 Sandro Tiziano Stoffel
Sandro Tiziano Stoffel Jie Gao2
Jie Gao2 Yasemin Hirst
Yasemin Hirst Christian Von Wagner
Christian Von Wagner- 1Institute of Pharmaceutical Medicine, University of Basel, Basel, Switzerland
- 2Department of Behavioural Science and Health, University College London, London, United Kingdom
- 3Applied Health Research Hub, University of Central Lancashire, Preston, United Kingdom
Background: Studies have shown that presenting information about positive trends in peer behavior can have a greater impact on individual behavior than simply communicating their current behavior. In a web-based experiment, we investigated whether highlighting a positive trend in the uptake of the English bowel cancer screening programme (BSCP) influences the intentions of men and women who initially had low intentions.
Methods: We recruited 1,194 men and women aged 25–49 who had no previous diagnosis of bowel cancer and no experience with the BSCP. These individuals, who had indicated low intentions to participate in screening, were selected from a survey panel. They were randomly assigned to one of four experimental conditions: (1) a control group without a normative message, (2) a group receiving a standard static social norms message communicating current uptake, (3) a group receiving a dynamic social norms message stating that screening participation has been increasing, and (4) a group receiving an extended dynamic social norms message combining a dynamic with a static social norm message. We measured the impact of these messages on their intentions to complete a screening test when invited, their perceived informativeness of the messages, and their active interest in learning more about bowel cancer and the screening test.
Results: None of the messages influenced intentions in the unadjusted regression; however, the extended dynamic social norms message significantly increased screening intentions compared to the control condition in the adjusted regression. Analysis of changes in intentions before and after the manipulation revealed that both dynamic social norms messages positively influenced changes in the unadjusted regression, while all three messages had a positive impact in the adjusted regression. None of the messages affected active interest or the perceived informativeness of the provided information.
Conclusion: Dynamic social norms messages, which highlight the positive trend in screening participation combined with the current uptake rate have the potential to enhance screening intentions.
Background
Studies have shown that individual decision-making and behavior are often influenced by the perception of others' behaviors (descriptive social norms) and what is approved by important people and society (injunctive norms) (Cialdini and Goldstein, 2004). Social norms provide a standard behavior for specific situations that people do not want to deviate from Schultz et al. (2007). Social norms can be defined as rules understood by group members (Cialdini and Trost, 1998). Previous studies have demonstrated that communicating social norms can influence health behaviors (Dempsey et al., 2018). These studies typically communicate a static descriptive social norms message. Recently, a new form of descriptive norms called dynamic social norms has been proposed. Unlike static norms, which focus on current behaviors, dynamic norms convey trends in behavior (Sparkman and Walton, 2017). Dynamic social norms have been shown to be more effective than static norms in promoting sustainable behaviors, such as reducing meat consumption (Sparkman and Walton, 2017), conserving water (Mortensen et al., 2019), and avoiding disposable to-go cups (Loschelder et al., 2019). Few studies have investigated how messages about changing social norms influence health behaviors so far. One study found that dynamic or static norms messages had no effect on COVID-19 vaccination intentions among unvaccinated people (Geber et al., 2022). However, another study found that dynamic social norms messages led to lower reports of planned weekly and heavy drinking among college students compared to static norms messages or no message at all (Graupensperger et al., 2021). Additionally, only a few studies have tested the influence of dynamic social norms on actual behavior (Sparkman and Walton, 2017; Mortensen et al., 2019; Loschelder et al., 2019), and none have focused on health behaviors. To date, no studies have evaluated the effects of dynamic social norms on colorectal cancer (CRC) screening intentions. Given the increase in screening uptake with the introduction of the more user-friendly Fecal Immunochemical Test (FIT) compared to the previously used Guaiac-based Fecal Occult Blood Test (gFOBT) (Moss et al., 2017; NHS England, 2024a), dynamic norm messages could potentially be a valuable strategy for enhancing communication efforts. Previous studies have only tested static social norms with mixed results (Stoffel et al., 2019; von Wagner et al., 2019; Taylor et al., 2022). While they seem to be effective in highly controlled online experiments with non-intenders (Stoffel et al., 2019; von Wagner et al., 2019), results were mixed for field experiments, with no impact detected in a study that communicated that the majority of people get screened (Stoffel et al., 2019) and a positive effect in a study that communicated to non-attenders that they are in the minority (Gorini et al., 2023).
The study aimed to test whether communicating dynamic rather than static social norms can further increase screening intentions by leading individuals to expect a stronger anticipated future norm and, consequently, a stronger desire to adhere to it (Sparkman and Walton, 2017). This is due to the dynamic messages aim to reflect an upward trend within the community, potentially fostering individuals' expectations of stronger social norms in the future. Specifically, we tested these messages among individuals with low initial screening intentions, as previous studies suggest they might be more open to personal change (Sparkman and Walton, 2019; Stoffel et al., 2019; von Wagner et al., 2019). The findings of this study not only contribute to current social norms research but also have important implications for communication strategies aimed at increasing screening participation. Notably, our study is among the first to examine the impact of dynamic social norms on health behaviors specifically. By demonstrating the potential effectiveness of these norms in encouraging CRC screening intentions and interest in reading further information about CRC screening, our research provides valuable insights that can inform future health communication interventions and strategies.
The current research
In this study, we aimed to determine if dynamic social norms could increase the intention to complete a FIT, a non-invasive screening test offered through the NHS Bowel Cancer Screening Programme (BCSP) to individuals aged 50–74 to detect hidden traces of blood in stool samples, which may indicate the presence of colorectal cancer or pre-cancerous conditions. We compared the effectiveness of a dynamic social norms message alone, and in combination with a static norms message, against a traditional static norms message and a control condition with no information about normative screening behavior.
Following previous experimental studies (Stoffel et al., 2019; von Wagner et al., 2019), we focused on individuals who had never been screened and were initially disinclined. However, unlike those studies, we also included individuals who initially stated they would probably complete the screening test, to test the messages with those who were not fully convinced yet. This approach helps minimize ceiling and social desirability effects often linked with self-reported intention measures (Michie and Abraham, 2004). Furthermore, by recruiting study participants who initially have low intentions to complete the screening test, we lower the chance of discouraging them with social norms messages. Previous studies have shown that these individuals generally have lower expectations about screening uptake (Sieverding et al., 2010a; von Wagner et al., 2019).
For the purpose of testing the hypothesis whether dynamic social norms messages are more effective than traditional static messages, in terms of motivating individuals with low initial intentions to complete a FIT, we conducted a study consisting of two steps. The first step consisted of a short web-based preliminary survey to identify eligible study participants for the experiment. The experiment conducted 1 week later, then compared the motivational impact of a dynamic social norm messages with and without standard static norms component with a control message that did not contain any prevalence information, and a traditional static social norms message. The experiment tested the following two working hypotheses (WH):
WH1. Providing a dynamic social norms message that describes an increasing trend in FIT uptake will lead to an increased intention to complete FIT among a population who previously stated low intentions to participate.
This first hypothesis builds on the previous literature that showed that emerging social norms are more effective than static messages in the context of sustainable behaviors (Sparkman and Walton, 2017; Mortensen et al., 2019; Loschelder et al., 2019)
WH2. A combination of an emerging social norms message and a static social norms message will further enhance the impact of a descriptive norm message, leading to a greater increase in screening intentions compared to using either type of message alone.
The second hypothesis suggests that by combining emerging and static social norms messages, study participants learn not only that many people are already participating, but that the number is still growing.
We also examined how informative the participants found the messages. Evidence-based information, when framed correctly, can improve knowledge, attitudes, and reduce negative emotions toward decision-making (Occa et al., 2021). Additionally, we measured how the normative messages affected participants' interest in learning more about the screening test's benefits and harms. This interest, shown by participants wanting to read more, served as a proxy for actual behavior, aligning with the intention-behavior gap literature (Sheeran et al., 2017; Sieverding et al., 2010b; Stoffel et al., 2019; von Wagner et al., 2019). This question together with three comprehension questions about the additional information also served to investigate whether the normative messages affect information-seeking behavior, as informed choice relies on knowledge consistent with the decision maker's values (Marteau et al., 2001).
Methods
Study participants
We recruited 3,368 men and women aged 25–49 from a commercial survey panel (Prolific). Prolific, a UK-based research platform founded in 2014, enables researchers to recruit participants with specific demographic filters. This platform ensures efficient data collection and ethical standards through fair compensation for participants' efforts. For this study, individuals with a previous diagnosis of bowel cancer or those who had already participated in a CRC screening program were excluded. The large age range was due to difficulties in recruiting enough screening-naïve participants—individuals with no prior experience or exposure to the BCSP process—for the preliminary study and the experiment. Note that our study participants would not have been invited for screening before turning 50.
Following previous studies, we provided participants with a brief description of the screening test and asked them to state their intentions to complete it using a fully-labeled Likert scale: “definitely not,” “probably not,” “probably yes,” and “definitely yes” (Stoffel et al., 2019; von Wagner et al., 2019). We excluded individuals who indicated they would definitely complete a FIT when invited (see Figure 1 for the flow through the study). This preliminary survey also collected details on respondents' age, sex, mother tongue, and expected participation in the BCSP (see Supplementary Table S1 for participant characteristics in the preliminary survey).
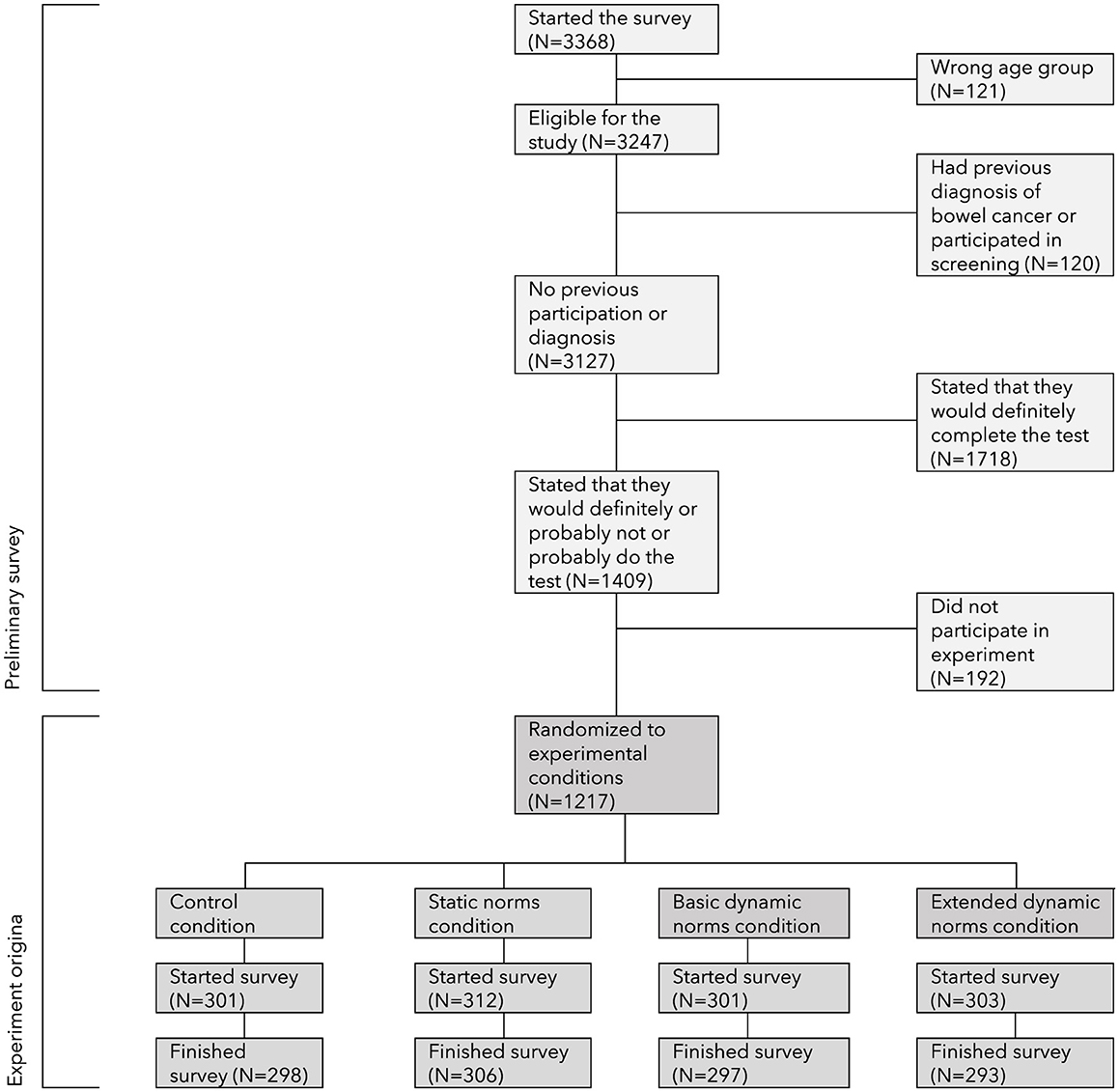
Figure 1. Flow through the study.
Procedures
Eligible participants were invited to join a web-based experiment 1 week later. The experiment used a 2 × 2 factorial design with two independent variables: (1) presence or absence of dynamic social norms messages, and (2) presence or absence of static social norms messages. The experiment was programmed in Qualtrics. Participants were randomly assigned to one of four groups: (1) a control group with no prevalence information; (2) a group with a static norms message; (3) a group with a basic emerging norms message; and (4) a group with an extended norms message that included both emerging and static norms messages. Each group received a short paragraph about colorectal cancer and the FIT (see Supplementary file 2). For the three experimental groups, this paragraph was followed by a highlighted normative message (see Table 1). To avoid bias from presenting information in a single format, participants in the experimental groups were further randomized to receive one of four different framings of the normative message (e.g., “7 out of 10,” “70%,” or “nearly three-quarters” for static messages, and “more and more,” “20% more,” or “one in five more” for basic emerging messages). Recent NHS England statistics (NHS England, 2024b) indicate that national uptake has risen to 67.8% since 2019, providing a basis for approximating the 70% rate used in this study. The messages were collaboratively developed with patients and public representatives during a subsequent workshop to ensure they accurately reflected this approximate rate. Table 1 shows that some messages were objective, while others were subjective. The subjective messages were inspired by previous research that found using verbal quantifiers instead of specific numbers was effective (Sparkman and Walton, 2017; Stoffel et al., 2019).
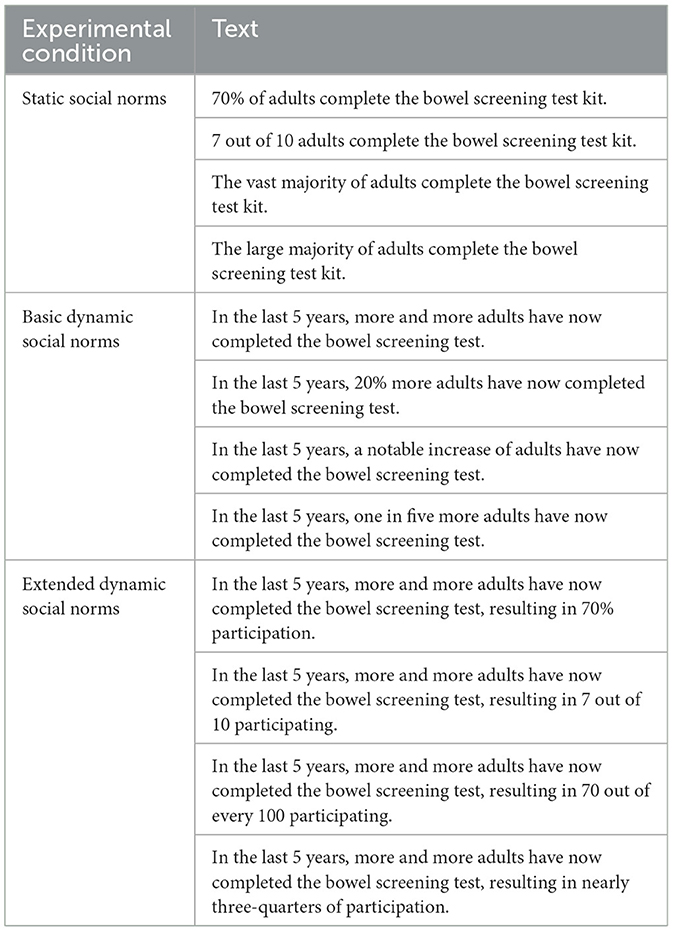
Table 1. Normative messages used in the experiment.
Measures
The primary outcome of the study was intention to complete a FIT after reading the information. The post-exposure intention question was framed as: “Given the previous information, would you take up the offer if you were invited to complete such a FIT test?”, recorded on the same fully labeled 4-point Likert scale as in the preliminary survey (Stoffel et al., 2019; von Wagner et al., 2019).
Secondary outcomes included findings on perceived informativeness of the messages and active interest in reading more about colorectal cancer and the FIT or skip it (Stoffel et al., 2019). Those that opted to read the information were asked three additional multiple-choice comprehension questions to measure engagement. Finally, respondents completed six questions from Dumenci et al. (2014) CHLT-6 questionnaire on cancer health literacy and three further sociodemographic questions on the study participant's marital status, education and employment. These variables were used as covariates in the adjusted regressions.
Statistical analysis
The sample size for the experiment was calculated before data collection, using estimates from a pilot study, to ensure it was large enough to detect at least a 10% difference in screening intentions between two experimental conditions, with 80% power and an alpha value of 0.05 (Cohen, 2013).
We report all measures, manipulations, and exclusions in the study. In addition to reporting screening intentions following the experimental manipulation, we present the change in intentions, calculated as the difference between the numerical value of the ex-ante [1;3] and ex-post [1;4] intentions. Due to the low frequencies observed in certain categories, we combined the −2 and −1 categories as well as the +2 and +3 categories, resulting in four final categories ranging from −1 to +2. The Supplementary material includes an alternative analysis using dichotomized screening intentions (“yes, probably” and “yes, definitely” combined vs. “probably not” and “definitely not”), consistent with approaches in previous literature (Stoffel et al., 2019; von Wagner et al., 2019).
We used Chi-square tests of independence and probit regressions (both binary and ordinal), adjusted for baseline intentions, expected participation rate, health literacy, and sociodemographic variables, to examine the effect of normative messages on dichotomized post-exposure intentions to complete a FIT, perceived informativeness, and active interest in reading about screening. We reported the regression coefficients (β), along with their 95% confidence intervals (CIs) and associated p-values. Regressions with the original intention scales can be found in Supplementary Table S5. Engagement with the additional information was analyzed using a Kruskal-Wallis test. All statistical analyses were conducted using Stata/IC version 16 (StataCorp LP, College Station, TX).
Results
Study participants
Figure 1 shows the flow of participants through the study. A total of 3,368 men and women living in England were invited to participate in the preliminary survey. Of these, 121 (3.6%) were outside the age range of 25–49, and 120 (5.1%) had a previous diagnosis of bowel cancer or had participated in screening. Regarding intentions to complete a FIT, 1,409 (45.1%) of those in the correct age range and without a previous cancer diagnosis or screening participation indicated that they would either “definitely not” (n = 64), “probably not” (n = 222), or “probably yes” (n = 1,123) do the test. The 1,718 who stated that they would definitely do the test were excluded, leaving a sample of 1,409 eligible study participants for the experiment. Of these, 192 (13.6%) did not choose to participate in the main experiment, and 23 (1.6%) did not finish it.
The final analytical sample of the experiment consisted of 1,194 participants. Table 2 shows that of these, 53.5% were female, 88.5% had English as their mother tongue, 61.2% were married or cohabiting, 82.6% were in paid employment, and 85.8% had A-level or higher education. Post-hoc comparisons showed that initial intentions, expectations about uptake and sociodemographic characteristics were similar between those who completed the experiment and those who did not, except for mother tongue; participants with English as their mother tongue were more likely not to participate in the experiment. Supplementary Figure S1 shows the distribution of the initial beliefs about uptake, with the median being 3 out of 10. Additionally, there were no statistically significant differences in sociodemographic characteristics across the four experimental (see Supplementary Table S1).
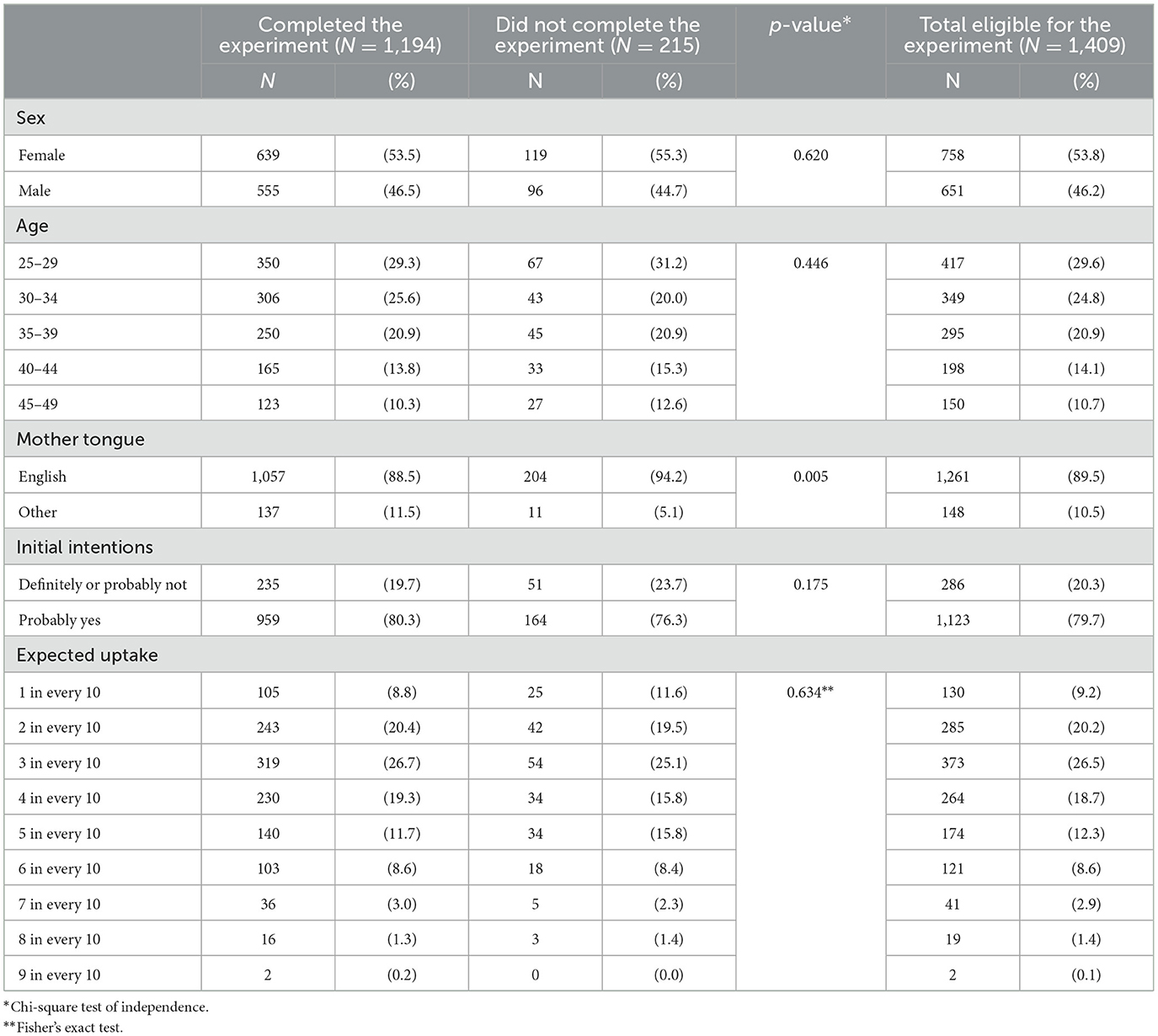
Table 2. Description of the eligible study sample (N = 1,409).
Impact on intentions to participate in CRC screening
Contrary to our first working hypothesis, Table 3 and Figure 2 show that the basic dynamic social norms message increased screening intentions compared to the control group in both the unadjusted regression (β = 0.11, 95% CI −0.06 to 0.28, p = 0.254) and the adjusted regression (β = 0.16, 95% CI −0.02 to 0.34, p = 0.087).
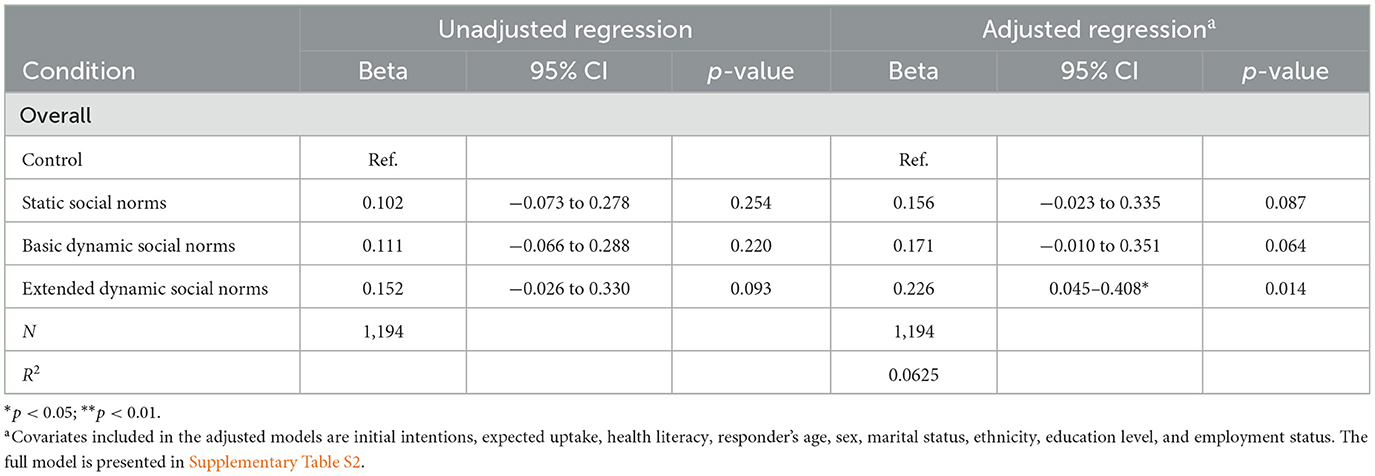
Table 3. Ordered probit regression on the effect of the normative messages on uptake intentions (N = 1,194).
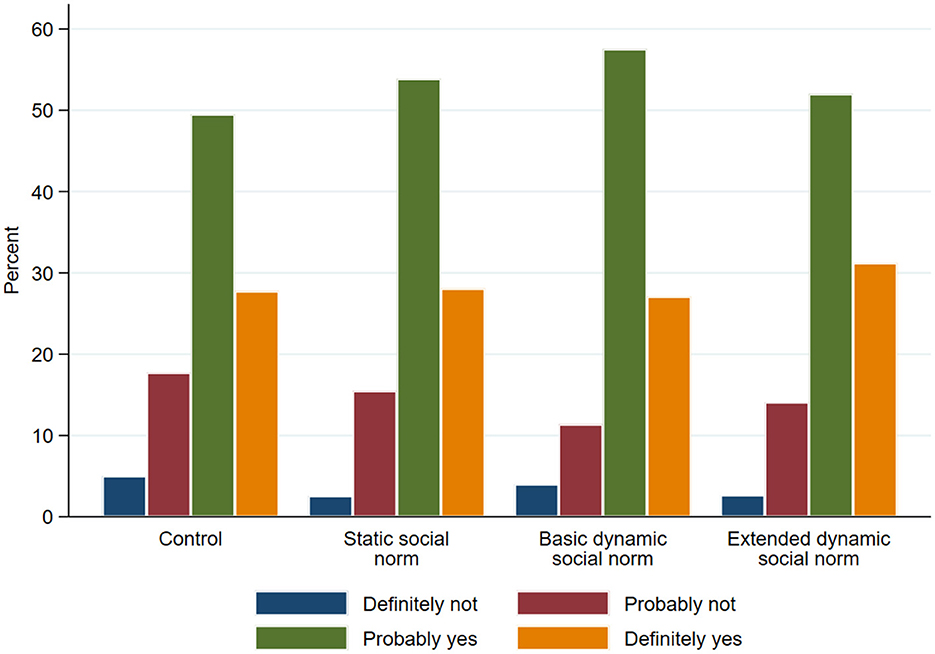
Figure 2. Distribution of the intentions scales after the reading the information (N = 1,194).
Similarly, contrary to our second working hypothesis, the difference between the extended dynamic social norms condition and the control condition was significant only in the fully adjusted regression model (β = 0.23, 95% CI 0.05–0.41, p = 0.014), but not in the unadjusted regression (β = 0.15, 95% CI −0.03 to 0.33, p = 0.093). Notably, the inclusion of initial intentions in the regression analysis resulted in the association for the extended dynamic social norms condition becoming significant. The static social norms message, however, was not associated with an increase in screening intentions in the unadjusted analysis (β = 0.10, 95% CI −0.07 to 0.29, p = 0.254), though it approached significance in the fully adjusted regression (β = 0.17, 95% CI −0.01 to 0.35, p = 0.064). Post-hoc Wald tests comparing regression coefficients revealed no significant differences between the coefficient for the static social norms condition and those for the basic and extended dynamic conditions (p = 0.876 and p = 0.447, respectively). Similarly, no significant differences were observed between the coefficients for the basic and extended dynamic social norms conditions (p = 0.547). The predicted intentions are presented in Supplementary Figure S2.
The full models are reported in Supplementary Table S2. Additional factors associated with greater screening intentions included having at least A-level qualifications (β = 0.24, 95% CI 0.06–0.43, p = 0.010), being married or cohabiting (β = 0.26, 95% CI 0.13–0.40, p < 0.001), initially indicating that they would probably undergo the screening test (β = 0.87, 95% CI 0.55–1.98, p < 0.001), and higher expected screening uptake (β = 0.05, 95% CI 0.01–0.09, p = 0.027).
Subgroup analyses were conducted based on age groups (25–34 vs. 35–49), initial screening intentions (“definitely not” and “probably not” vs. “probably yes”), and initial beliefs about screening uptake (believing that only up to 3 out of 10 participants would get screened vs. more than 3 out of 10). Supplementary Table S3 shows that the basic social norms message increased screening intentions among individuals aged 25–34 (β = 0.31, 95% CI 0.07–0.56, p = 0.012), while the extended dynamic social norms message increased intentions among those aged 35–49 (β = 0.31, 95% CI 0.02–0.60, p = 0.040). Similarly, the extended dynamic social norms message increased intentions among individuals who initially indicated that they would probably get screened (β = 0.24, 95% CI 0.04–0.45, p = 0.021; see Supplementary Table S4). All three messages increased screening intentions exclusively for individuals with low initial beliefs about screening uptake (see Supplementary Table S5).
The analysis of changes in intentions, presented in Table 4 and Supplementary Figure S3 reveals that both dynamic social norms messages had a positive impact on the change (basic: β = 0.21, 95% CI: 0.03–0.39, p = 0.021; extended: β = 0.24, 95% CI: 0.06–0.42, p = 0.018) in the unadjusted regressions and all messages in the adjusted regressions (static: β = 0.18, 95% CI: 0.00–0.36, p = 0.049; basic: β = 0.23, 95% CI: 0.05–0.41, p = 0.012 and extended: β = 0.25, 95% CI: 0.07–0.43, p = 0.006). The predicted probabilities of change are displayed in Supplementary Figure S4.
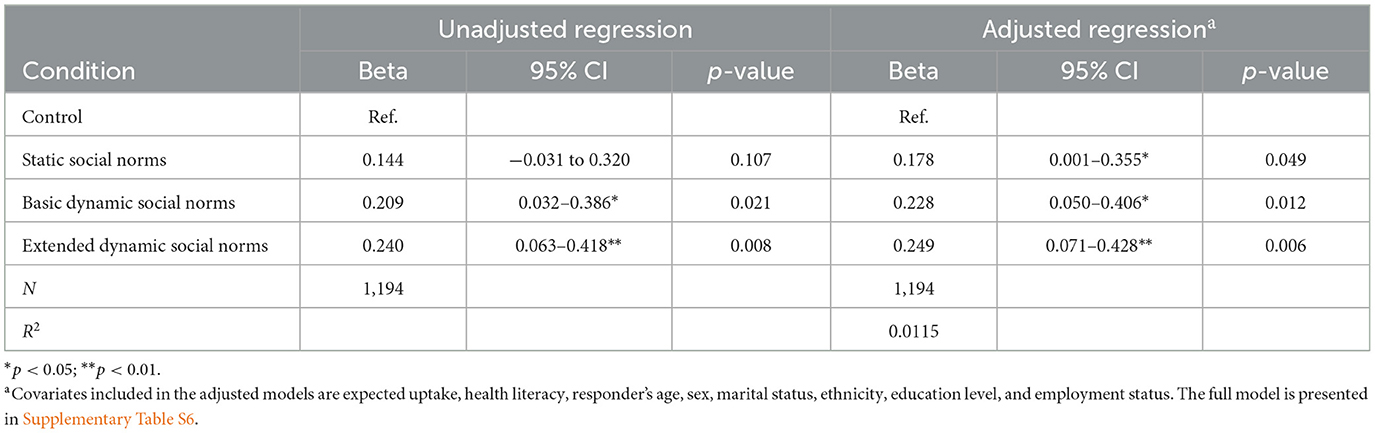
Table 4. Ordered probit regression on the effect of the normative messages on changing intentions [−1; 2] (N = 1,194).
The regression model with the dichotomized scale (see Supplementary Table S7) supports working hypothesis 1, indicating that the basic dynamic social norms message increased screening intentions compared to the control group in both unadjusted (84.9 vs. 77.2%; β = 0.29, 95% CI 0.05–0.52, p = 0.017) and adjusted regressions (β = 0.38, 95% CI 0.13–0.64, p = 0.004). The extended dynamic social condition was significant only in the fully adjusted regression (82.9 vs. 77.2%; β = 0.33, 95% CI 0.07–0.58, p = 0.012), but not in the unadjusted analysis (β = 0.20, 95% CI −0.03 to 0.44, p = 0.108). The static social norms message was not significant in unadjusted or adjusted regressions (82.0 vs. 77.2%; β = 0.17, 95% CI −0.06 to 0.40, p = 0.145; β = 0.22, 95% CI −0.02 to 0.47, p = 0.077). Post-hoc Wald tests showed no significant differences between coefficients. Supplementary Figure S5 illustrates the distribution of intentions across experimental conditions. Analyzing changes in dichotomized intentions from the preliminary survey to after the manipulation showed that 80.7% of participants did not change their intentions (see Supplementary Figure S6). Participants in the dynamic social norms conditions were less likely to decrease their intentions compared to those in the control or static conditions. Moreover, individuals exposed to any social norms message more frequently increased their screening intentions than those in the control condition [χ2(6,N = 1,194) = 13.59, p = 0.016].
Active interest in reading more about CRC screening
When examining whether the normative messages influenced information seeking and engagement, it was found that around 57% of respondents wanted to read more, regardless of the experimental condition. This was shown in Table 5 and Figure 3 [55.0–59.6%, χ2(3,N = 1,194) = 1.60, p = 0.660]. Further analysis, showed in Supplementary Table S8 confirmed that none of the experimental conditions significantly influenced information-seeking behavior, namely static social norms' (β = 0.12, 95% CI: −0.09 to 0.32, p = 0.268), “basic dynamic social norms” (β = 0.17, 95% CI: −0.04 to 0.37, p = 0.114), and “extended dynamic social norms” (β = 0.04, 95% CI: −0.16 to 0.25, p = 0.675).
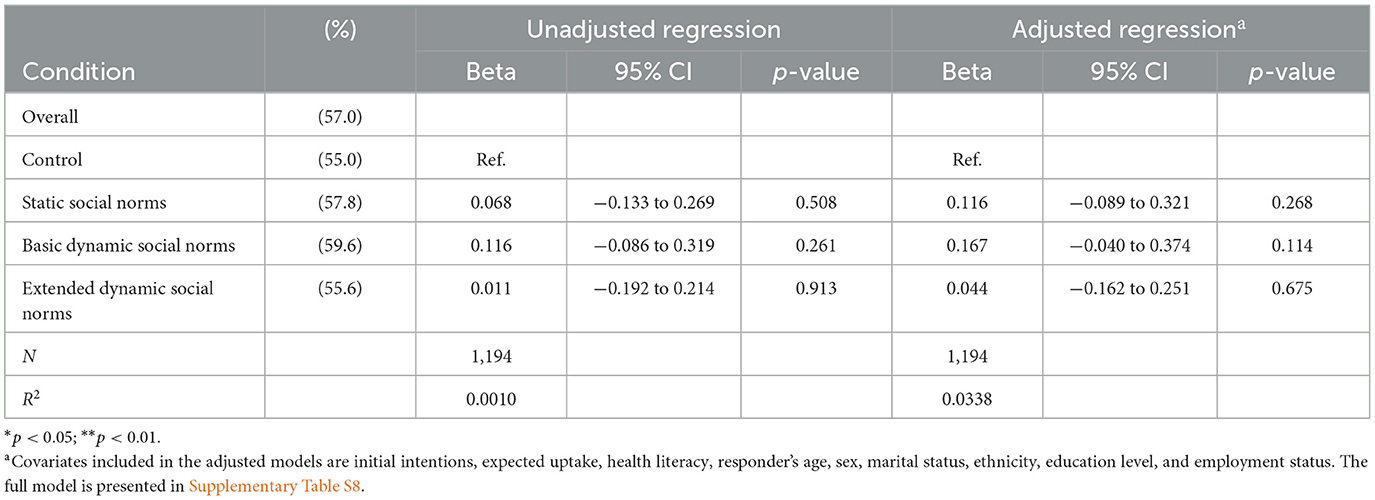
Table 5. Binary probit regression on the effect of the normative messages on “active interest” in reading more about the screening test (N = 1,194).
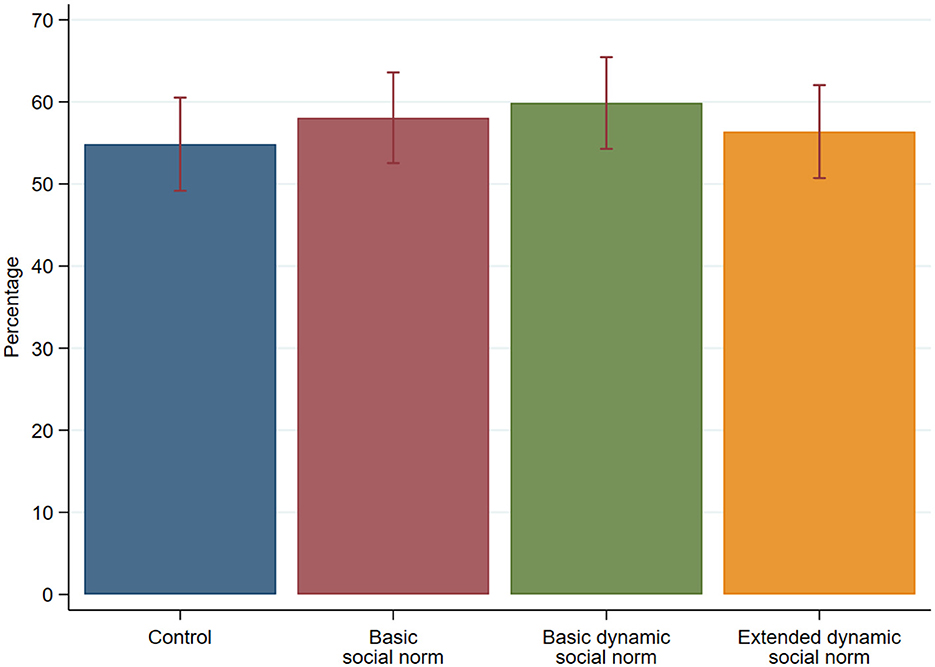
Figure 3. Histogram showing percentage that clicked “I want to read” in the experiment, error bars represent 95% confidence intervals (N = 1,194). Chi-Square test of independence indicates no statistically significant relationship between the active interest and the experimental conditions (chi-square with 3 degrees of freedom = 1.5991, p = 0.660). Independent of experimental condition, 57% of the study participants indicated that they want to read additional information. Furthermore, while most (85.6%) participants who read the additional information about the risk and benefits of the screening test got all three comprehension questions right, a Chi-Square test of independence test did not reveal any differences in BSS knowledge across the conditions (χ2 = 0.5148, p = 0.916, df = 3).
Additionally, 84.5% of participants who read the extra information about the bowel screening test answered all three comprehension questions correctly. However, a Kruskal-Wallis test showed no differences in knowledge across the conditions (χ2 = 0.108, p = 0.991, df = 3).
Perceived informativeness of the normative messages
A closer examination of how respondents perceived the messages shows that most found the information to be very informative (52.7%) or moderately informative (23.9%) (see Figure 4).
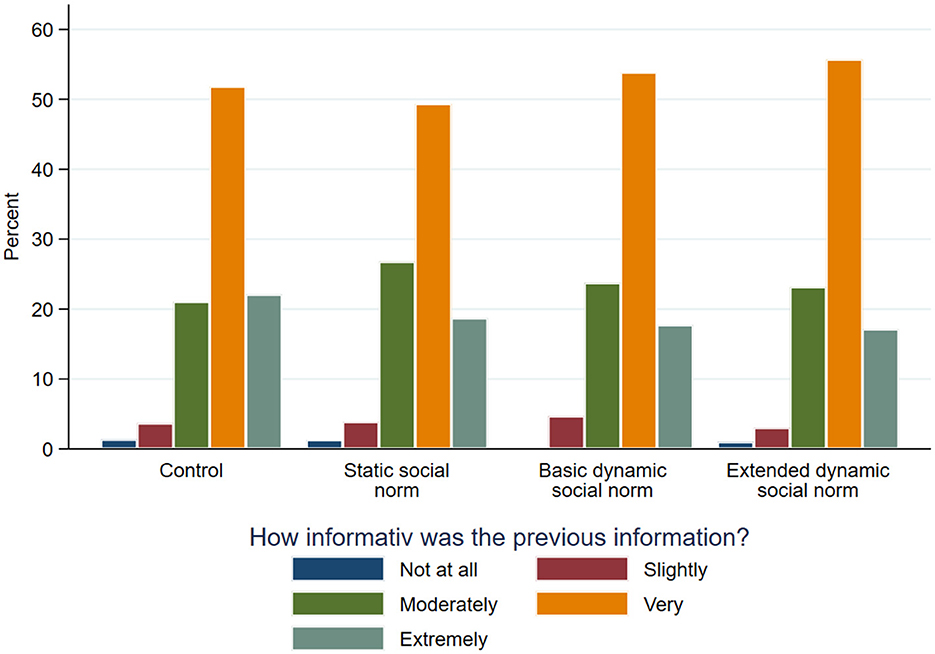
Figure 4. Perception of the provided information (N = 1,194). Chi-Square test of independence indicates no statistically significant relationship between the perception of the messages and the experimental conditions (chi-square with 12 degrees of freedom = 11.3615, p = 0.498).
A univariate Chi-square test [χ2(12) = 22.362, p = 0.498] and adjusted regressions show (see Table 6) that individuals did not perceive the messages containing the normative elements differently (“static social norms”: β = −0.15, 95% CI: −0.33 to 0.02, p = 0.089; “basic dynamic social norms”: β = −0.09, 95% CI: −0.26 to 0.09, p = 0.335 and “extended dynamic social norms”: β = −0.09, 95% CI: −0.27– to 0.09, p = 0.318).
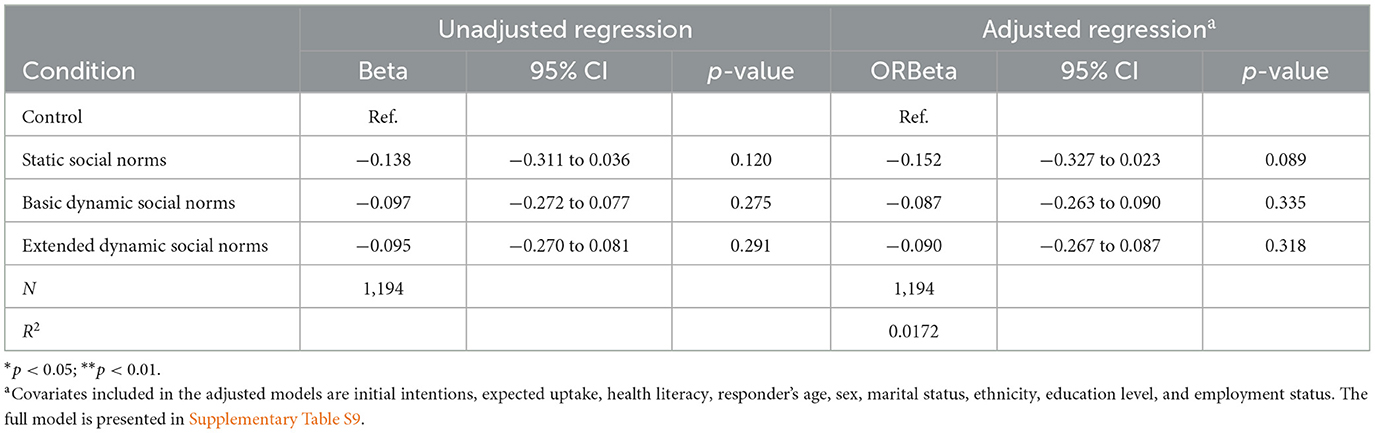
Table 6. Ordered probit regression on the effect of the normative messages on perceived informativeness of the provided information (N = 1,194).
Discussion
To our knowledge, this is the first study to test dynamic social norms messages in the context of colorectal cancer screening. Through a large online experiment involving individuals with lower initial intentions, we examined the effects of communicating static, dynamic, and combined dynamic-static social norms on screening intentions. Contrary to our first working hypothesis and previous studies in the context of sustainable and health behaviors, such as diet and physical activity (Sparkman and Walton, 2017; Mortensen et al., 2019; Loschelder et al., 2019), we found that communicating a positive trend in screening did not increase intentions to complete a FIT compared to a control condition without normative messages. However, combining a dynamic social norms message with a static one led to a greater increase in screening intentions, suggesting added value in incorporating static norms. This may be because static norms provide a reference point to complement the dynamic norms. A subgroup analysis further shows that, consistent with previous studies (von Wagner et al., 2019), the social norms messages influenced screening intentions only among those who initially had low expectations about screening uptake (in this case, < 3 out of 10). Note that overall post-exposure intentions were relatively high in all experimental conditions, and effect sizes were lower than anticipated from the pilot study, limiting the statistical power to compare intentions across the conditions. This is mainly due to the deviation from previous experimental studies on screening intentions, which also excluded individuals who would probably get screened (Stoffel et al., 2019; von Wagner et al., 2019). Furthermore, these two previous studies were on the invasive NHS bowel scope screening (BSS) test, which was more commonly met with resistance by the general population than the simple, home-based stool test (FIT) using in this experiment. We found no significant differences in how informative study participants found the messages and active interest in reading more about FIT across different conditions. Thus, the messages did not negatively influence information seeking, a concern noted in previous studies where simple normative messages have been shown to backfire, especially among resistant individuals, by triggering psychological reactance and promoting behavior contrary to the desired outcome (Schultz et al., 2007). People with negative initial intentions might have strong emotional reactions to screening (Petrova et al., 2015), which could explain why our messages didn't change their behavior or interest in more information.
Our study has several strengths and limitations. First, our experiment featured a relatively large sample size, allowing us to detect small effects. Additionally, our outcome measures included not only intentions but also active interest in reading more information as a behavioral proxy. By varying the way, the same underlying message was conveyed, we reduced the possibility that participants' responses were disproportionately influenced by a specific representation, thereby isolating the effect of the normative message itself rather than its framing. Importantly, none of the messages described uptake as exceeding 7 out of 10, in line with statistics from UK cancer screening programs (NHS England, 2024a). We also controlled for participants' mother tongue in our statistical analyses. The normative messages did not negatively influence information seeking and engagement, suggesting they did not undermine informed decision-making. Finally, the messages were co-developed with patient and public representatives to ensure they were easy to understand and not misleading.
In terms of limitations, our study sample consisted of men and women aged 25–49 who were not screening-eligible at the time they answered the survey, so the screening scenario may not have been relevant for them. Our decision to use non-eligible individuals was motivated by the logistical difficulties of recruiting a large sample of screening-naïve men and women aged exactly 50. A previous study found that younger populations tend to have a lower likelihood of participating in CRC screening (Klabunde et al., 2015). Therefore, the inclusion of a younger age group may affect the generalizability of our findings to the actual eligible population. This is particularly important as the subgroup analysis showed variations in how individuals aged 25–34 reacted to the messages compared to those aged 35–49. Similarly, including individuals who stated they would probably do the test led to higher baseline post-exposure intentions, but this was also due to practical reasons. Note that a separate analysis of only initially disinclined individuals did not show any statistically significant influence of the normative message, likely due to low statistical power. However, the direction of the effects was consistent with those who initially stated they would get screened. Furthermore, our study sample was drawn from a commercial online panel and may therefore not fully represent the broader population eligible for NHS FIT in England, in terms of ethnic composition and educational background. As the survey was self-reported and self-selected, this could have introduced bias from participants with a greater interest in the nature of this research.
Dividing the study into a preliminary survey and experiment, we inevitably lost a small group of eligible participants selected from the screening survey reducing the statistical power to compare intentions across conditions. Additionally, while we provided a brief introduction to FIT in the preliminary survey, we were unable to include a comprehension check in the due to limitations on the number of questions allowed by survey vendor, which may reduce the credibility of participants' responses regarding their intentions to participate in FIT. Fifth, we used different framings of the social norms messages to avoid bias from showing only one framing. However, we did not record which framings were displayed, so we cannot assess which framings were more effective. Instead, we report an average effect for each social norms message. Sixth, the messages were co-produced with patients and public representatives to ensure they were easy to understand and not misleading. There were significant differences in the framings: some were objectively defined by communicating a quantity, while others were subjectively defined using verbal quantifiers. Seventh, although adjusting for covariates improved the detection of significant effects, unmeasured factors, such as attitudes toward bowel cancer, could have further influenced the outcomes. Finally, we only assessed the perceived informativeness of the messages, not their persuasiveness or participants' beliefs about uptake after the social norms messages, to ensure that the study participants understood the messages (von Wagner et al., 2019). While the dynamic social norms message suggested that the positive trend would continue, leading to even higher uptake rates, we did not assess beliefs about screening uptake after the experimental manipulation. Therefore, it is unclear how study participants interpreted the messages, especially the subjective ones.
Implications and future research
These findings have important implications for the NHS BCSP, as screening participation has increased over the last 5 years (Moss et al., 2017; NHS England, 2024b). The NHS long-term plan aims to boost FIT participation rates for earlier cancer detection (NHS England, 2018). Given the positive effect of almost all social norms messages on screening intentions, future campaigns should incorporate these messages, especially among populations with low screening uptake. However, careful consideration of message framing and delivery methods is crucial to maximize impact. Additionally, future studies should investigate objectively and subjectively framed social norms separately. A previous study has shown that subjective social norms messages can have different effects on screening intentions than objectively framed ones (Stoffel et al., 2019). Analyzing the different framings separately would also help identify which ones are most effective. Such future studies should also test these social norms messages with a more diverse study sample that is more representative of the wider population.
Future research could explore the long-term effects of dynamic social norms on actual cancer screening behavior and investigate whether integrating personal risk perceptions and health literacy into normative messaging could create more tailored and effective interventions. Previous literature suggests that negatively framed dynamic messages can enhance moral norms and anticipated regret, thereby strengthening intentions to engage in health behaviors, such as increasing vegetable intake (Rivis et al., 2009; Stok et al., 2014). However, research on negatively framed social norms messages in cancer screening remains limited. Testing the effectiveness of such messages in future studies would be valuable.
Furthermore, while we recorded participants' perception of current FIT uptake rates in England, we did not examine the relationship between this perception and post-exposure intentions. Although most participants underestimated the actual uptake rate, a small portion expected a high uptake rate but still expressed low screening intentions. Future studies could investigate how perceptions of current uptake rates influence behavioral intentions, as previous research shows that normative messages are more persuasive among individuals who perceive higher engagement rates among their peers (Smith and Louis, 2008).
Previous studies indicate that even when individuals recognize the benefits of certain behaviors, they may resist change if they view the behavior as incompatible with their values, unimportant, or feel incapable of change (Sparkman and Walton, 2019). Addressing these underlying beliefs and barriers is essential for effective interventions. Finally, exploring strategies that initiate deeper cognitive engagement and address negative affective responses may improve the efficacy of normative messages, particularly among individuals with negative initial intentions.
Conclusion
This study showed that dynamic social norms messages can effectively encourage individuals to participate in cancer screenings. By highlighting the positive trend in screening participation alongside the current uptake rate, our messages successfully increased screening intentions among men and women with initially low intentions. Future research should explore the use of dynamic social norms across diverse settings, employing varied approaches and incorporating randomized controlled trials to strengthen the evidence base.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://osf.io/p8jh2/.
Ethics statement
The studies involving humans were approved by University College London (UCL) Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SS: Writing – original draft, Writing – review & editing. JG: Writing – original draft, Writing – review & editing. YH: Writing – original draft, Writing – review & editing. CV: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frbhe.2025.1566172/full#supplementary-material
References
Cialdini, R. B., and Goldstein, N. J. (2004). Social influence: compliance and conformity. Annu. Rev. Psychol. 55, 591–621. doi: 10.1146/annurev.psych.55.090902.142015
Cialdini, R. B., and Trost, M. R. (1998). Social Influence: Social Norms, Conformity and Compliance (Boston, MA; New York, NY).
Dempsey, R. C., McAlaney, J., and Bewick, B. M. (2018). A critical appraisal of the social norms approach as an interventional strategy for health-related behavior and attitude change. Front. Psychol. 9:2180. doi: 10.3389/fpsyg.2018.02180
Dumenci, L., Matsuyama, R., Riddle, D. L., Cartwright, L. A., Perera, R. A., Chung, H., et al. (2014). Measurement of cancer health literacy and identification of patients with limited cancer health literacy. J. Health Commun. 19, 205–224. doi: 10.1080/10810730.2014.943377
Geber, S., Tribelhorn, L., Hitchman, S. C., and Friemel, T. N. (2022). Dynamic norms for dynamic times? An experiment on the effects of dynamic and static norms messages on COVID-19 vaccination intention. SCM Stud. Commun. Media 11, 453–476. doi: 10.5771/2192-4007-2022-3-453
Gorini, G., Betti, E., Stoffel, S., Falini, P., Iossa, A., Senore, C., et al. (2023). Testing behavioral economics messages to increase non-responders' participation in organized colorectal cancer-screening programs: a randomized controlled trial. Prev. Med. 174:107615. doi: 10.1016/j.ypmed.2023.107615
Graupensperger, S., Lee, C. M., and Larimer, M. E. (2021). Leveraging dynamic norms to reduce alcohol use among college students: a proof-of-concept experimental study. Alcoholism 45, 2370–2382. doi: 10.1111/acer.14718
Klabunde, C., Blom, J., Bulliard, J. L., Garcia, M., Hagoel, L., Mai, V., et al. (2015). Participation rates for organized colorectal cancer screening programmes: an international comparison. J. Med. Screen. 22, 119–126. doi: 10.1177/0969141315584694
Loschelder, D. D., Siepelmeyer, H., Fischer, D., and Rubel, J. A. (2019). Dynamic norms drive sustainable consumption: norm-based nudging helps café customers to avoid disposable to-go-cups. J. Econ. Psychol. 75:102146. doi: 10.1016/j.joep.2019.02.002
Marteau, T. M., Dormandy, E., and Michie, S. (2001). A measure of informed choice. Health Expect. 4, 99–108. doi: 10.1046/j.1369-6513.2001.00140.x
Michie, S., and Abraham, C. (2004). Interventions to change health behaviours: evidence-based or evidence-inspired? Psychol. Health 19, 29–49. doi: 10.1080/0887044031000141199
Mortensen, C. R., Neel, R., Cialdini, R. B., Jaeger, C. M., Jacobson, R. P., and Ringel, M. M. (2019). Trending norms: a lever for encouraging behaviors performed by the minority. Soc. Psychol. Person. Sci. 10, 201–210. doi: 10.1177/1948550617734615
Moss, S., Mathews, C., Day, T. J., Smith, S., Seaman, H. E., Snowball, J., et al. (2017). Increased uptake and improved outcomes of bowel cancer screening with a faecal immunochemical test: results from a pilot study within the national screening programme in England. Gut 66, 1631–1644. doi: 10.1136/gutjnl-2015-310691
NHS England (2018). Cancer: Better care for major health conditions [Chapter 3]. The NHS Long Term Plan. National Health Service. Available online at: https://www.longtermplan.nhs.uk/online-version/chapter-3-further-progress-on-care-quality-and-outcomes/better-care-for-major-health-conditions/cancer/ (accessed September 20, 2024).
NHS England (2024a). Research and analysis: Bowel Cancer Screening Annual Report 2021 to 2022. National Health Service. Available online at: https://www.gov.uk/government/publications/bowel-cancer-screening-annual-report-2021-to-2022/bowel-cancer-screening-annual-report-2021-to-2022 (accessed September 16, 2024).
NHS England (2024b). NHS Launches Tool to Improve Bowel Cancer Screening for People With Sight Loss. National Health Service. Available online at: https://www.england.nhs.uk/2024/05/nhs-launches-tool-to-improve-bowel-cancer-screening-for-people-with-sight-loss/ (accessed January 21, 2024).
Occa, A., Morgan, S. E., Peng, W., Mao, B., McFarlane, S. J., Grinfeder, K., et al. (2021). Untangling interactivity's effects: the role of cognitive absorption, perceived visual informativeness, and cancer information overload. Pat. Educ. Counsel. 104, 1059–1065. doi: 10.1016/j.pec.2020.10.007
Petrova, D., Garcia-Retamero, R., and Cokely, E. T. (2015). Understanding the harms and benefits of cancer screening: a model of factors that shape informed decision making. Med. Decis. Making 35, 847–858. doi: 10.1177/0272989X15587676
Rivis, A., Sheeran, P., and Armitage, C. J. (2009). Expanding the affective and normative components of the theory of planned behavior: a meta-analysis of anticipated affect and moral norms. J. Appl. Soc. Psychol. 39, 2985–3019. doi: 10.1111/j.1559-1816.2009.00558.x
Schultz, P. W., Nolan, J. M., Cialdini, R. B., Goldstein, N. J., and Griskevicius, V. (2007). The constructive, destructive, and reconstructive power of social norms. Psychol. Sci. 18, 429–434. doi: 10.1111/j.1467-9280.2007.01917.x
Sheeran, P., Klein, W. M., and Rothman, A. J. (2017). Health behavior change: moving from observation to intervention. Ann. Rev. Psychol. 68, 573–600. doi: 10.1146/annurev-psych-010416-044007
Sieverding, M., Decker, S., and Zimmermann, F. (2010b). Information about low participation in cancer screening demotivates other people. Psychol. Sci. 21, 941–943. doi: 10.1177/0956797610373936
Sieverding, M., Matterne, U., and Ciccarello, L. (2010a). What role do social norms play in the context of men's cancer screening intention and behavior? Application of an extended theory of planned behavior. Health Psychol. 29:72. doi: 10.1037/a0016941
Smith, J. R., and Louis, W. R. (2008). Do as we say and as we do: The interplay of descriptive and injunctive group norms in the attitude–behaviour relationship. Br. J. Soc. Psychol. 47, 647–666. doi: 10.1348/014466607X269748
Sparkman, G., and Walton, G. M. (2017). Dynamic norms promote sustainable behavior, even if it is counternormative. Psychol. Sci. 28, 1663–1674. doi: 10.1177/0956797617719950
Sparkman, G., and Walton, G. M. (2019). Witnessing change: dynamic norms help resolve diverse barriers to personal change. J. Exp. Soc. Psychol. 82, 238–252. doi: 10.1016/j.jesp.2019.01.007
Stoffel, S. T., Goodwin, M., Sieverding, M., Vlaev, I., and von Wagner, C. (2019). Testing verbal quantifiers for social norms messages in cancer screening: evidence from an online experiment. BMC Public Health 19, 1–11. doi: 10.1186/s12889-019-6997-5
Stok, F. M., Verkooijen, K. T., de Ridder, D. T., de Wit, J. B., and De Vet, E. (2014). How norms work: self-identification, attitude, and self-efficacy mediate the relation between descriptive social norms and vegetable intake. Appl. Psychol. 6, 230–250. doi: 10.1111/aphw.12026
Taylor, L. C., Kerrison, R. S., Herrmann, B., and Stoffel, S. T. (2022). Effectiveness of behavioural economics-based interventions to improve colorectal cancer screening participation: a rapid systematic review of randomised controlled trials. Prev. Med. Rep. 26:101747. doi: 10.1016/j.pmedr.2022.101747
Keywords: social norms, dynamic social norms, static social norms, cancer screening, intentions, experiment
Citation: Stoffel ST, Gao J, Hirst Y and Von Wagner C (2025) The impact of dynamic social norms messages on motivation to participate in organized colorectal cancer-screening programmes: evidence from an online experiment. Front. Behav. Econ. 4:1566172. doi: 10.3389/frbhe.2025.1566172
Received: 24 January 2025; Accepted: 23 April 2025;
Published: 16 May 2025.
Edited by:
Adeline Delavande, University of Technology Sydney, AustraliaReviewed by:
Mehdi Farsi, Université de Neuchâtel, SwitzerlandLe Zhang, Macquarie University, Australia
Copyright © 2025 Stoffel, Gao, Hirst and Von Wagner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandro Tiziano Stoffel, c2FuZHJvLnN0b2ZmZWxAdW5pYmFzLmNo