 Hannelore Findeis
Hannelore Findeis Maria Strauß
Maria Strauß Hans-Ludwig Kröber2
Hans-Ludwig Kröber2- 1Klinik für Psychiatrie und Psychotherapie, Universitätsklinikum Leipzig, Leipzig, Germany
- 2Institut für Forensische Psychiatrie, Charité Berlin, Berlin, Germany
Introduction: There is evidence that there is a small group of people with schizophrenia spectrum disorders who are more likely to commit homicide than those in the general population. However, there is limited knowledge about the psychopathology that leads to homicide in this group. The aim of this study was to examine two commonly used definitions of the Threat/Control-Override (TCO) concept, which aims to identify a certain risk of serious violence in patients with schizophrenia spectrum disorders.
Methods: This is a sub analysis of a file-based, retrospective and exploratory cross-sectional study. All forensic homicide offenders with schizophrenia spectrum disorders who were detained at the Forensic Hospital Berlin as of 31 December 2014 were examined for the occurrence of TCO according to two commonly used definitions.
Results: Of a total of 419 forensic patients with schizophrenia spectrum disorders, 78 committed homicide (18.6%). The forensic homicide offenders with schizophrenia spectrum disorders were characterised by being male, unemployed, single and having committed (attempted) manslaughter. Irrespective of the definition used, the entire TCO complex was present in less than a third of the sample. In both definitions, Threat symptoms were slightly less frequent than Control-Override symptoms. While Threat symptoms occurred less frequently in Stompe et al.’s definition, Control-Override symptoms were the most common. With regard to Kröber’s definition of Threat and Control-Override, the situation is exactly the opposite.
Discussion: Regarding the entire TCO complex, Kröber’s definition seems a little more open and Stompe et al.’s more strict (38.5% vs. 35.9%). Since TCO only occurs in about one third of the subjects in both definitions, neither definition appears to be conclusive. A combination with proportions from both definitions could be a contribution to a future definition of TCO. The present study provides scarcely published primary data on psychopathology in homicide offenders with schizophrenia spectrum disorders, especially on the much discussed TCO concept in two definitions. In order to determine the most useful definition of TCO, to avoid false positives and to identify clear psychopathological risk symptoms, larger samples and comparative studies with offenders and non-offenders should be conducted in the future.
1 Introduction
The global prevalence of schizophrenic psychosis is estimated to be 0.5 – 1%. In Germany, 0.5% of patients with schizophrenia spectrum disorders are admitted to a forensic psychiatric hospital according to § 63 of the German Criminal Code (Strafgesetzbuch, StGB). This represents a relatively small group of offenders, and the majority of people with schizophrenia spectrum disorders will never commit a violent crime in their lives (1). These patients are more likely to become victims of a violent crime (2). Nevertheless, several studies have shown a moderately significant association between schizophrenia and violence (3–8; and many others), especially with serious violent crime (5, 9) and homicide (10–14). These findings were replicated numerous times in various study designs, samples and social systems (15).
It is believed that about 5 – 20% of all homicide offences are being committed by patients with schizophrenia spectrum disorders (16–18).
According to the German Criminal Code, homicide is defined as a crime against human life, such as murder, manslaughter, involuntary manslaughter, induced abortion, homicide on demand and attempts to commit these crimes. Only attempted and completed murder and manslaughter were committed by the subjects of this research.
There is evidence that the paranoid subtype is the most common in violent patients with schizophrenia spectrum disorders (4). According to Schanda et al. (13), this subtype is present in 63.4% of the male and 47.1% of the female homicide offenders with schizophrenia spectrum disorders. Moreover, there is evidence that the delusional misidentification of people is associated with a higher risk of committing serious violent crime (9, 19–21). According to this, Prüter (22) found that 80% of the serious violent offences of patients with schizophrenia spectrum disorders were directly associated with their individual delusional content. This finding was confirmed by the meta-analysis and systematic review of Witt et al. (7) and the retrospective study of Swanson et al. (23).
In addition to that, comorbid personality disorders (7, 24) and substance abuse are associated with a significant higher risk of committing serious violent crime (7, 25).
In order to bring light into the nature of the serious violent and homicidal behaviour of patients with schizophrenia spectrum disorders, several authors classified the offenders and offences depending on different characteristics (26 and 27 with regards to the nature of aggression that leads to the homicide offence; 1, 28 with regards to three different types of violent offenders with schizophrenia spectrum disorders depending on their course of disease; 29 with regards to three types of offences depending on the association of psychotic symptoms, the constellation of the homicide offence and the degree of violence that leads to the homicide; 30 with regards to two different types of offenders with schizophrenia spectrum disorders depending on their development of delinquency).
As a result of their retrospective study (n = 732), Link and Stueve (31) formulated a psychopathological syndrome which they called Threat/Control-Override (TCO) as another form of classification of homicidal behaviour and homicidal offences in patients with schizophrenia spectrum disorders. It is a psychopathological constellation that places patients with schizophrenia spectrum disorders at particular risk of committing a violent crime. Threat was defined as feeling threatened by radiation or body hallucinations. Control-Override was defined as feeling controlled by an external force through thought withdrawal or thought insertion, and being at the mercy of something evil with depersonalisation and derealisation. Earlier, in the 1980s, Taylor (9) described similar findings in which schizophrenic violent criminals were characterised by a degree of florid psychotic psychopathology.
The statistically significant relationship between TCO and a higher risk of committing violent crimes among patients with schizophrenia spectrum disorders has been replicated in several studies (32–37). Swanson et al. (35) showed that patients with TCO had a twofold risk of committing violent crimes compared to psychotic patients without TCO and a fivefold risk compared to the general population. Later, Link et al. (32) showed that both Threat and Control-Override symptoms were independently associated with violent behaviour in patients with schizophrenia spectrum disorders.
On the other hand, there has been early criticism of TCO studies. Mullen (38) criticised the authors of TCO studies for producing too many false positives (TCO among non-offenders) and not discussing them sufficiently. In addition, Appelbaum et al. (39), using data from the MacArthur Violence Risk Assessment Study, found that the apparently statistically significant relationship between TCO and violent behaviour in patients with schizophrenia spectrum disorders disappeared when “anger” and “impulsivity” were included as covariates. Instead, they found that violent behaviour was associated with the absence of Control-Override symptoms.
Using data from the MacArthur Violence Risk Assessment Study, Teasdale et al. (40) found that TCO was not suitable for predicting violent behaviour in women with schizophrenia spectrum disorders. Rather, they showed that TCO was statistically significantly associated with less violent behaviour in women with schizophrenia spectrum disorders. One possible explanation for this is that men and women react differently to (delusional) threats: While males react according to “fight-or-flight”, females tend to react according to “tend-and-befriend”, which implies less violent behaviour. For males, Teasdale et al. (40) found neither a positive nor a negative relationship between violence and the full TCO concept. However, the authors did find an isolated statistically significant relationship between Threat symptoms and violent behaviour (40).
Kröber and Lau (41) concluded that validation of the TCO concept in larger samples is still needed.
The retrospective comparative study by Stompe et al. (14, 42) with delinquent and non-delinquent subjects with schizophrenia spectrum disorders showed no statistical significance regarding the prevalence of TCO in the two groups. However, when comparing three groups of subjects with schizophrenia spectrum disorders – serious violent offenders, moderate violent offenders and non-offenders – there was a statistically significant association between TCO and the serious violent offender group. However, the lifetime prevalence of TCO symptoms was rather high in all groups (serious violent offenders 97.1%; non-offenders 90.5%; moderate violent offenders 76.6%). The accumulation of TCO in the serious violent offender group was mainly attributed to Threat symptoms. These were defined as a specific form of persecutory delusion in which the patient believes that his or her life is in acute danger. The prevalence of Threat symptoms was 70.7% in serious violent offenders, 16.7% in moderate violent offenders and 46.1% in non-offenders. Control-Override symptoms were not associated with a higher risk of violent behaviour (14, 42). Nederlof et al. (43) confirmed these findings in a multicentre cross-sectional study: The statistically significant association between TCO and violent behaviour was solely due to Threat symptoms. In addition, they found that the variables “anger” and “anxiety” were also statistically significantly associated with violent behaviour.
Witt et al. (7) did not find a statistically significant relationship between TCO and violent behaviour. However, it should be noted that the authors of this study counted aggressive verbal behaviour as violent behaviour, whereas the original definition only included physical violence (31).
The contradictory findings regarding TCO and serious violent behaviour and crime could be a result of different study designs, samples, survey methods and definitions of general terms such as violence, delinquency, psychosis and TCO itself (44). In addition, most authors use three to four criteria to define TCO, which may lead to an underreporting of relevant psychopathological symptoms (43). The most common definitions of TCO in the literature are summarised in Table 1.
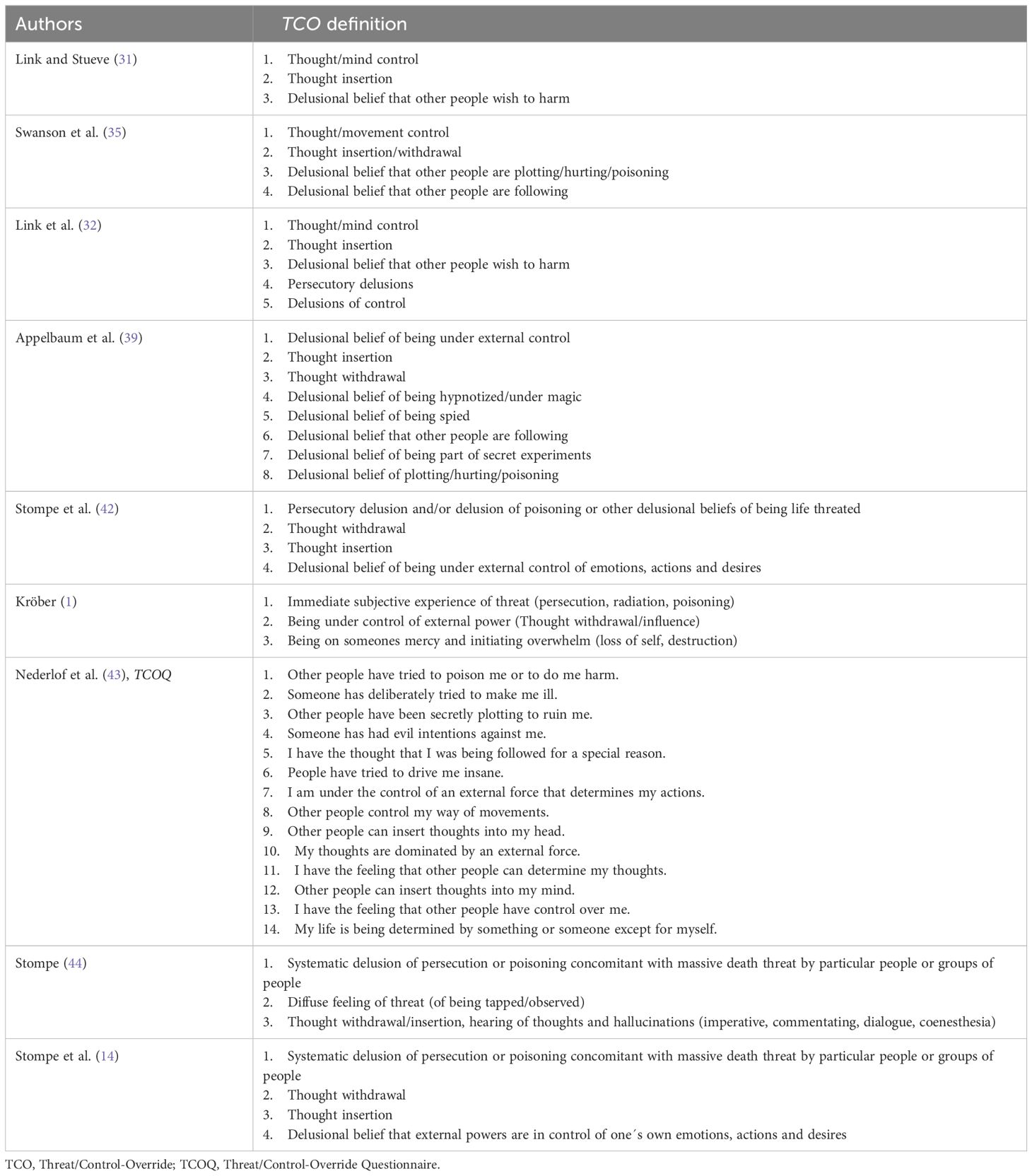
Table 1 TCO definitions.
In contrast to the definition of Swanson et al. (35), thought withdrawal, movement control and persecutory delusions are not part of the definition in the TCO concept of Link and Stueve (31). Appelbaum et al. (39) provided further information on the psychopathological symptom of movement control: The feeling of being hypnotised, trapped, spied on or followed, as well as the delusional belief of being part of secret experiments. According to Stompe (44), Threat is a systematised delusion of persecution or poisoning and the belief that one is in life-threatening danger from certain people. Like Swanson et al. (35), he distinguishes between persecutory delusions and delusions of poisoning. Following Kurt Schneider’s “Erstrang” symptoms, Stompe (44) describes the Control-Override symptoms as thought withdrawal and thought insertion, thought hearing and hallucinations (imperative, acoustic, dialogue, coenesthesia). Later, Stompe specified Threat as a serious persecutory delusion in which the patient is in a strong delusional belief of acute life-threatening danger (45).
Kröber (1) characterised TCO as a “very acute hallucinatory-paranoid syndrome” that is accompanied by an existential threat and a loss of self in a complex cognitive, emotionally aggressive situation.
Nederlof et al. (43) provided the most detailed definition of TCO to date with the Threat/Control-Override Questionnaire (TCOQ): the first six questions reflect Threat symptoms and the following eight questions reflect Control-Override symptoms (Table 1).
The TCO concept can be understood as a condensation of various typical but not specifically schizophrenic symptoms. According to the available literature, there seems to be a positive relationship between Threat and serious violent behaviour such as homicide.
A definitive definition of TCO is still lacking. For this reason, the present study aims to compare two established German-language definitions by studying a sample of homicide offenders with schizophrenia spectrum disorders who were detained at the Berlin Forensic Hospital under § 63 of the German Criminal Code (StGB) and to provide an appropriate definition of TCO.
Furthermore, a more comprehensive knowledge of the specific psychopathology of schizophrenic violence and the motivation for homicide offenders with schizophrenia spectrum disorders may not only help to identify future patients at high risk for violent behaviour, but also contribute to the destigmatisation of people with serious mental disorders (46, 47).
2 Material and methods
2.1 Study design and participants
The data in this study come exclusively from a dataset generated by the first author of this study. It is a sub analysis of a file-based, retrospective and exploratory cross-sectional study. The original study was conducted to obtain a complete overview of all forensic homicide offenders detained in the Berlin Forensic Hospital according to §§ 63 and 64 of the German Criminal Code (StGB). In this sub analysis all homicide offenders with schizophrenia spectrum disorders at the Berlin Forensic Hospital were assessed for certain sociodemographic and psychopathological variables. Diagnosis was made according to the ICD-10 (International Statistical Classification of Diseases and Related Health Problems). The sample consists exclusively of male and female subjects with schizophrenia spectrum disorders who had committed attempted or completed murder or manslaughter and who were incarcerated at the Berlin Forensic Hospital on 31 December 2014 (N = 78). The sample represents a total capture of the persons concerned.
2.2 Assessment/materials
The data were collected exclusively by the first author of the study between January 2014 and November 2015. For this purpose, the medical records of the patients from the Berlin Forensic Hospital were reviewed and both the conviction of the index offence and the forensic psychiatric examination were analysed. The medical records were reversibly pseudonymised and analysed with the approval of the Senate Administration for Justice Berlin. The protection of the data privacy of each patient was ensured according to the General Data Protection Regulation (Datenschutzgrundverordnung; (EU) 2016/679; in force since 25 May 2018). There was no personal exploration or written survey of the subjects.
The present study uses the TCO definitions of (14; Table 2) and (1; Table 3). Due to the lack of naming of concrete psychopathological symptoms in both definitions, an operationalisation was performed to transform the respective definitions of Threat and Control-Override into psychopathological symptoms that refer to the Manual for Assessment and Documentation of Psychopathology in Psychiatry (48).
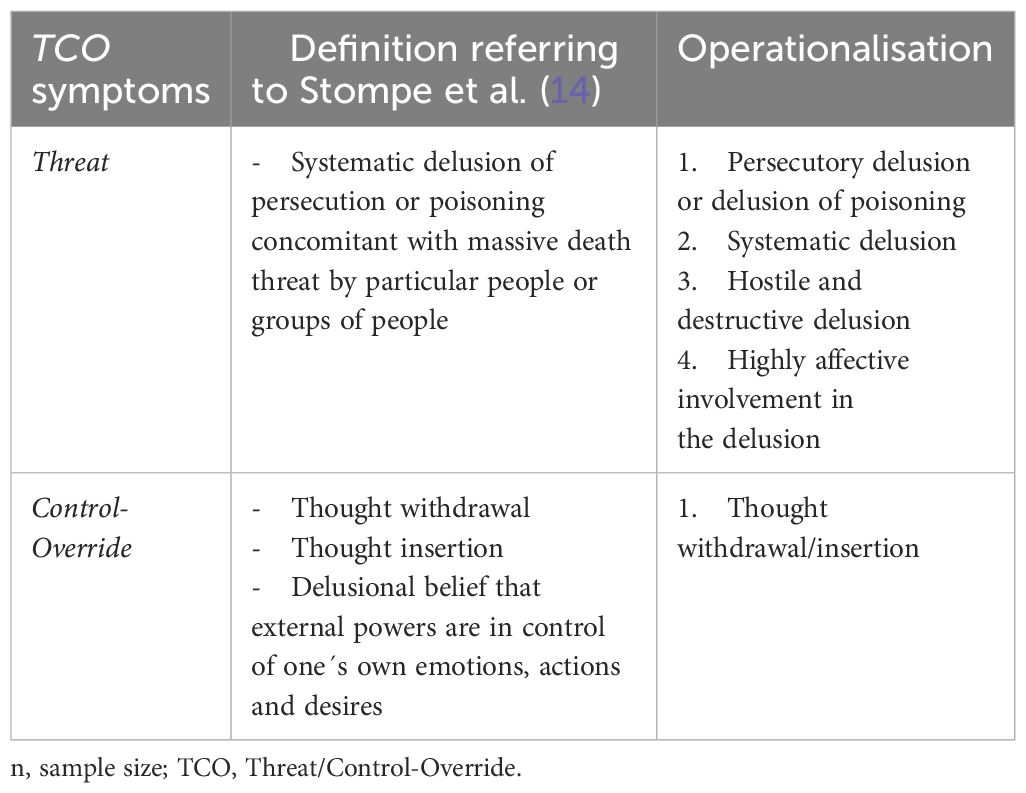
Table 2 Operationalisation of TCO symptoms referring to Stompe et al. (14).
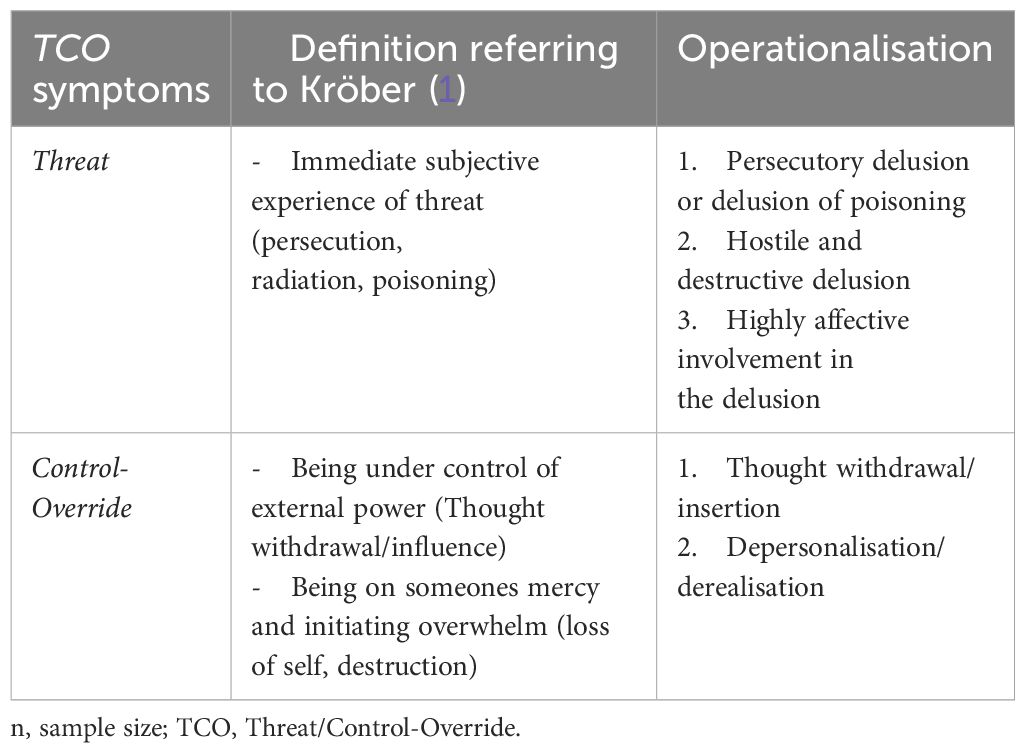
Table 3 Operationalisation of TCO symptoms referring to Kröber (1).
The definition of Stompe et al. (14) was chosen because it retrospectively compared offenders with schizophrenia spectrum disorders with moderate on the one hand and serious on the other hand, as well as with no offending at all. A statistically significant relationship with TCO was found only in the group of offenders subjects with schizophrenia spectrum disorders with serious crimes (14). Kröber (1) definition was chosen because of its precise description of common psychopathological symptoms. Threat and Control-Override were considered to be fulfilled if all attributed variables were consistent.
2.3 Analysis
The statistical analysis of the 24 variables was carried out with SPSS (IBM SPSS Statistics, for Mac, version 29.0) using descriptive statistics. Certain results are presented graphically.
3 Results
As of 31 December 2014, 419 patients with schizophrenia spectrum disorders were incarcerated in the Berlin Forensic Hospital. Of these, 78 were patients with attempted or completed homicide (18.6%). All were detained under § 63 of the German Criminal Code (StGB) and, with the exception of seven subjects with reduced criminal responsibility, all were found not guilty. Almost a quarter of the subjects committed (attempted) murder and more than three quarters committed (attempted) manslaughter. Sociodemographic variables are shown in Table 4.
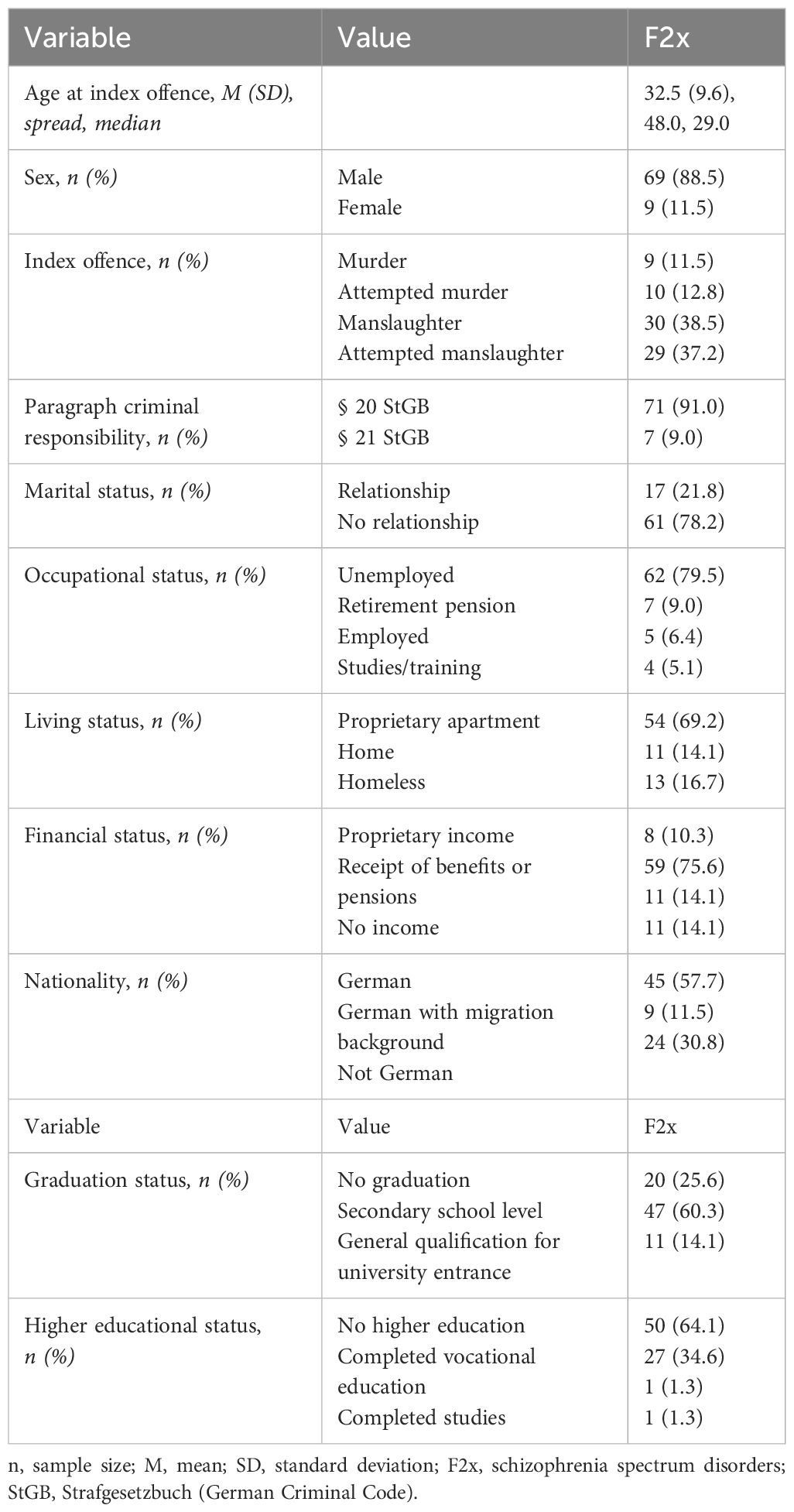
Table 4 Sociodemographic variables (n = 78).
The TCO-defining psychopathological symptoms were as follows (Table 5): systematic delusions were the most common (73.1%), followed by hostile and destructive delusions (70.5%) and highly affective involvement in the delusion (69.2%). Thought withdrawal or thought insertion (56.4%) and persecutory delusions (51.3%) occurred in just over half of the homicide offenders with schizophrenia spectrum disorders. About a third of the subjects suffered from depersonalisation and derealisation (34.6%) and less than a third from delusions of poisoning (26.9%).
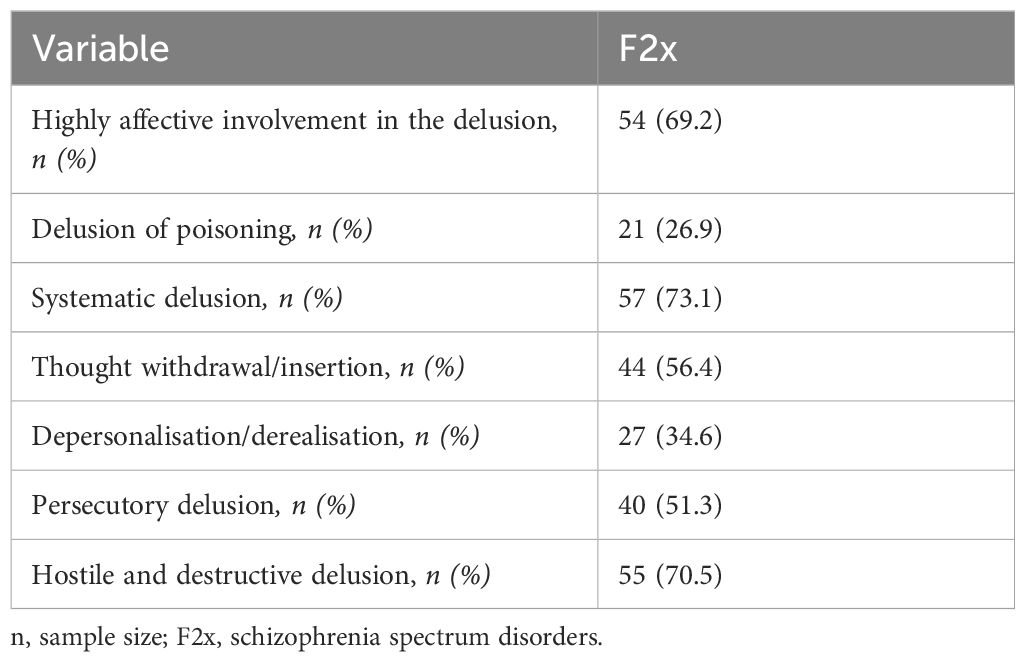
Table 5 Psychopathology at time of index offence (n = 78).
Following the definition of Stompe et al. (14), 33 subjects (42.3%) exhibited Threat symptoms at time of the index offence. Control-Override symptoms were present in 44 subjects (56.4%). The entire TCO complex occurred in 28 subjects (35.9%; Figure 1, Table 6). Following the definition of Kröber (1), 35 subjects (44.8%) showed Threat symptoms and 39 subjects (50.0%) Control-Override symptoms. The full TCO complex occurred in 30 subjects (38.5%; Figure 1, Table 6).
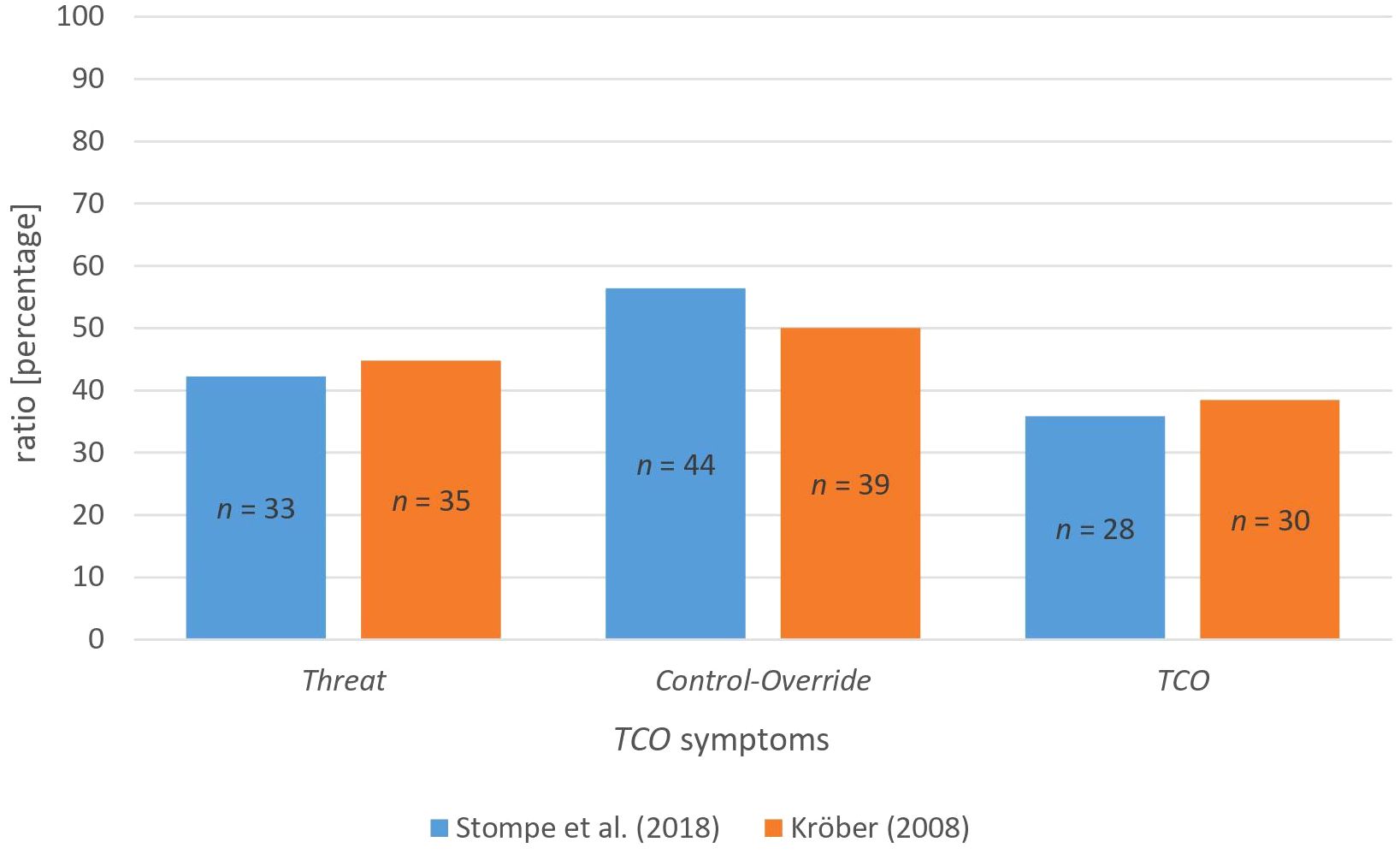
Figure 1 TCO symptoms (n = 78). Notes: n, sample size; TCO, Threat/Control-Override.
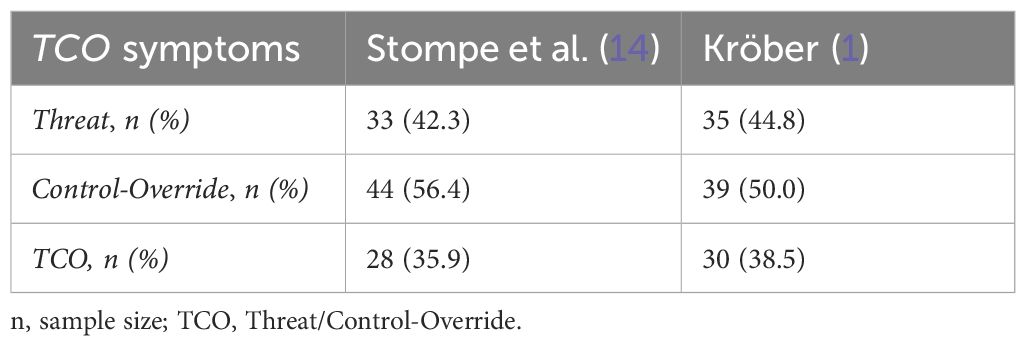
Table 6 Threat/Control-Override (n = 78).
4 Discussion
The results regarding sociodemographic data are in line with the available literature (14, 25, 49–51; and many others): More than three-quarters of all subjects are male, single, unemployed and in receipt of benefits or pensions. Regarding the age at the index offence (on average 32.5 years in the present study), the findings of Schanda (13; the majority of the subjects were older than 25 years) can be confirmed. In addition, almost one in five subjects was homeless at the time of the index offence.
In terms of psychopathology at the time of the index offence, the subjects most frequently suffered from both systematic, hostile and destructive delusions and persecutory delusions. The findings are consistent with the frequently replicated findings of specific and intense psychopathology at the time of the index offence (7, 14, 22, 23, 42, 52).
With regard to the occurrence of TCO, the entire complex was present in just over one third of all subjects. These findings are in contrast to the data of Stompe et al. (14), who found that almost two thirds of all examined subjects who committed a serious violent offence met the criteria for the entire TCO complex (70.9%). Contrary to reports in the literature (where TCO was present mainly due to Threat symptoms; 14, 40, 42, 43), Control-Override symptoms were more frequent than Threat symptoms in the present study. Furthermore, Threat symptoms according to the definition of Stompe et al. (14) occurred the least often, while Control-Override symptoms according to Stompe et al. (14) occurred the most often. An explanation for this could be the more open definition of Control-Override in the definition of Stompe et al. (14) and therefore more subjects fulfilling their criteria. Conversely, the precise definition of Threat symptoms, also compared to Kröber (1) definition, leads to fewer subjects showing these symptoms. In addition to systematic, hostile and destructive delusions and persecutory delusions, Stompe et al. (14) also include a highly affective involvement in the delusion in the definition of Threat. Kröber included derealisation and depersonalisation in his definition of Control-Override, which makes it stricter and ultimately fewer subjects exhibited Control-Override symptoms (50.0% vs. 56.4%).
The different results when comparing data from the literature and the present study could be explained as follows: Due to the lack of specific psychopathological symptoms in both definitions, an operationalisation was necessary to transform the definitions of Threat and Control-Override into AMDP-based psychopathological symptoms. This transformation may result in a lack of information on the psychopathology of homicide offenders with schizophrenia spectrum disorders at the time of the index offence and is therefore prone to error. Furthermore, it remains unclear whether Kröber (1) and Stompe et al. (14) meant their TCO definitions to be fulfilled when all operationalised symptoms were applicable, or whether one positive symptom was sufficient to fulfil the Threat or Control-Override criteria. In the present study, Threat and Control-Override were only counted as fulfilled when all operationalised variables were present in the subject.
TCO is said to represent a psychopathological symptom complex, the presence of which represents a particular risk of imminent violent offence in patients with schizophrenia spectrum disorders. As all subjects in the sample have committed a serious violent offence (homicide), TCO should theoretically be fulfilled for as many subjects as possible. In order to decide which of the two definitions of TCO examined is the most appropriate, both proved to be less sensitive in terms of recognising an imminent violent offence. The majority of subjects did not fulfil the TCO criteria according to the two definitions. Both the definition of Stompe et al. (14) and the definition of Kröber (1) seem to be rather inappropriate. A hypothesis is that the future application of a TCO definition based on the Threat symptoms of Kröber (1) and the Control-Override symptoms of Stompe et al. (14) could be useful. To avoid additional operationalisation, a future definition should capture psychopathological symptoms that are as precise and clearly explorable as possible. Furthermore the psychopathological symptoms that have to be fulfilled for both T- and CO-symptoms should be reconsidered regarding the question whether they all have to be applicable or whether two out of the three T-symptoms and one out of the two CO-symptoms are sufficient already. TCO could therefore be defined as follows: Two symptoms out of persecutory delusion or delusion of poisoning, hostile and destructive delusions and a highly affective involvement in the delusion and one symptom out of thought withdrawal and thought insertion.
Due to the post-hoc nature of the present study, the results do not allow any conclusions to be drawn about the predictive value of TCO for serious violent crime. The event studied (homicide) was established in the past and applied to the entire sample. The problem of the frequent false positive results described early on in the literature (14, 38, 40) can therefore not be solved with the present study. A critical examination of the TCO definition with regard to the avoidance of false positive results (patients with TCO who do not commit a violent offence) should be the subject of future studies.
There is a considerable difference in the scope of the sentences analysed in the index offence and in the forensic psychiatric examinations. It is not possible to prove whether, due to incomplete documentation, relevant information on the current subjects is missing. As the forensic psychiatric reports were written by different authorised experts and the sentences of the index offence were written by different authors, variations in diction or bias cannot be ruled out. Due to the small number of female subjects (n = 9), male and female subjects were analysed together in the present study. No face-to-face interviews were conducted. This could be a limitation, but at the same time the present file-based method represents a methodological strength of the study. The question of the study includes the development of the patients up to the commission of the index offence, and the forensic psychiatric examinations were carried out in the majority of cases at the time of the index offence. For this reason, the psychopathology of the patients could be better represented than by interviewing them (in most cases) many years after the index offence.
In addition, the present study represents a total survey of the sample studied. To the best of our knowledge, this study is the first to focus on a comparative investigation of the presence of TCO in forensic homicidal offenders with schizophrenia spectrum disorders depending on two different definitions of TCO.
Therefore, the present study provides little published primary data on psychopathology in forensic offenders with schizophrenia spectrum disorders, especially on the much debated TCO concept in two definitions. In order to identify clear psychopathological risk symptoms and to determine the most useful TCO definition, larger samples and comparative studies with offenders and non-offenders should be conducted in the future.
However, despite the persuasive evidence for a significant association between schizophrenia spectrum disorders and serious violent behaviour, it still remains unclear why the main part of the patients with schizophrenia spectrum disorders won´t commit any violent offence in their lives (despite of having similar psychotic symptoms; 28, 53) and therewith the final exploration of homicidal behaviour in patients with schizophrenia spectrum disorders.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Senatsverwaltung für Justiz des Landes Berlin. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians in accordance with the national legislation and institutional requirements.
Author contributions
HF: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. MS: Writing – review & editing, Validation, Supervision, Resources, Funding acquisition. HK: Writing – review & editing, Validation, Supervision, Methodology, Data curation, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The publication is funded by the Open Access Publishing Fund of Leipzig University supported by the German Research Foundation within the program Open Access Publication Funding Acknowledgments.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor PS declared a shared parent affiliation with the authors HF and MS at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kröber HL. Kann man die akute Gefährlichkeit schizophren Erkrankter erkennen? Forensische Psychiatrie Psychologie Kriminologie. (2008) 2:128–36. doi: 10.1007/S11757-008-0073-9
2. De Vries B, Van Busschbach JT, van der Stouwe ECD, Aleman A, Van Dijk JJM, Lysaker PH, et al. Prevalence rate and risk factors of victimization in adult patients with a psychotic disorder: A systematic review and meta-analysis. Schizophr Bull. (2019) 45:114–26. doi: 10.1093/SCHBUL/SBY020
3. Böker W, Häfner H. (1973). Gewalttaten geistesgestörter. Berlin: Springer. Available at: doi: 10.1007/978-3-642-86859-7
4. Eronen M, Hakola P, Tiihonen J. Factors associated with homicide recidivism in a 13-year sample of homicide offenders in Finland. Psychiatr Serv. (1996) 47:403–6. doi: 10.1176/PS.47.4.403
5. Schanda H. “Homicides and major mental disorders: A 25-year study”: Commentary reply. Acta Psychiatrica Scandinavica. (2006) 113(1):75. doi: 10.1111/j.1600-0447.2005.00681.x
6. Fazel S, Gulati G, Linsell L, Geddes JR, Grann M. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. (2009) 6:1–12. doi: 10.1371/JOURNAL.PMED.1000120
7. Witt K, van Dorn R, Fazel S. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS One. (2013) 8:1–13. doi: 10.1371/JOURNAL.PONE.0055942
8. Curic S. Psychiatrischer Beitrag: Korrelate zukünftiger Gewalt bei Personen, die wegen einer Schizophrenie behandelt werden. Forensische Psychiatrie Psychologie Kriminologie. (2019) 13:395–7. doi: 10.1007/s11757-019-00562-3
9. Taylor PJ. Motives for offending among violent and psychotic men. Br J Psychiatry : J Ment Sci. (1985) 147:491–8. doi: 10.1192/BJP.147.5.491
10. Eronen M, Hakola P, Tiihonen J. Mental disorders and homicidal behavior in Finland. Arch Gen Psychiatry. (1996) 53:497–501. doi: 10.1001/ARCHPSYC.1996.01830060039005
11. Wallace C, Mullen P, Burgess P, Palmer S, Ruschena D, Browne C. Serious criminal offending and mental disorder. Case linkage study. Br J Psychiatry : J Ment Sci. (1998) 172:477–84. doi: 10.1192/BJP.172.6.477
12. Erb M, Hodgins S, Freese R, Müller-Isberner R, Jöckel D. Homicide and schizophrenia: maybe treatment does have a preventive effect. Criminal Behav Ment Health : CBMH. (2001) 11:6–26. doi: 10.1002/CBM.366
13. Schanda H, Knecht G, Schreinze D, Stompe T, Ortwein-Swoboda G, Waldhoer T. Homicide and major mental disorders: A 25-year study. Acta Psychiatrica Scandinavica. (2004) 110(2):98–107. doi: 10.1111/j.1600-0047.2004.00305.x
14. Stompe T, Ritter K, Schanda H. Prädiktoren für Gewaltdelikte bei Schizophrenie. In: Stompe T, Schanda (Hrsg.) H, editors. Schizophrenie und Gewalt. Medizinisch wissenschaftliche Verlagsgesellschaft, Berlin (2018). p. 91–148.
15. Volavka J, Laska E, Baker S, Meisner M, Czobor P, Krivelevich I. History of violent behaviour and schizophrenia in different cultures. Analyses based on the WHO study on Determinants of Outcome of Severe Mental Disorders. Br J Psychiatry : J Ment Sci. (1997) 171:9–14. doi: 10.1192/bjp.171.1.9
16. Taylor PJ, Gunn J. Violence and psychosis. I. Risk of violence among psychotic men. Br Med J (Clinical Res Ed.). (1984) 288:1945. doi: 10.1136/BMJ.288.6435.1945
17. Côté G, Hodgins S. The prevalence of major mental disorders among homicide offenders. Int J Law Psychiatry. (1992) 15:89–99. doi: 10.1016/0160-2527(92)90029-Z
18. Oberlies D. Tötungsdelikte zwischen Männern und Frauen. Monatsschrift Für Kriminologie Und Strafrechtsreform. (1997) 80:133–47. doi: 10.1515/MKS-1997-800301
19. Häfner H, Böker W. Gewalttaten geistesgestörter. Gewalttaten Geistesgestörter. (1973) 231–73. doi: 10.1007/978-3-642-86859-7
20. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. (1986) 27:131–48. doi: 10.1016/0010-440X(86)90022-2
21. Link BG, Andrews H, Cullen FT. The violent and illegal behavior of mental patients reconsidered. Am Sociological Rev. (1992) 57:275. doi: 10.2307/2096235
22. Prüter C. Zusammenhang zwischen Wahn und Gewalt. Gibt es stereotype Delikte bei Wahnkranken? In: Lammel M, Sutarski S, Lau S, Bauer (Hrsg.) M, editors. Wahn und Schizophrenie. Psychopathologie und forensische Relevanz. Medizinisch wissenschaftliche Verlagsgesellschaft, Berlin (2011). p. 101–10.
23. Swanson JW, Swartz MS, Van Dorn RA, Elbogen EB, Wagner HR, Rosenheck RA, et al. A national study of violent behavior in persons with schizophrenia. Arch Gen Psychiatry. (2006) 63:490–9. doi: 10.1001/ARCHPSYC.63.5.490
24. Richard-Devantoy S, Olie JP, Gourevitch R. Risk of homicide and major mental disorders: A critical review. Encephale. (2009) 35:521–30. doi: 10.1016/j.encep.2008.10.009
25. Whiting D, Lichtenstein P, Fazel S. Violence and mental disorders: a structured review of associations by individual diagnoses, risk factors, and risk assessment. Lancet Psychiatry. (2021) 8:150–61. doi: 10.1016/S2215-0366(20)30262-5
26. Balcioglu YH, Kirlioglu Balcioglu SS, Oncu F, Turkcan A. Profiling homicides based on impulsive or proactive natures in male Schizophrenia patients. J Am Acad Psychiatry Law. (2023) 51:215–26. doi: 10.29158/JAAPL.220064-22
27. Felthous AR. Schizophrenia and impulsive aggression: a heuristic inquiry with forensic and clinical implications. Behav Sci Law. (2008) 26:735–58. doi: 10.1002/bsl.846
28. Kröber HL. Tötungsdelikte psychotisch Kranker – gibt es ein Sinnverstehen? Swiss Arch Neurol Psychiatr. (2014) 165:133–8.
29. Stompe T. Versuch einer Typologie von Tötungsdelikten schizophrener Patienten. Spektrum Psychiatr. (2013) SP 01|2013.
30. Hodgins S, Müller-Isberner R. Schizophrenia and violence. Nervenarzt. (2014) 85:273–8. doi: 10.1007/s00115-013-3900-y
31. Link BG, Stueve A. Psychotic Symptoms and the Violent/Illegal Behavior of Mental Patients Compared to Community Controls. (1994).
32. Link BG, Stueve A, Phelan J. Psychotic symptoms and violent behaviors: Probing the components of “threat/control-override” symptoms. Soc Psychiatry Psychiatr Epidemiol. (1998) 33:55–60. doi: 10.1007/s001270050210
33. Joyal CC, Putkonen A, Mancini-Marïe A, Hodgins S, Kononen M, Boulay L, et al. Violent persons with schizophrenia and comorbid disorders: a functional magnetic resonance imaging study. Schizophr Res. (2007) 91:97–102. doi: 10.1016/J.SCHRES.2006.12.014
34. Link BG, Monahan J, Stueve A, Cullen FT. Real in their consequences: A sociological approach to understanding the association between psychotic symptoms and violence. Am Sociological Rev. (1999) 64:316–32. doi: 10.2307/2657535
35. Swanson JW, Borum R, Swartz MS, Monahan J. Psychotic symptoms and disorders and the risk of violent behaviour in the community. Criminal Behav Ment Health. (1996) 6:309–29. doi: 10.1002/CBM.118
36. Nordström A, Dahlgren L, Kullgren G. Victim relations and factors triggering homicides committed by offenders with schizophrenia. J Forensic Psychiatry Psychol. (2006) 17:192–203. doi: 10.1080/14789940600631522
37. Swanson J, Estroff S, Swartz M, Borum R, Lachicotte W, Zimmer C, et al. Violence and severe mental disorder in clinical and community populations: the effects of psychotic symptoms, comorbidity, and lack of treatment. Psychiatry. (1997) 60:1–22. doi: 10.1080/00332747.1997.11024781
38. Mullen PE. A reassessment of the link between mental disorder and violent behaviour, and its implications for clinical practice. Aust New Z J Psychiatry. (1997) 31:3–11. doi: 10.3109/00048679709073793
39. Appelbaum PS, Robbins PC, Monahan J. Violence and delusions: data from the MacArthur Violence Risk Assessment Study. Am J Psychiatry. (2000) 157:566–72. doi: 10.1176/APPI.AJP.157.4.566
40. Teasdale B, Silver E, Monahan J. Gender, threat/control-override delusions and violence. Law Hum Behav. (2006) 30:649–58. doi: 10.1007/s10979-006-9044-x
41. Kröber HL, Lau S. Psychosen aus dem schizophrenen Formenkreis. In: Kröber HL, Dölling D, Leygraf N, Saß (Hrsg.) H, editors. Handbuch der Forensischen Psychiatrie Bd II, Psychopathologische Grundlagen und Praxis der Forensischen Psychiatrie im Strafrecht. Springer, Heidelberg Berlin (2010). p. 312–33.
42. Stompe T, Ortwein-Swoboda G, Schanda H. Schizophrenia, delusional symptoms, and violence: the threat/control override concept reexamined. Schizophr Bull. (2004) 30:31–44. doi: 10.1093/oxfordjournals.schbul.a007066
43. Nederlof AF, Muris P, Hovens JE. Threat/control-override symptoms and emotional reactions to positive symptoms as correlates of aggressive behavior in psychotic patients. J Nervous Ment Dis. (2011) 199:342–7. doi: 10.1097/NMD.0B013E3182175167
44. Stompe T. Die forensische Relevanz der inhaltlichen Dimension des schizophrenen Wahns. In: Lammel M, Sutarski S, Lau S, Bauer (Hrsg.) M, editors. Wahn und Schizophrenie. Psychopathologie und forensische Relevanz. Medizinisch wissenschaftliche Verlagsgesellschaft, Berlin (2011). p. 91–7.
45. Stompe T. Die Bedeutung des Wahns für die Risikoeinschätzung delinquenten Verhaltens schizophrener Patienten // Schizophrenia and Violence – The Impact of Delusions on Risk Assessment. J Für Neurologie Neurochirurgie Und Psychiatr. (2018) 19:104–10. doi: 10.1093/OXFORDJOURNALS.SCHBUL.A007066
46. Martino H, Rabenschlag F, Koch U, Attinger-Andreoli Y, Michel K, Gassmann J, et al. Positionspapier Entstigmatisierung. Grundlagen für eine nationale Kampagne zur Entstigmatisierung von psychischen Krankheiten und von Menschen mit Störungen der psychischen Gesundheit. Swiss Soc For Public Health. (2012) 5–21.
47. Schomerus G, Riedel-Heller S. Das Stigma psychischer Krankheit im Fokus. Nervenarzt. (2020) 91:777–8. doi: 10.1007/s00115-020-00964-3
48. AMDP. Arbeitsgemeinschaft für Methodik und Dokumentation in der Psychiatrie. AMDP. Available at: https://www.amdp.de/. Retrieved February 9, 2023aufgerufen am 25.04.2023.
49. Kutscher S, Schiffer B, Seifert D. Patients with schizophrenia in forensic-psychiatric hospitals (section 63 German Penal Code) in North Rhine-Westphalia. Fortschr Der Neurologie-Psychiatrie. (2009) 77:91–6. doi: 10.1055/S-0028-1109080/ID/43
50. Nielssen O, Large M. Rates of homicide during the first episode of psychosis and after treatment: a systematic review and meta-analysis. Schizophr Bull. (2010) 36:702–12. doi: 10.1093/SCHBUL/SBN144
51. Maier W, Hauth I, Berger M, Saß H. Zwischenmenschliche Gewalt im Kontext affektiver und psychotischer Störungen. Nervenarzt. (2016) 87:53–68. doi: 10.1007/S00115-015-0040-6
52. Buchanan A, Reed A, Wessely S, Garety P, Taylor P, Grubin D, et al. Acting on delusions. II: The phenomenological correlates of acting on delusions. Br J Psychiatry. (1993) 163:77–81. doi: 10.1192/BJP.163.1.77
Keywords: TCO, homicide, schizophrenia, psychopathology, forensic psychiatry
Citation: Findeis H, Strauß M and Kröber H-L (2024) The TCO concept in German forensic homicide offenders with schizophrenia spectrum disorders – new findings from a file-based, retrospective cross-sectional study. Front. Psychiatry 15:1404263. doi: 10.3389/fpsyt.2024.1404263
Received: 20 March 2024; Accepted: 22 May 2024;
Published: 11 June 2024.
Edited by:
Peter Schoenknecht, Leipzig University, GermanyReviewed by:
Yasin Hasan Balcioglu, Bakirkoy Prof Mazhar Osman Training and Research Hospital for Psychiatry, Neurology, and Neurosurgery, TürkiyeBenno Bartsch, Clinic of Forensic Psychiatry, Germany
Copyright © 2024 Findeis, Strauß and Kröber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hannelore Findeis, hannelore.findeis@medizin.uni-leipzig.de