 Xuemin Zhao
Xuemin Zhao Linfei Liu
Linfei Liu- 1Department of Internal Medicine, Chengde Medical University, Chengde, China
- 2Sericultural Research Institute, Chengde Medical University, Chengde, China
Introduction: There are insufficient epidemiological studies on the impact of age at first sexual intercourse (AFS) and age at first live birth (AFB) on postpartum depression (PPD) in pregnant women, and the conclusions of these studies are inconsistent.
Methods: We performed a Mendelian randomization (MR) study to determine the causal relationship between AFS or AFB and the risk of PPD. The summary data were extracted from genome-wide association study (GWAS) summary datasets. We selected the instrumental variables according to the P value of exposure-related single nucleotide polymorphisms (P<5 ×10-9 for AFS and P<5 ×10-8 for AFB) and estimated the linkage disequilibrium using the clump parameter (10,000 kb, r2 < 0.001). Single nucleotide polymorphisms were considered instrumental variables that were significantly associated with exposure factors without linkage disequilibrium. The F-statistics of the instrumental variables should all be larger than 10. A random-effects model of IVW was constructed as the main method in our study.
Results and discussion: MR studies based on GWAS data revealed that both AFS (OR = 0.4, P <0.001) and AFB (OR = 0.38, P <0.001) were negatively correlated with the risk of PPD. Early AFS and early AFB should be studied as possible risk factors for PPD in the future. Public health departments should attach importance to sex education for young girls. The results of our TSMR should be verified by high-quality prospective epidemiological studies in the future.
1 Introduction
Postpartum depression (PPD) negatively impacts approximately 10-30% of mothers, with suicide accounting for approximately 20% of postpartum deaths (1, 2). In addition to having adverse effects on mothers’ health for several months or even one year, PPD may also have serious consequences for children and families (3, 4). PPD is not conducive to forming a healthy mother−child relationship which is important for child development and may affect maternal attachment, sensitivity and parenting style, making children more prone to malnutrition and delaying development (5, 6). PPD patients are at increased risk of developing depressive episodes in the future and are more likely to be diagnosed with bipolar disorder (7, 8).
Identifying the risk factors for PPD is necessary for its effective prevention. To date, various environmental or genetic risk factors that may lead to PPD have been comprehensively studied, but the etiology and pathophysiology of PPD are not fully understood (9). The powerful risk factors for PPD include a history of psychiatric illness, such as depression; gestational diabetes; risky pregnancy; domestic violence; and lack of social support (5, 10, 11).These risk factors for PPD reduce individuals’ ability to cope with crisis conditions and increase susceptibility to stress. Stress and previous adverse life events, which are associated with neuroendocrine changes, are important risk factors for PPD (12). One study showed that there was no significant relationship between PPD and the age of first labor (13). Another study suggested a nonlinear correlation between age at first birth (AFB) and the risk of PPD (14). Adolescent sexual behavior may be harmful to female adolescent health and well-being (15, 16). Therefore, we speculate that early age at first sexual intercourse (AFS) and early age at first birth (AFB) are possible risk factors for PPD.
Both AFS and AFB have an impact on health (17). In Australia, 83% of 3848 surveyed students aged 15-24 years had sexual intercourse; the median age was 16 years, and there was no significant gender difference (18). In Transky, South Africa, teenagers make up approximately 25% of all mothers. However, epidemiological studies investigating the relationship between AFB and PPD, which are sensitive to confounding factors are very limited, and the results are controversial (13, 14). Genotypes are randomly assigned from parents to children, and confounding factors cannot affect the association between genetic variations (GVs) and outcomes, which indicates that their causal sequence is reasonable (19). MR estimates the causal relationship between AFS, AFB, and PPD using single nucleotide polymorphisms (SNPs) as instrumental variables (IVs) (20).
2 Materials and methods
Analysis of our MR (the flowchart is shown in Figure 1) was conducted to determine causal relationships between exposures and outcomes. The summary data for the relationships between AFS or AFB and PPD were extracted from GWAS summary datasets. AFS-related SNP data included 406,457 individuals of European ancestry (ukb-b-6591). AFB-related SNP data included 170,498 individuals of European ancestry (ukb-b-12405). PPD-related SNP data comprised 7,604 patients and 59,601 controls of European ancestry (finn-b-O15_POSTPART_DEPR).
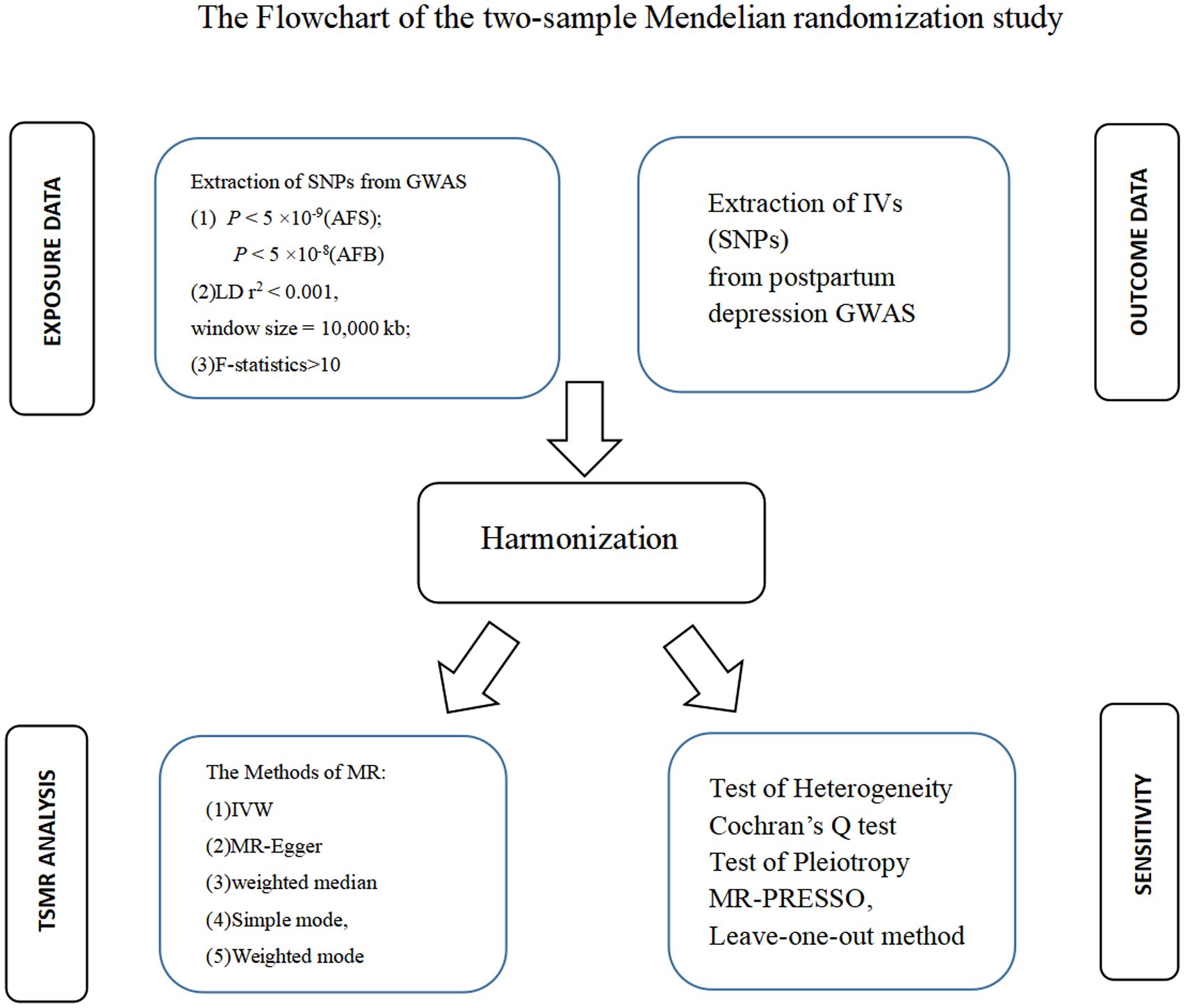
Figure 1 Flowchart of the two-sample Mendelian randomization study.
2.1 Selection of instrumental variables (IVs)
Three basic assumptions are prerequisites for completing MR: (1) IVs must be significantly correlated with the exposure. Second, IVs should influence the risk of outcomes only via exposure. Third, IVs are unrelated to any confounding factors, which are associated with exposure and the risk of outcome.
We selected the IVs according to the P value of exposure-related SNPs (P<5 ×10-9 for AFS-related SNP and P<5 ×10-8 for AFB-related SNP) and estimated the linkage disequilibrium (LD) using the clump parameter (10,000 kb, LD r2 < 0.001). SNPs were considered IVs that were significantly associated with exposure factors without LDs. The F-statistics of the IVs should be > 10, supporting that the IVs confidently predict exposure (21, 22). The IVs were not directly related to the risk of outcome (P>5 ×10-8).
2.2 Statistical analysis
We performed a statistical analysis (R version 4.2.2 software) for two-sample MR (TSMR) using the “TwoSampleMR” and “MR-PRESSO” packages. We primarily assessed the causality between AFS and the risk of PPD using a random-effects model of IVW (the main method for MR), the method of weighted median, the method of MR−Egger, the simple mode method and the weighted mode method. Underlying pleiotropy should be necessarily tested to confirm that genetic IVs are unrelated to all confounding factors associated with both AFS and the risk of PPD. Cochran’s Q test was used to detect heterogeneity between the IVs (IVW and MR Egger methods), and a value of P less than 0.05 indicated the presence of heterogeneity (POH). A nonzero intercept derived from MR−Egger regression was considered POH (P < 0.05). MR-PRESSO, which is composed of three components (global testing, outlier testing, and distortion testing), was used to detect the presence of pleiotropy (P < 0.05). The method of MR-Egger should be used as the main method for TSMR analyses in the presence of pleiotropy (23). The leave-one-out method should also be used to assess the impact of a single IV on the TSMR estimate. P < 0.05 was considered evidence of pleiotropy. Then, we assessed the causality between AFB and the risk of PPD using the same method described above.
3 Results
3.1 The causal relationship between AFS and PPD
3.1.1 TSMR analysis
The IVs of AFS were the 116 SNPs with F-statistics >10. The causal effect between AFS and the risk of PPD was revealed by the results of our TSMR as following odds ratios: (1) odds ratio = 0.4, P <0.001 (IVW); (2) odds ratio = 0.27, P =0.024 (MR-Egger); (3) odds ratio = 0.4, P <0.001 (weighted median); (4) odds ratio = 0.36, P > 0.05 (simple mode); and (5) odds ratio = 0.39, P> 0.05 (weighted mode). Significant differences were found using the three methods (MR-egger, IVW, and weighted median) (Figure 2). The results of all the five methods (ORs) are all less than 1. These results indicate that as AFS increases, the risk of PPD decreases. Therefore, we believe that early AFS leads to an increased risk of PPD (Figure 3).
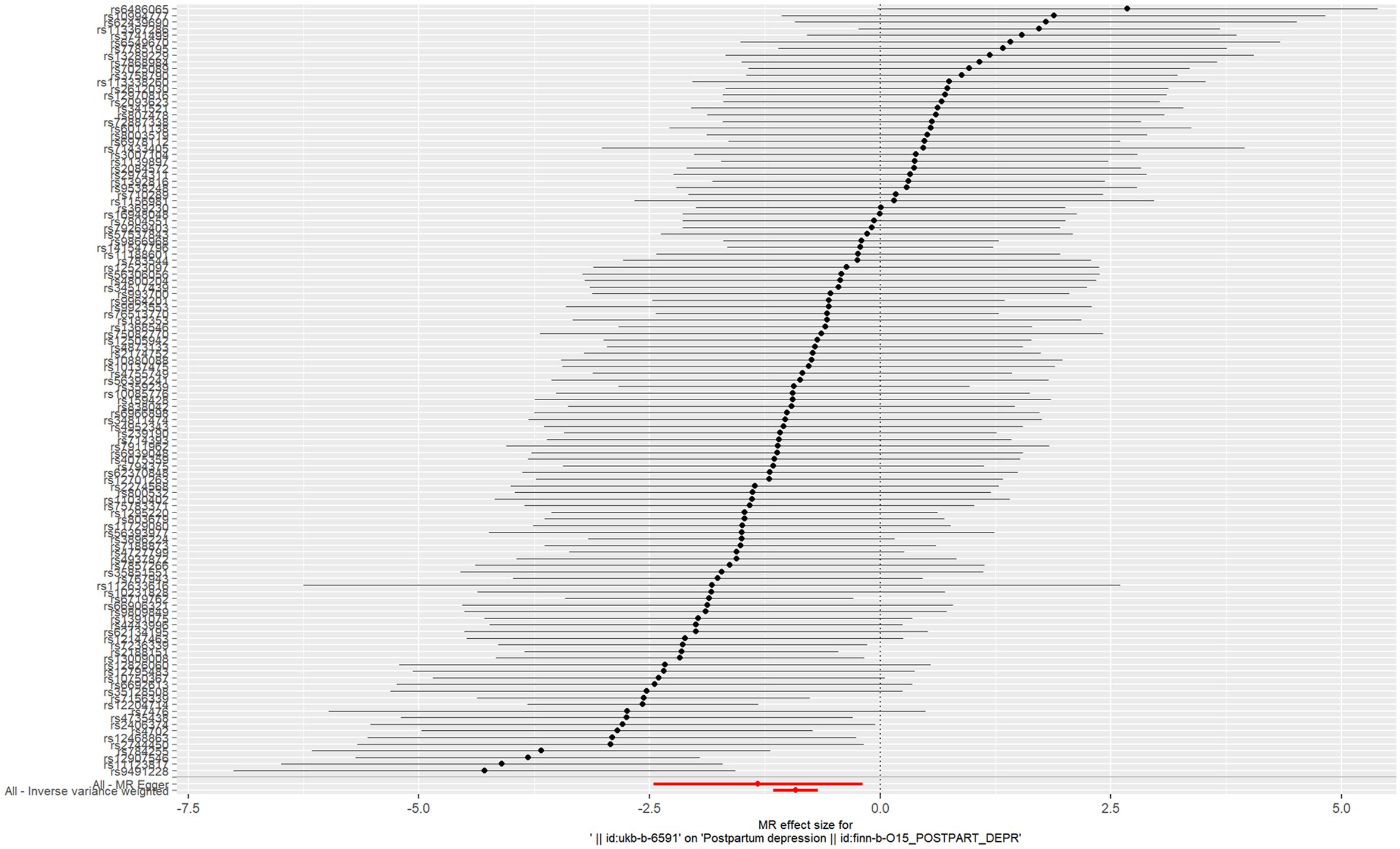
Figure 2 Forest plot of age at first sexual intercourse associated with postpartum depression.
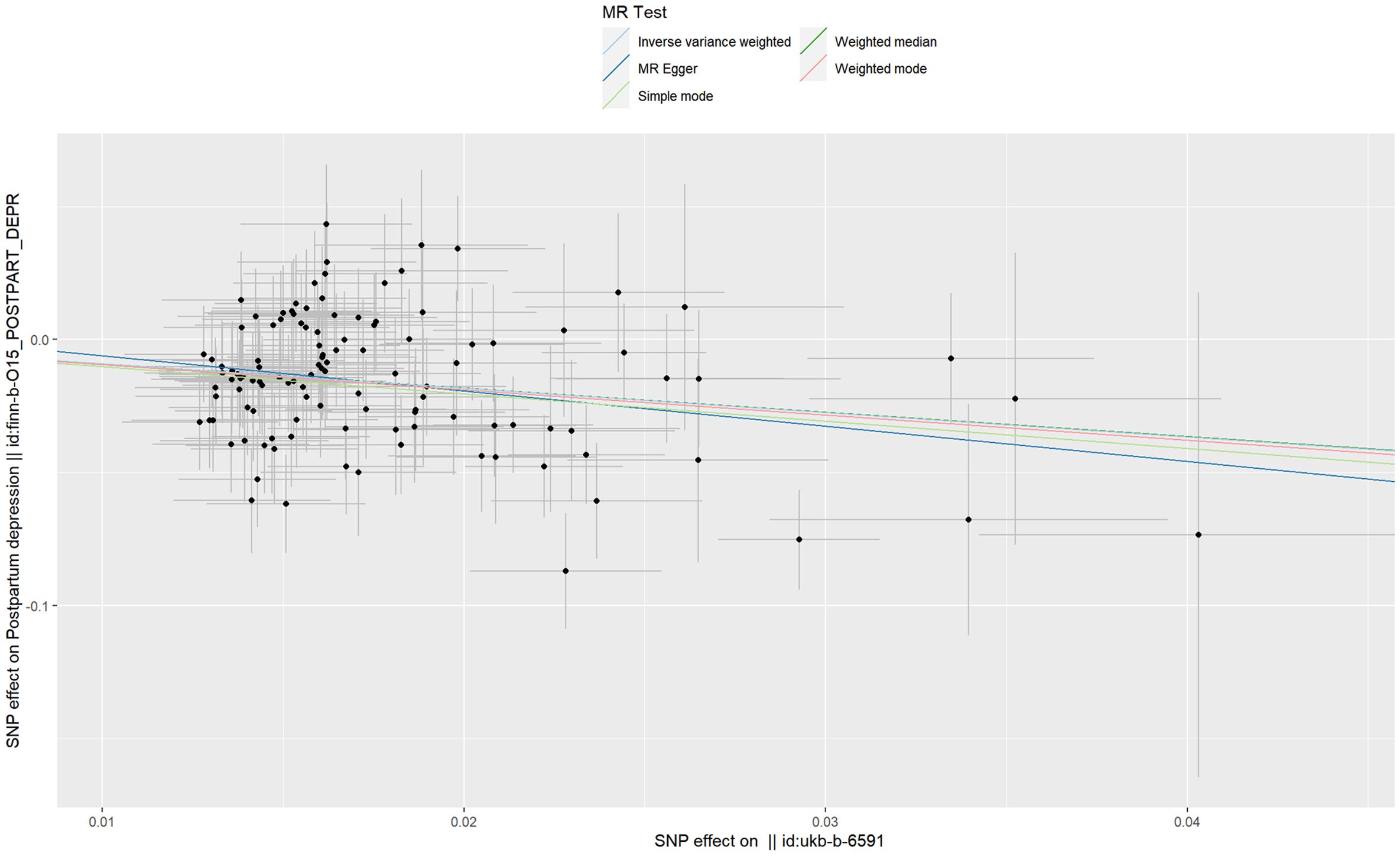
Figure 3 Scatter plot of age at first sexual intercourse associated with postpartum depression.
3.1.2 Sensitivity and pleiotropy analyses
Cochransp Q-test showed values of P less than 0.05 (0.044 for MR Egger and 0.047 for IVW), indicating that the heterogeneity among the 116 AFS-related SNPs was significant. The MR-PRESSO test confirmed that no significant pleiotropy was detected (P=0.058). Significant pleiotropy was also not found according to the intercept (P=0.472), which was obtained from the MR−Egger regression. Sensitivity analyses (leave-one-out method) were also performed. Moreover, the pooled estimate (beta) of the TSMR cannot be fundamentally impacted by each of the 116 SNPs (Figure 4). The results derived from the random-effects model of IVW about the causal relationship between AFS and PPD are robust.
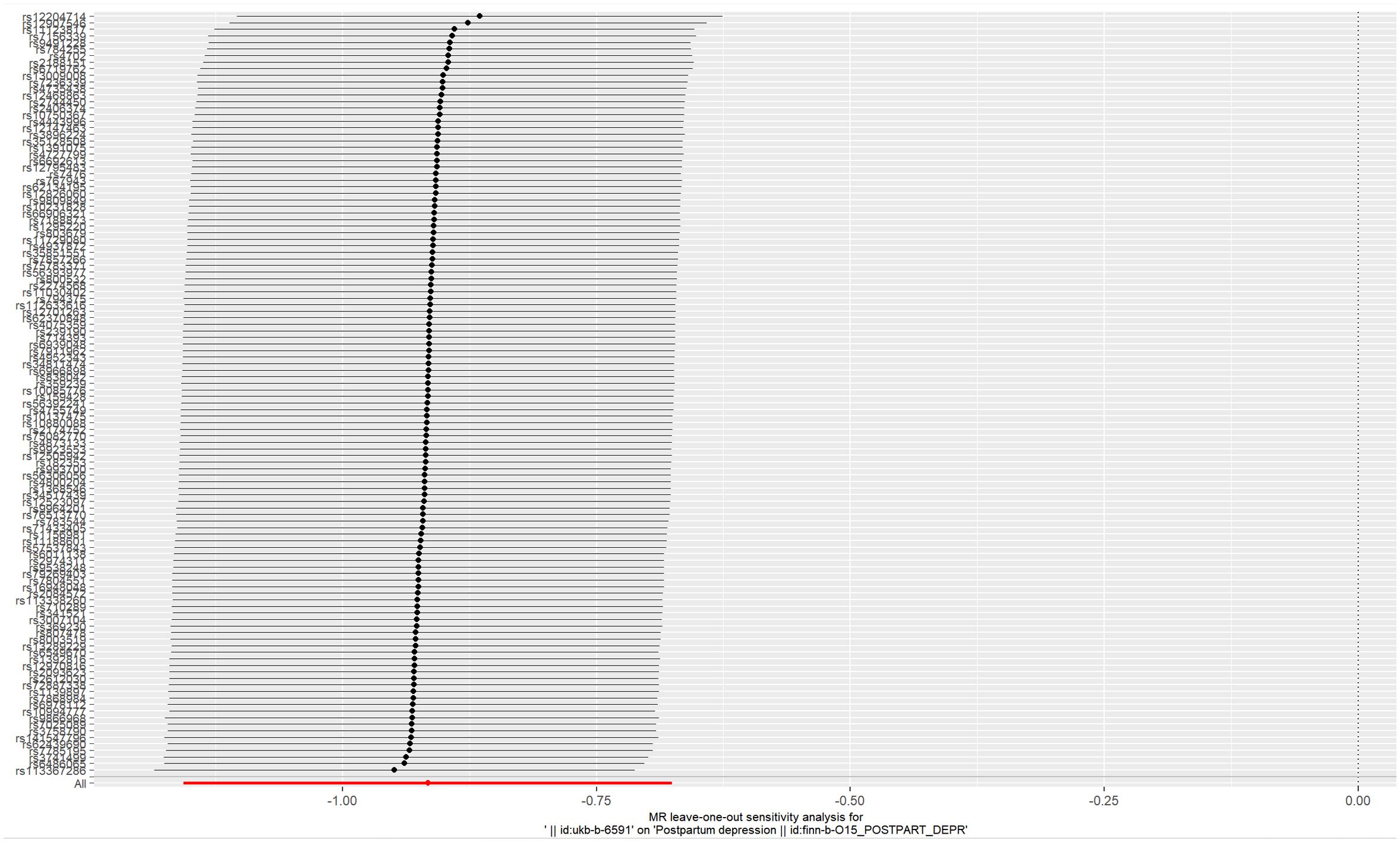
Figure 4 Plot of leave-one-out sensitivity analysis (IVW).
3.2 The causal relationship between AFB and PPD
3.2.1 TSMR analysis
The IVs of AFB were the 30 SNPs with F-statistics >10. The causal effect between AFB and the risk of PPD was revealed by the results of our TSMR as following odds ratios: (1) odds ratio = 0.38, P <0.001 (IVW); (2) odds ratio = 0.10, P = 0.04 (MR-Egger); (3) odds ratio = 0.42, P <0.001 (weighted median); (4) odds ratio = 0.40, P > 0.05 (simple mode); and (5) odds ratio = 0.43, P > 0.05 (weighted mode). Significant differences were found using the main methods (IVW) and the other two methods (MR-Egger, weighted median) (Figure 5), and the ORs of all the five methods were less than 1. These results indicate that as AFB increases, the risk of PPD decreases. Therefore, we believe that early AFB leads to an increased risk of PPD (Figure 6).
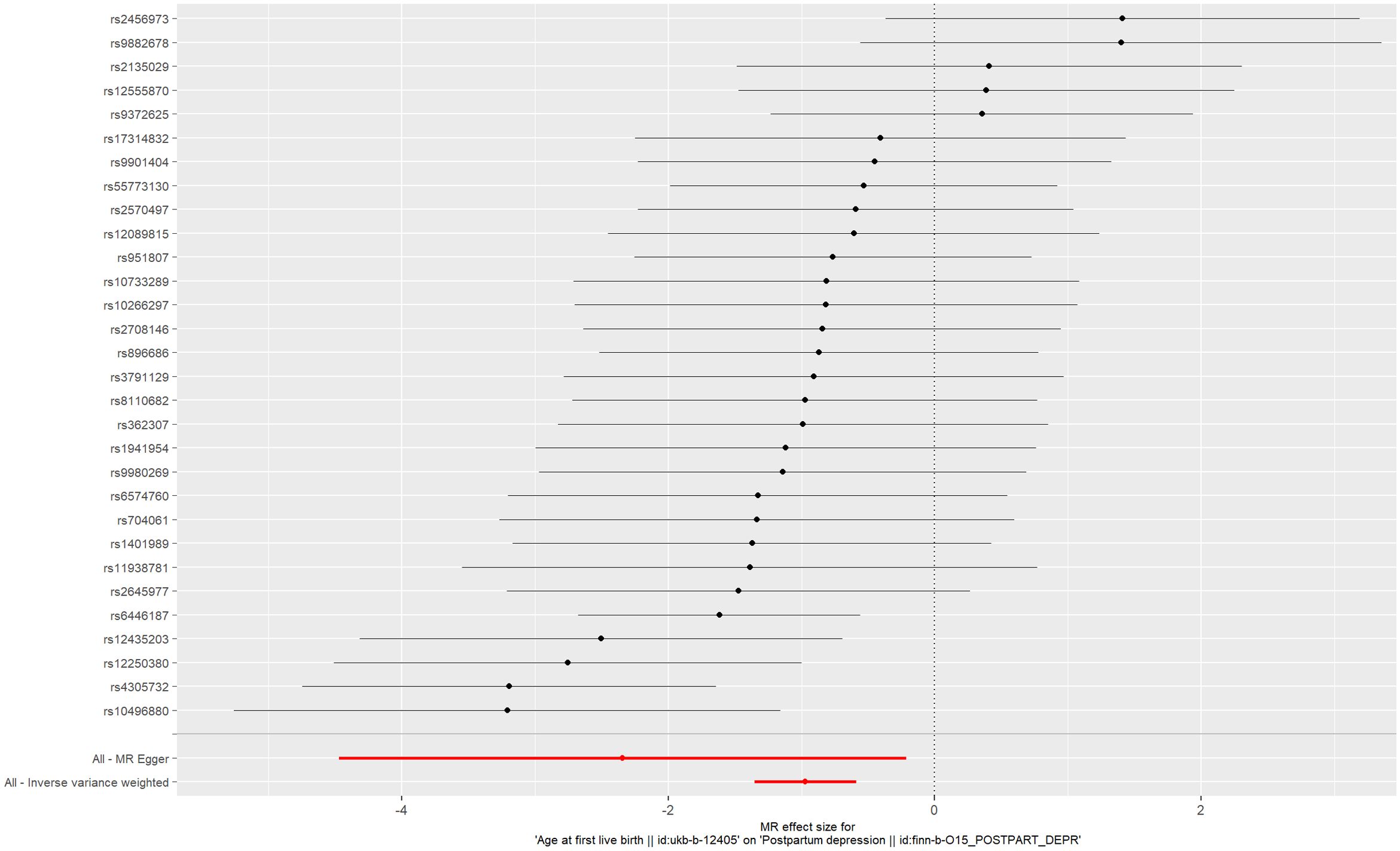
Figure 5 Forest plot of age at first live birth associated with postpartum depression.
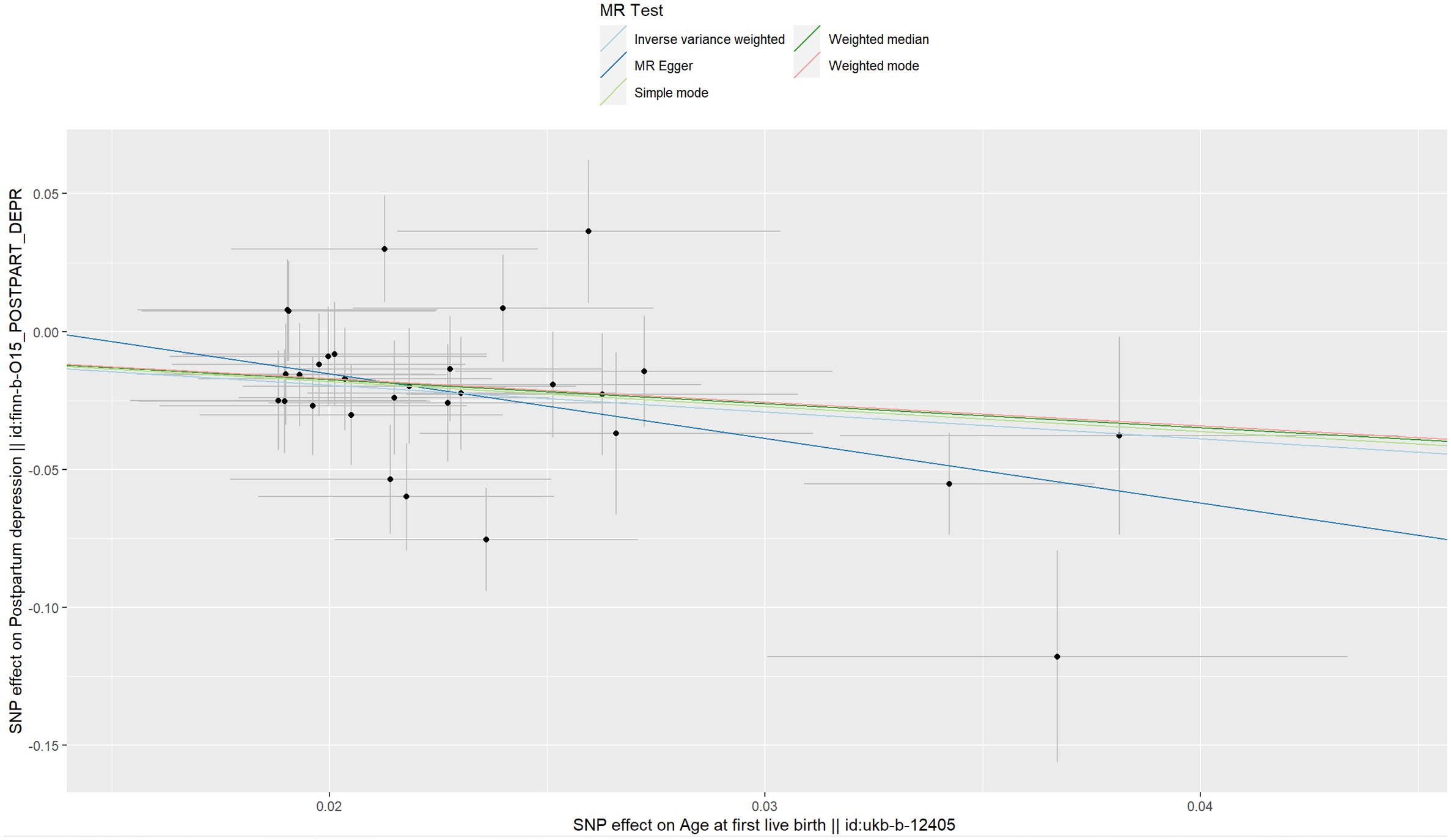
Figure 6 Scatter plot of age at first live birth associated with postpartum depression.
3.2.2 Sensitivity and pleiotropy analyses
Cochran’s Q-test showed values of P above 0.05 (0.065 for MR Egger and 0.051 for IVW), indicating that the heterogeneity between the 30 genetic variants of AFB was insignificant. The MR-PRESSO test confirmed that no significant pleiotropy was detected (P=0.066). Significant pleiotropy was also not found according to the intercept (P=0.211), which was obtained from the MR−Egger regression. Sensitivity analyses (leave-one-out method) were also performed. Moreover, the pooled estimate (beta) of the TSMR could not be fundamentally impacted by each of the 30 SNPs (Figure 7). The 30 genetic variants (SNPs) can be used as IVs for the analysis (IVW method) of TSMR. The results of our TSMR about the causal relationship between AFB and PPD are robust.
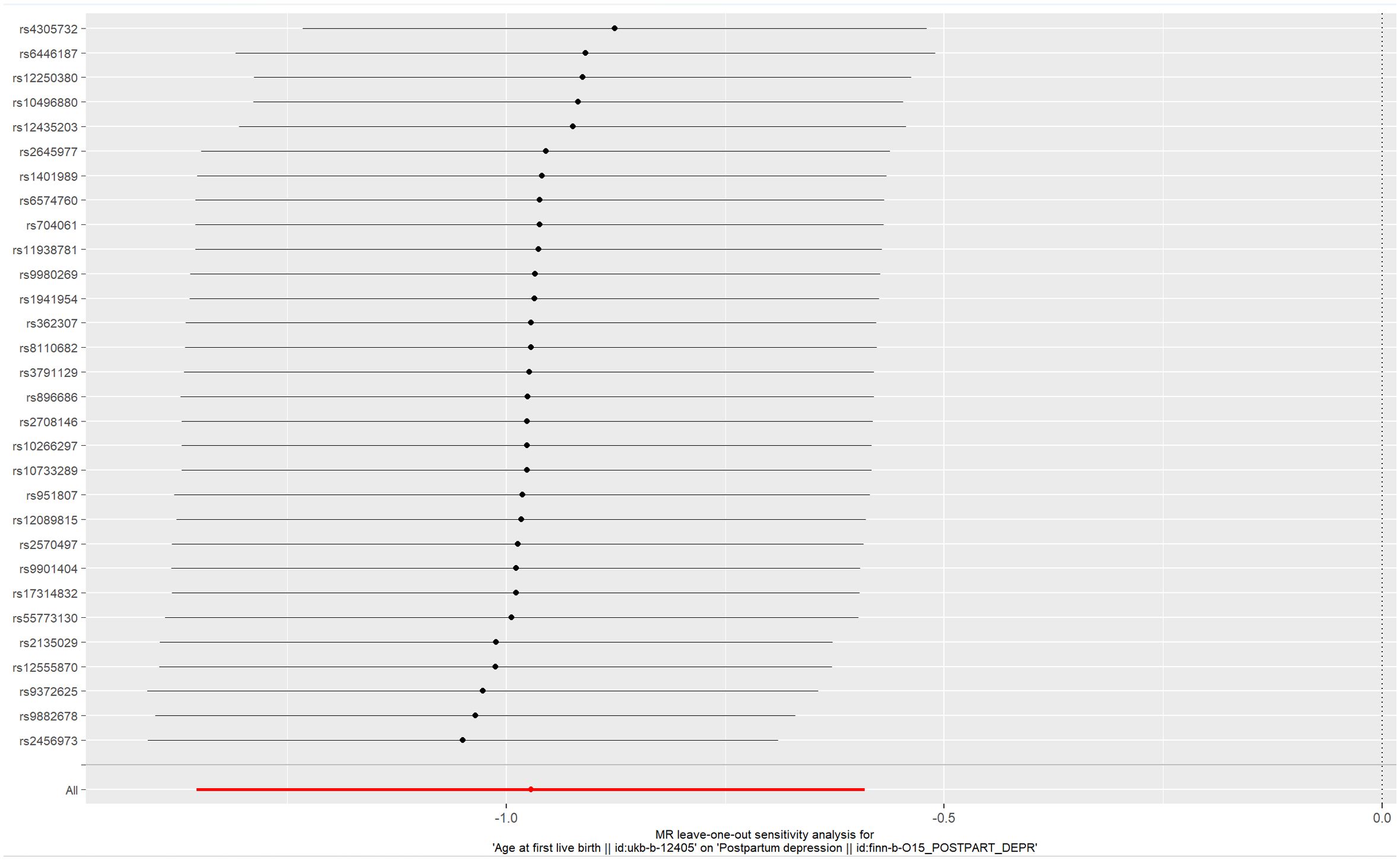
Figure 7 Plot of leave-one-out sensitivity analysis (IVW).
4 Discussion
Previous MR studies have shown that both early AFS and early AFB are risk factors for major depressive disorder (MDD) (24, 25). Most studies, including control groups of nonperinatal women, have concluded that PPD differs from nonperinatal depression in women (26, 27). There is currently no consensus about a significant clinical debate as to whether PPD differs enough from MDD to warrant a separate diagnosis, but treating early-onset PPD as a disorder different from MDD is more advantageous (28–31). PPD may present complex phenotypes of several diseases via different pathways (29). In the postpartum period, women with PPD are significantly more likely to exhibit bipolar symptoms, and bipolar PPD has a significantly earlier age of onset than unipolar depression (7, 8, 32). It is necessary to distinguish bipolar PPD from unipolar depression to help us understand the conflicting outcomes (33). Epidemiological studies have shown a negative correlation between maternal depression symptoms and maternal age (34, 35). However, another study suggested that women aged 32 and above have an increased risk of psychological distress compared to women aged 25-31 (36). Some studies also suggest that AFB is not related to PPD or exhibits a nonlinear relationship (13, 14). The exploration of causal relationships in epidemiological studies is influenced by confounding factors, such as familial confounding (37). Due to the unclear causal relationships between AFS or AFB and PPD, it is necessary to conduct a TSMR study on this controversial topic.
The causal inference between AFS, AFB, and PPD was evaluated by our TSMR study. When there was no pleiotropy, the TSMR was completed using the method of IVW (a random-effects model) as the main method (38, 39). When pleiotropy existed, we mainly used the method of MR-Egger (23). We found that both early AFS and early AFB are risk factors for PPD, and preventing early AFS is an effective way to delay early AFB. Girls who start sexual intercourse in early adolescence are more likely to conceive and have children during adolescence than girls who only start sexual intercourse during adolescence age (40). Therefore, early AFS is a more important risk factor that needs to be taken seriously. Sexual education for young girls may reduce the negative consequences of early sexual behavior (41).
There are several strengths in our study: (1) In the absence of sufficient epidemiological studies and consistent conclusions, we completed the first MR study on this issue. The results of the TSMR provides new evidence for us to understand the roles of AFS and AFB in PPD. (2) Large-scale GWAS datasets were used for our studies (397338 individuals of European ancestry for AFB and AFS, and 67205 individuals of European ancestry for PPD). (3) To obtain robust results, five computational methods (the random effects model of IVW, the method of weighted median method, the simple mode method, the method of MR−Egger, and the method of weighted mode) were used. However, several limitations should be discussed in our TMSR. (1) The results of our TSMR may not be suitable for non-European populations and should be verified in various races in the future. (2) Horizontal pleiotropy cannot be absolutely eliminated, and the results of our TSMR should be verified by high-quality prospective epidemiological studies. (3) The TSMR failed to explore the mechanism through which AFS and AFB affect PPD.
5 Conclusion
The MR study based on GWAS data revealed that both AFS (OR= 0.4, P <0.001) and AFB (OR= 0.38, P <0.001) were negatively correlated with the risk of PPD. Early AFS and early AFB should be studied as possible risk factors for PPD in the future. Public health departments should attach importance to sex education for young girls. The results of our TSMR should be verified by high-quality prospective epidemiological studies in the future.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: GWAS summary data (https://gwas.mrcieu.ac.uk/).
Author contributions
XZ: Writing – original draft, Writing – review & editing. LL: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by Initial Scientific Research Fund for High-Level Talents of Chengde Medical University (201809 and 202204).
Acknowledgments
We thank the IEU Open GWAS project (https://gwas.mrcieu.ac.uk/datasets/) for providing summary results data for the analyses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1287934/full#supplementary-material
References
1. Thirugnanasampanthar SS, Embleton L, Di Ruggiero E, Braitstein P, Oduor C, Dibaba Wado Y. School attendance and sexual and reproductive health outcomes among adolescent girls in Kenya: a cross-sectional analysis. Reprod Health. (2023) 20:29. doi: 10.1186/s12978-023-01577-0
2. Konjevod M, Gredicak M, Vuic B, Tudor L, Nikolac Perkovic M, Milos T, et al. Overview of metabolomic aspects in postpartum depression. Prog Neuropsychopharmacol Biol Psychiatry. (2023) 127:110836. doi: 10.1016/j.pnpbp.2023.110836
3. Alonazi HG, Jahan S. Prevalence of postpartum depression among women in childbearing age attending primary health care centres, Qassim Region. Health Psychol Res. (2022) 10:35642. doi: 10.52965/001c.35642
4. Alshahrani S, Al-Saleh NF, Siddiqui AF, Khalil SN, Alsaleem MA, AlHefdhi HA, et al. Burden and risk factors of postpartum depression in southwest Saudi Arabia. J Clin Med. (2023) 12(10):3444. doi: 10.3390/jcm12103444
5. Agrawal I, Mehendale AM, Malhotra R. Risk factors of postpartum depression. Cureus. (2022) 14:e30898. doi: 10.7759/cureus.30898
6. Brummelte S, Galea LA. Postpartum depression: Etiology, treatment and consequences for maternal care. Horm Behav. (2016) 77:153–66. doi: 10.1016/j.yhbeh.2015.08.008
7. Dudek D, Jaeschke R, Siwek M, Maczka G, Topor-Madry R, Rybakowski J. Postpartum depression: identifying associations with bipolarity and personality traits. Preliminary results from a cross-sectional study in Poland. Psychiatry Res. (2014) 215:69–74. doi: 10.1016/j.psychres.2013.10.013
8. Jaeschke RR, Dudek D, Topor-Madry R, Drozdowicz K, Datka W, Siwek M, et al. Postpartum depression: bipolar or unipolar? Analysis of 434 Polish postpartum women. Braz J Psychiatry. (2017) 39:154–9. doi: 10.1590/1516-4446-2016-1983
9. Luo F, Zhu Z, Du Y, Chen L, Cheng Y. Risk factors for postpartum depression based on genetic and epigenetic interactions. Mol Neurobiol. (2023) 60:3979–4003. doi: 10.1007/s12035-023-03313-y
10. Ghaedrahmati M, Kazemi A, Kheirabadi G, Ebrahimi A, Bahrami M. Postpartum depression risk factors: A narrative review. J Educ Health Promot. (2017) 6:60. doi: 10.4103/jehp.jehp_9_16
11. Liu X, Wang S, Wang G. Prevalence and risk factors of postpartum depression in women: A systematic review and meta-analysis. J Clin Nurs. (2022) 31:2665–77. doi: 10.1111/jocn.16121
12. Payne JL, Maguire J. Pathophysiological mechanisms implicated in postpartum depression. Front Neuroendocrinol. (2019) 52:165–80. doi: 10.1016/j.yfrne.2018.12.001
13. Oztora S, Arslan A, Caylan A, Dagdeviren HN. Postpartum depression and affecting factors in primary care. Niger J Clin Pract. (2019) 22:85–91. doi: 10.4103/njcp.njcp_193_17
14. Mirowsky J, Ross CE. Depression, parenthood, and age at first birth. Soc Sci Med. (2002) 54:1281–98. doi: 10.1016/s0277-9536(01)00096-x
15. Ramirez-Villalobos D, Monterubio-Flores EA, Gonzalez-Vazquez TT, Molina-Rodriguez JF, Ruelas-Gonzalez MG, Alcalde-Rabanal JE. Delaying sexual onset: outcome of a comprehensive sexuality education initiative for adolescents in public schools. BMC Public Health. (2021) 21:1439. doi: 10.1186/s12889-021-11388-2
16. Vasilenko SA. Sexual behavior and health from adolescence to adulthood: illustrative examples of 25 years of research from add health. J Adolesc Health. (2022) 71:S24–31. doi: 10.1016/j.jadohealth.2022.08.014
17. Mills MC, Tropf FC, Brazel DM, van Zuydam N, Vaez A, eQTLGen Consortium, et al. Identification of 371 genetic variants for age at first sex and birth linked to externalising behaviour. Nat Hum Behav. (2021) 5:1717–30. doi: 10.1038/s41562-021-01135-3. e QC.
18. Grunseit AC, Richters J. Age at first intercourse in an Australian national sample of technical college students. Aust N Z J Public Health. (2000) 24:11–6. doi: 10.1111/j.1467-842x.2000.tb00716.x
19. Li P, Wang H, Guo L, Gou X, Chen G, Lin D, et al. Association between gut microbiota and preeclampsia-eclampsia: a two-sample Mendelian randomization study. BMC Med. (2022) 20:443. doi: 10.1186/s12916-022-02657-x
20. Greenland S. An introduction to instrumental variables for epidemiologists. Int J Epidemiol. (2018) 47:358. doi: 10.1093/ije/dyx275
21. Pierce BL, Ahsan H, Vanderweele TJ. Power and instrument strength requirements for Mendelian randomization studies using multiple genetic variants. Int J Epidemiol. (2011) 40:740–52. doi: 10.1093/ije/dyq151
22. Ma C, Zhang W, Mao L, Zhang G, Shen Y, Chang H, et al. Hyperhomocysteinemia and intracranial aneurysm: A mendelian randomization study. Front Neurol. (2022) 13:948989. doi: 10.3389/fneur.2022.948989
23. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. (2017) 32:377–89. doi: 10.1007/s10654-017-0255-x
24. Wang Z, Lu J, Weng W, Fu J, Zhang J. Women's reproductive traits and major depressive disorder: A two-sample Mendelian randomization study. J Affect Disord. (2023) 326:139–46. doi: 10.1016/j.jad.2023.01.063
25. Lu Z, Sun Y, Liao Y, Kang Z, Feng X, Zhao G, et al. Identifying causal associations between early sexual intercourse or number of sexual partners and major depressive disorders: A bidirectional two-sample Mendelian randomization analysis. J Affect Disord. (2023) 333:121–9. doi: 10.1016/j.jad.2023.04.079
26. Johann A, Ehlert U. Similarities and differences between postpartum depression and depression at other stages of female life: a systematic review. J Psychosom Obstet Gynaecol. (2022) 43:340–8. doi: 10.1080/0167482X.2021.1962276
27. Hendrick V, Altshuler L, Strouse T, Grosser S. Postpartum and nonpostpartum depression: differences in presentation and response to pharmacologic treatment. Depress Anxiety. (2000) 11:66–72. doi: 10.1002/(sici)1520-6394(2000)11:2<66::aid-da3>3.0.co;2-d
28. Batt MM, Duffy KA, Novick AM, Metcalf CA, Epperson CN. Is postpartum depression different from depression occurring outside of the perinatal period? A review of the evidence. Focus (Am Psychiatr Publ). (2020) 18:106–19. doi: 10.1176/appi.focus.20190045
29. Di Florio A, Meltzer-Brody S. Is postpartum depression a distinct disorder? Curr Psychiatry Rep. (2015) 17:76. doi: 10.1007/s11920-015-0617-6
30. Mullard A. FDA approves first oral drug for postpartum depression, but rejects it for major depressive disorder. Nat Rev Drug Discovery. (2023) 22:774. doi: 10.1038/d41573-023-00134-5
31. Tebeka S, Gauld C, Belzeaux R, Peyre H, Dubertret C. Major depressive episode and postpartum depression: A network analysis comparison on the IGEDEPP cohort. Eur Psychiatry. (2023) 66:e51. doi: 10.1192/j.eurpsy.2023.2406
32. Sharma V, Doobay M, Baczynski C. Bipolar postpartum depression: An update and recommendations. J Affect Disord. (2017) 219:105–11. doi: 10.1016/j.jad.2017.05.014
33. Clark CT, Sit DK, Zumpf KB, Ciolino JD, Yang A, Fisher SD, et al. A comparison of symptoms of bipolar and unipolar depression in postpartum women. J Affect Disord. (2022) 303:82–90. doi: 10.1016/j.jad.2022.01.064
34. McMahon CA, Boivin J, Gibson FL, Hammarberg K, Wynter K, Saunders D, et al. Age at first birth, mode of conception and psychological wellbeing in pregnancy: findings from the parental age and transition to parenthood Australia (PATPA) study. Hum Reprod. (2011) 26:1389–98. doi: 10.1093/humrep/der076
35. Golovina K, Elovainio M, Hakulinen C. Association between depression and the likelihood of having children: a nationwide register study in Finland. Am J Obstet Gynecol. (2023) 228:211.e1– e11. doi: 10.1016/j.ajog.2022.10.016
36. Aasheim V, Waldenstrom U, Hjelmstedt A, Rasmussen S, Pettersson H, Schytt E. Associations between advanced maternal age and psychological distress in primiparous women, from early pregnancy to 18 months postpartum. BJOG. (2012) 119:1108–16. doi: 10.1111/j.1471-0528.2012.03411.x
37. Donahue KL, Lichtenstein P, Langstrom N, D'Onofrio BM. Why does early sexual intercourse predict subsequent maladjustment? Exploring potential familial confounds. Health Psychol. (2013) 32:180–9. doi: 10.1037/a0028922
38. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. (2015) 44:512–25. doi: 10.1093/ije/dyv080
39. Chen X, Kong J, Diao X, Cai J, Zheng J, Xie W, et al. Depression and prostate cancer risk: A Mendelian randomization study. Cancer Med. (2020) 9:9160–7. doi: 10.1002/cam4.3493
40. Waldron M, Heath AC, Turkheimer E, Emery R, Bucholz KK, Madden PA, et al. Age at first sexual intercourse and teenage pregnancy in Australian female twins. Twin Res Hum Genet. (2007) 10:440–9. doi: 10.1375/twin.10.3.440
Keywords: age at first birth, age at first sexual intercourse, postpartum depression, causal relationship, sex education
Citation: Zhao X and Liu L (2024) Mendelian randomization analyses for the causal relationship between early age at first sexual intercourse, early age at first live birth, and postpartum depression in pregnant women. Front. Psychiatry 15:1287934. doi: 10.3389/fpsyt.2024.1287934
Received: 08 September 2023; Accepted: 25 March 2024;
Published: 08 April 2024.
Edited by:
Shinsuke Hidese, Teikyo University, JapanReviewed by:
Kimberlyn Maravet Baig-Ward, University of Texas Southwestern Medical Center, United StatesMarcin Siwek, Jagiellonian University, Poland
Ali Montazeri, Iranian Institute for Health Sciences Research, Iran
Copyright © 2024 Zhao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuemin Zhao, zhaoxuemincmu@126.com