 Juliëtte J. C. M. van Munster1,2*†
Juliëtte J. C. M. van Munster1,2*† Wouter H. van der Valk1†
Wouter H. van der Valk1† Inge Stegeman3,4
Inge Stegeman3,4 Arno F. Lieftink3
Arno F. Lieftink3 Adriana L. Smit3,4
Adriana L. Smit3,4- 1Department of Otorhinolaryngology and Head & Neck Surgery, Leiden University Medical Center, Leiden University, Leiden, Netherlands
- 2Department of Neurosurgery, Leiden University Medical Center, Leiden University, Leiden, Netherlands
- 3Department of Otorhinolaryngology and Head & Neck Surgery, University Medical Center Utrecht, Utrecht, Netherlands
- 4Brain Center Rudolf Magnus, University Medical Center Utrecht, Utrecht, Netherlands
Objectives: An association between tinnitus distress with anxiety and depression is described in literature. A similar relationship might exist between tinnitus distress and personality traits, especially since associations between personality traits and other chronic diseases are already revealed. In this systematic review, we aim to investigate whether personality is a risk factor for tinnitus distress.
Design: We searched PubMed and EMBASE databases from inception up to December 31, 2018 for articles on the association between tinnitus distress and personality. Two researchers screened titles, abstracts, and full texts for eligibility. Directness of evidence and risk of bias were assessed. From the included studies, study characteristics and outcome data of tinnitus distress and personality traits were extracted.
Results: A total of 323 unique articles were screened of which 11 cross-sectional studies were eligible for critical appraisal and were used for data extraction. Including study populations were heterogenous, and studies scored high to moderate risk of bias. Nine out of 11 articles showed an association between tinnitus distress and the personality of neuroticism.
Conclusions: By limitations in the methodology of included studies, the evidence on specific personality traits as a risk factor for tinnitus distress is inconclusive. Some evidence on a positive association with neuroticism is identified. To draw conclusions about causal relations, these further studies should be of longitudinal design in a cohort setting. These studies should assess tinnitus distress using validated questionnaires with multiple personality dimensions and validated questionnaires to assess personality traits.
Introduction
Tinnitus is the presence of a buzzing or tinkling sound in one or both ears without an acoustic external source to the head and can be associated with a reduction in health-related quality of life (1–3). Growing evidence shows that many cases of tinnitus are associated with de-afferentation of the central auditory structures due to aging, noise exposure, otologic injury, or other causes. The prevalence of tinnitus varies widely, depending on the used methodology, selected population, and definition of tinnitus. For that reason, the prevalence of the adult population experiencing tinnitus is estimated to be 10–25% (4). Where only 1–7% of the adult tinnitus population seems to struggle with bothersome tinnitus, others experience this symptom without any difficulties, which underlines the heterogeneity of the experienced disease (4). This heterogeneity is not only the experienced diversity in the tinnitus itself (e.g., lateralization, temporal course, sound characteristics) but also due to differences in tinnitus-related problems such as sleep and concentration difficulties and accompanying co-morbidities. Tinnitus-related distress is diverse and can be described as a complex phenomenon associated with negative appraisal, selective attention, safety behaviors, beliefs, and a distorted perception of tinnitus (5, 6). Thereby, it is not surprising that the individual needs of patients for tinnitus-related healthcare are various (4, 7).
So far, it is unclear to what extent psychopathological disorders are predisposing to tinnitus complaints, do aggravate symptoms, or refrain patients from tinnitus relief by diverse tinnitus therapies (8–10). The same might be argued for possible influences of personality traits (10) whereby personality can be defined as the characteristic pattern of thinking, feeling, and behaving of an individual (11). Early appearance of personality after birth indicates that personality is partly genetic determined (12, 13). Many studies have investigated the association between personality and diseases, for instance, between personality and the development of cardiovascular disease and cancer (14–17). A similar relationship could exist between personality characteristics and tinnitus. In the cognitive tinnitus model, it is assumed that tinnitus provokes distress in persons who hold overly negatively thoughts about it, thereby motivating maintaining factors. Subsequently, patients gain a distorted perception of their tinnitus. In 2014, Mucci et al. analyzed the relationship between tinnitus and personality by reviewing the literature from 1968 to 2012 (5, 18). They concluded that tinnitus is associated with several personality characteristics, especially on neuroticism, though a clear distinction between tinnitus perception and tinnitus distress was not made and the quality of data was not assessed. Personality characteristics in patients with more distress might differ from others without high distress levels. A scoping review by Durai et al. in 2016 found associations between tinnitus distress and multiple personality traits such as high neuroticism and low extraversion (19). Still, this review has important limitations due to the scoping method: relevant studies may not have been identified, and a quality assessment was not performed.
To measure personality traits, a wide range of questionnaires can be used. Some questionnaires focus on specific personality traits (19) where other questionnaires are based on models dividing personality into dimensions, for instance, three (Eysenck's theory) or five dimensions [the five-factor model (FFM): the “Big Five”] (19, 20). The variance between factors in the FFM is substantial compared to the variance of other personality inventories (21), and thereby, the FFM adopted a prominent position in the field of personality assessment (22). Assessing personality traits by a validated instrument in tinnitus patients might contribute to a better understanding about the relationship between both. As differences in personality traits can influence tinnitus-related distress and the response on different tinnitus treatments, which is especially important for tinnitus patients with severe complaints of tinnitus, this insight might be of benefit to understand the disease and treatment outcome. Therefore, we aim to investigate whether personality is a risk factor for tinnitus distress by a systematic review of the literature.
Materials and Methods
Search Strategy
We searched PubMed and Embase to access records, which analyzed the relationship between tinnitus distress and personality up to December 2018. PubMed was searched by entering the following search criteria in PubMed: [personal*(Title/Abstract)] AND {[tinnitus (MeSH Terms)] OR tinnitus (Title/Abstract)}. A similar search strategy was used to search Embase. The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) was used as a writing guideline (23).
Study Selection
After removal of duplicates, two researchers (JM and WV) independently screened titles and abstracts of searched articles. Eligible full text articles were retrieved through the databases and by emailing the authors. Full text eligibility was determined by the in- and exclusion criteria listed in Table 1. We included studies if they included adults with tinnitus that correlated tinnitus distress with personality characteristics. With tinnitus distress, terms such as tinnitus loudness, annoyance, and handicap were also included. When there was a different opinion on eligibility, the two reviewers tried to reach consensus. Studies investigating a therapy for tinnitus were excluded since interventions can change personality traits (24). The third and fifth author (IS and AS) were consulted if no unanimity was achieved.
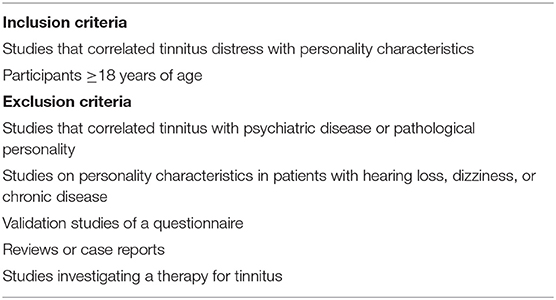
Table 1. Eligibility criteria.
Data Collection
Two researchers (JM and WV) extracted data regarding study design, study population, group size, setting, questionnaires regarding tinnitus distress and personality, and outcomes of the evaluation concerning tinnitus distress and personality. Primary outcome was the relationship between tinnitus distress and personality traits, as described by the FFM. The FFM is a taxonomy of five traits: neuroticism, extraversion, openness, agreeableness, and conscientiousness (25). The Big Five Personality Dimensions Scale, the NEO Five-Factor Inventory (NEO-FFI), and the Big Five Inventory (BFI) are based on the FFM. When included trials used personality trait questionnaires not based on the FFM categorization, these personality traits were matched to the FFM categories. For this, the literature was searched to find a correlation between the non-FFM personality trait category and the traits as defined and scored by the FFM (26–34). Those associations and stratifications between FFM personality traits and non-FFM traits are described in Table 2. Mean scores of the questionnaires including standard deviations and P-values were distracted from the articles when available. When a t-test was used, the F-ratio and P-value were documented.
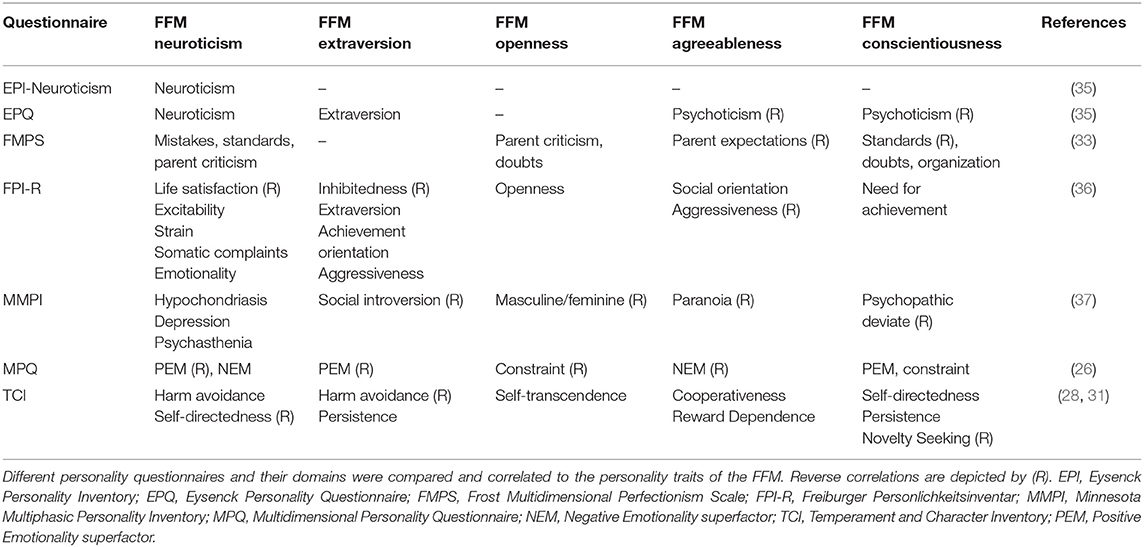
Table 2. Correlation between non-FFM personality questionnaires and the FFM personality traits based on the literature.
Risk of Bias
Critical appraisal of selected studies regarding risk of bias (RoB) was performed by two researchers (WV and JM), using the Newcastle–Ottawa Quality Assessment Scale, using different assessment scales for cohort studies and for case-control studies (38). This instrument is divided into three subdomains concerning the bias in selection, comparability, and exposure. Each subdomain consists of one to four categories of potential bias. A study can be awarded one or two stars depending on each item within the categories. Selection can be awarded with a maximum of four stars, comparability with a maximum of two stars, and outcome with a maximum of three stars. The more stars were earned, the lower the risk of bias of the study was rated.
Results
Study Selection
Our flow chart of the study selection, including reasons for exclusion of articles, is shown in Figure 1. After removal of duplicates, 323 unique records were identified. Of these, 255 articles were excluded based on title and abstract screening. After reading the full text of 68 articles, 11 articles were eligible for critical appraisal.
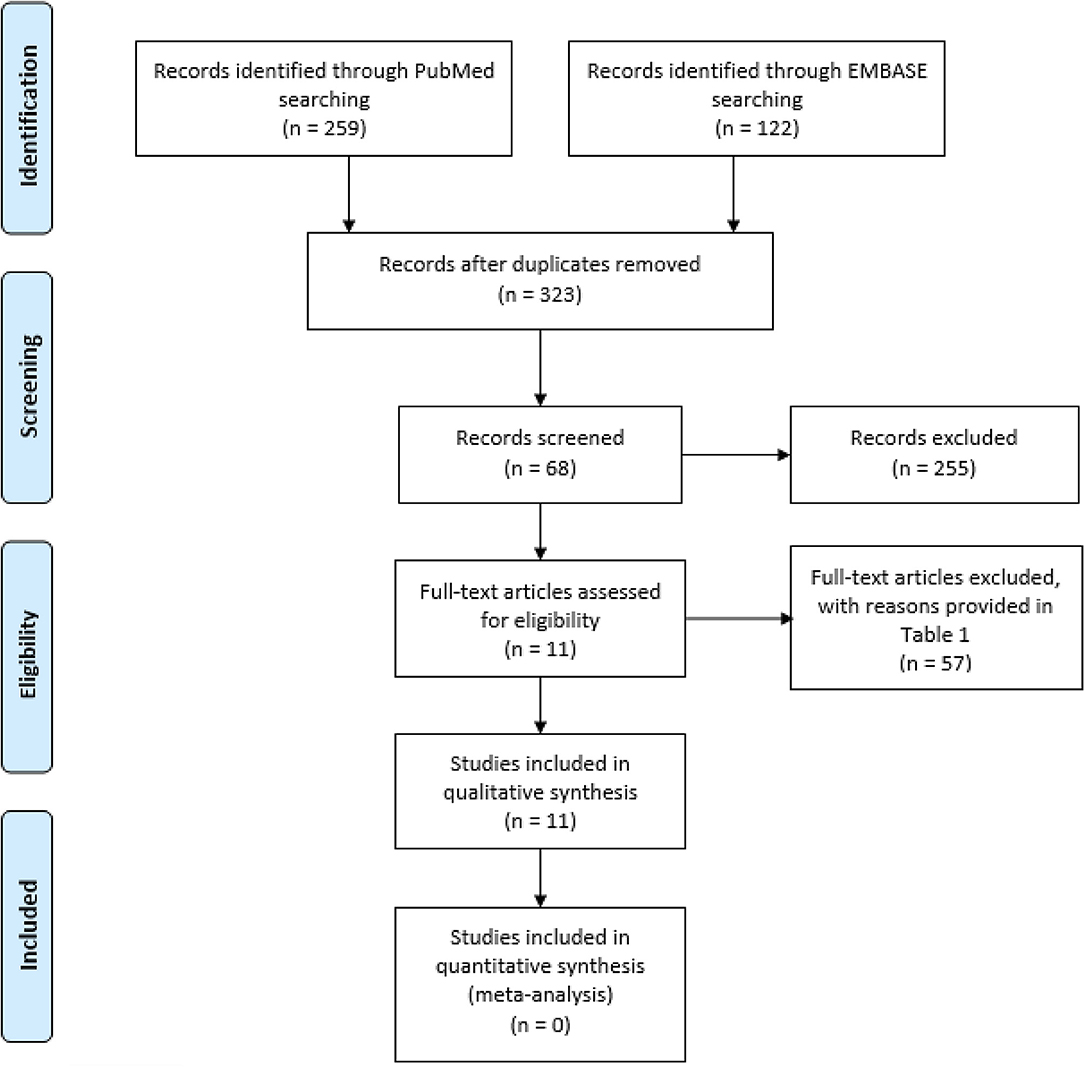
Figure 1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram of Study Selection (39).
Risk of Bias and Quality Assessment
Critical appraisal of the 11 articles is outlined in Table 3. None of the studies were awarded with the maximal amount of nine stars; the range is between three and six stars. The majority used a selected group of tinnitus patients by including them from outpatient clinics (40, 41, 43, 44, 46–49). Furthermore, none of the case-control studies did provide information about non-respondents, and all cohort studies were of cross-sectional study design hindering the assessment of adequate follow-up. In addition, the majority of studies did not correctly control for confounding factors (40, 41, 43–49). Together, this limits the number of stars awarded for all subdomains. Only two studies used a representative cohort of patients with tinnitus out of the general population; however, these studies used a single question of tinnitus distress in contrast to validated multi-item questionnaires (45, 50).
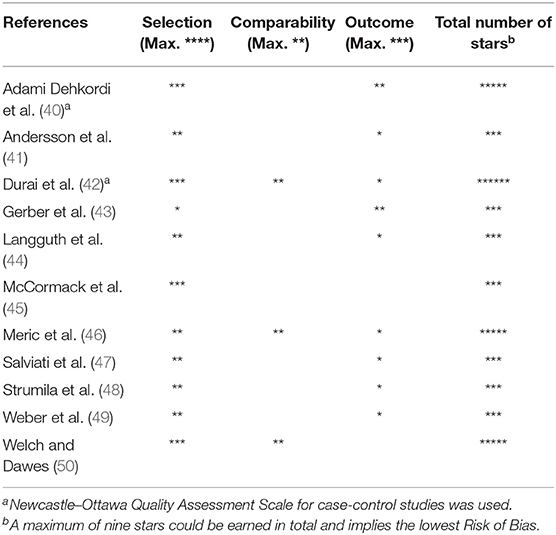
Table 3. Risk of bias assessment using the Newcastle–Ottawa Quality Assessment Scale.
Characteristics of Studies
There was a large heterogeneity in tinnitus questionnaires and personality questionnaires to measure tinnitus distress and personality traits, respectively, in the included studies. Because of this heterogeneity, no meta-analysis could be performed. Therefore, a descriptive analysis of the included articles is provided. All but three (42, 45, 50) studies included patients who visited the tinnitus department or Ear-, Nose-, Throat (ENT), which leads to a specific patient selection. The two cohort studies included patients from large-population studies in Dunedin (New Zealand) and the United Kingdom (UK) (45, 50) and assessed personality traits in a cross-sectional manner.
Synthesis of the Results
Extensive descriptions of the articles and outcomes are presented in Table 4.
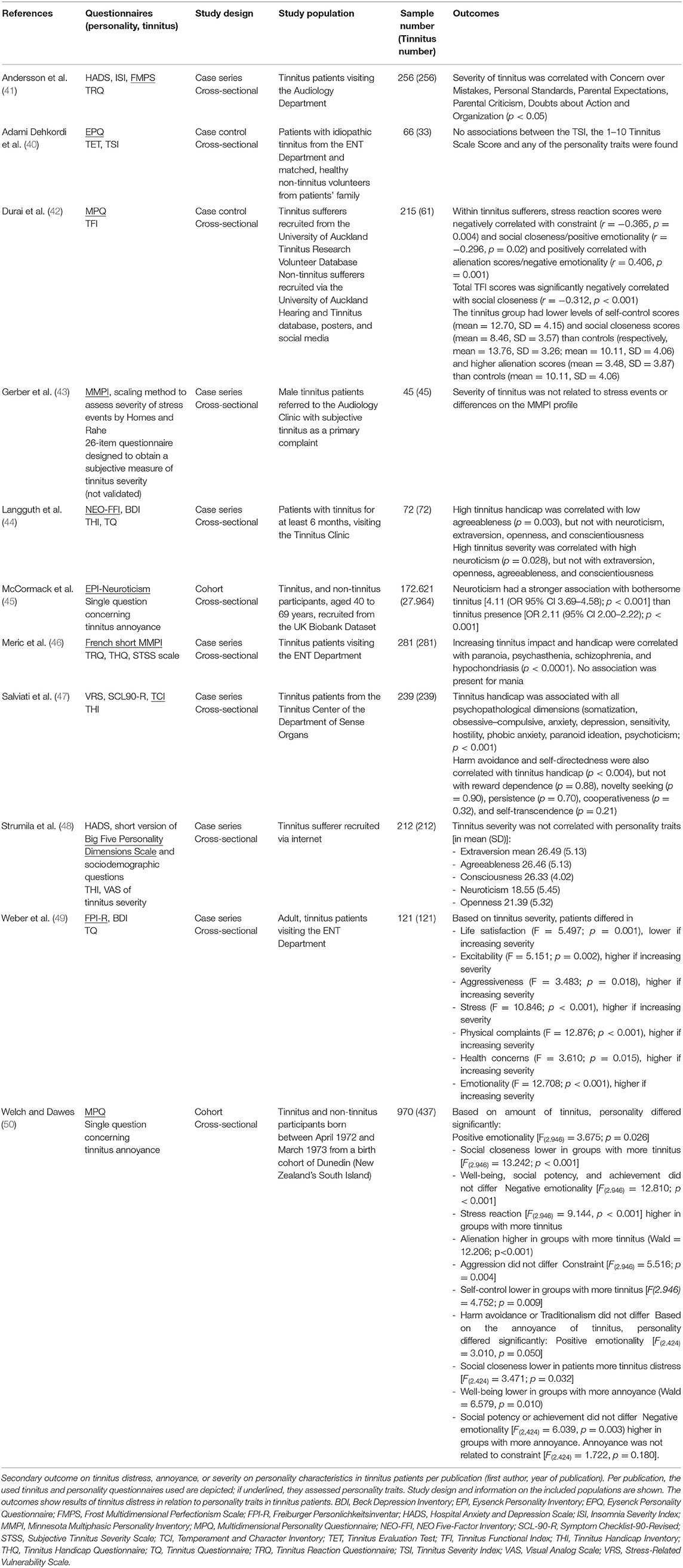
Table 4. Summary of studies on personality characteristics in tinnitus patients according to tinnitus distress.
Tinnitus Distress and Personality Traits
A majority (9 out of 11 studies) of the included studies showed one or more associations (both positive and negative) between tinnitus distress and personality (41, 44–47, 49, 50). Two out of 11 articles studied the association between tinnitus distress and the FFM personality traits by usage of the NEO five-factor inventory (44) or a short version of the Big Five Personality dimensions scale (48). Of those, Langguth et al. did find a negative association between scores on the Tinnitus Handicap Inventory (THI) and consciousness (correlation coefficient = −0.367, p = 0.003), and a positive association between tinnitus distress on the Tinnitus Questionnaire (TQ) and neuroticism (correlation coefficient = 0.276, p = 0.028) (44). Furthermore Strumila et al. (48) stated that high THI scores did not predict high scores on any of the personality traits, but neuroticism did influence distress of tinnitus perception (p <0.001, standardized coefficient 0.38).
The other nine studies used non-FFM-based questionnaires to assess personality traits in similar domains to the FFM division (40–43, 45–47, 49, 50). To be able to make a comparison, we converted these outcomes of personality traits to the FFM personality traits when a comparison between both was described in literature, as stated previously (Tables 2, 5). One study found a positive association between bothersome tinnitus and neuroticism [odds ratio (95% CI) = 4.11 (3.69–4.58), p < 0.001] using the EPI-neuroticism questionnaire (45). Eight of nine non-FFM-based studies indicated a positive correlation between neuroticism and increased tinnitus distress, including the New Zealand study, which represents a sample of the general population (Table 5) (40–42, 45–47, 49, 50). For the other categories of personality traits (extraversion, openness, agreeableness, and consciousness), we found no conclusive results about an association with tinnitus distress.
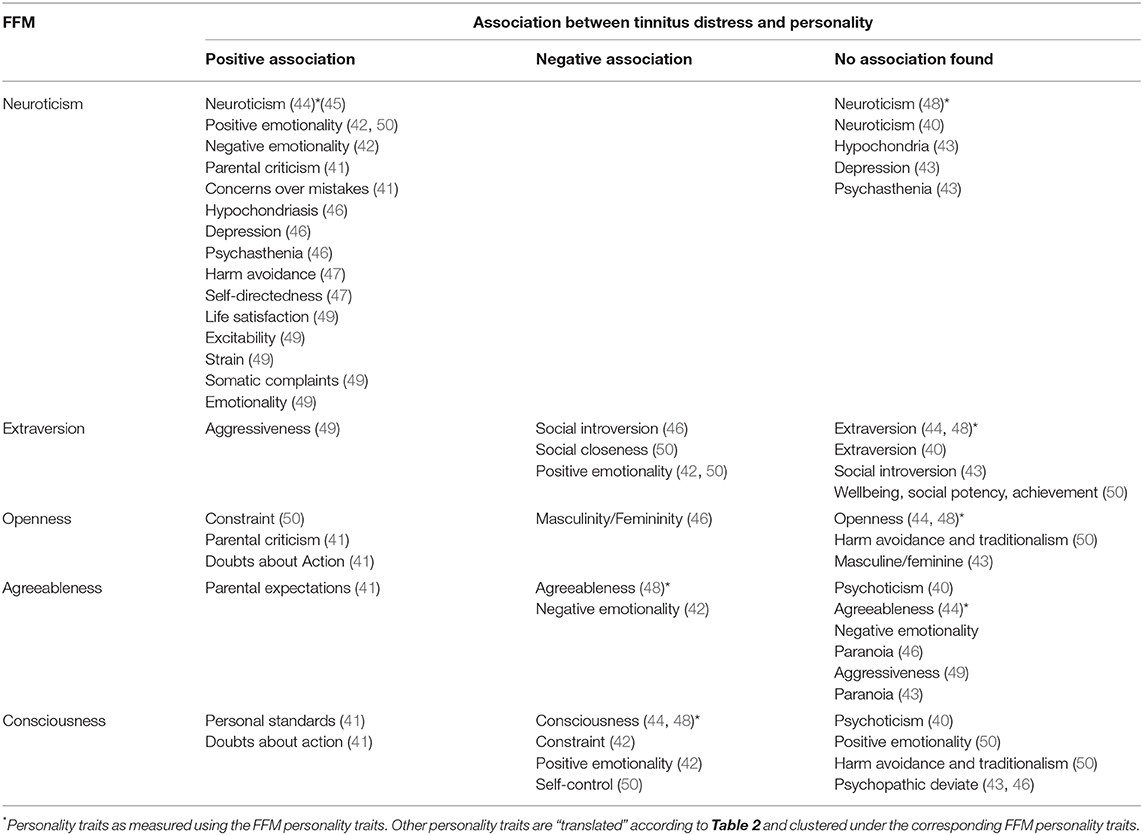
Table 5. Association of personality trait outcomes to tinnitus distress.
Discussion
In the present review, we studied personality traits as a risk factor for tinnitus distress, in which 11 cross-sectional studies with a high degree of heterogeneity in methods and outcomes were included. Owing to heterogeneity in the reported personality traits, it was not possible to perform a meta-analysis. Of the FFM, neuroticism was the only trait with a positive relationship with tinnitus distress in multiple studies. The association between neuroticism and tinnitus distress is in line with previous findings about emotional health and tinnitus: tinnitus distress shows close relationships with factors related to emotional health, and emotional health may be prognostic for the development of tinnitus distress (51, 52). One could argue that patients with more severe complaints of tinnitus are indeed more likely to have a neurotic personality, since neuroticism is described as the tendency to experience negative emotions. However, neuroticism is also associated with psychopathological symptoms of depression and anxiety (53), which complicates the causality of this association, since anxiety and depression are more prevalent among tinnitus patients (8, 19, 54). Moreover, both tinnitus and personality are potentially influenced by genetic factors (55, 56). Interestingly, of the FFM traits, the strongest associations were revealed between genetic variants and neuroticism (56–58). One of these studies used the same prospective cohort in the United Kingdom as the study of McCormack et al. (45) of which results were included in this systematic review. Indeed, this study found a positive association between neuroticism and tinnitus.
Several major limitations of this systematic review must be mentioned. Most of the studies included a selected population of tinnitus patients visiting an ENT department, audiological clinic, or tinnitus clinics and, thus, are not necessarily representative of the general population. For instance, headache-prone individuals have found to differ in personality profiles when comparing institutionalized patients to non-institutionalized controls from outside the clinic (59). Potentially, help-seeking tinnitus patients might differ in personality from non-help-seeking tinnitus patients. Owing to the selected sample of tinnitus patients used in the included studies in our review, generalization of outcomes is hindered. Moreover, most studies are prone to bias as scored by the Newcastle–Ottawa Quality Assessment Scale. For instance, confounders in the relation between personality traits and tinnitus distress exist, but not all studies described or analyzed these potential confounding factors such as gender (41, 48, 50). Additionally, as many different questionnaires were used to assess the personality traits, we used previously described correlations to convert the personality domains out of these questionnaires into the FFM categorization, to be able to compare outcomes of different studies. To our knowledge, however, this method is not validated nor described previously.
For all these reasons, the evidence we present in this systematic review about the relationship between personality and tinnitus is inconclusive. The aim of our review was to assess personality as a risk factor for tinnitus distress. Longitudinal cohort studies are needed to assess the causality of personality in tinnitus, address the limitations, and reveal additional potential confounders in this relationship.
The potential relationship of tinnitus distress with neuroticism may affect the success of specific tinnitus treatments, making the execution of high-quality studies on this topic of eminent importance. For example, cognitive behavioral treatment (CBT) targets the emotional reactivity and (dysfunctional) behavioral mechanisms. Studies assessing tinnitus outcome after CBT treatment show a reduction in disease-related distress and increased daily life functioning in individuals with subjective tinnitus (60–62). Interestingly, FFM personality can affect the tinnitus outcome after CBT treatment as demonstrated by Kleinstauber et al. in a clinical trial (63). Therefore, one should not only consider tinnitus distress (64) but also individual characteristics as personality traits to tailor tinnitus treatment for this heterogenous group of patients.
Conclusion
We endeavored to present the evidence on the relationship between tinnitus distress and personality traits in this systematic review. Owing to limitations in the methodology of included studies, the evidence on specific personality traits as a risk factor for tinnitus distress is inconclusive. Some evidence on a positive association with neuroticism is identified. To draw conclusions about causal relations, future studies should be of longitudinal design in a cohort setting. These studies should assess tinnitus distress using validated questionnaires with multiple personality dimensions and validated questionnaires to assess personality traits.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Author Contributions
This study was conceived and designed by JM, WV, IS, and AS. All authors contributed to acquisition, analysis, and interpretation of data. The drafting of the manuscripts was performed by JM and WV. Critical revision of the manuscript for important intellectual content as well as study supervision was performed by AS, IS, and AL.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Henry JA, Dennis KC, Schechter MA. General review of tinnitus: prevalence, mechanisms, effects, and management. J Speech Lang Hear Res. (2005) 48:1204–35. doi: 10.1044/1092-4388(2005/084)
2. Nondahl DM, Cruickshanks KJ, Dalton DS, Klein BE, Klein R, Schubert CR, et al. The impact of tinnitus on quality of life in older adults. J Am Acad Audiol. (2007) 18:257–66. doi: 10.3766/jaaa.18.3.7
3. Prestes R, Daniela G. Impact of tinnitus on quality of life, loudness and pitch match, and high-frequency audiometry. Int Tinnitus J. (2009) 15:134–8.
5. Mckenna L, Handscomb L, Hoare DJ, Hall DA. A scientific cognitive-behavioral model of tinnitus: novel conceptualizations of tinnitus distress. Front Neurol. (2014) 5:196. doi: 10.3389/fneur.2014.00196
6. Brüggemann P, Szczepek AJ, Rose M, Mckenna L, Olze H, Mazurek B. Impact of multiple factors on the degree of tinnitus distress. Front Hum Neurosci. (2016) 10:341. doi: 10.3389/fnhum.2016.00341
7. Nemholt SS, Schmidt JH, Wedderkopp N, Baguley DM. Prevalence of tinnitus and/or hyperacusis in children and adolescents: study protocol for a systematic review. BMJ Open. (2015) 5:e006649. doi: 10.1136/bmjopen-2014-006649
8. Geocze L, Mucci S, Abranches DC, Marco MA, Penido Nde O. Systematic review on the evidences of an association between tinnitus and depression. Braz J Otorhinolaryngol. (2013) 79:106–11. doi: 10.5935/1808-8694.20130018
9. Pinto PC, Marcelos CM, Mezzasalma MA, Osterne FJ, De Melo Tavares De Lima MA, Nardi AE. Tinnitus and its association with psychiatric disorders: systematic review. J Laryngol Otol. (2014) 128:660–4. doi: 10.1017/S0022215114001030
10. Trevis KJ, Mclachlan NM, Wilson SJ. A systematic review and meta-analysis of psychological functioning in chronic tinnitus. Clin Psychol Rev. (2018) 60:62–86. doi: 10.1016/j.cpr.2017.12.006
11. Andersen AM, Bienvenu OJ. Personality and psychopathology. Int Rev Psychiatr. (2011) 23:234–47. doi: 10.3109/09540261.2011.588692
12. Thomas A, Chess S, Zrull JP, Chairman DO. Temperament and development. J Am Acad Child Psychiatr. (1978) 17:732–3. doi: 10.1016/S0002-7138(09)61026-8
13. Cloninger CR, Svrakic DM, Przybeck TR. A psychobiological model of temperament and character. Arch Gen Psychiatr. (1993) 50:975–90. doi: 10.1001/archpsyc.1993.01820240059008
14. Eysenck HJ. Personality, cancer and cardiovascular disease: a causal analysis. Personal Individual Differ. (1985) 6:535–56. doi: 10.1016/0191-8869(85)90003-0
15. Eysenck HJ. Psychosocial factors, cancer, and ischaemic heart disease. BMJ. (1992) 305:457–9. doi: 10.1136/bmj.305.6851.457
16. Eysenck HJ. Prediction of cancer and coronary heart disease mortality by means of a personality inventory: results of a 15-year follow-up study. Psychol Rep. (1993) 72:499–516. doi: 10.2466/pr0.1993.72.2.499
18. Mucci S, Geocze L, Abranches DC, Antunez AE, Penido Nde O. [Systematic review of evidence on the association between personality and tinnitus]. Braz J Otorhinolaryngol. (2014) 80:441–7. doi: 10.1016/j.bjorl.2014.05.031
19. Durai M, Searchfield G. Anxiety and depression, personality traits relevant to tinnitus: a scoping review. Int J Audiol. (2016) 55:605–15. doi: 10.1080/14992027.2016.1198966
20. Vorkapić ST. The significance of preschool teacher's personality in early childhood education: analysis of eysenck's and big five dimensions of personality. Int J Psychol Behav Sci. (2012) 2:28–37. doi: 10.5923/j.ijpbs.20120202.05
21. O'connor BP. A quantitative review of the comprehensiveness of the five-factor model in relation to popular personality inventories. Assessment. (2002) 9:188–203. doi: 10.1177/10791102009002010
22. Hoekstra H, Ormel J, Fruyt F. NEO-PI-R/NEO-FFI Big Five Persoonlijkheidsvragenlijst. Amsterdam: Hogrefe Publishing (2007).
23. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) 339:b2535. doi: 10.1136/bmj.b2535
24. Roberts BW, Luo J, Briley DA, Chow PI, Su R, Hill PL. A systematic review of personality trait change through intervention. Psychol Bull. (2017) 143:117–41. doi: 10.1037/bul0000088
25. McCrae RR, John OP. An introduction to the five-factor model and its applications. J Pers. (1992) 60:175–215. doi: 10.1111/j.1467-6494.1992.tb00970.x
26. Church AT. Relating the tellegen and five-factor models of personality structure. J Pers Soc Psychol. (1994) 67:898–909. doi: 10.1037/0022-3514.67.5.898
27. Eysenck HJ. Five-Factor Model. (2001) Available online at: http://www.personalityresearch.org/bigfive/eysenck.html (accessed Febuary 18, 2020).
28. MacDonald DA, Holland D. Examination of relations between the NEO personality inventory-revised and the temperament and character inventory. Psychol Rep. (2002) 91:921–30. doi: 10.2466/pr0.2002.91.3.921
29. Hoekstra H, Ormel J, Fruyt F. Handleiding NEO-PI-R en NEO-FFI Persoonlijkheidsvragenlijsten Amsterdam: Hogrefe Publishing (2007).
30. Rushton JP, Irwing P. A general factor of personality (GFP) from the multidimensional personality questionnaire. Personal Indivi Differ. (2009) 47:571–6. doi: 10.1016/j.paid.2009.05.011
31. Capanna C, Struglia F, Riccardi I, Daneluzzo E, Stratta P, Rossi A. Temperament and character inventory-R (TCI-R) and big five questionnaire (BFQ): convergence and divergence. Psychol Rep. (2012) 110:1002–6. doi: 10.2466/02.03.09.PR0.110.3.1002-1006
32. Howard S, Hughes BM. Construct, concurrent and discriminant validity of type D personality in the general population: associations with anxiety, depression, stress and cardiac output. Psychol Health. (2012) 27:242–58. doi: 10.1080/08870446.2011.603423
33. Briley DA, Domiteaux M, Tucker-Drob EM. Achievement-relevant personality: relations with the big five and validation of an efficient instrument. Learn Individ Differ. (2014) 32:26–39. doi: 10.1016/j.lindif.2014.03.010
34. Lars. Das Freiburger Persönlichkeitsinventar. (2015) Available online at: http://www.typentest.de/blog/2015/11/das-freiburger-personlichkeitsinventar/ (accessed Febuary 18, 2020).
35. Costa PT, McCrae RR. Four ways five factors are basic. Personal Individ Differ. (1992) 13:653–65. doi: 10.1016/0191-8869(92)90236-I
36. Borkenau P, Ostendorf F. Untersuchungen zum fünf-faktoren-modell der persönlichkeit und seiner diagnostischen erfassung. [Investigations of the five-factor model of personality and its assessment]. Zeitschrift Differ Diagnosti Psychol. (1989) 10:239–51.
37. Cortina JM, Doherty ML, Schmitt N, Kaufman G, Smith RG. The big five personality factors in the IPI and MMPI: predictors of police performance. Person Psychol. (1992) 45:119–40. doi: 10.1111/j.1744-6570.1992.tb00847.x
38. Wells G, O'Connell D, Peterson J, Welch V, Losos M, Tugwell P, et al. The Newcastle-Ottawa Scale (NOS) For Assessing the Quality of Nonrandomised Studies in Meta-analyses. (2000) Available: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
39. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed1000097
40. Adami Dehkordi M, Javanbakht M, Sarfarazi Moghadam S, Meshkat M, Abolbashari S. Personality traits in patients with subjective idiopathic tinnitus. Iran J Otorhinolaryngol. (2015) 27:369–75. doi: 10.22038/IJORL.2015.4791
41. Andersson G, Airikka M-L, Buhrman M, Kaldo V. Dimensions of perfectionism and tinnitus distress. Psychol Health Med. (2005) 10:78–87. doi: 10.1080/13548500512331315389
42. Durai M, O'Keeffe MG, Searchfield GD. The personality profile of tinnitus sufferers and a nontinnitus control group. J Am Acad Audiol. (2017) 28:271–82. doi: 10.3766/jaaa.15103
43. Gerber KE, Nehemkis AM, Charter RA, Jones HC. Is tinnitus a psychological disorder? Int J Psychiatr Med. (1985) 15:81–7. doi: 10.2190/E59L-2PRU-GPAE-VJ8B
44. Langguth B, Kleinjung T, Fischer B, Hajak G, Eichhammer P, Sand PG. Tinnitus severity, depression, and the big five personality traits. Prog Brain Res. (2007) 166:221–5. doi: 10.1016/S0079-6123(07)66020-8
45. McCormack A, Edmondson-Jones M, Fortnum H, Dawes P, Middleton H, Munro KJ, et al. The prevalence of tinnitus and the relationship with neuroticism in a middle-aged UK population. J Psychosom Res. (2014) 76:56–60. doi: 10.1016/j.jpsychores.2013.08.018
46. Meric C, Gartner M, Collet L, Chery-Croze S. Psychopathological profile of tinnitus sufferers: evidence concerning the relationship between tinnitus features and impact on life. Audiol Neurootol. (1998) 3:240–52. doi: 10.1159/000013796
47. Salviati M, Bersani FS, Terlizzi S, Melcore C, Panico R, Romano GF, et al. Tinnitus: clinical experience of the psychosomatic connection. Neuropsychiatr Dis Treat. (2014) 10:267–75. doi: 10.2147/NDT.S49425
48. Strumila R, Lengvenyte A, Vainutiene V, Lesinskas E. The role of questioning environment, personality traits, depressive and anxiety symptoms in tinnitus severity perception. Psychiatr Q. (2017) 88:865–77. doi: 10.1007/s11126-017-9502-2
49. Weber JH, Jagsch R, Hallas B. [The relationship between tinnitus, personality, and depression]. Z Psychosom Med Psychother. (2008) 54:227–40. doi: 10.13109/zptm.2008.54.3.227
50. Welch D, Dawes PJ. Personality and perception of tinnitus. Ear Hear. (2008) 29:684–92. doi: 10.1097/AUD.0b013e318177d9ac
51. D'Amelio R, Archonti C, Schol S, Falkai P, Plinkert PK, Delb W. [Psychological distress associated with acute tinnitus]. Hno. (2004) 52:599–603. doi: 10.1007/s00106-003-0944-5
52. Wallhausser-Franke E, Delb W, Balkenhol T, Hiller W, Hormann K. Tinnitus-related distress and the personality characteristic resilience. Neural Plast. (2014) 2014:370307. doi: 10.1155/2014/370307
53. Muris P, Roelofs J, Rassin E, Franken I, Mayer B. Mediating effects of rumination and worry on the links between neuroticism, anxiety and depression. Personal Individ Differ. (2005) 39:1105–11. doi: 10.1016/j.paid.2005.04.005
54. Pattyn T, Van Den Eede F, Vanneste S, Cassiers L, Veltman DJ, Van De Heyning P, et al. Tinnitus and anxiety disorders: a review. Hear Res. (2016) 333:255–65. doi: 10.1016/j.heares.2015.08.014
55. Lo MT, Hinds DA, Tung JY, Franz C, Fan CC, Wang Y, et al. Genome-wide analyses for personality traits identify six genomic loci and show correlations with psychiatric disorders. Nat Genet. (2017) 49:152–6. doi: 10.1038/ng.3736
56. Maas IL, Brüggemann P, Requena T, Bulla J, Edvall NK, Hjelmborg JVB, et al. Genetic susceptibility to bilateral tinnitus in a Swedish twin cohort. Gene Med. (2017) 19:1007–12. doi: 10.1038/gim.2017.4
57. Okbay A, Baselmans BM, De Neve JE, Turley P, Nivard MG, Fontana MA, et al. Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat Genet. (2016) 48:624–33. doi: 10.1038/ng.3552
58. Smith DJ, Escott-Price V, Davies G, Bailey ME, Colodro-Conde L, Ward J, et al. Genome-wide analysis of over 106 000 individuals identifies 9 neuroticism-associated loci. Mol Psychiatr. (2016) 21:749–57. doi: 10.1038/mp.2016.49
59. Ziegler DK, Paolo AM. Headache symptoms and psychological profile of headache-prone individuals: a comparison of clinic patients and controls. Arch Neurol. (1995) 52:602–6. doi: 10.1001/archneur.1995.00540300076016
60. Martinez-Devesa P, Perera R, Theodoulou M, Waddell A. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev. (2010) 9:Cd005233. doi: 10.1002/14651858.CD005233.pub3
61. Hesser H, Weise C, Westin VZ, Andersson G. A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress. Clin Psychol Rev. (2011) 31:545–53. doi: 10.1016/j.cpr.2010.12.006
62. Cima RFF, Mazurek B, Haider H, Kikidis D, Lapira A, Norena A, et al. A multidisciplinary European guideline for tinnitus: diagnostics, assessment, and treatment. HNO. (2019) 67:10–42. doi: 10.1007/s00106-019-0633-7
63. Kleinstauber M, Weise C, Andersson G, Probst T. Personality traits predict and moderate the outcome of Internet-based cognitive behavioural therapy for chronic tinnitus. Int J Audiol. (2018) 57:538–44. doi: 10.1080/14992027.2018.1432902
Keywords: tinnitus, tinnitus distress, personality traits, five-factor model, neuroticism
Citation: van Munster JJCM, van der Valk WH, Stegeman I, Lieftink AF and Smit AL (2020) The Relationship of Tinnitus Distress With Personality Traits: A Systematic Review. Front. Neurol. 11:225. doi: 10.3389/fneur.2020.00225
Received: 06 November 2019; Accepted: 10 March 2020;
Published: 29 May 2020.
Edited by:
Agnieszka J. Szczepek, Charité – Universitätsmedizin Berlin, GermanyReviewed by:
Heike Argstatter, Deutsches Zentrum für Musiktherapieforschung, GermanyGrant Searchfield, The University of Auckland, New Zealand
Copyright © 2020 van Munster, van der Valk, Stegeman, Lieftink and Smit. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juliëtte J. C. M. van Munster, ai5qLmMubS52YW5fbXVuc3RlckBsdW1jLm5s
†These authors have contributed equally to this work