 Sarah Gregory1*
Sarah Gregory1* John Harrison2,3,4Janna Herrmann5Matthew Hunter1Natalie Jenkins1,6Alexandra König5,7
John Harrison2,3,4Janna Herrmann5Matthew Hunter1Natalie Jenkins1,6Alexandra König5,7 Nicklas Linz5
Nicklas Linz5 Saturnino Luz8Elisa Mallick5Hannah Pullen1,2Miles Welstead1,2Stephen Ruhmel9Johannes Tröger5Craig W. Ritchie1,2
Saturnino Luz8Elisa Mallick5Hannah Pullen1,2Miles Welstead1,2Stephen Ruhmel9Johannes Tröger5Craig W. Ritchie1,2- 1Edinburgh Dementia Prevention, Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
- 2Scottish Brain Sciences, Edinburgh, United Kingdom
- 3Department of Neurology, Alzheimer Center Amsterdam, Amsterdam University Medical Centers, Vrije Universiteit, Amsterdam, Netherlands
- 4King's College London, Institute of Psychiatry, Psychology and Neuroscience, London, United Kingdom
- 5ki:elements GmbH, Saarbrücken, Germany
- 6Institute of Neuroscience and Psychology, University of Glasgow, Glasgow, United Kingdom
- 7CoBTek (Cognition-Behaviour-Technology) Lab, Université Côte d'Azur, Nice, France
- 8Usher Institute, University of Edinburgh, Edinburgh, United Kingdom
- 9Janssen Research & Development, LLC, Raritan, NJ, United States
Introduction: Digital cognitive assessments are gathering importance for the decentralized remote clinical trials of the future. Before including such assessments in clinical trials, they must be tested to confirm feasibility and acceptability with the intended participant group. This study presents usability and acceptability data from the Speech on the Phone Assessment (SPeAk) study.
Methods: Participants (N = 68, mean age 70.43 years, 52.9% male) provided demographic data and completed baseline and 3-month follow-up phone based assessments. The baseline visit was administered by a trained researcher and included a spontaneous speech assessment and a brief cognitive battery (immediate and delayed recall, digit span, and verbal fluency). The follow-up visit repeated the cognitive battery which was administered by an automatic phone bot. Participants were randomized to receive their cognitive test results acer the final or acer each study visit. Participants completed acceptability questionnaires electronically acer each study visit.
Results: There was excellent retention (98.5%), few technical issues (n = 5), and good interrater reliability. Participants rated the assessment as acceptable, confirming the ease of use of the technology and their comfort in completing cognitive tasks on the phone. Participants generally reported feeling happy to receive the results of their cognitive tests, and this disclosure did not cause participants to feel worried.
Discussion: The results from this usability and acceptability analysis suggest that completing this brief battery of cognitive tests via a telephone call is both acceptable and feasible in a midlife-to-older adult population in the United Kingdom, living at risk for Alzheimer's disease.
1. Introduction
With neurodegenerative disease continuing to grow as a major global public health concern (Nichols et al., 2019), identifying risk factors and early biomarkers of neurodegenerative diseases has become increasingly important (Livingston et al., 2017, 2020). Currently, biomarkers for Alzheimer's disease (AD), the most common cause of dementia, tend to be expensive and invasive for the patient or research participant (Peskind et al., 2005; Wittenberg et al., 2019). Commonly used AD biomarkers include amyloid positron emission tomography scans (Chételat et al., 2020), cerebrospinal fluid amyloid and tau levels (Blennow and Zetterberg, 2018; Blennow et al., 2019), and plasma amyloid and tau concentrations (Hampel et al., 2018). These biomarkers are largely limited to specialist hospitals and are not globally accessible. Investigating speech as an AD biomarker may be an important contribution to decentralizing screening and profiling tools on a global scale.
Speech data are relatively easy to collect and require technological solutions that do not rely on specialist staff and facilities. Furthermore, it is a non-invasive and safe technique that may be more acceptable to patients, participants, and the public compared to currently used AD biomarkers, as a first procedure to identify those most likely to be AD biomarker positive. Previous studies have found important associations between features of speech and AD biomarkers (Boschi et al., 2017). Speech markers of interest include semantic processing errors, failure-to-stop errors, changes in connected speech, and declines in syntactic complexity (Ahmed et al., 2013; Venneri et al., 2018; Gollan et al., 2020; Mueller et al., 2021). Assessments of cognition made using speech and language technology have been found to be at least as equally discriminative between different groups when compared to traditional neuropsychological assessment (Garcia et al., 2020). These studies have collected data through face-to-face interactions between researchers and participants, which may again perpetuate the barriers to traditional biomarker testing access. Harnessing technology to gather these speech data remotely, be that via the telephone or videoconferencing platforms, will be an important step in widening access to research opportunities. This may even include digital assistants, such as Alexa, Siri, and Google Assistant, which collect “ambient intelligence” but would need to be considered within a well-designed ethical framework (Simon et al., 2022). These benefits are particularly relevant with the move to decentralized trials and trial access to traditionally underserved groups.
Evidence from studies collecting data remotely has shown comparative performance to human evaluators when making cognitive screening decisions (König et al., 2018; Konig et al., 2018; Themistocleous et al., 2020). A recent review by our group found that remote administration of cognitive tests (via telephone or video-calling) was typically consistent with in-person administration but variable and limited at the person/test level, with stronger evidence existing for videoconferencing over telephone calls, highlighting a need for further research in this area (Hunter et al., 2021). The COVID-19 pandemic drove the need to further explore the feasibility of conducting cognitive assessments via remote means, again with videoconferencing methods more typically considered for the adaptation of traditional cognitive assessments (Geddes et al., 2020). A number of cognitive assessments have also been adapted or even designed to be administered via telephone call with this form of assessment appearing to be viable, although not meant to replace gold-standard in-person evaluations (Carlew et al., 2020).
When developing new digital biomarkers, it should be of high priority that acceptability to users is also evaluated. Successful engagement with a novel tool can only arise when it has a favorable acceptability profile. A previous study using a different tool found that collecting speech data on the phone was acceptable to a group of older adults (Diaz-Asper et al., 2021). This study used a short cognitive task of language fluency, as well as a more narrative speech task, and is a helpful indicator of the likely acceptability of collecting speech biomarkers on the phone. Automated testing in the form of social robot administration and smartphone applications have previously been reported to be most feasible and acceptable to participants (Takaeda et al., 2019; Taylor et al., 2023), although in-person human cognitive testing remains mainstream in most clinical and research settings. The recent paradigm shift to digital neuropsychology warrants consideration from validity and ethical perspectives. Barriers to the digitalization of cognitive testing typically focus on operational issues, such as hardware and software barriers, as well as on the validity of the same test across different devices (Germine et al., 2019), with less attention paid to the acceptability of the digital version to patients and research participants. The use of artificial intelligence and machine learning in dementia detection is also a topic of ethical interest. As models derived from these techniques need to be trained on large data sets, these are commonly initially derived in data sets from research participants who often do not represent the general population living with dementia and, as such, have limits to their generalizability (Ford et al., 2023). Included acceptability in the earliest stages of digital biomarker design may be one opportunity to more holistically consider all ethical aspects of these new tools.
Disclosure of participant-level data in research studies is an area of increasing interest, and the routine disclosure of data collected on the phone is an important part of feasibility and acceptability testing. Previous studies suggest that there is a public demand for greater information about their risk factors and current disease status regarding AD, particularly surrounding disclosure of APOEε4 genotype and AD biomarkers (Unterman et al., 1993; Caselli et al., 2014; Ott et al., 2016). A number of studies have investigated the psychological impact of disclosure of genotype and biomarkers and typically found no associations with long-term psychological distress or risks of anxiety or depression (Green et al., 2009; Lim et al., 2016; Burns et al., 2017; Taswell et al., 2017; Wake et al., 2017; Grill et al., 2020). However, some studies have identified short-term adverse outcomes alongside positive experiences (Vanderschaeghe et al., 2017; Largent et al., 2020). Thus, there is a need to provide psychological safety considerations to prevent possible harm. Cognitive test results completed in research settings are rarely fed back, particularly not to healthy participants or those with mild cognitive impairment (MCI). Nevertheless, cognitive tasks are commonly utilized, and anecdotally many participants express interest in their personal test performance. Understanding the acceptability of providing these test results and the consequences is an important consideration.
The Speech on the Phone Assessment (SPeAk) study (Gregory et al., 2022) was designed to collect speech data on the phone at two time points from participants at risk for AD, using both semi-structured and structured speech tasks. This study aimed to assess the usability and acceptability of the study protocol in this population. There was also an analysis of the acceptability of receiving cognitive test results in the context of a research setting.
2. Methods
2.1. Study design
The SPeAk study was a prospective observational study. Fully described in a protocol paper (Gregory et al., 2022), briefly, the study involved participants completing a baseline and 3-month follow-up visit. An iPad with the Mili platform (previously called the Delta Testing App) was used to place the phone calls to participants and facilitate the assessments. The Mili platform has been validated in a previous study for the semantic fluency task (Tröger et al., 2018, 2019) and the speech biomarker for cognition (Tröger et al., 2022). The first visit was completed with a trained research assistant delivering verbatim task instructions, while the second visit used an automated voice to provide the instructions. Audio of both visits was recorded in the app.
2.2. Ethics
The SPeAk study was reviewed and given a favorable ethical opinion by the Edinburgh Medical School Research Ethics Committee (REC Reference 20-EMREC-007).
2.3. Participants
Participants were eligible for inclusion in the study if they had previously engaged in cognitive testing at the research site, through either the European Prevention of Alzheimer's Dementia Longitudinal Cohort Study (EPAD LCS; Ritchie et al., 2016, 2020) or the CHARIOT-Pro Substudy (Udeh-Momoh et al., 2021). Participants in these studies represent a spectrum of risk for future development of AD dementia from healthy volunteers to those with MCI. Based on previous study eligibility criteria, participants were aged 50 years or older, fluent in English, and did not have a diagnosis of dementia (although could have a diagnosis of MCI). For the SPeAk study, participants were required to have the capacity to provide informed consent, have access to a phone line (either a mobile phone or a landline), and be available to participate in both visits. As participants were required to have sufficient hearing ability to participate in cognitive testing for previous studies, there were no specific eligibility criteria related to hearing in this protocol. The primary aim of the study was to evaluate an algorithm predicting amyloid and tau status using speech features. The sample size calculation suggested a minimum of 66 participants was required to provide sufficient power for the primary aim. The results reported in this article reflect secondary outcome measures, and as such, there is the potential for any findings to be underpowered, as the overall sample size calculation was not conducted for these outcomes.
2.4. Recruitment
Study information was emailed to participants previously enrolled in the EPAD or CHARIOT-Pro Substudy who had provided consent to be contacted about future study opportunities. Participants were provided with an opportunity to ask questions about the study, either via email or a follow-up telephone call. Participants provided electronic consent using Online Survey software (https://www.onlinesurveys.ac.uk/), with consent verbally re-affirmed by the research assistant at the start of the first visit.
2.5. Demographics
At the start of the baseline visit, participants verbally reported gender, age, years of education, and current medications to the research assistant.
2.6. Cognitive testing
Participants completed cognitive assessments over the phone at the baseline visit and again at 3-month follow-up. At the baseline visit, participants completed two spontaneous speech tasks to provide an opportunity for the collection of more natural speech patterns. The cognitive assessments included three main tasks: list learning (immediate and delayed recall from the Rey Auditory Verbal Learning Test [RAVLT]; Bean, 2011) as well as forward digit span and fluency (phonemic and semantic). During the immediate recall list learning, task participants were read a list of 15 words, 1 per second, and were asked to repeat back as many words as they could remember, with the task repeated five times. After an approximately 10-min delay (during which the digit span and fluency tasks were administered), the participants were asked to recall as many of the 15 words as they could. The digit span task involved participants being read a series of numbers of increasing length (starting from two digits and working up to nine digits) and asked to repeat the series. Each digit sequence length had two trials. Participants completed two fluency tasks, for the semantic fluency task participants were asked to name as many animals as they could think of within 1 min, while for the phonemic fluency task participants were asked to name as many words beginning with the letter S as they could within a minute. During the baseline visits, three raters conducted the testing. All underwent the same training and delivered the task instructions verbatim to participants. The second visit was conducted using an automatic phonebot. The first testing session lasted up to 30 min, and the second testing session took ~15 min. All cognitive tasks were selected to represent domains sensitive to decline in early AD.
Speech data were also collected throughout the assessment, although no speech data are included in this current analysis. The speech data were collected by recording the cognitive assessments, from the spontaneous speech task onward. Language and speech variables were extracted on a linguistic and acoustic-level basis, including temporal, voice source, formant, semantic, and synthetic variables.
2.7. Results feedback
Participants received feedback after either each testing session or after their study completion and were equally randomized to each feedback condition using a random-number generator prior to enrolment. The feedback included scores on the immediate and delayed recall, digit span, and fluency tasks, with normative scores where available. A brief explanation of the experimental nature of the tasks and support-line phone numbers were included in the results feedback proforma. Any participants who performed outside of expected ranges had their data reviewed by the principal investigator (CWR), and additional feedback phone calls were provided if deemed clinically necessary. Feedback was only provided on the first variable extracted from the speech files (the classical neuropsychological outcome variables) and not on either of the speech features regarding language and speech descriptors.
2.8. Acceptability questionnaires
Participants were emailed a copy of an acceptability questionnaire on completion of the baseline and again for the 3-month follow-up visit. These questionnaires (12 questions, 11 Likert-scale questions, and 1 open-ended question or any other comments) asked participants to rate their experience of setting up the study visits, comfort in completing the tests in their home environment, preferences on the cognitive testing format, and experience on receiving results. To encourage participants to feel able to report their honest experiences of study participation, no participant identification was linked to the acceptability questionnaires. See the Supplementary material for acceptability questionnaires.
2.9. Data analysis
Descriptive statistics were used to describe the demographic details of the included participants, as well as the floor and ceiling effects of the tests. The test–retest reliability was compared using paired t-tests after tests of normality confirmed a normal distribution for all tasks. Change scores were calculated for each task using the Reliable Change Index (RCI). Participants with missing data were pairwise excluded from the final analysis. Summary statistics were used to describe the acceptability questionnaire data, as well as narrative synthesis of qualitative data from free-text fields. Baseline and 3-month responses were compared using paired t-tests. The statistical analysis was carried out using Excel and R Studio (Version 2022.07.1+554).
3. Results
3.1. Demographics
In total, 69 participants consented to participate in the SPeAk study. One participant declined to participate in any protocol activities post-consent, including the provision of demographic data, after changing their minds about completing the cognitive tasks. Thus, the data presented in this article are from the remaining 68 participants. There was a nearly equal split of men and women enrolled in the study (36 men [52.9%] vs. 33 women [47.1%]), with a mean age of 70.43 (SD: 6.94) years, and a high average education (16.10, SD: 3.68) years. Most participants were living as a couple (n = 50, 73.5%). On average, participants were taking 2.09 (SD 2.23) medications. Rater 1 completed the majority of the cognitive testing at the baseline visit (n = 55, 80.9%), with raters 2 and 3 completing nearly equivalent visits (n = 7, 10.3%; n = 6, 8.8%, respectively; see Table 1 for full demographic details).
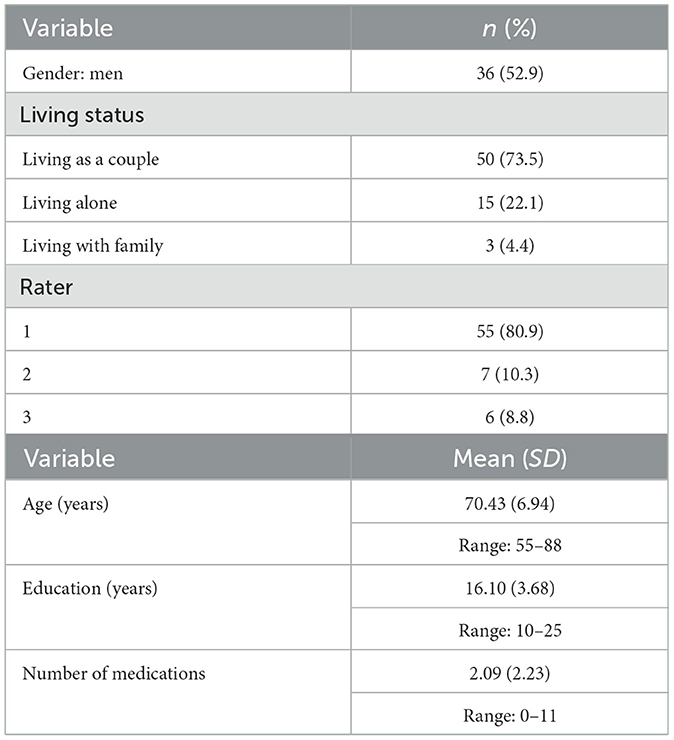
Table 1. Descriptive statistics for participants included in the SPeAk study (N = 68).
3.2. Retention
One participant withdrew from the study between the first and second visit due to not enjoying completing tasks on the phone, resulting in a retention rate of 98.5% (67 of 68 participants completed both visits).
3.3. Technological issues
A small number of technical or operational issues were reported during the study, with five technical issues resulting in the follow-up visit completed outside of the protocol window, one network issue causing a failed automated call that was resolved at a later attempt, one participant with hearing difficulties that impaired list learning completion at baseline but not follow-up, and two participants who misheard the letter during the phonemic fluency task during the follow-up visit. This resulted in nine technical or operational issues reported across the 135 visits completed (6.7%).
3.4. Cognitive test scores
Other than the withdrawn participant and the participant with hearing impairment at baseline, there were no missing data for any of the cognitive test outcomes. There was a significant decline in performance on the digit span task between baseline and follow-up visit as well as a significant improvement in performance on the phonemic fluency task at the second visit. It is possible that there was an actual decline in digit span abilities in the participant group during the 3-month study period; however, this may also reflect increased difficulty in completing the task when delivered by an automatic phonebot. The increase in performance on the phonemic fluency task is likely to reflect a small learning effect. There were no changes in performance on the immediate or delayed list learning or the semantic fluency tasks. The means, standard deviations, and ranges of test scores are presented in Table 2.
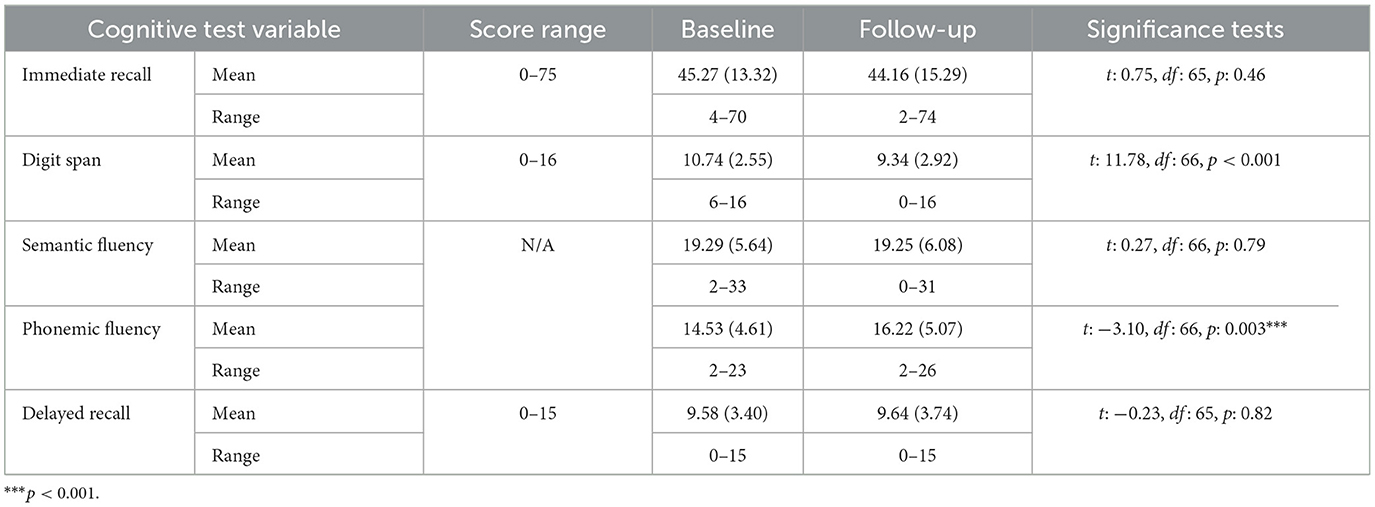
Table 2. Table of cognitive test scores at baseline and follow-up visit with comparative statistics included.
Analyses were conducted to understand the impact of gender, age, and education (known risk factors for neurodegeneration) on cognitive test performance. Women performed significantly better than men on immediate recall at both baseline and follow-up visits and on delayed memory tasks at the follow-up visit only. At the follow-up visit, women also performed significantly better on the semantic fluency task compared to men. Full details are presented in Table 3. Older age was significantly associated with poorer performance on all tasks except phonemic fluency at both visits and semantic fluency at baseline, where there was no significant association with age. Higher total years of education were associated with higher scores on digit span, phonemic fluency, immediate recall, and semantic fluency. There were no effects of the number of medications on any cognitive test scores.
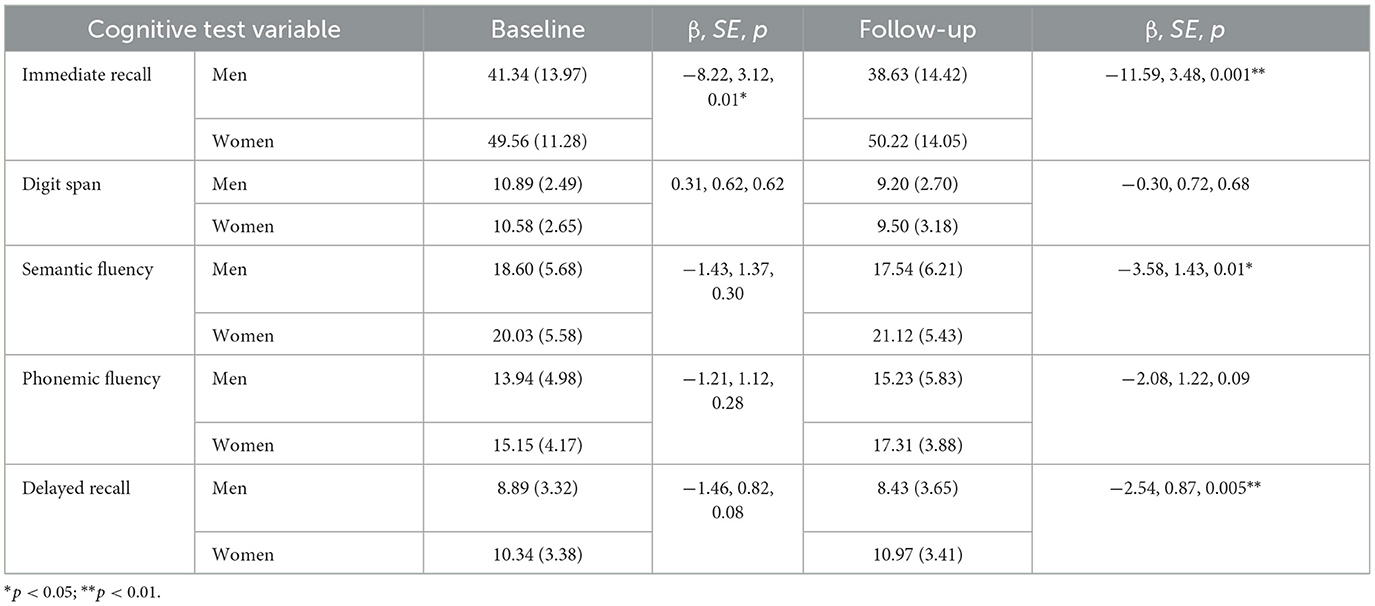
Table 3. Table of cognitive test scores at baseline and follow-up visit by gender.
Considering the RCIs for the five cognitive tests, one participant performed worse on all tasks at the follow-up visit. Across most tasks, there was a mix of better, worse, or no change in performance. The exception was for digit span where there was a slight bias toward a worse performance at the follow-up visit. This was particularly noticeable in men compared to women. Those who performed worse on this task were significantly older (71.96 ± 7.13 years) compared to those who performed better (68.36 ± 6.95 years) or had no reliable change (66.00 ± 4.22 years) on the tasks (p:0.02). There were no other significant differences in change scores by sex (see Supplementary Table 1), age, or education.
Disclosure status (after both visits or only after the follow-up visit) did not have any significant associations with test scores at the follow-up visit. There was a significant difference between the proportion of participants who performed worse at the follow-up visit for the delayed recall test depending on disclosure status however, as there was no association with the score results (β: 0.01, SE: 0.92, p: 0.99) this is likely to be a spurious finding.
3.5. Interrater reliability
As presented in Table 1, most of the baseline assessments were completed by rater 1 (n = 55, 80.9%), with the remaining assessments completed by raters 2 and 3 (n = 7, 10.3%, and n = 6, 8.8%, respectively). There were no significant differences between participants' cognitive test scores between raters for the memory tasks, digit span, or phonemic fluency. Semantic fluency scores were significantly higher for participants rated by rater 3 compared to rater 1 (β: 6.50. SE: 2.73, p: 0.02). All data were quality-checked by an independent rater, and no issues were identified, suggesting this is a random effect.
3.6. Acceptability
In total, 61 participants completed the acceptability questionnaire after their baseline visit (61/69, 88.4%), and 56 (56/67, 83.6%) completed it following their second visit.
3.6.1. Functionality of software
At both the baseline and follow-up visits, participants found it easy or extremely easy to set up the appointment, and in general, the sound quality of the call was rated as “OK” to “good”. There was a significant difference in the ease of the set-up, with the baseline appointment rated as easier to set up than the follow-up, with no significant differences between ratings of sound between the baseline and follow-up visits. The full results are available in Table 4.
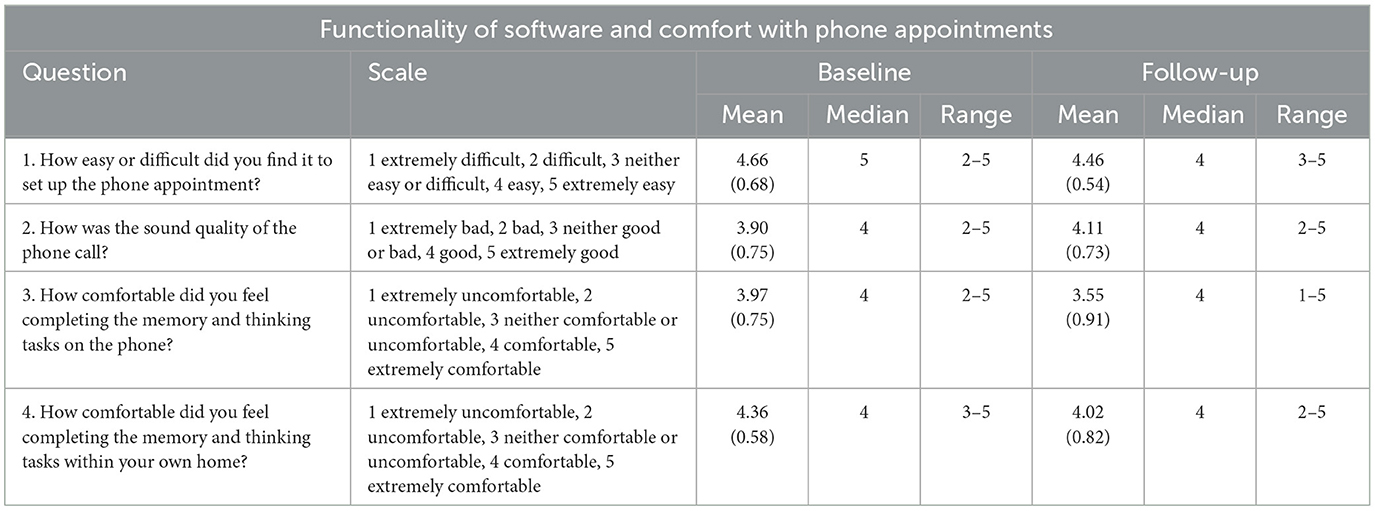
Table 4. Functionality of software and comfort with phone appointments.
Although generally rated as “OK” to “good”, some participants did provide additional feedback about the sound of the calls, both at baseline and follow-up visits, particularly relating to the word list task:
“Better sound quality would be a help—some words were indistinct and there seemed to be a slight echo as if the tester was in an empty room”. Baseline
“Sometimes difficult to pick up pronunciation of words over the phone compared to face-to-face”. Baseline
“In the computer test if I did not hear a word well I could not retrieve it”. Follow-Up
3.6.2. Comfort of participants
Participants were comfortable both with completing the assessments on the phone and completing these tasks within their home environments. Despite scores remaining in the comfortable range at follow-up, significance tests showed that participants reported significantly higher comfort at baseline compared to follow-up both with completing the tasks on the phone and in their own home. The full results are available in Table 4.
Reflecting the generally high rating scores, some participants provided positive feedback in their comments about how it felt to complete the tests at home:
“It was easy to do from home”. Baseline
“I did not find it strange doing the questions, conversation via the phone”. Baseline
However, other participants provided feedback on feeling less comfortable completing these tests in their own home:
“Although more relaxed I felt less relaxed answering them in my own home which surprised me”. Baseline
“At home there are distractions which made me hesitate and [do] less well with some questions”. Follow-up
“I was worried someone might knock on my back door or try to test or ring on the phone I was using”. Follow-up
3.6.3. Preferences
Despite the ease and comfort of participants in completing these tasks, participants did tend to express a preference for completing these tasks in person—which they had done during previous EPAD or CHARIOT Pro visits compared to on the phone. When asked to consider a preference between a human tester and an automatic phonebot, participants showed a preference for a human tester. These responses suggest that it is the human element that participants enjoy when taking part in research. These results should be considered within the context of the participants at the time of the study being in a government-mandated lockdown due to COVID-19, not social unrest, when social isolation may have been a factor in their preference for seeing or speaking to a real person.
Although there was a clear preference for in-person or with-person testing, participants indicated they would be happy to complete the memory tests on the phone again with either a human or an automatic phonebot. Although participants were generally happy with both settings, when we compared the baseline and follow-up scores, participants were significantly more positive about completing future tests with a human than an automatic phonebot.
When anticipating the second automatic phonebot phone call, participants expected it to be worse or the same as the first call with a human tester, with the actual experience rated as the same as the first call, which is interesting given the preference for the call involving a human tester. A comparison of the baseline and follow-up scores found the follow-up experience was reported as significantly higher than the baseline expectation. The full results are available in Table 5.
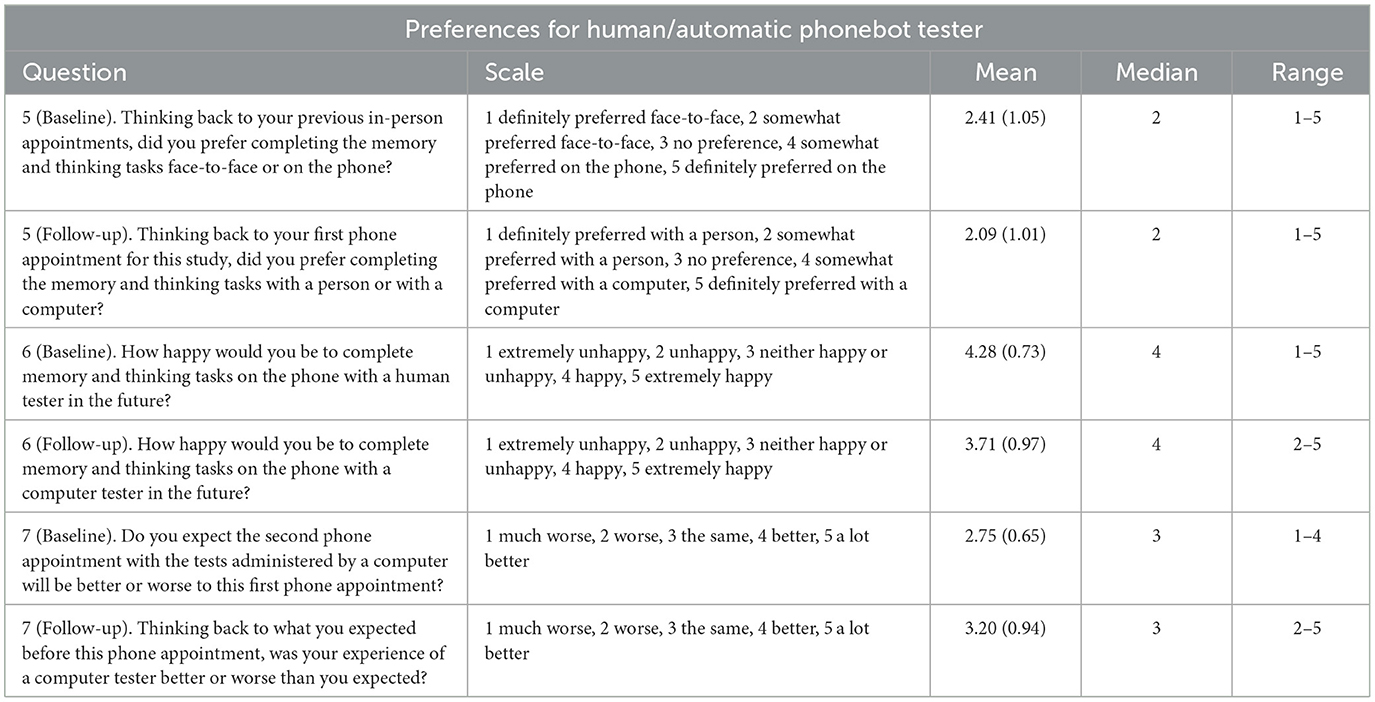
Table 5. Preferences for human/automatic phonebot tester.
Comments from participants represented a spectrum of preferences, with some participants commenting on the convenience of phone testing and the ease of completing these tasks having met the tester in person before:
“…the phone appointment is more convenient than traveling for face to face”. Baseline
“I think that it was easy to do the tasks over the phone as I have done them face to face before. Moreover, I had met the interviewer/task manager in person in recent years on the... study. I think both of these points had a bearing on my positive attitude to the tasks”. Baseline
A majority of participants who provided comments at the follow-up visit showed a clear preference for interacting with a person, either in person or on the phone:
“I prefer the human contact, although the computer was clear and concise”. Follow-up
“With the computer, it was hard to gauge how much think-time I had left. With a person, you can see if they are just watching the time.” Follow-up
Interestingly, some participants preferred different tasks with different rater types (human and computer):
“Bizarrely, I found the word list easier from the human tester but the number sequences easier from the computer tester.” Follow-up
“It is interesting that my computer scores for [list learning] and Digit span are lower than in the human call, because this actually reflects how I felt when doing them. For some reason, the categories were much easier to do with the computer—maybe because I didn't feel so stupid about the words that came into my head.” Follow-up
3.6.4. Experience of receiving results from cognitive testing
Participants were interested in receiving their results from the study, regardless of whether they received them after each study appointment or only on study completion. In general, participants reported they did not feel worried about receiving their results and, in fact, tended to report feeling happy to receive them.
Interestingly, participants did not report concerns over the timing of receiving their results, with those who did not receive results after the first session reporting that this did not bother them at all and those who received feedback after each session reporting feeling indifference to this.
Participants were happy with either receiving feedback after each session or at the conclusion, which is helpful for considering the timing of feedback in future studies. It should be noted that any cases in which results fell significantly outside of normative values were discussed with the study's principal investigator, and when required, specific feedback was given regarding recommendations to contact a general practitioner (GP), and referral letters were requested. The full results are available in Table 6.
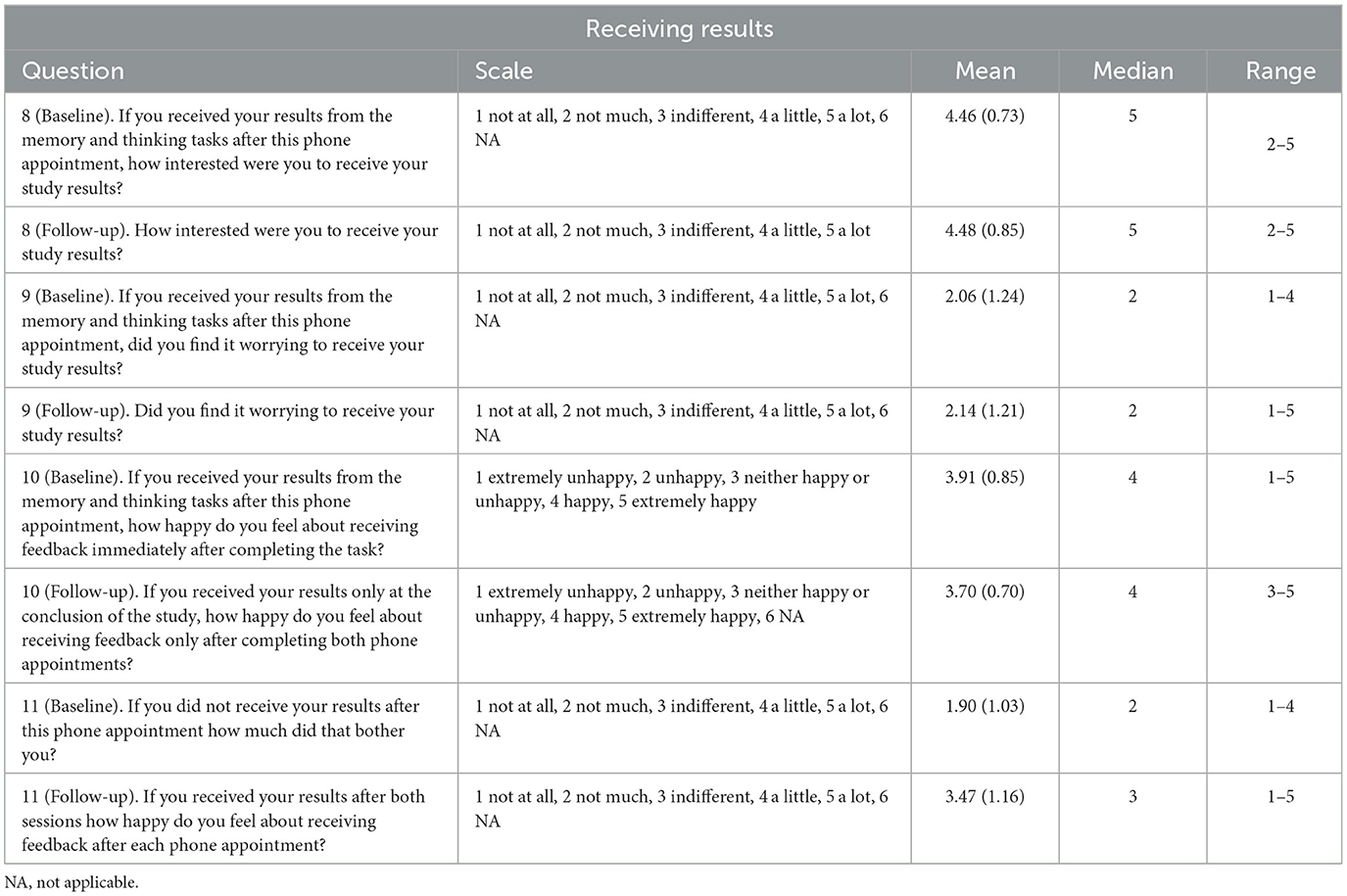
Table 6. Receiving results.
Generally, participants found that receiving results was interesting or reassuring:
“I think you know whether you have completed the tests well, or not, at the time. We all probably think we did worse than is actually true so receiving the results is actually positive as it shows they were not as bad as you thought.” Baseline
“I am interested in results but not much bothered and certainly not worried.” Baseline
“Getting results was interesting as this did not happen in the face-to-face surveys (at least, not for me).” Baseline
However, a few stated that some additional information on how to interpret the results would make these more helpful:
“Very interested to receive the results but would appreciate a bit more explanation—delayed recall—is it better to be higher or lower?” Follow-up
“I feel a little explanation in the results I received would help me understand them better, especially the first one; e.g. what do the numbers mean?” Baseline
Overall, participants found the process of engaging with a research project involving cognitive tests on the phone easy and comfortable. Although there was a clear preference for in-person, or with-person, testing, participants were happy to repeat on-the-phone testing in the future with either a human or an automatic phonebot. The feedback of results was seen as a positive aspect of the trial and did not appear to cause psychological distress.
4. Discussion
The results from this usability and acceptability analysis suggest that completing this brief battery of cognitive tests via a telephone call is both acceptable and feasible in a midlife-to-older adult population in the United Kingdom living at risk for AD. There were no obvious ceiling or floor effects for immediate recall, digit span, or fluency tasks. Some participants did perform at ceiling for the delayed recall task at both baseline and follow-up visits. There was a normal distribution of scores across the cognitive tasks at both visits, suggesting that these tasks perform as we would expect if administered in a face-to-face setting. Previous reviews have found that telephone-based cognitive testing is appropriate in the assessment of cognitive aging (Castanho et al., 2014). Participants enrolled in the study were free of dementia at enrolment. Comparing the scores to studies using the same subtests with in-person administration, we can see participants on average performed in the cognitively normal range (Harrison et al., 2000; Choi et al., 2014; Sirály et al., 2015). A recent review by our group found consistency between in-person and remote administration of cognitive tests for MCI and AD, although noted individual- and test-level variation (Hunter et al., 2021). As this group largely represented a cognitively healthy group, the findings are discussed in this context, with further work needed to understand feasibility and acceptability in populations with more cognitive impairment.
Three of the tasks (immediate recall, delayed recall, and semantic fluency) demonstrated no significant changes between baseline human testing and follow-up automatic phonebot testing, suggesting these are reliable to use in both administration modes. The RCI indicates individual-level changes in performance, which may reflect personal preferences of testing or cognitive fluctuations at the individual level. There were significant differences in performance on the digit span and phonemic fluency tasks between the baseline and follow-up visits. The digit span score significantly decreased between visits. As no other test scores decreased, it is unlikely that the cohort experienced significant cognitive decline in the interim 3-month period, and this decline in score may reflect some hearing, processing, or attentional difficulties when digits were read by the automated voice. This task may need further development before this can be used reliably in a fully automated manner. The increase in the phonemic fluency task may reflect a learning effect, although, interestingly, this was not seen in the semantic fluency task. This improvement in score is driven by women achieving a higher number of words at follow-up compared to baseline, with men's scores decreasing slightly at follow-up. These results reflect data from previous studies, suggesting a small majority of participants improve on a second attempt at fluency tasks (Harrison et al., 2000).
In general, women performed significantly better than men on a number of tasks at baseline and follow-up. This finding aligns with previous literature, where women appear to have an advantage in verbal memory compared to men despite carrying similar pathology burdens (Sundermann et al., 2017). Interestingly, while there is evidence in the literature for women outperforming men on phonemic fluency tasks (Hirnstein et al., 2022), we saw an effect for semantic but not phonemic fluency. It may be that the category of phonemic fluency was advantageous to both men and women to perform well (Hirnstein et al., 2022), leading to a lack of differentiation by gender, and it appears that women had a stronger learning effect compared to men on the semantic fluency task leading to a difference in scores at follow up. Age was significantly associated with most tasks, with education associated with task performance on a small number of tasks with a lack of consistency seen across visits. The importance of gender, age and education should be considered in further work to generate normative scores for these tasks when delivered via the telephone. Education has been reported as associated with performance on these cognitive tasks in previous studies (Zimmermann et al., 2014). Age and gender associations with cognitive test performance for these tasks are inconsistent in previous studies (Van der Elst et al., 2006; Zimmermann et al., 2014; Woods et al., 2016).
Participants found the experience of completing the tasks on the phone to be generally acceptable. The set-up of the appointment was easy for participants to engage with, and participants were comfortable with completing these tasks in their home environment. Although there was an expressed slight preference to complete tasks face-to-face, there was agreement that participants would be happy to repeat these tasks on the phone in the future with either a human or an automatic phonebot tester. Participants appreciated receiving the results of their cognitive tests, and there was no clear preference for receiving these after both visits or at the end of their study participation. While some information was provided on the results proforma, which was co-designed with participant advisors, on what scores might be expected for each task based on in-person testing normative scores, some participants did express a desire for more detailed information. This feedback can inform future studies, giving evidence to support the safe feedback of cognitive test results, with even more detailed proformas to establish the context of what the scores meant.
To the best of our knowledge, this is one of the first studies to evaluate participants' experiences of receiving cognitive test score results. Previous studies have evaluated the effects of disclosing APOE genotype and amyloid imaging results to cognitively healthy participants and found there was no increase in psychological distress, anxiety, or depression (Green et al., 2009; Grill et al., 2020). As acceptability of results disclosure was a secondary outcome, we did not gather any data on psychological distress or adjustment before and after results disclosure, and further work should explore this topic in more detail, as well as understand how to present this information to patients and participants in an understandable and meaningful way. However, participants self-reported the experience of receiving the results as overwhelmingly neutral or positive, along with no reports of psychological distress from any participants included in the study, suggesting there is likely little harm caused by disclosing test results from standardized tests used in a different format. As the phonemic fluency task was the only increase in mean scores at the follow-up visit, it is unlikely that result disclosure was associated with any change in test performance. There were a small number of problems that arose due to hearing difficulties. This should be noted as a consideration for wider implementation of phone-based speech and cognitive test data collection.
A key strength of this study was the initial co-design with participant panel members, whose input to the study design and materials was to ensure the project was of interest and comprehensible to the target population. The use of electronic data capture allowed participants to take part in a study during a period when in-person study engagement was limited due to the COVID-19 pandemic. The study has some limitations, with participation restricted to those who had previously engaged in cognitive testing. As such, there is a limit to the generalizability of testing-naïve participants. The participant population was also homogeneous, representing a highly educated cohort, which does not reflect the general population from which they were originally drawn. As this study recruited exclusively from those who had participated in the two earlier studies, there were no mitigations that were able to be put in place for this study; however, future studies should endeavor to explore the use of this technology in diverse populations. As previously mentioned, this should also be tested in a more cognitively impaired population to understand if this form of testing remains feasible and acceptable. It is also important to understand the usability of this tool regarding hearing impairment and the use of hearing aids. Further studies using this tool could include the use of brief hearing tests to establish the level of hearing impairment each participant has as well as record any diagnoses of hearing loss or hearing aid usage. This is important not only as a test that relies on hearing skills but also given the recognized importance of hearing loss as a risk factor for future dementia (Livingston et al., 2020). The testing order was fixed, and as such, we were not able to adjust for test order effects when interpreting changes in test scores.
To conclude, completing a short battery of cognitive tests on the telephone is both feasible and acceptable to an older adult population who are cognitively normal or at risk for future dementia. Future studies are needed to replicate this work in a more diverse participant population with a more pronounced cognitive decline. This study provides initial evidence on the value of feeding back cognitive test results to study participants, with further studies needed to explore more in-depth psychological safety of this approach.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Edinburgh Medical School Research Ethics Committee (EMREC). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SG: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Writing—original draft, Writing—review and editing. JHa: Conceptualization, Methodology, Supervision, Writing—review and editing. JHe: Formal analysis, Methodology, Project administration, Writing—review and editing. MH: Data curation, Formal analysis, Methodology, Project administration, Writing—review and editing. NJ: Data curation, Project administration, Writing—review and editing. AK: Conceptualization, Methodology, Writing—review and editing. NL: Conceptualization, Funding acquisition, Methodology, Writing—review and editing. SL: Conceptualization, Methodology, Writing—review and editing. EM: Project administration, Writing—review and editing. HP: Data curation, Methodology, Project administration, Writing—review and editing. MW: Data curation, Project administration, Writing—review and editing. SR: Writing—review and editing. JT: Data curation, Formal analysis, Writing—review and editing. CR: Conceptualization, Funding acquisition, Methodology, Supervision, Writing—review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Janssen Pharmaceutica NV through a collaboration agreement (Award/Grant number is not applicable). SG receives salary from a Medical Research Council grant [MRC UK Nutrition Research Partnership (NRP) Collaboration Award NuBrain (MR/T001852/1)].
Acknowledgments
We would like to thank the SPeAk study participants for taking part in this study. We would also like to thank the EPAD Scotland participant's panel for their initial review of the study.
Conflict of interest
SR is an employee of Janssen (the funder). JHe, NL, and AK are employees of ki:elements who own and provide the Mili platform. JHa reports receipt of personal fees in the past 2 years from Actinogen, AlzeCure, Aptinyx, Astra Zeneca, Athira Therapeutics, Axon Neuroscience, Axovant, Bial Biotech, Biogen Idec, Boehringer Ingelheim, Brands2life, Cerecin, Cognito, Cognition Therapeutics, Compass Pathways, Corlieve, Curasen, EIP Pharma, Eisai, GfHEU, Heptares, ki:elements, Lundbeck, Lysosome Therapeutics, MyCognition, Neurocentria, Neurocog, Neurodyn Inc, Neurotrack, the NHS, Novartis, Novo Nordisk, Nutricia, Probiodrug, Prothena, Recognify, Regeneron, reMYND, Roche, Rodin Therapeutics, Samumed, Sanofi, Signant, Syndesi Therapeutics, Treeway, Takeda, Vivoryon Therapeutics, and Winterlight Labs. Additionally, he holds stock options in Neurotrack Inc. and is a joint holder of patents with My Cognition Ltd. CR has received consultancy fees from Biogen, Eisai, MSD, Actinogen, Roche, and Eli Lilly, as well as payment or honoraria from Roche and Eisai.
The authors declare that this study received funding from Janssen Pharmaceutica NV (no grant number available). The funder had the following involvement in the study: study design, and preparation of the manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frdem.2023.1271156/full#supplementary-material
References
Ahmed, S., Haigh, A-M. F., de Jager, C. A., and Garrard, P. (2013). Connected speech as a marker of disease progression in autopsy-proven Alzheimer's disease. Brain 136, 3727–3737. doi: 10.1093/brain/awt269
Bean, J. (2011). “Rey auditory verbal learning test, rey AVLT,” in Encyclopedia of Clinical Neuropsychology, eds. J. S. Kreutzer, J. DeLuca, and B. Caplan (New York, NY, Springer New York), 2174–2175.
Blennow, K., Shaw, L. M., Stomrud, E., Mattson, N., Toledo, J., Buck, K., et al. (2019). Predicting clinical decline and conversion to Alzheimer's disease or dementia using novel Elecsys Aβ(1–42), pTau and tTau CSF immunoassays. Sci. Rep. 9, 19024. doi: 10.1038/s41598-019-54204-z
Blennow, K., and Zetterberg, H. (2018). Biomarkers for Alzheimer's disease: current status and prospects for the future. J. Int. Med. 284, 643–663. doi: 10.1111/joim.12816
Boschi, V., Catrikala, E., Consonni, M., Chesi, C., Moro, A., and Cappa, S. (2017). Connected speech in neurodegenerative language disorders: a review. Front. Psychol. 8, 269. doi: 10.3389/fpsyg.2017.00269
Burns, J. M., Johnson, D., Liebmann, E. P., Bothwell, R., Morris, J. K., and Vidoni, E. D. (2017). Safety of disclosing amyloid status in cognitively normal older adults. Alzheimer's Dement. 13, 1024–1030. doi: 10.1016/j.jalz.2017.01.022
Carlew, A. R., Fatima, H., Livingstone, J. R., Reese, C., Lacritz, L., Pendergrass, C., et al. (2020). Cognitive assessment via telephone: a scoping review of instruments. Arch. Clin. Neuropsychol. 35, 1215–1233. doi: 10.1093/arclin/acaa096
Caselli, R. J., Langbaum, J., Marchent, G., Licor, R., Hunt, K., Henslin, B. R., et al. (2014). Public perceptions of presymptomatic testing for Alzheimer disease. Mayo Clinic Proc. 89, 1389–1396. doi: 10.1016/j.mayocp.2014.05.016
Castanho, T. C., Amorim, L., Zihl, J., Palha, J. A., Sousa, N., and Santos, N. C. (2014). Telephone-based screening tools for mild cognitive impairment and dementia in aging studies: a review of validated instruments. Front. Aging Neurosci. 6, 16. doi: 10.3389/fnagi.2014.00016
Chételat, G., Arbizu, J., Barthel, H., Garibotto, V., Law, I., Morbelli, S., et al. (2020). Amyloid-PET and 18F-FDG-PET in the diagnostic investigation of Alzheimer's disease and other dementias. Lancet Neurol. 19, 951–962. doi: 10.1016/S1474-4422(20)30314-8
Choi, H. J., Lee, D. Y., Seo, E. H., Jo, M. K., Sohn, B. K., Choe, Y. M., et al. (2014). A normative study of the digit span in an educationally diverse elderly population. Psychiatry Investig. 11, 39–43. doi: 10.4306/pi.2014.11.1.39
Diaz-Asper, C., Chandler, C., Turner, R. S., Reynolds, B., and Elvevåg, B. (2021). Acceptability of collecting speech samples from the elderly via the telephone. Digital Health 7, 20552076211002103. doi: 10.1177/20552076211002103
Ford, E., Milne, R., and Curlew, K. (2023). Ethical issues when using digital biomarkers and artificial intelligence for the early detection of dementia. WIREs Data Mining Knowl. Disc. 13, e1492. doi: 10.1002/widm.1492
Garcia, S. F., Ritchie, C. W., and Luz, S. (2020). Artificial intelligence, speech, and language processing approaches to monitoring alzheimer's disease: a systematic review. J. Alzheimer's Dis. 78, 1547–1574. doi: 10.3233/JAD-200888
Geddes, M. R., O'Connell, M. E., Fisk, J. D., Gauthier, S., Camicioli, R., Ismail, Z., et al. (2020). Remote cognitive and behavioral assessment: report of the Alzheimer Society of Canada Task Force on dementia care best practices for COVID-19. Alzheimer's Dement. 12, e12111. doi: 10.1002/dad2.12111
Germine, L., Reinecke, K., and Chaytor, N. S. (2019). Digital neuropsychology: challenges and opportunities at the intersection of science and software. Clin. Neuropsychol. 33, 271–286. doi: 10.1080/13854046.2018.1535662
Gollan, T. H., Smirnov, D. S., Salmon, D. P., and Galasko, D. (2020). Failure to stop autocorrect errors in reading aloud increases in aging especially with a positive biomarker for Alzheimer's disease. Psychol. Aging 35, 1016–1025. doi: 10.1037/pag0000550
Green, R. C., Roberts, J. S., Cupples, J. A., Relkin, N. R., Whitehouse, P. J., Brown, T., et al. (2009). Disclosure of APOE genotype for risk of Alzheimer's disease. N. Engl. J. Med. 361, 245–254. doi: 10.1056/NEJMoa0809578
Gregory, S., Linz, N., König, A., Langel, K., Pullen, H., Luz, S., et al. (2022). Remote data collection speech analysis and prediction of the identification of Alzheimer's disease biomarkers in people at risk for Alzheimer's disease dementia: the Speech on the Phone Assessment (SPeAk) prospective observational study protocol. BMJ Open 12, e052250. doi: 10.1136/bmjopen-2021-052250
Grill, J. D., Raman, R., Ernstrom, K., Sultzer, D. L., Burns, J. M., Donohue, M. C., et al. (2020). Short-term psychological amyloid imaging results to research participants who do not have cognitive impairment. JAMA Neurol. 77, 1504–1513. doi: 10.1001/jamaneurol.2020.2734
Hampel, H., O'Bryant, S. E., Molinuevo, J. L., Zetterberg, H., Masters, C. L., Lista, S., et al. (2018). Blood-based biomarkers for Alzheimer disease: mapping the road to the clinic. Nat. Rev. Neurol. 14, 639–652. doi: 10.1038/s41582-018-0079-7
Harrison, J. E., Buxton, P., Husain, M., and Wise, R. (2000). Short test of semantic and phonological fluency: Normal performance, validity and test-retest reliability. Br. J. Clini. Psychol. 39, 181–191. doi: 10.1348/014466500163202
Hirnstein, M., Stuebs, J., Moè, A., and Hausmann, M. (2022). Sex/gender differences in verbal fluency and verbal-episodic memory: a meta-analysis. Persp. Psychol. Sci. 2022, 17456916221082116. doi: 10.1177/17456916221082116
Hunter, M. B., Jenkins, N., Dolan, C., Pullen, H., Ritchie, C., and Muniz-Terrara, G. (2021). Reliability of telephone and videoconference methods of cognitive assessment in older adults with and without dementia. J. Alzheimers. Dis. 81, 1625–1647. doi: 10.3233/JAD-210088
König, A., Linz, N., Tröger, J., Wolters, M., Alexandersson, J., and Robert, P. (2018). Fully automatic speech-based analysis of the semantic verbal fluency task. Dement. Geriatr. Cogn. Disord. 45, 198–209. doi: 10.1159/000487852
Konig, A., Satt, A., Sorin, A., Hooray, R., Derreumax, A., Davis, R., et al. (2018). Use of speech analyses within a mobile application for the assessment of cognitive impairment in elderly people. Curr. Alzheimer Res. 15, 120–129. doi: 10.2174/1567205014666170829111942
Largent, E. A., Harkins, K., van Dyck, C., Hachey, S., Sankar, P., and Karlawish, J. (2020). Cognitively unimpaired adults' reactions to disclosure of amyloid PET scan results. PLoS ONE 15, e0229137. doi: 10.1371/journal.pone.0229137
Lim, Y. Y., Maruff, P., Getter, C., and Snyder, P. J. (2016). Disclosure of positron emission tomography amyloid imaging results: a preliminary study of safety and tolerability. Alzheimer's Dement. 12, 454–458. doi: 10.1016/j.jalz.2015.09.005
Livingston, G., Huntley, J., Sommerlad, A., Ames, D., Ballard, C., Banerjee, S., et al. (2020). Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396, 413–446. doi: 10.1016/S0140-6736(20)30367-6
Livingston, G., Huntley, J., Sommerland, A., Ames, D., Ballard, C., Banerjee, S., et al. (2017). Dementia prevention, intervention, and care. Lancet 390, 2673–2734. doi: 10.1016/S0140-6736(17)31363-6
Mueller, K. D., Van Hulle, C. A., Koscik, R. L., Jonaitis, E., Peters, C. C., Betthauser, T. J., et al. (2021). Amyloid beta associations with connected speech in cognitively unimpaired adults. Alzheimers Dement (Amst) 13, e12203. doi: 10.1002/dad2.12203
Nichols, E., Szoeke, C E., Vollset, S E., Abbasi, N., Abd-Allah, F., et al. (2019). Global, regional, and national burden of Alzheimer's disease and other dementias, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18, 88–106. doi: 10.1016/S1474-4422(18)30403-4
Ott, B. R., Pelosi, M. A., Tremont, G., and Snyder, P. J. (2016). A survey of knowledge and views concerning genetic and amyloid positron emission tomography status disclosure. Alzheimer's Dement. 2, 23–29. doi: 10.1016/j.trci.2015.12.001
Peskind, E. R., Rieske, R., Quinn, J. F., Kaye, J., Clark, C., Farlow, M. R., et al. (2005). Safety and acceptability of the research lumbar puncture. Alzheimer Dis. Assoc. Disord. 19, 220–225. doi: 10.1097/01.wad.0000194014.43575.fd
Ritchie, C. W., Moliuevo, J., Truyen, L., Satlin, A., Greyten, S., Loveston, S., et al. (2016). Development of interventions for the secondary prevention of Alzheimer's dementia: the European Prevention of Alzheimer's Dementia (EPAD) project. Lancet Psychiat. 3, 179–186. doi: 10.1016/S2215-0366(15)00454-X
Ritchie, C. W., Muniz-Terrera, G., Kivipelto, M., Solomon, A., Tom, B., and Molinuevo, J. L. (2020). The European prevention of Alzheimer's dementia (EPAD) longitudinal cohort study: baseline data release V500.0. J. Prevent. Alzheimer's Dis. 7, 8–13. doi: 10.14283/jpad.2019.46
Simon, D. A., Evans, B. J., Shachar, C., and Cohen, I. G. (2022). Should Alexa diagnose Alzheimer's?: Legal and ethical issues with at-home consumer devices. Cell Reports Med. 3, 100692. doi: 10.1016/j.xcrm.2022.100692
Sirály, E., Szabó, Á., Szita, B., Kovács, V., Fodor, Z., Marosi, C., et al. (2015). Monitoring the early signs of cognitive decline in elderly by computer games: an MRI study. PLoS ONE 10, e0117918. doi: 10.1371/journal.pone.0117918
Sundermann, E. E., Biegon, A., Rubin, L. H., Lipton, R. B., Landau, S., Maki, P. M., et al. (2017). Does the female advantage in verbal memory contribute to underestimating Alzheimer's disease pathology in women versus men? J. Alzheimers Dis. 56, 947–957. doi: 10.3233/JAD-160716
Takaeda, K., Kamimura, T., Inoue, T., and Nishiura, Y. (2019). Reliability and acceptability of using a social robot to carry out cognitive tests for community-dwelling older adults. Geriatr. Gerontol. Int. 19, 552–556. doi: 10.1111/ggi.13655
Taswell, C., Donohue, C., Mastwyk, M., Villemagne, V., Masters, C., Rowse, C., et al. (2017). Safety of disclosing amyloid imaging results to MCI and AD patients. Am. J. Geriatric Psychiat. 25, S129. doi: 10.1016/j.jagp.2017.01.147
Taylor, J. C., Heuer, H. W., Clark, A. L., Wise, A. B., Manoochehri, M., Forsberg, L., et al. (2023). Feasibility and acceptability of remote smartphone cognitive testing in frontotemporal dementia research. Alzheimer's Dement. 15, e12423. doi: 10.1002/dad2.12423
Themistocleous, C., Eckerström, M., and Kokkinakis, D. (2020). Voice quality and speech fluency distinguish individuals with Mild Cognitive Impairment from Healthy Controls. PLoS ONE 15, e0236009. doi: 10.1371/journal.pone.0236009
Tröger, J., Baykara, E., Zhao, J., Huurne, D. T., Possemis, N., Mallick, E., et al. (2022). Validation of the remote automated ki:e speech biomarker for cognition in mild cognitive impairment: verification and validation following DiME V3 framework. Digital Biomark. 6, 107–116. doi: 10.1159/000526471
Tröger, J., Linz, N., Konig, A., Roberst, P., and Alexandersson, J. (2018). “Telephone-based dementia screening i: automated semantic verbal fluency assessment,” in Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare (New York, NY, USA: Association for Computing Machinery), 59–66.
Tröger, J., Linz, N., Konig, A., Roberst, P., Alexandersson, J., Peter, J., et al. (2019). Exploitation vs. exploration-computational temporal and semantic analysis explains semantic verbal fluency impairment in Alzheimer's disease. Neuropsychologia 131, 53–61. doi: 10.1016/j.neuropsychologia.2019.05.007
Udeh-Momoh, C. T., Watermeyer, T., Price, G., Loots, C. A., Reglinska-Matveyev, N., Ropacki, M., et al. (2021). Protocol of the cognitive health in ageing register: investigational, observational and trial studies in dementia research (CHARIOT): prospective readiness cohort (PRO) substudy. BMJ Open 11, e043114. doi: 10.1136/bmjopen-2020-043114
Unterman, T. G., Jentel, J. J., Oehler, D. T., Lacson, R. G., and Hofert, J. F. (1993). Effects of glucocorticoids on circulating levels and hepatic expression of insulin-like growth-factor (IGF)-binding proteins and igf-i in the adrenalectomized streptozotocin-diabetic rat. Endocrinology 133, 2531–2539. doi: 10.1210/endo.133.6.7694841
Van der Elst, W., Van Boxtel, M. P. J., Van Breukelen, G. J. P., and Jolles, J. (2006). Normative data for the animal, profession and letter M naming verbal fluency tests for dutch speaking participants and the effects of age, education, and sex. J. Int. Neuropsychol. Soc. 12, 80–89. doi: 10.1017/S1355617706060115
Vanderschaeghe, G., Schaeverbeke, J., Bruffaerts, R., Vandenberghe, R., and Dierickx, K. (2017). Amnestic MCI patients' experiences after disclosure of their amyloid PET result in a research context. Alzheimer's Res. Ther. 9, 92. doi: 10.1186/s13195-017-0321-3
Venneri, A., Jahn-Carta, C., de Marco, M., Quaranta, D., and Marra, C. (2018). Diagnostic and prognostic role of semantic processing in preclinical Alzheimer's disease. Biomark. Med. 12, 637–651. doi: 10.2217/bmm-2017-0324
Wake, T., Tabuchi, H., Funaki, K., Ito, D., Yamagata, B., Yoshizaki, T., et al. (2017). The psychological impact of disclosing amyloid status to Japanese elderly: a preliminary study on asymptomatic patients with subjective cognitive decline. Int. Psychogeriatr. 30, 635–639. doi: 10.1017/S1041610217002204
Wittenberg, R., Knapp, M., Karagiannidou, M., Dickson, J., and Schott, J. (2019). Economic impacts of introducing diagnostics for mild cognitive impairment Alzheimer's disease patients. Alzheimer's Dement. 5, 382–387. doi: 10.1016/j.trci.2019.06.001
Woods, D. L., Wyma, J. M., Herron, T. J., and Yund, E. W. (2016). Computerized analysis of verbal fluency: normative data and the effects of repeated testing, simulated malingering, and traumatic brain injury. PLoS ONE 11, e0166439. doi: 10.1371/journal.pone.0166439
Keywords: speech, biomarkers, Alzheimer's disease, cognition, acceptability, feasibility
Citation: Gregory S, Harrison J, Herrmann J, Hunter M, Jenkins N, König A, Linz N, Luz S, Mallick E, Pullen H, Welstead M, Ruhmel S, Tröger J and Ritchie CW (2023) Remote data collection speech analysis in people at risk for Alzheimer's disease dementia: usability and acceptability results. Front. Dement. 2:1271156. doi: 10.3389/frdem.2023.1271156
Received: 01 August 2023; Accepted: 19 September 2023;
Published: 13 October 2023.
Edited by:
Roozbeh Sadeghian, Harrisburg University of Science and Technology, United StatesReviewed by:
Celeste Annemarie De Jager Loots, Imperial College London, United KingdomAda Wai Tung Fung, Hong Kong Baptist University, Hong Kong SAR, China
Copyright © 2023 Gregory, Harrison, Herrmann, Hunter, Jenkins, König, Linz, Luz, Mallick, Pullen, Welstead, Ruhmel, Tröger and Ritchie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah Gregory, U2FyYWguR3JlZ29yeUBlZC5hYy51aw==