 Anna Lindner1
Anna Lindner1 Mario Kofler1
Mario Kofler1 Verena Rass1
Verena Rass1 Bogdan Ianosi1,2
Bogdan Ianosi1,2 Max Gaasch1
Max Gaasch1 Alois J. Schiefecker1
Alois J. Schiefecker1 Ronny Beer1Sebastian Loveys1Paul Rhomberg3Bettina Pfausler1Claudius Thomé4Erich Schmutzhard1
Ronny Beer1Sebastian Loveys1Paul Rhomberg3Bettina Pfausler1Claudius Thomé4Erich Schmutzhard1 Raimund Helbok1*
Raimund Helbok1*- 1Neurological Intensive Care Unit, Department of Neurology, Medical University of Innsbruck, Innsbruck, Austria
- 2Institute of Medical Informatics, University for Health Sciences, Medical Informatics and Technology, Hall, Austria
- 3Department of Neuroradiology, Medical University of Innsbruck, Innsbruck, Austria
- 4Department of Neurosurgery, Medical University of Innsbruck, Innsbruck, Austria
Background: Infectious complications (IC) commonly occur in patients with intracerebral hemorrhage (ICH) and are associated with increased length of hospitalization (LOS) and poor long-term outcome. Little is known about early ICH-related predictors for the development of IC to allow appropriate allocation of resources and timely initiation of preventive measures.
Methods: We prospectively enrolled 229 consecutive patients with non-traumatic ICH admitted to the neurocritical care unit (NICU) of a tertiary care hospital. Patients were screened daily for IC. Multivariable regression models using generalized linear models were used to identify associated factors with the occurrence of IC and to study their impact on functional outcome, which was assessed using the modified Rankin Scale Score (mRS) after 3 months. Unfavorable outcome was defined as mRS ≥3.
Results: The most common IC were pneumonia (n = 64, 28%) and urinary tract infection (n = 54, 24%), followed by sepsis (n = 9, 4%) and ventriculitis (n = 4, 2%). Patients with a higher admission ICH Score (>2) had higher odds to develop any IC during NICU stay (OR = 1.7, 95% CI 1.2–2.3, p = 0.02). Moreover, early-onset pneumonia (≤48 h after admission) was predictive of sepsis occurring at a later time-point (median at day 11 [IQR = 6–34 days], adjOR = 22.5, 95% CI 4.88–103.6, p < 0.001). Having at least one IC and pneumonia itself were independently associated with unfavorable 3-months outcome (adjOR = 3.0, 95% CI 1.41–6.54, p = 0.005; adjOR = 4.2, 95% CI 1.33–13.19, p = 0.015, respectively). All patients with sepsis died or had poor functional outcome.
Conclusions: Infectious complications are common in ICH patients and independently associated with unfavorable outcome. An ICH Score >2 on admission and early pneumonia may help to early identify patients at high risk of IC to allocate resources and start careful surveillance.
Introduction
Intracerebral hemorrhage (ICH) accounts for 9–27% of all strokes worldwide and is associated with high rates of disability and mortality (1). Approximately 40% of ICH patients die within 30 days and 55% within the first year (2). The majority of surviving patients are functionally disabled with only 12–39% reaching long-term functional independence (3, 4). Besides the primary brain damage secondary complications largely contribute to poor functional outcome (5, 6). Consequently, the prevention and adequate treatment of secondary complications, including infections, together with early risk stratification of these patients is of high interest (7). During NICU stay up to 70% of ICH patients are known to develop at least one complication (8) and 23–58% of patients may suffer from infectious complications (IC) (7, 9–12). While it is well-known that infections complicate hospital course and are associated with poor functional outcome, little is known about their chronological occurrence and their cumulative effect on outcome. Furthermore, it is not well-described if early infections trigger late infectious complications. The ICH Score (13) has recently been shown to be the most extensively validated severity score in ICH patients (14) and is commonly used in clinical practice to stratify mortality risk after ICH. However, its role in the prediction of infectious complications is unclear.
In this study, we intended [1] to investigate the chronological course of IC, [2] to identify early, potentially modifiable predictors including the ICH Score for the development of infections after ICH, and [3] to investigate whether early infections are predictive of later complications. Moreover, we aimed to [4] quantify the impact of IC on the length of NICU stay and functional outcome. We hypothesized that the ICH Score is a useful tool in IC prediction and that IC are associated with poor functional outcome.
Methods
Patient Selection and Care
Two hundred ninety-one consecutive patients with non-traumatic ICH admitted to the neurological ICU (NICU) at a tertiary care hospital between 2011 and 2016 were prospectively enrolled. Inclusion criteria were: (a) spontaneous ICH diagnosed on computed tomography (CT) or magnetic resonance imaging (MRI), (b) age > 18 years, (c) written informed consent according to local regulations in accordance with the declaration of Helsinki, and (d) completed follow-up at 3 months. 32/291 patients did not give consent to participate or were lost to follow-up. Another 30/291 patients were excluded because of early treatment withdrawal, leaving 229 patients eligible for the current analysis. Withdrawal of care was decided following the criteria of age >80 years, limited life expectancy due to comorbidities and massive ICH with clinical or radiographic signs of herniation (Figure 1). Approval for the study was granted by the hospital's institutional review board (Medical University Innsbruck, AN4088292/4.3).
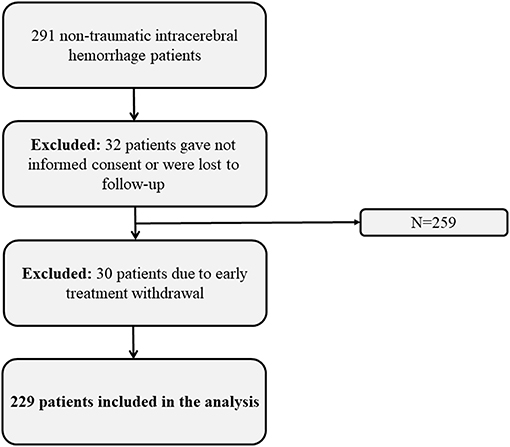
Figure 1. Flow chart showing the selection of eligible patients.
Clinical Management, Data Collection, Clinical and Radiographic Variables and Outcome
Following the local policy all patients diagnosed with an ICH are primarily admitted to an ICU. Less than 3% of patients were admitted to the stroke unit due to lack of available beds in the NICU during the study period. Patients' and disease specific characteristics, treatment interventions, hospital complications and outcomes were prospectively recorded in the institutional ICH database during weekly meetings held by the study team and treating neurointensivists. The Glasgow Coma Scale Score (GCS), the Acute Physiology And Chronic Health Evaluation (APACHE)—II (15), and the ICH Score (13) on admission, were used for clinical and radiographic grading. Clinical management conformed to American Heart Association and European Stroke association guidelines (5, 16). Vital signs and laboratory data were saved in a patient data management system (PDMS) (Centricity™ Critical Care 8.1 SP7; GE Healthcare Information Technologies, Germany).
Early neurological deterioration was defined as ≥2 points decrease in GCS or a new focal finding occurring within a 24 h period after admission or in the early postoperative phase. Mechanical ventilation, nasogastric tube feeding, hydrocephalus requiring external ventricular drain (EVD) placement and hematoma evacuation were determined as hospital-related procedures. Survival and functional outcome was assessed at 3 months after ictus by a study nurse blinded to the clinical course of the patient using the modified Rankin Scale Score (mRS) (17), with unfavorable outcome defined as mRS ≥3.
Definitions of Infectious Complications
Infectious complications were prospectively confirmed in a weekly study meeting and the date of onset was recorded, according to predefined criteria set forth by the Centers for Disease Control and Prevention criteria (CDC-criteria) (18), and the American Thoracic Society (19). Pneumonia was diagnosed in patients who had a new or progressive pulmonary infiltrate with clinical evidence of an infectious origin (two out of three: new onset of fever (≥38.3°C), leukocytosis (>12,000/mm3) or leukopenia (<4,000/mm3), purulent sputum). Pneumonia diagnosed within 48 h after admission was defined as early onset pneumonia, whereas pneumonia occurring >48 h after initiation of mechanical ventilation was defined as ventilator associated pneumonia (VAP) (19). Urinary tract infection (UTI) was diagnosed in patients with a positive microbiological culture of urine (105 colony forming units (CFU)/mL) with a maximum of two species of organisms and the occurrence of one of the following symptoms: fever (≥38.3°C), high frequency, urgency, dysuria, or suprapubic tenderness. Sepsis was defined according to the CDC-criteria (18) by either [1] isolation of pathogenic organisms in the blood culture, which could not be related to an infection at another location or [2] at least one of the following three clinical conditions: fever (≥38.3°C), chills, or hypotension (systolic blood pressure <100 mmHg) and any of the following: (a) common skin contaminant isolated from two blood cultures drawn on separate occasions, (b) common skin contaminant isolated from patient's blood culture with intravascular access device and physician institutes appropriate antimicrobial therapy, or (c) positive antigen test on blood and organism is not related to infection at another site. Ventriculitis was defined according to the CDC-criteria: presentation of pathogens in cerebrospinal fluid (CSF) culture, or in patients who had one of these conditions: fever (≥38.3°C), headache, meningism or cranial nerve signs, and at least one of the following findings in the CSF analysis: an increase in leukocytes, elevated protein and/or decreased glucose, positive culture, a positive antigen detection, detection of pathogens or antigens in the blood or an increased diagnostic single antibody titer (18). If the same infectious complication occurred twice during NICU stay, only the first occurrence was rated. First line antimicrobial treatment included ampicillin/sulbactam, doxycycline, or fluoroquinolones, followed by second line escalation therapy including aminopenicillin (piperacillin/tazobactam) or macrolide antibiotics. Third line treatments included vancomycin or linezolid against gram-positive rods and meropenem or cefepime for resistant gram-negative rods.
Statistical Analysis
Statistical analysis was performed using IBM-SPSS V24.0 (SPSS Inc, Armonk, NY). Continuous variables were assessed for normality using Shapiro-Wilk test. Values were reported as median and interquartile range [IQR]. We performed univariate analysis to identify clinically relevant risk factors for every type of IC using generalized linear models with a binary logistic function. Significantly associated factors (p < 0.1) in univariate analysis were included stepwise in multivariable logistic regression models using generalized linear models with a binary logistic function and Logit as link function and retained if significant (p < 0.05). The ICH Score was kept in all models as ordinal independent variable irrespective of its significance in order to account for disease severity. Factors associated with poor functional outcome were identified using the same approach and entered in multivariable generalized linear models. Of note, except the infratentorial hemorrhage location, all subcategories of the ICH Score were associated with poor outcome in univariate analysis.
ROC (receiver operating characteristic) curves were calculated for the ICH Score and each subcategory with the development of infectious complications as categorical variable. AUC for the ICH Score and GCS on admission were similar, however, based on the best model of fit (Akaike's Information Criterion, AIC), the predictive value of the ICH Score was significantly better as compared to the admission GCS Score. Moreover, a cox proportional-hazards regression was used, and the ICH Score was dichotomized at >2 and ≤2 based on the median. Furthermore, the median revealed the optimal cut-off point of the ICH Score for IC prediction evaluated by the Youden index to find the maximal sum of sensitivity and specificity. Statistical significance was judged to a p-value <0.05.
Results
General Characteristics
Patient characteristics, hospital complications and outcomes are presented in Table 1. Sixty-three patients/229 (28%) were comatose on admission. Hematoma location was supratentorial in 206 patients (90%) [cortical: 78 (34%), subcortical white matter: 39 (17%), basal ganglia: 55 (24%), thalamic: 34 (15%)] and infratentorial in 26 patients (10%) [cerebellum: 13 (6%), brainstem: 7 (3%)]. Fifty-six patients (25%) underwent hematoma evacuation within 24 h after admission. In-hospital mortality was 26% (n = 60).
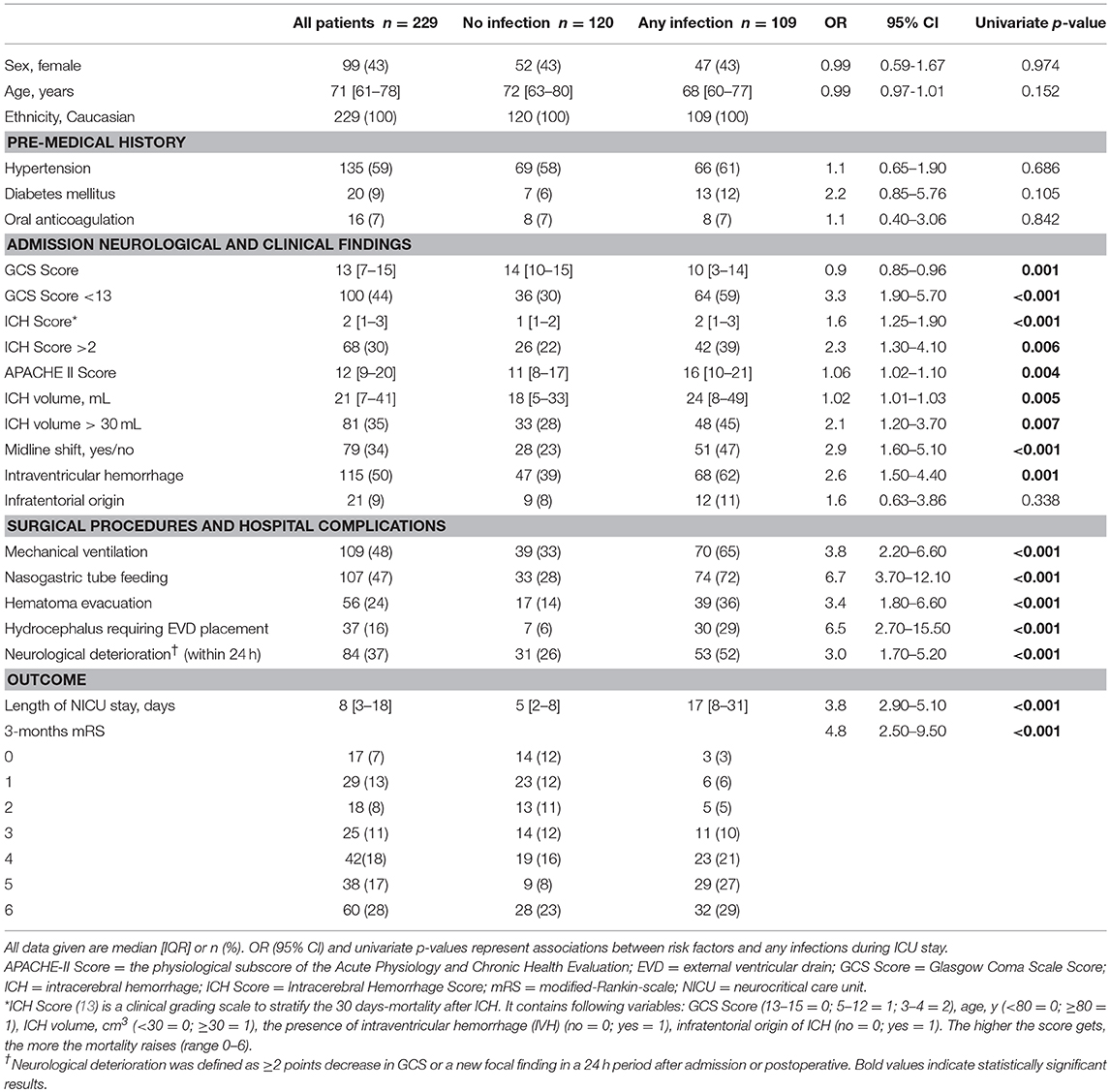
Table 1. Baseline characteristics, complications, and outcome.
Prevalence and Chronologic Course of Infectious Complications
During NICU stay, a total of 109 (48%) patients developed at least one infection. The most common IC were pneumonia (n = 64; 28%), UTI (n = 54; 24%), sepsis (n = 9; 4%) and ventriculitis (n = 4; 2%) (Figures 2A–D). Thirty-one percent (n = 71) of patients developed one infection, 13% (n = 30) two, 3% (n = 7) three, and 0.4% (n = 1) of patients four. In non-mechanically ventilated patients, pneumonia was diagnosed in 10 (4%) patients within the early phase and in 8 (3%) patients in the late phase after ictus. IC showed an initial peak (≤48 h after admission) attributable to early-onset pneumonia (65%) and a second peak at days 6–7 [IQR 4–12 days], associated with VAP (76%). In addition, we found another peak around day 16 most likely associated with catheter-related infections and sepsis (Figure 3). In 42% (27/64) of patients with pneumonia a positive bacterial culture was obtained identifying gram-negative (18/27, 67%) and gram-positive rods (9/27, 33%). Patients diagnosed with UTI had corresponding positive bacterial cultures in 84% (45/54, gram-negative rods: 35/45, 78%, gram-positive rods: 10/45, 22%). In 50% (2/4) of patients with ventriculitis gram-positive rods were found. All patients with sepsis had a positive bacterial culture (9/9, gram-negative rods: 4/9, 44%, gram-positive rods: 5/9, 56%).
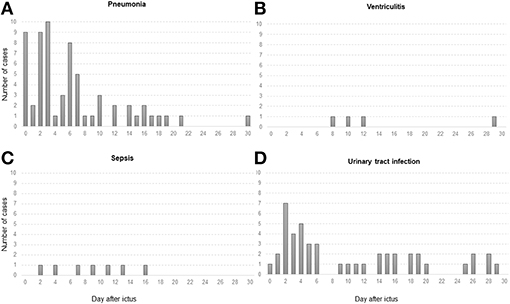
Figure 2. Graphs display absolute numbers of cases with infectious complications (y-axis) based on days after admission (x-axis) for (A) pneumonia, (B) ventriculitis, (C) sepsis, and (D) UTI (urinary tract infection). Pneumonia and UTI were mainly diagnosed in the first week after ictus (day 5 [IQR 2–9 days]; day 11 [IQR 3–25 days], respectively), whereas sepsis (C) and ventriculitis (B) occurred more frequently in the second week (day 11 [IQR 6–34 days]; day 11 [IQR 9–25 days], respectively).
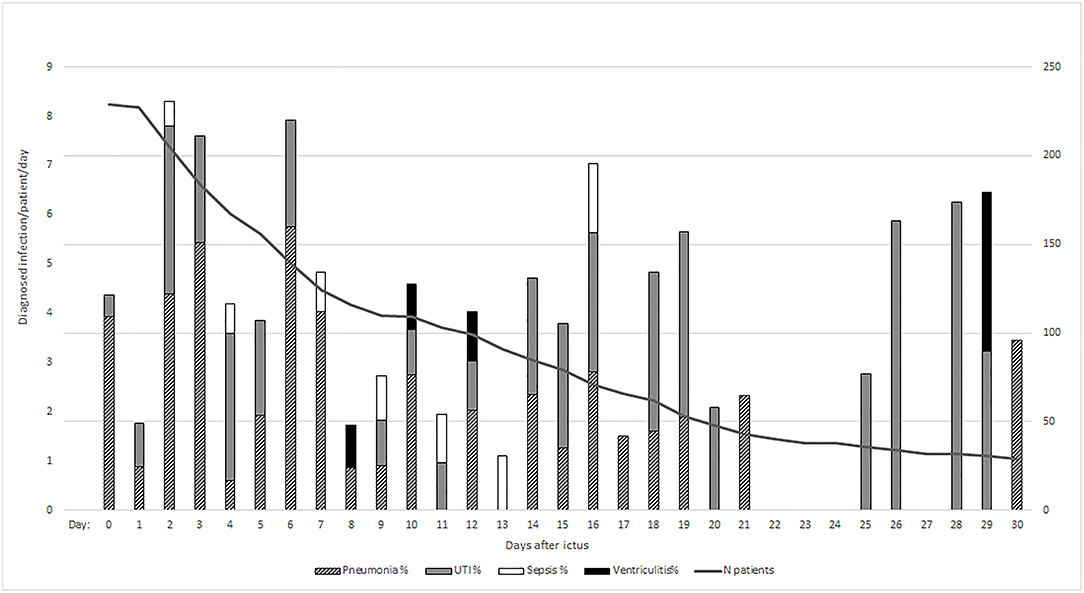
Figure 3. Represents relative prevalence of diagnosed infections per day/per patient to account for patients still admitted to the ICU. The absolute number of infections per day was divided by the number of patients per day. N patients, number of patients.
Risk Factors for Infectious Complications
In univariate analysis, clinical and radiographic severity on admission, early neurological deterioration, and hospital-related procedures were significantly associated with any IC (Table 1). In multivariable analysis, early neurological deterioration (adjOR = 4.0, 95% CI 2.1–7.71, p < 0.001), hematoma evacuation (adjOR = 4.9, 95% CI 2.5–9.68, p < 0.001), mechanical ventilation (adjOR = 9.6, 95% CI 4.15–22.1, p < 0.001), nasogastric tube feeding (adjOR = 16.5, 95% CI 6.3–43.11, p < 0.001) and evidence of midline shift >4 mm (adjOR = 2.3, 95% CI 1.22–4.46, p = 0.011) were associated with a higher risk of pneumonia after adjusting for ICH Score. Twenty-four patients (11%) developed early-onset pneumonia, which was associated with later occurring sepsis (adjOR = 22.5, 95% CI 4.88–103.6, p < 0.001). In addition, nasogastric tube feeding (adjOR = 10.4, 95% CI 1.13–96.71, p = 0.039), neurological deterioration (adjOR = 13.8, 95% CI 1.65–115.7, p = 0.016) and mechanical ventilation (adjOR = 11.3, 95% CI 1.22–105.32, p = 0.033) were associated with sepsis. All patients diagnosed with ventriculitis had an external ventricular drain (EVD). None of the analyzed variables were significantly associated with UTI.
ICH Score and Infectious Complications
The patients presented with a median ICH Score of 2 [IQR 1–3]. Patients with an ICH Score >2 were more likely to develop IC during NICU stay as compared to patients with an ICH Score ≤2 (40 vs. 32%, OR = 2.3, 95% CI 1.3–4.05, p = 0.006) (Table 3). In univariate analysis, patients with an ICH Score >2 developed IC earlier (Figure 4A). Moreover, patients with an ICH Score >2 were at higher risk for pneumonia (38 vs. 19%, OR = 3.6, 95% CI 1.9–6.6, p < 0.001) (Figures 4B,C).
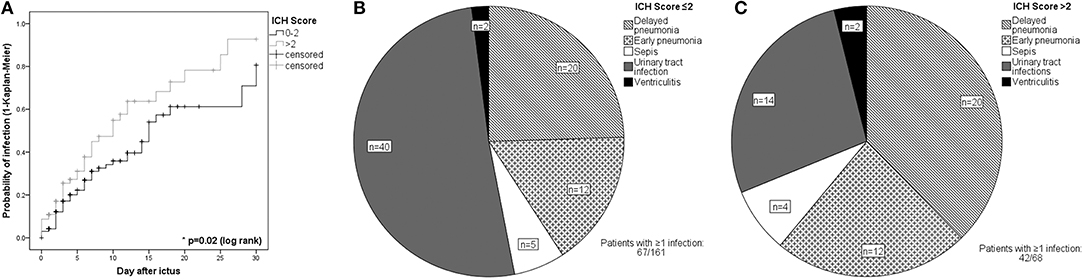
Figure 4. (A) Kaplan-Meier-Curve describing the probability of any infectious complication in patients with ICH Score ≤2 and >2. Patients were censored at the time of: withdrawal of care, NICU discharge, or death latest on day 30. Distribution of individual infections in patients with infections stratified by (B) an admission ICH Score ≤2 and (C) ICH Score >2.
Infectious Complications and Outcome
Having at least one infection during NICU stay was associated with unfavorable 3-months outcome (adjOR = 3.0, 95% CI 1.41–6.54, p = 0.005). For each additional IC, patients had a 2-fold higher risk of poor outcome after 3 months (95% CI 1.16–3.57, p = 0.013) after adjusting for ICH Score and APACHE Score (Table 2). All ICH patients with sepsis had a 3-months mRS ≥3. Pneumonia was independently associated with poor functional outcome (adjOR = 4.2, 95% CI 1.33–13.19, p = 0.015).
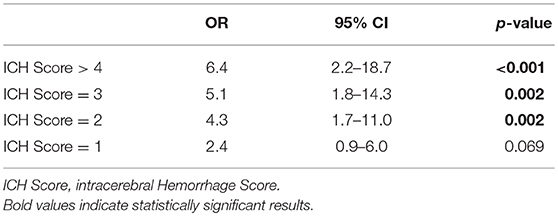
Table 2. Risk for infectious complications for each point increase of the ICH Score.
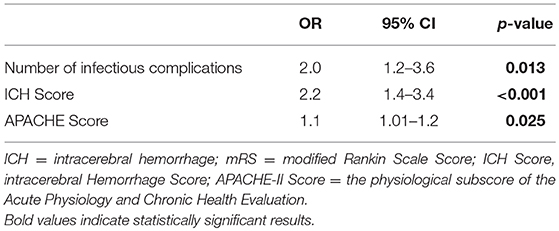
Table 3. Risk factors for poor functional outcome (mRS > 2) evaluated in 229 ICH patients.
Moreover, the number of IC per patient was associated with the length of NICU stay (Figure 5): ICH patients with one infection were prone to prolonged LOS (adjOR = 1.4, 95% CI 1.01–1.82, p = 0.047) when compared to patients with no infection. This association was even more pronounced in patients with ≥2 infections (adjOR = 6.9, 95% CI 4.12–11.55, p < 0.001).
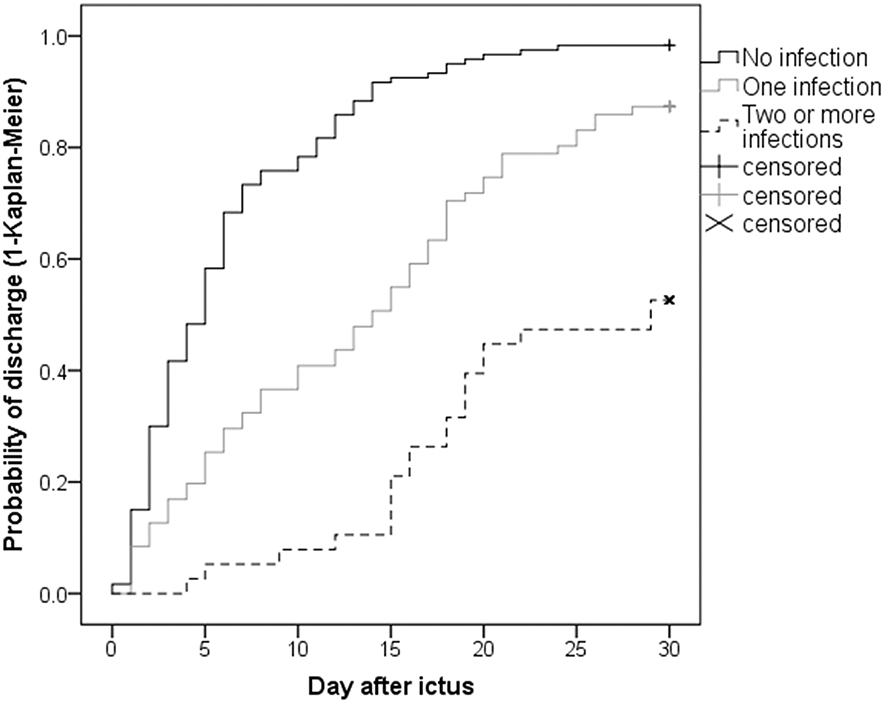
Figure 5. Length of NICU stay: Patients without any infection had a median LOS of 5 days [IQR 2–8 days], patients suffering from one infection 14 days [IQR 5–21 days], while patients suffering from two or more infections stayed 29 days [IQR 16–44 days] at NICU. All patients staying longer than 30 days were censored at day 30.
Discussion
In the current study we found [1] that IC are common after ICH with pneumonia having the highest incidence, [2] that an admission ICH Score >2 may serve as a valuable early predictor for the development of IC during NICU stay, [3] that early-onset pneumonia may help to identify people at risk for sepsis at a later timepoint and, [4] that the number of IC is independently associated with prolonged hospitalization and poor 3-months functional outcome.
In our cohort, 48% of ICH-patients developed at least one infection during NICU stay, which is similar to previously reported prevalence rates ranging from 23 to 58% (7, 9, 10, 12). It is important to mention that our cohort includes all clinical and radiographic severity grades since all ICH patients presenting to our emergency room were included in the study. Pneumonia was the most common IC followed by UTI, sepsis and ventriculitis, comparable to formerly reported prevalence rates of 10–20%, 8–17%, 1–3.6%, and 0.3–3%, respectively (7, 11, 12, 20).
It remains important to identify patients at higher risk of IC already on admission to allocate more resources for infectious surveillance and the early start of preventive measures. We found that the ICH Score, assessed on the day of admission, may be a useful tool to identify these patients. The ICH Score is based on the GCS Score, age, ICH volume, the presence of intraventricular hemorrhage (IVH) and infratentorial origin of ICH, and has been introduced in the prediction of 30 days mortality after ICH (13). While a lower GCS Score, higher ICH volume, the presence of IVH, and older age as part of the ICH Score, have previously shown to be associated with the development of infections, the sum-score would be even more applicable for clinical practice. The major contributor to an increased ICH Score in our cohort was a lower GCS Score followed by ICH volume and the presence of IVH (data not shown). Therefore, the association of higher ICH Score and the development of infectious complications may simply be explained by the initial disease severity. Additionally, patients with IVH are at higher risk for the development of fever and more frequently require EVD placement (21) which may in addition contribute to the development of IC. This hypothesis is supported by the higher occurrence rate of ventriculitis (11%) in our patients with EVD, while no other risk factors for ventriculitis could be identified (22). Moreover, infratentorial hematoma location has previously been associated with neurogenic dysphagia (23) and may also lead to IC including the development of pneumonia (11).
Since we prospectively recorded the day of onset of each infectious complication, we found that patients with an early-onset pneumonia had 23-fold higher odds of developing sepsis at a later time point. Respiratory tract infections are the most common IC in intensive care units (24). The association with sepsis is of interest and may stratify patients at risk early, however this association has not been consistently reported in literature and may be attributable to the prolonged need for invasive catheters or decreased bowel movement with transition of gramnegative bacteria.
In the current study we mainly identified non-modifiable risk factors for the development of IC including admission disease severity, mechanical ventilation, surgical intervention and early neurologic deterioration, which is in accordance with previous studies (10, 25, 26). In hemorrhagic stroke patients it has been shown that early neurological deterioration is associated with higher rates of hospital complications and poor outcome (27, 28). While mechanical ventilation is a known risk factor for VAP (19, 20, 29), neurogenic dysphagia is common after ICH and may contribute to the development of aspiration pneumonia in non-intubated patients (30, 31). Another risk factor for aspiration pneumonia includes nasogastric tube feeding which can be reduced by early percutaneous endoscopic gastrostomy (32). Proposed interventions to reduce the occurence of pneumonia in mechanically ventilated patients include interruption of sedation, early mobilization, head elevation to 30–45°, oral care with chlorhexidine, retaining of ventilator circuits, selective digestive tract decontamination and prophylactic probiotics (33, 34). However, it is important to mention that in most of these studies patients with acute brain injury were not included. Our infectious disease prevention bundle encompasses the use of chlorhexidin, early mobilization and head-up positioning. Interruption of sedation was not routinely done in our poor-grade patients at risk for raised ICP (35).
The strong association between IC and 3-months outcome independently of co-morbidities quantified by the APACHE II Score in our patient cohort confirms recent studies, underlining the contribution of infections to higher NICU mortality and worse functional outcome in survivors (7, 12). In accordance with previous prospective observational studies in ischemic stroke and SAH patients (12, 29, 36), pneumonia and sepsis were independently associated with poor functional outcome. Limited by the low patient number with ventriculitis in our cohort, we could not statistically confirm the findings of former studies showing an independent association with increased mortality and morbidity (29).
The average NICU LOS was similar as previously reported in ICH patients [8 days] (9, 12). Likewise, the identified association between all types of IC and prolonged length of NICU stay is consistent with previously published data (9, 11, 12).
Our results have to be interpreted with caution due to their limited generalizability to all ICUs given that critical care management and in specific, the surveillance bundle for IC may differ. Moreover, all patients with the whole range of clinical grades are admitted to the ICU, which may not reflect clinical practices in other centers. Furthermore, we did not investigate the impact of central line placement and antimicrobial chemotherapy which may have influenced the occurrence and impact of IC. Another important limitation is the retrospective analysis of prospectively collected data, thus only associations and not causalities can be concluded. Finally, the aim of the study was not to find the most accurate multivariable model but to analyze whether the ICH Score would qualify for the prediction of infectious complications.
Conclusion
Infections are frequent and serious in patients suffering from ICH. Their independent association with poor outcome warrants close surveillance and the earliest possible management when diagnosis is established. The association with prolonged NICU stay has a tremendous impact on the economic burden of this disease. Our findings may help to early identify patients at high risk for the development of IC.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Research Committee (Medical University Innsbruck, AN4088292/4.3) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all patients or legal representatives according to local regulatories.
Author Contributions
AL and RH study idea and design, data acquisition and analysis, manuscript writing and drafting, MK, VR, BI, MG, AS, RB, SL, PR, BP, ES, and CT contributed to the study idea, data acquisition, manuscript drafting. RH contributed to the study supervision. All authors read and approved this version of the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank the nursing staff and the entire team of the Neurological Intensive Care Unit for their ongoing contribution in the care of our patients.
References
1. Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. (2009) 8:355–69. doi: 10.1016/S1474-4422(09)70025-0
2. Huge V. Critical care management of intracerebral hemorrhage. Med Klin Intensivmed Notfmed. (2016) 36:225–32. doi: 10.1055/s-0036-1581991
3. van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. (2010) 9:167–76. doi: 10.1016/S1474-4422(09)70340-0
4. An SJ, Kim TJ, Yoon BW. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: an update. J Stroke. (2017) 19:3–10. doi: 10.5853/jos.2016.00864
5. Hemphill JC III, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2015) 46:2032–60. doi: 10.1161/STR.0000000000000069
6. Stein M, Hamann GF, Misselwitz B, Uhl E, Kolodziej M, Reinges MH. In-hospital mortality and complication rates in surgically and conservatively treated patients with spontaneous intracerebral hemorrhage in Central Europe: a population-based study. World Neurosurg. (2016) 88:306–10. doi: 10.1016/j.wneu.2015.11.075
7. Lord AS, Langefeld CD, Sekar P, Moomaw CJ, Badjatia N, Vashkevich A, et al. Infection after intracerebral hemorrhage: risk factors and association with outcomes in the ethnic/racial variations of intracerebral hemorrhage study. Stroke. (2014) 45:3535–42. doi: 10.1161/STROKEAHA.114.006435
8. Ali M, Lyden P, Sacco RL, Shuaib A, Lees KR, Investigators V. Natural history of complications after intracerebral haemorrhage. Eur J Neurol. (2009) 16:624–30. doi: 10.1111/j.1468-1331.2009.02559.x
9. Ohwaki K, Yano E, Nagashima H, Nakagomi T, Tamura A. Impact of infection on length of intensive care unit stay after intracerebral hemorrhage. Neurocrit Care. (2008) 8:271–5. doi: 10.1007/s12028-007-9007-1
10. Sykora M, Diedler J, Poli S, Rizos T, Turcani P, Veltkamp R, et al. Autonomic shift and increased susceptibility to infections after acute intracerebral hemorrhage. Stroke. (2011) 42:1218–23. doi: 10.1161/STROKEAHA.110.604637
11. Hinduja A, Dibu J, Achi E, Patel A, Samant R, Yaghi S. Nosocomial infections in patients with spontaneous intracerebral hemorrhage. Am J Crit Care. (2015) 24:227–31. doi: 10.4037/ajcc2015422
12. Murthy SB, Moradiya Y, Shah J, Merkler AE, Mangat HS, Iadacola C, et al. Nosocomial Infections and outcomes after intracerebral hemorrhage: a population-based study. Neurocrit Care. (2016) 25:178–84. doi: 10.1007/s12028-016-0282-6
13. Hemphill JC, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. (2001) 32:891–7. doi: 10.1161/01.STR.32.4.891
14. Gregorio T, Pipa S, Cavaleiro P, Atanasio G, Albuquerque I, Chaves PC, et al. Assessment and comparison of the four most extensively validated prognostic scales for intracerebral hemorrhage: systematic review with meta-analysis. Neurocrit Care. (2019) 30:449–66. doi: 10.1007/s12028-018-0633-6
15. Alizadeh AM, Hassanian-Moghaddam H, Shadnia S, Zamani N, Mehrpour O. Simplified acute physiology score II/acute physiology and chronic health evaluation II and prediction of the mortality and later development of complications in poisoned patients admitted to intensive care unit. Basic Clin Pharmacol Toxicol. (2014) 115:297–300. doi: 10.1111/bcpt.12210
16. Steiner T, Al-Shahi Salman R, Beer R, Christensen H, Cordonnier C, Csiba L, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. (2014) 9:840–55. doi: 10.1111/ijs.12309
17. van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. (1988) 19:604–7. doi: 10.1161/01.STR.19.5.604
18. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. (1988) 16:128–40. doi: 10.1016/0196-6553(88)90053-3
19. Society AT, America IDSo. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. (2005) 171:388–416. doi: 10.1164/rccm.200405-644ST
20. Divani AA, Hevesi M, Pulivarthi S, Luo X, Souslian F, Suarez JI, et al. Predictors of nosocomial pneumonia in intracerebral hemorrhage patients: a multi-center observational study. Neurocrit Care. (2015) 22:234–42. doi: 10.1007/s12028-014-0065-x
21. Honig A, Michael S, Eliahou R, Leker RR. Central fever in patients with spontaneous intracerebral hemorrhage: predicting factors and impact on outcome. BMC Neurol. (2015) 15:6. doi: 10.1186/s12883-015-0258-8
22. Humphreys H, Jenks PJ. Surveillance and management of ventriculitis following neurosurgery. J Hosp Infect. (2015) 89:281–6. doi: 10.1016/j.jhin.2014.12.019
23. Daniels SK, Pathak S, Mukhi SV, Stach CB, Morgan RO, Anderson JA. The relationship between lesion localization and dysphagia in acute stroke. Dysphagia. (2017) 32:777–84. doi: 10.1007/s00455-017-9824-0
24. Mayr FB, Yende S, Angus DC. Epidemiology of severe sepsis. Virulence. (2014) 5:4–11. doi: 10.4161/viru.27372
25. Kourbeti IS, Vakis AF, Ziakas P, Karabetsos D, Potolidis E, Christou S, et al. Infections in patients undergoing craniotomy: risk factors associated with post-craniotomy meningitis. J Neurosurg. (2015) 122:1113–9. doi: 10.3171/2014.8.JNS132557
26. Kurland DB, Khaladj-Ghom A, Stokum JA, Carusillo B, Karimy JK, Gerzanich V, et al. Complications associated with decompressive craniectomy: a systematic review. Neurocrit Care. (2015) 23:292–304. doi: 10.1007/s12028-015-0144-7
27. Lord AS, Gilmore E, Choi HA, Mayer SA, Collaboration V-I. Time course and predictors of neurological deterioration after intracerebral hemorrhage. Stroke. (2015) 46:647–52. doi: 10.1161/STROKEAHA.114.007704
28. Helbok R, Kurtz P, Vibbert M, Schmidt MJ, Fernandez L, Lantigua H, et al. Early neurological deterioration after subarachnoid haemorrhage: risk factors and impact on outcome. J Neurol Neurosurg Psychiatry. (2013) 84:266–70. doi: 10.1136/jnnp-2012-302804
29. Frontera JA, Fernandez A, Schmidt JM, Claassen J, Wartenberg KE, Badjatia N, et al. Impact of nosocomial infectious complications after subarachnoid hemorrhage. Neurosurgery. (2008) 62:80–7; discussion 7. doi: 10.1227/01.NEU.0000311064.18368.EA
30. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke. (2005) 36:2756–63. doi: 10.1161/01.STR.0000190056.76543.eb
31. Ribeiro PW, Cola PC, Gatto AR, da Silva RG, Luvizutto GJ, Braga GP, et al. Relationship between dysphagia, national institutes of health stroke scale score, and predictors of pneumonia after ischemic stroke. J Stroke Cerebrovasc Dis. (2015) 24:2088–94. doi: 10.1016/j.jstrokecerebrovasdis.2015.05.009
32. Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. (2014) 20:8505–24. doi: 10.3748/wjg.v20.i26.8505
33. Klompas M, Branson R, Eichenwald EC, Greene LR, Howell MD, Lee G, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. (2014) 35:S133–54. doi: 10.1086/677144
34. Schultz MJ, Haas LE. Antibiotics or probiotics as preventive measures against ventilator-associated pneumonia: a literature review. Crit Care. (2011) 15:R18. doi: 10.1186/cc9963
35. Helbok R, Kurtz P, Schmidt MJ, Stuart MR, Fernandez L, Connolly SE, et al. Effects of the neurological wake-up test on clinical examination, intracranial pressure, brain metabolism and brain tissue oxygenation in severely brain-injured patients. Crit Care. (2012) 16:R226. doi: 10.1186/cc11880
Keywords: intracerebral hemorrhage, risk factors, infections, critical care, neurology, infectious complications
Citation: Lindner A, Kofler M, Rass V, Ianosi B, Gaasch M, Schiefecker AJ, Beer R, Loveys S, Rhomberg P, Pfausler B, Thomé C, Schmutzhard E and Helbok R (2019) Early Predictors for Infectious Complications in Patients With Spontaneous Intracerebral Hemorrhage and Their Impact on Outcome. Front. Neurol. 10:817. doi: 10.3389/fneur.2019.00817
Received: 11 April 2019; Accepted: 15 July 2019;
Published: 06 August 2019.
Edited by:
Alejandro Bustamante, Vall d'Hebron University Hospital, SpainReviewed by:
Amit Kishore, Salford Royal NHS Foundation Trust, United KingdomGeorgios Tsivgoulis, National and Kapodistrian University of Athens, Greece
Copyright © 2019 Lindner, Kofler, Rass, Ianosi, Gaasch, Schiefecker, Beer, Loveys, Rhomberg, Pfausler, Thomé, Schmutzhard and Helbok. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raimund Helbok, cmFpbXVuZC5oZWxib2tAdGlyb2wta2xpbmlrZW4uYXQ=; cmFpbXVuZC5oZWxib2tAaS1tZWQuYWMuYXQ=