 Richard Drexler1*
Richard Drexler1* Sharona Ben-Haim2
Sharona Ben-Haim2 Christian G. Bien3
Christian G. Bien3 Valeri Borger4
Valeri Borger4 Francesco Cardinale5Alexandre Carpentier6
Francesco Cardinale5Alexandre Carpentier6 Fernando Cendes7
Fernando Cendes7 Sarat Chandra8
Sarat Chandra8 Hans Clusmann9Albert Colon10
Hans Clusmann9Albert Colon10 Marco de Curtis11Daniel Delev9
Marco de Curtis11Daniel Delev9 Giuseppe Didato11
Giuseppe Didato11 Lasse Dührsen1Jibril Osman Farah12
Lasse Dührsen1Jibril Osman Farah12 Marc Guenot13,14Saadi Ghatan15Claire Haegelen13,14Hajo Hamer16
Marc Guenot13,14Saadi Ghatan15Claire Haegelen13,14Hajo Hamer16 Jason S. Hauptmann17
Jason S. Hauptmann17 Rosalind L. Jeffree18,19Thilo Kalbhenn20
Rosalind L. Jeffree18,19Thilo Kalbhenn20 Josua Kegele21Niklaus Krayenbühl22Johannes Lang16
Josua Kegele21Niklaus Krayenbühl22Johannes Lang16 Bertrand Mathon6
Bertrand Mathon6 Georgios Naros21
Georgios Naros21 Julia Onken23
Julia Onken23 Fedor Panov15Christian Raftopoulos24Franz L. Ricklefs1Kim Rijkers25
Fedor Panov15Christian Raftopoulos24Franz L. Ricklefs1Kim Rijkers25 Michele Rizzi26
Michele Rizzi26 Karl Rössler27
Karl Rössler27 Olaf Schijns25,28Ulf C. Schneider23Andrea Spyrantis29
Olaf Schijns25,28Ulf C. Schneider23Andrea Spyrantis29 Adam Strzelczyk29Stefan Stodieck30
Adam Strzelczyk29Stefan Stodieck30 Manjari Tripathi8
Manjari Tripathi8 Sumeet Vadera31Mario A. Alonso-Vanegas32José Géraldo Ribero Vaz24Jörg Wellmer33Tim Wehner33
Sumeet Vadera31Mario A. Alonso-Vanegas32José Géraldo Ribero Vaz24Jörg Wellmer33Tim Wehner33 Manfred Westphal1Thomas Sauvigny1
Manfred Westphal1Thomas Sauvigny1- 1Department of Neurosurgery, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Department of Neurosurgery, University of California San Diego, San Diego, CA, United States
- 3Epilepsy Centre Bethel, Krankenhaus Mara, Bielefeld, Germany
- 4Department of Neurosurgery, University Hospital Bonn, Bonn, Germany
- 5“C. Munari” Epilepsy Surgery Center, Niguarda Hospital, Milan, Italy
- 6Department of Neurosurgery, Pitié-Salpêtrière Hospital, Paris, France
- 7Department of Neurology, University of Campinas, Campinas, Brazil
- 8Department of Neurosurgery, AIIMS, New Delhi, India
- 9Department of Neurosurgery, University Hospital RWTH Aachen, Aachen, Germany
- 10School for Mental Health and Neuroscience (MHeNS), University Maastricht (UM), Maastricht, Netherlands
- 11Epilepsy Unit, IRCCS “C. Besta” Neurological Institute Foundation, Milan, Italy
- 12The Walton Centre NHS Foundation Trust, Liverpool, United Kingdom
- 13Department of Functional Neurosurgery, P. Wertheimer Hospital, Hospices Civils de Lyon, Lyon, France
- 14Department for Neurosurgery, University of Lyon, Lyon, France
- 15Department of Neurosurgery, Icahn School of Medicine at Mount Sinai, New York, NY, United States
- 16Epilepsy Center, Department of Neurology, University of Erlangen-Nürnberg, Erlangen, Germany
- 17Department of Neurosurgery, University of Washington, Seattle, WA, United States
- 18Department of Neurosurgery, Royal Brisbane and Womens Hospital, Brisbane, QLD, Australia
- 19Herston Clinical School, University of Queensland, Brisbane, QLD, Australia
- 20Department of Neurosurgery (Evangelisches Klinikum Bethel), Bielefeld University, Medical School, Bielefeld, Germany
- 21Department of Neurology and Epileptology, Hertie Institute of Clinical Brain Research, University of Tubingen, Tubingen, Germany
- 22Division of Pediatric Neurosurgery, University Children's Hospital Zurich, University of Zurich, Zurich, Switzerland
- 23Department of Neurosurgery, Universitätsmedizin Charité-Berlin, Berlin, Germany
- 24Department of Neurosurgery, University Hospital St-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium
- 25Department of Neurosurgery, Academic Center for Epileptology UMC Maastricht, Maastricht, Netherlands
- 26Department of Neurosurgery, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy
- 27Department of Neurosurgery, Medical University Vienna, Vienna, Austria
- 28School for Mental Health and Neuroscience (MHeNS), University Maastricht (UM), Maastricht, Netherlands
- 29Department of Neurosurgery and Epilepsy Center Frankfurt Rhine-Main, Center of Neurology and Neurosurgery, Goethe-University Frankfurt, Frankfurt, Germany
- 30Hamburg Epilepsy Center, Protestant Hospital Alsterdorf, Department of Neurology and Epileptology, Hamburg, Germany
- 31Department of Neurological Surgery, University of California Irvine, Irvine, CA, United States
- 32National Institute of Neurology and Neurosurgery, Manuel Velasco Suarez, Mexico City, Mexico
- 33Ruhr - Epileptology, Department of Neurology, University Hospital Knappschafts-Krankenhaus, Ruhr - University Bochum, Bochum, Germany
Introduction: Optimizing patient safety and quality improvement is increasingly important in surgery. Benchmarks and clinical quality registries are being developed to assess the best achievable results for several surgical procedures and reduce unwarranted variation between different centers. However, there is no clinical database from international centers for establishing standardized reference values of patients undergoing surgery for mesial temporal lobe epilepsy.
Design: The Enhancing Safety in Epilepsy Surgery (EASINESS) study is a retrospectively conducted, multicenter, open registry. All patients undergoing mesial temporal lobe epilepsy surgery in participating centers between January 2015 and December 2019 are included in this study. The patient characteristics, preoperative diagnostic tools, surgical data, postoperative complications, and long-term seizure outcomes are recorded.
Outcomes: The collected data will be used for establishing standardized reference values (“benchmarks”) for this type of surgical procedure. The primary endpoints include seizure outcomes according to the International League Against Epilepsy (ILAE) classification and defined postoperative complications.
Discussion: The EASINESS will define robust and standardized outcome references after amygdalohippocampectomy for temporal lobe epilepsy. After the successful definition of benchmarks from an international cohort of renowned centers, these data will serve as reference values for the evaluation of novel surgical techniques and comparisons among centers for future clinical trials.
Clinical trial registration: This study is indexed at clinicaltrials.gov (NT 04952298).
Introduction
Surgeons strive for the best possible outcome from their operations with the greatest possible chance for recovery and cure of the patients. To optimize the outcome, the continuous monitoring and measurement of key elements of surgical procedures are indispensable. To this end, the number of clinical registries has increased in recent years (1). To evaluate surgical quality, recent initiatives aim to assess the best achievable results for several surgical procedures and reduce unwarranted variation between different centers (2–4). A standardized methodology to describe optimal outcomes in neurosurgery is lacking. The most appealing concept in surgery is a combination of various clinical indicators with risk stratification and a focus on treatment efficacy and adverse events. This offers a more reliable analysis than single-outcome indicators, such as survival or readmission rate (5–10). Nevertheless, an establishment of clinical databases from international centers with an accurate collection of demographic, management, and outcome data for respective surgical procedures is needed. The importance of establishing benchmarks has been demonstrated for various surgical procedures in general and visceral surgery (11–15). As yet, there is very little published about acceptable neurosurgical benchmarks. A benchmark establishes standardized reference values which represent the acceptable common outcome of high-volume centers and can be used for comparison and improvement. Best results are obtained from patients at the lowest risk (10). Therefore, the cohort must be divided into low-risk and high-risk patients according to the defined benchmark criteria that predict a potentially worse postoperative outcome.
The aim of this international multicenter register [Enhancing Safety in Epilepsy Surgery (EASINESS)] is to define robust and standardized outcome references after amygdalohippocampectomy and anteromedial temporal lobectomy for temporal lobe epilepsy. After the successful determination of benchmarks from an international cohort of renowned centers, these data will serve as reference values for the evaluation of novel surgical techniques and comparisons among centers for future clinical trials. They will provide feedback to participating centers to enable deficiencies in care to be addressed, thereby enabling quality improvement. This registry will demonstrate the feasibility and utility of risk-stratified benchmarked data for neurosurgical practice.
Materials and Methods
Study Design
The EASINESS is a retrospectively conducted, multicenter, open registry. The study is a procedure-specific registry, initiated by the Department of Neurosurgery, University Medical Center Hamburg-Eppendorf, Germany. The selected members of participating neurosurgical or epilepsy centers will be invited to form a Steering Committee, which will be responsible for the scientific goals and guarantee the reliability of the data analysis. Neurosurgical, neurological, and epilepsy units from all countries are invited to join the trial and to recruit patients if the center- and patient-specific inclusion criteria are met.
Study Setting and Type of Participants
All patients undergoing mesial temporal lobe epilepsy surgery between January 1, 2015 and December 31, 2019 are included in the study. The following surgical procedures are included: selective amygdalohippocampectomy including anterior parahippocampal gyrus/entorhinal cortex, anteromedial temporal lobe resection including amygdalohippocampectomy with approximately anterior third of the temporal neocortex, amygdala, uncus, hippocampus, anterior parahippocampal gyrus/entorhinal cortex, and anterior temporal lobe resection with two-thirds of the temporal neocortex, amygdala, uncus, hippocampus, and anterior parahippocampal gyrus/entorhinal cortex (16, 17). Patients who went through deep brain stimulation, vagus nerve stimulation, neocortical temporal resection only, or a recurrent resection are not included in this study.
Center-Specific Inclusion Criteria
The participating centers need to perform 30 or more seizure-specific resections as an average per year during the 5-year study period. This threshold is based on the recommendations of the German Society for Epileptology and the Austrian, German, and Swiss working group on presurgical epilepsy diagnosis and operative epilepsy treatment for certification as an epilepsy center performing epilepsy surgery (18, 19). International centers may be accepted on a case-by-case basis if they meet the alternative local guidelines for epilepsy center definition. The implantation of vagus nerve stimulators was not counted toward the number of seizure-specific procedures (Table 1).
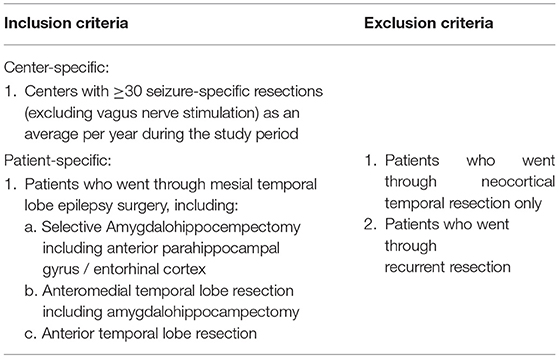
Table 1. Inclusion and exclusion criteria for centers and patients to participate in the Enhancing Safety in Epilepsy Surgery (EASINESS) registry.
Informed Consent
Written informed consent is not required in this retrospective study since all patient data are processed anonymously. The study was approved by the Institutional Ethics Committee centrally at University Medical Center Hamburg-Eppendorf and local governance approval was obtained by each site as necessary. The patients' data were extracted and analyzed following the declaration of Helsinki.
Data Collection
According to a standardized template for mesial temporal lobe epilepsy surgery, patient-specific data, surgical details, postoperative complications, and long-term seizure outcome including neuropsychological assessment will be recorded. The data acquisition will be electronic-based (case report form, CRF), and patient-specific data will be de-identified by the study center. The data will then be transferred into an electronic database and further analyses made at the Department of Neurosurgery, University Medical Center Hamburg-Eppendorf.
Case Report Form
The specially designed and developed Case Report Form (CRF) consists of four parts (Figure 1).
1. Patient characteristics: The first part of the CRF covers preoperative characteristics including patient demographic and baseline characteristics (sex, age, body mass index, educational status, neurological status), comorbidities (diabetes, congestive heart failure, coagulopathy, and COPD), and the American Society of Anesthesiologists (ASA) Physical Status Classification. In addition, seizure-specific features such as a history of neonatal seizure, febrile seizure, encephalitis or meningitis, age at epilepsy onset, type of seizure, average monthly frequency of seizures, and a number of anticonvulsive drugs at the time of surgery are registered. Furthermore, presurgical diagnostic tools (e.g., invasive monitoring, PET, SPECT, MEG) and possible lesions in MRI will be documented.
2. Surgical data: This part covers all aspects of mesial temporal lobe epilepsy surgery. Here, type of procedure, intraoperative navigation, resection of the dominant or non-dominant hemisphere, side of resection, and the operating duration are registered.
3. Postoperative complications: The fourth part addresses all questions of the outcome until discharge after index surgery. Postoperative complications such as stroke, surgical site infection, meningitis, reoperation, new neurological deficits, and in-hospital mortality will be recorded. In addition, the histological finding of the resected lesion is registered.
4. Follow-up: Long-term clinical and seizure outcome after 12 months and an optional later time will be recorded. Here, long-term complications such as reoperation, temporalis muscle atrophy, and neurological deficits are registered. To analyze the seizure-specific outcome after surgery, the International League Against Epilepsy (ILAE) outcome scale, neuropsychological assessment (verbal and figural memory, attention), and the number of antiseizure medications will be documented.
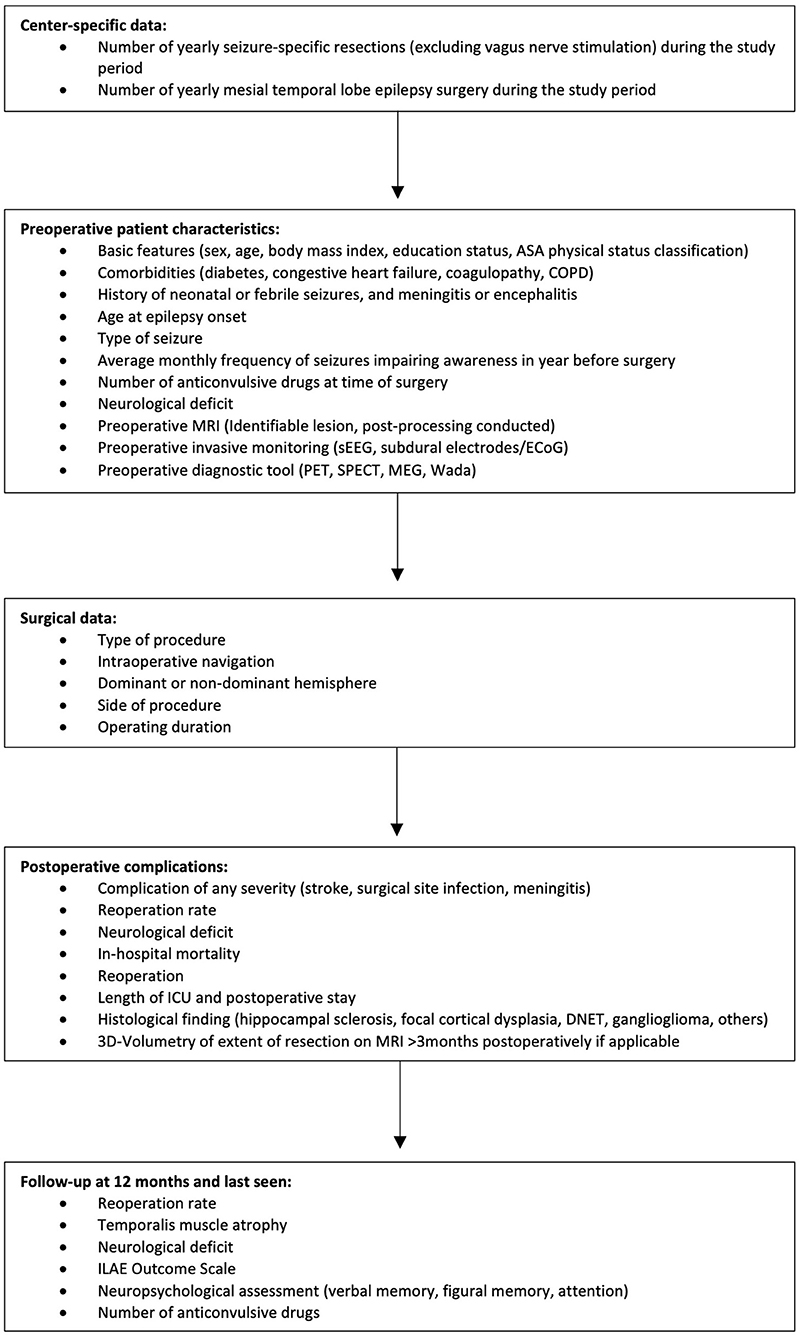
Figure 1. Study protocol of the Enhancing Safety in Epilepsy Surgery (EASINESS) registry.
Data Management
Data collection will be performed locally at each site and de-identified in an independent database, then submitted to the Department of Neurosurgery at University Medical Center Hamburg-Eppendorf (Germany). All results, including patient-specific data, surgical techniques, complications, and long-term outcomes, will be submitted for publication in peer-reviewed journals and/or reported at professional scientific meetings. Every participating center can submit further scientific questions which will be evaluated by the steering committee for approval or rejection. The by-laws of the steering committee are accessible from the principal investigator upon request. This study is indexed at clinicaltrials.gov (NT 04952298).
Statistics
The endpoints will be evaluated using descriptive statistics, and the key figures of the distributions will be presented in tables. Statistical analyses will be made as described in previous studies which established the concept of benchmarking for other surgical procedures (10, 11, 15). Hereby, the cohort is stratified into patients with a low-preoperative and high-preoperative risk profile according to comorbidities which are proven to negatively impact the postoperative course. Afterward, the benchmark cut-off for each outcome indicator is set at the 75th percentile of the median of all centers (10). Depending on the composition of the data, χ2, Mann-Whitney U, and t-tests, or Pearson or Spearman correlation coefficients, will be conducted. The relationships between multiple independent variables on the dependent variable(s) will be tested using multivariate regression analysis.
Registry Reports
The results of the EASINESS registry will be published by the Steering Committee and distributed to all participating centers following careful analysis by the principal investigators (R.D. and T.S.) at the Department of Neurosurgery, University Medical Center Hamburg-Eppendorf.
Discussion
In recent years, quality monitoring and improvement have become more important in the field of healthcare, especially in surgery (20, 21). As a various single- and multiple-outcome indicators for evaluating the quality of surgical procedures were introduced, the concept of benchmarking as introduced by Staiger et al. seems to be the most reliable concept for establishing standardized outcome references and defining acceptable outcomes (10). Benchmarking offers an opportunity to present valid, internationally applicable reference values which originate from the daily routine of a large representative cohort. This will be the first internationally validated benchmark data for neurosurgery and as such will demonstrate that such data collection is both feasible and useful.
Unlike data from randomized controlled trials, which have stringent patient selection criteria and questionable generalizability, this study has only a few patient-specific inclusion criteria, and the results will therefore be generalizable to usual neurosurgical practice.
The EASINESS is a retrospectively conducted, multicenter, open registry with narrowly defined inclusion criteria for international centers. The objective is the application of the previously described benchmarking to define robust and standardized outcome references after temporal lobe epilepsy surgery. Afterward, these benchmarks from an international cohort of high-volume centers will serve as reference values for the evaluation of novel surgical techniques and comparisons among centers or future clinical trials. Furthermore, EASINESS has been established with an interdisciplinary approach collecting outcome data from both a neurosurgical and epileptogenic perspective and presenting novel valuable data compared with existing registries.
Limitations of This Study
The results of this registry should be interpreted considering the limitation that the study design is a retrospective, non-randomized design which could introduce some bias.
Ethics Statement
The studies involving human participants were reviewed and approved by Local Ethics Committee Hamburg 2021-300051-WF. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
RD, LD, and TS contributed to conceptualization and design. All authors drafted the manuscript, critically revised it and collect the data.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Stey AM, Russell MM, Ko CY, Sacks GD, Dawes AJ, Gibbons MM. Clinical registries and quality measurement in surgery: a systematic review. Surgery. (2015) 157:381–95. doi: 10.1016/j.surg.2014.08.097
2. Khuri SF, Daley J, Henderson W, Hur K, Demakis J, Aust JB, et al. The Department of Veterans Affairs' NSQIP: the first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg. (1998) 228:491–507. doi: 10.1097/00000658-199810000-00006
3. Rowell KS, Turrentine FE, Hutter MM, Khuri SF, Henderson WG. Use of national surgical quality improvement program data as a catalyst for quality improvement. J Am Coll Surg. (2007) 204:1293–300. doi: 10.1016/j.jamcollsurg.2007.03.024
4. Kao LS, Lally KP, Thomas EJ, Tyson JE. Improving quality improvement: a methodologic framework for evaluating effectiveness of surgical quality improvement. J Am Coll Surg. (2009) 208:621–6. doi: 10.1016/j.jamcollsurg.2009.01.021
5. Dimick JB, Welch HG, Birkmeyer JD. Surgical mortality as an indicator of hospital quality: the problem with small sample size. JAMA. (2004) 292:847–51. doi: 10.1001/jama.292.7.847
6. Porter ME. What is value in health care? N Engl J Med. (2010) 363:2477–81. doi: 10.1056/NEJMp1011024
7. Donabedian A. The quality of care. How can it be assessed? JAMA J Am Med Assoc. (1988) 260:1743–8. doi: 10.1001/jama.260.12.1743
8. Salet N, Bremmer RH, Verhagen MAMT, Ekkelenkamp VE, Hansen BE, de Jonge PJF, et al. Is Textbook Outcome a valuable composite measure for short-term outcomes of gastrointestinal treatments in the Netherlands using hospital information system data? A retrospective cohort study. BMJ Open. (2018) 8:e019405. doi: 10.1136/bmjopen-2017-019405
9. Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care J Int Soc Qual Health Care. (2003) 15:523–30. doi: 10.1093/intqhc/mzg081
10. Staiger RD, Schwandt H, Puhan MA, Clavien P-A. Improving surgical outcomes through benchmarking. Br J Surg. (2019) 106:59–64. doi: 10.1002/bjs.10976
11. Muller X, Marcon F, Sapisochin G, Marquez M, Dondero F, Rayar M, et al. Defining benchmarks in liver transplantation: a multicenter outcome analysis determining best achievable results. Ann Surg. (2018) 267:419–25. doi: 10.1097/SLA.0000000000002477
12. Raptis DA, Sánchez-Velázquez P, Machairas N, Sauvanet A, Rueda de. Leon A, Oba A, et al. Defining benchmark outcomes for pancreatoduodenectomy with portomesenteric venous resection. Ann Surg. (2020) 272:731–7. doi: 10.1097/SLA.0000000000004267
13. Raptis DA, Linecker M, Kambakamba P, Tschuor C, Müller PC, Hadjittofi C, et al. Defining benchmark outcomes for ALPPS. Ann Surg. (2019) 270:835–41. doi: 10.1097/SLA.0000000000003539
14. Rössler F, Sapisochin G, Song G, Lin Y-H, Simpson MA, Hasegawa K, et al. Defining benchmarks for major liver surgery: a multicenter analysis of 5202 living liver donors. Ann Surg. (2016) 264:492–500. doi: 10.1097/SLA.0000000000001849
15. Sánchez-Velázquez P, Muller X, Malleo G, Park J-S, Hwang H-K, Napoli N, et al. Benchmarks in pancreatic surgery: a novel tool for unbiased outcome comparisons. Ann Surg. (2019) 270:211–8. doi: 10.1097/SLA.0000000000003223
16. Schramm J. Temporal lobe epilepsy surgery and the quest for optimal extent of resection: a review. Epilepsia. (2008) 49:1296–307. doi: 10.1111/j.1528-1167.2008.01604.x
17. Al-Otaibi F, Baeesa SS, Parrent AG, Girvin JP, Steven D. Surgical techniques for the treatment of temporal lobe epilepsy. Epilepsy Res Treat. (2012) 2012:1–13. doi: 10.1155/2012/374848
18. Schmitz B, Mayer T, Neubauer B, Rosenow F, Bast T. Definition von Epilepsiezentren [Internet]. (2010). Available online at: http://www.izepilepsie.de/cweb2/cgi-bin-noauth/cache/VAL_BLOB/4092/4092/1106/definitionepilepsiezentren.pdf
19. Rosenow F, Bast T, Czech T, Feucht M, Hans VH, Helmstaedter C, et al. Revised version of quality guidelines for presurgical epilepsy evaluation and surgical epilepsy therapy issued by the Austrian, German, and Swiss working group on presurgical epilepsy diagnosis and operative epilepsy treatment. Epilepsia. (2016) 57:1215–20. doi: 10.1111/epi.13449
20. Ettorchi-Tardy A, Levif M, Michel P. Benchmarking: a method for continuous quality improvement in health. Healthc Policy Polit Sante. (2012) 7:e101–119. doi: 10.12927/hcpol.2012.22872
Keywords: epilepsy, epilepsy surgery, temporal lobe epilepsy, outcome, benchmark, seizure outcome, amygdalohippocampectomy, anteromedial resection
Citation: Drexler R, Ben-Haim S, Bien CG, Borger V, Cardinale F, Carpentier A, Cendes F, Chandra S, Clusmann H, Colon A, Curtis Md, Delev D, Didato G, Dührsen L, Farah JO, Guenot M, Ghatan S, Haegelen C, Hamer H, Hauptmann JS, Jeffree RL, Kalbhenn T, Kegele J, Krayenbühl N, Lang J, Mathon B, Naros G, Onken J, Panov F, Raftopoulos C, Ricklefs FL, Rijkers K, Rizzi M, Rössler K, Schijns O, Schneider UC, Spyrantis A, Strzelczyk A, Stodieck S, Tripathi M, Vadera S, Alonso-Vanegas MA, Vaz JGR, Wellmer J, Wehner T, Westphal M and Sauvigny T (2021) Enhancing Safety in Epilepsy Surgery (EASINESS): Study Protocol for a Retrospective, Multicenter, Open Registry. Front. Neurol. 12:782666. doi: 10.3389/fneur.2021.782666
Received: 24 September 2021; Accepted: 05 November 2021;
Published: 13 December 2021.
Edited by:
Edoardo Ferlazzo, University of Catanzaro, ItalyReviewed by:
Rushna Ali, Spectrum Health, United StatesSandrine de Ribaupierre, Western University, Canada
Copyright © 2021 Drexler, Ben-Haim, Bien, Borger, Cardinale, Carpentier, Cendes, Chandra, Clusmann, Colon, Curtis, Delev, Didato, Dührsen, Farah, Guenot, Ghatan, Haegelen, Hamer, Hauptmann, Jeffree, Kalbhenn, Kegele, Krayenbühl, Lang, Mathon, Naros, Onken, Panov, Raftopoulos, Ricklefs, Rijkers, Rizzi, Rössler, Schijns, Schneider, Spyrantis, Strzelczyk, Stodieck, Tripathi, Vadera, Alonso-Vanegas, Vaz, Wellmer, Wehner, Westphal and Sauvigny. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Richard Drexler, ci5kcmV4bGVyQHVrZS5kZQ==