 Marie Salvetti1Guillaume Schnell2Nicolas Pichon3,4Maleka Schenck5Pierrick Cronier4,6Sebastien Perbet7
Marie Salvetti1Guillaume Schnell2Nicolas Pichon3,4Maleka Schenck5Pierrick Cronier4,6Sebastien Perbet7 Jean-Baptiste Lascarrou4,8Christophe Guitton9Olivier Lesieur4,10
Jean-Baptiste Lascarrou4,8Christophe Guitton9Olivier Lesieur4,10 Laurent Argaud4,11
Laurent Argaud4,11 Gwenhael Colin4,12Bernard Cholley13Jean-Pierre Quenot14
Gwenhael Colin4,12Bernard Cholley13Jean-Pierre Quenot14 Hamid Merdji15,16
Hamid Merdji15,16 Thomas Geeraerts17
Thomas Geeraerts17 Michael Piagnerelli18Gwenaelle Jacq1Marine Paul1Jonathan Chelly4,19Louise de Charentenay1
Michael Piagnerelli18Gwenaelle Jacq1Marine Paul1Jonathan Chelly4,19Louise de Charentenay1 Nicolas Deye4,20,21
Nicolas Deye4,20,21 Marc Danguy des Déserts22
Marc Danguy des Déserts22 Guillaume Thiery23Marc Simon24Vincent Das25Frederic Jacobs26Charles Cerf27Julien Mayaux28Pascal Beuret29Abdelkader Ouchenir30Antoine Lafarge31Bertrand Sauneuf4,32Cedric Daubin4,33Alain Cariou4,34,35Stein Silva4,36
Guillaume Thiery23Marc Simon24Vincent Das25Frederic Jacobs26Charles Cerf27Julien Mayaux28Pascal Beuret29Abdelkader Ouchenir30Antoine Lafarge31Bertrand Sauneuf4,32Cedric Daubin4,33Alain Cariou4,34,35Stein Silva4,36 Stephane Legriel1,4,37* for the Antigone investigators
Stephane Legriel1,4,37* for the Antigone investigators- 1Medical-Surgical Intensive Care Unit, Centre Hospitalier de Versailles—Site André Mignot, Le Chesnay, France
- 2Medical-Surgical Intensive Care Unit, GH Le Havre, Le Havre, France
- 3Medical-Surgical Intensive Care Unit, CHU de Limoges, Limoges, France
- 4AfterROSC, Paris, France
- 5Médecine Intensive Réanimation, Hôpital de Hautepierre, Hôpitaux Universitaires de Strasbourg, Strasbourg, France
- 6Intensive Care Unit, Sud-Francilien Hospital Center, Corbeil-Essonnes, France
- 7Department of Perioperative Medicine, University Hospital of Clermont-Ferrand, 58 Rue Montalembert, Université Clermont Auvergne, CNRS, INSERM, GReD, Clermont-Ferrand, France
- 8Medicine Intensive Reanimation, University Hospital, Nantes, France
- 9Medical-Surgical Intensive Care Unit, Centre Hospitalier du Mans, Le Mans, France
- 10Intensive Care Unit, Saint-Louis Hospital, La Rochelle, France
- 11Medical Intensive Care Unit, Hospices Civils de Lyon, Edouard Herriot Teaching Hospital, Lyon, France
- 12Medical-Surgical Intensive Care Unit, La Roche-sur-Yon District Hospital Centre, La Roche-sur-Yon, France
- 13Hôpital Européen Georges Pompidou, Assistance Publique-Hôpitaux de Paris, Université Paris Cité et Service d'Anesthésie-Réanimation Médecine Péri Opératoire, Paris, France
- 14Service de Médecine Intensive-Réanimation, CHU Dijon Bourgogne, Dijon, France
- 15Faculté de Médecine, Hôpitaux Universitaires de Strasbourg, Nouvel Hôpital Civil, Service de Médecine Intensive Réanimation, Université de Strasbourg (UNISTRA), Strasbourg, France
- 16UMR 1260, Regenerative Nano Medicine, INSERM, Fédération de Médecine Translationnelle de Strasbourg (FMTS), Université de Strasbourg, Strasbourg, France
- 17Department of Anaesthesiology, Critical Care and Perioperative Medicine, Toulouse University Hospital, Toulouse, France
- 18Intensive Care Unit, Marie-Curie Teaching Hospital, Université Libre de Bruxelles, Charleroi, Belgium
- 19Intensive Care Unit, Groupe Hospitalier Sud Ile de France, Melun, France
- 20Medical Intensive Care Unit, Lariboisière University Hospital, APHP, Paris, France
- 21INSERM UMR-S 942, Lariboisière Hospital, Paris, France
- 22Intensive Care Unit, Clermont Tonnerre Military Hospital, Brest, France
- 23Medical-Surgical Intensive Care Unit, Saint-Étienne University Hospital, Saint-Étienne, France
- 24Department of Intensive Care, Cliniques du Sud-Luxembourg of Arlon, Arlon, Belgium
- 25Medical-Surgical Intensive Care Unit, Centre Hospitalier Intercommunal André Grégoire, Montreuil, France
- 26Medical Intensive Care Unit, Beclère Teaching Hospital, Clamart, France
- 27Department of Intensive Care, Foch Hospital, Suresnes, France
- 28Department of Pulmonology and Intensive Care, Pitié-Salpêtrière Teaching Hospital, Paris, France
- 29Department of Intensive and Continuous Care, Roanne Hospital, Roanne, France
- 30Medical Intensive Care Unit, Louis Pasteur Hospital, Chartres, France
- 31Medical Intensive Care Unit, Saint Louis Teaching Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France
- 32General Intensive Care Unit, Cotentin Public Hospital Centre, Cherbourg-en-Cotentin, France
- 33Medical Intensive Care Unit, Caen Teaching Hospital, Caen, France
- 34Medical Intensive Care Unit, Cochin University Hospital, Assistance Publique-Hôpitaux de Paris and Université de Paris, Paris, France
- 35INSERM U970, Paris Cardiovascular Research Centre, Paris, France
- 36Critical Care Unit, University Teaching Hospital of Purpan, Toulouse, France
- 37UVSQ, INSERM, CESP, PsyDev Team, Paris-Saclay University, Villejuif, France
Background: Cardiac arrest is the most life-threatening complication of attempted suicide by hanging. However, data are scarce on its characteristics and outcome predictors.
Methods: This retrospective observational multicentre study in 31 hospitals included consecutive adults admitted after cardiac arrest induced by suicidal hanging. Factors associated with in-hospital mortality were identified by multivariate logistic regression with multiple imputations for missing data and adjusted to the temporal trends over the study period.
Results: Of 450 patients (350 men, median age, 43 [34–52] years), 305 (68%) had a psychiatric history, and 31 (6.9%) attempted hanging while hospitalized. The median time from unhanging to cardiopulmonary resuscitation was 0 [0–5] min, and the median time to return of spontaneous circulation (ROSC) was 20 [10–30] min. Seventy-nine (18%) patients survived to hospital discharge. Three variables were independently associated with higher in-hospital mortality: time from collapse or unhanging to ROSC>20 min (odds ratio [OR], 4.71; 95% confidence intervals [95%CIs], 2.02–10.96; p = 0.0004); glycaemia >1.4 g/L at admission (OR, 6.38; 95%CI, 2.60–15.66; p < 0.0001); and lactate >3.5 mmol/L at admission (OR, 6.08; 95%CI, 1.71–21.06; p = 0.005). A Glasgow Coma Scale (GCS) score of >5 at admission was associated with lower in-hospital mortality (OR, 0.009; 95%CI, 0.02–0.37; p = 0.0009).
Conclusion: In patients with hanging-induced cardiac arrest, time from collapse or unhanging to return of spontaneous circulation, glycaemia, arterial lactate, and coma depth at admission were independently associated with survival to hospital discharge. Knowledge of these risk factors may help guide treatment decisions in these patients at high risk of hospital mortality.
Introduction
Suicide is a public health issue that is responsible for ~700,000 deaths each year worldwide and 1.3% of all deaths in 2019 (1). Hanging is a common and particularly lethal suicide method used chiefly by young men with psychiatric or addictive comorbidities (2–5). Hanging can result in various types of injury and can lead to cardiac arrest (CA) via several mechanisms. In recent studies, cardiac arrest was present in initial management in 20%−60% of patients (4–7). The interruption of cervical blood flow by hanging results in early brain ischaemia, which is worsened by CA (2, 4, 5). Various cervical (2, 3, 5, 8–11) and thoracic (2, 3, 9) structures may be injured. Patients may also suffer damage to the heart, which is usually reversible, and/or acute pulmonary oedema (8, 12, 13).
Mortality and residual functional impairments are common after near-hanging. Death may occur immediately if resuscitation is not provided or after hospital management. In-hospital mortality rates have varied widely, from ~10% to nearly 80%, mainly due to the selection of patient characteristics (4, 5, 14, 15). One of the main determinants of mortality and residual neurological impairment is the occurrence of hanging-induced CA (4, 7, 9, 11, 14, 16). In a retrospective study of 886 ICU patients with hanging injuries, 450 patients had cardiac arrest, which was strongly associated with mortality (OR 19.50; 95%CI, 7.21–60.90) (17). This high rate of mortality is probably ascribable to CA-related systemic ischaemia-reperfusion syndrome with initial cardiogenic, vasoplegic hemodynamic failure, and anoxic brain injury (18).
To date, few studies have focussed specifically on outcome predictors in patients with hanging-induced CA. Therefore, this multicentre retrospective study aimed to describe patient characteristics and hospital survival after hanging-induced CA and identify predictors of in-hospital mortality.
Materials and methods
This study complies with the standards set by the French and Belgian legislation on retrospective clinical research aimed at protecting the confidentiality of personal data. The study protocol was approved by the ethics committee (Comité de Protection des Personnes de Paris, Ile de France XI, 13 September 2012, #XI/12061) and is registered on ClinicalTrials.gov (#NCT04096976). Survivors retrospectively received a written consent form as soon as they recovered decision-making competency; if they refused consent, they were excluded from the registry. All procedures involving the patients complied with the ethical standards of our institutional and national research committees and with the 1964 Declaration of Helsinki and its later amendments.
Study population
Consecutive adults admitted to one of the 31 university or university-affiliated ICUs in France and Belgium after successfully resuscitating people after a suicidal near-hanging injury between February 1992 and May 2014 were identified. Among them, patients older than 18 years who experienced CA, followed by the return of spontaneous circulation (ROSC), were included in the present study.
Patient and public involvement
It was not appropriate or possible to involve patients and/or the public in the design, conduct, report, or disseminate plans of our research.
Data collection
As previously described (17), we used a standardized form for each patient to collect demographic data, medical history, and the characteristics of the hanging-induced CA according to the Utstein-style guidelines (19).
Study outcomes
Hospital mortality was the primary outcome measure. We also described patient characteristics and identified independent predictors of in-hospital mortality as secondary outcomes.
Statistical analysis
Quantitative parameters were described as a median in the form of interquartile range (IQR) and qualitative parameters in the form of numbers (percentage). We compared the categorical variables using Fisher's exact test and compared the continuous variables using the Wilcoxon rank-sum test. We ordered categorical variables using the chi-square and the Kruskal-Wallis tests. We then performed logistic regression to identify associations between factors and hospital mortality. Continuous variables were checked for log-linearity. Non-log-linear variables were transformed into dummy variables according to their inflection point or median value. Non-collinear variables that yielded p-values <0.05 by univariate analysis or were clinically relevant were considered for inclusion into a multivariable model.
Stepwise model selection guided by the Akaike Information Criterion was performed. Variables tested were age; male sex; time from collapse or unhanging to ROSC; asystole as first recorded rhythm; GCS score, body temperature, pulse oximetry, glycaemia, and lactate at admission; and the total number of organ failures on day 1. Time of management (1992–1995, 1996–2000, 2001–2005, 2006–2010, or 2011–2014) and Simplified Acute Physiology Score (SAPS) II score on day one after admission were used for adjustment. Missing data were handled under the data-missing-at-random hypothesis using multiple imputations by chained equations (52 imputations, 10 iterations). Associations of factors with hospital mortality were reported as ORs with their 95%CIs. All tests were two-sided, and p-values of <0.05 were considered significant.
The analyses were performed using the R statistical programme, version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria).1
Results
Of the 886 patients admitted to the 31 participating hospitals after near-hanging during the 23-year study period, 450 (51%) experienced CA and were included in this study (Figure 1).
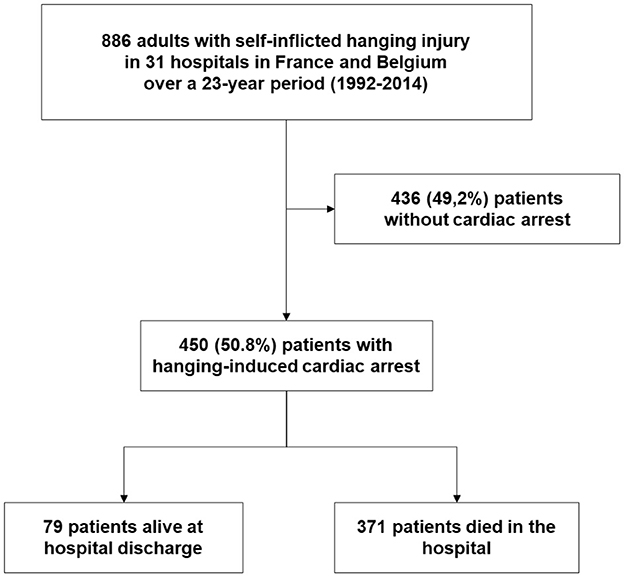
Figure 1. Patient flow chart.
Patient characteristics and on-scene management of cardiac arrest
Table 1 reports the main patient characteristics. Overall, presumed fatal comorbidities were very rare, but approximately two-thirds of patients had psychiatric diagnoses. For most patients, hanging was the first attempt at suicide. Cardiac arrest usually occurred at home, and approximately half of the patients received basic resuscitation using an automated external defibrillator before the arrival of emergency services. Asystole was the most common first recorded rhythm. Overall, a quarter of the patients received at least one external electric shock, and approximately three-quarters received adrenaline with a median cumulative dose of 3 mg before ROSC. The median time from collapse or unhanging to ROSC was 20 [10–30] min.
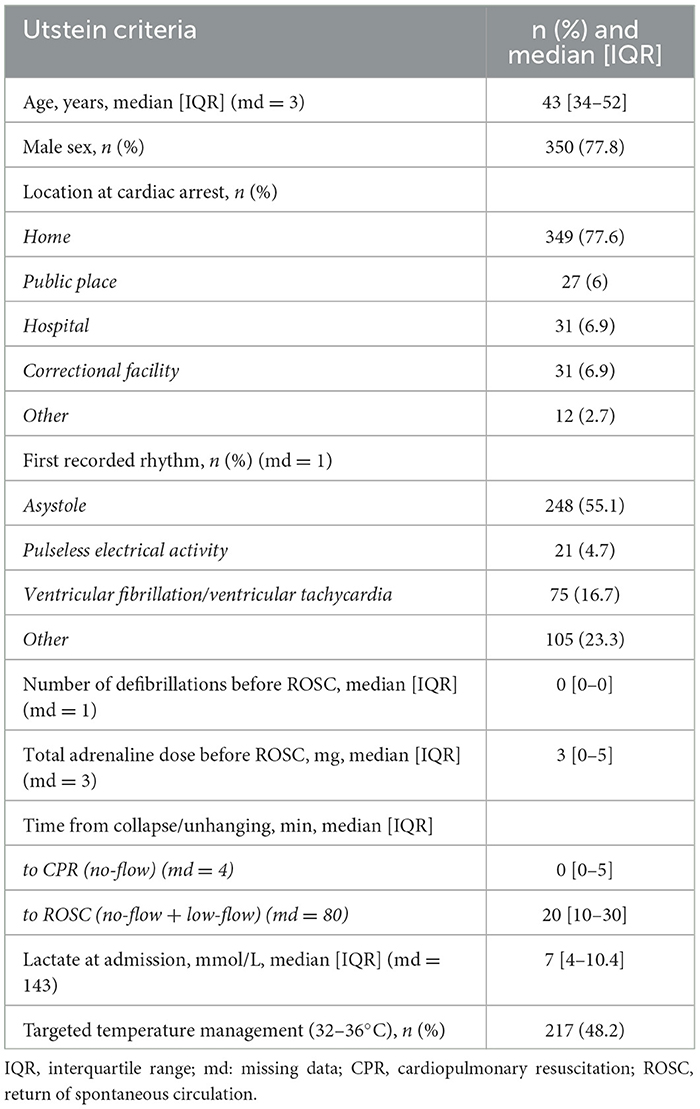
Table 1. Cardiac arrest the Utstein-style guidelines criteria in 450 patients with hanging-induced cardiac arrest.
In-hospital management of hanging-induced cardiac arrest
At admission, 71% of patients underwent cerebral and cervical computed tomography (CT), 5% cervical-spine radiography, and 3% cerebral and cervical magnetic resonance imaging (MRI). A bony cervical lesion with spinal injury was found in 5% of the 343 patients with cervical imaging and a vascular cervical lesion in 2% of those with vascular imaging. Targeted temperature management was used in 217 (48%) patients for a median effective duration of 24 [23–24] h.
Outcomes
Table 2 reports factors associated with in-hospital mortality. Mechanical ventilation was used for 4 [2–7] days, and the median length of hospital stay was 5 [2–9] days. Overall, in-hospital mortality was 82% (371/450).
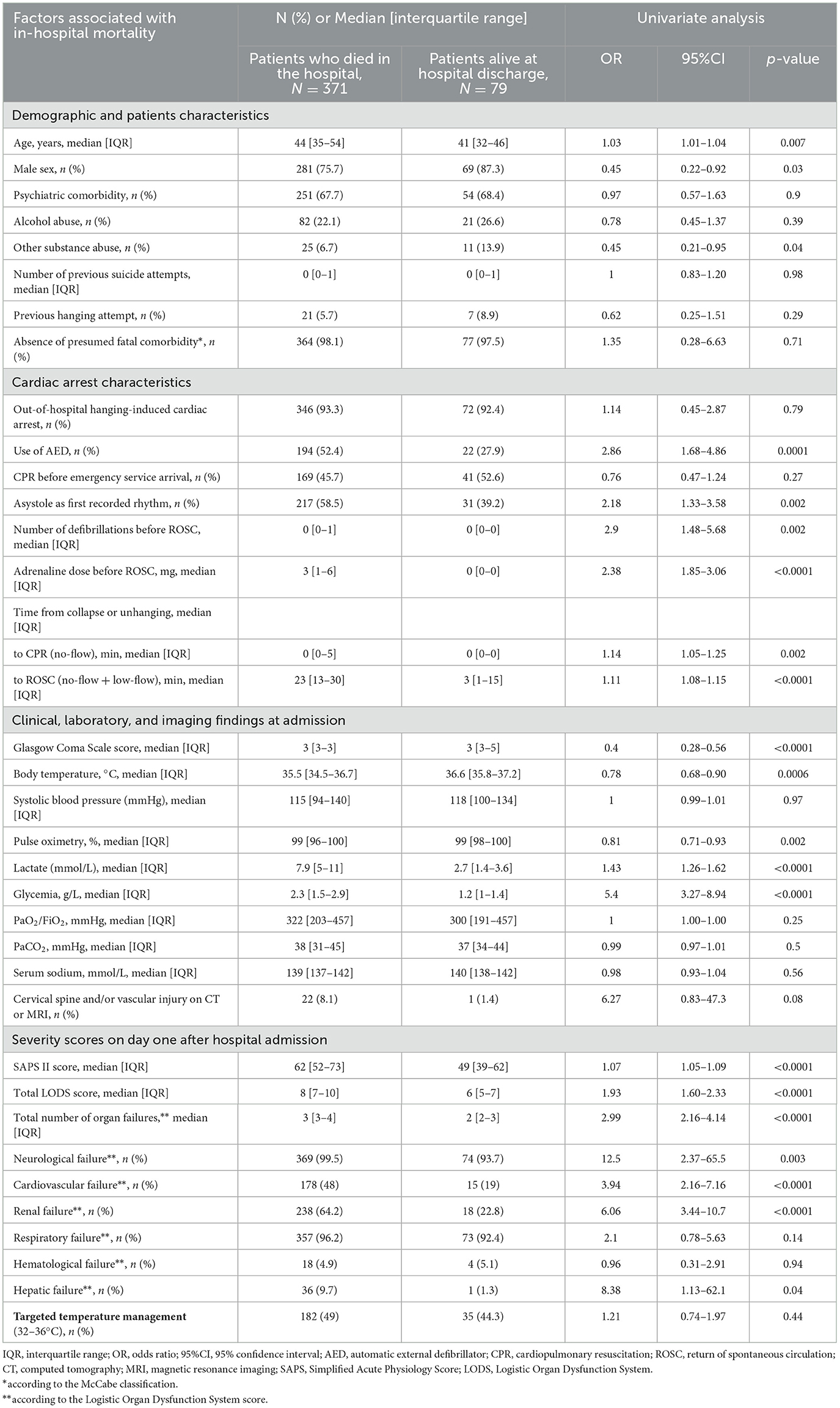
Table 2. Factors associated with in-hospital mortality in 450 patients after hanging-induced cardiac arrest.
Brain death occurred in 120 (27%) patients at a median time of 4 [2–5] days after CA. A decision to withdraw life-sustaining interventions was made for 162 (36%) patients at a median time of 5 [3–8] days after hanging. Of the 79 patients who survived to hospital discharge, 69 (87%) had a favorable neurological outcome defined as a Cerebral Performance Category (CPC) score of 1 or 2.
Predictors of hospital mortality
Using multivariate analysis after missing data imputation (Figure 2), we found that three variables were independently associated with higher hospital mortality: time from collapse or unhanging to ROSC >20 min (OR, 4.71; 95%CI, 2.02–10.96; p = 0.0004); glycaemia >1.4 g/L at admission (OR, 6.38; 95%CI, 2.60–15.66; p < 0.0001); and lactate >3.5 mmol/L at admission (OR, 6.08; 95%CI, 1.71–21.06; p = 0.005). In addition, a GCS score of >5 at admission was associated with lower in-hospital mortality (OR, 0.009; 95%CI, 0.02–0.37; p = 0.0009).
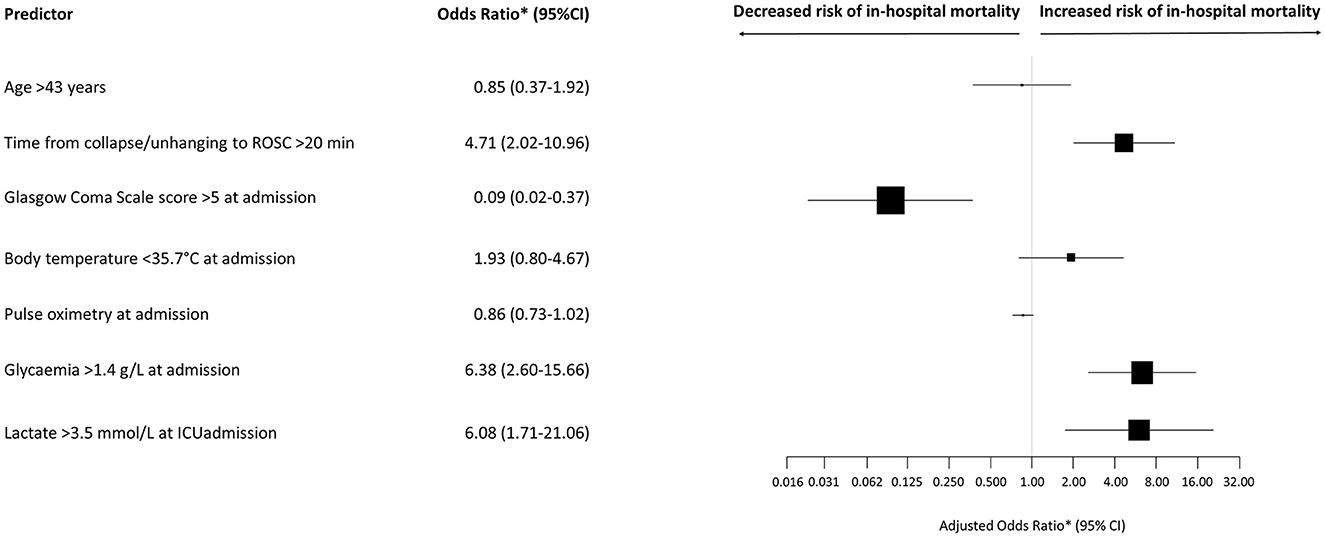
Figure 2. Odds ratios for hospital mortality. *Adjusted according to time of management (1992–1995, 1996–2000, 2001–2005, 2006–2010, or 2011–2014) and SAPS II score on day 1 after ICU admission. Data marker sizes reflect the relative size of each covariate. Error bars indicate 95% confidence intervals of odds ratios. ROSC, return of spontaneous circulation; ICU, intensive care unit.
Discussion
Of the 450 patients with hanging-induced CA, 79 (18%) were discharged alive from the hospital. Four factors were independently associated with the risk of hospital death: time from collapse or unhanging to ROSC >20 min, glycaemia >1.4 g/L at admission, and arterial lactate >3.5 mmol/L at admission were associated with higher hospital mortality, and a GCS score of >5 at admission was associated with lower hospital mortality.
Our 450 patients with CA constituted approximately half of the patients admitted to 31 hospitals after attempted suicide by hanging, which is within the previously reported 20%−60% range (4–7). The main characteristics of our patients were consistent with earlier reports (2–6, 20–23).
Our cohort had a higher frequency of basic CPR delivered before emergency-service arrival, i.e., 47% compared to 10%−30% (5, 20–23) in keeping with the shorter no-flow time and lower lactate level in our patients (5, 12, 21, 22). Further, there was an unexpectedly higher proportion of patients with an initial shockable rhythm compared to earlier studies (5, 20–23). Few studies have reported the frequency of cardiovascular or hemodynamic failure after hanging-induced cardiac arrest. In our population, two-fifths of patients had cardiovascular failure according to the LODS score. Previously reported serum lactate levels at admission were often higher than that reported in our study, ranging from 5 to 13 mmol/L. Kidney failure, often with shock, occurred in 30%−50% of patients with CA due to hanging or other causes, compared to 58% in our study (24, 25). Cervical CT or MRI were infrequently performed and rarely showed spinal or vascular injuries in our patients, in accordance with other data (2, 5, 9, 10). The devastating consequences of missing such injuries are prompting the increased use of contrast-enhanced cervical CT after hanging (3, 7, 9, 11).
Only 18% of our patients were discharged alive from the hospital. However, among them, 87% had a favorable neurological outcome with a CPC score of 1 or 2 at hospital discharge. Two studies from South Korea found noticeably higher survival rates of 43% and 52%, respectively, but with a persistent vegetative state in over 80% of survivors (21, 22). In an Australian study, 3% of patients survived to discharge, and most had limited or no disability (20). These results suggest differences across countries in criteria for treatment-limitation decisions. However, a recent study from North America had a 29% hospital survival rate with satisfactory neurological outcomes in most survivors (5).
A time from collapse or unhanging to ROSC longer than 20 min predicted hospital mortality in our study and another study (11). No-flow and low-flow times are well-established predictors of mortality after CA (26, 27). The two other predictors of higher mortality were high serum lactate and high glycaemia in keeping with other studies. Tight blood glucose control has been demonstrated to improve the neurological prognosis after CA (4). Further, a less severe consciousness impairment at admission was associated with hospital survival; the cut-off was a GCS score of >5, compared to 3–6 in other studies (5, 12, 22).
The retrospective design of our study is a major limitation that led to a substantial proportion of missing data for some variables. However, we used the multiple-chain equation method to counterbalance this weakness. We hypothesize that the longer the hanging time, the lower the probability of reaching ROSC. However, the exact duration of hanging-induced CA is generally unknown, and the no-flow and low-flow times should therefore be taken as minimum values. This limitation is inherent in our type of population. However, our study only included patients who achieved ROSC and could consequently be secondarily managed in the intensive care unit. Thus, while the delay between hanging and unhanging is unknown, we believe that the effect of this delay on ROSC is unlikely in our population. Moreover, whereas 71% of patients underwent cerebral and cervical computed tomography, we cannot provide information on the repetition of these explorations during real-time patient management to assess for structural damage and/or diffuse axonal injury. Practices may have changed over the 23-year study period. Moreover, the study period ended in 2014, and since then, further changes have occurred, notably regarding the use of targeted temperature management. However, in our study, targeted temperature management was not significantly associated with hospital survival. Finally, we did not obtain follow-up data after hospital discharge.
To conclude, in this retrospective multicentre observational study of 450 patients admitted to the hospital after hanging-induced CA, time from collapse or unhanging to ROSC, glycaemia, arterial lactate rate, and the GCS at admission were independently associated with hospital survival. Knowledge of these risk factors may help guide treatment decisions for this population of patients at high risk of hospital mortality.
Antigone investigators
Nicolas Girard (La Rochelle), Martin Cour (Lyon), Adriaan Prisacariu (Arlon), Auguste Dargent (Dijon), Ferhat Meziani (Strasbourg), Thibaut Baudic (Brest), Philippe Vignon (Limoges), Candice Belony (Le Chesnay), Charlene Leparq (Le Chesnay), Cecile Carre (Le Chesnay), Pauline Moriss (Le Chesnay), Emmanuelle Noel (Le Chesnay), Quentin De Roux (Creteil), Matthieu Resche-Rigon (Paris), Thomas Rossignol (Le Mans), Bruno Megarbane (Paris), Alexis Soummer (Suresnes), Alexandre Demoule (Paris), Pierre Kalfon (Chartres), Charlotte Martin (Toulouse), Elie Azoulay (Paris).
Data availability statement
Publicly available datasets were analyzed in this study. Ethical restrictions apply to the availability of these data regarding participant privacy prohibiting us from making the entire data set publicly available. However, after publication, data will be available to any researcher who provides a methodologically sound study proposal that is approved by the central study team. Proposals can be submitted to the Versailles Hospital (c2xlZ3JpZWxAZ2h0NzhzdWQuZnI=). Individual patients and hospitals will not be identifiable in any released data and all appropriate information governance protocols will be followed.
Ethics statement
The studies involving humans were approved by Comité de Protection des Personnes de Paris, Ile de France XI. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SL: conceived, designed, supervised the trial, coordinated the data collection, and performed the statistical analysis. SL, LC, MD, GS, NP, J-BL, JC, MSi, and GJ: collected the data. SL and MSa: analyzed and interpreted the data and wrote the first draft of the manuscript. All authors revised the manuscript for important intellectual content and approved the final version of the manuscript.
Funding
This work was supported by a grant (#12/17) from the DRCI de Versailles, a non-profit publicly funded research agency of the Versailles Hospital, France. The study was supported by the French public funding agency Délégation à la Recherche Clinique et à l'Innovation (DRCI), Versailles, France.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^http://www.R-project.org (accessed 20 December, 2022).
References
1. Suicide Worldwide in 2019: Global Health Estimates. Geneva: World Health Organization. (2021). Available online at: https://apps.who.int/iris/rest/bitstreams/1350975/retrieve
2. Martin MJ, Weng J, Demetriades D, Salim A. Patterns of injury and functional outcome after hanging: analysis of the National Trauma Data Bank. Am J Surg. (2005) 190:836–40. doi: 10.1016/j.amjsurg.2005.05.051
3. Boots RJ, Joyce C, Mullany DV, Anstey C, Blackwell N, Garrett PM, et al. Near-hanging as presenting to hospitals in Queensland: recommendations for practice. Anaesth Intensive Care. (2006) 34:736–45. doi: 10.1177/0310057X0603400610
4. Gantois G, Parmentier-Decrucq E, Duburcq T, Favory R, Mathieu D, Poissy J. Prognosis at 6 and 12months after self-attempted hanging. Am J Emerg Med. (2017) 35:1672–6. doi: 10.1016/j.ajem.2017.05.037
5. Hsu CH, Haac B, McQuillan KA, Tisherman SA, Scalea TM, Stein DM. Outcome of suicidal hanging patients and the role of targeted temperature management in hanging-induced cardiac arrest. J Trauma Acute Care Surg. (2017) 82:387–91. doi: 10.1097/TA.0000000000001281
6. Hsu CH, Haac BE, Drake M, Bernard AC, Aiolfi A, Inaba K, et al. EAST multicenter trial on targeted temperature management for hanging-induced cardiac arrest. J Trauma Acute Care Surg. (2018) 85:37–47. doi: 10.1097/TA.0000000000001945
7. Kim MJ, Yoon YS, Park JM, Cho J, Lim H, Kang H, et al. Neurologic outcome of comatose survivors after hanging: a retrospective multicenter study. Am J Emerg Med. (2016) 34:1467–72. doi: 10.1016/j.ajem.2016.04.036
8. Salim A, Martin M, Sangthong B, Brown C, Rhee P, Demetriades D. Near-hanging injuries: a 10-year experience. Injury. (2006) 37:435–9. doi: 10.1016/j.injury.2005.12.013
9. Nichols SD, McCarthy MC, Ekeh AP, Woods RJ, Walusimbi MS, Saxe JM. Outcome of cervical near-hanging injuries. J Trauma. (2009) 66:174–8. doi: 10.1097/TA.0b013e31817f2c57
10. Schellenberg M, Inaba K, Warriner Z, Alfson D, Roman J, Van Velsen V, et al. Near hangings: epidemiology, injuries, and investigations. J Trauma Acute Care Surg. (2019) 86:454–7. doi: 10.1097/TA.0000000000002134
11. Penney DJ, Stewart AH, Parr MJ. Prognostic outcome indicators following hanging injuries. Resuscitation. (2002) 54:27–9. doi: 10.1016/s0300-9572(02)00050-3
12. Champion S, Spagnoli V, Deye N, Megarbane B, Baud F. Cardiac impairment after hanging attempt: a preliminary descriptive study. Ann Cardiol Angeiol (Paris). (2013) 62:259–64. doi: 10.1016/j.ancard.2013.03.006
13. Viswanathan S, Muthu V, Remalayam B. Pulmonary edema in near hanging. J Trauma Acute Care Surg. (2012) 72:297–301. doi: 10.1097/TA.0b013e3182191298
14. Matsuyama T, Okuchi K, Seki T, Murao Y. Prognostic factors in hanging injuries. Am J Emerg Med. (2004) 22:207–10. doi: 10.1016/j.ajem.2004.02.012
15. Solhi H, Pazoki S, Mehrpour O, Alfred S. Epidemiology and prognostic factors in cases of near hanging presenting to a referral hospital in Arak, Iran. J Emerg Med. (2012) 43:599–604. doi: 10.1016/j.jemermed.2011.09.035
16. Kao CL, Hsu IL. Predictors of functional outcome after hanging injury. Chin J Traumatol. (2018) 21:84–7. doi: 10.1016/j.cjtee.2017.04.013
17. de Charentenay L, Schnell G, Pichon N, Schenck M, Cronier P, Perbet S, et al. Outcomes in 886 critically ill patients after near-hanging injury. Chest. (2020) 158:2404–13. doi: 10.1016/j.chest.2020.07.064
18. Nolan JP, Morley PT, Hoek TL, Hickey RW. Advancement Life support Task Force of the International Liaison committee on R. Therapeutic hypothermia after cardiac arrest an advisory statement by the Advancement Life support Task Force of the International Liaison committee on Resuscitation. Resuscitation. (2003) 57:231–5. doi: 10.1161/01.CIR.0000079019.02601.90
19. Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest: a statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. (2015) 96:328–40. doi: 10.1016/j.resuscitation.2014.11.002
20. Deasy C, Bray J, Smith K, Bernard S, Cameron P. Vacar steering committee. Hanging-associated out-of-hospital cardiac arrests in Melbourne, Australia. Emerg Med J. (2013) 30:38–42. doi: 10.1136/emermed-2011-201035
21. Lee BK, Jeung KW, Lee HY, Lim JH. Outcomes of therapeutic hypothermia in unconscious patients after near-hanging. Emerg Med J. (2012) 29:748–52. doi: 10.1136/emermed-2011-200493
22. Shin J, Lee H, Kim J, Kim J, Choi S, Jeung K, et al. Outcomes of hanging-induced cardiac arrest patients who underwent therapeutic hypothermia: a multicenter retrospective cohort study. Resuscitation. (2014) 85:1047–51. doi: 10.1016/j.resuscitation.2014.04.012
23. Wee JH, Park KN, Oh SH, Youn CS, Kim HJ, Choi SP. Outcome analysis of cardiac arrest due to hanging injury. Am J Emerg Med. (2012) 30:690–4. doi: 10.1016/j.ajem.2011.03.013
24. Chua HR, Glassford N, Bellomo R. Acute kidney injury after cardiac arrest. Resuscitation. (2012) 83:721–7. doi: 10.1016/j.resuscitation.2011.11.030
25. Hasper D, von Haehling S, Storm C, Jorres A, Schefold JC. Changes in serum creatinine in the first 24 hours after cardiac arrest indicate prognosis: an observational cohort study. Crit Care. (2009) 13:R168. doi: 10.1186/cc8144
26. Chan PS, Spertus JA, Krumholz HM, Berg RA Li Y, Sasson C, Nallamothu BK. Get With the guidelines-resuscitation registry I. A validated prediction tool for initial survivors of in-hospital cardiac arrest. Arch Intern Med. (2012) 172:947–53. doi: 10.1001/archinternmed.2012.2050
Keywords: near-hanging, intensive care unit, coma/therapy, outcome, cardiopulmonary resuscitation
Citation: Salvetti M, Schnell G, Pichon N, Schenck M, Cronier P, Perbet S, Lascarrou J-B, Guitton C, Lesieur O, Argaud L, Colin G, Cholley B, Quenot J-P, Merdji H, Geeraerts T, Piagnerelli M, Jacq G, Paul M, Chelly J, de Charentenay L, Deye N, Danguy des Déserts M, Thiery G, Simon M, Das V, Jacobs F, Cerf C, Mayaux J, Beuret P, Ouchenir A, Lafarge A, Sauneuf B, Daubin C, Cariou A, Silva S and Legriel S (2023) Epidemiology and outcome predictors in 450 patients with hanging-induced cardiac arrest: a retrospective study. Front. Neurol. 14:1240383. doi: 10.3389/fneur.2023.1240383
Received: 14 June 2023; Accepted: 11 August 2023;
Published: 25 September 2023.
Edited by:
Alexandra Reynolds, Mount Sinai Hospital, United StatesReviewed by:
Dana Klavansky, Icahn School of Medicine at Mount Sinai, United StatesIvan Da Silva, RUSH University Medical Center, United States
Franziska Herpich, Christiana Care Health System, United States
Copyright © 2023 Salvetti, Schnell, Pichon, Schenck, Cronier, Perbet, Lascarrou, Guitton, Lesieur, Argaud, Colin, Cholley, Quenot, Merdji, Geeraerts, Piagnerelli, Jacq, Paul, Chelly, de Charentenay, Deye, Danguy des Déserts, Thiery, Simon, Das, Jacobs, Cerf, Mayaux, Beuret, Ouchenir, Lafarge, Sauneuf, Daubin, Cariou, Silva and Legriel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stephane Legriel, c2xlZ3JpZWxAZ2h0NzhzdWQuZnI=