 Geoffroy Hautecloque1*
Geoffroy Hautecloque1* Christian Kempf2Camélia Stan1Marie-Hélène Arentz-Dugay1Francis Vuillemet1Guido Ahle1
Christian Kempf2Camélia Stan1Marie-Hélène Arentz-Dugay1Francis Vuillemet1Guido Ahle1 François Sellal1,3
François Sellal1,3 Martin Martinot4
Martin Martinot4- 1Department of Neurology, Hôpitaux Civils de Colmar, Colmar, France
- 2Clinical Research Department, Hôpitaux Civils de Colmar, Colmar, France
- 3Inserm U-1118, Strasbourg University, Strasbourg, France
- 4Department of Infectious Diseases, Hôpitaux Civils de Colmar, Colmar, France
Introduction: Thromboembolic events, including ischemic stroke, are major complications of coronavirus disease 2019 (COVID-19). The clinical characteristics of COVID-19-related stroke are not clearly defined, and few controlled studies assessed the underlying mechanisms of cerebrovascular complications of COVID-19. This single-center retrospective observational study compared stroke characteristics between patients with and without COVID-19.
Methods: This study included all patients hospitalized between March 1, 2020, and April 30, 2020, in Colmar Hospital for ischemic stroke as confirmed by imaging. The characteristics of patients with laboratory-confirmed severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection by real-time reverse transcriptase polymerase chain reaction or serology were compared with those without SARS-CoV-2 infection.
Result: Among 772 patients, nine COVID-19 patients were compared with 50 patients without COVID-19. The following inflammatory and procoagulant marker levels were significantly higher in the COVID-19 group than those in the control group: C-reactive protein, 57.3 ± 43.4 vs. 15.0 ± 30.6 mg/L, p < 0.001; fibrinogen, 5.89 ± 1.75 vs. 4.03 ± 1.26 g/L, p < 0.001; and D-dimer, 4,833.9 ± 6,549.4 vs. 1,028.6 ± 942.6 ng/ml, p < 0.001. The rates of multifocal cerebral territory involvement (4 vs. 7, p = 0.05), microvascular involvement (4 vs. 6, p = 0.04), and thrombophilia (4 vs. 4, p = 0.014) were significantly higher in the COVID-19 group than in the control group, whereas no significant intergroup differences were found in the stroke mechanisms, i.e., cardio-embolic, atherosclerotic, small vessel disease, and cryptogenic.
Conclusion: COVID-19-related stroke is characterized by hypercoagulability and hyperinflammation that may favor strokes via microvascular circulation abnormalities, microthrombus formation, and multifocal lesions.
Introduction
Coronavirus disease 2019 (COVID-19) is a polymorph disease caused by the novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) that emerged in December 2019 in China and rapidly spread worldwide. COVID-19 primarily affects the respiratory tract, with clinical presentation ranging from paucisymptomatic upper respiratory tract infection to systemic acute respiratory syndrome (1). Thromboembolic events have emerged as major manifestations of COVID-19, occurring in 7.7–30.0% of patients (2, 3), and ischemic stroke is a prominent thromboembolic complication of COVID-19, with an incidence ranging from 1.1 to 5% (4–6) among hospitalized patients with COVID-19. Although poorly understood, multiple factors, including disseminated intravascular coagulation, hypercoagulability, thrombophilia with anticardiolipin or anti-β2GP1 antibodies, cardiac injury, and arrhythmia, have been proposed in the etiology of stroke in patients with COVID-19 (7–9).
Colmar hospital is a 1,000-bed facility, and the main hospital of center Alsace GHT11 has a unique stroke unit for its territory of 410,000 inhabitants. In March 2020, Alsace in Northeastern France was hit by a major outbreak of COVID-19, and Hôpital Civil de Colmar was one of the most affected hospitals by the pandemic. In this single-center retrospective study, we assessed risk factors for ischemic stroke, including transient ischemic stroke, in patients with COVID-19 and elucidated the underlying mechanisms by comparing the characteristics of patients with laboratory-confirmed COVID-19 who experienced stroke with those of patients hospitalized for stroke without COVID-19 during the same period in our hospital.
Materials and Methods
Inclusion and Exclusion Criteria
The study included all patients hospitalized between March 1, 2020, and April 30, 2020, in Hôpital Civil de Colmar and had acute ischemic stroke or transient ischemic attack (TIA) upon admission or during hospitalization. Acute ischemic stroke has been defined as acute neurological dysfunction caused by an ischemic injury confirmed by the presence of cytotoxic edema on brain magnetic resonance imaging (MRI) (increased diffusion-weighted imaging signal and reduction of apparent diffusion coefficient). T2/fluid-attenuated inversion recovery (FLAIR), time-of-flight (TOF), and susceptibility-weighted imaging (SWI) sequences had also been performed to rule out differential diagnoses and to search for arterial occlusion when visualizable. When MRI could not be realized owing to the presence of a pacemaker, ischemic stroke was confirmed by the presence of a low density on computed tomography (CT). TIA was defined as a transient episode of neurological dysfunction caused by focal brain or retinal ischemia, without acute infarction (10). The COVID-19 group included patients with positive RT-PCR within 48 h of admission. The control group included patients hospitalized for ischemic stroke or TIA without COVID-19, i.e., negative for reverse transcriptase polymerase chain reaction (RT-PCR) or for serology performed during hospitalization. Patients who were hospitalized for stroke and were positive for SARS-CoV-2 by nasopharyngeal swab or sputum test 48 h after admission were excluded from the study, because they were suspected of contracting the infection during hospitalization, and those admitted with clinical signs of COVID-19 without confirmation by real-time RT-PCR or serology (Figure 1) were also excluded.
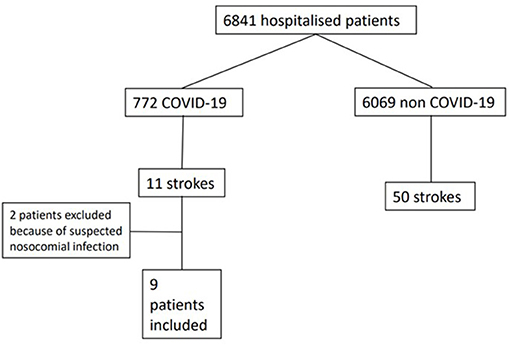
Figure 1. Flowchart.
Stroke Classification
In the present study, the causes of stroke were categorized according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification (11) and the embolic stroke of undetermined source criteria (12). Ischemic stroke due to atherosclerotic disease was defined as ≥50% narrowing in a large artery due to an atheroma plaque or intracranial stenosis of an artery perfusing the ischemic infarct territory. Involvement of a large artery was defined as the thrombotic occlusion in vertebral artery, basilar artery, first segment of posterior cerebral artery carotid artery, first and second segments of middle cerebral artery, or first portion of anterior cerebral artery. Stroke due to arteriogenic emboli (aortic arch atherosclerotic plaques or non-stenotic cerebral artery plaques with ulceration) were also considered as atherosclerotic causes of ischemic stroke. Stroke due to small vessel disease was defined as a small subcortical infarct (≤ 2 cm on diffusion-weighted imaging sequence or ≤ 1.5 cm on CT) in patients with cardiovascular risk factors for small vessel disease. Cardio-embolic infarct was defined based on the presence of a cardio-embolic source, such as atrial fibrillation or atrial dysrhythmia and stasis, patent foramen ovale with atrial septal aneurysm in patients aged <60 years, with no other obvious cause, or left ventricular dysfunction. Strokes associated with myocardial infarct/takotsubo cardiomyopathy/myocarditis were also considered to arise from a cardio-embolic source. Other etiologies included alternative mechanisms such as dissection or procoagulant state such as hereditary thrombophilia (activated protein C deficiency). Strokes without an overt etiology were classified as cryptogenic.
Data Collection
The following data were collected from the electronic medical records of patients: (1) demographic characteristics (age and sex); (2) comorbidities/high-risk conditions (history of hypertension, dyslipidemia, diabetes, obesity and high body mass index, smoking, atrial fibrillation, obstructive sleep apnea, peripheral artery disease, supra-aortic trunk stenosis, cardiopathy, stroke, and inflammatory disease); (3) stroke characteristics (TIA or stroke, National Institutes of Health Stroke Scale [NIHSS] score, large-artery occlusion, multi-territorial location, microvascular lesion [ <5 mm in size], time between the first COVID-19 symptoms and stroke, and stroke etiology); (4) laboratory data (C-reactive protein, coagulation parameters [D-dimer, fibrinogen, lupus anticoagulant, anticardiolipin antibody, and anti-β2 glycoprotein-1 antibody]); and (5) severity of COVID-19 infection (mild, moderate, or severe) (13).
Statistical Analysis
The patient baseline characteristics of the overall cohort and the COVID-19 and control groups were analyzed. Continuous variables were summarized as means with standard deviation (SD) and compared using Student's t-test or Wilcoxon's rank-sum test when the hypothesis of homoscedasticity was not satisfied. Categorical data were presented with numbers of missing values and absolute and relative counts and compared using the chi-squared test or Fisher's exact test when conditions were not satisfied for the chi-squared test. Given the retrospective, descriptive nature of the study, test results were given as an indication. No corrections for multiplicity were performed. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
The study was approved by the Comité d'Ethique des Facultés et Hôpitaux de Médecine, Odontologie et Pharmacie of the University Hospital of Strasbourg (approval no. CE-2020-32).
Results
Among a total of 6,841 patients hospitalized between March 1, 2020, and April 30, 2020, in Hôpital Civil de Colmar, 772 patients have been identified with SARS-CoV-2 infection, of whom 11 patients had a stroke. Two patients whose COVID-19 symptoms emerged more than 48 h (3 and 19 days) after hospitalization for stroke were excluded from the study. In total, nine patients (1.16%) were included, i.e., eight with ischemic stroke and one with TIA (Table 1). During the same period, among 6,069 patients without past or concomitant history of COVID-19 hospitalization, 43 patients were admitted for stroke and seven for TIA. In the control group, no clinical symptoms of COVID-19 have been observed, and RT-PCR was performed in 17 (34%) patients and serology in nine (18%). The stroke diagnosis was based on MRI in 60 of the patients (98.4%), whereas stroke was diagnosed based on CT in one patient (1.6%) with a pacemaker. All patients had intracranial and extracranial vascular imaging and cardiac evaluation including ECG, in-house continuous cardiac telemetry for at least 24 h, and transthoracic echocardiography. Young patients (age, <60 years) without obvious causes were screened for thrombophilia. Transesophageal ultrasound was performed in patients suspected of having a patent foramen ovale.
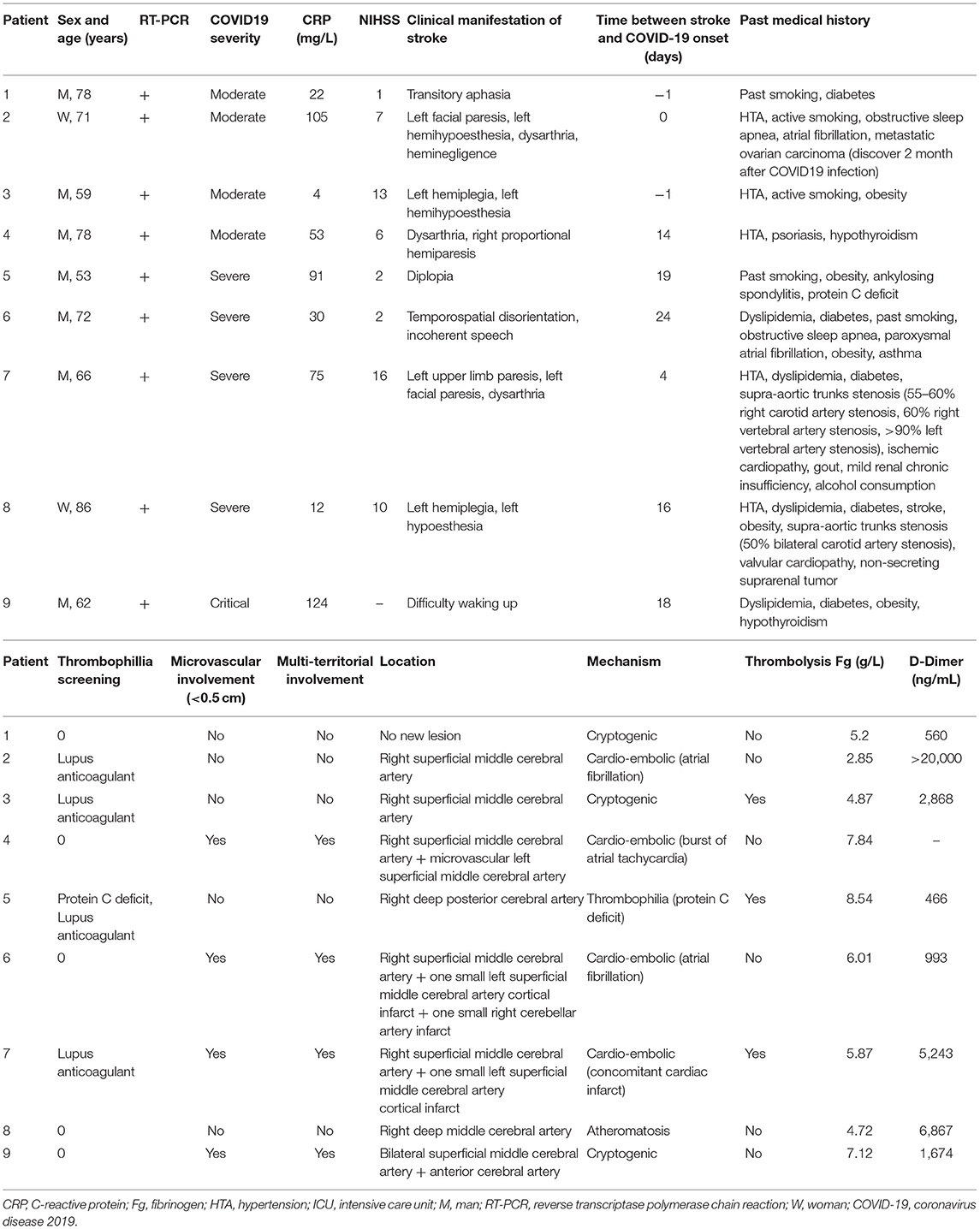
Table 1. Demographic, clinical, biological, and radiological data and mechanism of the nine COVID-19 patients.
The median ages were 69.4 ± 10.5 and 70.6 ± 13.2 years in the COVID-19 and control groups, respectively. Male patients comprised 77.8 and 70% of the COVID-19 and control groups, respectively. The percentages of patients with specific high-risk conditions are presented in Table 2. Only one of the nine patients with COVID-19 was admitted to the intensive care unit (ICU). The mean time interval between the first COVID-19 symptoms and the first stroke symptoms was 10.3 ± 9.8 days. TIAs occurred in one patient (11.1%) in the COVID-19 group and six patients (12.0%) in the control group (p > 0.999; Table 2).
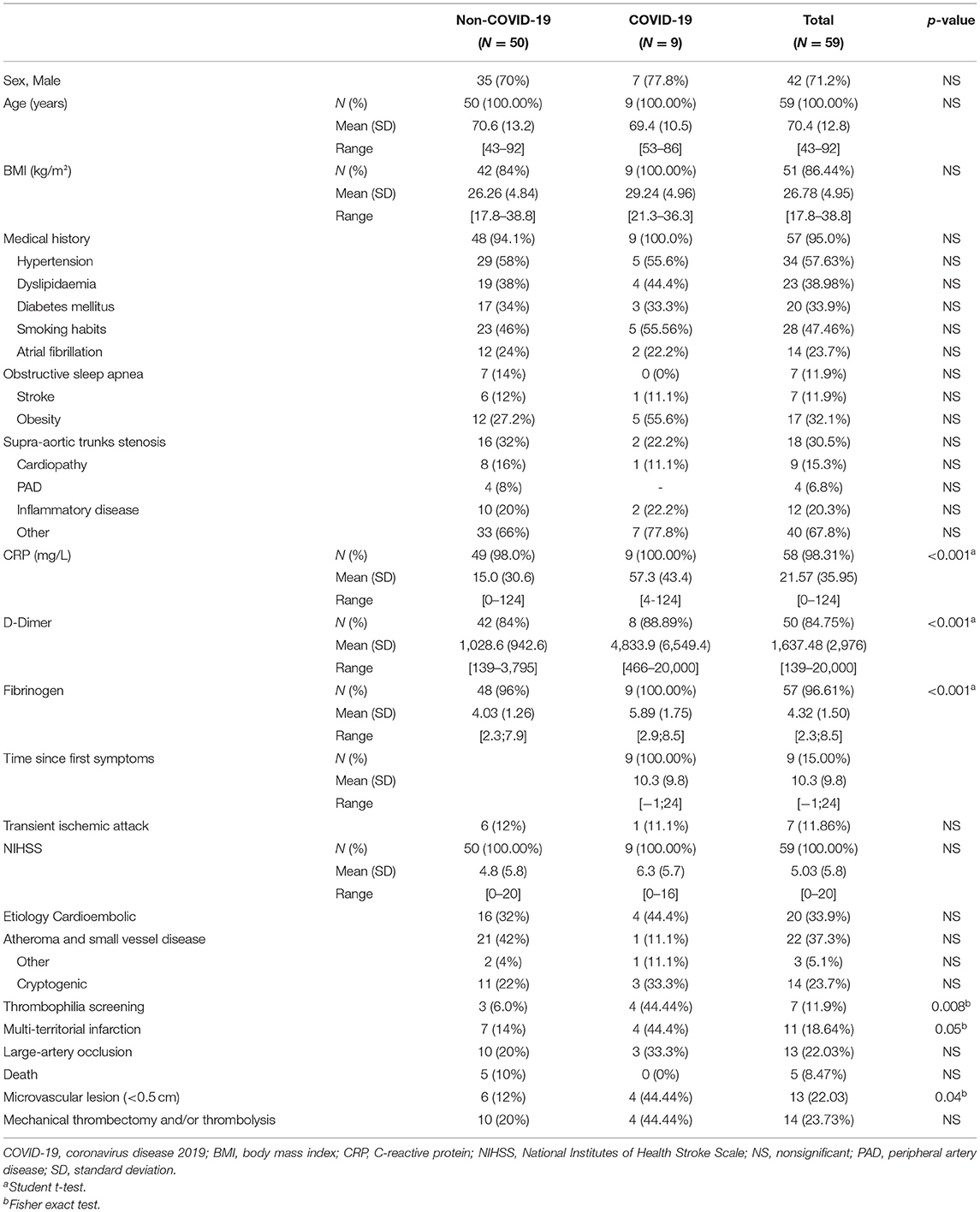
Table 2. Demographic, clinical, biological, and radiological data and mechanism in COVID-19 and control group.
The levels of laboratory markers for inflammation and thrombosis at the time of stroke were higher in the COVID-19 group compared with the control group (C-reactive protein, 57.3 ± 43.4 vs. 15.0 ± 30.6 mg/L, p < 0.001; fibrinogen, 5.89 ± 1.75 vs. 4.03 ± 1.26 g/L, p < 0.001; and D-dimer, 4,833.9 ± 6,549.4 vs. 1,028.6 ± 942.6 ng/ml, p < 0.001). The frequency of patients with positive thrombophilia parameters was higher in the COVID-19 group than in the control group (4/9 [44.4%] vs. 3/50 [6%]; p = 0.008). All seven patients were positive for lupus anticoagulant.
No clinical signs have been observed suspicious of a venous thromboembolic event among our COVID-19 patients.
The causes of stroke were not significantly different between the COVID-19 and control groups. Cardio-embolic factors were a stroke cause in four (44.4%) patients in the COVID-19 group and 16 (32.0%) patients in the control group (p = 0.47). Although not statistically significant, atherosclerosis and small vessel disease were less frequent causes of stroke in the COVID-19 group (1/9 [11.1%]) than in the control group (21/50 [42.0%]) (p = 0.13). Cryptogenic stroke was diagnosed in three (33.3%) patients in the COVID-19 group and 11 patients (22%) in the control group (p = 0.43). In the COVID-19 group, the only other etiology was found in a patient with a history of thrombophilia who was diagnosed with activated protein C deficiency several years before the stroke. In the control group, stroke was provoked by arterial dissection and in the context of neoplasia in each patient.
The stroke severity based on the NIHSS score was comparable between the two groups (6.3 [5.7] and 4.8 [5.8] in the COVID-19 and control groups, respectively; p = 0.467).
MRI revealed that more than one arterial territory was affected in four (44.4%) and four (8.2%) patients in the COVID-19 and control groups, respectively (p = 0.05). Additionally, regardless of the cause of stroke, four (44.4%) patients in the COVID-19 group and six (12.0%) patients in the control group had one or more microvascular infarcts (p = 0.04). In these four patients with COVID-19 and microvascular infarcts, macrovascular infarcts were observed in a different territory (Figure 2).
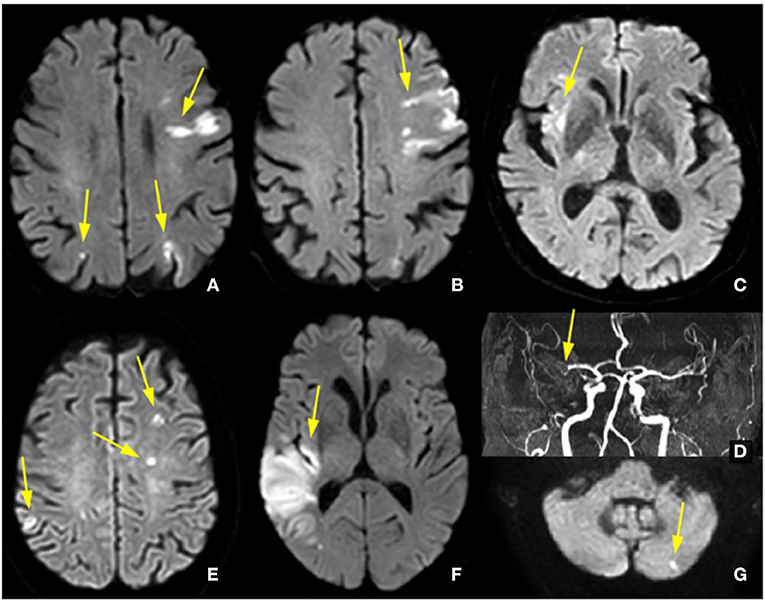
Figure 2. Micro- and macrovascular lesions with the involvement of multiple territories. (A,B) Diffusion-weighted images showing multiple bilateral ischemic lesions (arrows) in patient 4; (C,D) Diffusion-weighted images showing recent right insular infarct with thrombus in the right middle cerebral artery in patient 2; (E-G) Diffusion-weighted images showing multiple microvascular and macrovascular lesions in patient 6.
Mechanical thrombectomy was performed in one patient in the COVID-19 group (11.1%), and intravenous thrombolysis was performed in two (22.2%) and 10 (20.0%) patients in the COVID-19 and control groups, respectively, with combination therapy using both modalities in one patient in the COVID-19 group and in one patient in the control group. No death was observed attributable to the treatment in COVID-19 patients.
Discussion
In this study, among the 772 COVID-19 patients hospitalized in our center, eight cases of ischemic stroke and one of TIA were diagnosed. No intracerebral hemorrhages (ICHs) were diagnosed. However, in the literature, ICHs are more less frequent than ischemic stroke (14). When comparing ischemic stroke characteristics between patients with COVID-19 and those without COVID-19 during the first 2 months of the COVID-19 outbreak, ischemic stroke in patients with COVID-19 appeared to be associated with more frequent multifocal territorial involvement, with more microvascular lesions, and more patients were positive for thrombophilia screening. The levels of inflammatory and coagulation markers (C-reactive protein, D-dimer, and fibrinogen) were higher in the COVID-19 group than those in the control group.
These results are different from those described by Yaghi et al. (15), who found that patients admitted during the same period to stroke centers in the New York metropolitan area with ischemic strokes associated with acute severe COVID-19 were younger (63 ± 17 vs. 70 ± 18, p = 0.001), had higher NIHSS scores (19 vs. 8, p = 0.007), and had more cryptogenic strokes (65.6 vs. 30.4%, p = 0.003) than were those with ischemic strokes in the absence of COVID-19. Szegedi et al. (16) reported a median NIHSS score of 16 in a cohort of 198 patients with acute COVID-19 who experienced stroke, including 23 patients with hemorrhagic stroke. In the present cohort of nine patients with COVID-19 and stroke, the mean NIHSS score was much lower (6.3) than that reported in previous studies with or without control groups (15, 16), and NIHSS score was similar in the two groups (6.3 ± 5.7 vs. 4.8 ± 5.8, p = 0.47). In the study by Yaghi et al. (15), 81.3% of the patients were admitted to the ICU due to severe SARS-CoV-2 infection, and 75.0% were dead or critically ill at last follow-up. The mortality rate was 64% in the study by Szegedi et al. (16), whereas only one patient (11.1%) had severe SARS-CoV-2 infection with acute respiratory distress syndrome justifying an ICU transfer, and none of the nine patients with COVID-19 died in the present study. This difference might partially explain the lower stroke rate in the present study. The severity of SARS-CoV-2 infection is a known risk factor for stroke (4, 16). The difference in the NIHSS score between the current study cohort and the previous studies might thus reflect differences in the severity of COVID-19.
Whereas, COVID-19 is known to cause severe cardiac injury and arrhythmias (8), which may lead to the formation of cardiac thrombi, in the present study, we did not observe a predominant, cardio-embolic, etiological mechanism of stroke in the COVID-19 group. An atherothrombotic mechanism, which might have been triggered by the inflammatory response to COVID-19 and an increased risk of plaque rupture, was not frequently found in our series.
Multifocal strokes, which have been described in patients with COVID-19 (17, 18), arise from a cardio-embolic source, arterio-arterial emboli from large arteries such as the aorta, carotid artery, and basilar artery, or circulating thrombi. In the present study, as in the population described by Yaghi et al. (15) the rate of cardio-embolic and atheromatous causes was the same in both groups.
Another possible explanation for the predominance of multifocal strokes in the present study is microvascular involvement in SARS-CoV-2 infection. In the present cohort, lesions smaller than 0.5 cm in size, indicating microvascular damage due to microthrombus, were more common in the COVID-19 group (p = 0.04). Autopsy (9, 19) and in vivo (20) studies suggest that COVID-19 is associated with endothelial injury and thrombotic microangiopathy. SARS-CoV-2 infects host cells via angiotensin-converting enzyme 2 receptors, which are expressed on endothelial cells, and the infection of endothelial cells leads to endothelial dysfunction (i.e., endothelial injury and lymphocytic endotheliitis) with microthrombus deposition and impaired microcirculatory function (9). Microvascular involvement could also be a consequence of hyperinflammation and neutrophil extracellular traps caused by COVID-19. These traps generate thrombin for fibrin production and represent part of a continuum of sterile inflammation and thrombosis that can involve all vascular beds, including the microvascular circulation (3). Elevated inflammatory parameters in patients with COVID-19-related stroke favor this explanation.
In the present study, the levels of coagulation markers fibrinogen and D-dimer were higher in the COVID-19 group than in the control group, similar to that observed in the study by Yaghi et al. (15), although the age and rates of high-risk conditions were similar between the two groups. The elevation in the levels of these markers may not only be related to the inflammatory response (21) but also reflect COVID-19-related coagulopathy, which overlaps with disseminated intravascular coagulation and thrombotic microangiopathy (3), thereby leading to the formation of multiple microthrombi and multifocal and microvascular infarcts. Inflammation markers, together with thrombophilia, should thus be considered as major determinants for the development of stroke in patients with COVID-19.
In the present study, the rate of thrombophilia was significantly higher in the COVID-19 group than in the control group. Beyrouti et al. reported that five of the six patients with COVID-19-related stroke in their cohort were positive for lupus anticoagulant; one of the patients also had anticardiolipin and anti-β2 glycoprotein-1 antibodies (16). These results must be taken with caution, since infection might have triggered the changes observed in these parameters (22, 23). Moreover, evidence that any of these markers is associated with stroke at all and that the numbers are far too small to draw any serious conclusions is lacking. But several other studies reported that COVID-19 was associated with antiphospholipid syndrome (24–26). The relationship between antiphospholipid antibodies in COVID-19 and COVID-19-associated coagulopathy remains controversial (27).
The present study has several limitations. This was a retrospective study with a limited number of cases. The incidence of acute ischemic stroke in the present study (1.16%) was lower than that reported in other reports (28). Another limitation is that for the control group, COVID-19 negativity was based on the absence of suggestive symptoms, negative RT-PCR, and serological results when performed (at a time when diagnoses were lacking). Adding new tests was not possible, so the possibility of asymptomatic COVID-19 in this group cannot be excluded. Infection severity is a risk factor for thrombosis (16). Moreover, especially at the beginning of pandemic, MRI or time-division multiplexing (TDM) were not systematically performed in patients in the ICU and those who were elderly, due to the rapidly deteriorating life-threatening conditions; thus, some events might have been missed among patients with very serious clinical conditions. The current study findings should be confirmed in prospective studies. However, our strength is having a controlled group, which allowed us to interpret the data more confidently.
Conclusion
In the present study, we reported the different mechanisms of stroke in patients with COVID-19. Strokes affected several territories, with micro- and macro-vascular involvement. The main difference between the patients with and without COVID-19 who developed stroke was the presence of biological signs of hyperinflammation associated with thrombophilia. COVID-19-related strokes were frequently microvascular, suggesting endothelial inflammation and microthrombi due a procoagulant state as underlying causes. From a clinical standpoint, patients with COVID-19 should be considered to be at a higher risk for stroke. The low number of COVID-19 is, however, insufficient to draw robust conclusion, and larger cohorts are needed to confirm our results.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité d'Ethique des Facultés et Hôpitaux de Médecine, Odontologie et Pharmacie of the University Hospital of Strasbourg (approval no, CE-2020-32). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
GH, MM, and FS drafting/revising the manuscript for content, including medical writing for content, study concept or design, acquisition of data, analysis or interpretation of data, and study supervision and coordination. CS, M-HA-D, FV, and GA revising the manuscript for content and acquisition of data. CK revising the manuscript for content and statistical analysis and interpretation of data. All authors fulfill the criteria of authorship and no one else who fulfills the criteria has been excluded. All of them have approved the final submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We appreciate the efforts of Magali Eriey and Anne Pachart for their help in data collection.
References
1. Guan WJ Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. Lodigiani C, Iapichino G, Carenzo L, Cecconi M, Ferrazzi P, Sebastian T, et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. (2020) 191:9–14. doi: 10.1016/j.thromres.2020.04.024
3. Becker RC. COVID-19 update: COVID-19-associated coagulopathy. J Thromb Thrombolysis. (2020) 50:54–67. doi: 10.1007/s11239-020-02134-3
4. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. (2020) 77:683–90. doi: 10.1001/jamaneurol.2020.1127
5. Li Y, Li M, Wang M, Zhou Y, Chang J, Xian Y, et al. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study. Stroke Vasc Neurol. (2020) 5:279–84. doi: 10.1136/svn-2020-000431
6. Katsanos AH, Palaiodimou L, Zand R, Yaghi S, Kamel H, Navi BB, et al. The impact of SARS-CoV-2 on stroke epidemiology and care: a meta-analysis. Ann Neurol. (2021) 89:380–8. doi: 10.1002/ana.25967
7. Berger JR. COVID-19 and the nervous system. J Neurovirol. (2020) 26:143–8. doi: 10.1007/s13365-020-00840-5
8. Gupta A, Madhavan MV, Sehgal K, Nair N, Mahajan S, Sehrawat TS, et al. Extrapulmonary manifestations of COVID-19. Nat Med. (2020) 267:1017–32. doi: 10.1038/s41591-020-0968-3
9. Hernández-Fernández F, Sandoval Valencia H, Barbella-Aponte RA, Collado-Jiménez R, Ayo-Martín Ó, Barrena C, et al. Cerebrovascular disease in patients with COVID-19: neuroimaging, histological and clinical description. Brain. (2020) 143:3089–103. doi: 10.1093/brain/awaa239
10. Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. (2009) 40:2276–93. doi: 10.1161/STROKEAHA.108.192218
11. Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke. (1993) 24:35–41. doi: 10.1161/01.STR.24.1.35
12. Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O'Donnell MJ, et al. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol. (2014) 13:429–38. doi: 10.1016/S1474-4422(13)70310-7
13. Gandhi RT, Lynch JB, Del Rio C. Mild or moderate Covid-19. N Engl J Med. (2020) 383:1757–66. doi: 10.1056/NEJMcp2009249
14. Nannoni S, de Groot R, Bell S, Markus HS. Stroke in COVID-19: a systematic review and meta-analysis. Int J Stroke. (2021) 16:137–49. doi: 10.1177/1747493020972922
15. Yaghi S, Ishida K, Torres J, Mac Grory B, Raz E, Humbert K, et al. SARS-CoV-2 and stroke in a New York healthcare system. Stroke. (2020) 51:2002–11. doi: 10.1161/STROKEAHA.120.030335
16. Szegedi I, Orbán-Kálmándi R, Csiba L, Bagoly Z. Stroke as a potential complication of COVID-19-associated coagulopathy: a narrative and systematic review of the literature. J Clin Med. (2020) 9:3137. doi: 10.3390/jcm9103137
17. Morassi M, Bagatto D, Cobelli M, D'Agostini S, Gigli GL, Bnà C, et al. Stroke in patients with SARS-CoV-2 infection: case series. J Neurol. (2020) 267:2185–92. doi: 10.1007/s00415-020-09885-2
18. Beyrouti R, Adams ME, Benjamin L, Cohen H, Farmer SF, Goh YY, et al. Characteristics of ischaemic stroke associated with COVID-19. J Neurol Neurosurg Psychiatry. (2020) 91:889–91. doi: 10.1136/jnnp-2020-323586
19. Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. Lancet Respir Med. (2020) 8:681–6. doi: 10.1016/S2213-2600(20)30243-5
20. do Espírito Santo DA, Lemos ACB, Miranda CH. In vivo demonstration of microvascular thrombosis in severe COVID-19. J Thromb Thrombolysis. (2020) 50:790–4. doi: 10.1007/s11239-020-02245-x
21. Helms J, Tacquard C, Severac F, Leonard-Lorant I, Ohana M, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. (2020) 46:1089–98. doi: 10.1007/s00134-020-06062-x
22. Syrjänen J, Vaarala O, Iivanainen M, Palosuo T, Valtonen VV, Aho K. Anticardiolipin response and its association with infections in young and middle-aged patients with cerebral infarction. Acta Neurol Scand. (1988) 78:381–6. doi: 10.1111/j.1600-0404.1988.tb03673.x
23. Asherson RA, Cervera R. Antiphospholipid antibodies and infections. Ann Rheum Dis. (2003) 62:388–93.
24. Gkrouzman E, Barbhaiya M, Erkan D, Lockshin MD. Reality check on antiphospholipid antibodies in COVID-19-associated coagulopathy. Arthritis Rheumatol. (2021) 73:173–4. doi: 10.1002/art.41472
25. Zhang Y, Xiao M, Zhang S, Xia P, Cao W, Jiang W, et al. Coagulopathy and antiphospholipid antibodies in patients with Covid-19. N Engl J Med. (2020) 382:e38. doi: 10.1056/NEJMc2007575
26. Harzallah I, Debliquis A, Drénou B. Lupus anticoagulant is frequent in patients with Covid-19. J Thromb Haemost. (2020) 18:2064–5. doi: 10.1111/jth.14867
27. Borghi MO, Beltagy A, Garrafa E, Curreli D, Cecchini G, Bodio C, et al. Anti-phospholipid antibodies in COVID-19 are different from those detectable in the anti-phospholipid syndrome. Front Immunol. (2020) 11:584241. doi: 10.3389/fimmu.2020.584241
Keywords: COVID-19, coagulopathy, inflammation, cerebrovascular, observational study, ischemic stroke
Citation: Hautecloque G, Kempf C, Stan C, Arentz-Dugay M-H, Vuillemet F, Ahle G, Sellal F and Martinot M (2021) Multifocal and Microvascular Involvement in Ischemic Stroke During COVID-19: A Cohort Study With Comparison With Non-COVID-19 Stroke. Front. Neurol. 12:732194. doi: 10.3389/fneur.2021.732194
Received: 28 June 2021; Accepted: 13 September 2021;
Published: 25 October 2021.
Edited by:
Johannes Boltze, University of Warwick, United KingdomReviewed by:
Juan Moisés De La Serna, Universidad Internacional De La Rioja, SpainGian Luigi Gigli, University of Udine, Italy
Copyright © 2021 Hautecloque, Kempf, Stan, Arentz-Dugay, Vuillemet, Ahle, Sellal and Martinot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Geoffroy Hautecloque, Z2VvZmZyb3kuaGF1dGVjbG9xdWVAY2gtY29sbWFyLmZy