 Wolfgang H. Jost1*
Wolfgang H. Jost1* Tobias Bäumer2
Tobias Bäumer2 Andrea Bevot3Ulrich Birkmann4Carsten Buhmann5Maria Grosheva6
Andrea Bevot3Ulrich Birkmann4Carsten Buhmann5Maria Grosheva6 Orlando Guntinas-Lichius7Rainer Laskawi8Sebastian Paus9Christina Pflug10A. Sebastian Schroeder11
Orlando Guntinas-Lichius7Rainer Laskawi8Sebastian Paus9Christina Pflug10A. Sebastian Schroeder11 Björn Spittau12Armin Steffen13Bernd Wilken14Martin Winterholler15Steffen Berweck16
Björn Spittau12Armin Steffen13Bernd Wilken14Martin Winterholler15Steffen Berweck16- 1Parkinson-Klinik Ortenau, Wolfach, Germany
- 2Institute of Systemic Motor Science, CBBM, University of Lübeck, Lübeck, Germany
- 3Department of Neuropediatrics and Developmental Medicine, University Children’s Hospital Tübingen, Tübingen, Germany
- 4Department of Neurology, Schluckambulanz, GFO Clinics Troisdorf, Troisdorf, Germany
- 5Department of Neurology, University Hospital Hamburg-Eppendorf, Hamburg, Germany
- 6Department of Otorhinolaryngology, Head and Neck Surgery, Medical Faculty, University of Cologne, Cologne, Germany
- 7Department of Otorhinolaryngology, Jena University Hospital, Jena, Germany
- 8Department of Otorhinolaryngology, University Hospital Göttingen, Göttingen, Germany
- 9Department of Neurology, GFO Clinics Troisdorf, Troisdorf, Germany
- 10Department of Voice, Speech and Hearing Disorders, University Hospital Hamburg-Eppendorf, Hamburg, Germany
- 11Clinic for Child Neurology and Social Pediatrics, Child Center Maulbronn, Maulbronn, Germany
- 12Anatomy and Cell Biology, Medical School OWL, Bielefeld University, Bielefeld, Germany
- 13Department for Otorhinolaryngology, University of Lübeck, Lübeck, Germany
- 14Department of Pediatric Neurology, Klinikum Kassel, Kassel, Germany
- 15Department of Neurology, Sana Hospital Rummelsberg, Nuremberg/Schwarzenbruck, Germany
- 16Specialist Center for Pediatric Neurology, Neurorehabilitation and Epileptology, Schön Clinic, Vogtareuth, Germany
Sialorrhea is defined as a chronic excessive flow of saliva from the mouth, often with adverse consequences for health and quality of life of patients. In addition to currently used non-drug treatment and systemic drugs, intraglandular Botulinum Neurotoxin A (BoNT/A) injections have been examined in case studies, controlled trials and clinical practice. Two pivotal Phase III trials recently led to market approval in the USA and EU for IncobotulinumtoxinA [Xeomin®, IncoBoNT/A, Clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins, Merz Pharmaceuticals GmbH] for treatment of chronic sialorrhea in adults and pediatric patients. This review provides a multidisciplinary approach to discuss the current state of sialorrhea therapy as well as benefits and current limitations of BoNT/A injections. A consensus regarding treatment recommendations made available to physicians in Germany in 2022 has now been updated here for presentation to an international audience. This review provides a framework including a flow chart for patient selection, recommendations for dosing and the injection process, as well as a discussion of therapeutic goals, long-term benefits and safety aspects. This review is aimed at supporting physicians in developing multidisciplinary and individualized treatment approaches to achieve optimal benefits for patients.
1 Introduction
Sialorrhea is defined as a chronic excessive flow of saliva from the mouth that can have a serious impact on a patient’s health and quality of life. It is one of the symptoms that can accompany several neurological disorders. Current therapies include systemic drugs, even though often used off-label, as well as non-drug treatments. In addition, intraglandular Botulinum Neurotoxin A (BoNT/A) injections for patients with sialorrhea have been explored for many years, in clinical practice as well as in case studies and controlled trials (1–13). Two pivotal Phase III trials showed good efficacy and a favorable safety profile for IncobotulinumtoxinA [Xeomin®, IncoBoNT/A, Clostridium botulinum neurotoxin type A (150 kD), free from complexing proteins, Merz Pharmaceuticals GmbH] (1–3). This evidence recently led to its market approval in the USA and EU for treatment of chronic sialorrhea in adults and pediatric patients.
Following these studies and subsequent approvals, the experts involved in this review discussed the current state of sialorrhea therapy in clinical practice, the benefits of BoNT/A injections, and the current limitations and obstacles of this treatment. The multidisciplinary approach of these discussions was essential to assess the issues from different perspectives and to define best practices. Consensus regarding the treatment recommendations was reached by evaluating the clinical trial data, by discussing the current treatment guideline “Hypersalivation” from the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC) (14), and based on the broad practical experience of the contributing authors. These recommendations were made available to physicians in Germany in 2022 (15, 16) and have now been updated here for presentation to an international audience.
BoNT/A therapy for patients with sialorrhea is highly individualized and should be a collaborative effort between experts from different medical and therapeutic disciplines. The aim of this review is to provide a framework for developing multidisciplinary treatment concepts for sialorrhea on a case-by-case basis and to support treating physicians in their treatment decisions for optimal patient outcomes.
2 Etiology and characteristics of sialorrhea
In most cases chronic sialorrhea is caused by excessive collection of saliva in the mouth due to impairments in swallowing or in orofacial functions. A less common reason for hypersalivation is an overproduction of saliva in the glands due to a side effect of certain medications which is not addressed in this text here. The term “hypersalivation” is often used synonym for sialorrhea. Increased salivation is normal in the first 4 years of life and is regarded as pathological after that (17–19).
Sialorrhea can be a symptom of various neurological disorders, including neurodegenerative Parkinson’s syndromes, dementia, apraxia, Huntington’s disease, cerebrovascular diseases (e.g., stroke), inflammatory diseases of the central nervous system (e.g., multiple sclerosis, encephalitis, meningitis), motor neuron diseases (e.g., amyotrophic lateral sclerosis), brain tumors, craniocerebral trauma, intoxication, and cerebral palsy. Sialorrhea is also seen in disorders of the peripheral nervous system like caudal cranial nerve disorders and Guillain-Barré syndrome. Sialorrhea can also have other causes, e.g., head and neck cancers, defects after surgery or after radiation of head and neck or of the upper gastrointestinal tract. Furthermore, patients in palliative care and ventilated and/or tracheotomy patients can experience sialorrhea. Drug-induced sialorrhea can occur with parasympathomimetics (e.g., pyridostigmine) and neuroleptics (especially clozapine, risperidone, haloperidol, aripiprazole).
The consequences of chronic troublesome sialorrhea are two-fold. Firstly, sialorrhea can cause health issues, e.g., due to saliva causing skin maceration on face and hands or saliva entering the respiratory tract, which can lead to serious events like aspiration pneumonia. These issues are particularly troublesome because they add to the symptoms that patients experience due to their underlying neurological disorders. Secondly, sialorrhea has a severe impact on the quality of life of patients and caregivers, leading to social stigma, embarrassment, and withdrawal from social life. In the authors’ experience, patients and caregivers are sometimes neither aware of the extent of the sialorrhea symptoms and consequences nor of the treatment options that can provide relief. Physicians should actively discuss the issues with patients and/or their caregivers to determine whether treatment is required.
Several drugs and non-drug treatments for sialorrhea are available, albeit with known side effects particularly for systemic acting drugs. Now that IncoBoNT/A gained approval by the regulatory authorities both for adult and pediatric patients, it is a viable alternative or addition to existing therapy schemes. Unlike other drugs, BoNT/A acts locally, directly in the salivary glands. The most important salivary glands are the three major salivary glands, i.e., the paired parotid, submandibular, and sublingual glands (Figure 1). They are located in the neck, around the oral cavity. The parotid glands are the largest glands and extend vertically from the zygomatic arch to the anterior border of the sternocleidomastoid muscle and horizontally from the mastoid process to the parotid duct via the masseter muscle. They secrete saliva into the oral cavity via the parotid duct which opens through the buccal mucosa opposite of the second upper molar tooth. The sublingual glands are located in the floor of the mouth below the tongue. The submandibular glands are positioned inside the submandibular space below the mylohyoid line partly covered by the mandible. The sublingual and submandibular gland have a common duct, entering the oral cavity at the floor of the mouth to both sides of the frenulum of the tongue (20–22). The submandibular glands produce by far the largest volume of saliva (~70%), followed by the parotid gland (~25%). Salivary secretion is controlled by the autonomic nervous system and is an important first step of food digestion. It contributes to the degradation of complex carbohydrates, the wetting of solid food, and the release of nutrients and flavors. Furthermore, saliva ensures a continuous rinsing of oral surfaces, controlling biofilm development and, thus, protecting teeth from caries. The average production of saliva in adults is 1–1.5 L per day. The production of salvia can be stimulated and increased up to five times from the basal production value by eating or smelling food (23–25). While the submandibular glands are mainly responsible for the basal mucous and serous salvia, the parotid glands are responsible for the serous stimulated component (26, 27).

Figure 1. Schematic illustration of the location of the salivary glands. Actual position and size of the salivary glands show patient individual variability. Therefore, ultrasound-guided injection is recommended. (Modified according to Jost W., Atlas der Botulinumtoxin-Injektion © KVM—Der Medizinverlag, Berlin).
3 Botulinum Neurotoxin use for treatment of sialorrhea
Botulinum toxins are high molecular weight protein complexes derived from Clostridium botulinum bacteria. The molecules’ neurotoxin section is the pharmacologically active component. Botulinum Neurotoxins act by binding selectively to receptors on peripheral cholinergic nerve endings, where the toxin is internalized and ultimately inhibits the release of the neurotransmitter acetylcholine at the neuroglandular junction in a dose-dependent manner (28, 29). This leads to a reversible decrease in saliva production and—in many cases—to a clinically relevant improvement in sialorrhea.
Botulinum Neurotoxin Types A [IncobotulinumtoxinA (Xeomin®), OnabotulinumtoxinA (Botox®), AbobotulinumtoxinA (Dysport®)] and B [RimabotulinomtoxinB (Neurobloc®)] are used for medical purposes. For sialorrhea treatment, the toxin is injected into the large salivary glands, which leads to a decrease of salivary secretion. The recent clinical trials and subsequent marketing approvals for IncoBoNT/A in sialorrhea treatment confirm the effectiveness that physicians have observed for off-label use in clinical practice for almost two decades (30–32).
4 Clinical trials
Substantial evidence has been obtained in clinical trials to show efficacy and safety of BoNT (types A and/or B) for treatment of sialorrhea. Trials enrolled patients with Parkinson’s syndrome, amyotrophic lateral sclerosis, early childhood brain damage, ear/nose/throat tumors, tracheal cannulas and ventilation, and dysphagia of various types. In most trials, efficacy was evaluated by quantitative measurements of saliva production over time, accompanied by subjective assessments of patients’ quality of life (8–10, 12, 13, 19, 33–35). While efficacy and safety is comparable both with BoNT/A and BoNT/B, there is evidence of a clinically relevant tendency to form antibodies for serotype B (5, 33, 35).
Two Phase III trials using IncoBoNT/A were pivotal for gaining marketing approval for this compound (Xeomin®) from the Food and Drug Administration (FDA) and European Medicines Agency (EMA) for sialorrhea in adults (in 2018/2019) and in pediatric patients (in 2020/2021).
The first of these trials (SIAXI) was a randomized, placebo-controlled, double-blind study, treating adult patients with either 75 units or 100 units of IncoBoNT/A (74 patients per group), while 36 patients received placebo. The most frequent underlying conditions of the study patients were idiopathic Parkinson’s syndrome, atypical Parkinson’s syndrome, stroke, and traumatic brain injury. The BoNT/A injections in this trial were distributed among the parotid glands (60% of injection volume) and submandibular glands (40% of injection volume), leading to the approved treatment recommendations. Significant improvements in sialorrhea were seen during the 16-week follow-up phase after injection with 100 units BoNT/A, based on the unstimulated salivary flow rate (uSFR) and the subjective Global Impression of Change scale (GICS). Side effects (adverse events assessed as related to treatment) were observed in around 9% of patients in each treatment group (including placebo), none of which were serious (1). The placebo-controlled first cycle of the SIAXI study was followed by up to three further open-label, dose-blinded injection sessions (75 units or 100 units IncoBoNT/A) up to 48 weeks. The results of this extension period showed sustained efficacy with continued good tolerability and high patient adherence. For around 4% of patients treated with the 100 units dose, dysphagia was reported as a side effect (2). A clear advantage of using ultrasound guidance for injections (optional in this trial) was not observed. Marketing approval for sialorrhea treatment in adults was subsequently granted for the higher of the two dosages (100 units), as this showed a longer and somewhat stronger efficacy with a good safety profile.
The SIAXI trial was followed by a similarly designed Phase III trial for pediatric patients aged 2–17 years (SIPEXI). A total of 220 patients (body weight ≥ 12 kg) were included and received pre-specified body weight-adapted doses in the range of 20–75 U IncoBoNT/A (around 2 U/kg) or placebo. Patients weighing ≥ 30 kg received a fixed dose of 75 U. After consultation with the regulatory authorities, none of the patients under 6 years of age received placebo for ethical reasons. Ultrasound guidance of the injection procedure was mandatory in this trial. The body weight-dependent dosing scheme and the distribution among the parotid and submandibular glands, which was based on the SIAXI trial and clinical experience, proved adequate in this trial and was the basis for the approved dosing recommendations for children and adolescents (see Table 1). The SIPEXI trial showed good results, comparable to the SIAXI trial in adults. In the 16-week follow-up period after the first injection session, IncoBoNT/A was superior to placebo, both regarding the reduction in salivary flow rate and the subjective improvement measured on the GICS. The subsequent open-label extension period with up to three further injection sessions over up to 48 weeks confirmed efficacy and safety. An additive effect was observed over time, with treatment effects increasing with repeated injection cycles. This was more pronounced than in the SIAXI trial. Treatment was well-tolerated throughout the trial. In the first injection cycle, 2 patients aged 6–17 years experienced side effects after IncoBoNT/A treatment, none of which were serious. During the open-label extension period, 8 patients (5.5%) experienced side effects, including four patients with dysphagia. Tolerance in the 2–5-year-olds was similarly good; only one patient experienced side effects which were injection site reactions (3).
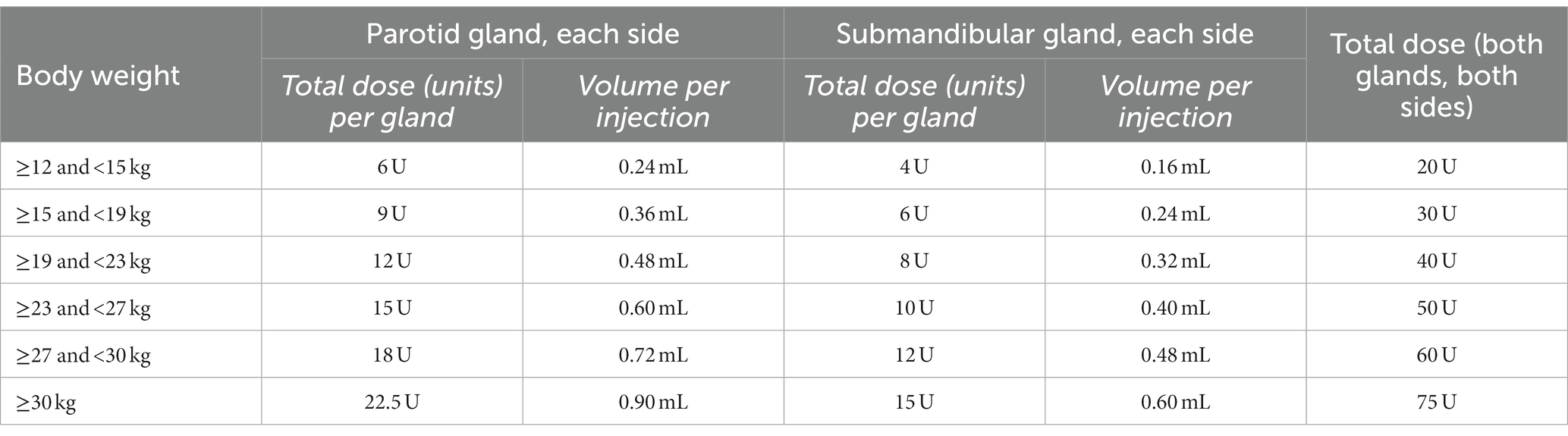
Table 1. Dosing scheme for weight-dependent dose determination for pediatric patients.
4.1 Patient selection for BoNT/A treatment
Sialorrhea treatment is highly individual due to the condition’s varied etiology and extent. No one-fits-all scheme can be prescribed, and physicians must take several factors into consideration when selecting patients for BoNT/A treatment. Generally, adult patients and pediatric patients aged 2 years or older (≥12 kg body weight) with troublesome sialorrhea can be considered for treatment. A patient’s subjective experience of the severity of clinical symptoms and their impact on quality of life must be at the core of any therapeutic decision. Standardized assessment tools and questionnaires can be used to evaluate quality of life and the level of social interactions (see section on therapeutic goals below). The treatment with IncoBoNT/A is approved for sialorrhea of neurological etiology. However, it is of importance to include the extent of the sialorrhea and its direct consequences into the treatment decision. It must be noted that when assessing pediatric patients with sialorrhea, their intellectual skills must be judged carefully, as these are often underestimated due to outward appearances.
The next step is a physical examination which should be extensive and multidisciplinary. It should determine or clarify an underlying neurological condition, assess muscle function, anatomy, and dental issues. Specialists should be consulted as needed, including otorhinolaryngologists, speech therapists, and phoniatricians.
Patients’ eligibility for BoNT/A treatment can be limited for various reasons and the treating physician must assess the circumstances carefully before making treatment decisions. Cases of suspected (micro-)aspiration, respiratory problems when eating, excessively long meals, or repeated pneumonia must be examined in detail. The German guideline “Hypersalivation” from the DGHNO-KHC (14) recommends a screening of swallowing ability and a phoniatric or ear/nose/throat examination, including endoscopic diagnostics [e.g., fiber-optic endoscopic evaluation of swallowing (FEES)] and/or X-ray videofluoroscopy (36–42). In this context, recent developments show the value of real-time magnetic resonance sequences as a promising option allowing an assessment that does not involve active participation by the patient (43, 44). As dysphagia is the most frequent cause of sialorrhea, a targeted assessment of any swallowing issues is essential before proceeding with treatment decisions. The authors recommend active questioning of the patient and/or caregiver according to the checklist provided in Table 2. Treatment of patients with pronounced dysphagia must be considered carefully, as dysphagia is also a rare side effect of BoNT/A injections (1–3). An unintended exacerbation of the existing dysphagia or issues due to the change in salivary flow may be problematic in such patients. This depends on whether the dysphagia is caused by disturbed secretion leading to aspiration of superfluous saliva or by difficulties in swallowing food or medication without residues in mouth and throat, whereby a reduction of salivary flow can be detrimental. The reduction of salivary flow by BoNT/A can increase the risk of dental issues due to increased biofilm formation. Patients with existing disorders like caries or gingivitis should receive dental treatments before and/or during BoNT/A therapy and adequate prophylaxis. Dental check-ups for children during the treatment with BoNT/A are recommended in general. In cases of drug-induced sialorrhea, a reduction, discontinuation or replacement of the causative drug should be discussed before considering the patient for BoNT/A treatment. Patients on anticoagulant therapy with vitamin K antagonists, new oral anticoagulants or high-dose heparin treatment should, if possible, pause their anticoagulant therapy before receiving BoNT/A injections. If this is not possible, the patient must be monitored for approx. 30 min after the injections to rule out complications due to hematoma formation in the floor of the mouth. Before treatment with IncoBoNT/A the contraindications must be observed as per product labeling; patients with known hypersensitivity to any of the product components or with an infection at the proposed injection site cannot be treated. The effect of IncoBoNT/A injections can be increased when combined with irradiation treatment of head and neck area (including salivary glands) and/or with simultaneous use of anticholinergics, which should be avoided. Furthermore, due to lack of data, IncoBoNT/A should not be used during pregnancy and lactation.
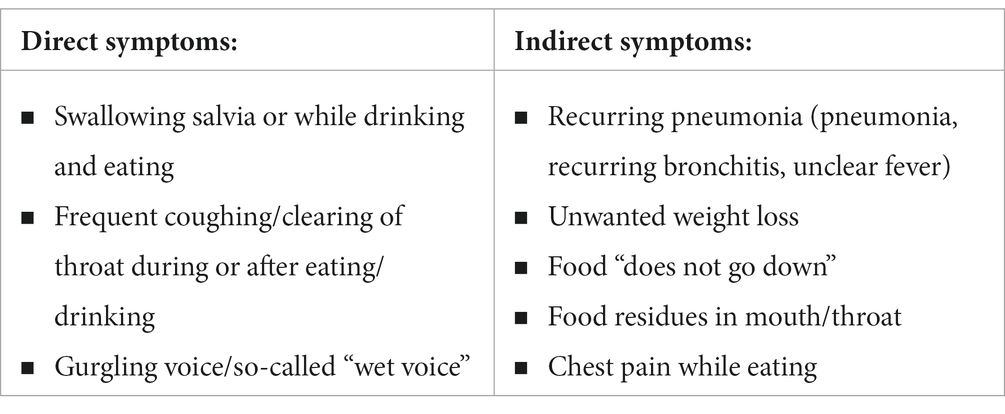
Table 2. Dysphagia anamnesis—checklist for active questioning.
The authors have developed a flow chart to guide physicians in selecting patients who can benefit from BoNT/A treatment (Figure 2). The chart is intended to close any gaps in diagnostics and to support well considered treatment decisions. Depending on the outcomes of the assessments, patients are identified as either eligible for BoNT/A treatment, eligible with limitations, or non-eligible.
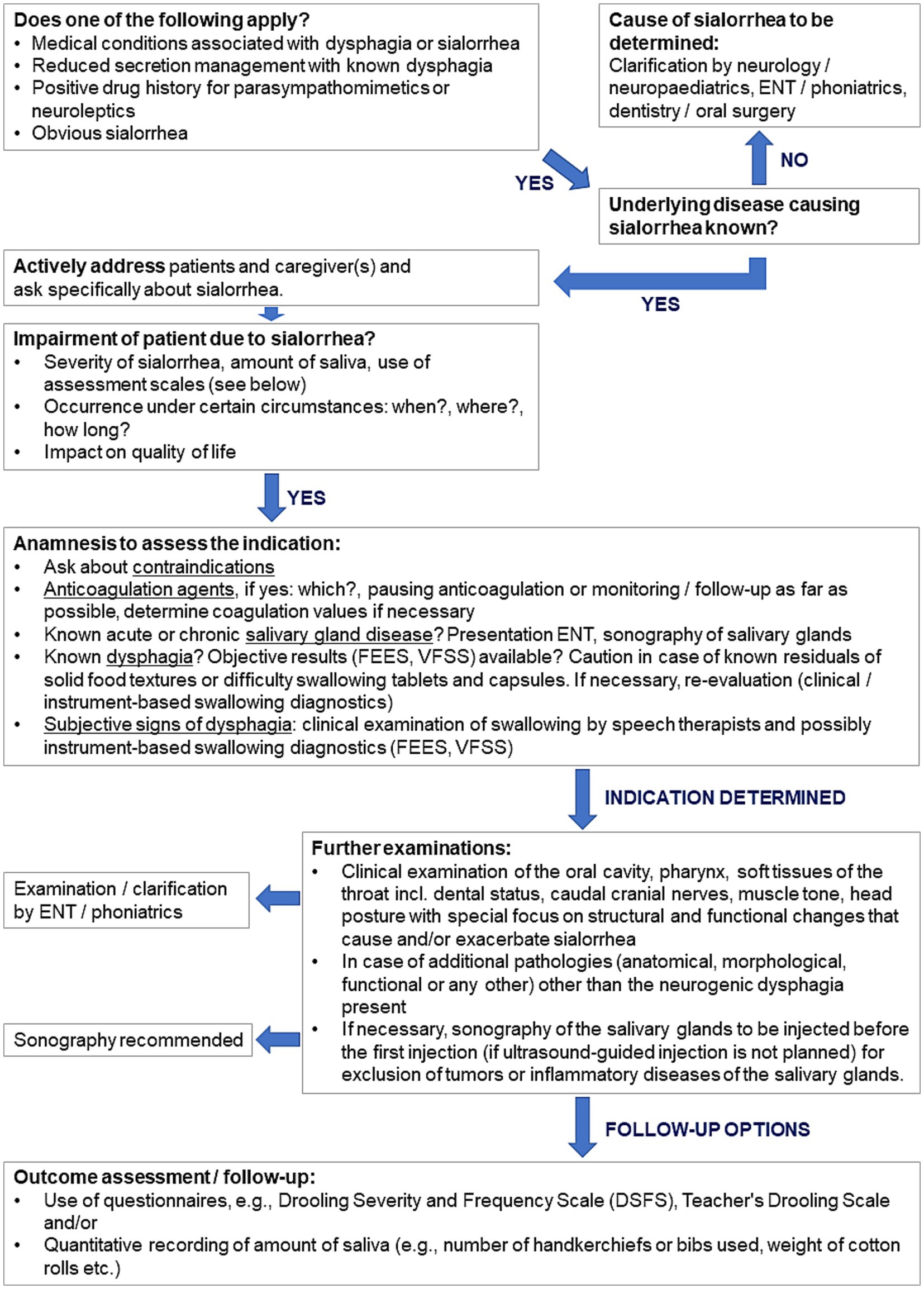
Figure 2. Flow chart for selection of patients for BoNT/A treatment. DSFS, Drooling Severity and Frequency Scale; ENT, Ear nose throat physician; FEES, flexible endoscopic evaluation of swallowing; VFSS, videofluoroscopic swallowing study.
4.2 Dosing recommendations
The approved total dose of IncoBoNT/A for the treatment of sialorrhea in adults is 100 units (reconstituted in 2 mL sterile saline 0.9%). This dose is distributed among the salivary glands in a pre-defined manner: the left and right parotid glands are injected with 30 units each (0.6 mL solution), and the left and right submandibular glands are injected with 20 units each (0.4 mL solution). The recommended time point for re-treatment is after 16 weeks, based on clinical trial experience (1).
For pediatric patients aged 2–17 years, dosing is weight-dependent and must be (re)calculated for each injection session. The dosing recommendations presented in Table 1 are based on the dosing scheme from the SIPEXI trial, where body weight-adapted dosing proved appropriate for reaching efficacy and safety goals. The recommended dosing scheme results in a total dose of around 2 U/kg body weight (3).
Both from a medical and a legal perspective, IncoBoNT/A (Xeomin®, Merz Pharmaceuticals GmbH, Germany) is recommended for treatment of sialorrhea, as it is currently the only approved BoNT/A product marketed for this indication.
4.3 Administration of BoNT/A injections and ultrasound guidance
As described above, an assessment of a patient’s suitability for BoNT/A injections, as well as the correct determination of the required dose are essential before treatment. As a next step, patients (and/or their caregivers) need to be informed and advised in detail about the potential benefits and risks of the treatment and about the actual procedure. Pain medication or sedation can be offered as necessary. The preparation of the BoNT/A solution must be performed according to the package leaflet.
Intraglandular injections of BoNT/A are performed transcutaneously into the paired parotid and submandibular glands, resulting in four injection sites among which the prescribed total dose is distributed. The transcutaneous route of administration has proved the safest option (45). As the parotid glands are larger than the submandibular glands (46, 47), they should be injected with a larger volume of IncoBoNT/A, as described above (14). The sublingual glands are not treated with BoNT/A due to their anatomic location and their minimal contribution to the overall amount of saliva produced.
While intraglandular injections can be performed using anatomical landmarks, the use of ultrasound guidance for a safe injection procedure is an important aspect of the latest treatment recommendations (48). It can minimize the risk of adverse events like swallowing difficulties due to local diffusion of the toxin into the floor of the mouth or pharyngeal musculature (6). This is of utmost importance in patients with sialorrhea, as they are often already dealing with the burden of their neurological disease. Sonographic guidance is mandatory when treating pediatric patients due to their smaller size and their variability in location. It is also highly recommended for treatment of adult patients. In the SIAXI trial, about half of the patients were injected with ultrasound guidance, which was optional in this trial. No difference in efficacy was seen between patients who received ultrasound guidance and those who did not (1). This indicates that orientation by anatomical landmarks may be sufficient to obtain a treatment effect. However, the results do not allow reliable conclusions regarding the difference in injection accuracy with and without sonographic needle guidance. This was explored in a small study with two injectors and six body donors, which showed a significantly higher injection accuracy for injections into the submandibular glands under ultrasound guidance; the difference was smaller for injections into the parotid glands (49). The submandibular glands are particularly difficult to inject due to their variation in size and due to their occasionally unexpected location in some patients (47). Thus, the German guideline “Hypersalivation” from the DGHNO-KHC (14) recommends sonographic guidance for effective and safe intraglandular injections of BoNT/A.
From a practical perspective, ultrasound needle guidance does not require high-end sonographic equipment. The authors recommend a linear ultrasonic transducer (from 7 MHz) as used for vascular sonography. The anatomic landmarks for the salivary glands are a useful starting point for localizing the glands by ultrasound and assessing their position and extent (48, 50). The landmark for finding the parotid glands is midway between the tragus and the angle of the jaw. Starting at the landmark about 2 cm below the mandible, midway between the mandibular angle and the tip of the chin, the submandibular gland is found dorsally toward the mandibular angle (51). The glands clearly contrast with the surrounding tissue due to their homogenous structure and clear demarcation. Once the gland is located, the ultrasound transducer should be placed centrally on the gland. The injection can be performed “in plane” (guiding the needle along the longitudinal axis of the transducer) or “off plane” (along the transverse axis). When injecting only one point, the needle is usually placed in the center of the gland and not near a duct; when injecting multiple times (usually no more than 2–3), the injection points are spaced appropriately across the gland. The transducer can be aligned horizontally or vertically during the injection and can be held at a slight angle to visualize the needle tip in the planned injection depth. The variability regarding the exact position of the parotid glands is low, allowing for similarly accurate injections with and without sonographic guidance. However, the position and size of the submandibular glands show notably more variability, making precise injections according to anatomical landmarks more difficult and potentially leading to injections at the edge or outside the gland. A schematic of the ultrasound procedure is shown in Figure 3.
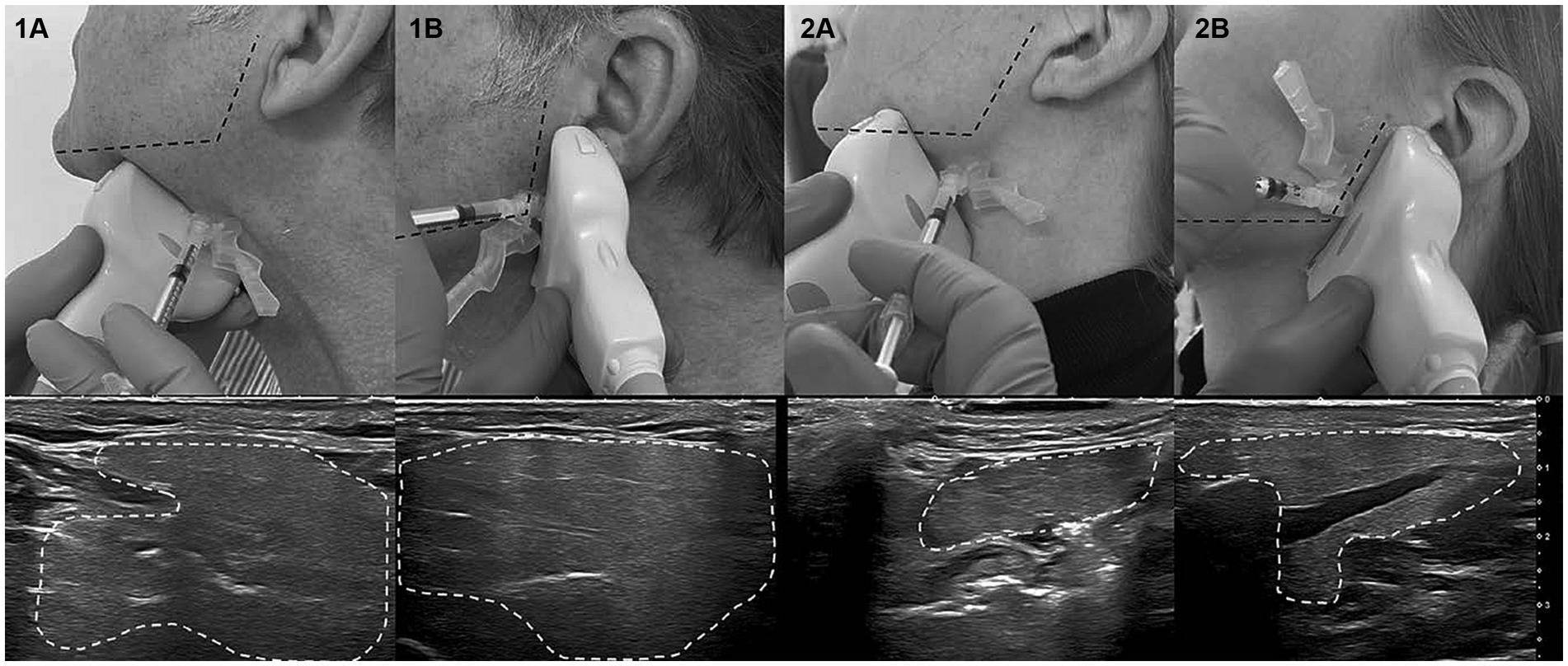
Figure 3. Demonstration of ultrasound-guided injection in subject 1 and 2 on the left side, respectively. (A) Submandibular gland, (B) Parotid gland. (Copyright Tobias Bäumer, Institute of Systemic Motor Science, CBBM, University of Lübeck).
4.4 Therapeutic goals and long-term benefits
The therapeutic goals for patients treated with BoNT/A for sialorrhea are highly individual, reflecting the heterogeneous patient population. The treating physician should discuss realistic goals with a patient and/or caregiver and agree on how to evaluate treatment outcomes. The overall goal is always the substantial reduction of sialorrhea, ideally decreasing salivary flow to a normal level. This has a direct impact on the extent of troublesome physical health issues, but also—and often most importantly—on quality of life. Patients and caregivers may experience social difficulties and stigmatization, embarrassment in public, and subsequent social withdrawal even within families. A reduction of (visible) hypersalivation can make a crucial difference regarding these aspects and can make situations like functional therapy sessions more comfortable. Furthermore, eating difficulties can be ameliorated, tracheostomy care can be facilitated, and aspiration pneumonia and skin maceration can be prevented. Thus, in essence, the improvements after BoNT/A treatment must be sufficiently large to lead to a notable improvement of patients’ everyday life.
A treatment effect can be expected within a week after IncoBoNT/A injections, the maximum effect is seen around 1 month after injection and the duration of effect is around 3 to 4 months (1). In cases where a short-term reduction of salivation is required, the time to effect may be bridged with careful use of anticholinergic medication (usually off-label).
Especially after a patient’s very first BoNT/A therapy session, close monitoring of treatment effects and possible side effects is advisable, e.g., by using questionnaires, patient diaries, or validated scales. For patients who experience notable benefits and improvements in their physical and psychosocial burden at the latest after the first two or three treatment sessions, a long-term re-treatment schedule should be developed. The results from the pivotal Phase III trials in adults and pediatric patients, which both included up to four treatment cycles, showed that IncoBoNT/A treatment effects increased with repeated injections (2, 3). In light of this evidence, physicians should neither immediately discontinue treatment nor increase the BoNT/A dose if the first cycle’s results disappointed. The authors recommend to re-inject with the planned dose and measure the effects over two or three cycles before evaluating the overall outcome. It can be challenging to convince patients and/or caregivers that this is useful, in particular if they experienced the injection procedure as stressful. In the long run, control visits should be scheduled around 4 months after injections to assess the need for re-treatment. From the authors’ clinical experience, it appears that re-injection intervals can be prolonged over time for many patients because treatment effects are sustained for longer, whereby the reason for this is not entirely clear yet.
Reliable outcome assessment tools are the foundation for all the above considerations. Improvements in quality of life are measurable by using standardized patient-reported outcome tools to follow-up with patients and/or their caregivers. In the authors’ experience, patient diaries are highly useful in theory but require high levels of compliance by the patient. A more direct assessment, also of the frequency of sialorrhea, can be performed by the treating physician using scales like the Teacher’s Drooling Scale (52), the Drooling Severity and Frequency Scale (DSFS) (53, 54), or a Global Impression of Change (GICS) assessment. These instruments can be administered at follow-up visits to examine the treatment effect or possible progression of sialorrhea. Direct measurements of amounts of saliva (e.g., by collecting and weighing fluid or soaked bibs/cotton rolls) are not used regularly in clinical practice due to their methodical weakness and difficulty of reproduction.
4.5 Safety aspects and troubleshooting
IncoBoNT/A treatment for sialorrhea is safe and well-tolerated with few side effects, as seen both in clinical trials and in clinical practice (1–3). The risk of side effects may be minimized by injecting with ultrasound guidance only, by using aspiration before injecting to avoid accidental application into a blood vessel, and by adhering to the recommended precautions and contraindications, as outlined above.
As laid out in the summary of product characteristics for IncoBoNT/A, possible side effects that can occur in connection with the injection procedure are local pain, inflammation, paresthesia, hematoma, and bleeding at the injection site. Pain or anxiety caused by the injection can lead to vasovagal reactions such as transient hypotension, nausea and syncope. Side effects that may occur in connection with the effects of IncoBoNT/A in adults with sialorrhea include dry mouth, dysphagia, paresthesia, speech disturbance, thickened saliva and subjective taste disturbance. Dysphagia occasionally occurs in children and adolescents. Thickened saliva, dry mouth, mouth pain and caries can also occur and should be taken into account. Some other typical issues that have been seen in clinical practice are outlined in this section, accompanied by the authors’ recommendations.
Patients may be disappointed by insufficient treatment effects. In such cases, it is advisable to perform several injection cycles at regular intervals and evaluate the outcomes after repeated treatments. If necessary, the BoNT/A dose may be gradually increased. The objective and subjective judgment of treatment effects can differ, and it is important to discuss realistic treatment goals with patients/caregivers before therapy starts. Treatment effects can be limited due to misplaced BoNT/A injections and sonographic needle guidance is also recommended for this reason. The patient’s underlying neurological condition may have deteriorated or progressed, leading to a worsening of symptoms that was not compensated for by BoNT/A. A secondary non-response to treatment due to the development of neutralizing antibodies to IncoBoNT/A was not observed in the clinical trials but cannot be ruled out as a rare (and potentially product-specific) cause of lack of treatment effect.
Patients may experience a dry mouth or xerostomia with highly viscous mucus. This can occur particularly in patients with tracheostomy tubes. Such cases require additional care to optimize salivary secretion management and provide relief. Fluid intake should be increased, oral care should be intensified (e.g., using creams, dexpanthenol sprays, glycerine sticks), and inhalation can be helpful, even in combination with a cough assist device or a vibrating vest in rare cases.
Patients may experience the occurrence or worsening of a swallowing disorder. In such cases, a potential progression of the underlying disease or newly emerging symptoms or diseases must be considered. Endoscopic swallowing diagnostics (FEES) are useful to determine such causes and to rule out the injection or diffusion of BoNT/A into the muscles of the floor of the mouth or pharynx as a causative factor. Changes in a dyskinetic movement disorder are also possible factors for changes in swallowing issues, particularly during child development phases, e.g., puberty. A decrease in BoNT/A dose should be considered if insufficient salivary flow is observed, leading to problems with food intake, due to potential over-treatment.
Patients may experience sialadenitis or mucositis of either infectious or non-infectious origin. Here, oral care must be intensified, analgesia can be offered, and antibiotic treatment or a consultation with an otorhinolaryngologist may be required.
Finally, patients may develop hematoma after injection. This must be monitored and, if possible, any ongoing anticoagulation therapy should be paused. After an event of post-injection hematoma, another occurrence should be prevented by compression of the injection site in the next treatment cycle.
The aim of the current dosing recommendations is a good balance between benefits and risks of BoNT/A treatment. If side effects are observed, physicians should lower the total dose and observe whether efficacy can still be achieved, while reducing adverse events. Based on clinical experience of the experts it may be considerable to start the treatment of adults by administering a total dose of 75 units instead of the recommended 100 units. Likewise, the total dose for pediatric patients can be lowered if clinically appropriate.
4.6 Comparison with other treatments
BoNT/A treatment for sialorrhea is a comparatively new therapeutic option. Other drugs have been used for years, mainly atropine, scopolamine, and glycopyrrolate, three antagonistic anticholinergics (17, 55–66). Of these, only glycopyrrolate is approved for sialorrhea treatment in pediatric patients with severe symptoms. The main issues with these systemic treatments concern their safety. They bear the risk of serious anticholinergic side effects, although glycopyrrolate has shown an acceptable safety profile without severe neurological complications. In randomized controlled trials, patients experienced a benefit from short-term use of glycopyrrolate and the safety risks were deemed acceptable (67, 68).
Invasive non-drug treatments like surgery are available, with their obvious disadvantages and risks. Surgical salivary gland interventions primarily include submandibulectomy and several forms of duct interruptions and ligatures, as well as relocation of the ducts of the large salivary glands. The latter requires careful consideration regarding a potentially increased risk of aspiration (53, 69–78). External radiation has been validated as another effective treatment option for sialorrhea (79–84), but its side effects and carcinogenic potential must be considered. Radiotherapy can reduce hypersalivation in cases where treatment with BoNT/A was not successful (85), and conversely, BoNT/A may be used for treatment of post-radiogenic hypersalivation (86). Other non-drug treatments like individualized functional therapy (e.g., swallowing training for patients with dysphagia), orthodontic treatments, or physiotherapy can also provide relief (87–91).
The main advantages of BoNT/A treatment over the abovementioned therapeutic options are first and foremost in the safety profile, in conjunction with good efficacy. BoNT/A is administered locally and acts directly in the salivary glands. This is an important advantage for patients for whom the systemic side effects of anticholinergics bear a high risk, including elderly patients with cognitive impairments, patient with hallucinations, children with intellectual disability, and patients with cardiovascular risk factors. In contrast to several techniques in swallowing programs, no therapy compliances or cognitive ability to perform the maneuvers are needed.
5 Conclusion
Chronic sialorrhea as a symptom of many neurological diseases can be a severe burden for patients and should receive adequate medical attention. It affects not only patients’ physical health but can severely impact quality of life by leading to social stigmatization, embarrassment, and withdrawal from social life. Previously available therapy options have shown only limited therapeutic success, for example due to patients’ lack of cooperation in swallowing therapy, persisting symptoms despite optimized drug therapy for Parkinson’s syndromes, or unacceptable side effects after the use of systemically acting anticholinergics, which are often used off-label.
A BoNT/A product has received medical approval for sialorrhea treatment of adults and children, giving physicians the possibility for application in a wide range of diseases. The approvals were based on results from two recent Phase III trials that showed that IncoBoNT/A is an effective and well-tolerated treatment for sialorrhea, also for repeated use. This confirms the benefits observed in previous smaller studies and in years of using BoNT/A off-label in clinical practice. It is recommended to perform the injections according to the approved dosing schemes, i.e., with 100 units of IncoBoNT/A, dissolved in 2 mL saline of 0.9% concentration and distributed among the paired parotid and submandibular glands, ideally using ultrasound guidance. When treating children, doses are determined according to body weight and ultrasound guidance is essential. BoNT/A treatment can lead to a clinically relevant decrease in sialorrhea and to meaningful improvements in quality of life. The long-lasting treatment effect supports good, long-term treatment adherence.
BoNT/A therapy for sialorrhea is highly individual and should be a multidisciplinary effort. In many cases, BoNT/A is the adequate first line treatment. The patient selection process for BoNT/A therapy is largely a diagnostic task to assess a patient’s risk factors and to determine the level of monitoring required during and after BoNT/A therapy. The group of patients who cannot be treated is comparably small. Treatment should be combined with other therapies like functional therapy, orthodontic treatments, or physiotherapy, depending on the individual patient’s needs. Especially important is the combination of BoNT/A treatment with intensive dysphagia therapy, with the latter supporting the diminishing effects of the injections in the intervals between BoNT/A treatment sessions. The combination of BoNT/A application and functional dysphagia therapy is rated highly useful by the experts editing this review and detailed assessments of such schemes in controlled trials would be valuable.
In summary, the authors of this review have outlined practical details of planning and executing BoNT/A treatment and provided recommendations based on their broad and longstanding experience. The aim of this review is to encourage and support physicians to use BoNT/A therapy and to achieve optimal therapeutic outcomes.
Author contributions
WJ: Writing – review & editing. TB: Writing – review & editing. AB: Writing – review & editing. UB: Writing – review & editing. CB: Writing – review & editing. MG: Writing – review & editing. OG-L: Writing – review & editing. RL: Writing – review & editing. SP: Writing – review & editing. CP: Writing – review & editing. ASc: Writing – review & editing. BS: Writing – review & editing. ASt: Writing – review & editing. BW: Writing – review & editing. MW: Writing – review & editing. SB: Writing – review & editing.
Funding
Merz Therapeutics supported the medical writing financially. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
The authors would like to thank Daniela Mueller at Cerner Enviza, Munich, Germany, for medical writing assistance.
Conflict of interest
The content of this review was created based on interdisciplinary consultations and cooperation with all authors and the consensus recommendations were developed during three working meetings. Merz Therapeutics GmbH supported these meetings financially but had no further influence on the recommendations and the content of this review. WJ is or was a consultant and speaker for AbbVie, Bial, Desitin, Kyowa Kirin, Stada, UCB, Zambon, Pharm Allergan, Ipsen Pharma, and Merz Therapeutics and was principal investigator of the SIAXI study. TB is a consultant for Merz Therapeutics and Pharm Allergan and a speaker for Merz Therapeutics, Pharm Allergan, and Ipsen. He received speaker and consultant fees from the Pelzerhaken Children’s Center, AbbVie/Allergan, Ipsen Pharma, and Merz Therapeutics. He received research grants from Deutsche Forschungsgemeinschaft (FG2698-2) and Ipsen Pharma. AB received consultant and speaker fees from Allergan/AbbVie, Merz Therapeutics, and Novartis. UB received consultant fees from Merz Therapeutics. CB received speaker and/or consultant fees from AbbVie, Bial, Desitin, Kyowa Kirin, Merz Therapeutics, STADA Pharm, TAD Pharma, UCB, and Zambon. MG received speaker and consultant fees from Merz Therapeutics, MSD, and Bayer Vital. OG-L received speaker and consultant fees from Merz Therapeutics, MEDICE, MEDEL, and Novartis. RL is a speaker for Merz Therapeutics. SP is or was a consultant for Bial, Idorsia, Ipsen, Merz Therapeutics, and TEVA and a speaker from AbbVie, Bayer, Bial, Ipsen, Merz Therapeutics, and Novartis. Furthermore, SP is or was involved in clinical studies (phase II and III) for Bayer, Ipsen, and Syneos Health. CP received honoraria as a speaker and/or consultant from AbbVie, Merz Therapeutics, InfectoPharm, and Olympus. ASc was a consultant and speaker for Allergan/AbbVie, Ipsen, Merz Therapeutics, Proveca, and Medice. ASt is a consultant and speaker for Merz Therapeutics, Inspire Medical, and ZOLL Respicardia. He received speaking honoraria and travel support from Intersect Medical and Clinigen. BW received speaker fees from AbbVie/Allergan, Takeda, Novartis, and Eisai. MW received honoraria as a speaker and/or consultant from AbbVie. SB received speaker fees from Merz Therapeutics, Ipsen Pharma, and Pharm Allergan and consultant fees from Merz Therapeutics and Ipsen Pharma. He was principal investigator of the SIPEXI study.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jost, WH, Friedman, A, Michel, O, Oehlwein, C, Slawek, J, Bogucki, A, et al. Siaxi: placebo-controlled, randomized, double-blind study of Incobotulinumtoxina for sialorrhea. Neurology. (2019) 92:e1982–91. doi: 10.1212/WNL.0000000000007368
2. Jost, WH, Friedman, A, Michel, O, Oehlwein, C, Slawek, J, Bogucki, A, et al. Long-term Incobotulinumtoxina treatment for chronic sialorrhea: efficacy and safety over 64 weeks. Parkinsonism Relat Disord. (2020) 70:23–30. doi: 10.1016/j.parkreldis.2019.11.024
3. Berweck, S, Bonikowski, M, Kim, H, Althaus, M, Flatau-Baqué, B, Mueller, D, et al. Placebo-controlled clinical trial of Incobotulinumtoxina for sialorrhea in children: Sipexi. Neurology. (2021) 97:e1425–36. doi: 10.1212/wnl.0000000000012573
4. Chaléat-Valayer, E, Porte, M, Buchet-Poyau, K, Roumenoff-Turcant, F, D'Anjou, MC, Boulay, C, et al. Management of Drooling in children with cerebral palsy: a French survey. Eur J Paediatr Neurol. (2016) 20:524–31. doi: 10.1016/j.ejpn.2016.04.010
5. Dashtipour, K, Bhidayasiri, R, Chen, JJ, Jabbari, B, Lew, M, and Torres-Russotto, D. Rimabotulinumtoxinb in sialorrhea: systematic review of clinical trials. J Clin Mov Disord. (2017) 4:9. doi: 10.1186/s40734-017-0055-1
6. Dogu, O, Apaydin, D, Sevim, S, Talas, DU, and Aral, M. Ultrasound-guided versus 'Blind' Intraparotid injections of botulinum toxin-a for the treatment of Sialorrhoea in patients with Parkinson's disease. Clin Neurol Neurosurg. (2004) 106:93–6. doi: 10.1016/j.clineuro.2003.10.012
7. Egevad, G, Petkova, VY, and Vilholm, OJ. Sialorrhea in patients with Parkinson's disease: safety and Administration of Botulinum Neurotoxin. J Parkinsons Dis. (2014) 4:321–6. doi: 10.3233/jpd-140379
8. Isaacson, SH, Ondo, W, Jackson, CE, Trosch, RM, Molho, E, Pagan, F, et al. Safety and efficacy of Rimabotulinumtoxinb for treatment of sialorrhea in adults: a randomized clinical trial. JAMA Neurol. (2020) 77:461–9. doi: 10.1001/jamaneurol.2019.4565
9. Mancini, F, Zangaglia, R, Cristina, S, Sommaruga, MG, Martignoni, E, Nappi, G, et al. Double-blind, placebo-controlled study to evaluate the efficacy and safety of botulinum toxin type a in the treatment of drooling in parkinsonism. Mov Disord. (2003) 18:685–8. doi: 10.1002/mds.10420
10. Martínez-Poles, J, Nedkova-Hristova, V, Escribano-Paredes, JB, García-Madrona, S, Natera-Villalba, E, Estévez-Fraga, C, et al. Incobotulinumtoxin a for sialorrhea in neurological disorders: a real-life experience. Toxins. (2018) 10:217. doi: 10.3390/toxins10060217
11. Mazlan, M, Rajasegaran, S, Engkasan, JP, Nawawi, O, Goh, KJ, and Freddy, SJ. A double-blind randomized controlled trial investigating the Most efficacious dose of botulinum toxin-a for sialorrhea treatment in Asian adults with neurological diseases. Toxins. (2015) 7:3758–70. doi: 10.3390/toxins7093758
12. Narayanaswami, P, Geisbush, T, Tarulli, A, Raynor, E, Gautam, S, Tarsy, D, et al. Drooling in Parkinson's disease: a randomized controlled trial of Incobotulinum toxin a and meta-analysis of botulinum toxins. Parkinsonism Relat Disord. (2016) 30:73–7. doi: 10.1016/j.parkreldis.2016.07.001
13. Ko, SH, Shin, YB, Min, JH, Shin, MJ, Chang, JH, Shin, YI, et al. Botulinum toxin in the treatment of drooling in tetraplegic patients with brain injury. Ann Rehabil Med. (2013) 37:796–803. doi: 10.5535/arm.2013.37.6.796
14. Steffen, A, Jost, W, Bäumer, T, Beutner, D, Degenkolb-Weyers, S, Groß, M, et al. Hypersalivation: update of the German S2k guideline (Awmf) in short form. J Neural Transm. (2019) 126:853–62. doi: 10.1007/s00702-019-02000-4
15. Jost, WH, Bäumer, T, Berweck, S, Laskawi, R, Spittau, B, Steffen, A, et al. Therapy of sialorrhea with botulinum toxin—an update. Fortschr Neurol Psychiatr. (2022) 90:222–32. doi: 10.1055/a-1802-3867
16. Jost, WH, Bäumer, T, Bevot, A, Birkmann, U, Buhmann, C, Grosheva, M, et al. Treatment of sialorrhea with botulinum neurotoxin type A—consensus practice recommendations for children and adults. Fortschr Neurol Psychiatr. (2022) 90:212–21. doi: 10.1055/a-1802-6006
17. Blasco, PA, and Allaire, JH. Drooling in the developmentally disabled: management practices and recommendations. Consortium on drooling. Dev Med Child Neurol. (1992) 34:849–62. doi: 10.1111/j.1469-8749.1992.tb11382.x
18. van Hulst, K, van den Engel-Hoek, L, Geurts, ACH, Jongerius, PH, van der Burg, JJW, Feuth, T, et al. Development of the drooling infants and Preschoolers scale (drips) and reference charts for monitoring saliva control in children aged 0-4 years. Infant Behav Dev. (2018) 50:247–56. doi: 10.1016/j.infbeh.2018.01.004
19. Verma, R, and Anand, KS. Botulinum toxin: a novel therapy for clozapine-induced Sialorrhoea. Psychopharmacology. (2018) 235:369–71. doi: 10.1007/s00213-017-4795-2
20. Kochhar, A, Larian, B, and Azizzadeh, B. Facial nerve and parotid gland anatomy. Otolaryngol Clin N Am. (2016) 49:273–84. doi: 10.1016/j.otc.2015.10.002
21. Pedersen, AML, Sørensen, CE, Proctor, GB, Carpenter, GH, and Ekström, J. Salivary secretion in health and disease. J Oral Rehabil. (2018) 45:730–46. doi: 10.1111/joor.12664
22. Proctor, GB, and Carpenter, GH. Salivary secretion: mechanism and neural regulation. Monogr Oral Sci. (2014) 24:14–29. doi: 10.1159/000358781
23. Holmberg, KV, and Hoffman, MP. Anatomy, biogenesis and regeneration of salivary glands. Monogr Oral Sci. (2014) 24:1–13. doi: 10.1159/000358776
24. Matsuo, R. Role of saliva in the maintenance of taste sensitivity. Crit Rev Oral Biol Med. (2000) 11:216–29. doi: 10.1177/10454411000110020501
25. Tabak, LA, Levine, MJ, Mandel, ID, and Ellison, SA. Role of salivary mucins in the protection of the Oral cavity. J Oral Pathol. (1982) 11:1–17. doi: 10.1111/j.1600-0714.1982.tb00138.x
26. Lakraj, AA, Moghimi, N, and Jabbari, B. Sialorrhea: anatomy, pathophysiology and treatment with emphasis on the role of botulinum toxins. Toxins. (2013) 5:1010–31. doi: 10.3390/toxins5051010
27. Edgar, WM. Saliva and dental health. Clinical implications of saliva: report of a consensus meeting. Br Dent J. (1990) 169:96–8. doi: 10.1038/sj.bdj.4807284
28. Rossetto, O, Pirazzini, M, Fabris, F, and Montecucco, C. Botulinum neurotoxins: mechanism of action. Handb Exp Pharmacol. (2021) 263:35–47. doi: 10.1007/164_2020_355
29. Xu, H, Shan, XF, Cong, X, Yang, NY, Wu, LL, Yu, GY, et al. Pre-and post-synaptic effects of botulinum toxin a on submandibular glands. J Dent Res. (2015) 94:1454–62. doi: 10.1177/0022034515590087
30. Bhatia, KP, Münchau, A, and Brown, P. Botulinum toxin is a useful treatment in excessive drooling in saliva. J Neurol Neurosurg Psychiatry. (1999) 67:697. doi: 10.1136/jnnp.67.5.697
31. Bushara, KO. Sialorrhea in amyotrophic lateral sclerosis: a hypothesis of a new treatment--botulinum toxin a injections of the parotid glands. Med Hypotheses. (1997) 48:337–9. doi: 10.1016/s0306-9877(97)90103-1
32. Jost, WH. Treatment of drooling in Parkinson's disease with botulinum toxin. Mov Disord. (1999) 14:1057. doi: 10.1002/1531-8257(199911)14:6<1057::aid-mds1033>3.0.co;2-4
33. George, KS, Kiani, H, and Witherow, H. Effectiveness of botulinum toxin B in the treatment of drooling. Br J Oral Maxillofac Surg. (2013) 51:783–5. doi: 10.1016/j.bjoms.2013.05.154
34. Giess, R, Naumann, M, Werner, E, Riemann, R, Beck, M, Puls, I, et al. Injections of botulinum toxin a into the salivary glands improve Sialorrhoea in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. (2000) 69:121–3. doi: 10.1136/jnnp.69.1.121
35. Ondo, WG, Hunter, C, and Moore, W. A double-blind placebo-controlled trial of botulinum toxin B for sialorrhea in Parkinson's disease. Neurology. (2004) 62:37–40. doi: 10.1212/01.wnl.0000101713.81253.4c
36. Langmore, SE, Schatz, K, and Olsen, N. Fiberoptic endoscopic examination of swallowing safety: a new procedure. Dysphagia. (1988) 2:216–9. doi: 10.1007/bf02414429
37. Holzapfel, K. “Radiologische Funktionsdiagnostik von Schluckstörungen,” in Schluckstörungen – Diagnostik und Rehabilitation. (Eds.) Bar-tolome G, Aufl. München: Elsevier. (2018). p. 123–149.
38. Murray, J, Langmore, SE, Ginsberg, S, and Dostie, A. The significance of accumulated oropharyngeal secretions and swallowing frequency in predicting aspiration. Dysphagia. (1996) 11:99–103. doi: 10.1007/bf00417898
39. Reynolds, J, Carroll, S, and Sturdivant, C. Fiberoptic endoscopic evaluation of swallowing: a multidisciplinary alternative for assessment of infants with dysphagia in the neonatal intensive care unit. Adv Neonatal Care. (2016) 16:37–43. doi: 10.1097/anc.0000000000000245
40. Rohrbach, S, and Gross, M. Transnasale Fiberoptisch-Endoskopische Schluckuntersuchung Bei Kindern. Monatsschr Kinderheilkd. (2014) 162:329–33. doi: 10.1007/s00112-014-3110-0
41. Schröter-Morasch, H, and Graf, S. Swallowing examination for Ent specialists. HNO. (2014) 62:324–34. doi: 10.1007/s00106-014-2844-2
42. Bader, CA, and Niemann, G. Dysphagia in Children with Cerebral Palsy--Fiberoptic-Endoscopic Findings. Laryngorhinootologie. (2010) 89:90–4. doi: 10.1055/s-0029-1237348
43. Olthoff, A, Carstens, PO, Zhang, S, von Fintel, E, Friede, T, Lotz, J, et al. Evaluation of dysphagia by novel real-time Mri. Neurology. (2016) 87:2132–8. doi: 10.1212/wnl.0000000000003337
44. Olthoff, A, Joseph, AA, Weidenmüller, M, Riley, B, and Frahm, J. Real-time Mri of swallowing: intraoral pressure reduction supports larynx elevation. NMR Biomed. (2016) 29:1618–23. doi: 10.1002/nbm.3621
45. Winterholler, MG, Erbguth, FJ, Wolf, S, and Kat, S. Botulinum toxin for the treatment of Sialorrhoea in Als: serious side effects of a transductal approach. J Neurol Neurosurg Psychiatry. (2001) 70:417–8. doi: 10.1136/jnnp.70.3.417
46. Ono, K, Morimoto, Y, Inoue, H, Masuda, W, Tanaka, T, and Inenaga, K. Relationship of the unstimulated whole saliva flow rate and salivary gland size estimated by magnetic resonance image in healthy young humans. Arch Oral Biol. (2006) 51:345–9. doi: 10.1016/j.archoralbio.2005.09.001
47. Scott, J. Age, sex and contralateral differences in the volumes of human submandibular salivary glands. Arch Oral Biol. (1975) 20:885–IN35. doi: 10.1016/0003-9969(75)90071-0
48. Jost, WH. The option of sonographic guidance in botulinum toxin injection for drooling in Parkinson's disease. J Neural Transm. (2016) 123:51–5. doi: 10.1007/s00702-015-1416-2
49. So, JI, Song, DH, Park, JH, Choi, E, Yoon, JY, Yoo, Y, et al. Accuracy of ultrasound-guided and non-ultrasound-guided botulinum toxin injection into cadaver salivary glands. Ann Rehabil Med. (2017) 41:51–7. doi: 10.5535/arm.2017.41.1.51
50. McGeachan, AJ, and CJ, MD. Management of Oral Secretions in neurological disease. Pract Neurol. (2017) 17:96–103. doi: 10.1136/practneurol-2016-001515
51. Loens, S, Bruggemann, N, Steffen, A, and Baumer, T. Localization of salivary glands for botulinum toxin treatment: ultrasound versus landmark guidance. Mov Disord Clin Pract. (2020) 7:194–8. doi: 10.1002/mdc3.12881
52. Camp-Bruno, JA, Winsberg, BG, Green-Parsons, AR, and Abrams, JP. Efficacy of benztropine therapy for drooling. Dev Med Child Neurol. (1989) 31:309–19. doi: 10.1111/j.1469-8749.1989.tb04000.x
53. Crysdale, WS, and White, A. Submandibular duct relocation for drooling: a 10-year experience with 194 patients. Otolaryngol Head Neck Surg. (1989) 101:87–92. doi: 10.1177/019459988910100114
54. Thomas-Stonell, N, and Greenberg, J. Three treatment approaches and clinical factors in the reduction of drooling. Dysphagia. (1988) 3:73–8. doi: 10.1007/bf02412423
55. De Simone, GG, Eisenchlas, JH, Junin, M, Pereyra, F, and Brizuela, R. Atropine drops for drooling: a randomized controlled trial. Palliat Med. (2006) 20:665–71. doi: 10.1177/0269216306071702
56. Hyson, HC, Johnson, AM, and Jog, MS. Sublingual atropine for sialorrhea secondary to parkinsonism: a pilot study. Mov Disord. (2002) 17:1318–20. doi: 10.1002/mds.10276
57. Matos Santana, TE, Capurso, NA, Ranganathan, M, and Yoon, G. Sublingual atropine in the treatment of clozapine-induced sialorrhea. Schizophr Res. (2017) 182:144–5. doi: 10.1016/j.schres.2016.10.039
58. Bachrach, SJ, Walter, RS, and Trzcinski, K. Use of glycopyrrolate and other anticholinergic medications for sialorrhea in children with cerebral palsy. Clin Pediatr. (1998) 37:485–90. doi: 10.1177/000992289803700805
59. Banfi, P, Ticozzi, N, Lax, A, Guidugli, GA, Nicolini, A, and Silani, VA. Review of options for treating sialorrhea in amyotrophic lateral sclerosis. Respir Care. (2015) 60:446–54. doi: 10.4187/respcare.02856
60. Blissit, KT, Tillery, E, Latham, C, and Pacheco-Perez, J. Glycopyrrolate for treatment of clozapine-induced sialorrhea in adults. Am J Health-Syst Pharm. (2014) 71:1282–7. doi: 10.2146/ajhp130636
61. Lee, ZI, Yu, KJ, Lee, DH, Hong, SK, Woo, SB, Kim, JM, et al. The effect of nebulized glycopyrrolate on posterior drooling in patients with brain injury: two cases of different brain lesions. Am J Phys Med Rehabil. (2017) 96:e155–8. doi: 10.1097/phm.0000000000000669
62. Man, WH, Colen-de Koning, JC, Schulte, PF, Cahn, W, van Haelst, IM, Doodeman, HJ, et al. The effect of glycopyrrolate on nocturnal sialorrhea in patients using clozapine: a randomized, crossover, double-blind placebo-controlled trial. J Clin Psychopharmacol. (2017) 37:155–61. doi: 10.1097/jcp.0000000000000657
63. Mier, RJ, Bachrach, SJ, Lakin, RC, Barker, T, Childs, J, and Moran, M. Treatment of sialorrhea with glycopyrrolate: a double-blind, Dose-Ranging Study. Arch Pediatr Adolesc Med. (2000) 154:1214–8. doi: 10.1001/archpedi.154.12.1214
64. Praharaj, SK, Munoli, RN, and Sharma, PS. Low-dose glycopyrrolate for clozapine-associated sialorrhea. J Clin Psychopharmacol. (2014) 34:392. doi: 10.1097/jcp.0000000000000102
65. Qurashi, I, Chu, S, Drake, R, Hartley, V, Chaudhry, I, Deakin, JFW, et al. Glycopyrrolate in comparison to hyoscine hydrobromide and placebo in the treatment of hypersalivation induced by clozapine (Gothic1): a feasibility study. Pilot Feasibility Stud. (2019) 5:79. doi: 10.1186/s40814-019-0462-1
66. Parr, JR, Weldon, E, Pennington, L, Steen, N, Williams, J, Fairhurst, C, et al. The drooling reduction intervention trial (Dri): a single blind trial comparing the efficacy of Glycopyrronium and hyoscine on drooling in children with Neurodisability. Trials. (2014) 15:60. doi: 10.1186/1745-6215-15-60
67. Zeller, RS, Davidson, J, Lee, HM, and Cavanaugh, PF. Safety and efficacy of glycopyrrolate Oral solution for Management of Pathologic Drooling in Pediatric patients with cerebral palsy and other neurologic conditions. Ther Clin Risk Manag. (2012) 8:25–32. Epub 2012/02/03. doi: 10.2147/TCRM.S27362
68. Zeller, RS, Lee, HM, Cavanaugh, PF, and Davidson, J. Randomized phase iii evaluation of the efficacy and safety of a novel glycopyrrolate Oral solution for the Management of Chronic Severe Drooling in children with cerebral palsy or other neurologic conditions. Ther Clin Risk Manag. (2012) 8:15–23. Epub 2012/02/03. doi: 10.2147/tcrm.S26893
69. Becmeur, F, Schneider, A, Flaum, V, Klipfel, C, Pierrel, C, and Lacreuse, I. Which surgery for drooling in patients with cerebral palsy? J Pediatr Surg. (2013) 48:2171–4. doi: 10.1016/j.jpedsurg.2013.06.017
70. Bekkers, S, Pruijn, IMJ, van der Burg, JJW, van Hulst, K, Kok, SE, Delsing, CP, et al. Surgery versus botulinum neurotoxin a to reduce drooling and improve daily life for children with neurodevelopmental disabilities: a randomized controlled trial. Dev Med Child Neurol. (2021) 63:1351–9. doi: 10.1111/dmcn.14924
71. Formeister, EJ, Dahl, JP, and Rose, AS. Surgical Management of Chronic Sialorrhea in Pediatric patients: 10-year experience from one tertiary care institution. Int J Pediatr Otorhinolaryngol. (2014) 78:1387–92. doi: 10.1016/j.ijporl.2014.06.005
72. Katona, G, Csákányi, Z, Lorincz, A, and Gerlinger, I. Bilateral submandibular duct relocation by high-frequency radiosurgery. Eur Arch Otorhinolaryngol. (2008) 265:1103–8. doi: 10.1007/s00405-008-0604-1
73. Kok, SE, van der Burg, JJ, van Hulst, K, Erasmus, CE, and van den Hoogen, FJ. The impact of submandibular duct relocation on drooling and the well-being of children with neurodevelopmental disabilities. Int J Pediatr Otorhinolaryngol. (2016) 88:173–8. doi: 10.1016/j.ijporl.2016.06.043
74. Mankarious, LA, Bottrill, ID, Huchzermeyer, PM, and Bailey, CM. Long-term follow-up of submandibular duct rerouting for the treatment of sialorrhea in the Pediatric population. Otolaryngol Head Neck Surg. (1999) 120:303–7. doi: 10.1016/s0194-5998(99)70266-4
75. Martin, TJ, and Conley, SF. Long-term efficacy of intra-Oral surgery for sialorrhea. Otolaryngol Head Neck Surg. (2007) 137:54–8. doi: 10.1016/j.otohns.2007.01.034
76. Noonan, K, Prunty, S, Ha, JF, and Vijayasekaran, S. Surgical Management of Chronic Salivary Aspiration. Int J Pediatr Otorhinolaryngol. (2014) 78:2079–82. doi: 10.1016/j.ijporl.2014.09.008
77. Reed, J, Mans, CK, and Brietzke, SE. Surgical Management of Drooling: a meta-analysis. Arch Otolaryngol Head Neck Surg. (2009) 135:924–31. doi: 10.1001/archoto.2009.110
78. Uppal, HS, De, R, D'Souza, AR, Pearman, K, and Proops, DW. Bilateral submandibular duct relocation for drooling: an evaluation of results for the Birmingham Children's hospital. Eur Arch Otorhinolaryngol. (2003) 260:48–51. doi: 10.1007/s00405-002-0516-4
79. Andersen, PM, Grönberg, H, Franzen, L, and Funegård, U. External radiation of the parotid glands significantly reduces drooling in patients with motor neurone disease with bulbar paresis. J Neurol Sci. (2001) 191:111–4. doi: 10.1016/s0022-510x(01)00631-1
80. Assouline, A, Levy, A, Abdelnour-Mallet, M, Gonzalez-Bermejo, J, Lenglet, T, Le Forestier, N, et al. Radiation therapy for hypersalivation: a prospective study in 50 amyotrophic lateral sclerosis patients. Int J Radiat Oncol Biol Phys. (2014) 88:589–95. doi: 10.1016/j.ijrobp.2013.11.230
81. Borg, M, and Hirst, F. The role of radiation therapy in the Management of Sialorrhea. Int J Radiat Oncol Biol Phys. (1998) 41:1113–9. doi: 10.1016/s0360-3016(98)00153-9
82. Neppelberg, E, Haugen, DF, Thorsen, L, and Tysnes, OB. Radiotherapy reduces sialorrhea in amyotrophic lateral sclerosis. Eur J Neurol. (2007) 14:1373–7. doi: 10.1111/j.1468-1331.2007.01983.x
83. Postma, AG, Heesters, M, and van Laar, T. Radiotherapy to the salivary glands as treatment of sialorrhea in patients with parkinsonism. Mov Disord. (2007) 22:2430–5. doi: 10.1002/mds.21752
84. Weikamp, JG, Schinagl, DA, Verstappen, CC, Schelhaas, HJ, de Swart, BJ, and Kalf, JG. Botulinum toxin-a injections vs radiotherapy for drooling in Als. Acta Neurol Scand. (2016) 134:224–31. doi: 10.1111/ane.12559
85. Hawkey, NM, Zaorsky, NG, and Galloway, TJ. The role of radiation therapy in the Management of Sialorrhea: a systematic review. Laryngoscope. (2016) 126:80–5. doi: 10.1002/lary.25444
86. Steffen, A, Wollenberg, B, Schönweiler, R, Brüggemann, N, and Meyners, T. Drooling following radiation. Botulinum toxin as a successful treatment modality. HNO. (2011) 59:115–7. doi: 10.1007/s00106-010-2232-5
87. Bartolome, G. “Grundlagen der funktionellen Dysphagietherapie (FDT),” in Schluckstörungen - Diagnostik und Rehabilitation. (Eds.) Bartolome G, Schröter-Morasch H, Hrsg. München-Jena: Urban & Fischer. (2018). p. 261–402.
88. Carnaby, G, Hankey, GJ, and Pizzi, J. Behavioural intervention for dysphagia in acute stroke: a randomised controlled trial. Lancet Neurol. (2006) 5:31–7. doi: 10.1016/s1474-4422(05)70252-0
89. Hinchey, JA, Shephard, T, Furie, K, Smith, D, Wang, D, and Tonn, S. Formal dysphagia screening protocols prevent pneumonia. Stroke. (2005) 36:1972–6. doi: 10.1161/01.STR.0000177529.86868.8d
90. Hussein, I, Kershaw, AE, Tahmassebi, JF, and Fayle, SA. The Management of Drooling in children and patients with mental and physical disabilities: a literature review. Int J Paediatr Dent. (1998) 8:3–11. doi: 10.1046/j.1365-263x.1998.00055.x
Keywords: sialorrhea, botulinum toxin, botulinum neurotoxin type A, BoNT/A, IncobotulinumtoxinA, hypersalivation, quality of life, practice recommendations
Citation: Jost WH, Bäumer T, Bevot A, Birkmann U, Buhmann C, Grosheva M, Guntinas-Lichius O, Laskawi R, Paus S, Pflug C, Schroeder AS, Spittau B, Steffen A, Wilken B, Winterholler M and Berweck S (2023) Botulinum neurotoxin type A in the interdisciplinary treatment of sialorrhea in adults and children—update and practice recommendations. Front. Neurol. 14:1275807. doi: 10.3389/fneur.2023.1275807
Edited by:
Domenico Antonio Restivo, University of Messina, ItalyReviewed by:
Marcello Esposito, Hospital Antonio Cardarelli, ItalyRaymond Lotilla Rosales, University of Santo Tomas, Philippines
Copyright © 2023 Jost, Bäumer, Bevot, Birkmann, Buhmann, Grosheva, Guntinas-Lichius, Laskawi, Paus, Pflug, Schroeder, Spittau, Steffen, Wilken, Winterholler and Berweck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfgang H. Jost, dy5qb3N0QHBhcmtpbnNvbi1rbGluaWsuZGU=