 Manina M. Etter1
Manina M. Etter1 Markus Möhlenbruch2
Markus Möhlenbruch2 Charlotte S. Weyland2
Charlotte S. Weyland2 Carlos Pérez-García3Manuel Moreu3Francesco Capasso4
Carlos Pérez-García3Manuel Moreu3Francesco Capasso4 Nicola Limbucci4Omid Nikoubashman5
Nicola Limbucci4Omid Nikoubashman5 Martin Wiesmann5Kristine Blackham1Ioannis Tsogkas1
Martin Wiesmann5Kristine Blackham1Ioannis Tsogkas1 Peter Sporns1
Peter Sporns1 Johanna Maria Ospel1
Johanna Maria Ospel1 Alex Brehm1
Alex Brehm1 Marios-Nikos Psychogios1*
Marios-Nikos Psychogios1*- 1Department of Neuroradiology, Clinic for Radiology and Nuclear Medicine, University Hospital Basel, Basel, Switzerland
- 2Department of Neuroradiology, University Hospital Heidelberg, Heidelberg, Germany
- 3Department of Neuroradiology, Hospital Clínico San Carlos, Madrid, Spain
- 4Neurovascular Interventional Unit, Careggi University Hospital, Florence, Italy
- 5Department of Neuroradiology, University Hospital RWTH Aachen, Aachen, Germany
Background: The application of a new coating to the delivery wire of the Trevo retriever has the potential to improve its handling. We therefore report our initial experience with this new stent retriever for mechanical thrombectomy of large and medium vessel occlusions.
Methods: We pooled data of four high-volume European stroke centers over the time period from October 2020 to February 2021. Patients were included in our study if the Trevo NXT stent retriever was used as a first-line device. Primary endpoints were first-pass near-complete or complete reperfusion, defined as mTICI score of ≥2c. Secondary endpoints were final reperfusion, National Institutes of Health Stroke Scale (NIHSS) at 24 h and discharge, device malfunctions, complications during the procedure, and subjective ratings of the interventionalists regarding device functionality.
Results: Eighty patients (39 women, mean age 74 ± 14 years) were eligible for our study. Median NIHSS at admission was 15 (IQR, 8–19), and median Alberta Stroke Program Early CT Score at baseline was 9 (IQR, 8–10). In 74 (93%) patients a primary combined approach was used as first-line technique. First-pass near-complete reperfusion was achieved in 43 (54%) and first-pass complete reperfusion in 34 (43%) patients. Final near-complete reperfusion was achieved in 66 (83%) patients after a median of 1.5 (1–3) passes, while final successful reperfusion was observed in 96% of our cases. We observed no device malfunctions. Median NIHSS at discharge was 2 (IQR, 0–5), and 3 patients (4%) suffered a symptomatic intracranial hemorrhage.
Conclusions: Based on our initial data, we conclude that the Trevo NXT is an effective and safe tool for mechanical thrombectomy especially when used for combined approaches.
Introduction
Mechanical thrombectomy is considered the standard of care for ischemic strokes caused by large vessel occlusions (LVO) (1). The main techniques can be generally divided into three major categories: (I) use of a stent retriever (SR) and subsequent withdrawal of the device with or without flow arrest by a balloon-guide catheter (BGC); (II) direct aspiration technique using a large-bore aspiration-catheter (ADAPT), placed at the face of the clot; and (III) primary combined approaches (PCA), where both an SR and an aspiration-catheter are used intracranially with additional extracranial aspiration through the guide catheter (2–4).
Among the different techniques for mechanical thrombectomy, various SRs are used in combined approaches. The Trevo ProVue SR is a well-established mechanical thrombectomy device as several studies have confirmed its efficacy in endovascular stroke therapy. In the Multicenter Randomized CLinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands (MR CLEAN), Trevo was the most frequently used SR (5). In the Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention With Trevo (DAWN) randomized trial, which showed thrombectomy to be superior compared to medical management alone, Trevo was the only SR used in the interventional arm (6). The device was also assessed in the Trevo retriever Registry, a prospective post-market study which documented reperfusion success after mechanical thrombectomy and functional outcomes at 90 days. Reperfusion success was defined by a modified thrombolysis in cerebral infarction (mTICI) score ≥2b, which was reached in 93% of the study population. Furthermore, functional independence at 90 days (defined as a modified Rankin Scale ≤2) was documented in 55% of patients (7).
In this retrospective study, we assessed the new-generation Trevo SR (Trevo NXT) for endovascular therapy of ischemic stroke due to large or medium vessel occlusions. We focused on its efficacy and peri-interventional safety.
Materials and Methods
Study Design and Patient Population
We pooled data of four high-volume European stroke centers over the time period from October 2020 to February 2021. Patients were included in our study if the Trevo NXT ProVue SR (Stryker Neurovascular, Kalamazoo, MI, USA) was used as the first-line device. No other inclusion or exclusion criteria were applied.
The National Institutes of Health Stroke Scale (NIHSS) was obtained at baseline, 24 h post procedure and at discharge by a certified stroke neurologist. All angiographies were rated by the treating interventionalist using the mTICI (8) scale. Non-contrast computed tomography (CT) or magnetic resonance imaging (MRI) was regularly performed within 24 h after treatment or immediately in symptomatic patients. Symptomatic intracranial hemorrhage (sICH) was defined as an intracranial hemorrhage that was associated with clinical deterioration, as documented by an increase of ≥4 points on the NIHSS. In intubated patients, sICH was defined by the European Cooperative Acute Stroke Study-2 (ECASS-2) criteria as any parenchymal hematoma grade I or larger (9).
As the company claims that the new Trevo NXT can be delivered and retracted through the microcatheter or the aspiration-catheter more easily compared to earlier Trevo generations, we surveyed the involved interventionalists on their subjective experience with the new device. The following questions were used: (a) How easy was advancing the SR through the microcatheter? (b) Could target placement of the SR be achieved? (c) How easy was retrieving the SR into the aspiration-catheter/BGC? and (d) In PCA, could a stable wedge position be achieved, or was the SR accidentally withdrawn into the aspiration-catheter? For questions (a) and (c) we used an evenly distributed ordinal five-point scale (ranging from 1 = very easy, 2 = easy, over 3 = neutral, to 4 = hard, and 5 = very hard), while (b) and (d) were yes/no questions. For this analysis, only cases in which a PCA was used as the first-line approach were included.
The primary endpoint was first-pass complete or near-complete reperfusion, defined as an mTICI ≥2c. Secondary endpoints were final reperfusion, NIHSS at 24 h and discharge, occurrence of sICH, device malfunctions, complications during the procedure, and the subjective ratings of the interventionalists.
Endovascular Procedure
Procedures were performed under conscious sedation, local anesthesia, or general anesthesia. Vital findings were monitored by anesthesiologists or stroke neurologists in all patients during the procedures. All procedures were done using a femoral artery access. The treating physician was free to choose the first-line technique, but in most cases the Stent retriever Assisted Vacuum Extraction (SAVE) technique was used as described elsewhere (4).
Device Characteristics
The Trevo NXT ProVue retriever is a further development of its predecessor, the Trevo XP ProVue retriever. While the stent itself was not changed and still offers full radiopaque visibility, the delivery wire received a new hydrophilic coated polymer jacket which enables a smoother and easier delivery and improved retraction into the aspiration-catheter. It is delivered through a 0.021-inch microcatheter (the 3 × 25 mm retriever can also be delivered through a 0.017-inch microcatheter). The device is available in working lengths from 25 to 35 mm and diameters from 3 to 6 mm. The wire length was increased to 200 cm, which improves its compatibility with tri-axial setups.
Statistical Methods
Statistical analysis was performed using GraphPad Prism 9 (GraphPad Software, San Diego, CA, USA, https://www.graphpad.com/, 2021). Parametric variables are stated as mean ± standard deviation (SD). Non-parametric or ordinary variables are presented as median and interquartile range (IQR). No interference statistics were performed.
Results
Out of 97 received data sheets, 80 patients were enrolled into this study. Ten of the 97 patients were excluded due to ADAPT being the first-line therapy, while in seven patients an SR other than the Trevo NXT ProVue was used for the first maneuver. All baseline characteristics are depicted in Table 1. Mean age was 74 ± 14 years, and 39 patients (49%) were female. The median NIHSS at admission was 15 (IQR, 8–19). Occlusion sites were internal carotid artery terminus (“ICA-T”) in 14 (18%), M1-segment in 38 (47%), M2-segment in 22 (28%), basilar artery in 4 (5%), P2-segment in 1 (1%), and vertebral artery in 1 (1%) patient. Median Alberta Stroke Program Early CT score (ASPECTS) on initial imaging was 9 (IQR 8–10). The majority of patients was treated either with a PCA (47/80) or PCA with balloon-guide (27/80), while the rest was treated with SR only (1/80) or with SR plus BGC (5/80). Most of the procedures were performed under conscious sedation or local anesthesia (67 patients). General anesthesia was used in the remaining 13 patients (16%).
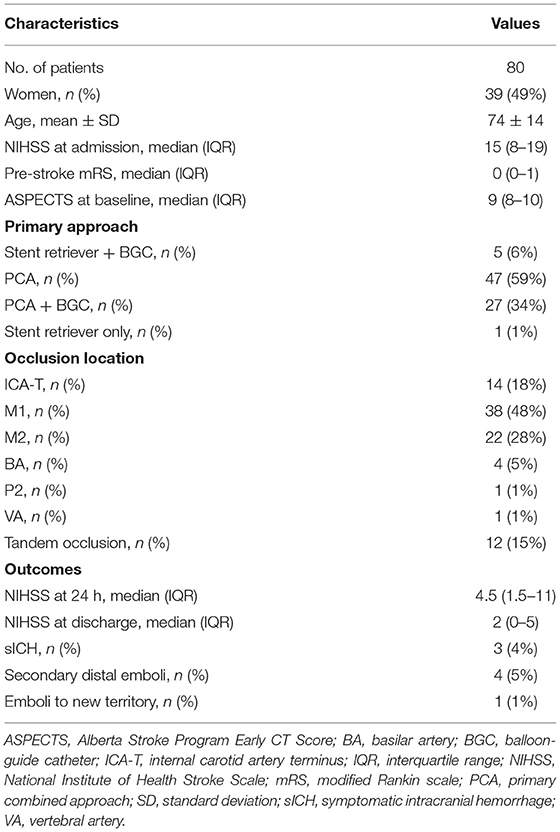
Table 1. Baseline characteristics of the patients.
First-pass complete or near-complete reperfusion (mTICI ≥2c) was achieved in 43 (54%) with complete reperfusion (mTICI 3) in 34 (43%) patients. The final complete or near-complete reperfusion (mTICI ≥2c) was observed in 66 (83%) and complete reperfusion (mTICI 3) in 45 (56%) patients after a median of 1.5 passes (IQR, 1–3). The rate of successful reperfusion (mTICI ≥2b) was 64% after one pass and 96% at the end of the procedure (Table 2). The overall median time from groin puncture to reperfusion was 39 min (IQR, 23–58.5). We documented 1 (1%) embolus in new territory (initial M1 to A1), and in 4 cases (5%) distal emboli were observed. In 3 patients (4%) an sICH was observed. In 2 cases the intracranial hemorrhage (ICH) was observed immediately on the post-mechanical thrombectomy scan in the angio-suite, while in the third case no immediate scan after MT was performed. It was observed on the first follow-up CT 4.5 h after the intervention. One ICH was mainly an extensive subarachnoid hemorrhage (SAH) in the basal cisterns and hemispheric sulci with small parenchymal hematoma in the left basal ganglia (affecting putamen) and insula; the other 2 ICHs were mainly parenchymal hematomas within the infarct area (both media territory left). In the case with the SAH no intravenous lysis was given, while in the other 2 cases it was given prior to the intervention. None of the sICHs were rated to be related to the intervention. In all cases the handling of the SR was continuously smooth. The median NIHSS 24 h post procedure was 4.5 (IQR, 1.5–11) and 2 (IQR, 0–5) at discharge.
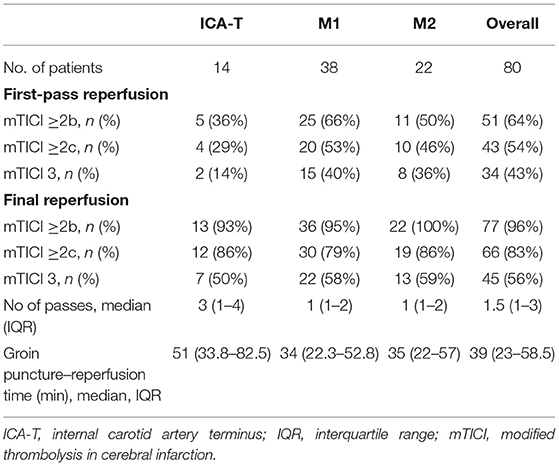
Table 2. Angiographic results stratified by occluded vessel and overall vessels.
A total of 158 passes were performed with the Trevo NXT; no device malfunctions were observed. Four complications were reported: 2 SAHs and 2 vasospasms (which resolved after application of nimodipine). Both vasospasms were observed in the segment where the SR was placed [one in the M2-segment of the right middle cerebral artery (MCA) and one in the M2-segment of the left MCA]. In both cases the Trevo NXT 4 ×35 mm SR was used.
A subgroup analysis of the angiographic results after stratification by occlusion site indicated higher first-pass complete or near-complete reperfusion results in the M1- and M2-segments compared to the ICA-T (53%/46% vs. 29%). Furthermore, the number of passes (median 3 for the ICA-T and 1 for the M1/M2) and the groin to reperfusion time (median 51 min for ICA-T vs. 34/35 min for M1/M2) were higher for ICA-T occlusions (see Table 2 for detailed results). The incremental improvement of the mTICI result declined from pass to pass (Table 3).
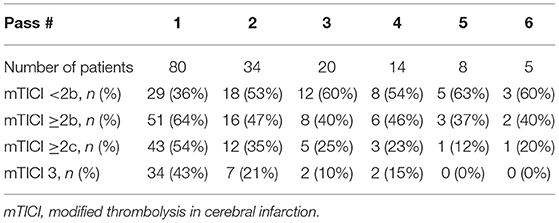
Table 3. Per pass reperfusion results.
Advancing the SR was rated “very easy” in 39%, “easy” in 47%, and “neutral” in 14% of our cases, while none of the procedures was rated as “hard.” Target placement of the SR was achieved in all cases. Withdrawing the SR toward the aspiration-catheter to reach the wedge position or retrieve it toward the BGC was rated as “very easy” in 51%, “easy” in 42%, and “neutral” in 7%. The wedge position could be sustained in 91% of the procedures.
Discussion
Early and complete arterial recanalization is the most important factor in achieving favorable clinical outcome after ischemic stroke due to LVO (10, 11). Mechanical thrombectomy is the standard of care for LVO and gaining momentum for medium vessel occlusions as well, as multiple randomized trials have demonstrated improved patient outcomes in the interventional arm (1, 12). In cases of tortuous proximal vessels or distal target lesions, pushing the SR through the microcatheter and retrieving the SR within the aspiration-catheter can be challenging. The design of the new Trevo NXT is supposed to help in these situations, due to the hydrophilic coating of the pusher wire. In this retrospective multicenter study, we evaluated the initial results with this new device. One of our main findings was that the rate of first-pass complete or near-complete reperfusion (mTICI ≥2c) was achieved in 54% of cases, which compares favorably to previously published data of the predecessor retriever (Table 4) (13, 14). Final mTICI ≥2c was achieved in 83%, and final complete reperfusion (mTICI 3) in 56% of the cases. First-pass mTICI ≥2c was achieved more often than in the Trevo 2000 Registry, where the rate was 28% (13). Regarding final reperfusion rates, mTICI 3 was documented in 56% of the Trevo 2000 Registry cases, which is identical to the final mTICI 3 rates of our study (56%) (7). Data of other newer-generation SRs were mostly comparable to our results: Ribo et al. reported 63% mTICI ≥2b and 47% mTICI ≥2c first-pass reperfusion using the Neva thrombectomy device, although with a small sample size of only 30 patients (16). Slightly inferior results with 52% first-pass mTICI ≥2b and 40% first-pass mTICI ≥2c were reported in the prospective ARISE II study, where the EmboTrap SR was assessed using a larger sample size (n = 227) (15). Results of the Aperio Hybrid SR were recently published, with 52% mTICI ≥2b and 31% mTICI ≥2c first-pass reperfusion in a sample of 48 patients, which are slightly inferior to our reperfusion rates (22). The Tigertriever, which can be radially adjusted, was recently evaluated in the multicentric Tiger Trial (n = 160), yielding similar reperfusion results with first-pass successful reperfusion rates of 58% and final near-complete reperfusion rates of 72% (18). Technical approaches varied within all these studies, limiting the degree to which reperfusion results can be compared. For example, while in this study the primarily used technique was a combined technique (93% of the cases), this approach was used only in a minority of cases in the Trevo 2000 Registry (7).
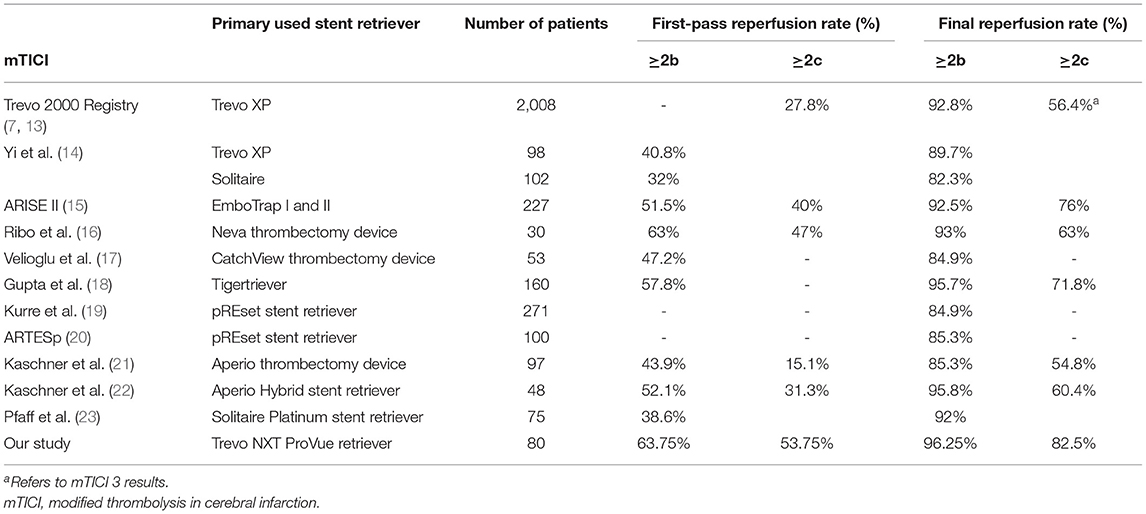
Table 4. Overview of recent studies evaluating stent retrievers.
Regarding the technical aspects using the Trevo NXT as first-line device, advancing the SR within the microcatheter was described as “easy” in the majority of cases, and target placement of the SR was achieved in all cases. Even in cases of curved proximal vessels or tortuous siphon we were able to push the 4 mm Trevo NXT through a 0.021-inch microcatheter without failing to reach the target position. While treating distal occlusions with the 3 mm Trevo NXT, pushing the device through a 0.017-inch microcatheter was feasible. In our subjective opinion, pushing the new 3 mm device through a 0.017-inch microcatheter was easier compared to previous Trevo generations, although we did not compare the 2 devices in this study. In terms of retrieving the SR into the aspiration-catheter or the BGC, we also received positive feedback from the interventionalists. These findings are consistent with the development of a hydrophilic coated polymer jacket, which was designed to enable a smoother and easier delivery and an improved retraction into the aspiration-catheter. Our experience is that even in tortuous proximal vessels it is much easier to push a rather rigid large-bore aspiration-catheter toward the face of the clot over the new SR after removal of the microcatheter. For physicians using the Solumbra technique (full retrieval of the SR within the aspiration-catheter) as their primary approach, the hydrophilic jacket provides an even smoother retrieval experience compared to older SRs. Nevertheless, we would not recommend this technique to be used as first-line approach, based on the higher occurrence of clot fragmentation and distal emboli (24). A potential disadvantage of the new coating is encountered when pulling the SR toward the tip of the aspiration-catheter for the SAVE maneuver (25): With conventional SRs, there is a point where a wedge position is reached and cannot be lost even with significant pulling power on the SR wire, due to entrapment of the clot between the SR and the aspiration-catheter. Using the new device, we noticed that continuous pull after reaching the wedge position can lead to unintentional withdrawal of the SR within the aspiration-catheter (9% of our cases) resulting in an unintended Solumbra maneuver.
Concerning safety, the Trevo NXT retriever can be regarded as safe. Complication rates were comparable to those of the literature (1). Both cases of SAH were unnoticed during the procedure and could not be clearly attributed to the SR (26).
The main limitation of our study is the retrospective design. Patients were included after initial stroke incident and treatment with mechanical thrombectomy. In addition, angiographic results and complications were rated by the treating physician and not by a core lab, which can lead to heterogenous judgments and potentially influence results. Finally, the Trevo NXT was chosen as the first-line device by the treating physician and not allotted in a randomized setup.
Conclusion
Based on our initial data, we conclude that the Trevo NXT is an effective and safe tool for mechanical thrombectomy especially when using combined approaches.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
AB, PS, IT, KB, and JO designed the data collection sheets and performed the analysis. MMö, CW, CP-G, MMo, FC, NL, ON, and MW contributed the data and helped to evaluate the data. ME and M-NP wrote the manuscript. All authors reviewed the manuscript critically, gave final approval of the submitted version, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Goyal M, Menon BK, Van Zwam WH, Dippel DWJ, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
2. Turk AS, Frei D, Fiorella D, Mocco J, Baxter B, Siddiqui A, et al. ADAPT FAST study: a direct aspiration first pass technique for acute stroke thrombectomy. J NeuroInterv Surg. (2018) 10:I4–I7. doi: 10.1136/neurintsurg-2014-011125.rep
3. Lapergue B, Blanc R, Gory B, Labreuche J, Duhamel A, Marnat G, et al. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER randomized clinical trial. JAMA. (2017) 318:443–52. doi: 10.1001/jama.2017.9644
4. Maus V, Behme D, Kabbasch C, Borggrefe J, Tsogkas I, Nikoubashman O, et al. Maximizing first-pass complete reperfusion with SAVE. Clin Neuroradiol. (2018) 28:327–38. doi: 10.1007/s00062-017-0566-z
5. Berkhemer OA, Fransen PSS, Beumer D„ van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. (2014) 372:11–20. doi: 10.1056/NEJMoa1411587
6. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, Yavagal DR, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. (2018) 378:11–21. doi: 10.1056/NEJMoa1706442
7. Binning MJ, Bartolini B, Baxter B, Budzik R, English J, Gupta R, et al. Trevo 2000: results of a large real-world registry for stent retriever for acute ischemic stroke. J Am Heart Assoc. (2018) 7:e010867. doi: 10.1161/JAHA.118.010867
8. Goyal M, Fargen KM, Turk AS, Mocco J, Liebeskind DS, Frei D, et al. 2C or not 2C: defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J Neurointerv Surg. (2014) 6:83–6. doi: 10.1136/neurintsurg-2013-010665
9. Hacke W, Kaste M, Fieschi C, Von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet. (1998) 352:1245–51. doi: 10.1016/S0140-6736(98)08020-9
10. Abbasi M, Liu Y, Fitzgerald S, Mereuta OM, Arturo Larco JL, Rizvi A, et al. Systematic review and meta-analysis of current rates of first pass effect by thrombectomy technique and associations with clinical outcomes. J Neurointerv Surg. (2021) 13:212–6. doi: 10.1136/neurintsurg-2020-016869
11. Nikoubashman O, Dekeyzer S, Riabikin A, Keulers A, Reich A, Mpotsaris A, et al. True first-pass effect: first-pass complete reperfusion improves clinical outcome in thrombectomy stroke patients. Stroke. (2019) 50:2140–6. doi: 10.1161/STROKEAHA.119.025148
12. Menon BK, Hill MD, Davalos A, Roos Y, Campbell BCV, Dippel DWJ, et al. Efficacy of endovascular thrombectomy in patients with M2 segment middle cerebral artery occlusions: meta-analysis of data from the HERMES Collaboration. J Neurointerv Surg. (2019) 11:1065–9. doi: 10.1136/heartjnl-2014-307109.258
13. Jadhav AP, Desai SM, Budzik RF, Gupta R, Baxter B, English JD, et al. First pass effect in patients with large vessel occlusion strokes undergoing neurothrombectomy: insights from the Trevo Retriever Registry. J NeuroInterv Surg. (2021) 13:619–22. doi: 10.1136/neurintsurg-2020-016952
14. Yi HJ, Lee DH, Kim SU. Effectiveness of Trevo stent retriever in acute ischemic stroke: comparison with Solitaire stent. Medicine. (2018) 97:e10747. doi: 10.1097/MD.0000000000010747
15. Zaidat O), Bozorgchami H, Ribó M, Saver JL, Mattle HP, Chapot R, et al. Primary results of the multicenter ARISE II Study (Analysis of Revascularization in Ischemic Stroke With EmboTrap). Stroke. (2018) 49:1107–15. doi: 10.1161/STROKEAHA.117.020125
16. Ribo M, Requena M, Macho J, Zamarro J, Machi P, Hernandez D, et al. Mechanical thrombectomy with a novel stent retriever with multifunctional zones: initial clinical experience with the NeVa™ thrombectomy device. J Neuroradiol. (2020) 47:301–5. doi: 10.1016/j.neurad.2019.03.007
17. Velioglu M, Onal Y, Agackiran A, Dogan Ak P, Karakas HM. Initial experience with the CatchView thrombectomy device for acute ischemic stroke. J NeuroInterv Surg. (2020). doi: 10.1136/neurintsurg-2020-016784. [Epub ahead of print].
18. Gupta R, Saver JL, Levy EI, Zaidat OO, Yavagal DR, Liebeskind DS, et al. A new class of radially adjustable stentrievers for acute ischemic stroke: primary results of the multicenter Tiger Trial. Stroke. (2021) 52:1534–44. doi: 10.1161/STROKEAHA.121.034436
19. Kurre W, Aguilar-Pérez M, Schmid E, Sperber W, Bäzner H, Henkes H. Clinical experience with the pREset stent retriever for the treatment of acute ischemic stroke–a review of 271 consecutive cases. Neuroradiology. (2014) 56:397–403. doi: 10.1007/s00234-014-1346-y
20. Prothmann S, Schwaiger BJ, Gersing AS, Reith W, Niederstadt T, Felber A, et al. Acute recanalization of thrombo-embolic ischemic stroke with pREset (ARTESp): the impact of occlusion time on clinical outcome of directly admitted and transferred patients. J Neurointerv Surg. (2017) 9:817–22. doi: 10.1136/neurintsurg-2016-012556
21. Kaschner MG, Weiss D, Rubbert C, Lee JI, Gliem M, Jander S, et al. One-year single-center experience with the Aperio thrombectomy device in large vessel occlusion in the anterior circulation: safety, efficacy, clinical outcome. Neurol Sci. (2019) 40:1443–51. doi: 10.1007/s10072-019-03861-z
22. Kaschner M, Lichtenstein T, Weiss D, Turowski B, Goertz L, Kluner C, et al. The new fully radiopaque aperio hybrid stent retriever: efficient and safe? An early multicenter experience. World Neurosurg. (2020) 141:e278–88. doi: 10.1016/j.wneu.2020.05.104
23. Pfaff J, Rohde S, Engelhorn T, Doerfler A, Bendszus M, Möhlenbruch MA. Mechanical thrombectomy using the new solitaire™ platinum stent-retriever: reperfusion results, complication rates and early neurological outcome. Clin Neuroradiol. (2019) 29:311–9. doi: 10.1007/s00062-017-0657-x
24. McTaggart RA, Tung EL, Yaghi S, Cutting SM, Hemendinger M, Gale HI, et al. Continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE): a technique which improves outcomes. J NeuroInterv Surg. (2017) 9:1154–9. doi: 10.1136/neurintsurg-2016-012838
25. Maus V, Henkel S, Riabikin A, Riedel C, Behme D, Tsogkas I, et al. The SAVE technique: large-scale experience for treatment of intracranial large vessel occlusions. Clin Neuroradiol. (2019) 29:669–76. doi: 10.1007/s00062-018-0702-4
26. Keulers A, Nikoubashman O, Mpotsaris A, Wilson SD, Wiesmann M. Preventing vessel perforations in endovascular thrombectomy: feasibility and safety of passing the clot with a microcatheter without microwire: the wireless microcatheter technique. J Neurointerv Surg. (2019) 11:653–8. doi: 10.1136/neurintsurg-2018-014267
Keywords: ischemic stroke, mechanical thrombectomy, stent retriever, primary combined approaches, medium vessel occlusion, large vessel occlusion
Citation: Etter MM, Möhlenbruch M, Weyland CS, Pérez-García C, Moreu M, Capasso F, Limbucci N, Nikoubashman O, Wiesmann M, Blackham K, Tsogkas I, Sporns P, Ospel JM, Brehm A and Psychogios M-N (2021) Initial Experience With the Trevo NXT Stent Retriever. Front. Neurol. 12:704329. doi: 10.3389/fneur.2021.704329
Received: 02 May 2021; Accepted: 11 June 2021;
Published: 16 July 2021.
Edited by:
Aristeidis H. Katsanos, McMaster University, CanadaReviewed by:
Michalis Mantatzis, Democritus University of Thrace, GreeceChristoph Johannes Maurer, Augsburg University Hospital, Germany
Copyright © 2021 Etter, Möhlenbruch, Weyland, Pérez-García, Moreu, Capasso, Limbucci, Nikoubashman, Wiesmann, Blackham, Tsogkas, Sporns, Ospel, Brehm and Psychogios. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marios-Nikos Psychogios, bWFyaW9zLnBzeWNob2dpb3NAdXNiLmNo