 Sahan Benedict Mendis
Sahan Benedict Mendis Vanessa Raymont2
Vanessa Raymont2 Naji Tabet
Naji Tabet- 1South London and Maudsley NHS Foundation Trust, London, United Kingdom
- 2Oxford Brain Health Clinical Trials Unit, Oxford, United Kingdom
- 3Center for Dementia Studies, Brighton and Sussex Medical School, Brighton, United Kingdom
Dementia is a global public health priority which cost global societies $818 billion in 2015 and is disproportionately impacting low and middle-income countries (LMICs). With limited availability of disease modifying drugs to treat Alzheimer's disease (AD), researchers have increasingly focused on preventative strategies which may promote healthy cognitive aging and mitigate the risk of cognitive impairment in aging. Lifelong bilingualism has been presented as both a highly debated and promising cognitive reserve factor which has been associated with better cognitive outcomes in aging. A recent metanalysis has suggested that bilingual individuals present on average 4.05 years later with the clinical features of AD than monolinguals. Bilinguals are also diagnosed with AD ~2.0 years later than monolingual counterparts. In this perspective piece we critically evaluate the findings of this metanalysis and consider the specific implications of these findings to LMICs. Furthermore, we appraise the major epidemiological studies conducted globally on bilingualism and the onset of dementia. We consider how both impactful and robust studies of bilingualism and cognition in older age may be conducted in LMICs. Given the limited expenditure and resources available in LMICs and minimal successes of clinical trials of disease modifying drugs we propose that bilingualism should be positioned as an important and specific public health strategy for maintaining healthy cognitive aging in LMICs. Finally, we reflect upon the scope of implementing bilingualism within the education systems of LMICs and the promotion of bilingualism as a healthy cognitive aging initiative within government policy.
Introduction
Twenty first century societies are rapidly transitioning to aging populations which are often characterized by a burden of age related conditions such as dementia (1). There are about 50 million individuals living with dementia (2); a figure that is forecasted to increase to 115 million by the year 2050 (3). The global economic cost of dementia was measured at US $818 billion in 2015 (4). The burden of dementia significantly impacts low and middle countries (LMICs)1 and by 2050 we anticipate that 71% of all people living with dementia will reside in LMICs (1).
Whilst there have been limited successes of clinical trials and disease modifying drugs (6), researchers have focused on developing public health strategies that may promote healthy aging and support the delay of onset of dementia (7). This approach may be germane to LMICs where minimal resources and unstable health systems may make running of clinical trials more challenging and logistically difficult. In these settings, dementia may be viewed as part of a normal aging process and a highly stigmatized condition and associated with limited provision of care for individuals with dementia. These additional factors may complicate how dementia prevention is addressed in non-communicable disease (NCD) policies in LMIC settings (8). There are potential promising economic benefits of delaying the onset of dementia. A recent study has demonstrated that a 1 year delay of onset of dementia reduces formal costs in 2030 by $70 billion and informal costs by $43 billion compared to no delay on dementia onset (9).
Cognitive reserve is a hypothetical construct which posits that enriching lifetime experiences and activities support the brain in mitigating the impact of pathological damage over time (10–15). This may enable individuals to cope better with brain damage and sustain greater degrees of brain damage before demonstrating functional deficits (10). Cognitive reserve factors have been associated with the delay of onset of dementia and better cognitive outcomes in aging (16). These factors include educational attainment (17), the cohesion of social networks (18), occupational complexity (19), enhanced physical activity, and cognitively stimulating activities (20). Bilingualism has been positioned as a powerful cognitive reserve factor (21) which may be associated with the delay in onset of dementia. Encouragingly cognitive reserve may be malleable even in older age which may provide significant opportunities for interventional studies of cognition in later life (22).
A recent metanalysis by Paulavicius et al. (23) revealed that studies that explored the relationship between bilingualism and age of onset of dementia revealed an average of 4.5 years in the delay of presentation of dementia amongst bilinguals. In this perspective piece, we critically review bilingualism as a cognitive reserve factor and examine the key studies of bilingualism explored in both high income countries (HICs) and LMICs. We discuss the implications of these findings to a global health context. We commentate on the key study findings of the above metanalysis. We address some of methodological limitations of the current evidence and suggest ways in which these can be overcome.
We propose that incorporating bilingualism into dementia public health policy to delay the onset of dementia is an important and specific strategy in maintaining healthy cognitive aging in LMICs. We reflect how bilingualism can be incorporated into governmental and educational policy and overall health strategy in LMICs settings and the challenges associated with this.
What is Bilingualism?
Bilingualism can be classified as individuals' ability to communicate using two languages either actively using speech or listening, or passively using writing, reading, or listening. The bilingual experience is a dynamic process and proficiency may differ according to the level of exposure to other users of each language and level of opportunity to use each language (24). Bilinguals can be described as either simultaneous; where an individual is exposed to both languages to a significant degree from birth, or alternatively sequential, where meaningful exposure to the second language is developed after the age of three (24). Bilingualism does not require any special education or intellectual ability. It is a common phenomenon, and ~50 % of the global population are proposed to have some bilingual or plurilingualism proficiency (25). Bilingual children and adults may experience difficulties with “lexical access” and reduced verbal fluency and this may lead to “tip of the tongue” experiences (26). Bilingual proficiency can be observed in different social and cultural contexts. Daily contact with two languages is observed globally in diverse settings, such as Europe (Switzerland, Belgium, and Luxemburg), Asia (India, Philippines), Africa (Senegal, South Africa), and North America (Canada).
The Case for Bilingualism as a Cognitive Reserve Factor
Lifelong bilingualism has been positioned as a cognitive reserve factor (21) and promoting buffering against age related cognitive decline. There are two distinct models of cognitive reserve; brain reserve and neuronal compensation (10, 27). The brain reserve model asserts that existing brain networks are more resilient toward deregulation because of heightened efficiency. This may be mediated through enhanced “brain hardware” (10), which may be practically achieved through increased dendritic volume, brain synapses or overall brain volume (10). These networks may facilitate brain activity when performing more complex tasks and may enable the brain to cope more effectively with degeneration. In neuronal compensation, the brain recruits additional areas that are not normally used to perform the skills that have been lost in the degenerated brain (10). Other models of cognitive reserve include a life course perspective (14), scaffolding theory (28), or the concept of brain maintenance (15).
Neuroimaging
Bilinguals simultaneously attend to two competing languages for selection which may induce neuroplasticity (29) and lead to remodeling of brain architecture and function (30). Schweizer and colleagues (21) who analyzed linear CT brain looking at brain atrophy, discerned that greater amounts of neuropathology are needed before the clinical symptoms of AD become apparent in bilinguals. Similarly, another study using PET demonstrated that bilinguals had greater regional glucose uptake than monolinguals (31). Bilingual brains have been shown to have specific activity in the frontotemporal and subcortical networks which are involved in interference inhibition, and may facilitate language switching (32). This was not demonstrated in monolinguals. Bilinguals may have increased capacity for conflict resolution through augmentation of anterior cingulate cortex activity (33).
The bilingual experience may promote more widely distributed neural activity (30), recruitment of overlapping neural regions which are not usually found in monolinguals (34) or enhancing neural activity in regions involved in executive function (30). Bilingual adults may display greater gray matter volume particular in the anterior cingulate cortex (35) parietal lobes (36), corpus callosum (37) the basal ganglia (30, 38) and the frontoparietal network (FPN) (30). Bilinguals show greater white matter integrity and gray matter functional connectivity compared to monolinguals (30). Functional MRI studies reveal that although bilinguals have equal performance in non-verbal executive tasks there is less frontal activation than monolinguals (30). This suggests that bilinguals do not rely on “top down” mechanisms in cognitive functions (30). Overall, researchers suggest that the shift from anterior to posterior brain activation amongst bilinguals “anterior-to-posterior and subcortical shift” /BAPSS (30) may provide some evidence why bilingualism is associated with improved cognitive performance in older age and delayed onset of dementia.
Neuropsychology, Epidemiology, and Lab Studies
The positive findings which are reflected in the neuroimaging studies of bilinguals are also depicted in multiple neuropsychological and epidemiological studies of bilingual adults. Bilinguals have been shown to outperform monolinguals in tests of executive function, such as cognitive control (39), working memory (40), inhibition (41), and attention (42). However, other researchers may refute findings linking bilingualism and improved executive function because many studies may be limited by small sample sizes (43), socioeconomic factors (44), education, and geographical location (45). These factors are known to have significant impact on performance of executive function (46). By contrast, Nichols et al. (47) compared the performance 11,041 (5,994 monolinguals and 5,047 bilinguals) participants on a battery of 12 executive tasks and found there was no significant difference between the two groups on executive function. These findings were independent of case mix factors (47). However, it is important to note that this study only included 744 people in the matched bilingual and monolingual sample and defined bilingualism based on a single question “How many languages do you speak (47)?” This simplistic and imprecise approach to measuring bilingual proficiency may misrepresent the nuanced complexities of bilingual proficiency and we suggest the findings of this study should be interpreted with some caution. The overall findings suggest that bilingualism and executive function research should be conducted in diverse sociocultural milieus to ascertain whether the bilingual advantage applies in different contexts.
A 12 year longitudinal Israel based study of 814 elderly Jewish people revealed trilinguals performed better on cognitive tasks than monolinguals and bilinguals (48). These findings were independent of educational achievement, occupation, age, place of birth, and immigration (48). A study explored 853 participants who were recruited into the Lothian cohort 1936 study (49). This followed adults whose age 11 IQ was measured as part of the Scottish Mental Survey 1947 (49). Repeated cognitive testing between 2008 and 2010 revealed that bilingual participants performed better than monolinguals in both reading and executive function tests, as well as in tests of intelligence (49). Another study observed that bilinguals with amnesic-type mild cognitive impairment had a reduced rate of conversion to AD compared to monolingual counterparts (50). This delay was not demonstrated in mild cognitive impairment participants with multiple domain deficits (50). Bilinguals are twice more likely to recover cognitively from stroke than monolinguals (51). Bilingualism has been associated with better ratio of CSF AD biomarkers (52).
Does Bilingualism Delay the Onset of Dementia? Key Findings From a Systematic Review
Having explored the contextual evidence supporting bilingualism as a cognitive reserve factor, we now evaluate the systematic review from Paulavicius et al. (23) exploring bilingualism and age of onset of dementia and the specific epidemiological studies exploring this relationship.
This systematic review reported findings from eight studies which examined the relationship between bilingualism and the age of onset of dementia. Metanalysis from these studies determined that bilinguals (53) with AD presented with delayed clinical features (694 individuals; mean difference MD 4.05 years; 95% CI:1.87–6.22) and are diagnosed (1,012 participants: MD 2.0 years; 95% CI 0.08–3.92) (23). This study incorporated studies which were cross sectional, cohort, case control or retrospective in design. Six of the selected studies consisted of only AD patients and four of the studies had a mixture of immigrant and non-immigrant populations. The study pooled data from four studies that had investigated the age of onset of AD symptoms (23). Secondly, five studies which determined the age of AD diagnosis were pooled. All the selected studies were retrospective in design (23). Another systematic review which examined the impact of bilingualism on the risk of cognitive decline found that bilingualism was not associated with a reduced incidence of dementia (54). This study only included prospective studies and studies of different types of dementia (54). Overall, studies suggest that bilingualism is associated with a delayed onset of clinical presentation of dementia but not reduced risk of developing dementia or reduced incidence of dementia (54–56).
Studies of Bilingualism in HICs
Tables 1, 2, respectively outlines the key studies of bilingualism conducted in HICs and LMICs. Twelve key studies of bilingualism were conducted in HICs (53, 57–59, 61, 63–66, 72, 73) and all investigated spoken bilingualism. Of the 12 studies, six studies were conducted in USA (58, 61–64, 67), four studies in Canada (53, 57, 59, 65), one study in Belgium (60) and one study in Wales (66). Nine studies involved a retrospective analysis of bilinguals vs. monolinguals. Eight studies revealed a delay of onset of dementia in bilinguals whilst four studies did not find a difference between monolinguals and bilinguals (63–66). Three studies were prospective and had a cohort or cross-sectional design (63–65) and did not find a delay of onset of dementia associated with bilingualism. All but one Canadian study revealed a positive relationship between bilingualism and delayed onset of dementia (53, 57, 59). Similar findings were found in the Belgium study (60). The sample size for these studies ranged from 86 to 1,616 subjects. Gollan et al. (58) explored bilingual objectively measures of linguistic proficiency using the Boston Naming Task. Zahodne et al. (63) also used an objective measure of English reading level. All studies used different operational definitions of bilingualism and different linguistic profiles and varying pairs of languages.
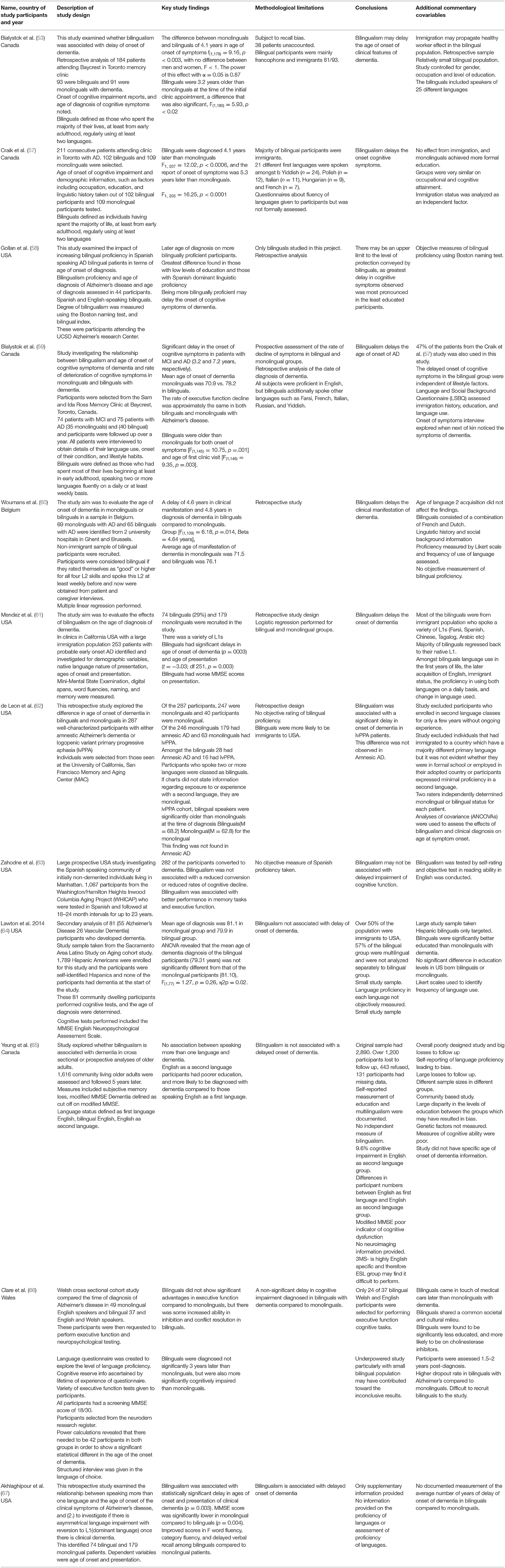
Table 1. Studies of bilingualism and age of onset of dementia in HICS.
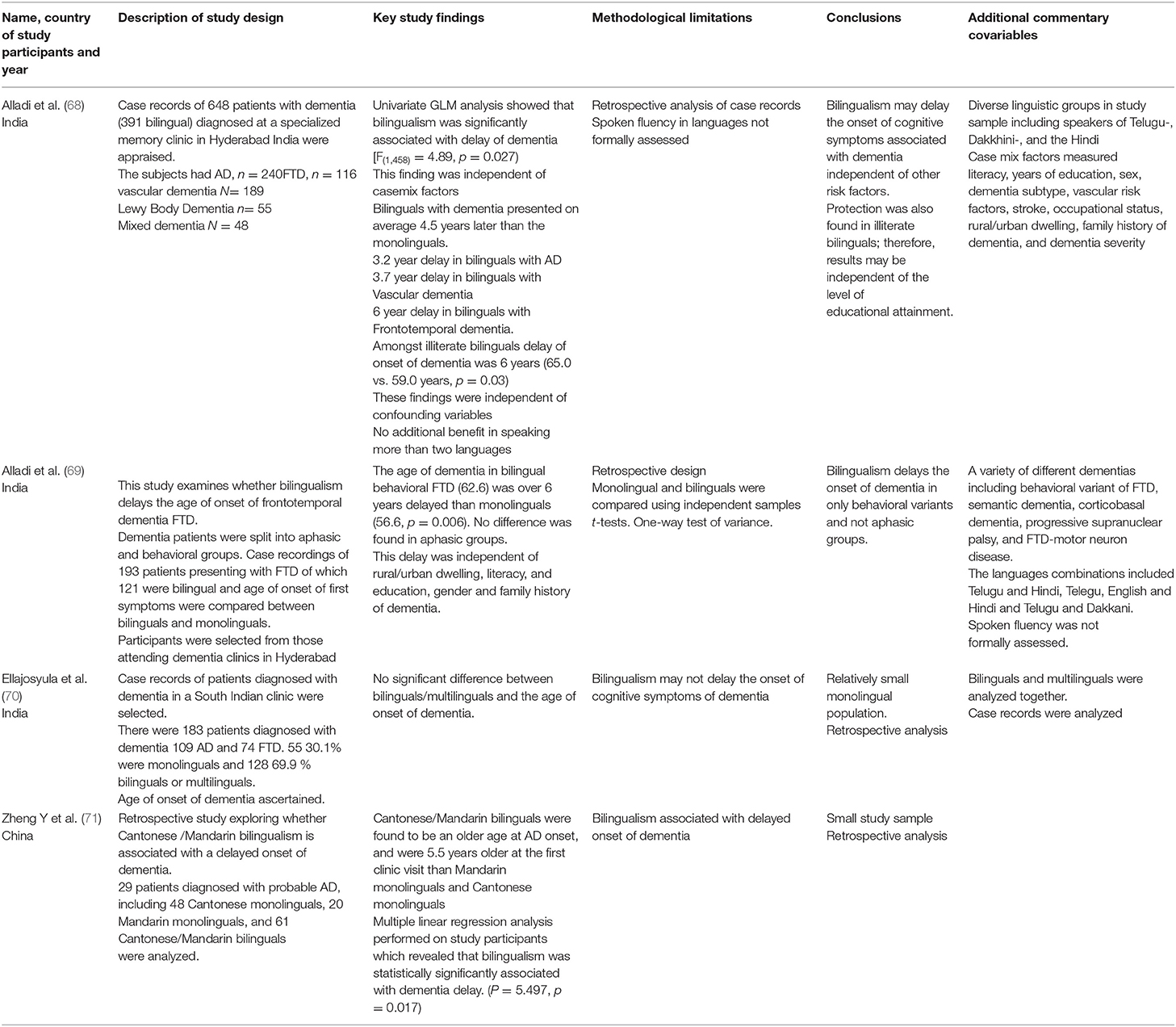
Table 2. Studies of Bilingualism and age of onset of dementia in LMICs.
Studies of Bilingualism and Age of Onset of Dementia in LMICs
Alladi and colleagues (68) evaluated hospital records of 648 patients of which 391 were bilinguals diagnosed with dementia in specialist clinics in Hyderabad, India and retrospectively evaluated age of diagnosis. This study examined patients with a variety of dementia diagnosis' including vascular dementia, Alzheimer's Disease (AD) and frontotemporal dementia (FTD) (68). This study identified that the bilinguals' mean age of dementia onset was 4.5 years later than monolinguals (68). Bilingualism was significantly associated with the delay of age of onset of dementia, with generalized linear modeling analysis revealing a significant level [F(1, 458) = 4.89, p = 0.027] after adjustment for immigration, socioeconomic status, illiteracy, education, and residence in rural and urban areas, number of languages spoken and occupational status (68). The study participants were from an autochthonous population where both the monolingual and bilingual participants were born and raised in India (68). This study evaluated important covariates as described above and determined that the findings were independent of these factors (68). In illiterate bilinguals the delay of onset of dementia was 6 years compared to monolingual counterparts (68).
A further Hyderabad based study explored the case records of 193 patients diagnosed with FTD of which 121 were bilingual (69). In this study the age of diagnosis was measured between bilinguals and monolinguals and determined that amongst bilinguals with behavioral variant FTD the age of onset of dementia was 5.7 years later in bilinguals 62.6 vs. 56.5 p = 0.006 in monolinguals (69). This finding was independent of the similar case mix factors as observed in the 2007 Hyderabad study (69). Ellajosyula et al. (70) investigated a retrospective South Indian sample of individuals diagnosed with either AD or FTD in a memory clinic. There were 183 patients with dementia where 55 were monolinguals and 129 were bilinguals or multilinguals (70). The study did not find a significant difference in the age of onset of dementia between the two groups (70).
A study explored the relationship between Mandarin and Cantonese bilingualism and age of onset of dementia in 129 patients diagnosed with probable AD, including 48 Cantonese monolinguals, 20 Mandarin monolinguals, and 61 Cantonese/Mandarin bilinguals (71). The study determined that bilingualism was independently associated with delay of onset of dementia [P = 5.497, p = 0.017 (71)].This study utilized the Bilingual Aphasia Test (BAT) (74) to obtain a detailed language history. All the key studies examined spoken bilingualism only.
Bilingualism and Cognitive Reserve Research: the Global Context
Our review of key studies investigating bilingualism and the age of the onset of dementia reveal a dearth of studies conducted in LMICs. It may be particularly challenging to directly extrapolate the findings from studies conducted in HICs to LMIC settings (75). Immigration and the potential healthy migrant effect may confound the findings of some studies conducted in HICs. In studies conducted in LMICs bilinguals observed may be from autochthonous populations and in populations where there is a lot of language switching (68). Many contextual challenges including the high prevalence of illiteracy and HIV, unemployment and key differences in employment in both rural and urban settings exist (75). Examples include the unskilled, illiterate craft maker, or illiterate factory worker. The differing ethnic and genetic profiles, such as ApoE may interact or modify the benefits of bilingualism on individuals (75). Other important issues include the high prevalence of head injuries and vascular risk factors and poorly resourced health systems may further complicate assessment and interpretation of research findings (75).
We determine that interactive factors, such as ethnicity, poverty, epigenetics, polluted environments, social deprivation, differing cultures, economics, and politics may have a significant impact in how bilingualism and cognitive reserve research is conducted and interpreted (75). A detailed list of potential interactive factors is outlined in Figure 1. We suggest that tools which formally assess bilingual fluency, such as a culturally amended Boston naming task or BAT, should accompany self-reported fluency of language use. We recommend strict and standardized study definitions of bilingualism should be employed in studies.
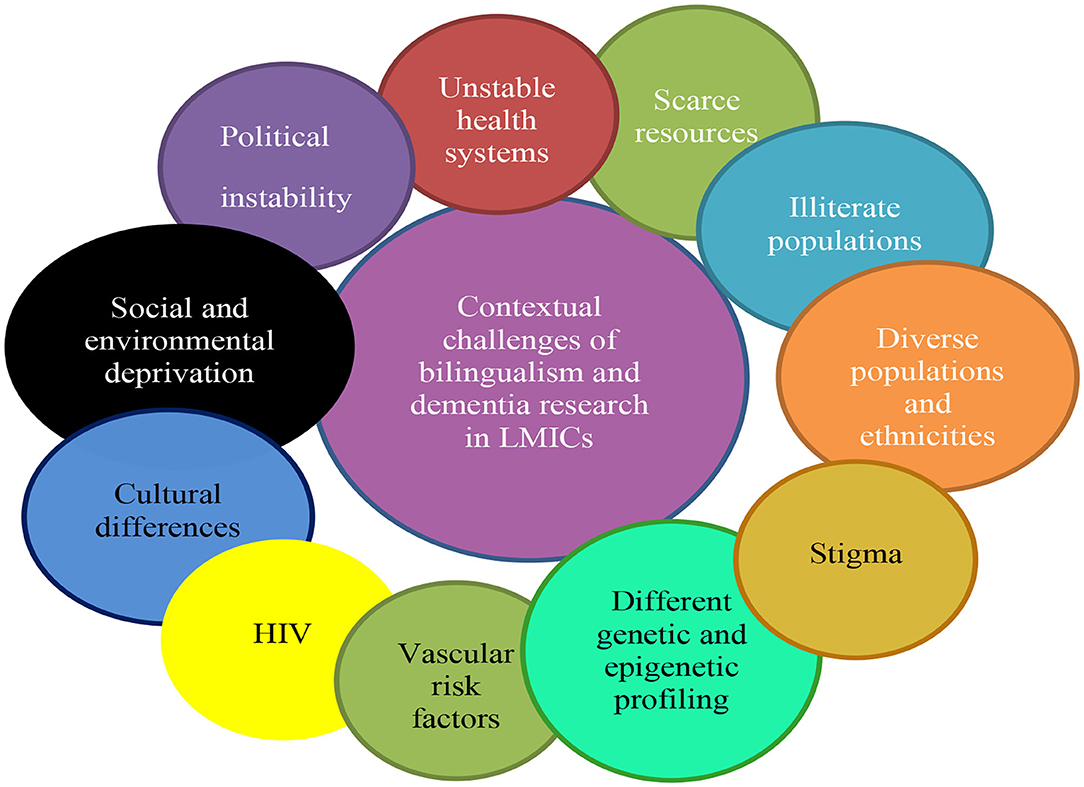
Figure 1. The key contextual challenges of bilingualism and cognitive reserve research in LMICs.
Specific challenges may arise when utilizing neuropsychological tests in many LMIC settings for bilingualism and dementia research. Traditionally these tests have been derived for educated and English-speaking western populations and may have limited applicability to other cultures (76, 77). Although, Alladi and colleagues (68) successfully used culturally and linguistically amended versions of the Addenbrookes Cognitive Examination and Dementia Rating Scale there are other specific challenges to consider. High rates of illiteracy in LMIC settings may further complicate the adaptation of these tests (77). There have been attempts to derive culturally unbiased and educationally fair testing (77). Researchers assert that focusing on cognitive tools that emphasizes visual skills, such as the Oxford Cognitive Screen (OCS-Plus) (78) may help to overcome this difficulty. The OCS-Plus is a visual orientated cognitive tool which assesses nine domains of cognition (78). A validation study of the OCS-Plus in a South African study sample in which 45% of the sample did not have any formal education revealed that the OCS-Plus had excellent construct and external validity in detecting cognitive impairment (79). Perhaps we should employ tools, such as OCS Plus in measuring cognition in certain LMICs where low education or literacy levels prevail.
Although the limited neuroimaging resources particularly in rural areas make it challenging to research bilingualism and cognitive reserve, there are examples of big, funded neuroimaging studies conducted in LMICs such as the Health and Aging in Africa: A Longitudinal Study of an INDEPTH Community in South Africa(HAALSI) (79) and the Bangladesh Early Adversity Neuroimaging study (BEAN) (80).We advocate that major global stakeholding funders encourage applicants to present novel approaches, such as researching cognitive reserve in the bilingual brain within LMIC settings. We recommend that both prospective and retrospective studies to be conducted in diverse linguistic and cultural milieu such as South Africa, parts of Latin America and central Asia. Reproducibility of findings in different settings are imperative to understanding how bilingualism and cognitive reserve research is operationalized in a variety of environs.
Future Research Directions
Finally, we address how future studies of bilingualism and cognitive reserve could be conducted to help us understand the potential benefits of bilingualism in a globalized context. We propose that studies of bilingualism could be performed in high risk and vulnerable populations, such as individuals with mild cognitive impairment (MCI), those with a strong family history of cognitive impairment or genetically susceptible populations. Furthermore, we suggest that prospective studies could be explored in bilingual and monolingual cohorts with a strong vascular history (75), culturally diverse illiterate populations (75), those with limited educational attainment (75), and in specific cultural groups (81). This may help to determine if and how bilingualism may moderate or delay the clinical presentation of cognitive impairment in those with pre-existing risk factors. There may be scope to conduct large longitudinal studies of bilingualism and cognitive aging in densely populated communities in Latin America (82) and mainland China (83) where a range of diverse risk factors are frequently present. Novel and region specific strategies which include the Latin American and Caribbean Consortium on Dementia (LAC-CD1) (84), an approach funded by the Alzheimer's Association and the Global Brain Health Institute may promote the practical implementation of these approaches.
With the advent of neuroimaging modalities and possible increased availability of investigations in LMICs it may be possible to examine how bilingualism may be linked with specific structural neuroimaging findings such as volumetric temporal lobe changes. More relevant information may also be gained from functional magnetic resonance imaging and diffusion tensor imaging. The use of specific neuroimaging techniques, such as fluorodeoxyglucose positron emission tomography (FDG-PET) may be helpful (85), as is the visualization of early amyloid and tau aggregates also assessed through PET. We suggest that studies can also explore the relationship between bilingual proficiency in older adults with the presence of CSF or plasma biomarkers for AD in addition to APOE status.
We emphasize that taking a detailed linguistic history is particularly salient in establishing bilingual proficiency in studies of bilingualism and cognitive reserve. Practical considerations include structured documentation of the level of frequency of language use, subjective linguistic competency, age of acquisition of languages, context of use, formal competency assessment of verbal fluency of languages, formal qualifications in each language and degree of language switching. These factors could be compiled in a structured linguistic competency questionnaire. We assert that by employing a more global and structured approach to linguistic competency we may be able to devise a rating scale which may provide an objective measure of linguistic proficiency.
Discussion
Bilingualism: A Global Public Health Strategy for Healthy Cognitive Aging
We now propose bilingualism as a significant public health initiative for healthy cognitive aging in LMICs and consider how this could be incorporated into policy. The G8 and WHO have highlighted that upscaling public health indicatives should be a focus on dementia management in LMICs (86). We encourage that adopting bilingualism into dementia policy in LMICs could be formalized through organizations such the Alzheimer's Disease International (87) and STRiDE: Strengthening responses to dementia in developing countries which advocate the public health approach (88).
There is an intrinsic value of delaying the onset of dementia (9). A delay of AD onset of 5 years may represent a 41% lower prevalence of lower cost of AD in 2050 (9). In HICs this delay may also equate to 2.7 additional life years and lower informal costs (9). We highlight that delaying the onset of dementia may be even more significant in LMICs where treatments are not freely available, and nursing and care needs are frequently placed on the children of those diagnosed with dementia. This may lead to significant losses of occupational and economic productivity amongst individuals of working age.
We discuss how bilingualism-based measures could be practically adopted within public health strategies in LMICs. One approach would be to promote bilingualism from childhood. Benson explored how bilingual language programs can be incorporated into school curriculum in LMICs using examples from Guinea-Bissau, Niger, Mozambique, and Bolivia (89). Benson suggests that bilingual teaching programs which are decentralized, linked to local culture and proficiency in mother tongue and include specialist language teachers may be more likely to be successful and welcomed by parents (89). Successful programs include the Nigerian six-year Yoruba medium project (90) and Guinea-Bissau bilingual project which integrated subject matter into themes, such as preventive health and improved gardening methods (91).
Whilst we have demonstrated the contribution of bilingualism toward cognitive reserve, we consider whether language learning in older age could be a feasible public health strategy to delay the onset of dementia in LMICs. Prior research has suggested that brain training may foster positive brain changes in healthy adults (92) and older people (93). This may indicate that mental stimulation may promote neuroplasticity even in the older adult. Learning a second language may cultivate healthy brain aging through engagement of additional brain networks (94).
A study which examined the benefits of one week of intensive Scottish Gaelic language training in older monolinguals revealed that these participants had improved in task switching cognitive tests (95). Improved cognitive performance was maintained at 9 months follow up in individuals who practiced Gaelic for at least 5 hours a week following the end of training (95). However, these findings were not replicated in a study of Spanish monolinguals who learnt Basque (96). Differences in the study design may have impacted the overall study findings. We suggest that future studies employ wide ranging and different bilingual linguistic profiles and are conducted in varied cultural and economic settings may help to discern more robust evidence in favor of bilingualism. Computer based approaches in language lessons has been explored (97), but we suggest less resource intense methods might be appropriate in LMICs.
Bak and colleagues (95) suggest that weekly 5 hours of minimum language training may be required to produce the cognitive benefits of bilingualism (95). In many LMICs where multiple languages are spoken, the principle language taught in schools may not necessarily be the mother tongue (89). Given this, we suggest that a personalized teaching program which incorporates local cultural practices and proficiency of inborne languages might be more beneficial in these settings. Conversely, in older populations where the proficiency may lie in the mother tongue, formal learning of a secondary language may be more advantageous in promoting healthy cognitive aging.
Conclusion
This perspective has examined the role of bilingualism as a cognitive reserve factor from a wide range of evidential sources. We have explored studies of bilingualism conducted in both HICs and LMICs and reflected upon an important metanalysis that demonstrated that bilingualism is associated with a significant delay of onset of dementia. We determine that many key studies of bilingualism are limited by inconsistent working definitions of bilingualism and few have utilized objective measures of bilingual fluency. Furthermore, while several retrospective bilingualism studies have identified a significant delay in dementia onset this finding has not been replicated in prospective studies. We suggest that future research should explore the reasoning behind this discrepancy. Contextual challenges in LMICs including the high prevalence of illiteracy, HIV, socio-cultural and environmental disparities, and differing risk factors may complicate the overall picture.
Whilst finding a definitive treatment is the gold standard in dementia research, we suggest that public health measures that may promote the delay of clinical features of dementia, such as language lessons for the elderly or augmenting pre-existing bilingual proficiency in older age is important. This may be particularly salient in LMICs where cheap, pragmatic, and easily accessible approaches are warranted. If we are to harness the key benefits that bilingualism may provide, we encourage major stakeholders including governmental and health system providers to develop social programs and interventions to support the preservation of a second language.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
SM was the principle author for this paper and derived the key topics for discussion in this paper. NT and VR provided general feedback and editorial comments. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This paper was completed as part as an NIHR academic clinical fellowship in Old Age Psychiatry based at Brighton and Sussex Medical School.
Footnotes
References
1. United Nations. Division World Population Aging. Department of Economic and Social Affairs Population (2015)
2. World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. World H, Organization (2019).
3. Prince MJ, Prina M, Guerchet M. World Alzheimer report 2013: Journey of caring: an analysis of long-term care for dementia. Alzheimer's Disease International (2013).
4. Wimo A, Guerchet M, Ali G-C, Wu Y-T, Prina AM, Winblad B, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. (2017) 13:1–7. doi: 10.1016/j.jalz.2016.07.150
6. Huang L-K, Chao S-P, Hu C-J. Clinical trials of new drugs for Alzheimer disease. J Biomed Sci. (2020) 27:18. doi: 10.1186/s12929-019-0609-7
7. Cahill S. WHO's Global Action Plan on the Public Health Response to Dementia: Some Challenges and Opportunities. Taylor & Francis (2020).
8. Ferri CP, Jacob K. Dementia in low-income and middle-income countries: different realities mandate tailored solutions. PLoS Med. (2017) 14:e1002271. doi: 10.1371/journal.pmed.1002271
9. Zissimopoulos J, Crimmins E, St Clair P. The value of delaying alzheimer's disease onset. Forum Health Econ Policy. (2014) 18:25–39. doi: 10.1515/fhep-2014-0013
10. Stern Y. Cognitive reserve. Neuropsychologia. (2009) 47:2015–28. doi: 10.1016/j.neuropsychologia.2009.03.004
11. Stern Y. Cognitive reserve and Alzheimer disease. Alzheimer Dis Asso Disord. (2006) 20:S69–74. doi: 10.1097/00002093-200607001-00010
12. Stern Y, Arenaza-Urquijo EM, Bartrés-Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. (2020) 16:1305–11. doi: 10.1016/j.jalz.2018.07.219
13. Satz P, Cole MA, Hardy DJ, Rassovsky Y. Brain and cognitive reserve: mediator (s) and construct validity, a critique. J Clin Exp Neuropsychol. 2011;33(1):121–30. doi: 10.1080/13803395.2010.493151
14. Richards M, Deary IJ. A life course approach to cognitive reserve: a model for cognitive aging and development? Ann Neurol. (2005) 58:617–22. doi: 10.1002/ana.20637
15. Nyberg L, Lövdén M, Riklund K, Lindenberger U, Bäckman L. Memory aging and brain maintenance. Trends Cogn Sci. (2012) 16:292–305. doi: 10.1016/j.tics.2012.04.005
16. Stern Y. Cognitive reserve in ageing and Alzheimer's disease. Lancet Neurol. (2012) 11:1006–12. doi: 10.1016/S1474-4422(12)70191-6
17. Roe CM, Xiong C, Miller JP, Morris JC. Education and Alzheimer disease without dementia. Support for the cognitive reserve hypothesis. Neurology. (2007) 68:223–8. doi: 10.1212/01.wnl.0000251303.50459.8a
18. Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer's disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol. (2006) 5:406–12. doi: 10.1016/S1474-4422(06)70417-3
19. Boots EA, Schultz SA, Almeida RP, Oh JM, Koscik RL, Dowling MN, et al. Occupational complexity and cognitive reserve in a middle-aged cohort at risk for Alzheimer's disease. Arch Clin Neuropsychol. (2015) 30:634–42. doi: 10.1093/arclin/acv041
20. Cheng S-T. Cognitive reserve and the prevention of dementia: the role of physical and cognitive activities. Curr Psychiatry Rep. (2016) 18:85. doi: 10.1007/s11920-016-0721-2
21. Schweizer TA, Ware J, Fischer CE, Craik FIM, Bialystok E. Bilingualism as a contributor to cognitive reserve: evidence from brain atrophy in Alzheimer's disease. Cortex. (2012) 48:991–6. doi: 10.1016/j.cortex.2011.04.009
22. Lenehan ME, Summers MJ, Saunders NL, Summers JJ, Ward DD, Ritchie K, et al. Sending your grandparents to university increases cognitive reserve: the Tasmanian healthy brain project. Neuropsychology. (2016) 30:525. doi: 10.1037/neu0000249
23. Paulavicius AM, Mizzaci CC, Tavares DRB, Rocha AP, Civile VT, Schultz RR, et al. Bilingualism for delaying the onset of Alzheimer's disease: a systematic review and meta-analysis. Eur Geriatr Med. (2020) 11:651–8. doi: 10.1007/s41999-020-00326-x
24. American Speech Language Hearing Association. Knowledge and Skills Needed by Speech-Language Pathologists and Audiologists to Provide Culturally and Linguistically Appropriate Services. Association AS-L-H (2004).
25. Hammer K. Bilingual: life and reality, by François Grosjean, Cambridge, Massachusetts, and London, England, Harvard University Press, 2010, 276 pp., $26.95,£ 19.95 (hardcover), ISBN 978-0-674-04887-4. Sociolinguistic Studies. (2013) 6:595–602. doi: 10.1558/sols.v6i3.595
26. Pyers JE, Gollan TH, Emmorey K. Bimodal bilinguals reveal the source of tip-of-the-tongue states. Cognition. (2009) 11:323–9. doi: 10.1016/j.cognition.2009.04.007
27. Stern Y. What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc. (2002) 8:448–60. doi: 10.1017/S1355617702813248
28. Goh JO, Park DC. Neuroplasticity and cognitive aging: the scaffolding theory of aging and cognition. Restor Neurol Neurosci. (2009) 27:391–403. doi: 10.3233/RNN-2009-0493
29. Bialystok E, Craik FI, Luk G. Bilingualism: consequences for mind and brain. Trends Cogn Sci. (2012) 16:240–50. doi: 10.1016/j.tics.2012.03.001
30. Grundy JG, Anderson JAE, Bialystok E. Neural correlates of cognitive processing in monolinguals and bilinguals. Ann N Y Acad Sci. (2017) 1396:183–201. doi: 10.1111/nyas.13333
31. Kowoll ME, Degen C, Gorenc L, Küntzelmann A, Fellhauer I, Giesel F, et al. Bilingualism as a contributor to cognitive reserve? evidence from cerebral glucose metabolism in mild cognitive impairment and Alzheimer's disease. Front Psychiatry. (2016) 7:62. doi: 10.3389/fpsyt.2016.00062
32. Hervais-Adelman AG, Moser-Mercer B, Golestani N. Executive control of language in the bilingual brain: integrating the evidence from neuroimaging to neuropsychology. Front Psychol. (2011) 2:234. doi: 10.3389/fpsyg.2011.00234
33. Price CJ, Green DW, Von Studnitz R. A functional imaging study of translation and language switching. Brain. (1999) 122:2221–35. doi: 10.1093/brain/122.12.2221
34. Abutalebi J, Green DW. Neuroimaging of language control in bilinguals: neural adaptation and reserve. Bilingualism Lang Cogn. (2016) 19:689–98. doi: 10.1017/S1366728916000225
35. Abutalebi J, Guidi L, Borsa V, Canini M, Della Rosa PA, Parris BA, et al. Bilingualism provides a neural reserve for aging populations. Neuropsychologia. (2015) 69:201–10. doi: 10.1016/j.neuropsychologia.2015.01.040
36. Wei M, Joshi AA, Zhang M, Mei L, Manis FR, He Q, et al. How age of acquisition influences brain architecture in bilinguals. J Neurolinguistics. (2015) 36:35–55. doi: 10.1016/j.jneuroling.2015.05.001
37. Coggins Iii PE, Kennedy TJ, Armstrong TA. Bilingual corpus callosum variability. Brain Lang. (2004) 89:69–75. doi: 10.1016/S0093-934X(03)00299-2
38. Alexander GE, Crutcher MD. Functional architecture of basal ganglia circuits: neural substrates of parallel processing. Trends Neurosc. (1990) 13:266–71. doi: 10.1016/0166-2236(90)90107-L
39. Bialystok E, Craik F, Luk G. Cognitive control and lexical access in younger and older bilinguals. J Exp Psychol Learn Mem Cogn. (2008) 34:859. doi: 10.1037/0278-7393.34.4.859
40. Grundy JG, Timmer K. Bilingualism and working memory capacity: a comprehensive meta-analysis. Second Lang Res. (2016) 33:325–40. doi: 10.1177/0267658316678286
41. Hernández M, Costa A, Fuentes LJ, Vivas AB, Sebastián-Gallés N. The impact of bilingualism on the executive control and orienting networks of attention. Bilingualism Lang Cogn. (2010) 13:315–25. doi: 10.1017/S1366728909990010
42. Brito NH, Murphy ER, Vaidya C, Barr R. Do bilingual advantages in attentional control influence memory encoding during a divided attention task? Bilingualism Lang Cogn. (2016) 19:621–9. doi: 10.1017/S1366728915000851
43. Paap KR, Johnson HA, Sawi O. Should the search for bilingual advantages in executive functioning continue? Cortex. (2016) 74:305–14. doi: 10.1016/j.cortex.2015.09.010
44. Morton JB, Harper SN. What did Simon say? Revisiting the bilingual advantage. Dev Sci. (2007) 10:719–26. doi: 10.1111/j.1467-7687.2007.00623.x
45. Blumenfeld HK, Marian V. Cognitive control in bilinguals: advantages in Stimulus–Stimulus inhibition. Bilingualism (Cambridge, England). (2014) 17:610. doi: 10.1017/S1366728913000564
46. Noble KG, Norman MF, Farah MJ. Neurocognitive correlates of socioeconomic status in kindergarten children. Dev Sci. (2005) 8:74–87. doi: 10.1111/j.1467-7687.2005.00394.x
47. Nichols ES, Wild CJ, Stojanoski B, Battista ME, Owen AM. Bilingualism affords no general cognitive advantages: a population study of executive function in 11,000 People. Psychol Sci. (2020) 31:548–67. doi: 10.1177/0956797620903113
48. Kavé G, Eyal N, Shorek A, Cohen-Mansfield J. Multilingualism and cognitive state in the oldest old. Psychol Aging. (2008) 23:70. doi: 10.1037/0882-7974.23.1.70
49. Bak TH, Nissan JJ, Allerhand MM, Deary IJ. Does bilingualism influence cognitive aging? Ann neurol. (2014) 75:959–63. doi: 10.1002/ana.24158
50. Ossher L, Bialystok E, Craik FI, Murphy KJ, Troyer AK. The effect of bilingualism on amnestic mild cognitive impairment. J Gerontol B Psychol Sci Soc Sci. (2013) 68:8–12. doi: 10.1093/geronb/gbs038
51. Alladi S, Bak TH, Mekala S, Rajan A, Chaudhuri JR, Mioshi E, et al. Impact of bilingualism on cognitive outcome after stroke. Stroke. (2016) 47:258–61. doi: 10.1161/STROKEAHA.115.010418
52. Estanga A, Ecay-Torres M, Ibañez A, Izagirre A, Villanua J, Garcia-Sebastian M, et al. Beneficial effect of bilingualism on Alzheimer's disease CSF biomarkers and cognition. Neurobiol Aging. (2017) 50:144–51. doi: 10.1016/j.neurobiolaging.2016.10.013
53. Bialystok E, Craik FI, Freedman M. Bilingualism as a protection against the onset of symptoms of dementia. Neuropsychologia. (2007) 45:459–64. doi: 10.1016/j.neuropsychologia.2006.10.009
54. Mukadam N, Sommerlad A, Livingston G. The relationship of bilingualism compared to monolingualism to the risk of cognitive decline or dementia: a systematic review and meta-analysis. J Alzheimers Dis. (2017) 58:45–54. doi: 10.3233/JAD-170131
55. Anderson JA, Hawrylewicz K, Grundy JG. Does bilingualism protect against dementia? A meta-analysis. Psychon Bull Rev. (2020) 27:952–65. doi: 10.3758/s13423-020-01736-5
56. Brini S, Sohrabi HR, Hebert JJ, Forrest MR, Laine M, Hämäläinen H, et al. Bilingualism is associated with a delayed onset of dementia but not with a lower risk of developing it: a Systematic review with Meta-Analyses. Neuropsychol Rev. (2020) 30:1–24. doi: 10.1007/s11065-020-09426-8
57. Craik FI, Bialystok E, Freedman M. Delaying the onset of Alzheimer disease: bilingualism as a form of cognitive reserve. Neurology. (2010) 75:1726–9. doi: 10.1212/WNL.0b013e3181fc2a1c
58. Gollan TH, Salmon DP, Montoya RI, Galasko DR. Degree of bilingualism predicts age of diagnosis of Alzheimer's disease in low-education but not in highly educated Hispanics. Neuropsychologia. (2011) 49:3826–30. doi: 10.1016/j.neuropsychologia.2011.09.041
59. Bialystok E, Craik FI, Binns MA, Ossher L, Freedman M. Effects of bilingualism on the age of onset and progression of MCI and AD: evidence from executive function tests. Neuropsychology. (2014) 28:290. doi: 10.1037/neu0000023
60. Woumans E, Santens P, Sieben A, Versijpt J, Stevens M, Duyck W. Bilingualism delays clinical manifestation of Alzheimer's disease. Bilingualism Lang Cogn. (2015) 18:568–74. doi: 10.1017/S136672891400087X
61. Mendez MF, Chavez D, Akhlaghipour G. Bilingualism delays expression of Alzheimer's clinical syndrome. Dementia and Geriatric Cognitive Disorders. (2019) 48:281–9. doi: 10.1159/000505872
62. de Leon J, Grasso SM, Welch A, Miller Z, Shwe W, Rabinovici GD, et al. Effects of bilingualism on age at onset in two clinical Alzheimer's disease variants. Alzheimers Dement. (2020) 16:1704–13. doi: 10.1002/alz.12170
63. Zahodne LB, Schofield PW, Farrell MT, Stern Y, Manly JJ. Bilingualism does not alter cognitive decline or dementia risk among Spanish-speaking immigrants. Neuropsychology. (2014) 28:238. doi: 10.1037/neu0000014
64. Lawton DM, Gasquoine PG, Weimer AA. Age of dementia diagnosis in community dwelling bilingual and monolingual Hispanic Americans. Cortex. (2014) 66:141–5. doi: 10.1016/j.cortex.2014.11.017
65. Yeung CM, John PDS, Menec V, Tyas SL. Is bilingualism associated with a lower risk of dementia in community-living older adults? Cross-sectional and prospective analyses. Alzheimer Dis Assoc Disord. (2014) 28:326–32. doi: 10.1097/WAD.0000000000000019
66. Clare L, Whitaker CJ, Craik FI, Bialystok E, Martyr A, Martin-Forbes PA, et al. Bilingualism, executive control, and age at diagnosis among people with early-stage Alzheimer's disease in Wales. J Neuropsychol. (2016) 10:163–85. doi: 10.1111/jnp.12061
67. Akhlaghipour G, Chavez D, Mendez M. Bilingualism associated with delay in dementia onset and loss of the second language (5259). Neurology. (2020) 94:5259.
68. Alladi S, Bak TH, Duggirala V, Surampudi B, Shailaja M, Shukla AK, et al. Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology. (2013) 81:1938–44. doi: 10.1212/01.wnl.0000436620.33155.a4
69. Alladi S, Bak TH, Shailaja M, Gollahalli D, Rajan A, Surampudi B, et al. Bilingualism delays the onset of behavioral but not aphasic forms of frontotemporal dementia. Neuropsychologia. (2017) 99:207–12. doi: 10.1016/j.neuropsychologia.2017.03.021
70. Ellajosyula R, Narayanan J, Ramanan S, Chandrashekar S, Sabnis P. Bilingualism Does Not Delay the Age at Onset of Dementia-A Study From Memory Clinic in South India (P6. 206). AAN Enterprises (2015).
71. Zheng Y, Wu Q, Su F, Fang Y, Zeng J, Pei Z. The protective effect of cantonese/ mandarin bilingualism on the onset of Alzheimer disease. Dement Geriatr Cogn Disord. (2018) 45:210–9. doi: 10.1159/000488485
72. Bialystok E, Poarch G, Luo L, Craik FIM. Effects of bilingualism and aging on executive function and working memory. Psychol Aging. (2014) 29:696–705. doi: 10.1037/a0037254
73. Akhlaghipour G, Chavez D, Mendez M. Bilingualism Associated With Delay in Dementia Onset and Loss of the Second Language (5259). AAN Enterprises (2020).
74. Paradis M. Principles underlying the Bilingual Aphasia Test (BAT) and its uses. Clin Linguist Phon. (2011) 25:427–43. doi: 10.3109/02699206.2011.560326
75. Alladi S, Hachinski V. World dementia: one approach does not fit all. Neurology. (2018) 91:264–70. doi: 10.1212/WNL.0000000000005941
76. Waheed W, Mirza N, Waheed MW, Malik A, Panagioti M. Developing and implementing guidelines on culturally adapting the Addenbrooke's cognitive examination version III (ACE-III): a qualitative illustration. BMC Psychiatry. (2020) 20:492. doi: 10.1186/s12888-020-02893-6
77. Watermeyer T, Calia C. Neuropsychological assessment in preclinical and prodromal Alzheimer disease: a global perspective. J Glob Health. (2019) 9:010317. doi: 10.7189/jogh.09.010317
78. Demeyere N, Haupt M, Webb S, Strobel L, Milosevich E, Moore M, et al. The Oxford Cognitive Screen – Plus (OCS-Plus): a tablet based short cognitive screening tool for milder cognitive impairment. PsyArXiv. (2020). doi: 10.31234/osf.io/b2vgc
79. Humphreys GW, Duta MD, Montana L, Demeyere N, McCrory C, Rohr J, et al. Cognitive function in low-income and low-literacy settings: validation of the tablet-based Oxford cognitive screen in the health and aging in Africa: a longitudinal study of an INDEPTH Community in South Africa (HAALSI). J Gerontol B Psychol Sci Soc Sci. (2017) 72:38–50. doi: 10.1093/geronb/gbw139
80. Perdue KL, Jensen SK, Kumar S, Richards JE, Kakon SH, Haque R, et al. Using functional near-infrared spectroscopy to assess social information processing in poor urban Bangladeshi infants and toddlers. Dev Sci. (2019) 22:e12839. doi: 10.1111/desc.12839
81. Calia C, Johnson H, Cristea M. Cross-cultural representations of dementia: an exploratory study. J Glob Health. (2019) 9:011001. doi: 10.7189/jogh.09.011001
82. Parra MA, Baez S, Sedeño L, Gonzalez Campo C, Santamaría-García H, Aprahamian I, et al. Dementia in Latin America: paving the way toward a regional action plan. Alzheimers Dement. (2021) 17:295–313. doi: 10.1002/alz.12202
83. Jia L, Quan M, Fu Y, Zhao T, Li Y, Wei C, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. (2020) 19:81–92. doi: 10.1016/S1474-4422(19)30290-X
84. (LAC-CD) LAaCCoD. Available online at: http://lac-cd.org/home/ (accessed March 10, 2021).
85. Ou Y-N, Xu W, Li J-Q, Guo Y, Cui M, Chen K-L, et al. FDG-PET as an independent biomarker for Alzheimer's biological diagnosis: a longitudinal study. Alzheimers Res Ther. (2019) 11:57. doi: 10.1186/s13195-019-0512-1
86. Reich MR, Takemi K. G8 and strengthening of health systems: follow-up to the Toyako summit. Lancet. (2009) 373:508–15. doi: 10.1016/S0140-6736(08)61899-1
87. Wortmann M. Dementia: a global health priority - highlights from an ADI and World Health Organization report. Alzheimers Res Ther. (2012) 4:40. doi: 10.1186/alzrt143
88. Farina N, Ibnidris A, Alladi S, Comas-Herrera A, Albanese E, Docrat S, et al. A systematic review and meta-analysis of dementia prevalence in seven developing countries: a STRiDE project. Glo Public Health. (2020) 15:1–16. doi: 10.1080/17441692.2020.1792527
89. Benson C. Real and Potential Benefits of Bilingual Programmes in Developing Countries. Int J Bilingual Educ Bilingualism. (2002) 5:303–17. doi: 10.1080/13670050208667764
90. Fafunwa AB. Education in the mother-tongue: a nigerian experiment–the six-year (yoruba medium) primary education project at the University of Ife, Nigeria. West Afr J Educ. (1975) 19:213–27.
91. Benson CJ. Teaching Beginning Literacy in the “mother Tongue”: A Study of the Experimental Crioulo/Portuguese Primary Project in Guinea-Bissau. Los Angeles, CA: University of California, (1994).
92. Lampit A, Hallock H, Valenzuela M. Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers. PLoS Med. (2014) 11:e1001756. doi: 10.1371/journal.pmed.1001756
93. Valenzuela MJ, Jones M, Caroline Rae WW, Graham S, Shnier R, Sachdev P. Memory training alters hippocampal neurochemistry in healthy elderly. NeuroReport. (2003) 14:1333–7. doi: 10.1097/01.wnr.0000077548.91466.05
94. Rodríguez-Fornells A, Cunillera T, Mestres-Missé A, de Diego-Balaguer R. Neurophysiological mechanisms involved in language learning in adults. Philos Trans R Soc B Biol Sci. (2009) 364:3711–35. doi: 10.1098/rstb.2009.0130
95. Bak TH, Long MR, Vega-Mendoza M, Sorace A. Novelty, challenge, and practice: The impact of intensive language learning on attentional functions. PloS ONE. (2016) 11:e0153485. doi: 10.1371/journal.pone.0153485
96. Ramos S, Fernández García Y, Antón E, Casaponsa A, Duñabeitia JA. Does learning a language in the elderly enhance switching ability? J Neurolinguistics. (2017) 43:39–48. doi: 10.1016/j.jneuroling.2016.09.001
Keywords: bilingualism, cognitive reserve, dementia, healthy cognitive aging, global public health, low and middle income countries, contextual challenges
Citation: Mendis SB, Raymont V and Tabet N (2021) Bilingualism: A Global Public Health Strategy for Healthy Cognitive Aging. Front. Neurol. 12:628368. doi: 10.3389/fneur.2021.628368
Received: 11 November 2020; Accepted: 16 March 2021;
Published: 15 April 2021.
Edited by:
Maira Okada de Oliveira, University of São Paulo, BrazilReviewed by:
John A. E. Anderson, Center for Addiction and Mental Health (CAMH), CanadaAnthoula Charalampos Tsolaki, Aristotle University of Thessaloniki, Greece
Copyright © 2021 Mendis, Raymont and Tabet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sahan Benedict Mendis, c2FoYW4ubWVuZGlzQG5ocy5uZXQ=