 Fernando Zanela Areas1,2Marcelo Liborio Schwarzbold1,2,3,4
Fernando Zanela Areas1,2Marcelo Liborio Schwarzbold1,2,3,4 Alexandre Paim Diaz1,4Igor Kunze Rodrigues3,5,6Daniel Santos Sousa3,7Camila Leite Ferreira8João Quevedo8,9Katia Lin1,3,10
Alexandre Paim Diaz1,4Igor Kunze Rodrigues3,5,6Daniel Santos Sousa3,7Camila Leite Ferreira8João Quevedo8,9Katia Lin1,3,10 Emil Kupek3,11
Emil Kupek3,11 Cristiane Ritter12,13
Cristiane Ritter12,13 Felipe Dal Pizzol3,12,13
Felipe Dal Pizzol3,12,13 Roger Walz1,2,3,10*
Roger Walz1,2,3,10*- 1Centro de Neurociências Aplicadas, Universidade Federal de Santa Catarina, Hospital Universitário, Florianópolis, Brazil
- 2Programa de Pós-Graduação em Neurociências, UFSC, Florianópolis, Brazil
- 3Programa de Pós-Graduação em Ciências Médicas, UFSC, Florianópolis, Brazil
- 4Serviço de Psiquiatria, Departamento de Clínica Médica, HU, UFSC, Florianópolis, Brazil
- 5Serviço de Neurocirurgia, HU, UFSC, Florianópolis, Brazil
- 6Serviço de Neurocirurgia, Hospital Regional de São José Homero de Miranda Gomes, São José, Brazil
- 7Serviço de Neurocirurgia, Hospital Governado Celso Ramos, Florianópolis, Brazil
- 8Laboratório de Neurociências, Programa de Pós-Graduação em Ciências da Saúde, Universidade do Extremo Sul Catarinense, Criciúma, Brazil
- 9Department of Psychiatry and Behavioral Sciences McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, TX, United States
- 10Serviço de Neurologia, Departamento de Clínica Médica, HU, UFSC, Florianópolis, Brazil
- 11Departmento de Saúde Pública, UFSC, Florianópolis, Brazil
- 12Hospital São José, Criciúma, Brazil
- 13Laboratório de Fisiopatologia Experimental, Programa de Pós-Graduação em Ciências da Saúde, UNESC, Criciúma, Brazil
Traumatic brain injury (TBI) is a worldwide social, economic, and health problem related to premature death and long-term disabilities. There were no prospective and multicentric studies analyzing the predictors of TBI related mortality and estimating the burden of TBI in Brazil. To address this gap, we investigated prospectively: (1) the hospital mortality and its determinants in patients admitted with severe TBI we analyzed in three reference centers; (2) the burden of TBI estimated by the years of life lost (YLLs) due to premature death based on the hospital mortality considering the hospital mortality. Between April 2014 and January 2016 (22 months), all the 266 patients admitted with Glasgow coma scale (GCS), ≤ 8 admitted in three TBI reference centers were included in the study. These centers cover a population of 1,527,378 population of the Santa Catarina state, Southern Brazil. Most patients were male (n = 230, 86.5%), with a mean (SD) age of 38 (17) years. Hospital mortality was 31.1% (n = 83) and independently associated with older age, worse cranial CT injury by the Marshall classification, the presence of subarachnoid hemorrhage in the CT, lower GCS scores and abnormal pupils at admission. The final multiple logistic regression model including these variables showed an overall accuracy for hospital mortality of 77.9% (specificity 88.6%, sensitivity 53.8%, PPV 67.7%, and NPV 81.1%). The estimated annual incidence of hospitalizations and mortality due to severe TBI were 9.5 cases and 5.43 per 100,000 inhabitants, respectively. The estimated YLLs in 22 months, in the 2 metropolitan areas were 2,841, corresponding to 1,550 YLLs per year and 101.5 YLLs per 100,000 people every year. The hospital mortality did not change significantly since the end of the 1990s and was similar to other centers in Brazil and Latin America. Significant predictors of hospital mortality were the same as those of studies worldwide, but their strength of association seemed to differ according to countries income. Present study results question the extrapolation of TBI hospital mortality models for high income to lower- and middle-income countries and therefore have implications for TBI multicentric trials including countries with different income levels.
Introduction
Traumatic brain injury (TBI) is a worldwide social, economic, and health problem related to premature death and long-term disabilities (1–5). Depending on the TBI severity and its complications, even in the absence of motor impairment, the TBI may result in cognitive deficits (6, 7), endocrine (8) and psychiatric disorders (9–11) affecting work capacity (12), and impairing the quality of life (9).
Based on their Gross National Income per capita value, the World Bank classified the countries as having lower, middle, or high income. It is believed the incidence and mortality of TBI are higher in lower- and middle-income countries (LMIC) than in high-income countries (HIC) (5, 13, 14). Differences in the rescue time and the medical care may result in a higher proportion of patients surviving with a disability in HIC in comparison to LMIC (13). Interestingly, the proportion of survivors patients remaining with disability following a severe TBI seems to be similar between LMIC and HIC, and patients LMIC shows better recovery after a mild or moderate TBI. The reduced levels of disability in LMIC may be partly explained by excess mortality following severe TBI, as well by the differences in the definition of disability between settings, socio-cultural and environmental particularities which affect how society interprets and reacts to disability (13).
In Brazil, like in several other LMIC, the TBI related mortality and morbidity are not systematically recorded and only two studies evaluated prospectively the hospital mortality of patients with TBI and determined its independent predictors (15, 16) In our previous single center, 748 patients from Florianópolis, the Santa Catarina State capital (Southern Brazil), admitted with coma Glasgow scale (GCS) ≤ 8 were included between January 1994 and December 2003 (16). Another Brazilian study included patients admitted at the emergency unit of the University of São Paulo Hospital with an admission GCS score who had an abnormal brain computerized tomography (CT) scan (n = 1,275) between September 2003 and December 2009. The older age, lower GCS, worse cranial Computed Tomography (CT) lesions by Marshall CT classification and the pupillary abnormality remained as independent predictors of hospital mortality in both studies. These predictors are associated with mortality and in TBI patients worldwide, although the strength of the association may differ according to the country's income level (3, 13). In both studies, the binary regression models showed a global accuracy for hospital mortality of 77%.
Diagnostic and therapeutic decisions are based on the patient's prognosis. Prognostic models are statistical models that combine two or more variables of patient's data to predict clinical outcome. There were no prospective and multicentric studies analyzing the predictors of TBI related mortality and estimating the burden of TBI in Brazil. To address this gap, we investigated prospectively: (1) the hospital mortality and its determinants in patients admitted with severe TBI we analyzed in three reference centers; (2) the burden of TBI estimated by the years of life lost (YLLs) due to premature death based on the hospital mortality considering the hospital mortality, the life expectancy, as well as the population covered by the TBI reference centers during the study period.
Methods
Patients
All patients with severe TBI admitted to the intensive care unities of three reference hospitals for brain trauma in the public health system of in Santa Catarina state, southern Brazil, between April 2014 and January 2016 (22 months) were included in this study. The Hospital Governador Celso Ramos (HGCR) in the city of Florianópolis and the Hospital Homero de Miranda Gomes (HHMG) in the city of São José cover the Greater Florianópolis metropolitan area with the population of 940,935 inhabitants. The Hospital São José (HSJ) in the city Criciúma, which covers another metropolitan area with 586,443 inhabitants also participate in this study. The population was determined by the official Brazilian Census Survey of 2014. Both metropolitan areas are crossed by the busiest national Brazilian highway (called BR-101), with a mean daily local traffic of 175,000 vehicles.
Inclusion criteria were GCS score 8 or lower after acute neurosurgical resuscitation, without sedation, or deterioration to that level within 48 h of the hospital admission. The same research protocol design was used in previous studies (6, 16–19).
Hospital Mortality, Predictive Variables, and Burden of TBI
The primary endpoint was in-hospital mortality. The demographic, clinical, neuroradiological, and neurosurgical analyzed variables were: gender, age, cause of TBI, Marshall classification of cranial CT, intracranial pressure monitoring (ICP), decompressive craniectomy, presence of subarachnoid hemorrhage (SAH) as evidenced by CT, associated trauma, admission GCS, admission pupils' response, reference trauma center, injury severity score (ISS), systolic and diastolic blood pressure at ICU admission, glucose, sodium, hemoglobin, and leucocyte at the ICU admission. These variables were included in the research protocol based on previous studies of other authors and our experience in severe TBI research (3, 4, 6–12, 16). All the CT scans were evaluated by the neurosurgeon and the ICU specialist. A decompressive craniectomy was done only in 13 (5%) patients, according to the personal decision of the neurosurgeon and other particularities including the age, hemodynamic state, the presence of multiple traumas. They had hemispheric edema and midline shift > 5 mm, diffuse brain edema with a refractory elevation of intracranial pressure, or when the neurosurgeon has the impression that the brain remains tense even after the mass lesions were evacuated.
To estimate the burden related to severe TBI we did the sum of the years of life lost (YLLs) due to premature mortality (20, 21) among patients who died during the hospitalization. We also estimated the cumulative YLLs per year. Because in Brazil virtually all cases of TBI are treated by the public health system at the reference centers for trauma, it was possible to estimate the YLLs per year per 100,000 inhabitants. The life expectancy reported by the Brazilian Institute of Geography and Statistics (IBGE) in the state of Santa Catarina in 2017 was 72.5 year for men and 79.6 years for women. The burden of severe TBI was determined according to the formulas below:
YLLs per patient = Life expectancy – age of death due to severe TBI
Cumulative YLLs in 22 months = ∑ (YLLs patient 1 + …. + YLLs patient 83
YLLs per year = (Cumulative YLLs in 22 months / 22) x 12
YLLs per year per 100,000 inhabitants = [YLLs per year / (Population)] x 100,000.
Statistical Analysis
After a descriptive analysis of patients' characteristics, we did a univariate binary logistic regression to identify the variables associated with hospital mortality with a type I error significance level ≤ 0.20 (see Table 1). These variables were included in the multiple binary regression model using a forward conditional method to determine the independent predictors of hospital mortality. Because the univariate analysis showed that Marshall III and Evacuated mass showed the same prognosis, they were categorized together in the multiple regression analysis. The ISS score was arbitrarily categorized using the mean ISS score of patients as the cut-off. The glucose levels were arbitrarily divided into 3 categories. Leukocytosis was defined as more than 11.000 leucocytes/mm3, and there were no patients with leukopenia in our sample. The magnitude of the association between the outcome and the independent variables was measured by the odds ratio (OR) and respective 95% confidence interval (CI). A type I error ≤ 0.05 was considered statistically significant. No adjustment for multiple comparisons was made because the independent variables included had a clinical relevance. The model discrimination was assessed by the area under the ROC curve generated using the predicted probabilities from the model. Statistical analysis was performed using the SPSS program 20.0 (Chicago, IL).

Table 1. Distribution of clinical, demographic, radiological, and neurosurgical variables of patients admitted with severe traumatic brain injury according to the hospital mortality.
The probability of death for an individual patient can be calculated based on the formula including the respective B coefficient for each category of the variables showed in the final regression model (see Table 2) using the formula below:
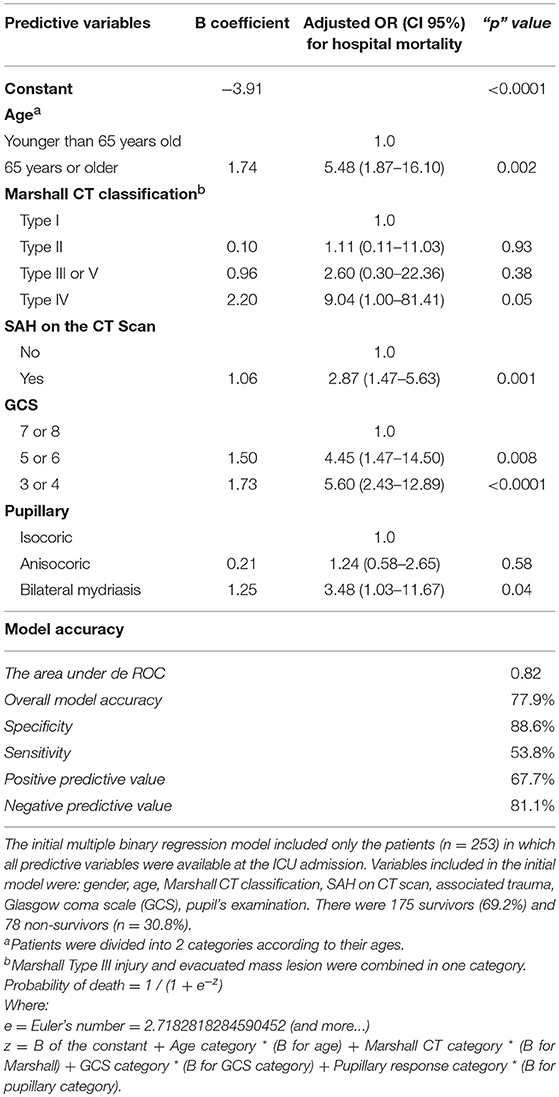
Table 2. The clinical, demographic, radiological, and neurosurgical variables independently associated with a hospital mortality of patients admitted with severe traumatic brain injury.
Probability of death = 1 / (1 + e−z)
Where:
e = Euler's number = 2.7182818284590452 (and more…)
z = B of the constant + variable A category * (B for variable A category) + variable B category * (B for variable B category) + variable C category * (B for variable C category) + variable D category * (B for variable D category)
B = Coefficients of the binary regression, for the constant and for each category of the variables included in the final binary regression model.
Results
There were 266 hospitalizations due to severe TBI resulting in 83 (31.1%) deaths during the study period of 22 months. Considering the population of 1,527,378 inhabitants covered by the participating centers, the hospitalization rate was 9.5 cases per 100,000 habitants per year and the mortality was 5.43 per 100,000 habitants per year. During the study period, there were 2,841 YLLs, corresponding to 1,550 YLLs per year and 101.5 YLLs per 100,000 people per year in the metropolitan areas analyzed.
Table 1 shows the distribution of demographic, clinical, radiological and neurosurgical characteristics of the patients admitted with severe TBI according to their hospital mortality. Hospital mortality was not associated with the TBI etiology, ICP monitoring, reference trauma center, and systemic blood pressure, sodium, hemoglobin levels at the ICU admission (p > 0.20). There was a trend for lower hospital mortality among patients with associated trauma other than TBI (p = 0.18), as well for increased hospital mortality among females (p = 0.15), older ages (p = 0.08), and leukocytosis at ICU admission (p = 0.06). The mortality was significantly higher among patients with worse injury on the CT scan according to Marshall CT classification (p < 0.05), presence of SAH on CT scan (p < 0.001), lower GCS score at ICU admission (p < 0.0001), higher ISS on ICU admission (p = 0.004), and higher glucose levels at ICU admission (p < 0.01).
Table 2 shows the clinical, demographic, radiological, and neurosurgical variables independently associated with hospital mortality, as determined by the binary multiple regression analysis. Older age, worse lesion on Marshall CT classification, the presence of SAH, lower GCS scores and abnormal pupils' examination at ICU admission remained independently associated with the hospital mortality. The final model showed an overall accuracy of 77%, with a specificity of 88.5%, and a sensitivity of 53%. Because the gunshot wounds constitute a separate population from blunt injury, we did a multiple binary regression using the variables shown in Table 2 and including the cause of TBI, attributing 1 to the OR for death by physical aggression. The accuracy of the model remains the same. There was a non-significant trend for higher mortality in the severe TBI caused by gunshot (Adjusted OR 4.3, CI 95% 0.6 to 33.3, p = 0.15) than physical aggression (data not shown).
We also ran a multiple binary logistic regression model including the variables gender, age, Marshall CT classification, SAH on CT scan, pupils' examination, injury severity score (ISS), GCS, glucose levels, and leukocytes levels at ICU admission. For this analysis, 113 patients had all these predictive variables available at the ICU admission. The age, SAH on CT scan, pupil's examination and ISS score (instead of GCS) remained in the model which showed an overall accuracy of 77%, with a specificity of 90.2%, and a sensitivity of 41.9% (details not shown).
Discussion
This is the first prospective, a multicentric study assessing hospital mortality due to severe TBI in Brazil. The results were similar to our (16) and others (15, 22) previous single-center studies in Brazil and multicentric studies in Latin America (14, 23). The hospital mortality in the present study was similar in the three centers analyzed (range between 28.5 to 36.1%) and did not change significantly in comparison to the mortality registered in the city of Florianópolis, at the HGCR, between 1994 and 2003 (16). A large Chinese retrospective TBI study (n = 7,145) from 47 hospitals recruited between 1 December 2008 and 20 August 2009 showed a 21.8% hospital mortality among the 1626 (22.8%) patients admitted with GCS ≤ 8, which was closer to the observed in HIC and lower than in Brazil and other LMIC (24). Although the differences in the medical care between HIC and LMIC countries may exist, we believe the delay between the accident and the effective rescue and hospitalization is an important factor that contributes to the higher mortality of our patients with severe TBI in our center in comparison to HIC. Unfortunately, during the course of this study, we did not obtain reliable information to investigate this hypothesis.
We show that older age, Marshall CT classification, presence SAH on the CT scan, lover GCS scores, and pupillary abnormalities were independent predictors of hospital mortality. Our results are in agreement with the International Mission on Prognosis and Analysis of Clinical Trials in TBI study (IMPACT) (25) The regression model including these variables showed a similar accuracy (77.9%) to predict the hospital mortality as two previous prospective studies conducted at the HGCR in the city of Florianópolis between 1994 and 2003 (16) and at the São Paulo university hospital between 2003 and 2009 (15). The lower mortality observed in São Paulo compared to the present study may be due to the inclusion of some patients with higher GCS scores (range between 3 and 15) as opposed to the patients with severe TBI (GCS ≤ 8) in the present study. In accordance to the São Paulo study (15), we did not confirm our previous study evidencing the association between the concomitant thoracic trauma and lower hospital mortality (16), and we have none plausible explanation for this conflicting results. Interestingly, although hormonal (18), immunologic (19), or biochemical markers (17) in the blood collected during the acute phase of severe TBI has been associated to hospital mortality and sometimes even improved the prognostic models, the age, pupillary examination and GCS score at admission always remained independently associated with hospital mortality in our previous studies (17–19). This indicated the consistency of these variables to predict hospital mortality in our population.
Based on the regression model described by Junior et al. in the aforementioned São Paulo study (15), the probability of death during hospitalization in a Brazilian patient with 65-year-old age, with a GCS of 7, a Marshall CT classification of 4, and isochoric pupils is estimated to be around 47.7%. Based on the present study, the estimated mean probability for hospital death for the patient described above was about 50.7%. For this analysis, subarachnoid hemorrhage in the CT was considered absent because this variable was not analyzed in the São Paulo study. However, if the same patient had a CT with subarachnoid hemorrhage the probability of death would rise to 75% in our model. For comparison, we also applied the well-known CRASH model to the same hypothetical Brazilian patient above. Because in our protocol we did not evaluate the presence of petechial hemorrhages and no obliteration of the third ventricle or basal cisterns, we run the CRASH model in the absence of both variables, which results in 46%. Including petechial hemorrhages, the risk increases to 52.5% and if the patients also had obliteration of the third ventricle or basal cisterns the risk became 68.7%. Because the CRASH model is applicable to patients up to 8 h after the accident, the reader should be aware of the lack of confirmation of the time course between the accident and hospitalization in our sample.
In the present study, the burden of severe TBI was estimated by the YLLs metrics based on hospital mortality. This approach did not take into account patients who died after the hospitalization, resulting in an underestimation of the YLLs in our sample. Based on our clinical observation, we believe the mortality in the first year after the hospitalization can be up to 15%, but this remains to be confirmed by further empirical studies. One randomized, prospective, multicentric trial on intracranial-pressure monitoring (23) in Bolivia and Ecuador (n = 324) shows a 14-day mortality of 25.5% which increased to 40% in the 6 months after hospitalization.
The reader should be aware of some the limitations of our study: (i) the sample was comprised by patients with severe TBI and admitted to a reference trauma facility, which may limit generalizability to non-reference center; (ii) the lower number of cases and variability in decision criteria for decompressive craniectomy does not allow to establish acceptable conclusions about the impact of this therapeutic modality on hospital mortality of our patients; (iii) the outcome was restricted to hospital mortality; (iv) the burden of TBI was estimated based on the hospital mortality and not the disability-adjusted life years (DALYs); (v) because 2 of the 3 hospitals involved in this study are references for trauma occurring at BR-101, the busiest Brazilian highway that runs through diverse metropolitan areas, some of the included patients maybe were not living in the cities of the metropolitan areas used to estimate the population in risk for severe TBI. Nevertheless, the strengths of our study are: (i) the prospective and multicentric study design; (ii) acute patients with severe TBI in the geographic areas of the study are almost exclusively assisted by the three participating reference centers, implying the inclusion of virtually all severe TBI patients in these regions during the period of study; (iii) this is the first prospective study estimating the disease burden of TBI in Brazilian patients.
Conclusions
This is the first multicentric and prospective study on hospital mortality and the burden of TBI based on YLLs in Brazil. The burden of TBI determined by disability-adjusted life years (DALYs) remains to be investigated in Brazil. Older age, Marshall CT classification, presence SAH on the CT scan, lower GCS scores, and pupillary abnormalities are independent predictors of hospital mortality. The hospital mortality due to severe TBI was similar to those from other trauma centers in Brazil and Latin America and did not change significantly since the end of the 1990s. Present study findings are in agreement with the view that extrapolation from predictive TBI models in HIC to LMIC may lead to inaccurate estimation of TBI-related hospital mortality. These results have implications for further TBI multicentric trials including countries with different income levels.
Ethics Statement
This study was carried out in accordance with the recommendations of Comitê de Ética em Pesquisa em Seres Humanos da Universidade (Plataforma Brazil Registration 02832612.6.1001.0121). Informed consent to participate was signed by each patient's family.
Author Contributions
AD, JQ, KL, EK, FD, and RW: study design, literature revision, manuscript revision. RW and FD: statistical analysis and manuscript writing. FA, IR, MS, DS, CF, CR, and FD: data collection, and manuscript revision.
Funding
This work was supported by PRONEX Program (NENASC Project, process 56802/2010) and PPSUS Program (TO 201302248) of FAPESC-CNPq-MS, Santa Catarina, Brazil. RW, KL, EK, CR, and FD are Research Fellows from CNPq (Brazilian Council for Science and Technology Development). FA received a fellowship for his Ph.D. degree from Fundação de Amparo a Pesquisa do Estado do Amazonas (FAPEAM).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Roozenbeek B, Maas AIR, Menon DK. Changing patterns in the epidemiology of traumatic brain injury. Nat Rev Neurol. (2013) 9:231–6. doi: 10.1038/nrneurol.2013.22
2. Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung Y-C, Punchak M, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. (2018) 130:1039–408. doi: 10.3171/2017.10.JNS17352
3. Perel PA, Arango M, Clayton T, Edwards P, Komolafe E, Poccock S, et al. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ. (2008) 336:425–9. doi: 10.1136/bmj.39461.643438.25
4. Steyerberg EW, Mushkudiani N, Perel P, Butcher I, Lu J, Mchugh GS, et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. (2008) 5:e165. doi: 10.1371/journal.pmed.0050165
5. Rubiano AM, Carney N, Chesnut R, Puyana JC. Global neurotrauma research challenges and opportunities. Nature. (2015) 527:S193–7. doi: 10.1038/nature16035
6. De Souza RL, Thais ME, Cavallazzi G, Diaz AP, Schwarzbold ML, Nau AL, et al. Side of pupillary mydriasis predicts the cognitive prognosis in patients with severe traumatic brain injury. Acta Anaesthsiol Scand. (2015) 59:392–405. doi: 10.1111/aas.12447
7. De Oliveira Thais MER, Cavallazzi G, Formolo DA, De Castro LDA, Schmoeller R, Guarnieri R, et al. Limited predictive power of hospitalization variables for long-term cognitive prognosis in adult patients with severe traumatic brain injury. J Neuropsychol. (2014) 8:125–39. doi: 10.1111/jnp.12000
8. Hohl A, Daltrozo JB, Pereira CG, Weber TR, Pinto HF, Gullo JS, et al. Late evaluation of the pituitary-gonadal axis in survivors of severe traumatic brain injury. Arq Bras Endocrinol Metabol. (2009) 53: 1012–9. doi: 10.1590/S0004-27302009000800016
9. Diaz AP, Schwarzbold ML, Thais ME, Hohl A, Bertotti MM, Schmoeller R, et al. Psychiatric disorders and health-related quality of life after severe traumatic brain injury: a prospective study. J Neurotrauma. (2012) 29:1029–37. doi: 10.1089/neu.2011.2089
10. Schwarzbold M, Diaz A, Hohl A, Linhares MN, Walz R, Martins ET, et al. Psychiatric disorders and traumatic brain injury. Neuropsychiatr Dis Treat. (2008) 4:797–816. doi: 10.2147/NDT.S2653
11. Schwarzbold ML, Diaz AP, Nunes JC, Sousa DS, Hohl A, Guarnieri R, et al. Validity and screening properties of three depression rating scales in a prospective sample of patients with severe traumatic brain injury. Rev Bras Psiq. (2014) 36:8–11. doi: 10.1590/1516-4446-2013-1308
12. Diaz AP, Schwarzbold ML, Thais ME, Cavallazzi G, Schmoeller R, Nunes JC, et al. Personality changes and return to work after severe traumatic brain injury: a prospective study. Rev Bras Psiq. (2014) 36:213–9. doi: 10.1590/1516-4446-2013-1303
13. de Silva MJ, Roberts I, Perel P, Edwards P, Kenward MG, Fernandes J, et al. Patient outcome after traumatic brain injury in high-, middle- and low-income countries: analysis of data on 8927 patients in 46 countries. Int J Epidemiol. (2009) 38:452–8. doi: 10.1093/ije/dyn189
14. Bonow RH, Barber J, Temkin NR, Videtta W, Rondina C, Petroni G, et al. The outcome of severe traumatic brain injury in Latin America. World Neurosurg. (2018) 111:2–5. doi: 10.1016/j.wneu.2017.11.171
15. Junior JR, Welling LC, Schafranski M, Yeng LT, do Prado RR, Koterba E, et al. Prognostic model for patients with traumatic brain injuries and abnormal computed tomography scans. J Clin Neurosci. (2017) 42:122–8. doi: 10.1016/j.jocn.2017.03.012
16. Martins ET, Linhares MN, Sousa DS, Schroeder HK, Meinerz J, More M, et al. Mortality in severe traumatic brain injury: a multivariated. J Trauma. (2009) 67:85–90. doi: 10.1097/TA.0b013e318187acee
17. Hohl A, Gullo JDS, Silva CCP, Bertotti MM, Felisberto F, Nunes JC, et al. Plasma levels of oxidative stress biomarkers and hospital mortality in severe head injury: a multivariate analysis. J Crit Care. (2012) 27:e11–9. doi: 10.1016/j.jcrc.2011.06.007
18. Hohl A, Ronsoni MFMF, Debona R, Ben J, Schwarzbold ML, Diaz AP, et al. Role of hormonal levels on hospital mortality for male patients with severe traumatic brain injury. Brain Inj. (2014) 28:1262–9. doi: 10.3109/02699052.2014.915986
19. Schneider FMS, De Souza MN, Librio Schwarzbold M, Paim Diaz A, Costa Nunes J, Hohl A, et al. Interleukin-10 is an independent biomarker of severe traumatic brain injury prognosis. Neuroimmunomodulation. (2012) 19: 377–85. doi: 10.1159/000342141
20. Murray CJL, Lopez AD. The global burden of disease: a comprehensive assessment of mortality and disability from deceases, injuries and risk factors in 1990 and projected to 2010. Harvard Univ Press. (1996) 1:1–35. doi: 10.1186/1471-2458-13-863
21. Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, Abdulkader RS, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1260–344. doi: 10.1016/S0140-6736(17)32130-X
22. da Costa LGV, Carmona MJC, Malbouisson LM, Rizoli S, Rocha-Filho JA, Cardoso RG, et al. Independent early predictors of mortality in polytrauma patients: a prospective, observational, longitudinal study. Clinics. (2012) 72:461–8. doi: 10.6061/clinics/2017(08)02
23. Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, et al. A trial of intracranial-pressure monitoring in traumatic brain injury. N Eng J Med. (2012) 367:2471–81. doi: 10.1056/NEJMoa1207363
24. Jiang JY, Xu SY, Zhou ZW, Yang YL, Qing HP, Qian SK, et al. Head trauma in China. Injury. (2013) 44:1453–7. doi: 10.1016/j.injury.2012.08.045
Keywords: traumatic brain injury, mortality, prognosis, burden of disease, Brazil
Citation: Areas FZ, Schwarzbold ML, Diaz AP, Rodrigues IK, Sousa DS, Ferreira CL, Quevedo J, Lin K, Kupek E, Ritter C, Dal Pizzol F and Walz R (2019) Predictors of Hospital Mortality and the Related Burden of Disease in Severe Traumatic Brain Injury: A Prospective Multicentric Study in Brazil. Front. Neurol. 10:432. doi: 10.3389/fneur.2019.00432
Received: 16 November 2018; Accepted: 09 April 2019;
Published: 25 April 2019.
Edited by:
Leonardo Cruz de Souza, Federal University of Minas Gerais, BrazilReviewed by:
Marco Fidel Avila-Rodriguez, Universidad del Tolima, ColombiaJohn K. Yue, University of California, San Francisco, United States
Copyright © 2019 Areas, Schwarzbold, Diaz, Rodrigues, Sousa, Ferreira, Quevedo, Lin, Kupek, Ritter, Dal Pizzol and Walz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roger Walz, cm9nZXJ3YWx6QGhvdG1haWwuY29t