 Mariana Melo Moreira1*
Mariana Melo Moreira1* Marta Carriço2
Marta Carriço2 Manuel Luís Capelas1,3
Manuel Luís Capelas1,3 Nuno Pimenta3,4,5
Nuno Pimenta3,4,5 Teresa Santos3,6
Teresa Santos3,6 Susana Ganhão-Arranhado3,7,8
Susana Ganhão-Arranhado3,7,8 Antti Mäkitie3,9,10,11
Antti Mäkitie3,9,10,11 Paula Ravasco3,12,13
Paula Ravasco3,12,13- 1Universidade Católica Portuguesa, Faculty of Health Sciences and Nursing (FCSE), Lisboa, Portugal
- 2Champalimaud Foundation, Nutrition Service of Champalimaud Clinical Center, Lisbon, Portugal
- 3Universidade Católica Portuguesa, Center for Interdisciplinary Research in Health (CIIS), Lisbon, Portugal
- 4Polytechnic Institute of Santarém, Sport Sciences School of Rio Maior, Rio Maior, Portugal
- 5Sport Physical Activity and Health Research and Innovation Center (SPRINT), Santarém Polytechnic University, Rio Maior, Portugal
- 6Faculdade de Ciências Sociais e Tecnologia, Universidade Europeia de Lisboa, Lisbon, Portugal
- 7Atlântica, Instituto Universitário, Barcarena, Portugal
- 8CINTESIS, Centre for Health Technology and Services Research, Porto, Portugal
- 9Department of Otorhinolaryngology-Head and Neck Surgery, Helsinki University Hospital and University of Helsinki, Helsinki, Finland
- 10Research Program in Systems Oncology, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 11Division of Ear, Nose and Throat Diseases, Department of Clinical Sciences, Intervention and Technology, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden
- 12Universidade Católica Portuguesa, Católica Medical School, Rio de Mouro, Portugal
- 13Center for Interdisciplinary Research Egas Moniz, Egas Moniz School of Health & Science, Almada, Portugal
Introduction: The effectiveness of the supplementation of prebiotics, probiotics and synbiotics as a therapeutic approach in colorectal cancer (CRC) remains unclear. The aim of this systematic review is to critically examine the current scientific evidence on the impact of modulating the microbiota, through the use of prebiotics, probiotics and synbiotics, in patients diagnosed with CRC undergoing treatment, to determine the potential therapeutic use of this approach.
Methods: This systematic review was made according to the PRISMA 2020 guidelines. Inclusion criteria were randomized controlled trials (RCT) comparing the impact of pre-, pro-, or synbiotic supplementation with placebo or standard care in patients with CRC undergoing treatment. Exclusion criteria were non-human studies, non-RCTs, and studies in languages other than English or Portuguese. Six databases were consulted, namely, Cochrane Library, Pubmed, Scopus, Cinahl, MedicLatina and Web of Science until May of 2023. RAYYAN software was used to manage the search results and risk of bias was assessed according to the guidelines of the Cochrane Collaboration using the Rob 2.0 tool.
Results: Twenty-four RCTs met the inclusion criteria and were included in this review. Administration of pre-, pro-, or synbiotics improved surgical outcomes such as the incidence of infectious and non-infectious postoperative complications, return to normal gut function, hospital length of stay, and antibiotic usage. The supplementation of these microorganisms also alleviated some symptoms from chemotherapy and radiotherapy, mainly diarrhea. Evidence on the best approach in terms of types of strains, dosage and duration of intervention is still scarce.
Conclusions: Pre-, pro-, and synbiotics supplementation appears to be a beneficial therapeutic approach in CRC treatment to improve surgical outcomes and to alleviate side-effects such as treatment toxicity. More RCTs with larger sample sizes and less heterogeneity are needed to confirm these potential benefits and to determine the best strains, dosage, and duration of administration in each situation.
Systematic review registration: https://www.crd.york.ac.uk/prospero, identifier CRD42023413958.
1 Introduction
According to GLOBOCAN, in 2022, colorectal cancer (CRC) ranked as the third most diagnosed cancer, with over 1.9 million new cases, and the second most deadly malignancy causing roughly 904,000 deaths. This accounted for 9.3% of cancer-related deaths (1). GLOBOCAN also estimates that by 2040 the burden of CRC will rise to 3.2 million new cases and 1.6 million deaths with most cases predicted to occur in developing countries with the numbers increasing along with the increase of the Human Development Index. Conversely, in highly developed countries, where the screening is now a routine, numbers are expected to stabilize or even decline (2, 3).
Surgery stands as the primary treatment for CRC, but chemotherapy and radiotherapy are also commonly used as neoadjuvant or adjuvant treatments. These approaches often lead to several side-effects such as postoperative infectious complications, diarrhea, vomiting, nausea, etc. (4–6). More recently, immunotherapy and targeted therapy have emerged as viable options in select cases (5, 7).
The etiology of CRC is multifactorial, involving genetic factors, epigenetic alterations, and environmental factors such as being overweight, smoker, heavy drinker and following an unhealthy diet (8–10). More recently, the development of CRC has also been associated with chronic inflammation, immune system dysfunction, and dysbiosis. Dysbiosis is the compositional and functional alteration caused by an imbalance between symbiotic and opportunistic microbiomes. It can be categorized in three types: loss of beneficial microbes, expansion of pathogenic microbes, and loss of microbial diversity (11, 12).
Over the past decade, the relationship between the gut microbiota and CRC has gained significant attention with studies showing that patients with CRC harbor a distinct microbiota composition compared to healthy control subjects (3, 13). These studies show that CRC patients’ microbiota has lower bacterial diversity, lower abundance of commensal bacteria such as Akkermansia muciniphila, Lactobacillus rhamnosus and Bifidobacterium breve, and higher abundance of pro-carcinogenic bacteria such as Fusobacterium nucleatum, Escherichia coli, Bacteroides fragilis, Streptococcus gallolyticus and Peptostreptococcus anaerobius (3, 10, 13, 14). Studies have also shown that butyrate-producing bacteria are less represented in CRC patients. Butyrate is a short-chain fatty acid with very important health-promoting and antineoplastic properties such as being the main energy source for colonocytes, maintaining the mucosal barrier integrity, reducing pro-inflammatory cytokines, and inducing apoptosis (9, 15, 16).
The microbiota has been studied not only as a potential risk factor for CRC but also as a therapeutic approach in the treatment of this malignancy through its modulation with pre-, pro-, and synbiotics (17, 18). Prebiotics are defined as a non-digestible food ingredient that promote changes in the composition and/or activity of the microbiota conferring health benefits to the host (3). On the other hand, according to the most accepted definition and the one proposed by the expert panel convened by the International Scientific Association of Probiotics and Prebiotics in 2014, probiotics are “live microorganisms which, when administered in an adequate amount, confer a health benefit to the host” (19). The most commonly used strains are from the Lactobacillus, Bifidobacterium, Streptococcus and Enterococcus genera (10, 14). When prebiotics and probiotics are administered together, in a way that prebiotics promote the growth and survival of probiotics, it’s called a synbiotic (20, 21).
Recent studies indicate that modulating the microbiota, through the supplementation of pre-, pro-, or synbiotics, appears to have an impact on CRC treatment. This can be due to the reduction of postoperative infectious and non-infectious complications and side-effects of chemotherapy and radiotherapy or even directly on the efficacy of the drugs used in chemotherapy or, more recently, on the sensitivity to immunotherapy (12, 22, 23).
While some systematic reviews have delved into this area (24–31), the majority focused on only one treatment for CRC, or one outcome and some results appear to be contradictory. To overcome these previous limitations, the aim of this systematic review is to critically examine the present scientific evidence, including more recent findings, on the impact of modulating the microbiota, through the use of pre-, pro-, and synbiotics, in CRC patients undergoing treatment. This is also performed to determine the potential therapeutic use of this approach.
2 Materials and methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (32) and was registered in the PROSPERO database (registration number CRD42023413958).
2.1 Literature search
This systematic review was conducted in six databases, namely, Cochrane Library, Pubmed, Scopus, Cinahl, MedicLatina and Web of Science, until May 2023. The MESH terms or equivalents and search terms for title and abstract were selected according to the Population, Intervention, Comparison, Outcome and Study (PICOS) model. The MESH terms used for the Pubmed database are shown in Table 1. The search strategy for the databases is shown in detail in Appendix 1. The results were filtered to identify studies in the English or Portuguese language. The references of the selected studies were also scanned to identify additional studies missed in the initial search.
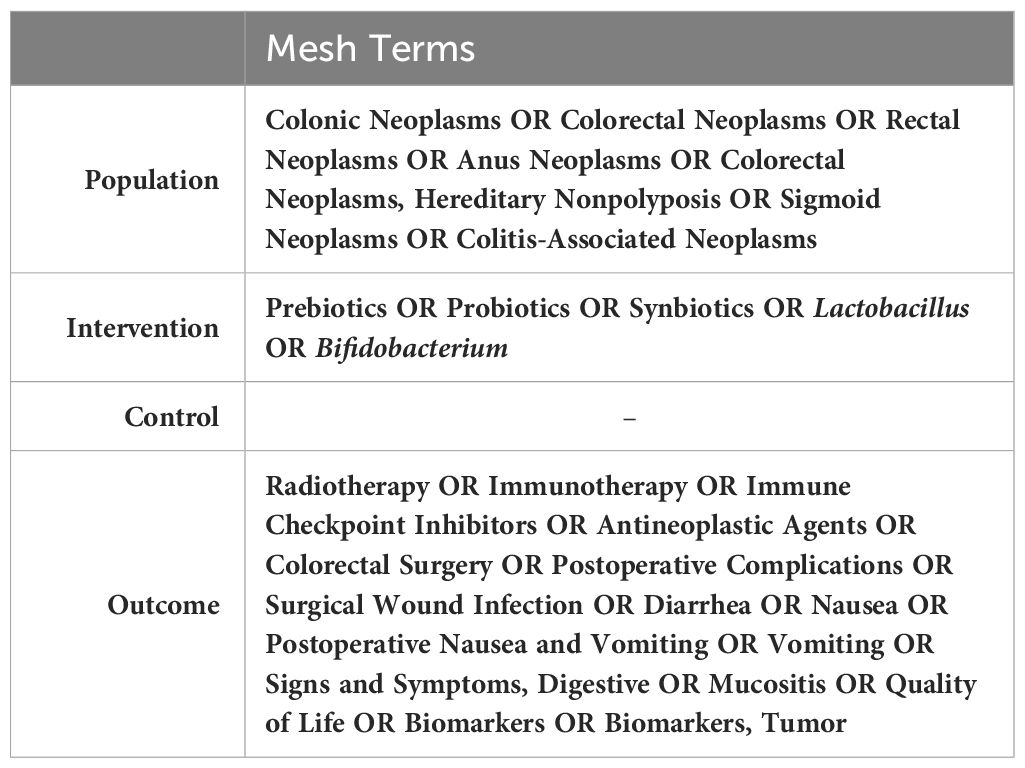
Table 1 Mesh terms used for research in Pubmed database.
2.2 Inclusion and exclusion criteria
The inclusion criteria were based on the PICOS model. The selected population comprised patients diagnosed with CRC (colon cancer or rectal cancer), the intervention was the supplementation with pre-, pro-, or synbiotics. The considered control treatment was placebo or standard care, the primary outcomes were the impact of this intervention on the efficacy, toxicity, or side-effects of treatments such as chemotherapy, radiotherapy, surgery or immunotherapy and the studies selected were randomized controlled studies.
The exclusion criteria were studies in languages other than English or Portuguese, studies where the population were patients with other types of cancer and studies where the intervention wasn’t exclusively the supplementation of prebiotics, probiotics or synbiotics.
2.3 Study selection
The studies obtained from the initial search were uploaded to the RAYYAN software and were analyzed and selected by two independent reviewers (MM and MC). The articles were screened by title and abstract and then full text of relevant studies were retrieved and assessed based on the inclusion and exclusion criteria. Disagreements in study selections were resolved by discussion between the two reviewers.
2.4 Data extraction
Data such as author, publication year, participant, placebo, and intervention details and outcomes were extracted from articles considered eligible and compiled in a summary table.
2.5 Risk of bias assessment
The risk of bias of all included studies was assessed through the RoB 2.0 tool, according to the guidelines of the Cochrane Collaboration (33), using Review Manager Software (Revman Web 5.5 - online). Risk of bias was assessed in the following domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other bias. The risk of bias was then classified as high, low, or unclear risk.
3 Results
3.1 Study selection
A total of 2308 studies were obtained from the initial search through six databases, namely, Cochrane Library, Pubmed, Scopus, CINAHL, MedicLatina and Web of Science. These results were uploaded to the RAYYAN software, and the duplicates were identified (n = 784). After the duplicates were removed, 1524 articles remained and were screened by title and abstract. Afterwards, 1480 articles were excluded for reasons such as being non-human studies, being reviews or case reports or not being relevant to this review. The remaining 44 studies were full text screened for eligibility and 24 studies were included in this review. The other 20 studies were excluded because they did not meet the inclusion criteria or were unavailable in full-text format. The studies that did not meet the inclusion criteria are shown in Appendix 2. The PRISMA flow diagram, shown in Figure 1, summarizes the selection process.
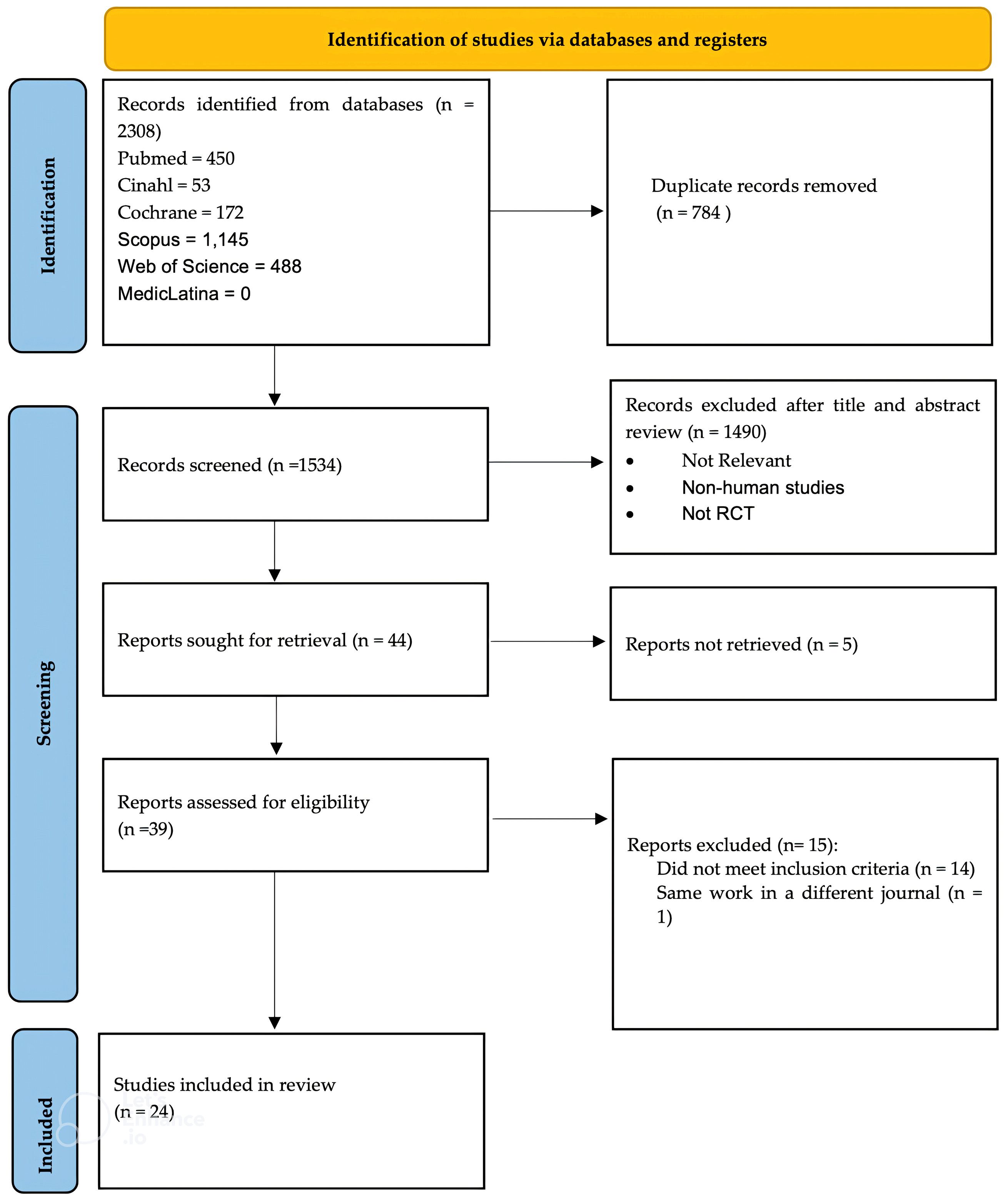
Figure 1 PRISMA flowchart that summarizes the screening and selection process.
3.2 Description of the selected studies
The 24 studies included in this review were all randomized controlled studies. The year of publication ranged from 2007 to 2023, where approximately 70% of the studies were published in the last 10 years. In terms of geographic localization the included studies are from China (n=6) (34–39), Turkey (n=2) (40, 41), Slovenia (n=2) (42, 43), Japan (n=2) (44, 45), Greece (n=2) (46, 47), Brazil (n=2) (48, 49), Iran (n=2) (50, 51), Malaysia (n=1) (52), Finland (n=1) (53), Sweden (n=1) (54), Slovakia (n=1) (55), Republic of Korea (n=1) (56) and Bosnia and Herzegovina (n=1) (57). There were a total of 2204 participants, 1139 in the intervention groups and 1065 in the control groups. Of these, 1220 participants were male, 984 were female, and their age ranged from 19 to 92 years. Considering the intervention, 11 out of the 24 studies used a mixture of probiotics (34–39, 46, 52, 55–57), 8 used synbiotics (42, 43, 45, 47–51), 3 used a single probiotic (44, 53, 54) and 2 studies used Kefir (40, 41). Species of the Lactobacillus, Bifidobacterium and Enterococcus genera were the most commonly used for the probiotics or synbiotics intervention. Placebo was used for the control group in 18 of the studies (34–42, 46–50, 52, 54–56) while the other 6 used standard care treatment (43–45, 51, 53, 57). Characterization of these studies is shown in Table 2.
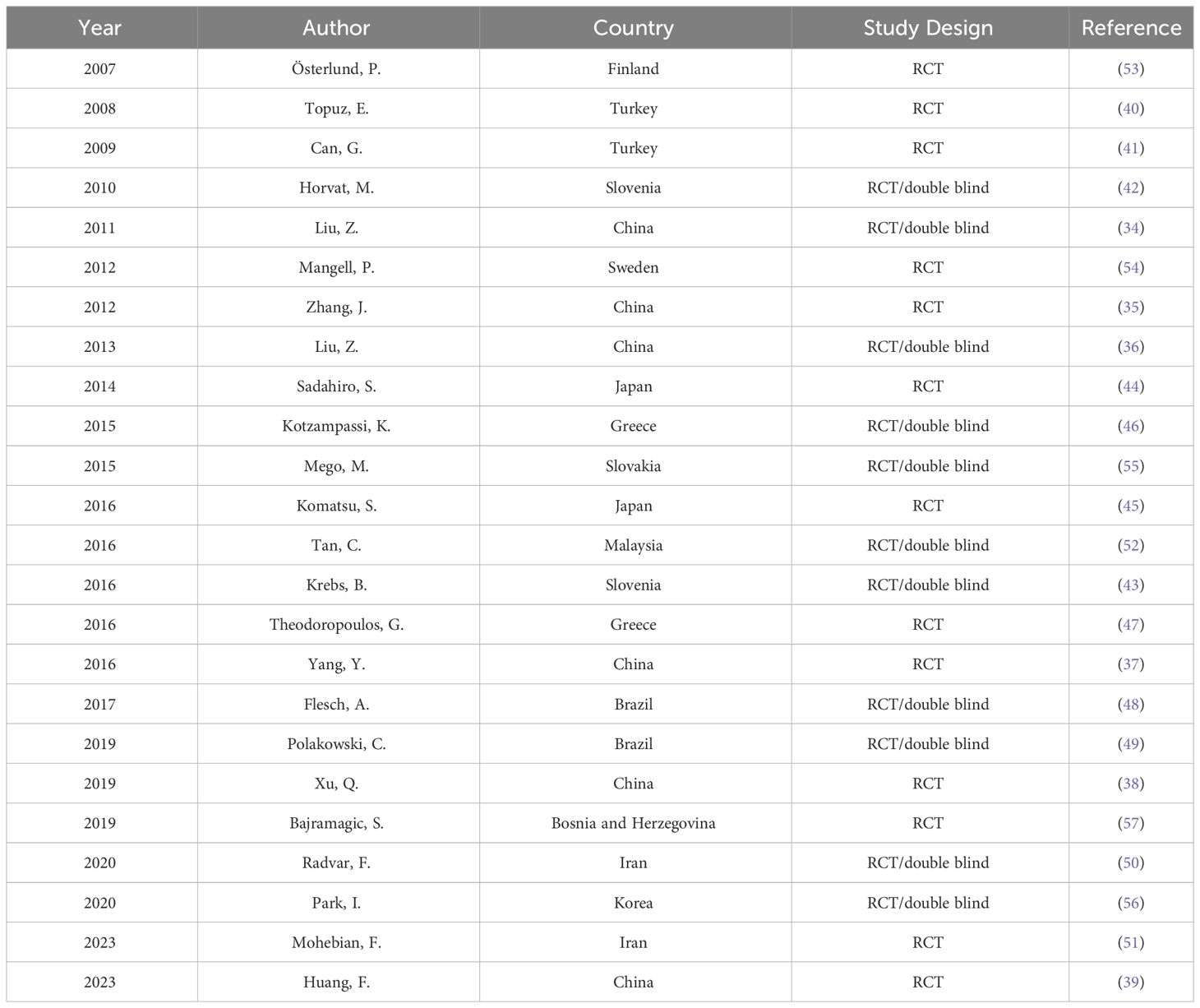
Table 2 Characteristics of the 24 included studies.
3.3 Risk of bias assessment
The summary results of the risk-of-bias assessment are shown in Figure 2. All studies included in this review were randomized but 7 studies failed to mention how the randomization was done (35, 38–40, 43, 54, 57). Therefore, there is an unclear risk of bias in this parameter and in 1 study randomizations were performed by one of the authors leading to a high risk of bias (44). In terms of allocation concealment, 7 studies had an unclear risk of bias as there was no clear description if allocation was concealed until the beginning of the intervention (38–41, 43, 44, 57). Ten studies presented a high risk of bias in the performance domain because participants and/or personnel weren’t blinded during the intervention (38–41, 43–45, 51, 53, 57). Blinding of outcome assessment risk was unclear in 8 studies (38–41, 43, 44, 51, 57) and high in 2 studies (45, 53) while incomplete data outcome risk was unclear in only 2 of the studies (38, 43). Nineteen of the studies were considered to have an unclear risk in terms of selective reporting (35, 37–45, 48–52, 54–57) and 2 studies were considered to have a high risk of other bias because they were ended prematurely before full recruitment of participants was completed (46, 55).
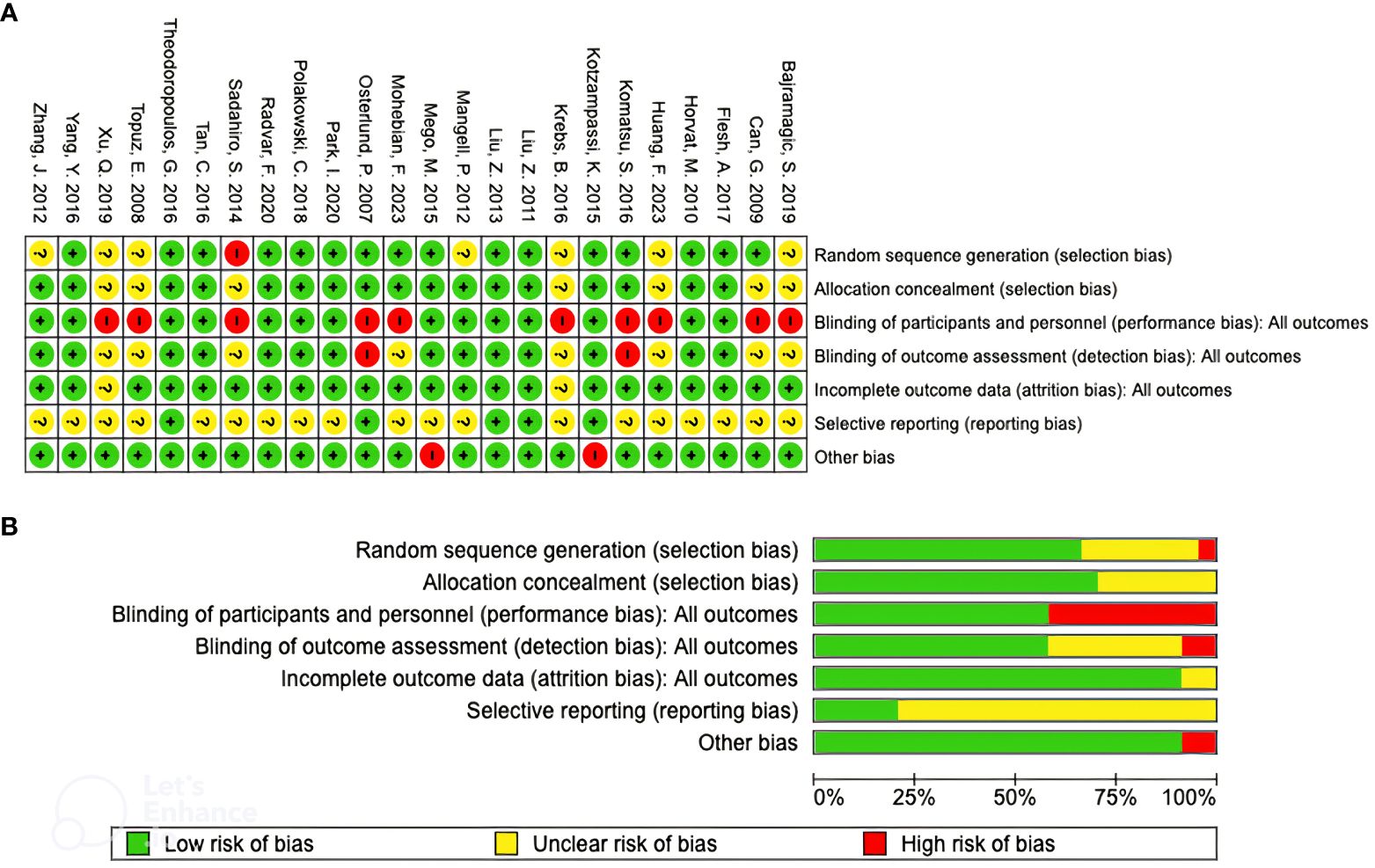
Figure 2 Risk of bias summary (A) and risk of bias assessment graph (B).
3.4 Outcomes
Out of the 24 included studies, 17 evaluated the impact of probiotics or synbiotics supplementation in colorectal cancer surgery (34–38, 42–49, 52, 54, 56, 57) while the remaining 7 studied the impact on treatment with chemotherapy (39–41, 50, 51, 53, 55). One study selected patients undergoing chemoradiotherapy so outcomes on the impact of this approach in treatment with radiotherapy was also assessed (50). None of the studies evaluated the impact of probiotics or synbiotics supplementation in CRC patients undergoing immunotherapy.
3.4.1 Surgery
The impact of probiotics or synbiotics supplementation in CRC patients undergoing surgery treatment was assessed in 17 studies (34–38, 42–49, 52, 54, 56, 57). Details from each study are shown in Table 3. Six studies used synbiotics for the intervention (42, 43, 45, 47–49), 9 used a mixture of probiotics strains (34–38, 46, 52, 56, 57) and 2 studies used a single strain in the intervention (44, 54). The administration of the probiotic/synbiotic was done pre-operatively in 6 studies (35, 38, 42, 43, 49, 52), pre- and post-operatively in 8 studies (34, 36, 37, 44, 45, 48, 54, 56) and 3 studies focused on the post-operative period (46, 47, 57). Considering control groups, 4 studies used standard care (43–45, 57) while the remaining 13 used placebo (34–38, 42, 46–49, 52, 54, 56).
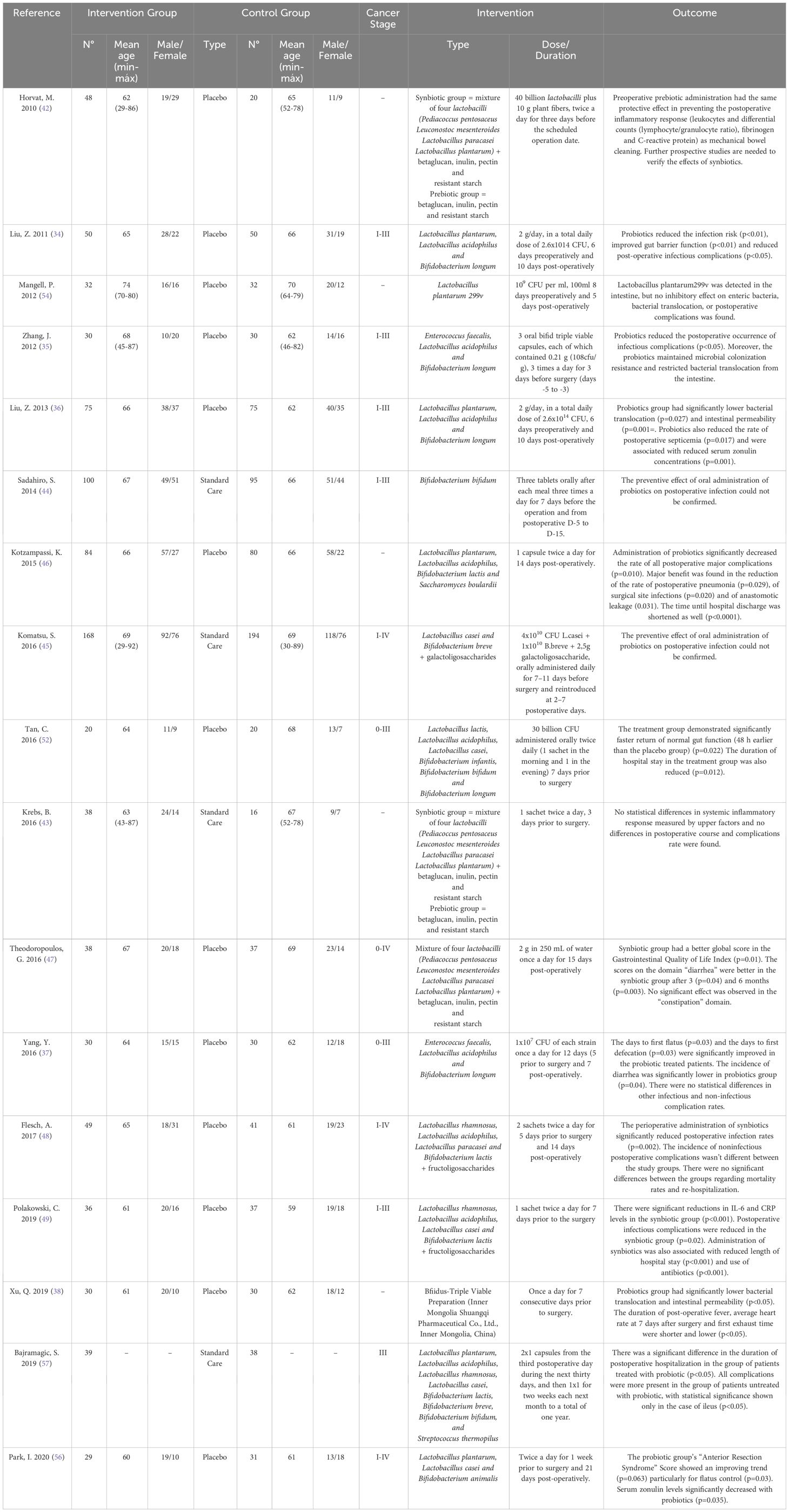
Table 3 Details of the included studies that assessed the impact on surgery outcomes.
3.4.1.1 Post-operative complications
Fourteen studies (34–37, 43–46, 48, 49, 52, 54, 56, 57) assessed the incidence of post-operative infectious complications such as wound infection, septicemia, and pneumonia. Among them, 9 studies (34–37, 46, 48, 49, 56, 57) reported that the supplementation of probiotics or synbiotics could decrease the incidence of post-operative infectious complications, with significant results being observed in all but 2 of the studies (37, 57). Additionally, 5 studies (43–45, 52, 54) found no differences between the intervention and the control group.
In a study by Flesch et al., where the intervention group took synbiotics for 5 days before surgical procedure and for 14 days after surgery, it was observed that only one patient in the synbiotics group presented surgical wound infection, while 9 such cases were diagnosed in the control group (p=0.002). Furthermore, there was a significant difference between groups in relation to other infectious complications such as intra-abdominal abscess (n=3) and pneumonia (n=4) in the control group and no cases in the synbiotics group (p=0.001) (48).
A study by Liu et al., where patients received a mixture of probiotics for 6 days preoperatively and 10 days post-operatively, also reported a significant difference in postoperative infectious complications between the intervention and the control group, being the incidence of post-operative septicemia 73% in the control group and 55% in the probiotics group (p= 0.017) (36). In contrast, Komatsu et al. reported no statistical differences in postoperative infectious complications between the intervention and control group where synbiotics were administered from day 7 to day 11 before surgery and reintroduced from day 2 to day 7 postoperative (45). Mangell et al. also noted a higher number of complications in the placebo compared with the intervention group, where an administration of a single strain for 8 days preoperatively and 5 days postoperative was performed, although, this difference did not reach statistical significance (54). Four studies (34, 36, 38, 56) demonstrated a lower bacterial translocation and intestinal permeability in the intervention group and 2 of the studies reported lower zonulin levels which is used as a biomarker of impaired gut function barrier (36, 56).
Regarding non-infectious postoperative complications such as diarrhea, ileus, and anatomic leakage, 8 studies (34, 36–38, 46, 49, 56, 57) indicated that the supplementation of probiotics and synbiotics could decrease their incidence, with all studies showing statistically significant results but one (49). Additionally, 1 study (48) found no statistical difference between the intervention and the control group when considering non-infectious complications.
A study by Yang et al. reported a lower incidence of diarrhea in the intervention group (26.7%) compared to the placebo (53.3%) (p=0.035), after administration of probiotics for 12 days (5 prior to surgery and 7 postoperatively). The results concerning anastomotic leakage and abdominal distension were essentially quite comparable between the 2 groups (37).
Similarly, Bajramagic et al. also reported a lower number of non-infectious complications in the intervention group after administration of probiotics for 30 days starting on day 3 postoperative, but this difference was only statistically significant for ileus development (57).
Another study, where the intervention group received a mixture of probiotics for 6 days preoperatively and 10 days post-operatively, also observed a significant lower incidence of non-infectious complications, compared with the placebo group: diarrhea (10% vs. 30%, p< 0.05), abdominal cramping (26% vs. 38%, p< 0.05) and distension (22% vs. 36%, p< 0.05), and a shorter duration of pyrexia (>38.5°C) (5.9 days vs. 7.2 days, p< 0.05) (34).
Polakowski et al. also evaluated the incidence of postoperative non-infectious complications after synbiotic supplementation, for 7 days prior to surgery. Even though the incidence was higher in the control group, it did not reach statistical significance (p=0.42) (49).
Conversely, in the study by Flesch et al. the incidence of non-infectious postoperative complications such as nausea, vomiting, abdominal distension, ileus, diarrhea or constipation was not different between the study groups (p=0.161) (48).
3.4.1.2 Return to normal gut function
Nine studies (34, 37, 42, 43, 46, 47, 52, 54, 56) evaluated the time to return to normal gut function. Six studies (34, 37, 46, 47, 52, 56) found that the supplementation of probiotics or synbiotics could significantly improve the return to normal gut function, and other 3 studies (42, 43, 54) found some improvements in the intervention group, but the results did not reach statistical difference.
A study by Tan et al., where the intervention group received a mixture of probiotics for 7 days prior to surgery, demonstrated a significantly earlier return of normal gut function compared to the placebo group (108.5 h vs. 156.5 h respectively, p=0.022) (52).
Another study reported a significant improvement in the days to first flatus (3.63 ± 0.67 days in the placebo group versus 3.27 ± 0.58 days in the probiotics group, p = 0.0274) and the days to first defecation (4.53 ± 1.11 days in the placebo group versus 3.87 ± 1.17 days in the probiotics group, p = 0.0268), after probiotics administration for 12 days (5 prior to surgery and 7 postoperative) (37).
In a study by Liu et al. a shorter time to first defecation when comparing the supplementation of a mixture of probiotics for 6 days preoperatively and 10 days post-operatively to placebo (3.3 days vs. 4.2 days, p< 0.05) was reported (34).
Horvat et al. demonstrated that patients receiving synbiotics and prebiotics twice a day for 3 days prior to surgery, passed flatus and stool after the operation earlier than the control. However, this difference did not reach statistical difference (2.3 days with synbiotics, 2.2 with prebiotics, and 2.5 days in the control, p=0.41) (42).
3.4.1.3 Hospital length of stay
Eleven studies (34–37, 42, 43, 46, 48, 49, 52, 57) assessed the length of hospital stay after surgery. While 7 studies (36, 42, 43, 46, 49, 52, 57) found that the supplementation of probiotics or synbiotics could decrease the duration of hospital stay [significantly except for 2 studies (42, 43)], another 4 studies (34, 35, 37, 48) found no statistical difference between the intervention and the control group.
One study, where patients received probiotics for 7 days prior to surgery, the length of hospital stay was shorter for the intervention group in comparison to the placebo group (6.5 vs. 13 days, p=0.012) (52). Another study, where synbiotic supplementation was also administered for 7 days prior to surgery, reported a shorter length of hospitalization in the synbiotic group compared with the placebo group [3.0 (3-5) days, vs. 4.0 (3-21) days (p <0.001)] (49).
In contrast the study by Zhang et al. did not find differences in length of stay after probiotics administration for 3 days prior to surgery (35) contrary to studies by Krebs et al. (43) and Flesch et al. (48) that reported a shorter length of stay in the intervention groups, although they did not reach statistical significance.
3.4.1.4 Usage of antibiotics
In terms of use of antibiotics, 2 studies (36, 49) found that the supplementation of probiotics or synbiotics could decrease the duration of antibiotic usage, and another 2 studies (34, 37) found no statistical difference between the intervention and the control group. Specifically, the study by Liu et al. reported a shorter duration of antibiotic therapy in the probiotics group compared with the control (5.69 vs. 7.29 days, p=0.001) (36). In agreement to Liu et al., Polakowski et al. also reported a shorter duration of antibiotic usage in the synbiotic group compared to the placebo group (1.42 vs. 3.74, p<0.001) (49). Contrary to these results, studies by Liu et al. and Yang et al. did not find significant differences in length of antibiotic therapy between the intervention and control groups (34, 37).
3.4.2 Chemotherapy
Seven studies (39–41, 50, 51, 53, 55) assessed the effect of probiotics or synbiotics supplementation in CRC patients undergoing chemotherapy treatment. Details from each study are shown in Table 4. One study used synbiotics for the intervention group (50), 3 used a mixture of probiotics strains (39, 51, 55), 2 studies used kefir and one study used a single strain in the intervention group (53). For the control group, 2 studies used standard of care (51, 53), while the remaining 5 used some type of placebo (39–41, 50, 55).
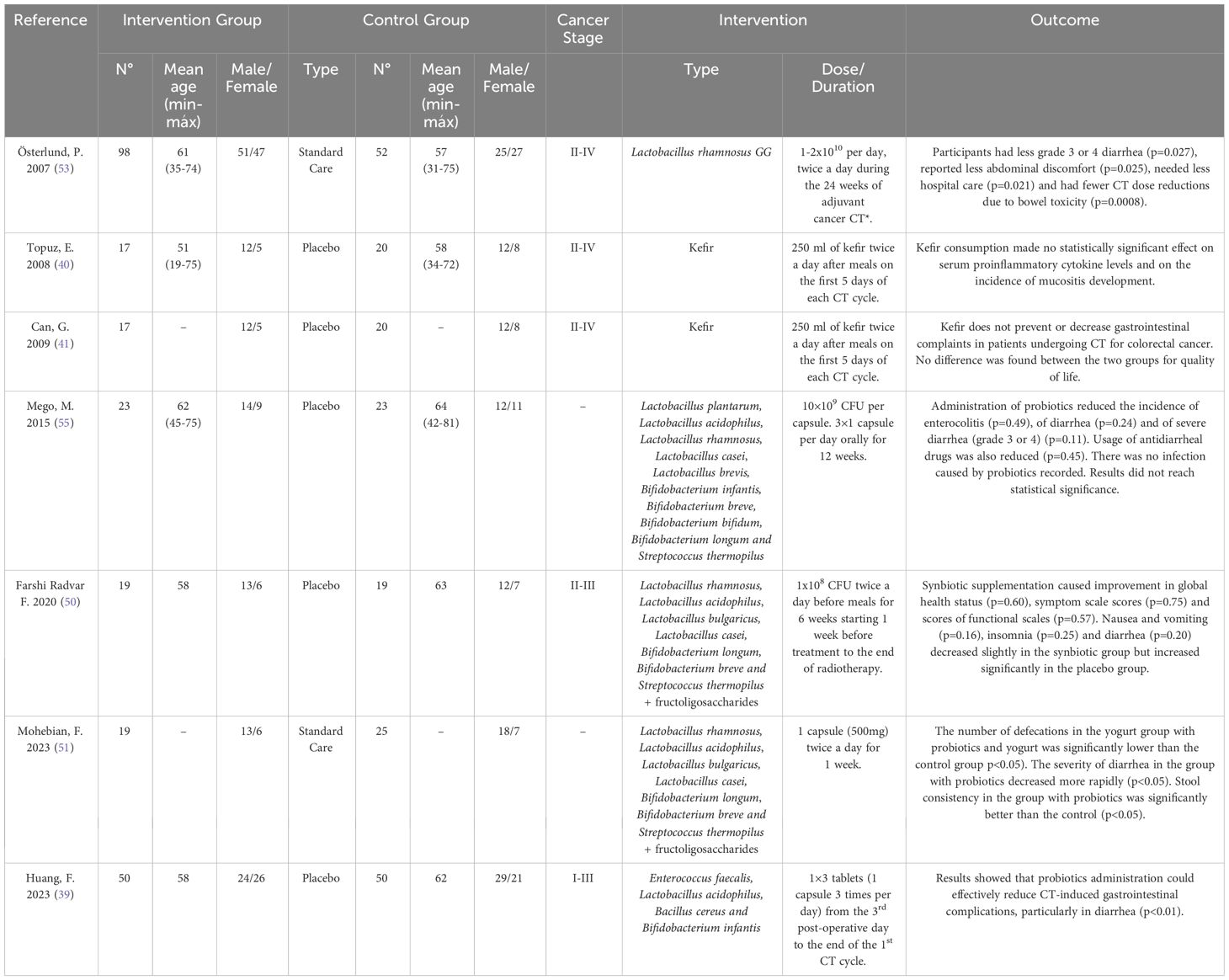
Table 4 Details of the included studies that assessed the impact on chemotherapy and radiotherapy outcomes.
The impact of probiotics or synbiotics supplementation on the incidence of diarrhea was assessed in all studies but one (40). Significant improvement of this side-effect was reported in 3 of the following studies: (1) Österlund et al. reported a lower incidence of diarrhea grade 3 – 4 in patients who received Lactobacillus rhamnosus twice a day for the 24 weeks of adjuvant chemotherapy (22% vs 37%, p=0.027) (53), comparing to the placebo group; (2) Mohebian et al. noted a lower severity of diarrhea and improved stool consistency in patients who took a mixture of probiotics twice a day for one week (51); and (3) Huang et al. also demonstrated a lower incidence of diarrhea in patients who received probiotics from day 3 postoperative to the end of the first neoadjuvant chemotherapy cycle, in a total of 6 weeks (16% vs. 40%, p=0,008) (39). Mego et al. also observed a lower incidence of overall diarrhea and lower incidence of grade 3 – 4 diarrhea when probiotics were administered 3 times a day for 12 weeks, however, these results did not reach statistical difference when compared to the placebo (0% vs. 17.4% p=0.11 and 39.1% vs. 60.9% p=0.24 respectively) (55). In contrast, a study by Can et al., where 250ml of kefir was consumed during the first 5 days of each chemotherapy cycle, reported that this intervention did not prevent diarrhea but increased constipation (41).
Besides lower incidence of diarrhea, the study by Huang et al. also reported, when compared to placebo, lower incidences of abdominal pain (6% vs 24%, p=0.025), abdominal distension (10% vs 28%, p=0.041) and constipation (8% vs 28%, p=0.019) in the group who took probiotics (39). Furthermore, Österlund et al. also demonstrated a lower abdominal discomfort resulting from flatulence and less abdominal distension in patients who took Lactobacillus rhamnosus (2% vs. 12%, p=0,025). This study also showed statistical significance for less chemotherapy-dose reductions due to bowel toxicity (21% vs 47%, p=0,008) in the intervention group (53). Accordingly, Farshi Radvar et al. demonstrated that synbiotic administration for 6 weeks, starting one week before chemoradiotherapy, decreased the incidence of symptoms such as nausea, vomiting, appetite loss and diarrhea, even though these results weren’t statistically significant, the placebo group has significant increases in these symptoms (50).
One study assessed the impact of kefir supplementation on mucositis development and reported no preventive effect of supplementation during the first 5 days of each chemotherapy cycle (40).
3.4.3 Radiotherapy
Farshi Radvar et al. assessed the impact of synbiotics supplementation during radiotherapy, in rectal cancer patients undergoing neoadjuvant chemoradiotherapy. All of the participants received pelvic radiotherapy 5 times a week for 5 to 6 weeks and an intravenous dose of chemotherapy daily for 5 days in the beginning and at the end of radiotherapy. Participants in the intervention group took synbiotics for 6 weeks starting 1 week before beginning chemoradiotherapy. Quality of life was assessed through the European Organization for Cancer Research and Treatment of Cancer’s 30-item quality of life questionnaire version 3.0 which is composed of 3 scales: global health status, functional scale, and symptom scale (50, 58).
The results showed that, in terms of global health status, the synbiotic group had a higher improvement (69.73 to 74.12; p=0.39) compared to the control group (68.42 to 68.85; p=0.96) but the results weren’t of statistical significance (p=0.60). No improvements were observed in the functional scale but the synbiotic group had a decrease in the overall mean of the symptom scale (18.45 to 16.95; p=0.56) while the control group had an increase (21.37 to 24.88; p=0.29), although the results showed no statistical significance between the 2 groups (p=0.22). Particularly, nausea and vomiting (4.38 to 3.50; p=0.71) and diarrhea (33.33 to 26.31; p=0.49) decreased slightly in the synbiotic group and increased [(10.52 to 17.54; p=0.17), and (45.51 to 57.89; p=0.27) respectively] in the placebo group. This study also evaluated the quality of life in both groups, showing that the synbiotic group had a bigger increase in this parameter compared to the placebo group, but no statistically significant difference was reached (69.73 to 74.12 vs. 68.42 to 68.85, p=0.60) (50).
4 Discussion
CRC treatment has evolved in recent years, yet the accompanying side-effects still significantly impact patients’ quality of life and prognosis (6, 59). For this reason, it remains imperative to explore solutions that may decrease the occurrence of associated toxicity and complications in order to achieve a more successful outcome (4). In the present systematic review, we aimed to critically examine the current scientific evidence on the impact of pre-, pro-, and synbiotics used for modulating the microbiota, in CRC patients undergoing treatment, and to determine the potential therapeutic use of such approach.
Gut microbiota, specifically dysbiosis, has been associated with the development and progression of CRC (60). Specific bacteria such as Fusobacterium nucleatum, Escherichia coli, Bacteroides fragilis, Streptococcus gallolyticus and Peptostreptococcus anaerobius are frequent in CRC patients and have been linked with its development in various studies. Studies show that dysbiosis and the presence of these bacteria may alter the inflammatory, genomic, and metabolic processes in the host in a way that promotes carcinogenesis through different mechanisms such as the ability to induce DNA damage, interference with the DNA damage repair, impact on signaling pathways and immune suppression (60–63). Dysbiosis has also been observed in cancer patients undergoing immunotherapy and chemotherapy and has been associated with the efficacy of these treatments and their gastrointestinal toxicity and side-effects (62, 64). Consequently, gut microbiota modulation, in order to restore gut microbiota balance, through pre-, pro- and synbiotics has been studied as a potential therapeutic agent, potentiating cancer treatment effect or preventing and managing treatment-related toxicity or complications (65, 66).
Surgery remains the primary treatment for nearly all CRC patients. Although effective, surgery can lead to postoperative infectious or non-infectious complications that may impact prognosis (67, 68). In this systematic review, studies showed that the probiotics and synbiotics supplementation can have a role in reducing the incidence of postoperative complications. However, some evidence remains contradictory, and no conclusions can be drawn regarding the optimal formulation, duration and dosage of the intervention. Studies with shorter intervention duration and those using only one strain of probiotics appeared to yield less significant results (43, 44, 54), suggesting that a mixture of probiotic strains for a longer period of time may be more effective to reduce the incidence of postoperative complications. Accordingly, the following three systematic reviews and meta-analyses reported that the supplementation of probiotics and synbiotics can reduce the incidence of postoperative complications in CRC patients: (1) Chen et al. reported that probiotic or synbiotic administration significantly reduced the risk of developing postoperative infectious complications by 37% (RR = 0.63; 95%CI: 0.54–0.74) (28); (2) Veziant et al. reported that there were significantly fewer infectious complications in the probiotic or synbiotic group (RR = 0.59; 95%CI: 0.47–0.75) (29); (3) Araújo et al. reported that probiotic supplementation reduced the incidence of surgical site infection (OR = 0.53; 95%CI: 0.36 - 0.78) (31). These systematic reviews and meta-analyses also highlight that more evidence is needed regarding which strains of probiotics to use and what is the ideal intervention duration.
Probiotics and synbiotics may also facilitate a faster return to normal gut function, reduce hospital length of stay and decrease antibiotics usage after surgery, as evidenced by the majority of studies (34, 36, 37, 46, 47, 49, 52, 56, 57). However, three studies showed no significant results and (42, 43, 48) other two showed no difference between the control and intervention groups (35, 37). The heterogeneity between studies, considering sample size and type, dosage and duration of the intervention may explain the differences between the results. A systematic review and meta-analysis by Amitay et al. reported that perioperative probiotics/synbiotics administration was associated with faster return to normal gut function, shorter postoperative antibiotics use, and shorter length of hospital stay (30). Zeng et al. also reported a shorter duration of antibiotic therapy but found no statistical differences in hospital length of stay (26) whereas An et al. concluded that probiotics may result in little to no difference in hospital length of stay after colorectal cancer surgery (69).
Both chemotherapy and radiotherapy can lead to several toxicity-related side-effects. Their dose or intensity reductions may thus be necessary, which in turn can result in less efficient outcome. In the past years, studies and systematic reviews have reported that gut modulation interventions can reduce the incidence of cancer treatment-related side-effects such as diarrhea and mucositis. However, most studies have included several types of cancers and not only CRC patients, which weakens conclusions, as results cannot be extrapolated (70–72).
This systematic review includes all studies that assessed the impact of probiotic or synbiotic supplementation in chemotherapy or radiotherapy exclusively in CRC patients. It was found that these interventions may have a potential role in alleviating gastrointestinal symptoms and overall quality of life of these patients (39, 50, 51, 53). Two studies using kefir in the intervention group, reported no improvements, as so kefir may not be an effective approach (40, 41). One study found no statistical significance when comparing probiotics to placebo, but this study ended prematurely due to slow accrual with only 46 out of the planned 220 patients, which may have compromised statistical power (55). Mahdavi et al. (27) reported that probiotics were not related to diarrhea incidence in patients undergoing chemotherapy, but, this systematic review only included three studies, compared to six studies included in the present review, which may explain the difference between the findings. Even though the evidence is promising, more studies with lower heterogeneity and exclusive for CRC patients are necessary to allow strong conclusions about the impact of these interventions in chemotherapy and radiotherapy toxicity and side-effects.
As previously mentioned, studies included in this review exhibit high heterogeneity between them in terms of used strains, dose, and duration of the intervention. Nonetheless, it can be observed that among studies where probiotics or synbiotics supplementation had a beneficial effect, some strains were present in the intervention across most of them. This is the case of species such as Lactobacillus rhamnosus, Lactobacillus acidophilus, Lactobacillus plantarum and Bifidobacterium lactis. These are well known beneficial bacteria that help maintain a functional and structured gut barrier with preclinical studies showing that Lactobacillus spp. and Bifidobacterium spp. have anticancer functions such as inhibition of cell proliferation, induction of cancer cell apoptosis, modulation of host immunity and reduction of inflammation (62, 66). Furthermore, these strains are butyrate-producing bacteria which can repair and enhance gut barrier function and appears to inhibit proliferation of CRC cells (61). Taking this into account, administration of a combination of Lactobacillus rhamnosus, Lactobacillus acidophilus, Lactobacillus plantarum, and Bifidobacterium lactis can be recommended for these types on interventions.
In terms of efficacy of probiotics versus synbiotics in CRC treatment, more robust evidence is needed in order to make stronger conclusions. The prebiotics contained in the synbiotics used in the studies included in the present review varied from fructoligosaccharides and galactoligosaccharides to betaglucan, inulin, pectin, and resistant starch with fructoligosaccharides being the one present in most of the studies with results of statistical significance that used synbiotics. The consumption of these types of prebiotics has been associated with increased counts of Lactobacillus spp. and Bifidobacterium spp. and as a result, higher levels of short-chain fatty acids including butyrate which, as previously mentioned, have anticancer properties (73, 74). Yet, in the present review, interventions with synbiotics do not appear to be more efficient than interventions with probiotics. Again, randomized controlled studies with less heterogeneity and larger sample sizes are needed in order to determine which gut modulation intervention is more adequate to improve CRC treatment.
Some studies have showed that gut microbiota composition differs across CRC progression. Notably patients with early-stage CRC (stage I-II) exhibit a distinct microbiota compared to those with late-stage CRC (stage III-IV) (9, 75). This raises questions about whether the efficacy of pre-, pro-, and synbiotic supplementation differs based on CRC stage. The majority of the studies encompassed in this systematic review included patients with different stages of CRC but didn’t divide them accordingly. A systematic review from Dikeocha et al. (24) reported that probiotics supplementation has beneficial effects regardless of CRC stage. Nonetheless, future studies should take this information into consideration and compare the effectiveness of these types of interventions in different stages of CRC. Similarly, it has been noted that gut microbiota composition varies depending on the location of the CRC tumor with tumors on the left-side of the colon presenting a different microbiota than those on the right-side (76, 77). To our knowledge, no study accounted for this distinction by dividing the intervention group based on the tumor location. However, it would be interesting to future studies to investigate whether these factors influence the effectiveness of the intervention.
Although this systematic review also aimed to study the impact of microbiota modulation in immunotherapy, no studies meeting our inclusion criteria, specifically focusing on CRC patients undergoing immunotherapy were found. This treatment is a relatively new approach for CRC patients so it’s possible that research may still be ongoing, and results will be published upcoming years regarding the role of pre-, pro-, and synbiotic supplementation in CRC patients undergoing immunotherapy (7, 78). Nevertheless, a recent meta-analysis, that included 6 studies, reported that probiotics improved the efficacy of immune checkpoint inhibitors in non-small cell lung cancer patients with the intervention group having better overall survival and higher objective response rate and disease control rate (79).
One point that also has to be considered is the safety of these interventions in CRC patients. Prebiotics, probiotics and synbiotics are in general considered safe, specially the most common studied and used strains such as Lactobacillus and Bifidobacterium (14, 80). In addition, none of the studies included in this review reported major adverse reactions caused by the intervention. Yet, microbiota modulation may impact the prognosis, the immune function and toxicity, as so safe strains have to be confirmed and immunocompromised patients should be carefully monitored. More studies to assess the safety of gut modulation in this population are needed (81).
This systematic review has limitations, including high heterogeneity between intervention groups (strains, dose, and duration) and different primary outcomes, which compromise the accuracy of comparisons between studies. Most studies had a small sample size, and some had a short intervention time which decreases the probability of obtaining statistically significant results. Additionally, not all existing databases were searched, and only studies in English or Portuguese were full text screened and included in this review which may have led to a loss of relevant data.
Nonetheless, this review has its strengths. A comprehensive search was performed in several electronic databases and all current available evidence, including more recent studies, was analyzed. The search was not limited in terms of interval of years of publication, and it studied the impact of pre-, pro-, and synbiotic supplementation in different types of CRC treatment and not just one specific treatment.
5 Conclusion
In conclusion, the comprehensive analysis conducted in this systematic review suggests that supplementation with prebiotics, probiotics, and synbiotics may be beneficial for patients undergoing treatment for CRC. There is moderate evidence that this type of intervention in CRC patients may potentially facilitate return to normal gut function and decrease the occurrence of both infectious and non-infectious postoperative complications, reduce hospital length of stay, and mitigate antibiotic usage. Furthermore, there is also some evidence suggesting that probiotic and synbiotic administration may help lessen some side effects, mainly diarrhea, associated with chemo- and radiotherapy. Interventions with more than one strain type, and longer duration, appear to be more effective. Randomized controlled studies with less heterogeneity and larger sample sizes are needed in order to determine the best approach regarding strain selection, dosage, and duration of the intervention in gut modulation interventions in CRC patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
MM: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. MC: Data curation, Investigation, Writing – review & editing. MC: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. NP: Writing – review & editing. TS: Writing – review & editing. SG: Writing – review & editing. AM: Writing – review & editing. PR: Formal analysis, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2024.1395966/full#supplementary-material
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 1–35. doi: 10.3322/caac.21834
2. Morgan E, Arnold M, Gini A, Lorenzoni V, Cabasag CJ, Laversanne M, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut. (2023) 72:338–44. doi: 10.1136/gutjnl-2022-327736
3. Wang Y, Li H. Gut microbiota modulation: a tool for the management of colorectal cancer. J Transl Med. (2022) 20:178. doi: 10.1186/s12967-022-03378-8
4. Kumar A, Gautam V, Sandhu A, Rawat K, Sharma A, Saha L. Current and emerging therapeutic approaches for colorectal cancer: A comprehensive review. World J Gastrointest Surg. (2023) 15:495–519. doi: 10.4240/wjgs.v15.i4.495
5. Tang G, Zhang L. Update on strategies of probiotics for the prevention and treatment of colorectal cancer. Nutr Cancer Routledge. (2022) p:27–38. doi: 10.1080/01635581.2020.1865420
6. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer (2019). Available at: http://www.thelancet.com.
7. Johdi NA, Sukor NF. Colorectal cancer immunotherapy: options and strategies. Front Immunol. (2020) 11:1624. doi: 10.3389/fimmu.2020.01624
8. Wu W, Ouyang Y, Zheng P, Xu X, He C, Xie C, et al. Research trends on the relationship between gut microbiota and colorectal cancer: A bibliometric analysis. Front Cell Infect Microbiol. (2023) 12:1027448/full. doi: 10.3389/fcimb.2022.1027448/full
9. Torres-Maravilla E, Boucard AS, Mohseni AH, Taghinezhad- SS, Cortes-Perez NG, Bermúdez-Humarán LG. Role of gut microbiota and probiotics in colorectal cancer: Onset and progression. Microorganisms. (2021) 9:1021. doi: 10.3390/microorganisms9051021
10. Cheng Y, Ling Z, Li L. The intestinal microbiota and colorectal cancer. Front Immunol. (2020) 11:61505. doi: 10.3389/fimmu.2020.615056
11. Wierzbicka A, Mańkowska-Wierzbicka D, Mardas M, Stelmach-Mardas M. Role of probiotics in modulating human gut microbiota populations and activities in patients with colorectal cancer—a systematic review of clinical trials. Nutrients. (2021) 13:1160. doi: 10.3390/nu13041160
12. Pandey H, Tang DWT, Wong SH, Lal D. Gut microbiota in colorectal cancer: biological role and therapeutic opportunities. Cancers (Basel) MDPI. (2023) 15:866. doi: 10.3390/cancers15030866
13. Zhao L, Cho WC, Nicolls MR. Colorectal cancer-associated microbiome patterns and signatures. Front Genet. (2021) 12. doi: 10.3389/fgene.2021.787176
14. Kvakova M, Kamlarova A, Stofilova J, Benetinova V, Bertkova I. Probiotics and postbiotics in colorectal cancer: Prevention and complementary therapy. World J Gastroenterol. (2022) 28:3370–82. doi: 10.3748/wjg.v28.i27.3370
15. Eslami M, Yousefi B, Kokhaei P, Hemati M, Nejad ZR, Arabkari V, et al. Importance of probiotics in the prevention and treatment of colorectal cancer. J Cell Physiol. (2019) 234:17127–43. doi: 10.1002/jcp.28473
16. Hou H, Chen D, Zhang K, Zhang W, Liu T, Wang S, et al. Gut microbiota-derived short-chain fatty acids and colorectal cancer: Ready for clinical translation? Cancer Lett. Elsevier Ireland Ltd. (2022) 526:225–35. doi: 10.1016/j.canlet.2021.11.027
17. Gao ZY, Cui Z, Yan YQ, Ning LJ, Wang ZH, Hong J. Microbe-based management for colorectal cancer. Chin Med J (Engl). (2021) 134:2922–30. doi: 10.1097/CM9.0000000000001887
18. Chen M, Lin W, Li N, Wang Q, Zhu S, Zeng A, et al. Therapeutic approaches to colorectal cancer via strategies based on modulation of gut microbiota. Front Microbiol. (2022) 13:945533. doi: 10.3389/fmicb.2022.945533
19. Martín R, Langella P. Emerging health concepts in the probiotics field: Streamlining the definitions. Front Microbiol. (2019) 10:1047. doi: 10.3389/fmicb.2019.01047
20. Miarons M, Roca M, Salvà F. The role of pro-, pre- and symbiotics in cancer: A systematic review. J Clin Pharm Ther. (2021) 46:50–65. doi: 10.1111/jcpt.13292
21. Kaźmierczak-Siedlecka K, Daca A, Fic M, van de Wetering T, Folwarski M, Makarewicz W. Therapeutic methods of gut microbiota modification in colorectal cancer management–fecal microbiota transplantation, prebiotics, probiotics, and synbiotics. Gut Microbes. (2020) 11:1518–30. doi: 10.1080/19490976.2020.1764309
22. Fong W, Li Q, Yu J. Gut microbiota modulation: a novel strategy for prevention and treatment of colorectal cancer. Oncogene Springer Nature. (2020) 39:4925–43. doi: 10.1038/s41388-020-1341-1
23. Molska M, Reguła J. Potential mechanisms of probiotics action in the prevention and treatment of colorectal cancer. Nutrients MDPI AG. (2019) 11:2453. doi: 10.3390/nu11102453
24. Dikeocha IJ, Al-Kabsi AM, Eid EEM, Hussin S, Alshawsh MA. Probiotics supplementation in patients with colorectal cancer: A systematic review of randomized controlled trials. Nutr Rev. (2022) 80:22–49. doi: 10.1093/nutrit/nuab006
25. Madrigal-Matute J, Escandell SB. Colorectal cancer and microbiota modulation for clinical use. A Systematic Review. (2021) 75:123–39. doi: 10.1101/2021.09.01.21262956
26. Zeng J, Ji Y, Liang B, Zhang G, Chen D, Zhu M, et al. The effect of pro/synbiotics on postoperative infections in colorectal cancer patients: A systematic review and meta-analysis. Complement Ther Clin Pract. (2021) 43:101370. doi: 10.1016/j.ctcp.2021.101370
27. Mahdavi R, Faramarzi E, Nikniaz Z, Farshiradvar F. Role of probiotics and synbiotics in preventing chemoradiotherapy-associated toxicity in colorectal cancer patients: A systematic review. Iran J Med Sci Shiraz. (2023) 48:110–7. doi: 10.30476/ijms.2022.92793.2411
28. Chen Y, Qi A, Teng D, Li S, Yan Y, Hu S, et al. Probiotics and synbiotics for preventing postoperative infectious complications in colorectal cancer patients: a systematic review and meta-analysis. Tech Coloproctol. (2022) 26:425–36. doi: 10.1007/s10151-022-02585-1
29. Veziant J, Bonnet M, Occean BV, Dziri C, Pereira B, Slim K. Probiotics/synbiotics to reduce infectious complications after colorectal Surgery: A systematic review and meta-analysis of randomised controlled trials. Nutrients. (2022) 14:3066. doi: 10.3390/nu14153066
30. Amitay EL, Carr PR, Gies A, Laetsch DC, Brenner H. Probiotic/synbiotic treatment and postoperative complications in colorectal cancer patients: systematic review and meta-analysis of randomized controlled trials. Clin Transl Gastroenterol. (2020) 11:e00268. doi: 10.14309/ctg.0000000000000268
31. Araújo MM, Montalvão-Sousa TM, Teixeira P da C, Figueiredo ACMG, Botelho PB. The effect of probiotics on postsurgical complications in patients with colorectal cancer: a systematic review and meta-analysis. Nutr Rev. (2023) 81:493–510. doi: 10.1093/nutrit/nuac069
32. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
33. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
34. Liu Z, Qin H, Yang Z, Xia Y, Liu W, Yang J, et al. Randomised clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery - A double-blind study. Aliment Pharmacol Ther. (2011) 33:50–63. doi: 10.1111/j.1365-2036.2010.04492.x
35. Zhang JW, Du P, Gao J, Yang BR, Fang WJ, Ying CM. Preoperative probiotics decrease postoperative infectious complications of colorectal cancer. Am J Med Sci. (2012) 343:199–205. doi: 10.1097/MAJ.0b013e31823aace6
36. Liu ZH, Huang MJ, Zhang XW, Wang L, Huang NQ, Peng H, et al. The effects of perioperative probiotic treatment on serum zonulin concentration and subsequent postoperative infectious complications after colorectal cancer surgery: A double-center and double-blind randomized clinical trial. Am J Clin Nutr. (2013) 97:117–26. doi: 10.3945/ajcn.112.040949
37. Yang Y, Xia Y, Chen H, Hong L, Feng J, Yang J, et al. The effect of perioperative probiotics treatment for colorectal cancer: short-term outcomes of a randomized controlled trial. Oncotarget. (2016) 7:8432–40. doi: 10.18632/oncotarget.v7i7
38. Xu Q, Xu P, Cen Y, Li W. Effects of preoperative oral administration of glucose solution combined with postoperative probiotics on inflammation and intestinal barrier function in patients after colorectal cancer surgery. Oncol Lett. (2019) 18:694–8. doi: 10.3892/ol
39. Huang F, Li S, Chen W, Han Y, Yao Y, Yang L, et al. Postoperative probiotics administration attenuates gastrointestinal complications and gut microbiota dysbiosis caused by chemotherapy in colorectal cancer patients. Nutrients. (2023) 15:356. doi: 10.3390/nu15020356
40. Topuz E, Derin D, Can G, Kürklü E, Çinar S, Aykan F, et al. Effect of oral administration of kefir on serum proinflammatory cytokines on 5-FU induced oral mucositis in patients with colorectal cancer. Invest New Drugs. (2008) 26:567–72. doi: 10.1007/s10637-008-9171-y
41. Can G, Topuz E, Derin D, Durna Z, Aydiner A. Effect of kefir on the quality of life of patients being treated for colorectal cancer. Oncol Nurs Forum. (2009) 36:E335-42. doi: 10.1188/09.ONF.E335-E342
42. Horvat M, Krebs B, Potrč S, Ivanecz A, Kompan L. Preoperative synbiotic bowel conditioning for elective colorectal surgery. Wien Klin Wochenschr. (2010) 122:26–30. doi: 10.1007/s00508-010-1347-8
43. Krebs B. Prebiotic and synbiotic treatment before colorectal surgery – randomised double blind trial. Coll Antropol. (2016) 40:35–40.
44. Sadahiro S, Suzuki T, Tanaka A, Okada K, Kamata H, Ozaki T, et al. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surg (United States). (2014) 155:493–503. doi: 10.1016/j.surg.2013.06.002
45. Komatsu S, Sakamoto E, Norimizu S, Shingu Y, Asahara T, Nomoto K, et al. Efficacy of perioperative synbiotics treatment for the prevention of surgical site infection after laparoscopic colorectal surgery: a randomized controlled trial. Surg Today. (2016) 46:479–90. doi: 10.1007/s00595-015-1178-3
46. Kotzampassi K, Stavrou G, Damoraki G, Georgitsi M, Basdanis G, Tsaousi G, et al. A four-probiotics regimen reduces postoperative complications after colorectal surgery: A randomized, double-blind, placebo-controlled study. World J Surg. (2015) 39:2776–83. doi: 10.1007/s00268-015-3071-z
47. Theodoropoulos GE, Memos NA, Peitsidou K, Karantanos T, Spyropoulos BG, Zografos G. Synbiotics and gastrointestinal function-related quality of life after elective colorectal cancer resection [Internet]. Ann Gastroenterol. (2016) 29:56–62.
48. Flesch AT, Tonial ST, Contu PDC, Damin DC. A administração perioperatória de simbióticos em pacientes com câncer colorretal reduz a incidência de infecções pós-operatórias: Ensaio clínico randomizado duplo-cego. Rev Col Bras Cir. (2017) 44:567–73. doi: 10.1590/0100-69912017006004
49. Polakowski CB, Kato M, Preti VB, Schieferdecker MEM, Ligocki Campos AC. Impact of the preoperative use of synbiotics in colorectal cancer patients: A prospective, randomized, double-blind, placebo-controlled study. Nutrition. (2019) 58:40–6. doi: 10.1016/j.nut.2018.06.004
50. Farshi Radvar F, Mohammad-Zadeh M, Mahdavi R, Andersen V, Nasirimotlagh B, Faramarzi E, et al. Effect of synbiotic supplementation on matrix metalloproteinase enzymes, quality of life and dietary intake and weight changes in rectal cancer patients undergoing neoadjuvant chemoradiotherapy. Med J Nutr Metab. (2020) 13:225–35. doi: 10.3233/MNM-200413
51. Mohebian F, Zarankesh SM, Jenabian A, Ranjbar H. The effectiveness of yogurt+ Probiotic on chemotherapy-related diarrhea in patients with colorectal cancer: A randomized clinical trial. Middle East J Cancer. (2023) 14:127–35. doi: 10.30476/mejc.2021.91324.1620
52. Tan CK, Said S, Rajandram R, Wang Z, Roslani AC, Chin KF. Pre-surgical administration of microbial cell preparation in colorectal cancer patients: A randomized controlled trial. World J Surg. (2016) 40:1985–92. doi: 10.1007/s00268-016-3499-9
53. Österlund P, Ruotsalainen T, Korpela R, Saxelin M, Ollus A, Valta P, et al. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: A randomised study. Br J Cancer. (2007) 97:1028–34. doi: 10.1038/sj.bjc.6603990
54. Mangell P, Thorlacius H, Syk I, Ahrné S, Molin G, Olsson C, et al. Lactobacillus plantarum 299v does not reduce enteric bacteria or bacterial translocation in patients undergoing colon resection. Dig Dis Sci. (2012) 57:1915–24. doi: 10.1007/s10620-012-2102-y
55. Mego M, Chovanec J, Vochyanova-Andrezalova I, Konkolovsky P, Mikulova M, Reckova M, et al. Prevention of irinotecan induced diarrhea by probiotics: A randomized double blind, placebo controlled pilot study. Complement Ther Med. (2015) 23:356–62. doi: 10.1016/j.ctim.2015.03.008
56. Park IJ, Lee JH, Kye BH, Oh HK, Cho YB, Kim YT, et al. Effects of probiotics on the symptoms and surgical outcomes after anterior resection of colon cancer (Postcare): A randomized, double-blind, placebo-controlled trial. J Clin Med. (2020) 9:1–16. doi: 10.3390/jcm9072181
57. Bajramagic S, Hodzic E, Mulabdic A, Holjan S, Smajlovic SV, Rovcanin A. Usage of Probiotics and its Clinical Significance at Surgically Treated Patients Sufferig from Colorectal Carcinoma. Med Arch. (2019) 73:316–20. doi: 10.5455/medarh.
58. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The european organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. JNCI J Natl Cancer Institute. (1993) 85:365–76. doi: 10.1093/jnci/85.5.365
59. Rodriguez-Arrastia M, Martinez-Ortigosa A, Rueda-Ruzafa L, Ayora AF, Ropero-Padilla C. Probiotic supplements on oncology patients’ treatment-related side effects: A systematic review of randomized controlled trials. Int J Environ Res Public Health. (2021) 18:4265. doi: 10.3390/ijerph18084265
60. Avuthu N, Guda C. Meta-analysis of altered gut microbiota reveals microbial and metabolic biomarkers for colorectal cancer. Microbiol Spectr. (2022) 10:e0001322. doi: 10.1128/spectrum.00013-22
61. Qu R, Zhang Y, Ma Y, Zhou X, Sun L, Jiang C, et al. Role of the gut microbiota and its metabolites in tumorigenesis or development of colorectal cancer. Advanced Sci. (2023) 10:e2205563. doi: 10.1002/advs.202205563
62. Rebersek M. Gut microbiome and its role in colorectal cancer. BMC Cancer. (2021) 21:1325. doi: 10.1186/s12885-021-09054-2
63. Coker OO, Liu C, Wu WKK, Wong SH, Jia W, Sung JJY, et al. Altered gut metabolites and microbiota interactions are implicated in colorectal carcinogenesis and can be non-invasive diagnostic biomarkers. Microbiome. (2022) 10:35. doi: 10.1186/s40168-021-01208-5
64. Hou X, Zheng Z, Wei J, Zhao L. Effects of gut microbiota on immune responses and immunotherapy in colorectal cancer. Front Immunol. (2022) 13:1030745. doi: 10.3389/fimmu.2022.1030745
65. Danis R, Mego M, Antonova M, Stepanova R, Svobodnik A, Hejnova R, et al. Orally administered probiotics in the prevention of chemotherapy (± Radiotherapy)-induced gastrointestinal toxicity: A systematic review with meta-analysis of randomized trials. Integr Cancer Ther. (2022) 21:15347354221144309. doi: 10.1177/15347354221144309
66. Zhao LY, Mei JX, Yu G, Lei L, Zhang WH, Liu K, et al. Role of the gut microbiota in anticancer therapy: from molecular mechanisms to clinical applications. Signal Transduct Target Ther. (2023) 8:201. doi: 10.1038/s41392-023-01406-7
67. Shinji S, Yamada T, Matsuda A, Sonoda H, Ohta R, Iwai T, et al. Recent advances in the treatment of colorectal cancer: A review. J Nippon Med School. (2022) 89:246–54. doi: 10.1272/jnms.JNMS.2022_89-310
68. Molenaar CJL, van Rooijen SJ, Fokkenrood HJP, Roumen RMH, Janssen L, Slooter GD. Prehabilitation versus no prehabilitation to improve functional capacity, reduce postoperative complications and improve quality of life in colorectal cancer surgery. Cochrane Database Systematic Rev. (2022) 5:CD013259. doi: 10.1002/14651858.CD013259.pub2
69. An S, Kim K, Kim MH, Jung JH, Kim Y. Perioperative probiotics application for preventing postoperative complications in patients with colorectal cancer: A systematic review and meta-analysis. Med (Kaunas). (2022) 58:1644. doi: 10.3390/medicina58111644
70. Frey-Furtado L, Magalhães I, Azevedo MJ, Sampaio-Maia B. The role of biotics as a therapeutic strategy for oral mucositis - A systematic review. Probiotics Antimicrob Proteins. (2023). doi: 10.1007/s12602-023-10116-z
71. Minervini G, Franco R, Marrapodi MM, Fiorillo L, Badnjević A, Cervino G, et al. Probiotics in the treatment of radiotherapy-induced oral mucositis: systematic review with meta-analysis. Pharmaceuticals. (2023) 16:654. doi: 10.3390/ph16050654
72. Feng J, Gao M, Zhao C, Yang J, Gao H, Lu X, et al. Oral administration of probiotics reduces chemotherapy-induced diarrhea and oral mucositis: A systematic review and meta-analysis. Front Nutr. (2022) 9:823288. doi: 10.3389/fnut.2022.823288
73. Dou Y, Yu X, Luo Y, Chen B, Ma D, Zhu J. Effect of fructooligosaccharides supplementation on the gut microbiota in human: A systematic review and meta-analysis. Nutrients. (2022) 14:3298. doi: 10.3390/nu14163298
74. Cruz BCS, Sarandy MM, Messias AC, Gonçalves RV, Ferreira CLLF, Peluzio MCG. Preclinical and clinical relevance of probiotics and synbiotics in colorectal carcinogenesis: A systematic review. Nutr Rev Oxford Univ Press. (2020) p:667–87. doi: 10.1093/nutrit/nuz087
75. Liu J, Huang X, Chen C, Wang Z, Huang Z, Qin M, et al. Identification of colorectal cancer progression-associated intestinal microbiome and predictive signature construction. J Transl Med. (2023) 21:373. doi: 10.1186/s12967-023-04119-1
76. Kneis B, Wirtz S, Weber K, Denz A, Gittler M, Geppert C, et al. Colon cancer microbiome landscaping: differences in right- and left-sided colon cancer and a tumor microbiome-ileal microbiome association. Int J Mol Sci. (2023) 24:3265. doi: 10.3390/ijms24043265
77. Zhong M, Xiong Y, Ye Z, Zhao J, Zhong L, Liu Y, et al. Microbial community profiling distinguishes left-sided and right-sided colon cancer. Front Cell Infect Microbiol. (2020) 10. doi: 10.3389/fcimb.2020.498502
78. Yuan H, Gui R, Wang Z, Fang F, Zhao H. Gut microbiota: A novel and potential target for radioimmunotherapy in colorectal cancer. Front Immunol. (2023) 14:1128774. doi: 10.3389/fimmu.2023.1128774
79. Zhang L, Jin Q, Chai D, Kuang T, Li C, Guan Y, et al. The correlation between probiotic use and outcomes of cancer patients treated with immune checkpoint inhibitors. Front Pharmacol. (2022) 13:937874. doi: 10.3389/fphar.2022.937874
80. Lin S, Shen Y. The efficacy and safety of probiotics for prevention of chemoradiotherapy-induced diarrhea in people with abdominal and pelvic cancer: A systematic review and meta-analysis based on 23 randomized studies. Int J Surgery. (2020) 84:69–77. doi: 10.1016/j.ijsu.2020.10.012
Keywords: probiotics, synbiotics, prebiotics, microbiota, colorectal neoplasms, systematic review
Citation: Moreira MM, Carriço M, Capelas ML, Pimenta N, Santos T, Ganhão-Arranhado S, Mäkitie A and Ravasco P (2024) The impact of pre-, pro- and synbiotics supplementation in colorectal cancer treatment: a systematic review. Front. Oncol. 14:1395966. doi: 10.3389/fonc.2024.1395966
Received: 04 March 2024; Accepted: 22 April 2024;
Published: 14 May 2024.
Edited by:
Ralf Weiskirchen, RWTH Aachen University, GermanyReviewed by:
Karolina Kaźmierczak-Siedlecka, Medical University of Gdansk, PolandChaochao Wang, The Affiliated Hospital of Southwest Medical University, China
Cihua Zheng, The Second Affiliated Hospital of Nanchang University, China
Copyright © 2024 Moreira, Carriço, Capelas, Pimenta, Santos, Ganhão-Arranhado, Mäkitie and Ravasco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Melo Moreira, marianamelopm@gmail.com