 Giulio Mastria1,2*†
Giulio Mastria1,2*† Alessandro Viganò3*†
Alessandro Viganò3*† Alessandra Corrado1Valentina Mancini1,4Cristina Pirillo1
Alessandra Corrado1Valentina Mancini1,4Cristina Pirillo1 Simone Badini1Barbara Petolicchio1
Simone Badini1Barbara Petolicchio1 Massimiliano Toscano1,5
Massimiliano Toscano1,5 Marta Altieri1Roberto Delle Chiaie1
Marta Altieri1Roberto Delle Chiaie1 Vittorio Di Piero1,6
Vittorio Di Piero1,6- 1Department of Human Neurosciences, Sapienza—University of Rome, Rome, Italy
- 2My Space Lab, Department of Clinical Neuroscience, Centre Hospitalier Universitaire Vaudois (CHUV), University of Lausanne, Lausanne, Switzerland
- 3Fondazione Don Carlo Gnocchi Onlus (IRCCS), Milan, Italy
- 4Developmental Imaging and Psychopathology Laboratory, University of Geneva School of Medicine, Geneva, Switzerland
- 5Department of Neurology—Fatebenefratelli Hospital, Rome, Italy
- 6University Consortium for Adaptive Disorders and Head Pain—UCADH, Pavia, Italy
Chronic migraine (CM) is often complicated by medication overuse headache (MOH) and psychiatric comorbidities that may influence the clinical outcome. This study aimed to investigate the relationship between psychiatric comorbidities and the effect of transcranial direct current stimulation (tDCS) in patients with CM with or without MOH. We recruited 16 consecutive CM patients who had an unsatisfactory response to at least three pharmacological preventive therapies. They were treated with anodal right-prefrontal and cathodal occipital tDCS (intensity: 2 mA, time: 20 min) three times per week for 4 weeks. All patients underwent a psychopathological assessment before and after treatment, and five of them were diagnosed with bipolar disorder (BD). After treatment, all the patients showed a significant decrease of severe and overall headache days per month. Despite having a higher migraine burden at baseline, patients with CM and BD showed a significantly greater reduction of severe headaches and psychiatric symptoms. Overall, tDCS seems to be effective in the treatment of CM patients with a poor response to different classes of pharmacological therapies, whereas BD status positively influences the response of migraineurs to tDCS.
Introduction
Chronic migraine (CM) is a severe condition characterized by more than 15 headache days per month, 8 of which presenting migraine features, lasting at least 3 months (1). It represents the most common type of headache referring to specialized headache centers. CM is often irresponsive to medical treatment, especially when complicated by medication overuse headache (MOH) (ICHD-III 8.2) (2). Treatment adherence is quite poor and heavily affected by side effects (3, 4). Therefore, there is an increasing interest in therapeutic alternatives with fewer side effects, including non-pharmaceutical treatments. The poor outcome of preventive treatments is mostly attributable to CM multifactorial pathophysiology, in which electrophysiological alterations, psychiatric comorbidities, and environmental factors concur to reverberate pain (2).
Non-invasive neurostimulation through transcranial direct current stimulation (tDCS) has recently been suggested as a potentially useful tool for migraine prevention (5). In a simplified view, when tDCS is applied with two electrodes, one serving as the anode and the other as a cathode, positive stimulation increases neuronal excitability, whereas negative stimulation decreases it in most of the settings (6). TDCS may provide a safe and effective treatment, given the absence of severe side effects, generally occurring during the stimulation and rarely outlasting it (7). Moreover, tDCS may influence several areas of the brain according to the chosen montage (8), modifying targeted mechanisms of migraine (9) and therefore allowing a tailored intervention on each patient's pathophysiological profile.
Psychiatric comorbidities are frequently associated with CM, with or without MOH. Depression and anxiety are particularly common among these patients (10), as well as bipolar disorder (BD), both in its full-blown presentations and in the milder subthreshold forms of the bipolar spectrum, such as cyclothymia or type A behavioral pattern (11, 12).
The presence of such comorbidities has a detrimental impact on treatment outcome (13), being associated with a worse clinical condition, development of MOH, and reduced efficacy of pharmacological preventive therapies (14). TDCS has been applied to treat psychiatric diseases (15); therefore, it is reasonable to expect that specific montages might be effective in the treatment of both migraine and psychiatric comorbidities.
Cortical disexcitability in migraine, likely caused by a disruption of thalamocortical circuits (16), seems to be a relevant target for treatment. Indeed, in episodic migraine (EM) patients, a pattern of hyperresponsivity to sensory stimulation is observed during the interictal period. Hyperresponsivity has two main features: an average low-amplitude initial response followed by a lack of physiological habituation (i.e., a potentiation) of subsequent responses to repeated stimuli. By contrast, in the same interictal phase, CM patients show a normal level of preactivation and a normal habituation pattern, indistinguishable from that observed in EM patients during migraine attacks (16). This led to the hypothesis that CM is a permanent ictal-like state or “never-ending attack” (17), independently of the presence of the attack itself. Medication overuse may probably have a facilitating effect on this enduring altered excitability state, sticking patients in a preictal state, when normal preactivation is combined with lacking habituation (18). Taking together these results, we considered CM, either with or without MOH, as a “hyperexcitability disorder.” The fact that hyperexcitability is a common feature of the visual cortex in CM, with or without MOH, as well as in EM during the attack, has been highlighted by recent studies on flash-sound multisensorial perception (19, 20) and has been found to be greater in MOH patients with triptan abuse (18, 19).
The theory of cortical disexcitability in migraine provided a model for the development of different neuromodulation protocols. However, at present, there is no standard tDCS protocol for the treatment of migraine, as tDCS studies have yielded contrasting results. This inconsistency may be partially explained by the heterogeneity of the montages applied (21–26). Another relevant factor is the variability in the plastic and metaplastic effects of neuromodulation in migraine patients. Several studies showed that metaplastic changes in motor, auditory, or visual cortex induced by neurostimulation in healthy subjects (27–30) can be also found in migraine patients (31, 32), but they are influenced by the phase of the migrainous cycle in which neurostimulation is delivered (32). This additional source of variability may have affected the outcome of therapeutic trials with neuromodulation in the recent years.
Besides the occipital cortex, other brain areas have been also targeted by neurostimulation treatments for migraine. In a seminal repetitive transcranial magnetic stimulation trial in patients with CM, Brighina et al. found that excitatory stimulation of the left dorsolateral prefrontal cortex (lDLPFC) was associated with a better outcome compared to placebo (33), paving the road for subsequent noninvasive interventions. Unfortunately, the subsequent trials yielded contrasting results when lDLPFC was targeted (34, 35).
In recent years, the role of the right dorsolateral prefrontal cortex (rDLPFC) dysfunction has been highlighted in CM patients with psychiatric comorbidities and MOH (36, 37). Moreover, anodal stimulation of the rDLFPC in a dual montage is recommended as non-invasive neuromodulation therapy in addiction-related craving, a condition that could be similar to that of CM patients with MOH who are withdrawing acute medication for migraine (38, 39).
Considering the role of the visual cortex in the physiopathology of migraine and of the rDLPFC in medication overuse and psychiatric comorbidities in CM patients, in the present study we decided to pair occipital cathodal stimulation with anodal stimulation on the rDLPFC. We designed a pilot study recruiting difficult-to-treat patients who failed more than three previous preventive lines of therapy and/or had a relapse in analgesic overuse, despite several withdrawal attempts. These patients are at higher risk of comorbidities, including psychiatric disorders, and show a higher rate of failure to any preventive therapy. Considering (2) the lack of previous studies using neuromodulation on these target patients and (3) the new montage used, we decided to use a proof-of-concept design with no sham stimulation to test tolerability and feasibility of such a protocol. Regarding the potential efficacy of the tDCS treatment, we evaluated the reduction of the migraine burden and medication overuse. A second objective was to differentiate the clinical responses according to the psychiatric comorbidity profile of each patient.
Materials and Methods
Subjects and Clinical Records
The study was conducted at the Headache Center of Policlinico Umberto I in Rome. We recruited all consecutive patients (aged 18–65 years) diagnosed with CM (ICHD-III), according to the ICHD-III, with or without MOH (ICHD-III 8.2). Inclusion criteria were as follows: failure of three or more preventive treatments and/or relapse of MOH despite three or more withdrawal attempts. Exclusion criteria were as follows: other major neurological diseases, familial or personal history of seizures, cardiac arrhythmia, implanted pacemaker or metallic hardware in the head or neck, or contraindication to receive tDCS. Migraine preventive treatment was allowed only if it was unmodified and ineffective for ≥4 months prior to the beginning of the stimulation. All the patients were naive to tDCS.
Patients were asked to fill a headache diary to record clinical headache data (including medication intake) during the 30-day-long baseline assessment (t0), the 30 days of tDCS treatment (t30), and the 30 days of follow-up period (t60). Patients' quality of life at t0 was assessed using the Migraine Disability Assessment (MIDAS) and Six-item Headache Impact Test (HIT-6) scale. Moreover, we collected data about the main risk factors for migraine chronification, as listed by May and Schulte (2). All patients were instructed on MOH risks, and acute medication therapy withdrawal was verbally recommended.
Psychiatric Assessment
Patients were recruited irrespectively of their psychiatric status and underwent a psychiatric interview by a trained psychiatrist before tDCS. Specifically, they were examined by means of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Axis I Disorders (SCID-I) (40), the Akiskal's Temps-A scale for affective temperaments (41), the Diagnostic Criteria for Psychosomatic Medicine (DCPR) (42), and the Young Mania Rating Scale (YMRS) (43). All scales were administered before and within 2 weeks after the treatment.
All subjects gave written informed consent. This study was approved by the Ethics Committee of Human Experimentation of Policlinico Umberto I University Hospital and conformed to the latest version of the Declaration of Helsinki.
Stimulation
TDCS was performed using a programmable DC brain stimulator (E.M.S., Bologna, Italy) with two rubber electrodes (5 × 5 cm) in sponges soaked with 3% saline. The anode was placed over the right dorsolateral prefrontal cortex (DLPFC) centered on F4 in the 10–20 electroencephalography system, and the cathode was positioned on the occipital cortex centered on Oz. During each session, a current of 2 mA was delivered for 20 min, with a fade-in/fade-out period of 20 s to decrease discomfort. TDCS was applied for 3 days per week for 4 weeks in the same hour of the day for each patient. In order to minimize variability, stimulation was applied during the morning and early afternoon hours (9 a.m. to 2 p.m.). The three stimulation sessions per week were scheduled individually with every patient and maintained stable throughout the treatment period.
Outcome Measures and Statistical Analysis
We assessed the feasibility and safety of our tDCS stimulation protocol measured as number of dropouts and number and severity of reported side effects. Regarding the potential efficacy of tDCS as preventive therapy, our primary endpoint was the reduction of total headache days. Secondary outcomes were the reduction of severe and moderate headache days, acute medication intake, and psychiatric symptoms changes, as measured by validated scales. As subanalysis, we compared primary and secondary outcome measures between relevant subgroups (e.g., BD vs. non-BD, anxious vs. non-anxious patients).
We used the Shapiro–Wilks test to assess the normality of the variables. Hence, we used parametric and non-parametric tests on the basis of variables distributions. Repeated-measures analysis of variance (ANOVA) was used to investigate the effect of tDCS both at group level and between subgroups. Time points (t0, t30, t60) represent the within-group effect (time) and subgroups effect between groups (group) (e.g., patients with BD vs. patients without BD). For subgroups analysis, post hoc comparison and Bonferroni correction were used. Variables measured only twice (at baseline and posttreatment, as tests for psychiatric assessment) were compared using Student t test for paired sample or Wilcoxon signed ranks test according to their distribution. Spearman test was used for the correlation analysis as variables were normally distributed. Results were considered significant at p < 0.05 and were given by mean ± standard deviation. Statistical calculations were carried out using R statistical package (version 3.5.3).
Results
Sixteen CM patients (four males; mean age = 53.88 ± 6.93 years) were recruited. All the patients were diagnosed with migraine without aura. Ten of 16 had MOH. The most overused drugs were non-steroidal anti-inflammatory drugs (38%), followed by combination drugs (19%), whereas only one patient overused triptans alone. At the moment of the recruitment, only one patient was under pharmacological prophylactic treatment for migraine having the other patients spontaneously discontinued for reported lack of efficacy; the number and classes of previous attempted prophylactic treatments are listed in Table 1. Eleven of 16 had already attempted a preventive therapy with onabotulinumtoxin without benefit. Risk factors for migraine chronification are listed in order of prevalence in Table 2.
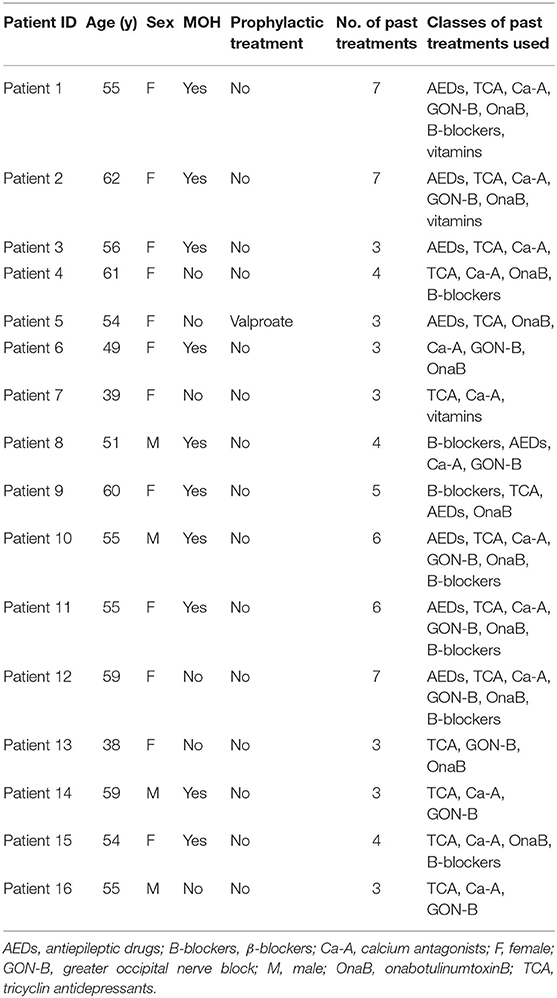
Table 1. Demographic and clinical information of the population of the study.
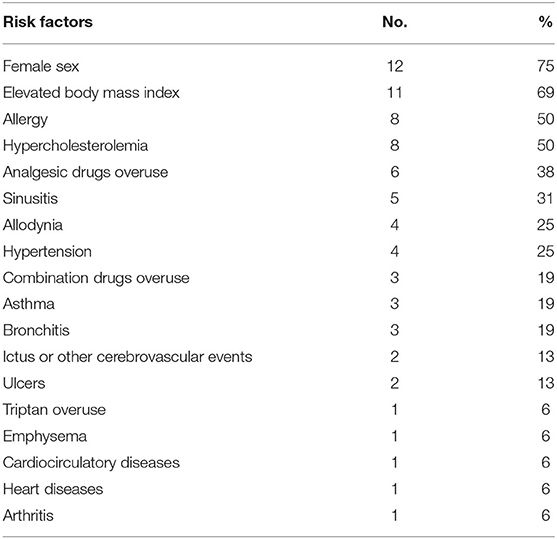
Table 2. Prevalence of factors associated with an increased risk for migraine chronification expressed as the number of patients and percentage of the sample.
At baseline (t0), mean headache days were 20.50 ± 5.13. Severe headache days were 6.13 ± 5.95. MIDAS and HIT-6 mean scores were 81.38 ± 73.88 and 63.31 ± 4.55, respectively, indicating the highest level of disability associated with headache.
The SCID-I identified five patients affected by BD, whereas Akiskal's Temps-A scale for affective temperaments revealed six more patients within the bipolar spectrum, presenting cyclothymic or hyperthymic temperament. Overall, 11 (69%) of 16 patients displayed clinical or subthreshold presentations within the bipolar spectrum. SCID-I results showed that eight patients (50%) met the criteria for an anxiety disorder, two (12.5%) for a depressive disorder, and five (31%) for a somatoform disorder. Only four patients (25%) did not meet the criteria for any psychiatric comorbidity. Using DCPR, nine patients (56%) were found positive for type A, a behavioral pattern characterized by a strong competitivity, aggression, and hypervigilance.
Safety and Efficacy of tDCS as Preventive Treatment
None of the 16 patients dropped out during the treatment period. No relevant adverse events were reported. In total, seven of 16 patients (44%) showed an improvement after tDCS. Repeated-measures ANOVA on total headache days showed a main effect of time: F(2, 30) = 7.03, p = 0.012. Post hoc analysis revealed a significant reduction of total headache days from 20.5 ± 6.89 at baseline to 16.87 ± 7.8 at t30 (t = 2.45, p = 0.027) and to 14.81 ± 9.13 at t60 (−27% compared to baseline, t = 2.96, p = 0.01) (Figure 1). A main effect of time [F(2, 26) = 7.07, p = 0.012] was also found for acute medication intake, which decreased from 18.64 ± 10.76 at baseline to 13.57 ± 12.24 at t30 (t = 2.51, p = 0.026) and to 11.71 ± 12.36 at t60 (−35% compared to baseline, t = 0.007, p = 0.02) (Figure 1A). Seven of 10 patients recovered from MOH. The reduction of severe headache days from 6.13 ± 5.95 at baseline to 4.56 ± 5.88 at t60 [−26%, main effect of time: F(2, 30) = 2.57, p = 0.36] was not significant, whereas moderate headache attacks decreased [main effect of time: F(2, 28) = 5.46, p = 0.04] from 8.87 ± 8.85 at baseline to 5.8 ± 7.55 at t30 (t = 2.39, p = 0.03) and to 5.13 ± 7.70 at t60 (t = 2.48, p = 0.027 compared to baseline) (Figure 1). Two patients complained a worsening of migraine after the stimulation.
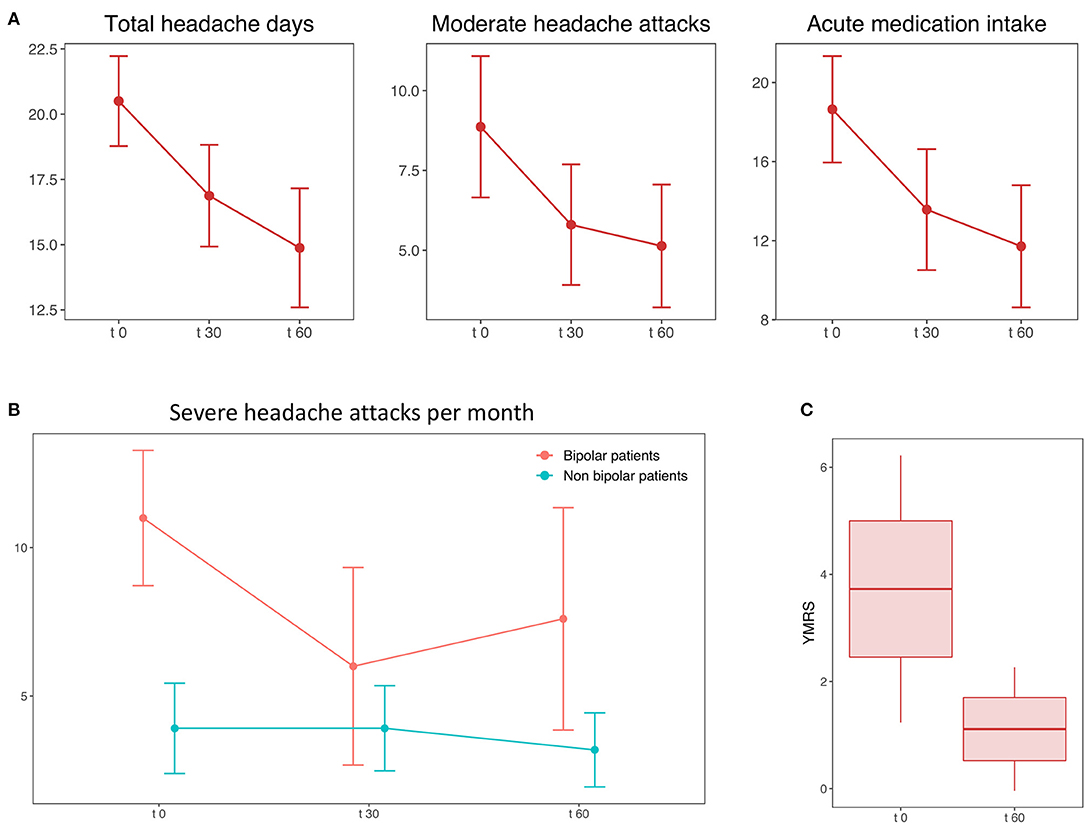
Figure 1. (A) The figure shows the mean and standard error of the number of total headache days (left plot), moderate attacks (central plot), and acute medication intake per month (right plot) at the baseline (t0), during the treatment (t30), and the follow-up period (t60). (B) Mean and standard error of the number of severe headache attacks at baseline (t0), during the treatment (t30), and the follow-up period (t60) in patients with (red line) and without (green line) bipolar disorder. (C) Significant decrease of Young Mania Rating Scale (YMRS) score before and after the treatment. The boxplot shows the mean, standard error and 90% CI of the score.
Subgroups Analysis
Among all the psychiatric comorbidities observed, only the presence of clinical or subclinical forms of BD seemed to influence the outcome of the treatment. A repeated-measures ANOVA on the number of severe headache attacks found a significant interaction of time and group (patients with and without BD) [F(2, 28) = 5.53, p = 0.036] (Figure 2). In details, patients with comorbid BD had a higher number of severe headache days/month at baseline (11.16 ± 4.68 vs. 3.1 ± 4.51; t = 2.59, p = 0.02), but showed a better response to tDCS compared to patients without BD (−3.4 ± 4.03 at t30 vs. −0.73 ± 3.03; −36% vs. −19%) with a significant reduction of severe headache days after 1 month of treatment (t0 vs. t60: t = 4.08, p = 0.01). No other significant result was found comparing the other subgroups.
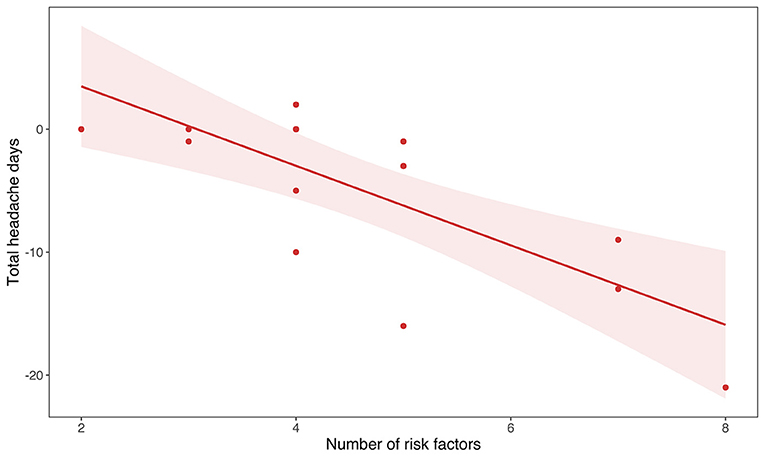
Figure 2. The graph shows the correlation between the total number of risk factors in each subject as listed in Table 1 and the reduction of the total number of headache days before and after the treatment (R = −0.7, p = 0.002).
After 1 month of tDCS, bipolar manic symptoms measured by YMRS in patients within the bipolar spectrum decreased from 4.55 ± 4.24 to 1.11 ± 1.76 (t = 2.97, p = 0.017) (Figure 1C). The number of risk factors for chronicity did not differ between patients with BD (t = 1.06, p = 0.3) and within the bipolar spectrum (t = 5.9, p = 0.557) and those who were not. The number of risk factors for migraine chronification was positively correlated with the reduction of total headache days (Spearman ρ = −0.7, p = 0.002) (Figure 1B). Allodynia had no impact on migraine at baseline (Spearman ρ = 0.36, p = 0.166) and the clinical response to tDCS (Spearman ρ = 0.32, p = 0.22).
Discussion
In this proof-of-concept study, we demonstrated the feasibility and safety of a tDCS protocol based on the combination of cathodal stimulation over the visual cortex and anodal stimulation of the rDLPFC for migraine treatment. Moreover, we found that this protocol was effective as preventive therapy in difficult-to-treat CM, reducing migraine burden and medication intake. As CM is characterized by cortical hypersensitivity and an ictal-like habituation pattern (16), especially in the visual cortex (44, 45), we applied an inhibitory stimulation on the occiput to reduce the hyperexcitable state of the visual cortex. Moreover, inhibitory stimulation of the visual cortex was found effective in modifying the nociception at the brainstem level (46).
We decided to pair occipital cathodal stimulation with anodal stimulation of the rDLPFC. The choice of targeting the rDLPFC was based on its role in medication overuse and psychiatric diseases often comorbid with migraine, such as BD and depression (37, 47). Previous studies have shown that the reversion of DLPFC hypoactivity in BD is achieved after either pharmacological or psychotherapeutic successful treatment of BD symptoms (48). Moreover, rDLPFC dysfunction seems to be directly related to the intensity of psychiatric symptoms in migraine (37). Additionally, anodal tDCS on rDLPFC is effective in treating craving in drug abusers (15). Chronic migraineurs with MOH, which are the majority in our sample, have cerebral abnormalities in common with patients suffering from substance addiction (36, 38). This can also explain the reduction in analgesic use observed in our patients after tDCS.
To the best of our knowledge, this is the first study aiming to investigate the relationship between psychiatric comorbidities and the effect of tDCS treatment in CM patients. In our sample, we found a 69% prevalence of patients within the bipolar spectrum. According to the present literature, BD prevalence in migraineurs is approximately 19%, whereas in the general population the prevalence of BD is 2–4% (49). Other studies found a higher prevalence of migraine among patients with milder BD type II (34.8–70%) compared to those affected by the severe BD type I (19%) (12, 50).
We showed that patients with CM and BD had a heavier migraine burden at baseline. On the other hand, patients with CM and BD showed a better response to tDCS. The reduction of the migraine burden was paralleled by a more general improvement in psychiatric symptoms in patients within the bipolar spectrum, as measured by YMRS. A possible explanation is that, in addition to the direct effect on visual cortex hyperexcitability, our stimulation might have influenced also other brain areas involved in both CM and BD. Apart from local activity, tDCS is also able to durably induce long-range modulation of brain cortex excitability (8), having complex and pleiotropic effects on brain activity. In particular, occipital stimulation has been previously used to target the brainstem and the cerebellum (46).
The prefrontal–thalamic–cerebellar circuit is involved in cognitive, sleep, and social impairment in BD (51, 52). Accordingly, prefrontal–occipital tDCS stimulation improved sleep quality, visuospatial memory, and executive functions in euthymic BD patients (53, 54). Interestingly, cerebellum is also involved in the processing of nociceptive stimuli (55–57). Therefore, incidental modulation of cerebellar activity by means of occipital tDCS might account for the parallel improvement in BD and migraine symptoms in our sample.
Finally, we highlighted a correlation between the number of risk factors and the clinical benefit of the patients. One possible explanation is that some risk factors (e.g., asthma, arterial hypertension, and elevated body mass index), or risk related to the pharmacological therapy of comorbidities, might have prevented patients from receiving some lines of treatment (e.g., β-blockers or valproate) or have caused a precocious discontinuation. For this reason, in patients with a high number of risk factors, tDCS could be effectively used because of the absence of side effects or drug interactions.
However, some limitations of this study are worth to be mentioned. First, a major limitation is that a placebo effect cannot be ruled out, and the current results must be confirmed by a randomized sham-controlled trial. Estimating the placebo effect in clinical trials for migraine treatment is not straightforward, as it may vary according to the complexity of the procedure (58). Our study tested the effect of a new montage on a pool of difficult-to-treat patients (on average 4.4 lines of treatment per patients, with 11 patients who had previously attempted a preventive therapy with onabotulinumtoxin without any benefit) reporting good tolerability and no dropouts. Moreover, 44% of the patients experienced an improvement, and seven patients reverted from MOH, encouraging the use of these preliminary data to calculate the appropriate sample size for a randomized controlled trial.
The lack of previous studies using this type of montage prevented us from predetermining our own sample size on a statistical basis, which is a second limitation to the current pilot study. The sample size was simply limited by the availability of patients matching the inclusion criteria for the study in our headache center. However, the final sample size is in line with the recommendations for pilot studies (59). To minimize the bias in evaluating the efficacy of the treatment, we planned a primary outcome—i.e., testing prefrontal–occipital tDCS efficacy on the basis of total and severe days of headache—and a limited number of exploratory analyses, to keep the number of statistical tests to a minimum. Moreover, we applied Bonferroni correction, which is the most conservative correction in post hoc comparisons, to minimize the type I error (60).
In third place, the lack of a complete neurophysiological evaluation prevented us from directly assessing the effect of tDCS at the neural level. The inclusion of neurophysiological parameters in future studies would allow to evaluate the efficacy of the tDCS treatment and to compare different tDCS protocols on more solid bases.
Indeed, plastic changes induced by neurostimulation can vary according to the phases of the migraine cycle (32). Therefore, there is the possibility that the stimulation may act differently depending on the frequency of the migraine attacks (i.e., CM vs. EM patients). In order to minimize the effect of such variability, we only included patients with CM in our sample, with an average number of 20.5 days of headache days per month.
Moreover, without a direct neurophysiological read-out, we could only speculate about the brain networks affected by the stimulation. In particular, we could not directly assess the neural effects of stimulating the right rather than the left DLPFC, or the lack of lateralization in the case of the occipital cortex. Indeed, the use of a midline cathodal stimulation over the visual cortex does not allow disentangling between a lateralized effect on the activation of one hemisphere and the presence of interhemispheric interactions. However, while an impairment of the interhemispheric inhibition at the level of the sensory–motor cortex has been recently described in migraine, this seems to be a feature of migraine with aura, which was not present in our sample (61).
Conclusions
In our proof-of-concept study, anodal rDLPFC and cathodal occipital tDCS was found to be safe and effective in reducing both the number of total headache days and acute medication intake per month in difficult-to-treat CM patients. Moreover, we found that, in spite of a worse clinical status at baseline, patients with comorbid BD had a better response to tDCS with respect to both headache and psychiatric symptoms. Although in most of clinical trials on migraine prevention using central non-invasive neurostimulation patients affected by psychiatric comorbidities are excluded, in this proof-of-concept study we aimed to investigate the impact of psychiatric comorbidities on the outcome of tDCS treatment in CM patients. If on one hand, this choice makes it harder to assess whether the stimulation acts directly on migraine pathophysiology or not, on the other hand it is a pragmatic approach to be implemented in difficult-to-treat CM patients, in which psychiatric comorbidities are often present.
Data Availability Statement
The datasets presented in this article are not readily available because access is subject to approval by the Policlinico Umberto I Ethics Committee. Requests to access the datasets should be directed to Z2l1bGlvbWFzdHJpYUBtc24uY29t.
Ethics Statement
The studies involving human participants were reviewed and approved by Policlinico Umberto I Ethics Commitee. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
GM, AV, VM, RD, and VD contributed to the design of the study. GM, AC, VM, CP, and SB collected the data. GM, AV, and VM analyzed the data and wrote the first draft of the paper. All the authors revised the paper for intellectual content.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Headache Classification Committee of the International Headache Society (IHS). The International classification of headache disorders, 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
2. May A, Schulte LH. Chronic migraine: risk factors, mechanisms and treatment. Nat Rev Neurol. (2016) 12:455–64. doi: 10.1038/nrneurol.2016.93
3. Hepp Z, Dodick DW, Varon SF, Chia J, Matthew N, Gillard P, et al. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: a retrospective claims analysis. Cephalalgia. (2017) 37:470–85. doi: 10.1177/0333102416678382
4. Evers S, Áfra J, Frese A, Goadsby PJ, Linde M, May A, et al. EFNS guideline on the drug treatment of migraine - revised report of an EFNS task force. Europ J Neurol. (2009) 16:968–81. doi: 10.1111/j.1468-1331.2009.02748.x
5. Shirahige L, Melo L, Nogueira F, Rocha S, Monte-Silva K. Efficacy of noninvasive brain stimulation on pain control in migraine patients: a systematic review and meta-analysis. Headache. (2016) 56:1565–96. doi: 10.1111/head.12981
6. Rahman A, Reato D, Arlotti M, Gasca F, Datta A, Parra LC, et al. Cellular effects of acute direct current stimulation: somatic and synaptic terminal effects. J Physiol. (2013) 591:2563–78. doi: 10.1113/jphysiol.2012.247171
7. Rizzerio BG, Fregni F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int J Neuropsychopharmacol. (2011) 14:1133–45. doi: 10.1017/S1461145710001690
8. DaSilva AF, Truong DQ, DosSantos MF, Toback RL, Datta A, Bikson M. State-of-art neuroanatomical target analysis of high-definition and conventional TDCS montages used for migraine and pain control. Front Neuroanat. (2015) 9:89. doi: 10.3389/fnana.2015.00089
9. Coppola G, Bracaglia M, Di Lenola D, Iacovelli E, Di Lorenzo C, Serrao M, et al. Lateral inhibition in the somatosensory cortex during and between migraine without aura attacks: correlations with thalamocortical activity and clinical features. Cephalalgia. (2015) 36:568–78. doi: 10.1177/0333102415610873
10. Lampl C, Thomas H, Tassorelli C, Katsarava Z, Laínez JM, Lantéri M, et al. Headache, Depression and anxiety: associations in the eurolight project. J Headache Pain. (2016) 17:59. doi: 10.1186/s10194-016-0649-2
11. Oedegaard KJ, Neckelmann D, Fasmer OB. Type a behaviour differentiates bipolar ii from unipolar depressed patients. J Affect Disord. (2006) 90:7–13. doi: 10.1016/j.jad.2005.10.005
12. Fasmer OB. The prevalence of migraine in patients with bipolar and unipolar affective disorders. Cephalalgia. (2001) 21:894–99. doi: 10.1046/j.1468-2982.2001.00279.x
13. Bergman-Bock S. Associations between migraine and the most common psychiatric co-morbidities. Headache. (2017) 58:346–53. doi: 10.1111/head.13146
15. Lefaucheur J-P, Antal A, Ayache SS, Benninger DH, Brunelin J, et al. Evidence-Based guidelines on the therapeutic use of transcranial direct current stimulation (TDCS). Clin Neurophys. (2017) 128:56–92. doi: 10.1016/j.clinph.2016.10.087
16. De TM, Ambrosini A, Brighina F, Coppola G, Perrotta A, Pierelli F, et al. Altered processing of sensory stimuli in patients with migraine. Nat Rev Neurol. (2014) 10:144–55. doi: 10.1038/nrneurol.2014.14
17. Schoenen J. Is chronic migraine a never-ending migraine attack? Pain. (2011) 152:239–40. doi: 10.1016/j.pain.2010.12.002
18. Coppola G, Currà A, Di Lorenzo C, Parisi V, Gorini M, Sava SL, et al. Abnormal cortical responses to somatosensory stimulation in medication-overuse headache. BMC Neurol. (2010) 10:126. doi: 10.1186/1471-2377-10-126
19. Maccora S, Bolognini N, Cosentino G, Baschi R, Vallar G, Fierro B, Brighina F. Multisensorial perception in chronic migraine the role of medication overuse. J Pain. (2020) 21:919–29. doi: 10.1016/j.jpain.2019.12.005
20. Brighina F, Bolognini N, Cosentino G, Maccora S, Paladino P, Baschi R, et al. Visual cortex hyperexcitability in migraine in response to sound-induced flash illusions. Neurology. (2015) 84:2057–61. doi: 10.1212/WNL.0000000000001584
21. Viganò A, D'Elia TS, Sava SL, Auvé M, De Pasqua V, Colosimo A, et al. Transcranial Direct Current Stimulation (TDCS) of the visual cortex: a proof-of-concept study based on interictal electrophysiological abnormalities in migraine. J Headache Pain. (2013) 14:23. doi: 10.1186/1129-2377-14-23
22. Rocha S, Melo L, Boudoux C, Foerster Á, Araújo D, Monte-Silva K. Transcranial direct current stimulation in the prophylactic treatment of migraine based on interictal visual cortex excitability abnormalities: a pilot randomized controlled trial. J Neurol Sci. (2015) 349:33–9. doi: 10.1016/j.jns.2014.12.018
23. DaSilva AF, Mendonca ME, Zaghi S, Lopes M, DosSantos MF, Spierings EL, et al. TDCS-induced analgesia and electrical fields in pain-related neural networks in chronic migraine. Headache. (2012) 52:1283–95. doi: 10.1111/j.1526-4610.2012.02141.x
24. Antal A, Kriener N, Lang N, Boros K, Paulus W. Cathodal transcranial direct current stimulation of the visual cortex in the prophylactic treatment of migraine. Cephalalgia. (2011) 31:820–8. doi: 10.1177/0333102411399349
25. Baschi R, Vecchio E, Sava SL, De Pasqua V, Schoenen J, Magis D. EHMTI-0217. neurophysiological study of tdcs effects in healthy volunteers. J Headache Pain. (2014) 15:E3. doi: 10.1186/1129-2377-15-s1-e3
26. Pinchuk D, Pinchuk O, Sirbiladze K, Shugar O. Clinical effectiveness of primary secondary headache treatment by transcranial direct current stimulation. Front Neurol. (2013) 4:25. doi: 10.3389/fneur.2013.00025
27. Bocci T, Caleo M, Tognazzi S, Francini N, Briscese L, Maffei L, et al. Evidence for metaplasticity in the human visual cortex. J Neural Transm. (2014) 121:221–31. doi: 10.1007/s00702-013-1104-z
28. D'amour JA, Froemke RC. Inhibitory and excitatory spike-timing-dependent plasticity in the auditory cortex. Neuron. (2015) 86:514–28. doi: 10.1016/j.neuron.2015.03.014
29. Froemke RC. Plasticity of cortical excitatory-inhibitory balance. Annu Rev Neurosci. (2015) 38:195–219. doi: 10.1146/annurev-neuro-071714-034002
30. Viganò A, Toscano M, Puledda F, Di Piero V. Treating Chronic Migraine with Neuromodulation: The Role of Neurophysiological Abnormalities and Maladaptive Plasticity. Front Pharm. (2019) 10:32. doi: 10.3389/fphar.2019.00032
31. Antal A, Lang N, Boros K, Nitsche M, Siebner HR, Paulus W. Homeostatic metaplasticity of the motor cortex is altered during headache-free intervals in migraine with aura. Cerebral Cortex. (2008) 18:2701–5. doi: 10.1093/cercor/bhn032
32. Cosentino G, Fierro B, Vigneri S, Talamanca S, Paladino P, Baschi R, et al. Cyclical changes of cortical excitability and metaplasticity in migraine: evidence from a repetitive transcranial magnetic stimulation study. Pain. (2014) 155:1070–78. doi: 10.1016/j.pain.2014.02.024
33. Brighina Filippo B, Piazza A, Vitello G, Aloisio A, Palermo A, Daniele O, et al. RTMS of the prefrontal cortex in the treatment of chronic migraine: a pilot study. J Neurol Sci. (2004) 227:67–71. doi: 10.1016/j.jns.2004.08.008
34. Conforto AB, Amaro E, Gonçalves AL, Mercante JPP, Guendler VZ, Ferreira JR, et al. Randomized, proof-of-principle clinical trial of active transcranial magnetic stimulation in chronic migraine. Cephalalgia. (2014) 34:464–72. doi: 10.1177/0333102413515340
35. Feng Y, Zhang B, Zhang J, Yin Y. Effects of non-invasive brain stimulation on headache intensity and frequency of headache attacks in patients with migraine: a systematic review and meta-analysis. Headache. (2019) 59:1436–47. doi: 10.1111/head.13645
36. Chen Z, Chen X, Liu M, Dong Z, Ma L, Yu S. Altered functional connectivity architecture of the brain in medication overuse headache using resting state FMRI. J Headache Pain. (2017) 18:25. doi: 10.1186/s10194-017-0735-0
37. Lirng J-F, Chen H-C, Fuh J-L, Liang J-F, Wang S-J. Increased myo-inositol level in dorsolateral prefrontal cortex in migraine patients with major depression. Cephalalgia. (2014) 35:702–9. doi: 10.1177/0333102414557048
38. Fumal A, Laureys S, Di Clemente L, Boly M, Bohotin V, Vandenheede M, et al. Orbitofrontal cortex involvement in chronic analgesic-overuse headache evolving from episodic migraine. Brain. (2006) 129:543–50. doi: 10.1093/brain/awh691
39. Schwedt TJ, Chong CD. Medication overuse headache: pathophysiological insights from structural and functional brain research, MRI. Headache. (2017) 57:1173–78. doi: 10.1111/head.13037
40. Gorgens KA. Structured clinical interview for DSM-IV (SCID-I/SCID-II). Encycl Clin Neuropsych. (2011) 1:2410–17. doi: 10.1007/978-0-387-79948-3_2011
41. Akiskal HS, Mendlowicz MV, Jean-Louis G, Rapaport MH, Kelsoe JR, Gillin JC, et al. TEMPS-A: validation of a short version of a self-rated instrument designed to measure variations in temperament. J Affect Disord. (2005) 85:45–52. doi: 10.1016/j.jad.2003.10.012
42. Porcelli P, Rafanelli C. Criteria for psychosomatic research (DCPR) in the medical setting. Curr Psych Rep. (2010) 12:246–54. doi: 10.1007/s11920-010-0104-z
43. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
44. Boulloche N, Denuelle M, Payoux P, Fabre N, Trotter Y, Geraud G. Photophobia in migraine: an interictal PET study of cortical hyperexcitability and its modulation by pain. J Neurol Neurosurg Psychiatry. (2010) 81:978–84. doi: 10.1136/jnnp.2009.190223
45. Chen W-T, Wang S-J, Fuh J-L, Lee Y-C, Hämäläinen MS, et al. visual cortex excitability and plasticity associated with remission from chronic to episodic migraine. Cephalalgia. (2012) 32:537–43. doi: 10.1177/0333102412443337
46. Sava SL, de Pasqua V, Magis D, Schoenen J. Effects of visual cortex activation on the nociceptive blink reflex in healthy subjects. PLoS ONE. (2014) 9:e100198. doi: 10.1371/journal.pone.0100198
47. Schneider MR, Klein CC, Weber W, Bitter SM, Elliott KB, Strakowski SM, et al. The effects of carbamazepine on prefrontal activation in manic youth with bipolar disorder. Psychiat Res Neuroimag. (2014) 223:268–70. doi: 10.1016/j.pscychresns.2014.04.011
48. Garrett AS, Miklowitz DJ, Howe ME, Singh MK, Acquaye TK, Hawkey CG, et al. Changes in brain activation following psychotherapy for youth with mood dysregulation at familial risk for bipolar disorder. Progr Neuro-Psychopharm Biol Psychiatry. (2015) 56:215–20. doi: 10.1016/j.pnpbp.2014.09.007
49. Kivilcim Y, Altintas M, Domac FM, Erzincan E, Gulec H. Screening for bipolar disorder among migraineurs: the impact of migraine-bipolar disorder comorbidity on disease characteristics. Neuropsych Dis Treatment. (2017) 13:631–41. doi: 10.2147/ndt.s121448
50. Ortiz A, Cervantes P, Zlotnik G, Van De Velde C, Slaney C, Garnham J, et al. Cross-Prevalence of migraine and bipolar disorder. Bipolar Disord. (2010) 12:397–403. doi: 10.1111/j.1399-5618.2010.00832.x
51. McKenna BS, Eyler LT. Overlapping prefrontal systems involved in cognitive and emotional processing in euthymic bipolar disorder and following sleep deprivation: a review of functional neuroimaging studies. Clin Psychol Rev. (2012) 32:650–63. doi: 10.1016/j.cpr.2012.07.003
52. Minichino A, Bersani FS, Trabucchi G, Albano G, Primavera M, Delle Chiaie ET, et al. The role of cerebellum in unipolar and bipolar depression: a review of the main neurobiological findings. Riv Psichiatr. (2014) 49:124–31. doi: 10.1708/1551.16907
53. Minichino A, Bersani FS, Spagnoli F, Corrado A, De Michele F, Calò WK, et al. Prefronto-cerebellar transcranial direct current stimulation improves sleep quality in euthymic bipolar patients: a brief report. Behav Neurol. (2014) 2014:1–3. doi: 10.1155/2014/876521
54. Bersani FS, Minichino A, Bernabei L, Spagnoli F, Vergnani L, Corrado A, et al. Prefronto-cerebellar transcranial direct current stimulation improves visuospatial memory, executive functions, and neurological soft signs in patients with euthymic bipolar disorder. Neuropsych Dis Treat. (2015) 11:2265. doi: 10.2147/ndt.s79108
55. Moulton Eric A, Schmahmann JD, Becerra L, Borsook D. The cerebellum and pain: passive integrator or active participator? Brain Res Rev. (2010) 65:14–27. doi: 10.1016/j.brainresrev.2010.05.005
56. Moulton A, Elman EI, Pendse G, Schmahmann J, Becerra L, Borsook D. Aversion-related circuitry in the cerebellum: responses to noxious heat and unpleasant images. J Neurosci. (2011) 31:3795–804. doi: 10.1523/jneurosci.6709-10.2011
57. Borsook D, Moulton EA, Tully S, Schmahmann JD, Becerra L. Human cerebellar responses to brush and heat stimuli in healthy and neuropathic pain subjects. Cerebellum. (2008) 7:252–72. doi: 10.1007/s12311-008-0011-6
58. Meyer AND, Payne VL, Meeks DW, Rao R, Singh H. Physicians' diagnostic accuracy, confidence, and resource requests: a vignette study. JAMA Internal Med. (2013) 173:1952–61. doi: 10.1001/jamainternmed.2013.10081
59. Kianifard F, Islam MZ. A guide to the design and analysis of small clinical studies. Pharm Statist. (2010) 10:363–68. doi: 10.1002/pst.477
60. Narum SR. Beyond bonferroni: less conservative analyses for conservation genetics. Conserv Genet. (2006) 7:783–87. doi: 10.1007/s10592-005-9056-y
Keywords: tDCS, migraine, bipolar disorder, cerebellar stimulation, occipital cortex stimulation, dorsolateral prefrontal cortex stimulation, migraine overuse headache
Citation: Mastria G, Viganò A, Corrado A, Mancini V, Pirillo C, Badini S, Petolicchio B, Toscano M, Altieri M, Delle Chiaie R and Di Piero V (2021) Chronic Migraine Preventive Treatment by Prefrontal–Occipital Transcranial Direct Current Stimulation (tDCS): A Proof-of-Concept Study on the Effect of Psychiatric Comorbidities. Front. Neurol. 12:654900. doi: 10.3389/fneur.2021.654900
Received: 17 January 2021; Accepted: 29 March 2021;
Published: 13 May 2021.
Edited by:
Massimiliano Valeriani, Bambino Gesù Children Hospital (IRCCS), ItalyReviewed by:
Filippo Brighina, University of Palermo, ItalyTommaso Bocci, University of Milan, Italy
Copyright © 2021 Mastria, Viganò, Corrado, Mancini, Pirillo, Badini, Petolicchio, Toscano, Altieri, Delle Chiaie and Di Piero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giulio Mastria, Z2l1bGlvbWFzdHJpYUBtc24uY29t; Alessandro Viganò, YXZpZ2Fub0Bkb25nbm9jY2hpLml0
†These authors have contributed equally to this work