 Romain Coutelle
Romain Coutelle Nathalie Coulon
Nathalie Coulon Carmen M. Schröder
Carmen M. Schröder Olivier Putois
Olivier Putois- 1Hôpitaux Universitaires de Strasbourg, Department of Psychiatry, University of Strasbourg, Strasbourg, France
- 2INSERM 1114, Strasbourg, France
- 3TSA-SDI Expert Center and Psychosocial Rehabilitation Reference Center, Alpes Isère Hospital (Saint-Egrève Psychiatric Hospital), Grenoble, France
- 4CNRS UPR 3212, Strasbourg, France
- 5SuLiSoM UR 3071, Faculté de Psychologie, Université de Strasbourg, Strasbourg, France
- 6Institut d’Immunologie et d’Hématologie, Institut Thématique Interdisciplinaire TRANSPLANTEX NG, Université de Strasbourg, Strasbourg, France
Introduction: Autism Spectrum Disorder (ASD) diagnosis is relatively consensual in typical forms. The margins of the spectrum and their degree of extension, however, are controversial. This has far-reaching implications, which extend beyond theoretical considerations: first, peripheral forms of autism are more prevalent than central forms; second, we do not know how relevant typical-targeted recommendations are for atypical forms. In DSM-IV-TR, these margins of autism were studied within the category of Pervasive Developmental Disorder – Not Otherwise Specified (PDD-NOS). In spite of its low reliability, this former diagnosis was of particular interest to shed light on the gray area of margins. The aim of this systematic is therefore to investigate the clinical characteristics of PDD-NOS in comparison with Autistic Disorder.
Method: A stepwise systematic PRISMA literature review was conducted by searching PubMed and Web Of Science databases to select corresponding studies.
Results: The systematic review included 81 studies comprising 6,644 children with PDD-NOS. Cross-sectional and longitudinal studies comparing PDD-NOS and AD showed that PDD-NOS corresponds to milder form of autism with less impact and less associated disorder, with the exception of schizophrenia and mood disorder.
Discussion: Our review challenges initial views of PDD-NOS, and shows the clinical relevance of this diagnosis when dealing with the margins of autism, and the de facto diversity included in the spectrum. However, in view of the many limitations of PDD-NOS (low reliability, instability through time, low acceptability), we suggest taxonomic changes in DSM-5: we introduce a new category based on three main dimensions related to socialization impairment, emotional lability and psychotic symptoms.
Conclusion: Our review argues for a distinction between AD and PDD-NOS on clinical characteristics and thus highlights the need to study the margins of autism. While the limitations of the PDD-NOS category made it irrelevant to investigate these margins from a research perspective, we believe that a multidimensional approach for mental health professionals taping socialization, emotion lability and psychotic symptoms would be interesting. Our review therefore encourage future studies to test relevant criteria for a new category and possibly identify developmental trajectories, specific interventions and treatments.
Introduction
Since 2013 and the DSM-5, the diagnostic category of Autism Spectrum Disorder (ASD) has included 2 behavioral dimensions which represent the core defining features of ASD (1): (a) communication and social interaction deficits on the one hand, and (b) repetitive behaviors and restricted interests on the other hand (1). The term “ASD” suggests that the core features of the disorder can be measured dimensionally and, that they fall along a continuum of severity. No diagnostic subtypes are listed (1); instead, specifiers are provided to indicate associated dimensions, such as intellectual and/or language impairment, as well as the severity level of core ASD symptoms (2). Further, any known genetic or medical disorders are recorded and other co-occurring neurodevelopmental, mental, or behavioral disorders are indicated (2) to characterize subgroups.
In the DSM-5 (2), whatever the level of severity, even in the mildest forms, ASD symptoms are viewed as intrinsically autistic. However, to take one example, this conceptualization does not take into account the overlap between, on the one hand, some ASD symptoms, and on the other, Intellectual disability (3, 4), language impairment (5, 6), Attention Deficit/Hyperactivity Disorder (7, 8) or schizophrenia (9, 10). Moreover, mild ASD symptoms might be more akin to a natural variant of typical development than a formal disorder (11). Boundaries issues with typical development are also longitudinal, as has been shown in studies on “optimal outcome” or “Loss of Autism Diagnosis (LAD)” (12). These studies (13) focused on a group of individuals meeting criteria for ASD in childhood who no longer met them later in development. This definition entailed clear documentation of early ASD diagnosis, not meeting current diagnostic criteria (with ADOS scores similar to neurotypical peers with no history of ASD), and having overall cognitive, language, and social functioning standardized test scores within the average range (12). Confirmation that meeting criteria for ASD is not necessarily a lifelong state appears evident in the strikingly similar proportions (about 9%) of individuals experiencing LAD in prospective and retrospective studies (12). In line with the scope of our review, it is worth noticing that one study (14) showed that among ASD children included at age 2, those with PDD-NOS were significantly more likely than those with AD to move off the spectrum by age 4. ASD symptoms might be thus less specific than suspected in the DSM-5, especially in milder forms.
Envisioned in line with Kannner’s (15) first description and seminal work, autism is relatively consensual in its typical forms (full syndrome) (16). However the margins of the spectrum and their degree of extension are controversial (17) because of overlaps with other dimensions and blurred boundaries with typical development. This question is much more than a theoretical issue, since peripheral or “marginal” forms of autism might be more prevalent than central forms (see below). Furthermore, one could question the usefulness and relevance of recommendations made for typical forms when facing atypical ones. Past conceptualizations (18) contrasted the more prototypical form of autism, called “Autistic Disorder (AD),” with the margins of autism studied within the Pervasive Developmental Disorder - Not Otherwise Specified (PDD-NOS) category. Is therefore of special interest to explore these margins through the lens of this former diagnosis.
The PDD-NOS diagnosis category was first introduced in 1987 (19) to contrast with typical forms for autism labeled “Autistic Disorder” (AD). The DSM-III-R (19) states that “this category should be used when there is a qualitative impairment in the development of reciprocal social interaction and of verbal and nonverbal communication skills, but the criteria are not met for autistic disorder, schizophrenia or schizotypal or schizoid personality disorder. Some people with this diagnosis will exhibit a markedly restricted repertoire of activities and interests, but others will not.” In DSM-IV (20) and DSM-IV-TR (18), AD and PDD-NOS were included within the Pervasive Developmental Disorders (PDDs) that prelude ASD. PDDs also included Asperger Syndrome (AS), Childhood Disintegrative Disorder and Rett Syndrome (18, 20).
In DSM-IV-TR (18), the PDD-NOS category included atypical autism, i.e., presentations that did not meet the criteria for AD because of late age of onset, atypical symptomatology, or subthreshold symptomatology, or all of these. These recommendations echoed Towbin’s conceptualization (21) described in a reference textbook section published in 1997. He recommended the use of PDD-NOS in 4 indications: (a) as a temporary diagnosis when data are lacking or when the child is too young; (b) to designate a mild form of ASD; (c) in the case of late age of onset of autistic symptoms; (d) to depict a clinical picture with early symptom onset and impairment in social reciprocity (21). In terms of diagnostic use, the PDD-NOS, often envisioned as a diagnosis of subthreshold autism, seems to cover a wide range of clinical variability, sometimes referred to as heterogeneity; it would benefit from being studied in a more positive manner, by drawing on its clinical diversity (22).
Epidemiological studies show that at least half of PDD were PDD-NOS. In 2005, Fombonne (23) found a PDD-NOS prevalence of 37.1 per 10,000 for a PDD prevalence of 63 per 10,000 and an AD prevalence of 13 per 10,000. In 2010 in the United States, the results of the Centers for Disease Control and Prevention (CDC) showed a PDD prevalence of 14.6 per 1,000 in a population of 363,749 8-year old children (24). PDD-NOS were 46% of the PDD, AD 43% and AS 11%. Noticeably, between 2006 and 2010 the distribution of AD and PDD-NOS has not undergone substantial changes (24).
The diagnosis of PDD-NOS had a low inter-rater reliability. The inter-rater reliability was good to excellent (k from 0.95 to 0.67) for the distinction between PDD and non-PDD. However, the disentanglement of different subtypes of PDD was much less reliable (k from 0.18 to 0.65) (25–27). The DSM-IV-TR criteria were therefore more successful in differentiating PDD (25) from other psychiatric disorders than in distinguishing between the three main subtypes of PDD, namely AD, PDD-NOS and AS (28). In line with these results, a study (29) tried to assess the variation between behavioral phenotypes and clinical diagnoses of different autism spectrum disorders across 12 university-based sites. They found that clinical distinctions among categorical diagnostic subtypes of PDDs (AD, PDD-NOS and AS) were not reliable even across sites with well-documented fidelity, using standardized diagnostic instruments (29).
In spite of its low reliability, the former diagnosis of PDD-NOS is very interesting to study the margins of autism because of both its conceptualization at the end of the spectrum, and its high prevalence. The aim of our systematic review is thus to investigate the clinical characteristics of PDD-NOS in comparison with AD. The objectives were therefore to study comparatively (in both diagnoses) synchronic and diachronic characteristics such as autism symptoms, cognitive function, daily impact, associated mental health or physical health condition and developmental trajectory from infancy to adolescence. The comparison is intended to address the distinction between the typical form and the margins of autism as well as the relevance of the PDD-NOS/AD distinction. Our study therefore aims to determine whether this distinction helps mental health professionals to account for diversity within the spectrum, and to identify divergent trajectories, better than the current ASD category.
Materials and methods
This study follows the Preferred Reporting Items for Systematic Reviews and Meta-analyses reporting guidelines (PRISMA) (30).
Search strategy and selection criteria
A stepwise systematic literature review (30) was conducted by searching PubMed, MEDLINE, and Web Of Science databases for published peer-reviewed papers using the following keywords: “PDD-NOS” OR “Pervasive Developmental Disorder Not Otherwise Specified” from January first 1987 (the year of the DSM-III-R publication, introducing this diagnostic category for the first time) to June 16th 2022. The keywords were screened in the titles and abstracts.
Eligibility criteria
Inclusion criteria
To be included in this review, the articles had to meet all following criteria: (a) include children and/or adolescents (31), (b) compare toddlers, children or adolescents with PDD-NOS with children with AD (c) be published in English, (d) use a quantitative design. RC and OP applied the eligibility criteria and screened the records to select included studies.
Exclusion criteria
The following exclusion criteria were used: (a) no reviews, comments or clinical cases, (b) methodological features: number of participants included in the AD or the PDD-NOS groups ≤10, adults included only, lack of comparison group, comparison with a group different from AD (e.g., AS), participants whose diagnosis has been confirmed by a classification other than the DSM-III or the DSM-IV, test validation studies, (c) epidemiological data in order to focus on mostly clinical well-characterized populations, (d) therapeutic trials, (e) anatomical, biological or fMRI studies (isolated, contradictory and/or non-replicated results) are (difficult to interpret), (f) language other than English, and (g) qualitative studies.
Outcome measures and data extraction
The following variables were extracted: First author (second, third author and journal if needed to distinguish from other studies); Year of publication; Sample Size; Age (mean ± SD); Sex (% Males); Functioning level when available and when age at inclusion (at baseline in longitudinal studies) > 6 y.o. (to assess comorbid ID); Objective; Design of the Study; Methods (only with longitudinal studies); Main assessment tools; Results.
Quality assessment
All included studies were observational, with a similar comparative framework. Quality assessments in such observational studies is controversial, with no clear agreement on rating methods (32). We therefore did not assess quality.
Results
Database
Our search from 1987 to 2022, undertaken on June 16th 2022, found 510 articles on PubMed and 431 on Web of Science. After manually removing all duplicates, 681 references remained. Based on their titles and abstracts, 256 papers were excluded for lack of relevance as they displayed no separate groups for AD and PDD-NOS. Most of these articles focused on PDDs (not PDD-NOS), ASD or grouped PDD-NOS, AD and/or AS into common groups. Other articles studied PDD-NOS in specific groups such as X-Fra, cerebral palsy, Down Syndrome... Our search strategy yielded 425 full-text articles assessed for eligibility. After conducting a full-text analysis of all these papers and excluding those not meeting our inclusion criteria, we ended up with 81 relevant studies, 67 of which were cross-sectional and 14 longitudinal.
Studies
A total of 6,644 children with PDD-NOS and 11,156 children with AD were included. 47 studies were from the United States (58%), 12 from Netherlands (15%), 5 from Turkey (6%), 3 from Italy (4%), and 3 from Sweden (4%) The mean age in each group (when available) was 5.85 and 5.84 years, respectively. The mean age was low because many studies included toddlers or/and pre-schoolers with PDD-NOS (52%). Sex was not systematically specified in each group. Based on available data, PDD-NOS groups comprised 75.1% of males. IQ was not always specified, in particular in studies in toddlers or preschoolers. Based on available IQ measures, average IQ was 81.93.
Within the 67 selected cross-sectional studies, we distinguished those relating to (a) autism symptoms (22 studies), (b) perinatal, developmental and functional aspects (31 studies), (c) associated mental health conditions (14 studies) and (d) associated physical health conditions (6 studies). We chose these categories in part because they best served our goal, of investigating the clinical characteristics (autism symptoms, associated conditions/dimensions, developmental trajectories and adaptive behavior) of PDD-NOS in comparison with AD, and in part because they were those that best matched selected studies. All cross-sectional studies could be included in these three categories. As explained above, 14 longitudinal studies were also selected (Figure 1).
Figure 1. PRISMA flowchart.
The total number of the studies presented in the corresponding tables (Tables 1–5) is 87 and not 81 because Carigi et al.’s study informed the 4 domains, and was thus selected in the corresponding categories (33). Walker et al. study informed 2 domains (34). Finally, Mandy et al.’s study informed 3 domains (35).
Table 1. Autism symptoms in PDD-NOS in comparison of AD.

Table 2. Perinatal, developmental and functional aspects in PDD-NOS in comparison of AD.
Table 3. Associated mental health conditions in PDD-NOS in comparison with AD.
Table 4. Associated physical health conditions in PDD-NOS in comparison with AD.
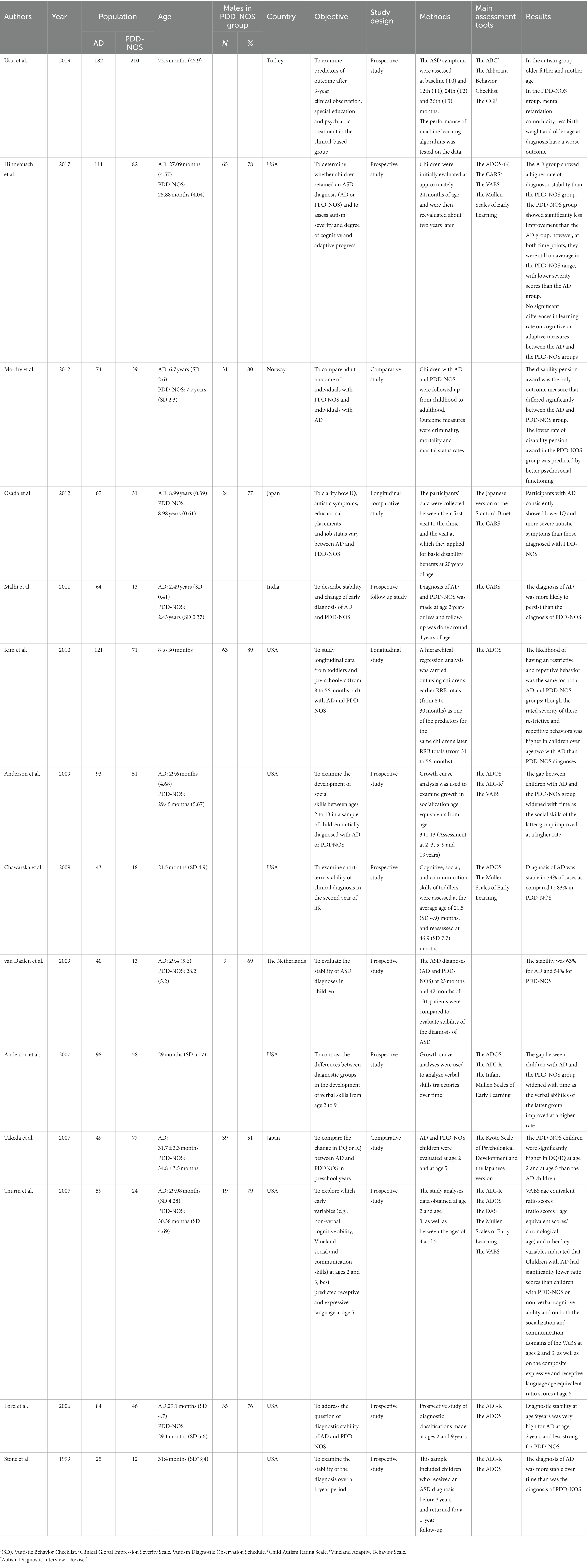
Table 5. Longitudinal studies comparing developmental trajectories in AD and PDD-NOS.
Cross-sectional studies
Autism symptoms
Studies on autism symptoms in PDD-NOS in comparison with AD deeply investigated the social-communication domain. 13 studies (33, 34, 36–46) (Table 1) showed a lesser socialization impairment whereas 3 studies (including one on gaze performance) (47–49) did not show any differences (Table 1).
7 studies found lower restrictive and repetitive behaviors (34, 35, 42, 43, 46, 50, 51) (Table 1). However, 3 studies did not show such a difference (33, 41, 52) (Table 1).
The mean age of onset of parental concerns in the group with AD was comparable to that reported in the PDD-NOS group (53). These parental concerns in PDD-NOS referred to non-specific problems linked to sleeping, eating, and level of activity (53).
Perinatal, developmental and functional aspects
Three studies (54–56) showed distinct perinatal risk factors in PDD-NOS in comparison with AD (Table 2). However, involved factors differed: hyperbilurinemia (55), higher exposure to smoking during pregnancy (56), threatened abortion, a labor duration of less than 1 h, cephalopelvic disproportion, and deliverance by an elective or emergency cesarean section (54). Even if perinatal risk factors might differ, odds ratios for birth defects were similar for AD and PDD-NOS (57).
Early development was less impacted in PDD-NOS with respect to AD (Table 2). Pointing was less impaired in PDD-NOS than in AD (33, 58). Skill loss was less frequent in PDD-NOS (58, 59). Children with AD began crawling significantly later than those with PDD-NOS (60). Using the Revised Educational Profile, Portoghese et al. showed that all behavioral areas and almost all assessed developmental domains (with the exception of the cognitive verbal) were more severely impaired in the AD group than in the PDD-NOS group (61). Children with AD and ID displayed a Visual Rooting Reflex more often than children with PDD-NOS and ID (62), suggesting less severe neurological impairments.
The investigation of language development in PDD-NOS in comparison with AD did not show any difference or particularity (63, 64) (Table 2). Also, fine and gross motor development did not differ between the 2 groups (35, 65). However, Ghaziuddin et al. found lower clumsiness in PDD-NOS (66).
Regarding socio-emotional development, social cognitive performance did not differ between both groups (67). One study shows a distinct profile of emotional information treatment in PDD-NOS in comparison with AD (68) (Table 2).
Children with PDD-NOS and AD did not differ with respect to global intellectual functioning (35, 69, 70). However, one study (35) showed higher visio-spatial performance in PDD-NOS when others did not (71, 72) (Table 2).
Executive functions lead to contradictory results, showing lesser impairment in PDD-NOS (73, 74) or no difference (75) (Table 2).
Sensory profile did not differ between the two groups (76).
Adaptive function was higher in PDD-NOS in 2 studies (34, 77). However, other studies did not show any difference (78, 79) (Table 2).
Quality of life of children and parents was less impaired in the PDD-NOS groups (33, 80) (Table 2).
Only one study showed an impact of sex on AD vs. PDD-NOS (81).
Associated mental health conditions
Children with PDD-NOS showed less challenging behavior than those with AD (82–86). Symptoms related to ADHD were overrepresented in the AD group (38, 85) (Table 3). Studies showed more Conduct Disorder (87) and Oppositional Defiant Disorder (88) in the PDD-NOS group.
Anxiety led to contradictory results (Table 3). Anxiety has been shown to be higher in the AD group (83, 85, 89) or in the PDD-NOS group (90). A study investigated the interaction between diagnosis (AD or PDD-NOS) and communication deficits (91). Children with AD experienced less anxiety as communication deficits increased while children with PDD-NOS experience more anxiety as communication deficits increased highlighting distinct type of interaction (91).
Chien et al. showed that children with PDD-NOS had a higher risk for developing Schizophrenia Spectrum Disorder, Bipolar Disorder, Major Depressive Disorder than those with AD (92). These results concur with another study comparing youth with ASD attending a specialty clinic to those attending a general psychiatry clinic (88). The latter group suffered from a greater burden of psychopathologies (Major Depressive Disorder and psychosis), higher levels of dysfunction and more pharmacotherapy [cf Carigi et al. (33); Table 3].
Associated physical health conditions
Studies showed less sleep disorders in the PDD-NOS-group (33, 93, 94) but another did not (35) (Table 4). Feeding disorders were less common in the PDD-NOS group than in the AD group (35, 93, 94). However, one study did not confirm this result (85) (Table 4).
Parmeggiani et al. showed that pathological neurological examination, cerebral lesions, abnormal EEG background activity and associated genetic pathologies were more common in PDD-NOS. Moreover, Epilepsy seizure in PDD-NOS had an earlier onset (2 years 8 months) and a better outcome (95).
Longitudinal studies
Longitudinal studies showed lower diagnosis stability in PDD-NOS than in AD (27, 96–99) with the exception of Chawaska et al. study (100) (Table 5).
Cognitive development was less impaired in PDD-NOS (Osada et al., Takeda et al., Thurm et al.) (101–103). However, another study did not show such a better outcome in this group (96).
As a whole, autistic symptoms were lower in the PDD-NOS group than in the AD group (96, 101) (Table 5). More specifically, studies showed better communication and socialization skill outcomes in PDD-NOS than in AD (103–105). Kim et al.’s study showed that the likelihood of having restrictive and repetitive behavior was the same for both AD and PDD-NOS groups; though the rated severity of these restrictive and repetitive behaviors was higher in children over age 2 with AD than with children with a PDD-NOS diagnosis (106).
Regarding functional outcome, a study form Norway (107) showed that the disability pension award at adulthood was the only outcome measure differing significantly between the AD and PDD-NOS groups previously included during childhood.
Within the PDD-NOS group, worse outcome was associated with ID, lesser birth weight and older age at diagnosis (108). Moreover, a better psychosocial functioning during childhood predicted a lower rate of disability pension award in the PDD-NOS group (107).
Discussion
We conducted a systematic review of PDD-NOS in comparison with AD. Cross-sectional and longitudinal studies comparing PDD-NOS and AD showed a clear trend for lower communication and socialization impairment in children with PDD-NOS. Results on restrictive and repetitive behaviors were more contradictory. Early development was less impacted in PDD-NOS as well as the quality of life of children and families. Children with PDD-NOS showed less challenging behavior than those with AD. Schizophrenia and mood disorders appeared to be higher in PDD-NOS whereas feeding and sleep disorders tend to be less prevalent.
With regard to our results, PDD-NOS appeared as category both quantitatively and qualitatively distinct from AD. In a quantitative perspective, PDD-NOS was a lesser variant of autism with respect to the trajectory of autism symptoms, some associated mental and physical health conditions, or quality of life. This perspective is consistent with the spectrum approach of the DSM-5 (2) and a possible continuum between AD and PDD-NOS within ASD. However, in a qualitative perspective, PDD-NOS differed from AD because of higher associated schizophrenia and mood disorders. These results were unexpected with respect to a spectrum approach and suggest specific links between the margins of autism and other psychiatric dimensions. Our review coheres with Tsai and Ghaziuddin’s review (109) which concluded that the literature appeared to suggest that PDDNOS can be separated from AD, and, therefore, does not seem to lie on a “continuum” with that disorder. These authors recommended systematic research to settle the issue and that PDDNOS should be regarded as a separate category to facilitate ongoing research (109). In contrast, a recent systematic review on PDD-NOS (110) concluded that in regard of the limited consistency, sensibility, and stability of this disorder, it would be more consistent to include this diagnosis within ASD. Noticeably, the authors still recommended to collect information from professionals on adults who received a PDD-NOS diagnosis in childhood.
Our search on PubMed found 510 references. On the same period, from 1987 to 2022, the term “Autistic disorder” gave 24,639 references. PDD-NOS was thus referenced 48 times less than AD, and was therefore much less studied. However, the high prevalence of the PDD-NOS category demonstrates its high clinical relevance. This clinical importance of PDD-NOS in psychiatry was also emphasized by a study comparing youth with PDDs attending a specialty clinic for autism with those attending a general psychiatry clinic (88). More autism clinic youth met criteria for AD; more of those referred to the psychiatry clinic met the criteria for PDD-NOS (88). The discrepancy between the past clinical use of the PDD-NOS category and the scarcity of research in the field (in comparison with AD) might be due to the difficulty of studying the margins of autism because of their heterogeneity and complexity - which our review aimed to underline. PDD-NOS therefore illustrated a gap between clinical and research issues and the need to address heterogeneity from a research perspective. Based on research rather than clinical consideration of the PDD-NOS, the DSM-5 missed the complexity of the margins and opted for a continuum approach and ASD.
With regard to the 4 recommendations proposed by Towbin on the use of the PDD-NOS diagnosis category (21), it appears that, firstly, although PDD-NOS is related to earlier developmental disorders, the age of parental concern does not differ between AD and PDD-NOS. The latter result suggests that the PDD-NOS is not commonly used in the case of a later age of onset of autistic symptoms. Towbin (21) and Mandy et al. (35) suggested that PDD-NOS depicted a clinical picture with early onset of symptoms, an impairment in social reciprocity and less to no restrictive and repetitive behaviors. We showed, however, the lack of clear support to the claim of lesser frequency of restrictive and repetitive behaviors in PDD-NOS. Towbin also recommended using PDD-NOS as a temporary diagnosis when data are lacking or when the child is too young (21). This recommendation concurs with less diagnostic stability in PDD-NOS in infants and pre-schoolers, as is shown by our results. Finally, our review mostly supports the recommendation referring to PDDS-NOS as a lesser variant of autism with respect to the trajectory of autism symptoms, associated mental and physical health conditions, or quality of life.
Chien et al. showed that PDD-NOS was more associated than AD with schizophrenia and mood disorder (92). This result concurs with Joshi et al.’s study comparing youth with PDDs attending a specialty clinic for autism to those attending a general psychiatry clinic (88). General psychiatry clinic youth with PDDs (with more PDD-NOS than AD) suffered from more Major Depressive Disorder and psychosis. This result echoes the results of the Sporn et al.’s retrospective study, showing that 25% of the 76 patients who reported early onset schizophrenia had a diagnosis of PDDs during their childhood, with a clear predominance of PDD-NOS (111). In a reference sample of childhood onset schizophrenia, Rapaport et al. also found a high frequency of PDD-NOS (112).
The importance of associated psychosis and mood disorder in PDDs also echoes past syndromic conceptualization such as Multiple Complex Developmental Disorder (MCDD) (113), Pathological Demand Avoidance (PDA) (114) or Multi-Dimensional Impairments (MDI) (115) which linked social impairment, emotional lability and signs of psychosis (without a diagnosis of early onset schizophrenia). These signs of psychosis referred to thought disorder (MCDD), delusions (MCDD), poor ability to distinguish fantasy from reality (MDI, PDA). It is important to stress that MCDD and PDA were initially coined to deal with heterogeneity within PDD-NOS. However, both syndromes were not limited to the PDD-NOS category (116, 117).
The results of our review highlight that PDD-NOS was of great interest because of its high prevalence and clinical relevance. This diagnosis was useful to take into account milder forms of autism. However, it was less reliable and less stable through time than AD. Moreover, a qualitative study emphasized (118) that the autistic community might not acknowledge this diagnosis. This study was a phenomenological analysis of discussion forum dialog among 76 adult participants with self-reported diagnosis of AD and AS but not PDD-NOS (118). Participants constantly agreed that PDD-NOS should be removed in the DSM-5. Several participants expressed concern that the PDD-NOS diagnosis was not specific and reliable enough. They called the diagnosis “a junk category,” “a receptacle” (118).
Our review emphasized lower socio-communication impairments in PDD-NOS than in AD. In DSM-5, ASD diagnosis required three criteria out of three in this domain, namely deficits in social–emotional reciprocity, deficits in nonverbal communicative behaviors used for social interaction and deficits in developing, maintaining, and understanding relationship (2). To diagnose PDD-NOS, only two of them was required (18). It might therefore be suspected that the social and communication deficit characteristic of PDD-NOS wasn’t important enough for it to remain in the autism spectrum. A review and meta-analysis (119) showed that 70% of PDD-NOS did not meet the criteria for ASD. Another hypothesis postulated that PDD-NOS might belong to the Social Communication Disorder (SCD) diagnosis category. However, this category must meet all three criteria for the social-communication domain, as in ASD (2). Thus, it appears that PDD-NOS has been excluded from ASD and SCD.
Our review challenged initial views of PDD-NOS and showed that this diagnosis mostly included milder forms of autism. PDD-NOS was very clinically relevant to deal with the margins of autism and the diversity within the spectrum. However, PDD-NOS encountered too many limitations (low reliability, instability through time, low acceptability) to be retained in the DSM-5. The fact is that many PDD-NOS did not join either ASD or SCD. Thus, in order to take into account past research on PDD-NOS and the margin of autism, we argue for the creation of a new category alongside ASD and SCD, based on three main dimensions related to socialization impairment, emotional lability and psychotic symptoms and coined on PDA, MCDD and MDI. Criteria for this new category could be selected from the most valid criteria for these three syndromes and tested against the ASD criteria, to ensure that they are truly distinct. In our view, this new category would provide an opportunity for mental health professionals, along with SCD and ASD, to better take into account the neurodevelopmental disorders that have an impact on the development of social communication and its heterogeneity. From a clinical point of view, this new category would trigger the search for associated psychotic symptoms or emotional lability that might currently be understudied by professionals. In addition, new developmental trajectories, specific interventions and treatments could be identified, which would in turn make it possible to better inform and help the people concerned and their families.
Limitations
The first limitation of our study comes from the terms selected for the database search. Few studies directly addressed differences between PDD-NOS and AD. However, when the DSM-IV-TR was in use, some studies included participants with PDDs including those with AD, PDD-NOS or another PDD subtype often compared to controls. In the latter case, PDD-NOS was only mentioned in the abstract or in the title when there was a difference within PDDs subgroups. That is why we may have over-selected references showing a difference between PDD-NOS and AD, and under-selected negative studies that did not. The second limitation is that we studied all clinical features of PDD-NOS. For example, some characteristics such as quality of life were rarely studied and were only related to two references. The third limitation is sample overlap between studies, as 25% of the studies were from Matson et al. Finally, our results cannot be extended to females with PDD-NOS, individuals with PDD-NOS and ID, or adults with PDD-NOS.
Conclusion
Our systematic review shows that PDD-NOS corresponds to milder form of autism with less impact and less associated disorder, with the exception of schizophrenia and mood disorder. Our review challenges initial views of PDD-NOS, echoes past syndromic conceptualizations such as MCDD, PDA or MDI, and argues for a quantitative and qualitative distinction between AD and PDD-NOS. The PDD-NOS diagnosis was very clinically relevant to deal with the margins of autism and the diversity within the spectrum, and therefore massively used by professionals in the field. However, PDD-NOS had many limitations (low reliability, instability through time, low acceptability) and was therefore understudied, thereby generating a discrepancy between clinical and research issues. Thus, in order to overcome this gap and to take into account past research on PDD-NOS, we suggest taxonomic changes in DSM-5, through the introduction of a new category based on three main dimensions: socialization impairment, emotional lability and psychotic symptoms. Future studies are therefore needed to test relevant criteria for this new category and possibly identify developmental trajectories, specific interventions and treatments.
Author contributions
RC and OP designed the systematic review and selected the studies following PRISMA guidelines. OP was contributed mainly in epistemological and methodological. RC wrote the first complete draft of the manuscript. OP, NC, and CS provided substantial modification to the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ASD, Autism Spectrum Disorder; ADHD, Attention Deficit Hyperactivity Disorder; DSM, Diagnostic and Statistical Manual; ID, Intellectual Disability; MCDD, Multiple Complex Developmental Disorder; MDI, Multi-Dimensional Impairments; PDA, Pathological Demand Avoidance; PDDs, Pervasive Developmental Disorders; PDD-NOS, Pervasive Developmental Disorder - Not Otherwise Specified; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SCD, Social Communication Disorder.
References
1. Ousley, O, and Cermak, T. Autism Spectrum disorder: defining dimensions and subgroups. Curr Dev Disord Rep. (2014) 1:20–8. doi: 10.1007/s40474-013-0003-1
2. American Psychiatric Association. DSM-5: Diagnostic and statistical manual of mental disorders. fifth ed. Washington, DC: American Psychiatric Association (2013).
3. Thurm, A, Farmer, C, Salzman, E, Lord, C, and Bishop, S. State of the field: differentiating intellectual disability from autism Spectrum disorder. Front Psych. (2019) 10:526. doi: 10.3389/fpsyt.2019.00526
4. Vaan, G, Vervloed, M, Knoors, H, and Verhoeven, L. “Autism Spectrum disorders in people with sensory and intellectual disabilities–symptom overlap and differentiating characteristics.” Intech. (2013). p. 477–498.
5. Félix, J, Santos, ME, and Benitez-Burraco, A. Specific language impairment, autism Spectrum disorders and social (pragmatic) communication disorders: is there overlap in language deficits? A review. Rev J Autism Dev Disord. (2022) 4:1–21. doi: 10.1007/s40489-022-00327-5
6. Taylor, LJ, Maybery, MT, Grayndler, L, and Whitehouse, AJO. Evidence for shared deficits in identifying emotions from faces and from voices in autism spectrum disorders and specific language impairment. Int J Lang Commun Disord. (2015) 50:452–66. doi: 10.1111/1460-6984.12146
7. Antshel, KM, and Russo, N. Autism Spectrum disorders and ADHD: overlapping phenomenology, diagnostic issues, and treatment considerations. Curr Psychiatry Rep. (2019) 21:34. doi: 10.1007/s11920-019-1020-5
8. Taurines, R, Schwenck, C, Westerwald, E, Sachse, M, Siniatchkin, M, and Freitag, C. ADHD and autism: differential diagnosis or overlapping traits? A selective review. Atten Defic Hyperact Disord. (2012) 4:115–39. doi: 10.1007/s12402-012-0086-2
9. Barneveld, PS, Pieterse, J, de Sonneville, L, van Rijn, S, Lahuis, B, van Engeland, H, et al. Overlap of autistic and schizotypal traits in adolescents with autism Spectrum disorders. Schizophr Res. (2011) 126:231–6. doi: 10.1016/j.schres.2010.09.004
10. Pina-Camacho, L, Parellada, M, and Kyriakopoulos, M. Autism spectrum disorder and schizophrenia: boundaries and uncertainties. BJPsych Advances. (2016) 22:316–24. doi: 10.1192/apt.bp.115.014720
12. Eigsti, I-M, Fein, D, and Larson, C. Editorial perspective: another look at “optimal outcome” in autism spectrum disorder. J Child Psychol Psychiatry. (2023) 64:332–4. doi: 10.1111/jcpp.13658
13. Fein, D, Barton, M, Eigsti, I-M, Kelley, E, Naigles, L, Schultz, RT, et al. Optimal outcome in individuals with a history of autism. J Child Psychol Psychiatry. (2013) 54:195–205. doi: 10.1111/jcpp.12037
14. Sutera, S, Pandey, J, Esser, EL, Rosenthal, MA, Wilson, LB, Barton, M, et al. Predictors of optimal outcome in toddlers diagnosed with autism spectrum disorders. J Autism Dev Disord. (2007) 37:98–107. doi: 10.1007/s10803-006-0340-6
16. Mottron, L, and Bzdok, D. Autism spectrum heterogeneity: fact or artifact? Mol Psychiatry. (2020) 25:3178–85. doi: 10.1038/s41380-020-0748-y
17. Mottron, L, and Dawson, M. The autistic spectrum. Handb Clin Neurol. (2013) 111:263–71. doi: 10.1016/B978-0-444-52891-9.00029-4
18. American Psychiatric Association. DSM-IV-TR. Diagnostic and statistical manual of mental disorders fourth edition (text revision). Washington, DC: American Psychiatric Association (2000).
19. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd ed., rev. ed. Washington, DC: American Psychiatric Association (1987).
20. American Psychiatric Association. DSM-IV. Diagnostic and statistical manual of mental disorders. fourth ed. Washington, DC: American Psychiatric Association (1994).
21. Towbin, KE. Pervasive developmental disorders not otherwise specified In: Volkmar FR, Paul R, Klin A, Cohen D, editors. Handbook of autism and pervasive developmental disorders. 2nd ed. New York: J. Wiley (1997). 123–47.
22. Tincani, M, Travers, J, and Boutot, A. Race, culture, and autism Spectrum disorder: understanding the role of diversity in successful educational interventions. Res Prac Persons with Severe Disab. (2009) 34:81–90. doi: 10.2511/rpsd.34.3-4.81
23. Fombonne, E. Epidemiology of autistic disorder and other pervasive developmental disorders. J Clin Psychiatry. (2005) 66:3–8.
24. Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. (2014) 63:1–21. doi: 10.15585/mmwr.ss6706a1
25. Klin, A, Lang, J, Cicchetti, DV, and Volkmar, FR. Brief report: interrater reliability of clinical diagnosis and DSM-IV criteria for autistic disorder: results of the DSM-IV autism field trial. J Autism Dev Disord. (2000) 30:163–7. doi: 10.1023/A:1005415823867
26. Mahoney, WJ, Szatmari, P, MacLean, JE, Bryson, SE, Bartolucci, G, Walter, SD, et al. Reliability and accuracy of differentiating pervasive developmental disorder subtypes. J Am Acad Child Adolesc Psychiatry. (1998) 37:278–85. doi: 10.1097/00004583-199803000-00012
27. van Daalen, E, Kemner, C, Dietz, C, Swinkels, SHN, Buitelaar, JK, and van Engeland, H. Inter-rater reliability and stability of diagnoses of autism spectrum disorder in children identified through screening at a very young age. Eur Child Adolesc Psychiatry. (2009) 18:663–74. doi: 10.1007/s00787-009-0025-8
28. Witwer, AN, and Lecavalier, L. Examining the validity of autism Spectrum disorder subtypes. J Autism Dev Disord. (2008) 38:1611–24. doi: 10.1007/s10803-008-0541-2
29. Lord, C, Petkova, E, Hus, V, Gan, W, Lu, F, Martin, DM, et al. A multisite study of the clinical diagnosis of different autism spectrum disorders. Arch Gen Psychiatry. (2012) 69:306–13. doi: 10.1001/archgenpsychiatry.2011.148
30. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
31. Putois, O, Golse, B, Delvenne, V, and Keren, M. The complexity of psychiatric care, from pregnancy to adolescence: beyond the endogenous-exogenous dichotomy. Frontiers Research Topic. (2022). Available at: https://www.frontiersin.org/research-topics/32433/the-complexity-of-psychiatric-care-from-pregnancy-to-adolescence-beyond-the-endogenous-exogenous-dic
32. Jüni, P, Witschi, A, Bloch, R, and Egger, M. The hazards of scoring the quality of clinical trials for meta-analysis. JAMA. (1999) 282:1054–60. doi: 10.1001/jama.282.11.1054
33. Carigi, T, Muratori, F, Termine, C, Veggiotti, P, Derhemi, L, Di Nardo, R, et al. Diagnostic boundaries of autism disorder vs pervasive developmental disorder nos comparative observational study and literature review. Curr Clin Pharmacol. (2014) 9:377–86. doi: 10.2174/15748847113086660068
34. Walker, DR, Thompson, A, Zwaigenbaum, L, Goldberg, J, Bryson, SE, Mahoney, WJ, et al. Specifying PDD-NOS: a comparison of PDD-NOS, Asperger syndrome, and autism. J Am Acad Child Adolesc Psychiatry. (2004) 43:172–80. doi: 10.1097/00004583-200402000-00012
35. Mandy, W, Charman, T, Gilmour, J, and Skuse, D. Toward specifying pervasive developmental disorder-not otherwise specified. Autism Res. (2011) 4:121–31. doi: 10.1002/aur.178
36. Fodstad, JC, Matson, JL, Hess, J, and Neal, D. Social and communication behaviours in infants and toddlers with autism and pervasive developmental disorder-not otherwise specified. Dev Neurorehabil. (2009) 12:152–7. doi: 10.1080/17518420902936748
37. Hattier, MA, and Matson, JL. An examination of the relationship between communication and socialization deficits in children with autism and PDD-NOS. Res Autism Spectr Disord. (2012) 6:871–80. doi: 10.1016/j.rasd.2011.12.001
38. Horovitz, M, and Matson, JL. Communication deficits in babies and infants with autism and pervasive developmental disorder-not otherwise specified (PDD-NOS). Dev Neurorehabil. (2010) 13:390–8. doi: 10.3109/17518423.2010.501431
39. Karabekiroglu, K, and Akbas, S. Identifying and differentiating PDD-NOS: a comparison with autism and ADHD. Eur Child Adolesc Psychiatry. (2011) 20:S143–3.
40. Klin, A, Sparrow, SS, de Bildt, A, Cicchetti, DV, Cohen, DJ, and Volkmar, FR. A normed study of face recognition in autism and related disorders. J Autism Dev Disord. (1999) 29:499–508. doi: 10.1023/a:1022299920240
41. Matson, JL, Dempsey, T, and Fodstad, JC. Examination of group differences using the autism Spectrum disorders-diagnostic for children (ASD-DC). J Dev Phys Disabil. (2009) 21:235–43. doi: 10.1007/s10882-009-9138-8
42. Matson, JL, Fodstad, JC, and Dempsey, T. What symptoms predict the diagnosis of autism or PDD-NOS in infants and toddlers with developmental delays using the baby and infant screen for aUtIsm traits. Dev Neurorehabil. (2009) 12:381–8. doi: 10.3109/17518420903029501
43. Matson, JL, Dempsey, T, LoVullo, SV, Fodstad, JC, Knight, C, Sevin, JA, et al. The moderating effects of intellectual development on core symptoms of autism and PDD-NOS in toddlers and infants. Res Dev Disabil. (2013) 34:573–8. doi: 10.1016/j.ridd.2012.03.031
44. Mayes, L, Volkmar, F, Hooks, M, and Cicchetti, D. Differentiating pervasive developmental disorder not otherwise specified from autism and language disorders. J Autism Dev Disord. (1993) 23:79–90. doi: 10.1007/BF01066420
45. Sipes, M, Matson, JL, and Horovitz, M. Autism spectrum disorders and motor skills: the effect on socialization as measured by the baby and infant screen for children with aUtIsm traits (BISCUIT). Dev Neurorehabil. (2011) 14:290–6. doi: 10.3109/17518423.2011.587838
46. Verté, S, Geurts, HM, Roeyers, H, Rosseel, Y, Oosterlaan, J, and Sergeant, JA. Can the Children’s communication checklist differentiate autism spectrum subtypes? Autism. (2006) 10:266–87. doi: 10.1177/1362361306063299
47. Falck-Ytter, T, Fernell, E, Hedvall, AL, von Hofsten, C, and Gillberg, C. Gaze performance in children with autism spectrum disorder when observing communicative actions. J Autism Dev Disord. (2012) 42:2236–45. doi: 10.1007/s10803-012-1471-6
48. Kozlowski, AM, Matson, JL, and Belva, BC. Social skills differences between the autism Spectrum disorders. J Dev Phys Disabil. (2012) 24:125–34. doi: 10.1007/s10882-011-9260-2
49. Mahoney, EB, Breitborde, NJK, Leone, SL, and Ghuman, JK. An examination of social interaction profiles based on the factors measured by the screen for social interaction. Res Dev Disabil. (2014) 35:2487–94. doi: 10.1016/j.ridd.2014.06.008
50. Buitelaar, JK, Van der Gaag, R, Klin, A, and Volkmar, F. Exploring the boundaries of pervasive developmental disorder not otherwise specified: analyses of data from the DSM-IV autistic disorder field trial. J Autism Dev Disord. (1999) 29:33–43. doi: 10.1023/A:1025966532041
51. Matson, JL, Dempsey, T, and Fodstad, JC. Stereotypies and repetitive/restrictive behaviours in infants with autism and pervasive developmental disorder. Dev Neurorehabil. (2009) 12:122–7. doi: 10.1080/17518420902936730
52. Joseph, L, Thurm, A, Farmer, C, and Shumway, S. Repetitive behavior and restricted interests in young children with autism: comparisons with controls and stability over 2 years. Autism Res. (2013) 6:584–95. doi: 10.1002/aur.1316
53. Chawarska, K, Paul, R, Klin, A, Hannigen, S, Dichtel, LE, and Volkmar, F. Parental recognition of developmental problems in toddlers with autism spectrum disorders. J Autism Dev Disord. (2007) 37:62–72. doi: 10.1007/s10803-006-0330-8
54. Glasson, EJ, Bower, C, Petterson, B, de Klerk, N, Chaney, G, and Hallmayer, JF. Perinatal factors and the development of autism: a population study. Arch Gen Psychiatry. (2004) 61:618–27. doi: 10.1001/archpsyc.61.6.618
55. Juul-Dam, N, Townsend, J, and Courchesne, E. Prenatal, perinatal, and neonatal factors in autism, pervasive developmental disorder-not otherwise specified, and the general population. Pediatrics. (2001) 107:E63. doi: 10.1542/peds.107.4.e63
56. Visser, JC, Rommelse, N, Vink, L, Schrieken, M, Oosterling, IJ, van der Gaag, RJ, et al. Narrowly versus broadly defined autism spectrum disorders: differences in pre- and perinatal risk factors. J Autism Dev Disord. (2013) 43:1505–16. doi: 10.1007/s10803-012-1678-6
57. Dawson, S, Glasson, EJ, Dixon, G, and Bower, C. Birth defects in children with autism spectrum disorders: a population-based, nested case-control study. Am J Epidemiol. (2009) 169:1296–303. doi: 10.1093/aje/kwp059
58. Thurm, A, Manwaring, SS, Luckenbaugh, DA, Lord, C, and Swedo, SE. Patterns of skill attainment and loss in young children with autism. Dev Psychopathol. (2014) 26:203–14. doi: 10.1017/S0954579413000874
59. Meilleur, A-AS, and Fombonne, E. Regression of language and non-language skills in pervasive developmental disorders. J Intellect Disabil Res. (2009) 53:115–24. doi: 10.1111/j.1365-2788.2008.01134.x
60. Matson, JL, Mahan, S, Kozlowski, AM, and Shoemaker, M. Developmental milestones in toddlers with autistic disorder, pervasive developmental disorder--not otherwise specified and atypical development. Dev Neurorehabil. (2010) 13:239–47. doi: 10.3109/17518423.2010.481299
61. Portoghese, C, Buttiglione, M, Pavone, F, Lozito, V, De Giacomo, A, Martinelli, D, et al. The usefulness of the revised psychoeducational profile for the assessment of preschool children with pervasive developmental disorders. Autism. (2009) 13:179–91. doi: 10.1177/1362361308100687
62. de Bildt, A, Mulder, EJ, Van Lang, NDJ, de With, SAJ, Minderaa, RB, Stahl, SS, et al. The visual rooting reflex in individuals with autism spectrum disorders and co-occurring intellectual disability. Autism Res. (2012) 5:67–72. doi: 10.1002/aur.225
63. Huemer, SV, and Mann, V. A comprehensive profile of decoding and comprehension in autism Spectrum disorders. J Autism Dev Disord. (2010) 40:485–93. doi: 10.1007/s10803-009-0892-3
64. Kjellmer, L, Hedvall, Å, Holm, A, Fernell, E, Gillberg, C, and Norrelgen, F. Language comprehension in preschoolers with autism spectrum disorders without intellectual disability: use of the Reynell developmental language scales. Res Autism Spectr Disord. (2012) 6:1119–25. doi: 10.1016/j.rasd.2012.03.003
65. Matson, JL, Mahan, S, Fodstad, JC, Hess, JA, and Neal, D. Motor skill abilities in toddlers with autistic disorder, pervasive developmental disorder-not otherwise specified, and atypical development. Res Autism Spectr Disord. (2010) 4:444–9. doi: 10.1016/j.rasd.2009.10.018
66. Ghaziuddin, M, and Butler, E. Clumsiness in autism and Asperger syndrome: a further report. J Intellect Disabil Res. (1998) 42:43–8. doi: 10.1046/j.1365-2788.1998.00065.x
67. Buitelaar, JK, van der Wees, M, Swaab-Barneveld, H, and van der Gaag, RJ. Theory of mind and emotion-recognition functioning in autistic spectrum disorders and in psychiatric control and normal children. Dev Psychopathol. (1999) 11:39–58. doi: 10.1017/s0954579499001947
68. Begeer, S, Terwogt, MM, Rieffe, C, Stegge, H, Olthof, T, and Koot, HM. Understanding emotional transfer in children with autism spectrum disorders. Autism. (2010) 14:629–40. doi: 10.1177/1362361310378322
69. de Bruin, EI, Verheij, F, and Ferdinand, RF. WISC-R subtest but no overall VIQ–PIQ difference in Dutch children with PDD-NOS. J Abnorm Child Psychol. (2006) 34:254–62. doi: 10.1007/s10802-005-9018-3
70. Zander, E, and Dahlgren, SO. WISC-III index score profiles of 520 Swedish children with pervasive developmental disorders. Psychol Assess. (2010) 22:213–22. doi: 10.1037/a0018335
71. Hill, TL, Varela, RE, Kamps, JL, and Niditch, LA. Local processing and social skills in children with autism Spectrum disorders: the role of anxiety and cognitive functioning. Res Autism Spectr Disord. (2014) 8:1243–51. doi: 10.1016/j.rasd.2014.06.005
72. Schlooz, WAJM, and Hulstijn, W. Boys with autism spectrum disorders show superior performance on the adult embedded figures test. Res Autism Spectr Disord. (2014) 8:1–7. doi: 10.1016/j.rasd.2013.10.004
73. Blijd-Hoogewys, EMA, Bezemer, ML, and van Geert, PLC. Executive functioning in children with ASD: an analysis of the BRIEF. J Autism Dev Disord. (2014) 44:3089–100. doi: 10.1007/s10803-014-2176-9
74. Verté, S, Geurts, HM, Roeyers, H, Oosterlaan, J, and Sergeant, JA. Executive functioning in children with an autism Spectrum disorder: can we differentiate within the spectrum? J Autism Dev Disord. (2006) 36:351–72. doi: 10.1007/s10803-006-0074-5
75. Peters-Scheffer, N, Didden, R, Sigafoos, J, Green, VA, and Korzilius, H. Behavioral flexibility in children with autism spectrum disorder and intellectual disability. Res Autism Spectr Disord. (2013) 7:699–709. doi: 10.1016/j.rasd.2013.02.016
76. O’Donnell, S, Deitz, J, Kartin, D, Nalty, T, and Dawson, G. Sensory processing, problem behavior, adaptive behavior, and cognition in preschool children with autism spectrum disorders. Am J Occup Ther. (2012) 66:586–94. doi: 10.5014/ajot.2012.004168
77. Paul, R, Miles, S, Cicchetti, D, Sparrow, S, Klin, A, Volkmar, F, et al. Adaptive behavior in autism and pervasive developmental disorder-not otherwise specified: microanalysis of scores on the Vineland adaptive behavior scales. J Autism Dev Disord. (2004) 34:223–8. doi: 10.1023/b:jadd.0000022612.18116.46
78. Allen, DA, Steinberg, M, Dunn, M, Fein, D, Feinstein, C, Waterhouse, L, et al. Autistic disorder versus other pervasive developmental disorders in young children: same or different? Eur Child Adolesc Psychiatry. (2001) 10:67–78. doi: 10.1007/s007870170049
79. Perry, A, Flanagan, HE, Dunn Geier, J, and Freeman, NL. Brief report: the Vineland adaptive behavior scales in young children with autism spectrum disorders at different cognitive levels. J Autism Dev Disord. (2009) 39:1066–78. doi: 10.1007/s10803-009-0704-9
80. Kose, S, Erermis, S, Ozturk, O, Ozbaran, B, Demiral, N, Bildik, T, et al. Health related quality of life in children with autism Spectrum disorders: the clinical and demographic related factors in Turkey. Res Autism Spectr Disord. (2013) 7:213–20. doi: 10.1016/j.rasd.2012.09.009
81. Volkmar, FR, Szatmari, P, and Sparrow, SS. Sex differences in pervasive developmental disorders. J Autism Dev Disord. (1993) 23:579–91. doi: 10.1007/BF01046103
82. Horovitz, M, Matson, JL, Rieske, RD, Kozlowski, AM, and Sipes, M. The relationship between race and challenging behaviours in infants and toddlers with autistic disorder and pervasive developmental disorder-not otherwise specified. Dev Neurorehabil. (2011) 14:208–14. doi: 10.3109/17518423.2011.566596
83. Horovitz, M, Matson, JL, and Sipes, M. Gender differences in symptoms of comorbidity in toddlers with ASD using the BISCUIT-part 2. Dev Neurorehabil. (2011) 14:94–100. doi: 10.3109/17518423.2010.546825
84. Kozlowski, AM, and Matson, JL. An examination of challenging behaviors in autistic disorder versus pervasive developmental disorder not otherwise specified: significant differences and gender effects. Res Autism Spectr Disord. (2012) 6:319–25. doi: 10.1016/j.rasd.2011.06.005
85. Matson, JL, Fodstad, JC, Mahan, S, and Sevin, JA. Cutoffs, norms, and patterns of comorbid difficulties in children with an ASD on the baby and infant screen for children with aUtIsm traits (BISCUIT-part 2). Res Autism Spectr Disord. (2009) 3:977–88. doi: 10.1016/j.rasd.2009.06.001
86. Sipes, M, Matson, JL, Horovitz, M, and Shoemaker, M. The relationship between autism spectrum disorders and symptoms of conduct problems: the moderating effect of communication. Dev Neurorehabil. (2011) 14:54–9. doi: 10.3109/17518423.2010.532850
87. Gjevik, E, Eldevik, S, Fjæran-Granum, T, and Sponheim, E. Kiddie-SADS reveals high rates of DSM-IV disorders in children and adolescents with autism spectrum disorders. J Autism Dev Disord. (2011) 41:761–9. doi: 10.1007/s10803-010-1095-7
88. Joshi, G, Faraone, SV, Wozniak, J, Petty, C, Fried, R, Galdo, M, et al. Examining the clinical correlates of autism spectrum disorder in youth by ascertainment source. J Autism Dev Disord. (2014) 44:2117–26. doi: 10.1007/s10803-014-2063-4
89. Davis, TE, Fodstad, JC, Jenkins, WS, Hess, JA, Moree, BN, Dempsey, T, et al. Anxiety and avoidance in infants and toddlers with autism spectrum disorders: evidence for differing symptom severity and presentation. Res Autism Spectr Disord. (2010) 4:305–13. doi: 10.1016/j.rasd.2009.10.002
90. Snow, AV, and Lecavalier, L. Comparing autism, PDD-NOS, and other developmental disabilities on parent-reported behavior problems: little evidence for ASD subtype validity. J Autism Dev Disord. (2011) 41:302–10. doi: 10.1007/s10803-010-1054-3
91. Davis, TE, Moree, BN, Dempsey, T, Reuther, ET, Fodstad, JC, Hess, JA, et al. The relationship between autism spectrum disorders and anxiety: the moderating effect of communication. Res Autism Spectr Disord. (2011) 5:324–9. doi: 10.1016/j.rasd.2010.04.015
92. Chien, Y-L, Wu, C-S, and Tsai, H-J. The comorbidity of schizophrenia Spectrum and mood disorders in autism Spectrum disorder. Autism Res. (2021) 14:571–81. doi: 10.1002/aur.2451
93. Gok, S, Ozturk, SN, Karaca, R, İlbars, S, and Nogay, NH. Evaluation of sleep disturbances, gastrointestinal problems and eating behaviors in Turkish children with autistic disorder and PDD-NOS. Advan Autism. (2020) 7:101–13. doi: 10.1108/AIA-12-2019-0049
94. Kozlowski, AM, Matson, JL, Belva, B, and Rieske, R. Feeding and sleep difficulties in toddlers with autism spectrum disorders. Res Autism Spectr Disord. (2012) 6:385–90. doi: 10.1016/j.rasd.2011.06.012
95. Parmeggiani, A, Posar, A, Antolini, C, Scaduto, MC, Santucci, M, and Giovanardi-Rossi, P. Epilepsy in patients with pervasive developmental disorder not otherwise specified. J Child Neurol. (2007) 22:1198–203. doi: 10.1177/0883073807306265
96. Hinnebusch, AJ, Miller, LE, and Fein, DA. Autism Spectrum disorders and low mental age: diagnostic stability and developmental outcomes in early childhood. J Autism Dev Disord. (2017) 47:3967–82. doi: 10.1007/s10803-017-3278-y
97. Lord, C, Risi, S, DiLavore, PS, Shulman, C, Thurm, A, and Pickles, A. Autism from 2 to 9 years of age. Arch Gen Psychiatry. (2006) 63:694–701. doi: 10.1001/archpsyc.63.6.694
98. Malhi, P, and Singhi, P. Adaptive behavior functioning in children with autism. Indian J Pediatr. (2015) 82:677–81. doi: 10.1007/s12098-015-1692-8
99. Stone, WL, Lee, EB, Ashford, L, Brissie, J, Hepburn, SL, Coonrod, EE, et al. Can autism be diagnosed accurately in children under 3 years? J Child Psychol Psychiatry. (1999) 40:219–26. doi: 10.1111/1469-7610.00435
100. Chawarska, K, Klin, A, Paul, R, Macari, S, and Volkmar, F. A prospective study of toddlers with ASD: short-term diagnostic and cognitive outcomes. J Child Psychol Psychiatry. (2009) 50:1235–45. doi: 10.1111/j.1469-7610.2009.02101.x
101. Osada, H, Tachimori, H, Koyama, T, and Kurita, H. Longitudinal developmental courses in Japanese children with autism spectrum disorder. Child Psychiatry Hum Dev. (2012) 43:895–908. doi: 10.1007/s10578-012-0301-6
102. Takeda, T, Koyama, T, and Kurita, H. Comparison of developmental/intellectual changes between autistic disorder and pervasive developmental disorder not otherwise specified in preschool years. Psychiatry Clin Neurosci. (2007) 61:684–6. doi: 10.1111/j.1440-1819.2007.01740.x
103. Thurm, A, Lord, C, Lee, L-C, and Newschaffer, C. Predictors of language acquisition in preschool children with autism spectrum disorders. J Autism Dev Disord. (2007) 37:1721–34. doi: 10.1007/s10803-006-0300-1
104. Anderson, DK, Lord, C, Risi, S, DiLavore, PS, Shulman, C, Thurm, A, et al. Patterns of growth in verbal abilities among children with autism spectrum disorder. J Consult Clin Psychol. (2007) 75:594–604. doi: 10.1037/0022-006X.75.4.594
105. Anderson, DK, Oti, RS, Lord, C, and Welch, K. Patterns of growth in adaptive social abilities among children with autism Spectrum disorders. J Abnorm Child Psychol. (2009) 37:1019–34. doi: 10.1007/s10802-009-9326-0
106. Kim, SH, and Lord, C. Restricted and repetitive behaviors in toddlers and preschoolers with autism spectrum disorders based on the autism diagnostic observation schedule (ADOS). Autism Res. (2010) 3:162–73. doi: 10.1002/aur.142
107. Mordre, M, Groholt, B, Knudsen, AK, Sponheim, E, Mykletun, A, and Myhre, AM. Is long-term prognosis for pervasive developmental disorder not otherwise specified different from prognosis for autistic disorder? Findings from a 30-year follow-up study. J Autism Dev Disord. (2012) 42:920–8. doi: 10.1007/s10803-011-1319-5
108. Usta, MB, Karabekiroglu, K, Sahin, B, Aydin, M, Bozkurt, A, Karaosman, T, et al. Use of machine learning methods in prediction of short-term outcome in autism spectrum disorders. Psychiatry Clin Psychopharmacol. (2019) 29:320–5. doi: 10.1080/24750573.2018.1545334
109. Tsai, LY, and Ghaziuddin, M. DSM-5 ASD moves forward into the past. J Autism Dev Disord. (2014) 44:321–30. doi: 10.1007/s10803-013-1870-3
110. Carbone, A, and Dell’Aquila, A. The diagnosis of “pervasive developmental disorder not otherwise specified”: a systematic literature review. Children (Basel). (2023) 10:844. doi: 10.3390/children10050844
111. Sporn, AL, Addington, AM, Gogtay, N, Ordoñez, AE, Gornick, M, Clasen, L, et al. Pervasive developmental disorder and childhood-onset schizophrenia: comorbid disorder or a phenotypic variant of a very early onset illness? Biol Psychiatry. (2004) 55:989–94. doi: 10.1016/j.biopsych.2004.01.019
112. Rapoport, J, Chavez, A, Greenstein, D, Addington, A, and Gogtay, N. Autism spectrum disorders and childhood-onset schizophrenia: clinical and biological contributions to a relation revisited. J Am Acad Child Adolesc Psychiatry. (2009) 48:10–8. doi: 10.1097/CHI.0b013e31818b1c63
113. Cohen, DJ, Paul, R, and Volkmar, FR. Issues in the classification of pervasive and other developmental disorders: toward DSM-IV. J Am Acad Child Psychiatry. (1986) 25:213–20. doi: 10.1016/S0002-7138(09)60228-4
114. Newson, E, Maréchal, KL, and David, C. Pathological demand avoidance syndrome: a necessary distinction within the pervasive developmental disorders. Arch Dis Child. (2003) 88:595–600. doi: 10.1136/adc.88.7.595
115. McKenna, K, Gordon, CT, Lenane, M, Kaysen, D, Fahey, K, and Rapoport, JL. Looking for childhood-onset schizophrenia: the first 71 cases screened. J Am Acad Child Adolesc Psychiatry. (1994) 33:636–44. doi: 10.1097/00004583-199406000-00003
116. de Bruin, EI, de Nijs, PFA, Verheij, F, Hartman, CA, and Ferdinand, RF. Multiple complex developmental disorder delineated from PDD-NOS. J Autism Dev Disord. (2007) 37:1181–91. doi: 10.1007/s10803-006-0261-4
117. Green, J, Absoud, M, Grahame, V, Malik, O, Simonoff, E, Le Couteur, A, et al. Pathological demand avoidance: symptoms but not a syndrome. Lancet Child Adolesc Health. (2018) 2:455–64. doi: 10.1016/S2352-4642(18)30044-0
118. Linton, KF, Krcek, TE, Sensui, LM, and Spillers, JLH. Opinions of people who self-identify With autism and Asperger’s on DSM-5 criteria. Res Soc Work Pract. (2014) 24:67–77. doi: 10.1177/1049731513495457
Keywords: autism spectrum disorder, pervasive developmental disorder, DSM-IV-TR, DSM-5, pathological demand avoidance, diversity, heterogeneity
Citation: Coutelle R, Coulon N, Schröder CM and Putois O (2023) Investigating the borders of autism spectrum disorder: lessons from the former diagnosis of pervasive developmental disorder not otherwise specified. Front. Psychiatry. 14:1149580. doi: 10.3389/fpsyt.2023.1149580
Edited by:
Marie Gomot, Inserm UMR1263 iBrain, FranceReviewed by:
Celia M. Rasga, National Health Institute Doutor Ricardo Jorge (INSA), PortugalAgostino Carbone, Sapienza University of Rome, Italy
Copyright © 2023 Coutelle, Coulon, Schröder and Putois. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Romain Coutelle, romain.coutelle@chru-strasbourg.fr