instituto de Salud Carlos III (PI16/01772) and cofinanced by the European Development Regional Find “A way to achieve Europe” (ERDF) and SEPAR (211/2012). ER-F is the recipient of a postdoctoral fellowship from “Fundación Científica de la Asociación Española Contra el Cáncer” and supported by FMM-2013/0075 of “Fundación Mutua Madrileña.” JR-P is supported by FIS 2014/1737 from the Spanish Ministry of Health. RF is supported in part by the Spanish Ministry of Economy and Competitiveness—Instituto de Salud Carlos III (FIS-PI14/00004); DG is supported by National Institutes of Health grant 1R01HL130984 and by the Herbert T. Abelson Chair in Pediatrics.
References
1. Glazer AM, Winkelmann RR, Farberg AS, Rigel DS. Analysis of trends in US melanoma incidence and mortality. JAMA Dermatol (2017) 153(2):225–6. doi:10.1001/jamadermatol.2016.4512
2. Lu X, Kang Y. Hypoxia and hypoxia-inducible factors: master regulators of metastasis. Clin Cancer Res (2010) 16(24):5928–35. doi:10.1158/1078-0432.CCR-10-1360
3. Vaupel P, Mayer A. Hypoxia in cancer: significance and impact on clinical outcome. Cancer Metastasis Rev (2007) 26(2):225–39. doi:10.1007/s10555-007-9055-1
4. Rohwer N, Cramer T. Hypoxia-mediated drug resistance: novel insights on the functional interaction of HIFs and cell death pathways. Drug Resist Updat (2011) 14(3):191–201. doi:10.1016/j.drup.2011.03.001
5. Keith B, Johnson RS, Simon MC. HIF1alpha and HIF2alpha: sibling rivalry in hypoxic tumour growth and progression. Nat Rev Cancer (2011) 12(1):9–22. doi:10.1038/nrc3183
6. Parks SK, Cormerais Y, Pouyssegur J. Hypoxia and cellular metabolism in tumour pathophysiology. J Physiol (2017) 595(8):2439–50. doi:10.1113/JP273309
7. Leung E, Cairns RA, Chaudary N, Vellanki RN, Kalliomaki T, Moriyama EH, et al. Metabolic targeting of HIF-dependent glycolysis reduces lactate, increases oxygen consumption and enhances response to high-dose single-fraction radiotherapy in hypoxic solid tumors. BMC Cancer (2017) 17(1):418. doi:10.1186/s12885-017-3402-6
8. Hanna SC, Krishnan B, Bailey ST, Moschos SJ, Kuan PF, Shimamura T, et al. HIF1alpha and HIF2alpha independently activate SRC to promote melanoma metastases. J Clin Invest (2013) 123(5):2078–93. doi:10.1172/JCI66715
9. Marconi A, Borroni RG, Truzzi F, Longo C, Pistoni F, Pellacani G, et al. Hypoxia-inducible factor-1alpha and CD271 inversely correlate with melanoma invasiveness. Exp Dermatol (2015) 24(5):396–8. doi:10.1111/exd.12679
10. Forsythe JA, Jiang BH, Iyer NV, Agani F, Leung SW, Koos RD, et al. Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol Cell Biol (1996) 16(9):4604–13. doi:10.1128/MCB.16.9.4604
11. Goodsell DS. The molecular perspective: VEGF and angiogenesis. Stem Cells (2003) 21(1):118–9. doi:10.1634/stemcells.21-1-118
12. Wang JY, Sun T, Zhao XL, Zhang SW, Zhang DF, Gu Q, et al. Functional significance of VEGF-a in human ovarian carcinoma: role in vasculogenic mimicry. Cancer Biol Ther (2008) 7(5):758–66. doi:10.4161/cbt.7.5.5765
13. Simonetti O, Lucarini G, Brancorsini D, Nita P, Bernardini ML, Biagini G, et al. Immunohistochemical expression of vascular endothelial growth factor, matrix metalloproteinase 2, and matrix metalloproteinase 9 in cutaneous melanocytic lesions. Cancer (2002) 95(9):1963–70. doi:10.1002/cncr.10888
14. Konstantina A, Lazaris AC, Ioannidis E, Liossi A, Aroni K. Immunohistochemical expression of VEGF, HIF1-a, and PlGF in malignant melanomas and dysplastic nevi. Melanoma Res (2011) 21(5):389–94. doi:10.1097/CMR.0b013e328347ee33
15. Mills CN, Joshi SS, Niles RM. Expression and function of hypoxia inducible factor-1 alpha in human melanoma under non-hypoxic conditions. Mol Cancer (2009) 8:104. doi:10.1186/1476-4598-8-104
16. Kuphal S, Winklmeier A, Warnecke C, Bosserhoff AK. Constitutive HIF-1 activity in malignant melanoma. Eur J Cancer (2010) 46(6):1159–69. doi:10.1016/j.ejca.2010.01.031
17. Gacevic M, Jovic M, Zolotarevski L, Stanojevic I, Novakovic M, Miller K, et al. Association of vascular endothelial growth factor expression with patohistological parameters of cutaneous melanoma. Vojnosanit Pregl (2016) 73(5):449–57. doi:10.2298/VSP140804027G
18. Brychtova S, Bezdekova M, Brychta T, Tichy M. The role of vascular endothelial growth factors and their receptors in malignant melanomas. Neoplasma (2008) 55(4):273–9.
19. Bayer-Garner IB, Hough AJ Jr, Smoller BR. Vascular endothelial growth factor expression in malignant melanoma: prognostic versus diagnostic usefulness. Mod Pathol (1999) 12(8):770–4.
20. Pisacane AM, Risio M. VEGF and VEGFR-2 immunohistochemistry in human melanocytic naevi and cutaneous melanomas. Melanoma Res (2005) 15(1):39–43. doi:10.1097/00008390-200502000-00007
21. Giatromanolaki A, Sivridis E, Kouskoukis C, Gatter KC, Harris AL, Koukourakis MI. Hypoxia-inducible factors 1alpha and 2alpha are related to vascular endothelial growth factor expression and a poorer prognosis in nodular malignant melanomas of the skin. Melanoma Res (2003) 13(5):493–501. doi:10.1097/01.cmr.0000056268.56735.4c
22. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet (2014) 383(9918):736–47. doi:10.1016/S0140-6736(13)60734-5
23. Levy P, Kohler M, McNicholas WT, Barbe F, McEvoy RD, Somers VK, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers (2015) 1:15015. doi:10.1038/nrdp.2015.15
24. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population—a review on the epidemiology of sleep apnea. J Thorac Dis (2015) 7(8):1311–22. doi:10.3978/j.issn.2072-1439.2015.06.11
25. Sanchez-de-la-Torre M, Campos-Rodriguez F, Barbe F. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med (2013) 1(1):61–72. doi:10.1016/S2213-2600(12)70051-6
26. Gileles-Hillel A, Kheirandish-Gozal L, Gozal D. Biological plausibility linking sleep apnoea and metabolic dysfunction. Nat Rev Endocrinol (2016) 12(5):290–8. doi:10.1038/nrendo.2016.22
27. Gozal D. CrossTalk proposal: the intermittent hypoxia attending severe obstructive sleep apnoea does lead to alterations in brain structure and function. J Physiol (2013) 591(Pt 2):379–81. doi:10.1113/jphysiol.2012.241216
28. Gozal D, Ham SA, Mokhlesi B. Sleep apnea and cancer: analysis of a nationwide population sample. Sleep (2016) 39(8):1493–500. doi:10.5665/sleep.6004
29. Gozal D, Farre R, Nieto FJ. Obstructive sleep apnea and cancer: epidemiologic links and theoretical biological constructs. Sleep Med Rev (2016) 27:43–55. doi:10.1016/j.smrv.2015.05.006
30. Martinez-Garcia MA, Campos-Rodriguez F, Barbe F. Cancer and OSA: current evidence from human studies. Chest (2016) 150(2):451–63. doi:10.1016/j.chest.2016.04.029
31. Almendros I, Wang Y, Becker L, Lennon FE, Zheng J, Coats BR, et al. Intermittent hypoxia-induced changes in tumor-associated macrophages and tumor malignancy in a mouse model of sleep apnea. Am J Respir Crit Care Med (2014) 189(5):593–601. doi:10.1164/rccm.201310-1830OC
32. Almendros I, Montserrat JM, Ramirez J, Torres M, Duran-Cantolla J, Navajas D, et al. Intermittent hypoxia enhances cancer progression in a mouse model of sleep apnoea. Eur Respir J (2012) 39(1):215–7. doi:10.1183/09031936.00185110
33. Almendros I, Montserrat JM, Torres M, Dalmases M, Cabanas ML, Campos-Rodriguez F, et al. Intermittent hypoxia increases melanoma metastasis to the lung in a mouse model of sleep apnea. Respir Physiol Neurobiol (2013) 186(3):303–7. doi:10.1016/j.resp.2013.03.001
34. Martinez-Garcia MA, Martorell-Calatayud A, Nagore E, Valero I, Selma MJ, Chiner E, et al. Association between sleep disordered breathing and aggressiveness markers of malignant cutaneous melanoma. Eur Respir J (2014) 43(6):1661–8. doi:10.1183/09031936.00115413
35. Nieto FJ, Peppard PE, Young T, Finn L, Hla KM, Farre R. Sleep-disordered breathing and cancer mortality: results from the Wisconsin Sleep Cohort Study. Am J Respir Crit Care Med (2012) 186(2):190–4. doi:10.1164/rccm.201201-0130OC
36. Li L, Lu J, Xue W, Wang L, Zhai Y, Fan Z, et al. Target of obstructive sleep apnea syndrome merge lung cancer: based on big data platform. Oncotarget (2017) 8(13):21567–78. doi:10.18632/oncotarget.15372
37. Owens RL, Gold KA, Gozal D, Peppard PE, Jun JC, Lippman SM, et al. Sleep and breathing … and cancer? Cancer Prev Res (Phila) (2016) 9(11):821–7. doi:10.1158/1940-6207.CAPR-16-0092
38. Dal MM, Brant A, Blackford AL, Griffin JF, Shindo K, Barkley T, et al. Obstructive sleep apnea and pathological characteristics of resected pancreatic ductal adenocarcinoma. PLoS One (2016) 11(10):e0164195. doi:10.1371/journal.pone.0164195
39. Almendros I, Khalyfa A, Trzepizur W, Gileles-Hillel A, Huang L, Akbarpour M, et al. Tumor cell malignant properties are enhanced by circulating exosomes in sleep apnea. Chest (2016) 150(5):1030–41. doi:10.1016/j.chest.2016.08.1438
40. Lee S, Kim BG, Kim JW, Lee KL, Koo DL, Nam H, et al. Obstructive sleep apnea is associated with an increased risk of colorectal neoplasia. Gastrointest Endosc (2017) 85(3):568–73. doi:10.1016/j.gie.2016.07.061
41. Vilaseca A, Nguyen DP, Vertosick EA, Corradi RB, Musquera M, Perez M, et al. Obstructive sleep apnea and Fuhrman grade in patients with clear cell renal cell carcinoma treated surgically. World J Urol (2017) 35(1):51–6. doi:10.1007/s00345-016-1830-6
42. Hakim F, Wang Y, Zhang SX, Zheng J, Yolcu ES, Carreras A, et al. Fragmented sleep accelerates tumor growth and progression through recruitment of tumor-associated macrophages and TLR4 signaling. Cancer Res (2014) 74(5):1329–37. doi:10.1158/0008-5472.CAN-13-3014
43. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol (2013) 177(9):1006–14. doi:10.1093/aje/kws342
44. Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med (2015) 3(4):310–8. doi:10.1016/S2213-2600(15)00043-0
45. Mesarwi OA, Shin MK, Bevans-Fonti S, Schlesinger C, Shaw J, Polotsky VY. Hepatocyte hypoxia inducible factor-1 mediates the development of liver fibrosis in a mouse model of nonalcoholic fatty liver disease. PLoS One (2016) 11(12):e0168572. doi:10.1371/journal.pone.0168572
46. Drager LF, Yao Q, Hernandez KL, Shin MK, Bevans-Fonti S, Gay J, et al. Chronic intermittent hypoxia induces atherosclerosis via activation of adipose angiopoietin-like 4. Am J Respir Crit Care Med (2013) 188(2):240–8. doi:10.1164/rccm.201209-1688OC
47. Semenza GL, Prabhakar NR. Neural regulation of hypoxia-inducible factors and redox state drives the pathogenesis of hypertension in a rodent model of sleep apnea. J Appl Physiol (1985) (2015) 119(10):1152–6. doi:10.1152/japplphysiol.00162.2015
48. Sacramento JF, Ribeiro MJ, Rodrigues T, Guarino MP, Diogo LN, Seica R, et al. Insulin resistance is associated with tissue-specific regulation of HIF-1alpha and HIF-2alpha during mild chronic intermittent hypoxia. Respir Physiol Neurobiol (2016) 228:30–8. doi:10.1016/j.resp.2016.03.007
49. Belaidi E, Morand J, Gras E, Pepin JL, Godin-Ribuot D. Targeting the ROS-HIF-1-endothelin axis as a therapeutic approach for the treatment of obstructive sleep apnea-related cardiovascular complications. Pharmacol Ther (2016) 168:1–11. doi:10.1016/j.pharmthera.2016.07.010
50. Gozal D, Gileles-Hillel A, Cortese R, Li Y, Almendros I, Qiao Z, et al. Visceral white adipose tissue after chronic intermittent and sustained hypoxia in mice. Am J Respir Cell Mol Biol (2017) 56(4):477–87. doi:10.1165/rcmb.2016-0243OC
51. Briancon-Marjollet A, Pepin JL, Weiss JW, Levy P, Tamisier R. Intermittent hypoxia upregulates serum VEGF. Sleep Med (2014) 15(11):1425–6. doi:10.1016/j.sleep.2014.07.006
52. Kahler CM, Wechselberger J, Molnar C, Prior C. Serum levels of vascular endothelial growth factor are elevated in patients with obstructive sleep apnea and severe night time hypoxia. Am J Respir Crit Care Med (2003) 167(1):92–3. doi:10.1164/ajrccm.167.1.368
53. Lavie L, Kraiczi H, Hefetz A, Ghandour H, Perelman A, Hedner J, et al. Plasma vascular endothelial growth factor in sleep apnea syndrome: effects of nasal continuous positive air pressure treatment. Am J Respir Crit Care Med (2002) 165(12):1624–8. doi:10.1164/rccm.20110-040OC
54. Gozal D, Lipton AJ, Jones KL. Circulating vascular endothelial growth factor levels in patients with obstructive sleep apnea. Sleep (2002) 25(1):59–65. doi:10.1093/sleep/25.1.59
Keywords: melanoma, intermittent hypoxia, obstructive sleep apnea, hypoxia-inducible factor, vascular endothelial growth factor
Citation: Almendros I, Martínez-García MÁ, Campos-Rodríguez F, Riveiro-Falkenbach E, Rodríguez-Peralto JL, Nagore E, Martorell-Calatayud A, Hernández Blasco L, Bañuls Roca J, Chiner Vives E, Sánchez-de-la-Torre A, Abad-Capa J, Montserrat JM, Pérez-Gil A, Cabriada-Nuño V, Cano-Pumarega I, Corral-Peñafiel J, Diaz-Cambriles T, Mediano O, Dalmau-Arias J, Farré R and Gozal D (2018) Intermittent Hypoxia Is Associated With High Hypoxia Inducible Factor-1α but Not High Vascular Endothelial Growth Factor Cell Expression in Tumors of Cutaneous Melanoma Patients. Front. Neurol. 9:272. doi: 10.3389/fneur.2018.00272
Received: 03 December 2017; Accepted: 06 April 2018;
Published: 26 April 2018
Edited by:
Lena Lavie, Technion – Israel Institute of Technology, IsraelReviewed by:
Slava Berger, Johns Hopkins Medicine, United StatesThomas Penzel, Charité Universitätsmedizin Berlin, Germany
Maria Rosaria Bonsignore, Università degli Studi di Palermo, Italy
Copyright: © 2018 Almendros, Martínez-García, Campos-Rodríguez, Riveiro-Falkenbach, Rodríguez-Peralto, Nagore, Martorell-Calatayud, Hernández Blasco, Bañuls Roca, Chiner Vives, Sánchez-de-la-Torre, Abad-Capa, Montserrat, Pérez-Gil, Cabriada-Nuño, Cano-Pumarega, Corral-Peñafiel, Diaz-Cambriles, Mediano, Dalmau-Arias, Farré and Gozal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Gozal, ZGdvemFsQHVjaGljYWdvLmVkdQ==