 Victor Schulze-Zachau1*
Victor Schulze-Zachau1* Gontran Verset2Pieter De Bondt3Katrien De Keukeleire4Falk Gühne5Martin Heuschkel6Ralf-Thorsten Hoffmann7
Gontran Verset2Pieter De Bondt3Katrien De Keukeleire4Falk Gühne5Martin Heuschkel6Ralf-Thorsten Hoffmann7 Elena Bozzi8
Elena Bozzi8 Rosa Sciuto9
Rosa Sciuto9 Marnix Lam10
Marnix Lam10 Jordi Deportós Moreno11
Jordi Deportós Moreno11 Roxane Debrus12Christoph J. Zech1
Roxane Debrus12Christoph J. Zech1- 1Radiology and Nuclear Medicine Clinic, University Hospital Basel, Basel, Switzerland
- 2Hôpital Universitaire de Bruxelles (HUB)-Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
- 3Department of Nuclear Medicine, Onze-Lieve-Vrouwziekenhuis (OLV) Aalst, Aalst, Belgium
- 4Radiology Department, Algemeen Stedelijk Ziekenhuis (ASZ) Aalst, Aalst, Belgium
- 5Jena University Hospital, Clinic of Nuclear Medicine, Jena, Germany
- 6Nuclear Medicine Clinic, Rostock University Medical Center, Rostock, Germany
- 7Diagnostic and Interventional Radiology Institute, University Hospital Carl Gustav Carus Technische Universität (TU) Dresden, Dresden, Germany
- 8Interventional Radiology Department, University Hospital Pisa, Pisa, Italy
- 9Nuclear Medicine Clinic, Istituti Fisioterapici Ospitalieri (IFO) Regina Elena Hospital Roma, Rome, Italy
- 10Nuclear Medicine Clinic, University Medical Center Utrecht, Utrecht, Netherlands
- 11Nuclear Medicine Clinic, Hospital Germans Trias i Pujol, Barcelona, Spain
- 12Terumo Europe, Leuven, Belgium
Purpose: Holmium-166 has emerged as a promising option for selective internal radiotherapy (SIRT) for hepatic malignancies, but data on routine clinical use are lacking. The purpose of this study was to describe the safety and effectiveness of Holmium-166 SIRT in real-world practice through retrospective analysis of a multicenter registry.
Methods: Retrospective analysis was conducted on Holmium-166 SIRT procedures performed between July 15, 2019, and July 15, 2021, across seven European centers. Treatment planning, treatment realization and post-treatment follow-up were conducted according to routine local practice. Safety and effectiveness data were extracted from the patients’ health records. Primary endpoint analysis was assessed for the entire study population with separate analysis for subgroups with hepatocellular carcinoma, metastatic colorectal cancer and intrahepatic cholangiocarcinoma.
Results: A total of 167 SIRT procedures in 146 patients (mean age 66 ± 11 years, 68% male) were retrospectively evaluated. Most common tumor entities were hepatocellular carcinoma (n=55), metastatic colorectal cancer (n=35), intrahepatic cholangiocarcinoma (n=19) and metastatic neuroendocrine tumors (n=10). Nine adverse events grade ≥ 3 according to Common Terminology Criteria for Adverse Events were recorded, including one fatal case of radioembolization-induced liver disease. Response rates and median overall survival for the above mentioned subgroups were comparable to results from previous Holmium-166 trials as well as to results from Yttrium-90 registries.
Conclusion: This study confirms that the safety and effectiveness of Holmium-166 SIRT derived from prospective trials also applies in routine clinical practice, reinforcing its potential as a viable treatment option for primary and secondary liver cancer.
1 Introduction
Selective internal radiotherapy (SIRT), also known as trans-arterial radioembolization (TARE), is a minimally invasive procedure during which radioactively-loaded microspheres are injected into the hepatic arteries in order to treat hepatic malignancies. According to guidelines, SIRT represents a treatment modality for patients with only or predominantly hepatic disease not suitable for surgery or ablative therapy or with failure of systemic therapy or inacceptable side effects (1–5). Hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (iCC) and hepatic metastases, e.g. from colorectal cancer (mCRC), are typical target entities. Before performing therapeutic SIRT, treatment planning is carried out with a reduced activity in order to simulate distribution of the therapeutic dose and to detect potential pulmonary or gastrointestinal shunting. Recent literature underlines the potential suitability of SIRT for individualized medicine (6, 7) and the development of radiation segmentectomy (8).
While Yttrium-90 (90Y) represents the conventional isotope for SIRT with technetium-99m macroaggregated albumin (99mTc-MAA) used for planning the treatment, an alternative platform based on Holmium-166 (166Ho) has been developed since the 1990s. 166Ho microspheres for SIRT are commercially available as QuiremSpheres™ (Quirem BV, Deventer, the Netherlands), and QuiremScout™ (Quirem BV, Deventer, the Netherlands) (9). The use of 166Ho offers interesting advantages: treatment planning and treatment can be performed using identical microspheres, which reduces discrepancy between both procedures and allows for optimized predictability of the distribution of the therapeutic injection (10) and improved prediction of pulmonary uptake of the activity (11). Furthermore, the element Holmium is a chemical lanthanide with paramagnetic properties, which enables quantification of hepatic 166Ho dose via MRI (9). This offers the possibility of intraprocedural MRI-based dosimetry, which has recently shown to be feasible (12). Following the administration of the scout dose, SPECT imaging of the thorax and abdomen is conducted in order to detect unintended delivery to the lungs or upper abdominal organs. The SPECT images obtained hereby serve as comparison to the post-treatment images in order to assess activity deposition outside the liver, the percentage of activity that has reached the lungs, the uniformity of the dose distribution, and the ratio of absorbed dose between the tumor and healthy tissues. For 166Ho SIRT, dedicated software (Q-suiteTM, Quirem BV, Deventer, The Netherlands) is available both for treatment planning and for dose reconstruction during treatment evaluation.
Several studies agreed on general safety and efficacy of 166Ho SIRT for various hepatic malignancies (13–16). However, recent publications point out the value of so called real-world evidence in addition to the findings derived from controlled trials (17). Real-world data can be defined as comprising any data not acquired with a primary scientific intention, such as electronic health records. Information on patient subgroups underrepresented in prospective trials may be available in real-world data and rare or late occurring side effects may be revealed. Furthermore, real-world data can help to analyze and evaluate the process of implementation of healthcare innovations into clinical routine.
The objective of this real-world, multi-center, retrospective registry was to describe the safety and effectiveness of 166Ho SIRT in real-world practice.
2 Materials and methods
2.1 Inclusion criteria
All consecutive patients treated with 166-Ho-SIRT for primary liver tumors or metastasis between July 15, 2019 and 15 July, 2021 in seven participating European centers were included. The study has been approved by the responsible ethical boards and has received the institutional approval number BASEC-Nr 2021–02357. Treatment allocation decisions were made by a local interdisciplinary tumor board. In Europe, SIRT is typically indicated for the treatment of primary and metastatic liver tumors not amenable to resection or ablation. 166Ho and 90Y SIRT have similar indications and contraindications. Contraindications include life expectancy of less than three months, pregnancy, clinical liver failure, disseminated extrahepatic disease and extrahepatic spread of radiation dose predicted by the treatment planning procedure.
Patients previously included in prospective studies with 166Ho SIRT were not included. Data collection took place between December 2021 and March 2022.
2.2 Treatment
Pre-treatment work-up and the treatment itself were performed according to routine practice in the study sites. Both 99mTc-MAA or 166Ho Scout could serve as surrogate marker during the treatment planning procedure. Treatment was performed in a single session or in multiple sessions. A recommendation that the absorbed whole liver radiation dose should not exceed 60 Gy has been developed. Guidelines for conducting the SIRT procedure were developed by European Association of Nuclear Medicine (EANM) (3).
The technical performance of SIRT was evaluated through pre- and post-treatment dosimetry and clinical practice descriptors: administered activity, liver volume, treatment approach (selective, lobar, whole liver), treatment volume, dosimetry outcomes in terms of target and normal liver dose (either recorded from post-treatment imaging or based on injected activity and target volume). Software used to perform the treatment planning and treatment procedures could be conventional software used at the study site or Q-Suite™. Calculation of treatment activity and post-treatment dose evaluations were performed according to local clinical routine.
The typical imaging techniques employed for dose estimation (work-up SPECT imaging of surrogates 99mTc-MAA or 166Ho Scout and MR imaging of therapeutic 166Ho microspheres) have been discussed in previous studies (8, 17). The process of voxel-level dosimetry using Q-Suite is outlined in the manufacturer’s instructions for use (https://www.quirem.com/ifu/). In short, SPECT-based dosimetry involves two main steps of calibrating the activity map and reconstructing the dose map. During dose estimation of work-up, first, the SPECT image is scaled to the intended activity for each target liver. Then, using conversion factor of 16 [MBq/J], absorbed dose is derived from activity map. For assessing the dose after treatment using SPECT image, first either a pre-established system calibration or a patient-specific calibration factor (based on the total counts in a user-defined volume and the total administered activity) is used to convert counts to Bq. After calibration, an absorbed dose map is reconstructed, either based on a local deposition model or a pre-defined dose-point kernel. MR-based dose evaluation after treatment is described in detail elsewhere (18). The imaging techniques employed in this retrospective observational study were dependent on the investigator’s choice and routine clinical practice.
2.3 Data collection
At each participating institution, a retrospective search of the patients’ electronic health records was conducted including the clinical information system (CIS), the picture archiving and communication system (PACS) and the laboratory information system (LIS), which usually contained data from pathologic examinations, too. The search followed a predefined list of variables. If certain variables could not be obtained in the electronic health records of the institution, the search was expanded to external health care providers such as general practitioners.
The following data were extracted: patient baseline characteristics, pre-treatment patient status, SIRT work-up procedure(s), SIRT procedures, post-treatment evaluation, occurrence of adverse events of specific interest (AESIs) and of adverse events (AEs) grade 3 or higher according to CTCAE (Common Terminology Criteria for Adverse Events) version 5.0. Th.
2.4 Safety assessment
Safety primary endpoint analysis was performed for short term (30 days), median term (1–12 months), long term (>12 months), and overall safety (at any time). The primary safety endpoint was defined in terms of reported incidence of AEs according to CTCAE grade ≥ 3, or any of the following AESIs known to be associated with SIRT regardless of their CTCAE grading: acute pancreatitis, gastric ulceration, gastritis, radiation pneumonitis, radioembolization-induced liver disease (REILD), and cholecystitis. Safety assessment was also performed based on routine blood tests with an emphasis on the liver function parameters obtained at baseline, after the SIRT procedure and throughout the follow-up period of 12 months with specific time windows of 1 week, 3, 6, 9, and 12 months.
2.5 Efficacy assessment
Progression Free Survival (PFS) was defined as the time from first SIRT procedure until overall progression or death. Hepatic Progression Free Survival (hPFS) was defined as the time from first SIRT procedure until hepatic progression or death. Overall survival (OS) was defined as the time from first SIRT procedure until death from any cause.
Tumor response in the liver according to mRECIST and/or RECIST 1.1 was analyzed at 3 months (+/- 14 days) after SIRT had been completed, or beyond the 3-months point, depending on the available information, and evaluated as best overall response. Disease control (DC) rate was defined as the sum of objective response (complete or partial response) and stable disease rates.
2.6 Statistical analyses
Patient demographics, baseline characteristics, and procedure characteristics were summarized with mean, standard deviation, median and range for continuous variables and with frequencies, percentages, and 95% confidence intervals for discrete variables.
Treatment response was reported as percentage of all patients with known outcome. For time to event clinical endpoints, Kaplan-Meier survival curves were presented.
All analyses were conducted using SAS v9.4 (SAS Institute, Cary, NC) or the latest available SAS software.
2.7 Ethical considerations
The study was approved by the Ethics Committees of all participating institutions. Due to the retrospective nature of the study, a waiver of informed consent was requested to the Ethics Committees in charge and approved.
3 Results
3.1 Patient characteristics and data collection
A total of 157 patients were recorded, including eight patients who did not receive the therapeutic dose due to unfavorable outcomes of the treatment planning procedure, and three patients who received the therapeutic dose but for whom treatment date was not available, which precluded time to event analysis. 146 patients from seven participating centers were included in the final analysis (Figure 1). These included 55 cases of HCC, 19 iCC, 35 mCRC, and 37 liver metastases of other origins. Baseline characteristics of the study population and treatment intent are presented in Table 1. Disease characteristics of the 55 patients with HCC are presented in Table 1. Among the 19 patients with iCC, 9 patient (47%) were treated with palliative intent, 1 (5%) with curative intent, 3 (16%) were treated for downstaging and another 3 (16%) – for bridging to resection.

Figure 1 Flow chart of the study. HCC, hepatocellular carcinoma; iCC, intrahepatic cholangiocarcinoma; mCRC, metastatic colorectal cancer; mNET, metastatic neuroendocrine tumor; SIRT, selective internal radiotherapy.
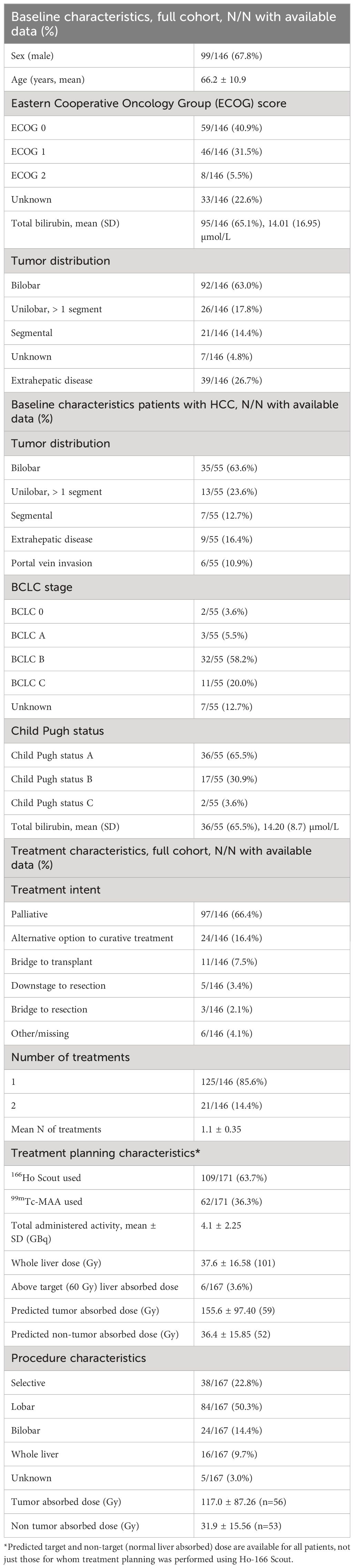
Table 1 Patient baseline and treatment characteristics.
3.2 Treatment
A total of 167 treatment procedures were performed. Of all patients, 85.6% (125) received a single treatment session with 166Ho SIRT, and 14.4% (21) received two treatment sessions with 166Ho SIRT (Figure 1). The median number of days between the first and second treatment session was 43 days (range 8–354 days). No patients received 3 or more treatments. Details on treatment planning are provided in Table 1 and Figure 1.
Average whole liver absorbed dose was available for 101 patients, of whom 95 had a whole liver average absorbed dose < 60 Gy. Six patients (5.9%) exceeded the 60 Gy whole liver recommendation: three patients by < 10 Gy, and three patients had a whole liver absorbed dose of between 80 and 90 Gy. For further details of post-treatment SPECT, see Table 1.
3.3 Tumor response
Among the patients with available tumor response assessment criteria, mRECIST was used in 48 cases, and RECIST 1.1 was used in 30 cases. For evaluation at three months after SIRT (+/- 14 days), response assessment was available for 39.7% (58 evaluated) of patients (Table 2). Best response and disease control rates beyond three months in different subgroups per diagnosis are presented in Figure 2. Tumor absorbed dose per best response beyond three months is presented on Figure 3.
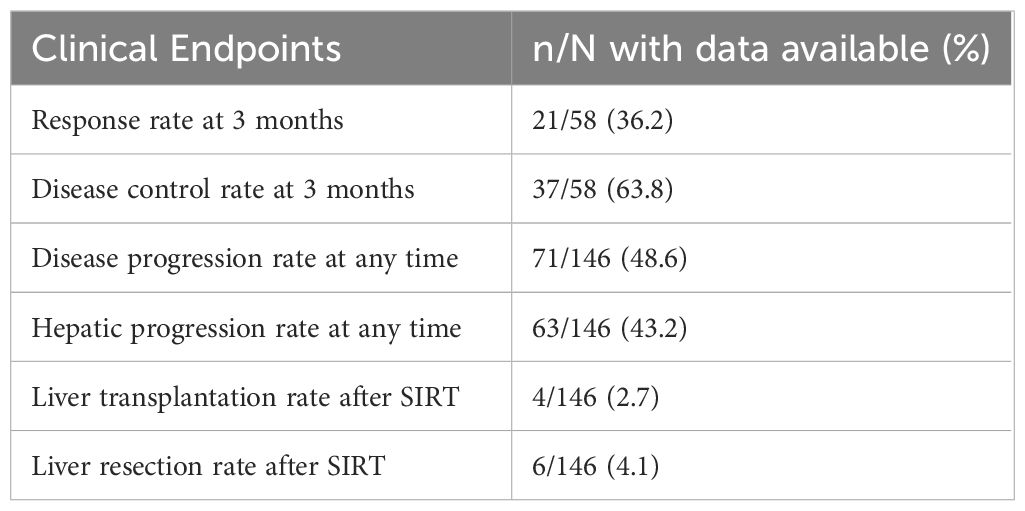
Table 2 Tumor response rate and treatment outcomes, all subgroups.
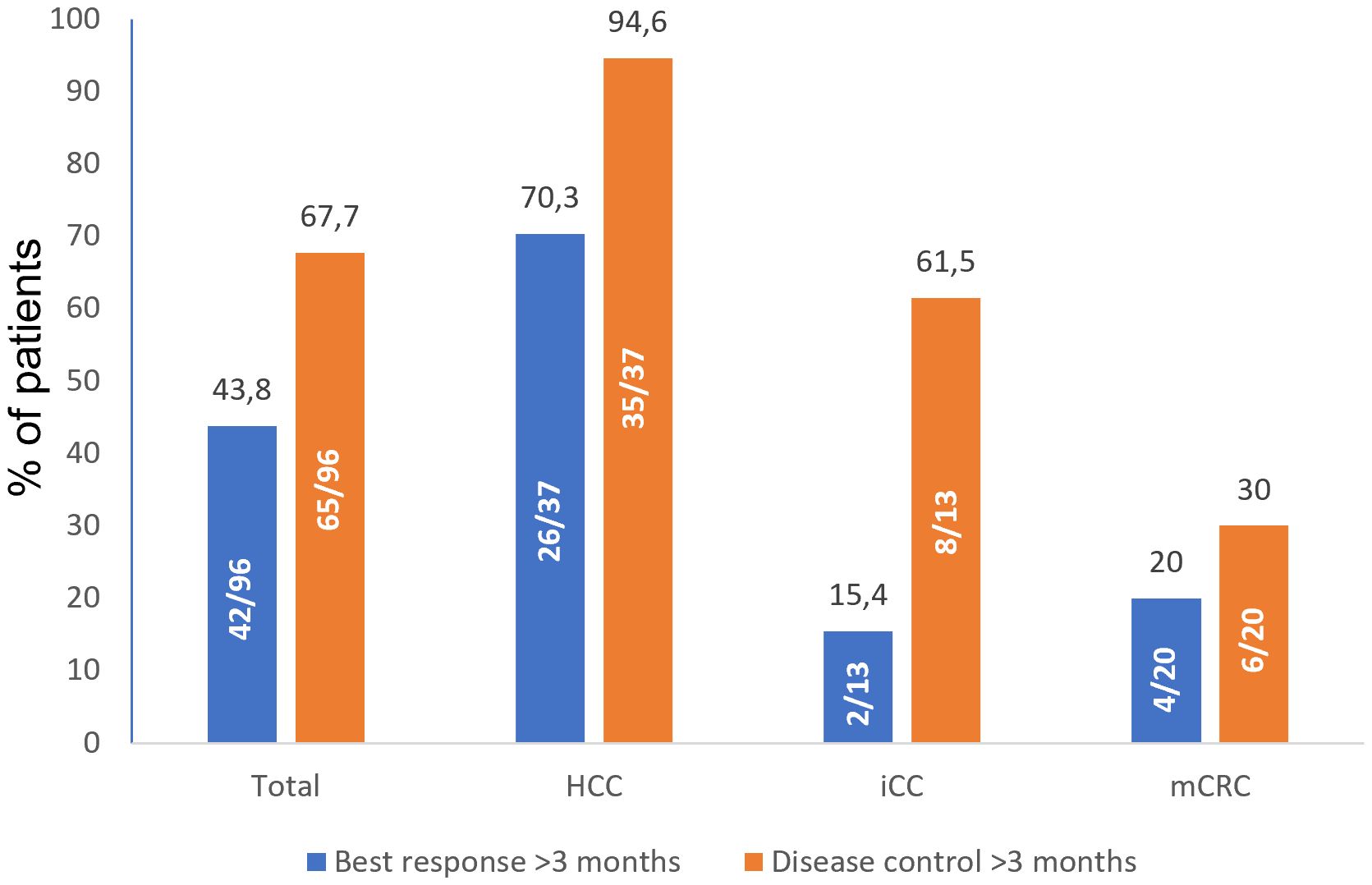
Figure 2 Best response and disease control rates (%) beyond three months. Best response was defined as combination of tumor responses in target and non-target lesions; disease control was defined as combination of complete response, partial response, and stable disease. HCC, hepatocellular carcinoma; iCC, intrahepatic cholangiocarcinoma; mCRC, metastatic colorectal cancer.
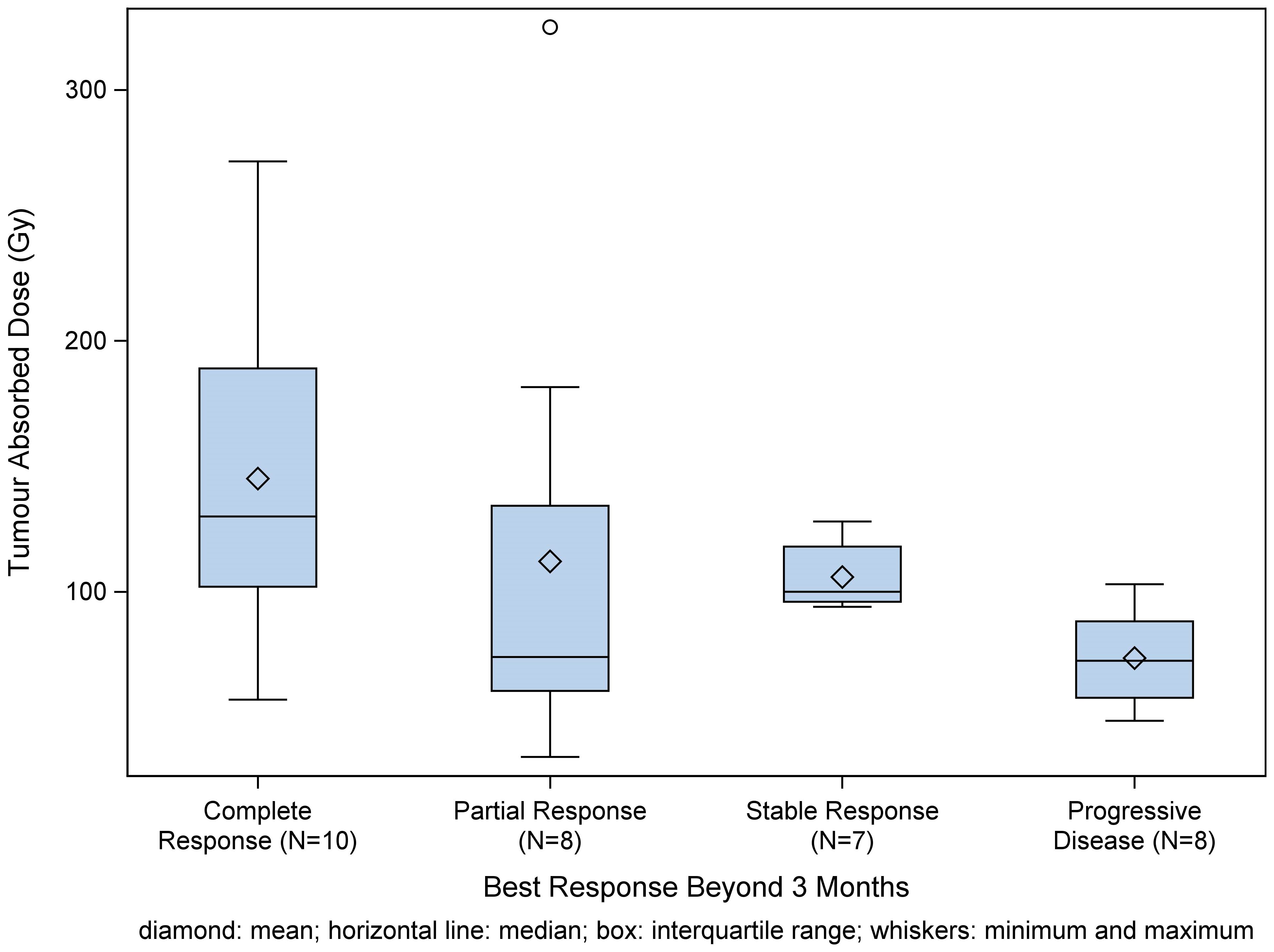
Figure 3 Box plot of tumor absorbed dose per best response category beyond three months shows a non-significant trend towards dose-response-relationship. Best response was defined as combination of tumor responses in target and non-target lesions; disease control was defined as combination of complete response, partial response, and stable disease.
3.4 Survival
Survival outcomes were analyzed for patients with HCC (n=55), mCRC (n=35) and iCC (n=19). Patients were followed for a median of 7.1 months (range 0.1- 26.4 months]. The proportion of censored patients was 54.1% for OS, 33.8% for PFS and 37.9% for hPFS.
Median PFS was 5.3 months (95% CI 3.8–7) in the total evaluable population, of which 33.8% (49) of patients were censored. Median PFS was 9.1 months in HCC (95% CI 7.1–14), 3.2 months in mCRC (95% CI 2.8-n.e. (non-estimable)), 3.9 months in iCC (95% CI 3.0–8).
Overall median hPFS was 6.5 months (95% CI 4.1, 9) (Figure 4), with 37.9% (55) of patients in this population censored. Median hPFS was 9.7 months in HCC (95% CI 7.1–14), 3.2 months in mCRC (95% CI 2.8–5) and 6.6 months in iCC (95% CI 3.0–8).
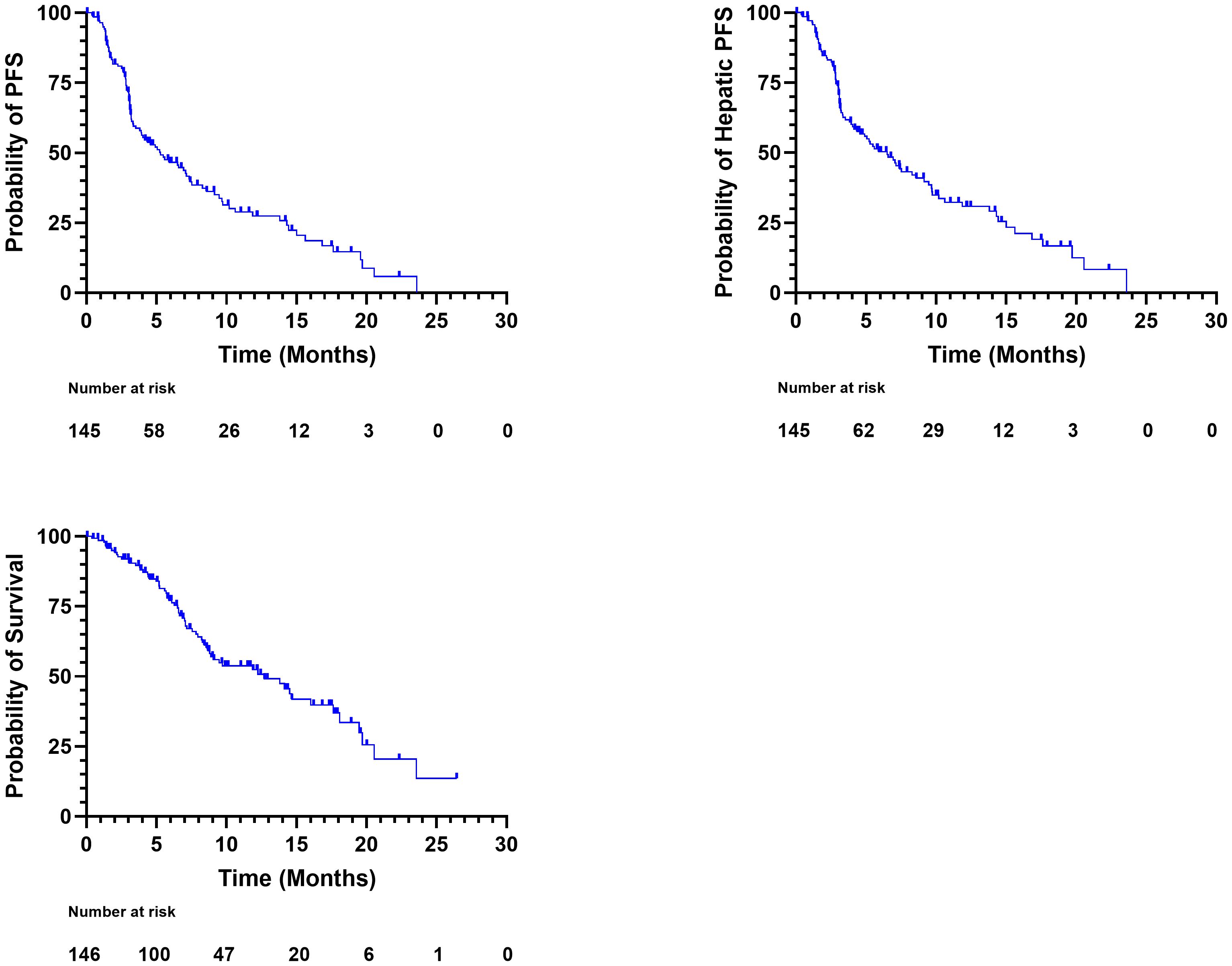
Figure 4 Kaplan-Meier plots of progression free survival (upper left), hepatic progression free survival (hPFS) (upper right) and overall survival (OS) (lower left) for the total population.
Overall median OS was 12.7 months (95% CI 8.8–18) (Figure 4). 54.1% (79) of the total population was censored. Median OS was 14.7 months in HCC (95% CI 13.8-n.e.), 8.9 months in mCRC (95% CI 7.1–14) and 8.3 months in iCC (95% CI 6.6–24), respectively.
3.5 Hepatocellular injury markers
Both AST and ALT demonstrated a post-treatment increase. Mean AST increased from 38.99 ± 37.42 IU/L (mean ± SD) at baseline to the maximal value of 157.63 ± 796.61 IU/L at 90 days. Mean ALT increased from 29.29 ± 27.38 IU/L at baseline to 66.42 ± 237.22 IU/L at 90 days (Figure 5). Both parameters returned to baseline levels (42.52 ± 48.74 IU/L for AST and 26.17 ± 29.65 IU/L for ALT) at 270 days (9 months). Bilirubin levels showed a gradual increase from the baseline value of (mean ± SD) 1.763 ± 12.82 µmol/L to the maximum value of 260.611 ± 994.45 µmol/L at 180 days, returning back to 181.546 ± 641.91 µmol/L at 270 days and 51.303 ± 75.91 µmol/L at 360 days (12 months).
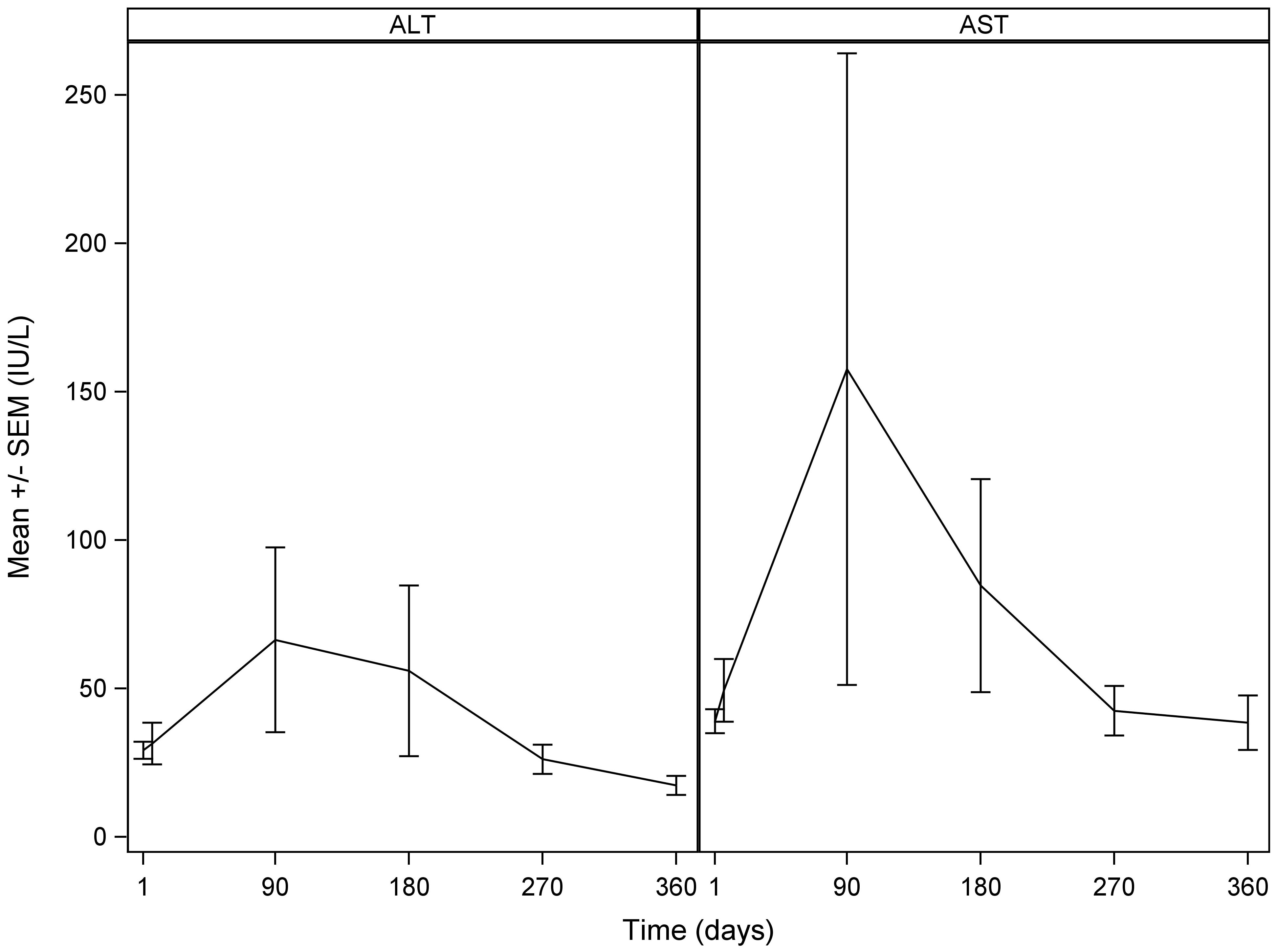
Figure 5 Mean alanine aminotransferase (ALT) (left) and aspartate transaminase (AST) (right): mean ± standard deviation with standard error over time. Time in days refers to the number of days after the SIRT treatment.
3.6 Safety
Among the three patients who received a 80–90 Gy liver absorbed dose, one reported epigastric pain as an AE with onset 31 days after the procedure with possible relation to the procedure, which later resolved. In five (3.4%) patients, at least one AESI was reported. Acute pancreatitis, or radiation pneumonitis were not reported. Gastric ulceration was reported in 2.1% (3) of patients (Table 3). A total of five fatal AEs were recorded in the study, three of them possibly or probably related to the treatment device and/or procedure. One fatal case of cholecystitis with onset of 32 days after the procedure was reported, and assessed as possibly related to the procedure and the treatment device. REILD was reported in one patient (0.7%) with an onset of 89 days after the first, and 39 days after the second treatment, which resulted in the patient’s death. A probable relation to the procedure and possible relation to the device was reported. In this case, SIRT was performed with a palliative intent in a patient with bilobar HCC, BCLC stage B, Child Pugh score A with slightly elevated total bilirubin of 30 µmol/l at baseline. No extrahepatic disease or portal vein invasion was reported. Separate treatments of left and right liver lobe were performed at an interval of two months with average absorbed lobar doses of approximately 55 Gy and 60 Gy, respectively. One case of acute or chronic renal failure was recorded 91 days after the treatment, and resulted in the patient’s death. This case was assessed as possibly related to the treatment procedure, but not to the device.
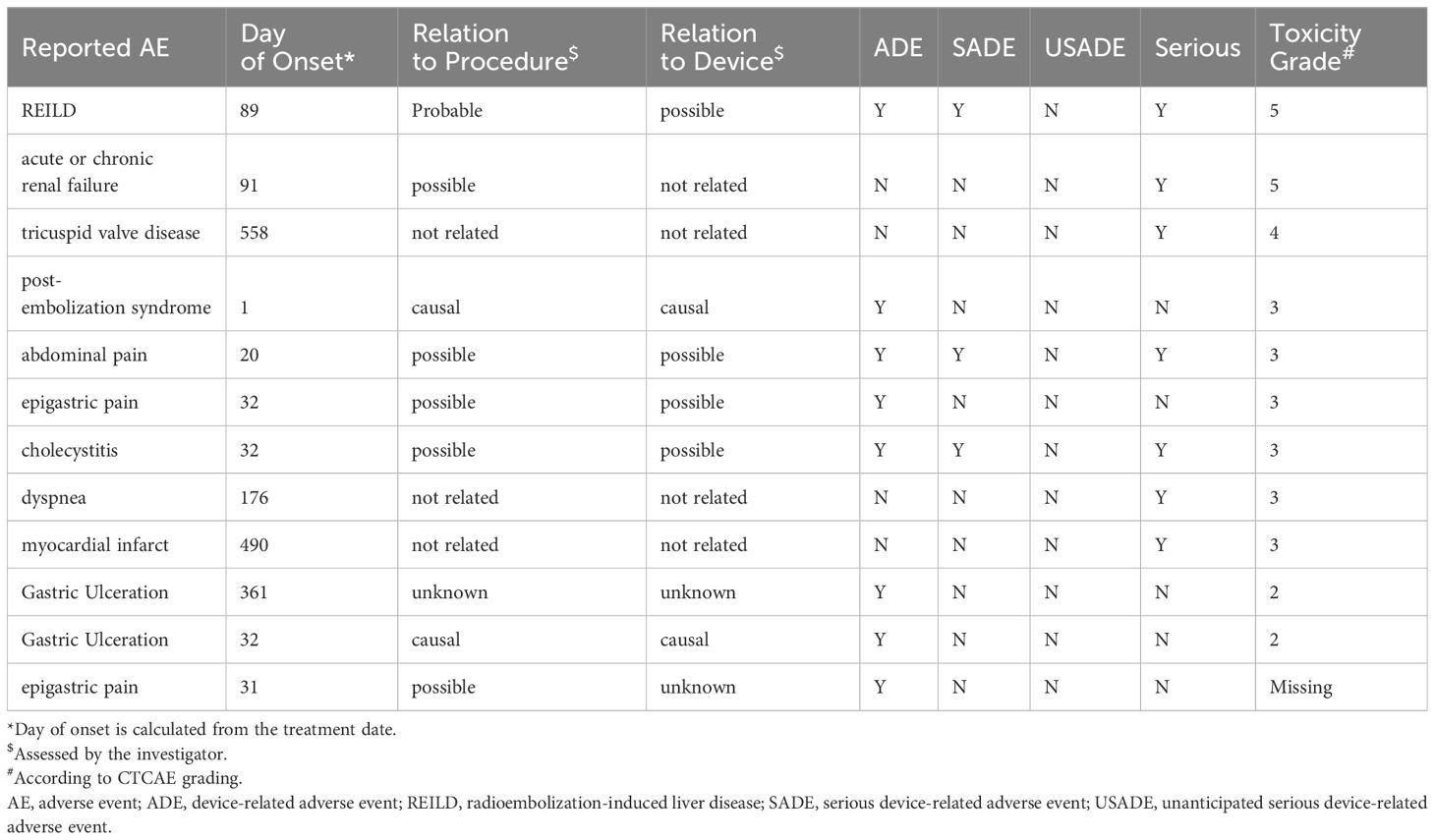
Table 3 Adverse Events reported by toxicity grade and day of onset.
4 Discussion
This real-world, multi-center, retrospective study aimed at characterizing the safety and performance of 166Ho SIRT in routine clinical practice as opposed to prospective clinical trials.
Response and disease control rates both at and beyond three months vary in previous studies, and the results of the present study are within this range (13, 14, 16, 18, 19). Different magnitude of tumor response and disease control was achieved in different indications, with HCC patients having higher percentages of both than iCC and mCRC patients. That may suggest that SIRT yields different response dependent on the tumor type, possibly mediated through tumor vascularity and consecutive differences in absorbed dose. Median OS for mCRC and HCC are in line with results from HEPAR II, SIM and HEPAR Primary, respectively. Median OS found in the CIRT registry for mCRC and HCC treated with 90Y SIRT is similar, too. The RESIN registry showed a higher median OS for patients with mCRC treated with 90Y SIRT of 15.0 months (95% CI 13.3–16.9) compared to 8.9 months in the present study (95% CI 8.8–18). However, our results correspond to those of the pooled analysis of 2,517 patients from 23 studies reported by White et al. (20)in which weighted OS estimate was 9.6 months (95% CI 8.9–10.4). A relatively low number of patients receiving a liver transplantation after SIRT was recorded in this study. This may reflect the fact that the study included a more advanced patient population, possibly highlighting the context of SIRT usage in real-world practice. In patient cohorts with an earlier stage of disease, the proportion of patients qualifying for post-SIRT liver transplantation may be higher.
A dose-response-relationship of 166Ho SIRT has already been established (20). While the prediction of normal liver absorbed dose was accurate, the predicted tumor absorbed dose had been overestimated by approximately 30 Gy. This overestimation derived mainly from two centers, which contributed to a large number of the overall available datapoints. That could be possibly explained by dose calculation errors, such as partial volume effects, misregistration of CT and SPECT images. Saturation effects of the gamma camera, different catheter position between treatment planning and treatment, periprocedural occlusion of arterial branches and timepoint of dosimetry might contribute to the explanation of this finding. However, since accurate dose prediction is one of the advantages of 166Ho -SIRT in comparison to 90Y SIRT with 99mTc-MAA for treatment planning, the overestimation of tumor absorbed dose should call attention to possible confounders.
Overall, the frequency of AEs reported in the present study is low compared to earlier 166Ho studies and is probably underreported (12, 13, 15, 21). Radioembolization induced liver disease (REILD) represents a rare but dangerous complication of SIRT and occurred in one patient (0.7%) with lethal outcome. Renal failure represents the only other lethal AE and was reported as possibly related to the procedure.
This study has several limitations. The retrospective nature and the single-arm design invariably contain limitations. The heterogeneous study population limits the comparison to previous studies. PFS (33.8%) and hPFS (37.9%) assessments had a high proportion of censored patients. Overall survival analysis had the highest proportion of censored patients (54.1%), which is in line with expectations: As survival analysis typically requires longer follow-up to observe the event of interest, the probability of a patient not to reach an event is high for patients treated at the end of the inclusion window. The retrospective design contains a risk of underreporting of AEs. However, AEs grade 4 or 5 according to CTCAE represent severe incidents, which are typically well documented in the patients’ health records. Therefore, it is reasonable to assume that the low frequency of severe AEs in this study can be interpreted as a sign of overall good tolerability of 166Ho SIRT. This is not only in line with previous 166Ho SIRT studies (12, 13, 15, 21), but also with recent preliminary results from the CIRT registry (22) and data from the RESIN registry (23), showing similar safety profiles for 90Y SIRT.
Another limitation of this study is the heterogeneity of imaging protocols for 166Ho microsphere treatments. Although the accuracy of dosimetry relies on imaging modality and reconstruction protocols (24, 25), standardization in imaging for 166Ho is lacking. We are convinced that imaging standardization will be paramount for achieving consistent and harmonized absorbed dose measurements. Meanwhile, the heterogeneity of imaging in our patient cohort reflects current real-world practice.
This observational study did not aim at comparing the treatment planning characteristics of 99mTc-MAA and 166Ho Scout microspheres. However, published studies on this topic are available (9).
Finally, data granularity for specific questions is limited, for instance, the presence but not the degree of portal vein thrombosis was collected.
Strengths of this study include the high number of patients and the diversity of malignancies, treatment intentions and procedure characteristics. Data origin from multiple international centers further adds to the validity of the study.
Overall, this study confirms that the safety and effectiveness of 166Ho SIRT derived from prospective trials also applies in routine clinical practice. Treatment effectiveness of 166Ho SIRT was in line with treatment effectiveness reported in prospective Ho-166 SIRT trials as well as in large 90Y SIRT registries.
Data availability statement
The raw data of this research are available from the corresponding author on reasonable request within the boundaries of the ethical committee approval. Requests to access the datasets should be directed to VS-Z, victor.schulze-zachau@usb.ch.
Ethics statement
The studies involving humans were approved by the ethics committees of all participating centers. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this project consisted of retrospective collection of pseudonymized data in a patient cohort with a high mortality.
Author contributions
VS-Z: Writing – review & editing, Writing – original draft, Visualization, Validation, Methodology, Investigation, Formal Analysis, Data curation. GV: Writing – review & editing, Investigation. PD: Writing – review & editing, Investigation. KD: Writing – review & editing, Investigation. FG: Writing – review & editing, Investigation. MH: Writing – review & editing, Investigation. RH: Writing – review & editing, Investigation. EB: Writing – review & editing, Investigation. RS: Writing – review & editing, Investigation. ML: Writing – review & editing, Investigation. JDM: Writing – review & editing, Investigation. RD: Writing – review & editing, Visualization, Resources, Project administration, Funding acquisition. CZ: Writing – review & editing, Validation, Supervision, Methodology, Investigation, Funding acquisition, Formal Analysis.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was financially supported including publication fee by Terumo Europe N.V., Researchpark Haasrode 1520 Interleuvenlaan, 40 B-3001 Leuven Belgium. Terumo Europe provided support for data collection and statistical analysis. The authors interpreted the data and drafted and edited the manuscript. The first and the last author take full responsibility for the manuscript. Author VS-Z has received a research grant for excellent young researchers from Basel University, Basel, Switzerland (Grant number U.350.1008).
Conflict of interest
Author GV is a consultant for Terumo/Quirem, speaker/advisory board member for Roche, Eisai and Astra-Zeneca. Author ML is a consultant for Terumo, Boston Scientific and Novartis and received research support from Terumo, Boston Scientific and Novartis. The department of Radiology and Nuclear Medicine of the UMC Utrecht receives royalties from Terumo. Author RD was employed by Terumo Europe.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer MS declared a past collaboration with the author ML to the handling editor.
The authors declare that this study received funding from Terumo Europe N.V. Terumo Europe financially supported the study including publication fee. Furthermore, Terumo Europe provided support for data collection and statistical analysis. The authors interpreted the data and drafted and edited the manuscript. The first and the last author take full responsibility for the manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AE, adverse event; AESI, adverse event of special interest; ALT, Alanine transaminase; AST, Aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; 166Ho, Holmium-166; SIRT, Selective internal radiotherapy; SAE, severe adverse event; TARE, Transarterial radioembolization; MRI, Magnetic resonance imaging; HCC, Hepatocellular Carcinoma; iCC, Intrahepatic cholangiocarcinoma; mNET, metastatic Neuroendocrine Tumor; mCRC, metastatic colorectal carcinoma; PFS, progression-free survival; hPFS, hepatic progression-free survival; REILD, Radioembolization induced liver disease; OS, Overall survival; RECIST, Response Evaluation Criteria in Solid Tumors; mRECIST, modified Response Evaluation Criteria in Solid Tumors; CTCAE, National Cancer Institute’s Common Terminology Criteria for Adverse Events; 90Y, Yttrium-90; 99Tc-MAA, Technecium-99 macroaggregated albumin.
References
1. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. (2016) 27:1386–422. doi: 10.1093/annonc/mdw235
2. Valle JW, Borbath I, Khan SA, Huguet F, Gruenberger T, Arnold D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2016) 27:v28–37. doi: 10.1093/annonc/mdw324
3. Weber M, Lam M, Chiesa C, Konijnenberg M, Cremonesi M, Flamen P, et al. EANM procedure guideline for the treatment of liver cancer and liver metastases with intra-arterial radioactive compounds. Eur J Nucl Med Mol Imaging. (2022) 49:1682–99. doi: 10.1007/s00259-021-05600-z
4. Galle PR, Forner A, Llovet JM, Mazzaferro V, Piscaglia F, Raoul J-L, et al. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. (2018) 69:182–236. doi: 10.1016/j.jhep.2018.03.019
5. Spreafico C, Sposito C, Vaiani M, Cascella T, Bhoori S, Morosi C, et al. Development of a prognostic score to predict response to Yttrium-90 radioembolization for hepatocellular carcinoma with portal vein invasion. J Hepatol. (2018) 68:724–32. doi: 10.1016/j.jhep.2017.12.026
6. Garin E, Tselikas L, Guiu B, Chalaye J, Edeline J, de Baere T, et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol Hepatol. (2021) 6:17–29. doi: 10.1016/S2468–1253(20)30290–9
7. Levillain H, Bagni O, Deroose CM, Dieudonné A, Gnesin S, Grosser OS, et al. International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres. Eur J Nucl Med Mol Imaging. (2021) 48:1570–84. doi: 10.1007/s00259–020-05163–5
8. Kim E, Sher A, Abboud G, Schwartz M, Facciuto M, Tabrizian P, et al. Radiation segmentectomy for curative intent of unresectable very early to early stage hepatocellular carcinoma (RASER): a single-centre, single-arm study. Lancet Gastroenterol Hepatol. (2022) 7:843–50. doi: 10.1016/S2468–1253(22)00091–7
9. Stella M, Braat AJAT, van Rooij R, de Jong HWAM, Lam MGEH. Holmium-166 radioembolization: current status and future prospective. Cardiovasc Intervent Radiol. (2022) 45:1634–45. doi: 10.1007/s00270-022-03187-y
10. Smits MLJ, Dassen MG, Prince JF, Braat AJAT, Beijst C, Bruijnen RCG, et al. The superior predictive value of 166Ho-scout compared with 99mTc-macroaggregated albumin prior to 166Ho-microspheres radioembolization in patients with liver metastases. Eur J Nucl Med Mol Imaging. (2020) 47:798–806. doi: 10.1007/s00259-019-04460-y
11. Elschot M, Nijsen JFW, Lam MGEH, Smits MLJ, Prince JF, Viergever MA, et al. (99m)Tc-MAA overestimates the absorbed dose to the lungs in radioembolization: a quantitative evaluation in patients treated with 166Ho-microspheres. Eur J Nucl Med Mol Imaging. (2014) 41:1965–75. doi: 10.1007/s00259–014-2784–9
12. Roosen J, Westlund Gotby LEL, Arntz MJ, Fütterer JJ, Janssen MJR, Konijnenberg MW, et al. Intraprocedural MRI-based dosimetry during transarterial radioembolization of liver tumours with holmium-166 microspheres (EMERITUS-1): a phase I trial towards adaptive, image-controlled treatment delivery. Eur J Nucl Med Mol Imaging. (2022) 49:4705–15. doi: 10.1007/s00259-022-05902-w
13. Prince JF, van den Bosch MAAJ, Nijsen JFW, Smits MLJ, van den Hoven AF, Nikolakopoulos S, et al. Efficacy of radioembolization with 166 ho-microspheres in salvage patients with liver metastases: A phase 2 study. J Nucl Med. (2018) 59:582–8. doi: 10.2967/jnumed.117.197194
14. Reinders MTM, van Erpecum KJ, Smits MLJ, Braat AJAT, de Bruijne J, Bruijnen RCG, et al. Safety and efficacy of holmium-166 radioembolization in hepatocellular carcinoma – the HEPAR Primary study. J Nucl Med. (2022). doi: 10.2967/jnumed.122.263823
15. van Roekel C, van den Hoven AF, Bastiaannet R, Bruijnen RCG, Braat AJAT, de Keizer B, et al. Use of an anti-reflux catheter to improve tumor targeting for holmium-166 radioembolization—a prospective, within-patient randomized study. Eur J Nucl Med Mol Imaging. (2021) 48:1658–68. doi: 10.1007/s00259–020-05079–0
16. Braat AJAT, Bruijnen RCG, van Rooij R, Braat MNGJA, Wessels FJ, van Leeuwaarde RS, et al. Additional holmium-166 radioembolisation after lutetium-177-dotatate in patients with neuroendocrine tumour liver metastases (HEPAR PLuS): a single-centre, single-arm, open-label, phase 2 study. Lancet Oncol. (2020) 21:561–70. doi: 10.1016/S1470–2045(20)30027–9
17. Basch E, Schrag D. The evolving uses of “Real-world” Data. JAMA. (2019) 321:1359–60. doi: 10.1001/jama.2019.4064
18. Smits ML, Nijsen JF, van den Bosch MA, Lam MG, Vente MA, Mali WP, et al. Holmium-166 radioembolisation in patients with unresectable, chemorefractory liver metastases (HEPAR trial): a phase 1, dose-escalation study. Lancet Oncol. (2012) 13:1025–34. doi: 10.1016/S1470–2045(12)70334–0
19. Drescher R, Köhler A, Seifert P, Aschenbach R, Ernst T, Rauchfuß F, et al. Clinical results of transarterial radioembolization (TARE) with holmium-166 microspheres in the multidisciplinary oncologic treatment of patients with primary and secondary liver cancer. Biomedicines. (2023) 11:1831. doi: 10.3390/biomedicines11071831
20. White J, Carolan-Rees G, Dale M, Morgan HE, Patrick HE, See TC, et al. Analysis of a national programme for selective internal radiation therapy for colorectal cancer liver metastases. Clin Oncol. (2019) 31:58–66. doi: 10.1016/j.clon.2018.09.002
21. Bastiaannet R, van Roekel C, Smits MLJ, Elias SG, van Amsterdam WAC, Doan D, et al. First evidence for a dose–response relationship in patients treated with 166Ho radioembolization: A prospective study. J Nucl Med. (2020) 61:608. doi: 10.2967/jnumed.119.232751
22. Braat AJAT, Prince JF, van Rooij R, Bruijnen RCG, van den Bosch MAAJ, Lam MGEH. Safety analysis of holmium-166 microsphere scout dose imaging during radioembolisation work-up: A cohort study. Eur Radiol. (2018) 28:920–8. doi: 10.1007/s00330–017-4998–2
23. Helmberger T, Golfieri R, Pech M, Pfammatter T, Arnold D, Cianni R, et al. Clinical application of trans-arterial radioembolization in hepatic Malignancies in Europe: first results from the prospective multicentre observational study CIRSE registry for SIR-spheres therapy (CIRT). Cardiovasc Intervent Radiol. (2021) 44:21–35. doi: 10.1007/s00270-020-02642-y
Keywords: selective internal radiotherapy, transarterial radioembolization, Holmium-166, Holmium-166 microspheres, hepatic malignancy
Citation: Schulze-Zachau V, Verset G, De Bondt P, De Keukeleire K, Gühne F, Heuschkel M, Hoffmann R-T, Bozzi E, Sciuto R, Lam M, Deportós Moreno J, Debrus R and Zech CJ (2024) Safety and efficacy of Holmium-166 selective internal radiotherapy of primary and secondary liver cancer confirmed by real-world data. Front. Oncol. 14:1404621. doi: 10.3389/fonc.2024.1404621
Received: 21 March 2024; Accepted: 24 May 2024;
Published: 11 June 2024.
Edited by:
Francesco Tovoli, University of Bologna, ItalyReviewed by:
Chiara Mazzarelli, Niguarda Ca’ Granda Hospital, ItalyAimin Jiang, The First Affiliated Hospital of Xi’an Jiaotong University, China
Martina Stella, Medpace, United States
Copyright © 2024 Schulze-Zachau, Verset, De Bondt, De Keukeleire, Gühne, Heuschkel, Hoffmann, Bozzi, Sciuto, Lam, Deportós Moreno, Debrus and Zech. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victor Schulze-Zachau, victor.schulze-zachau@usb.ch; victor.schulze-zachau@posteo.ch