 Janet H. Van Cleave1*
Janet H. Van Cleave1* Alizendie Guerra2Eva Liang3Carolina Gutiérrez4Ron J. Karni5
Alizendie Guerra2Eva Liang3Carolina Gutiérrez4Ron J. Karni5 Marcely Tsikis1Geanise Pearl C. Nguyen5
Marcely Tsikis1Geanise Pearl C. Nguyen5 Allison P. Squires2
Allison P. Squires2
- 1Department of Nursing Research, UTHealth Houston Cizik School of Nursing, Houston, TX, United States
- 2NYU Meyers College of Nursing, New York, NY, United States
- 3Office of Research and Innovation, Stony Brook School of Nursing, Stony Brook, NY, United States
- 4Department of Physical Medicine and Rehabilitation, UTHealth Houston, McGovern Medical School, Houston, TX, United States
- 5Department of Otorhinolaryngology–Head & Neck Surgery, UTHealth Houston, McGovern Medical School, Houston, TX, United States
Introduction: Translations of patient-reported measures may not account for structural and cultural differences in shared languages spoken in multiple countries, such as English, Spanish, Arabic, or Russian. The objective of this research was to create a cross-cultural Spanish translation of the New York University (NYU) Electronic Patient Visit Assessment (ePVA)© for head and neck cancer (HNC), a patient-reported symptom measure available only in English.
Methods: Using the Content Validity Index (CVI) methodology, an expert panel of nurses (n = 6) proficient in Spanish and English independently reviewed and rated a forward translation of the ePVA, a measure consisting of 21 categories of symptoms common to HNC. The panel rated the cultural relevance (1 = not relevant, 2 = somewhat relevant, 3 = very relevant, 4 = highly relevant) and translation equivalence (1 = yes or 0 = no) of each ePVA item. The CVI cultural relevance and translation equivalence scores for each item (item CVI) were calculated as the proportion of experts agreeing that the item was very relevant or highly relevant and the translation was equivalent. The scale CVI score was an average of the item CVI scores; the minimum accepted scale CVI score was .80. Items with CVI scores <0.59 were labeled as problematic items and evaluated through cognitive interviews with native Spanish-speaking patients (N = 4) diagnosed with HNC.
Results: The translation was acceptable in cultural relevance (average CVI score = 0.95) and equivalence (average CVI score = 0.84). Cognitive interviews revealed 9 problematic items that differed in words and meaning, primarily addressing pain and swallowing symptoms. These items were refined and included in the final translation of the Spanish ePVA.
Conclusion: These study findings underscore the need for survey instrument translations that account for variations in shared languages spoken across countries.
1 Introduction
More than 25 million residents of the United States (US) have limited English proficiency (LEP) (1, 2), defined as individuals who do not speak English as their primary language and have a limited ability to read, write, or understand the English language (1, 3). These communication barriers for those with LEP have healthcare consequences. Those with LEP often experience longer hospital stays and unplanned emergency room revisits within 72 h after hospital discharge because of difficulty understanding hospital discharge instructions and obtaining prescriptions (1, 4). In cancer care, patients with LEP may face additional barriers to care. Research has demonstrated that those with LEP and diagnosed with cancer have lower rates of clinical trial engagement and patient portal messaging than English-speaking patients (5). Use of patient-reported symptom monitoring (PROM) may overcome communication barriers for patients with LEP. PROMs in routine cancer care are associated with increased symptom control and decreased emergency room and urgent care visits (6–11).
PROMs can be an important tool of management for patients with head and neck cancer (HNC) because of the high symptom burden experienced by the HNC population. HNC is the 6th most common cancer worldwide (12). Over 72,000 individuals in the US and 947,000 worldwide are diagnosed with HNC annually (13, 14). HNC comprises tumors that arise from the lip, oral cavity, pharynx, larynx, and paranasal sinuses. The most common risk factors for HNC are tobacco and alcohol use disorders. Other risk factors are exposure to human papillomavirus (HPV), Epstein–Barr Virus, and Betel nut chewing, which is common in Asian countries (15–19). HNC is more likely to occur in men than women (Men: 72.4%; Women: 27.6%) (13).
In the US, most patients are treated aggressively with multimodal therapies (surgery, chemotherapy, radiation therapy, and immunotherapy). This aggressive treatment has contributed to an increased 5-year survival rate from 60%–68% over the past 20 years (20), expanding the number of survivors with HNC to 540,150 in 2025 (21). The increased survival in HNC comes with a human cost; up to 60% of survivors with HNC experience substantial symptom burden (e.g., severe difficulty swallowing, chronic pain) and functional morbidity (e.g., limitations in movement and inability to work) (22–24).
Quality care for patients with HNC includes close systematic monitoring of patients' symptoms and functional morbidity, enabling clinicians to make early, real-time interventions that optimize patient outcomes (25–28). Thus, our team explored implementing a PROM in HNC clinical care. The initial step in this project was to conduct a systematic literature review of symptom and function measures to identify valid and reliable PROMs that patients can answer in approximately 10 min while waiting for their oncology visits. This literature review showed that the existing valid and reliable instruments have properties that limit their use in routine clinical practice. Many instruments were lengthy, complicated, and intended for general cancer populations, which posed an unneeded respondent burden for patients with HNC. Some instruments contained a priori assumptions on associations between specific symptoms and functional morbidity (e.g., “I cannot eat because of pain”), potentially introducing unintentional bias into data. Moreover, the existing instruments did not fully capture the long-term symptom experience and functional morbidity after treatment completion experienced by the growing number of patients living longer with HNC. Hence, we developed a patient-centered PROM, New York University (NYU) Electronic Patient Visit Assessment (ePVA)©, using rigorous measurement theory including content validity analysis. Subsequent testing of the ePVA has provided evidence of its reliability and convergent validity with health-related quality of life (HRQoL), patient and provider acceptance, and an association with clinically significant differences in patients' symptoms and acute care use (29–31).
Like many measures used as PROMs, the ePVA was developed in English, which impedes its use among patients with LEP (32). The team decided to translate the ePVA from English to Spanish to improve communication with the Hispanic immigrants with LEP. A challenge with the translation process was that the Hispanic population in the US constitutes a diverse population with origins in multiple states and countries, including Puerto Rico, Central America, and South America (33). To overcome this challenge, the team used the Content Validity Index (CVI) methodology, a comprehensive and systematic approach to translation that accounts for cross-cultural differences in shared languages.
The CVI methodology is an approach derived from measurement theory and is useful for determining consensus among experts (34–36). Squires et al. (37) expanded the CVI methodology for use in cross-cultural translations of measures to overcome limitations in existing guidelines that focused on technical aspects of cross-cultural translation, had limited content expert feedback, and did not use a systematic method of identifying problematic items requiring further refinement (37). The expansion of the CVI methodology incorporated a systematic process of independent analysis that includes content expert input of qualitative data to assess the back translation, analysis of cultural relevance and translation equivalence, and identification of problematic survey items that require further refinement (37). The CVI methodology has been used to develop and validate a survey for RN4CAST, a comparative nursing workforce study conducted in 12 European countries using 11 languages with modifications for regional dialects (37), and multiple workforce assessment studies (37–44).
The objective of this article is to describe our experience using the CVI methodology in translating the ePVA from English to Spanish (i.e., the Spanish ePVA). This article will present the CVI methodology used to create the Spanish ePVA, analyze the quality of the Spanish ePVA translation, and discuss the benefits and limitations of the CVI methodology in translating PROMs. The study's specific aims are to (1) Produce a Spanish ePVA with acceptable cultural relevance and translation equivalence using CVI methodology and (2) Evaluate and refine problematic items of the Spanish ePVA using cognitive interviews.
2 Methods
2.1 Study design
The translation of the ePVA from English to Spanish was accomplished using a comprehensive and systematic approach guided by the CVI methodology. This approach encompasses recommended good practices in the translation of PROMs by using experts to evaluate the forward and back translations, using ratings to identify problematic items, and conducting interviews with the targeted population to refine the translated PROMs (35, 45). Further, this method evaluates the cultural relevance and translation equivalence of the individual Spanish ePVA items and average scale CVI.
2.2 NYU electronic patient visit assessment (ePVA)© for HNC
The ePVA's development, reliability, and clinical usefulness in symptom monitoring for patients with HNC have been described elsewhere (29, 30, 46). The ePVA is a PROM consisting of 21 categories of symptoms common to HNC (i.e., pain, eye, ear, nasal, mouth, voice, fibrosis, edema, skin, gastrointestinal, fatigue, movement limitation, sleep, breathing, difficulty eating or drinking, swallowing, communication, social activities, anxiety, depression, and daily activities). The ePVA's design was based on the Theory of Unpleasant Symptoms (47), a middle-range theory that conceptually maps the link between symptoms and outcomes such as HRQoL (29, 30). The measure consists of binomial questions (yes = 1/no = 0) to indicate the presence or absence of the symptom. Some questions are conditional, with branching logic to tailor the assessment to the patient's health status and limit the respondent burden. For example, one question asks if the patient has experienced pain in the past 7 days. If the patient answers “yes,” the ePVA directs the patient to complete a multidimensional pain assessment. If the patient responds “no,” the ePVA leads the patient to answer questions about a different symptom. Prior research has shown that the ePVA measure has acceptable reliability using the Kuder-Richardson Formula 20 measure for questionnaires with binary variables (alpha = .82 -.85) and convergent validity with HRQoL (29, 30, 46, 48).
2.3 Translation procedures
The translation process of the Spanish ePVA consisted of forward translation, expert panel independent review and rating of the forward and back translation, and cognitive interviews with native Spanish-speaking patients (n = 4) with HNC to evaluate problematic items (See Figure 1).
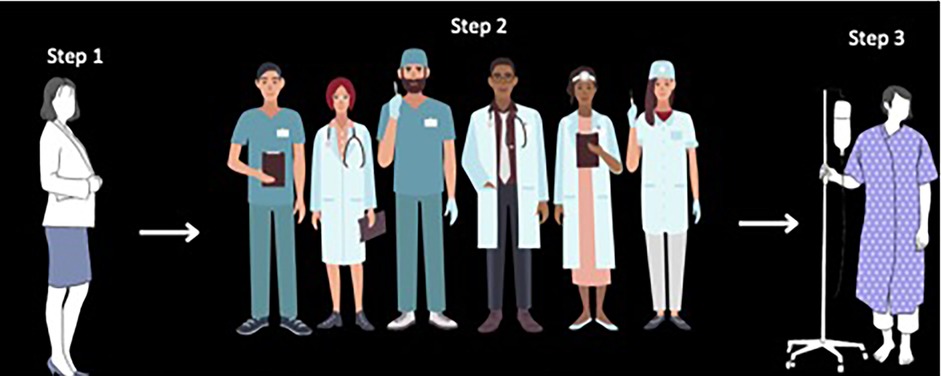
Figure 1. Translation process of the Spanish NYU electronic patient visit assessment (ePVA) for head and neck cancer. The content validity index (CVI) methodology consisted of a three-step process. Step 1—Forward Translation: The senior author (AS), fluent in Spanish and English with expertise in language discordance and its effect on healthcare outcomes and use of CVI for cross-cultural translations of surveys, completed a forward translation of the ePVA. Step 2—Independent Review and Rating of Forward Translation: An expert panel (N = 6) fluent in Spanish and English and qualified as a nurse to understand and interpret medical terminology independently reviewed and rated a forward translation of the ePVA. The panel rated relevance (1 = not relevant, 2 = somewhat relevant, 3 = very relevant, 4 = highly relevant) and translation equivalence (1 = Yes or 0 = No) of each ePVA item. The panel members also recorded their recommendations when they disagreed with the relevance or translation equivalence of the forward translation of the Spanish ePVA, thus providing qualitative data on the back translation of the Spanish ePVA. The item-CVI relevance and translation equivalence scores were calculated as the proportion of experts agreeing that the item was “very” or “highly” relevant and the translation was equivalent. Items with CVI scores of <0.59 were labeled as potentially problematic items. Step 3: The team conducted cognitive interviews with native Spanish-speaking patients (N = 4) with head and neck cancer to evaluate potentially problematic items.
2.3.1 Forward translation
The senior author (AS), fluent in English and Spanish with expertise in language discordance and its effect on healthcare outcomes and the use of CVI for cross-cultural translations of surveys, conducted the forward translation of each ePVA question stem and response option to Spanish, totaling 368 items. The study team entered the English ePVA and the corresponding forward translation in Spanish as a survey in the Research Electronic Data Capture (REDCap) database, a secure web-based software platform designed to support data capture for research studies (49, 50).
2.3.2 Expert panel independent review and rating of the forward and back translation of the ePVA
The research team recruited content experts from across the US to independently review and rate the forward and back translation of the ePVA by issuing a call across the US through a national nursing organization. The requirements to serve on the expert panel were fluency in English and Spanish and qualified as a nurse to understand and interpret medical terminology. Six persons responded to the call; the regions that influenced the panel members' Spanish proficiency were Mexico (n = 2), South America (n = 2), or not reported (n = 2). The panel independently compared the English and Spanish versions of the ePVA for the cultural relevance and translation equivalence of each item by rating cultural relevance using a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant, 3 = very relevant, 4 = highly relevant) and translation equivalence (1 = yes, 0 = no). Panel members also entered qualitative data in text fields to record their recommendations when they disagreed with the cultural relevance or translation equivalence of the forward translation of the Spanish ePVA.
2.3.2.1 Analysis of the quality of the Spanish ePVA translation
The analysis of the quality of the Spanish ePVA translation was conducted using CVI values at the item and scale levels. A CVI value was computed for each item's cultural relevance and translation equivalence (i.e., item-level CVI or I-CVI). The I-CVI for cultural relevance was computed as the proportion of the expert panel in agreement that the item was very relevant or highly relevant (36, 37). The proportion's numerator was the number of experts rating the item as either “3” or “4,” and the denominator was the number of experts completing the assessment. The I-CVI for translation equivalence was computed as the proportion of experts rating the item as having translation equivalence. The proportion's numerator was the number of experts rating the item as “1,” and the denominator was the number of experts completing the assessment. The measure's scale-level CVI (i.e., S-CVI) was calculated as the average of all I-CVIs (i.e., S-CVI/Ave). The minimally acceptable value of translation quality was S-CVI/Ave = 0.80 (51), and the goal was S-CVI/Ave ≥ 0.90 (36).
2.3.2.2 Using modified kappa scores to identify problematic items
Each item's modified kappa score (mKappa) was calculated to adjust the I-CVI score for chance agreement among panel members. This calculation incorporates the probability of chance agreement (Pc), using the equation Pc = [N!/A! (N–A)!] × 0.5 N, where N is the number of experts and A is the number of experts who agree the item was relevant (scores 3 and 4) (35, 36). The probability of chance agreement or disagreement (i.e., mKappa) was calculated as mKappa = [I-CVI-Pc]/[1-Pc] (36). The items with mKappa scores <0.59 were categorized as problematic items, requiring further review using cognitive interviews (36).
2.3.3 Cognitive interviews
The study team conducted cognitive interviews with patients who were native Spanish-speaking patients diagnosed with HNC regarding the problematic items. The methodology described by Knafl et al. (52) guided the construction of the semi-structured interview guide, procedures, and analysis to explore patients' understanding and interpretation of the problematic items (See Supplementary A) (52). The patient eligibility criteria for the cognitive interviews were individuals 18 years and older with histologically diagnosed HNC, fluent in Spanish, and could provide informed consent. The study team recruited all race, ethnicity, and genders before, during, or after HNC treatment (i.e., surgery, chemotherapy, radiation therapy, or a combination of these modalities).
Ultimately, four native Spanish-speaking partients were enrolled in the study. The participants' demographic data were obtained from both participants and the participants' electronic health records (See Figure 2). After the participant provided informed consent, a study team member fluent in Spanish and English read each question to the participants and recorded the participants' responses on a Microsoft Excel spreadsheet. After eliciting similar answers from three consecutive participants, the team stopped conducting cognitive interviews.
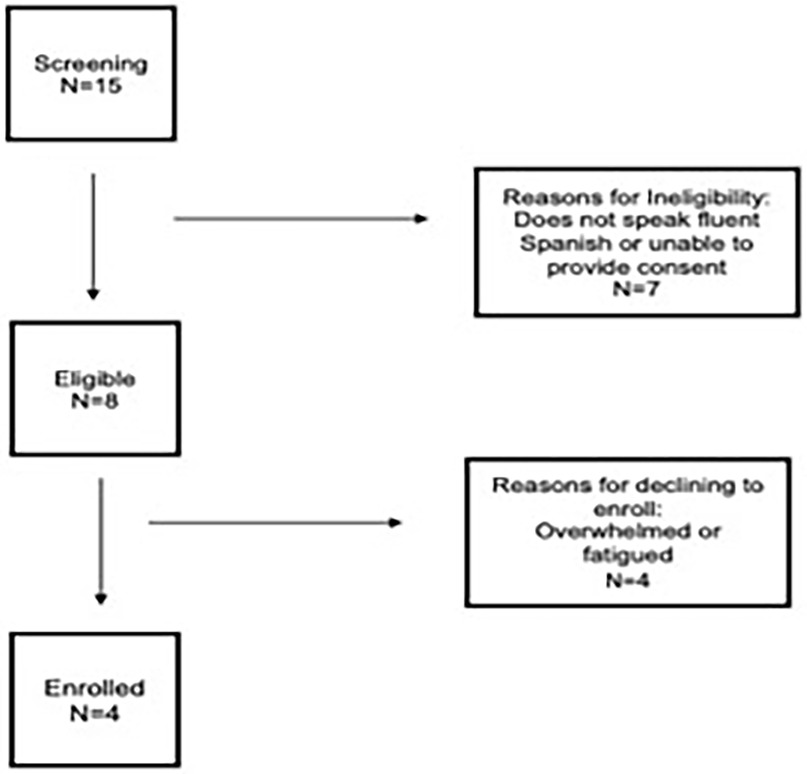
Figure 2. Participant recruitment and enrollment for cognitive interviews.
2.3.3.1 Cognitive interviews analysis
After completing the cognitive interviews, team members analyzed a summary table of the cognitive interviews (52). This analysis systematically compared items' mKappa scores, the expert panels' qualitative data on the Spanish ePVA's back translation, and participants' responses to the cognitive interviews to identify the problematic aspects of the items. The team discussed all items until they achieved consensus on retaining, deleting, or modifying the items for the final translation of the Spanish ePVA. Memos of discussions and decisions ensured the trustworthiness of the analysis. The final version of the Spanish ePVA underwent beta testing by nurses and patients with HNC whose Hispanic heritage included Puerto Rico, Central America, and South America.
3 Results
3.1 Aim 1: produce a Spanish ePVA with acceptable cultural relevance and translation equivalence using CVI methodology
The quality of the Spanish translation of the ePVA was evaluated using S-CVI/Ave scores of cultural relevance and translation equivalence. The analysis found the S-CVI/Ave score for cultural relevance was 0.95, meeting the team's goal criteria of S-CVI/Ave of ≥0.90. A review of individual items' mKappa scores for cultural relevance found only two items with a rating of <0.59, indicating these items as problematic. A further review of the items revealed grammatical errors in the forward translation. The team corrected the errors and included the refined items in the Spanish ePVA.
The S-CVI/Ave for translation equivalence was 0.84, meeting the minimally acceptable value of S-CVI/Ave = .80. A review of individual items' mKappa scores for translation equivalence revealed 55 items with a rating of <0.59, indicating these items as problematic. A further review of these items revealed that 31 of the 55 problematic items had typographical or grammatical errors in the forward translation. The team corrected these errors and included these items in the Spanish ePVA. The remaining 24 problematic items were further analyzed using cognitive interviews.
3.2 Aim 2: evaluate and refine problematic items of the Spanish ePVA using cognitive interviews
The team conducted cognitive interviews with patients with HNC (n = 4) whose native language was Spanish to evaluate the remaining 24 problematic items. The participants were men with a median age of 61.5 (range 56–70) (See Table 1). The origin country influencing their Spanish language was Puerto Rico (n = 2) or not reported (n = 2). All participants were undergoing chemotherapy with or without radiation therapy. After informed consent, the participants answered questions followed by probes (See Supplementary A – Cognitive Interview Probes). The analysis of the cognitive interviews revealed two key problems with the 24 items—(1) different words or grammatical structures representing similar concepts or meanings, and (2) different words or grammatical structures representing different concepts or meanings across cultures.
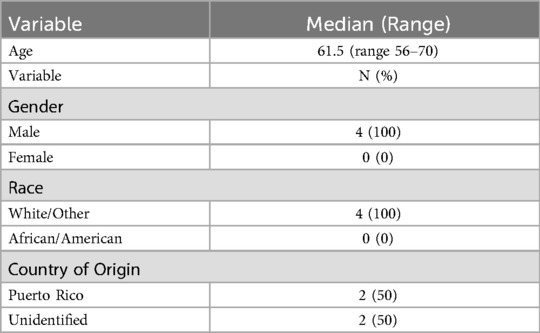
Table 1. Demographic characteristics of patient participants for cognitive interviews (n = 4).
3.2.1 Different words or grammatical structures representing similar concepts or meanings
The analysis found that 15 of the 24 problematic items differed in words or grammatical structure but represented similar concepts or meanings to participants (See Table 2). These items included instructions for answering the ePVA questionnaire and the following symptoms: pain, skin, eye, mouth, gastrointestinal, voice, movement, breathing, social function, and swallowing. For example, the term itchy skin had alternate translations of “picazones,” “picazón,” or “picazon la piel,” yet the participants considered the different translations as equivalent. The team discussed and refined all items to account for cross-cultural variations and included the items in the final translation of the Spanish ePVA.
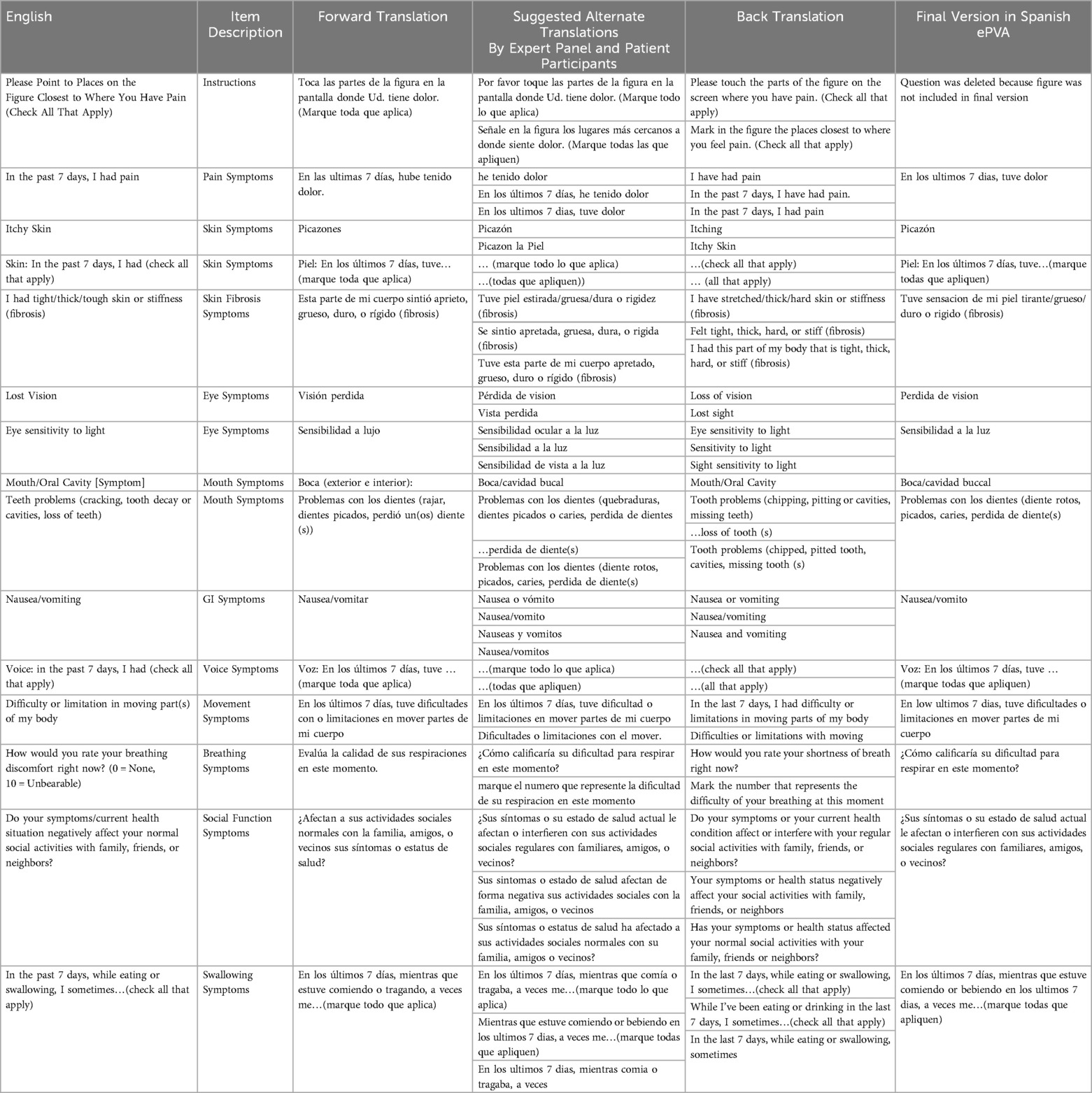
Table 2. Spanish ePVA items with different words or grammatical structures representing similar concepts or meanings.
3.2.2 Different words or grammatical structures representing different concepts or meanings
The cognitive interviews regarding the remaining 9 problematic items revealed that these items differed in words or grammatical structure and represented different concepts or meanings to the participants (See Table 3). The items primarily involved pain (3 of 9) and swallowing (3 of 9). Other symptoms were ear, movement, and breathing. For example, the term “stabbing” as a descriptor of pain had alternate translations of “puñalada,” “dolor punzante”, and “punzante.” The participants interpreted the items as “pain from a stabbing,” “stabbing pain,” and “throbbing pain.” From the cognitive interviews, it was unclear that a cross-cultural translation equivalent existed for the swallowing term “gagging.” Ultimately, the team decided to replace the term “gagging” with a field for patients to enter free text to describe their swallowing problems. The team discussed and refined all other items to account for cross-cultural variations and included the items in the final translation of the Spanish ePVA.
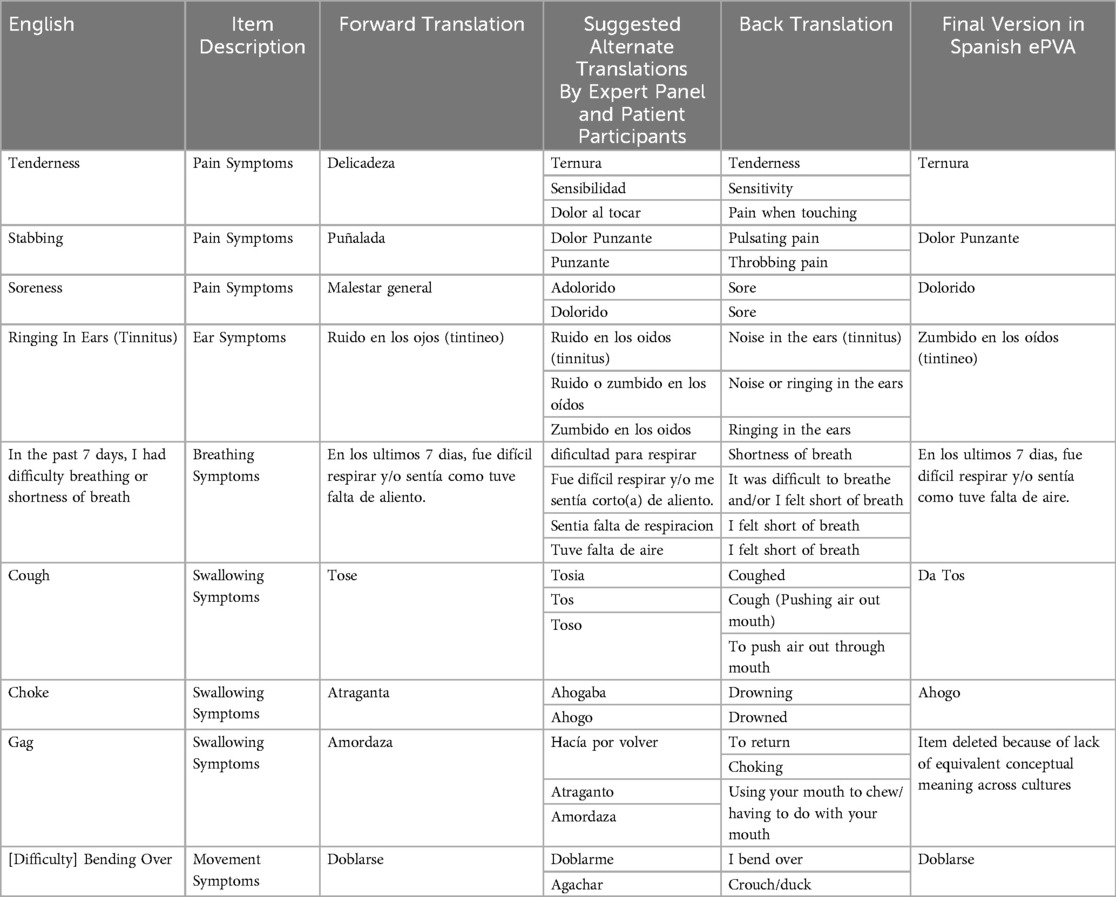
Table 3. Spanish ePVA items With different words or grammatical structures representing different concepts or meanings.
4 Discussion
Nearly 46.2 million immigrants lived in the US in 2022, the highest number in the nation's history (53). Translating healthcare materials is critical to providing quality healthcare for those with LEP; however, translations may not account for structural and cultural differences in shared languages across countries, such as English, Spanish, Arabic, or Russian. This manuscript reports the use of CVI methodology, a comprehensive and systematic translation approach, to produce the Spanish ePVA PROM with acceptable cultural relevance and translation equivalence.
Traditionally, translating an English measure into another language consists of two independent translators agreeing on a standard version, which is then retranslated back into English (back translation) by two other translators in agreement on one version. These agreed-upon back translations may be evaluated by bilingual experts for their conceptual equivalence, use of everyday language, and clarity (54). Finally, the English back translation is compared with the original by one of the persons who developed the instrument.
However, these traditional methods may not capture the cultural variations within shared languages. Immigrant populations may speak common languages across countries, but the cultures and traditions of their ancestral country influence the grammatical structure and conceptual meanings. Methodologies that produce quality translations include processes that result in a questionnaire with acceptable cultural relevance and translation equivalence for use in multicultural populations with LEP (55).
4.1 The benefits and limitations of the CVI methodology
The CVI methodology incorporates the aforementioned steps and includes quantitative ratings of the cultural relevance and translation equivalence and qualitative comments by experts evaluating the translation. This approach identifies problematic items and informs additional research to refine the final translation, such as cognitive interviews. Accordingly, the benefit of the CVI methodology over traditional methods is that it reduces inherent bias by identifying problematic items that affect the translation's quality. The CVI methodology may require more resources than traditional methods, such as independent translators for the cognitive interviewing component. As artificial intelligence advances, machine translations of written documents may increase to preserve resources. The quality of machine translations has improved dramatically; nevertheless, these translations may require a native speaker to check to ensure their cultural relevance and translation equivalence (56). Researchers using machine translations will need to plan for these resources accordingly as part of the translation process.
4.2 Public health implications
This research has public health implications for patients with LEP. Notably, the 9 problematic items that differed in grammatical structure and conceptual meaning across Spanish-speaking cultures represented the critical symptoms of HNC: pain, swallowing, and breathing. A possible rationale for this finding is that symptoms represent an individual's perception of the biological activity of cancer and its treatment (57, 58), and are affected by psychosocial factors, including anxiety, depression, and patients' perception of vulnerability (57, 59, 60). Thus, capturing an individual's perception of symptoms may pose challenges in cross-cultural translations and hamper communication between patients and providers regarding the presence and severity of symptoms. Indeed, a retrospective study of patients with lung cancer found that Hispanic patients had a higher pain burden than White patients (61). Evolving research has also uncovered that symptom disparities may arise from the intersection of minority populations, medical conditions, and non-medical drivers of health (62). For example, researchers have found that the presence of a higher number of comorbid conditions, lower education levels, and lower income among these populations may drive pain disparities in minority populations (63, 64). Our research adds to this body of work by suggesting that cross-cultural differences in shared languages among patients with LEP may also contribute to symptom disparities across cancer types.
PROMs may help reduce these disparities in symptoms. Research shows that systematic use of PROMs during cancer care is associated with improved symptom control, decreased acute care use, and prolonged survival (6–8). Barriers to PROMs for patients with LEP include a lack of validated PROMs translated into non-English languages and insufficient time and resources to accommodate patients with LEP (65). The findings from this study underscore the need to translate PROMs into different languages using methodologies such as CVI that account for cultural differences in shared languages. Further research is needed to help clinicians and researchers better understand whether these structural and cultural differences in language contribute to symptom disparities.
4.3 Strengths and limitations of the research
This research study on using the CVI methodology to produce the Spanish ePVA has strengths and weaknesses. A strength is the recruitment of translators with origins in multiple countries and regions to provide a cross-cultural translation of the ePVA. The limitations include that the project was a single-site study at a research-intensive academic center in the northeastern US. Further, the population for the cognitive interviews did not include women despite the recruitment of all genders and races. Additionally, the CVI methodology is intended as a beginning step in developing measures and should always be followed with additional psychometric testing. With these limitations, the team may have missed key cultural nuances that could decrease the performance of the Spanish ePVA. To offset these limitations, the team has conducted follow-up beta testing of the Spanish ePVA with men and women and is planning for additional analyses, including additional psychometric testing to analyze the performance of the Spanish ePVA in studies with larger populations.
5 Conclusion
Translations of health materials may not account for structural and cultural differences in shared languages across countries, such as English, Spanish, Arabic, or Russian. This manuscript presents the use of the CVI methodology with cognitive interviews to translate the ePVA from English into Spanish, resulting in a PROM with acceptable cultural relevance and translation equivalence. The CVI approach may require additional resources but can produce measures that facilitate communication between the patient with LEP and providers, potentially decreasing symptom disparities in patients with LEP.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by NYU Langone Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JV: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AG: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. EL: Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – review & editing. CG: Supervision, Writing – review & editing. RK: Supervision, Writing – review & editing. MT: Data curation, Investigation, Writing – review & editing. GN: Supervision, Writing – review & editing. AS: Conceptualization, Methodology, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Janet H. Van Cleave received funding from: NIH/NCI R01CA282149. Johnson & Johnson Innovations. Oncology Nursing Foundation RE-01. The funding sources had no role in the design of this study
Acknowledgments
We would like to thank Jeremiah Lorico MS, RN, Michele Crespo-Fierro, PhD, MPH, RN, AACRN, CNE, FAAN, and Karla Rodriguez, CNE, DipACCLM, DNP, RN for their assistance in the Spanish translation of the NYU Electronic Patient Visit Assessment (ePVA)©.
Conflict of interest
The copyrights in the ePVA are owned by New York University (NYU). If NYU receives income from licensing the ePVA, then JV may receive a portion of the license income.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2025.1582127 /full#supplementary-material.
References
1. Garcia Farina E, Rowell J, Revette A, Haakenstad EK, Cleveland JLF, Allende R, et al. Barriers to electronic patient-reported outcome measurement among patients with cancer and limited English proficiency. JAMA Netw Open. (2022) 5:E2223898. doi: 10.1001/jamanetworkopen.2022.23898
2. Hofstetter J, McHugh M. Expanding Language Access in Federally Supported Programs: Practical Solutions for Persistent Problems. Migration Policy Institute (2024). June 2024. Available at: https://www.migrationpolicy.org/research/language-access-federally-supported-programs, (Accessed April 22, 2025).
3. U.S. Department of Agriculture Economic Research Service. Limited English Proficiency (LEP). Updates (2023).
4. Sliwinski K, Squires AP. Limited English proficiency is an overlooked research demographic. Am J Nurs. (2024) 124:8. doi: 10.1097/01.NAJ.0001023892.43938.b4
5. Roy M, Purington N, Liu M, Blayney DW, Kurian AW, Schapira L. Limited English proficiency and disparities in healthcare engagement among patients with breast cancer. JCO Oncol Pract. (2021) 17:e1837–45. doi: 10.1200/OP.20.01093
6. Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol. (2016) 34:557–65. doi: 10.1200/JCO.2015.63.0830
7. Basch E, Deal AM, Dueck AC, Scher HI, Kris MG, Hudis C, et al. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA. (2017) 318:197–8. doi: 10.1001/jama.2017.7156
8. Denis F, Basch E, Septans AL, Bennouna J, Urban T, Dueck AD, et al. Two-year survival comparing web-based symptom monitoring vs routine surveillance following treatment for lung cancer. JAMA. (2019) 321:306–7. doi: 10.10001/jama.2018.18085
9. Centers for Medicare & Medicaid Services. Enhancing Oncology Model (2022). Available at: https://innovation.cms.gov/innovation-models/enhancing-oncology-model (Accessed April 14, 2024).
10. Chong A, Witherspoon E, Honig B, Ela E, Cavanagh H, Strawbridge L. Reflections on the oncology care model and looking ahead to the enhancing oncology model. JCO Oncol Pract. (2022) 18:685–90. doi: 10.1200/OP.22.00329
11. Patel TA, Jain B, Parikh RB. The enhancing oncology model: leveraging improvement science to increase health equity in value-based care. J Natl Cancer Inst. (2023) 115:125–30. doi: 10.1093/jnci/djac194
12. Ratko TA, Douglas GW, de Souza JA, Belinson SE, Aronson N. Radiotherapy Treatments for Head and Neck Cancer Update. Rockville, MD: Agency for Healthcare Research and Quality (2014). Available at: https://www.ncbi.nlm.nih.gov/books/NBK269025/
13. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. (2025) 75:10–45. doi: 10.3322/caac.21871
14. World Health Organization International Agency for Research on Cancer. Global Cancer Observatory. Cancer Fact Sheets (2025). Available at: https://gco.iarc.who.int/today/en/fact-sheets-cancers (Accessed April 11, 2025).
15. Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol. (2008) 26:612–9. doi: 10.1200/JCO.2007.14.1713
16. Su YY, Chien CY, Luo SD, Huang TL, Lin WC, Fang FM, et al. Betel nut chewing history is an independent prognosticator for smoking patients with locally advanced stage IV head and neck squamous cell carcinoma receiving induction chemotherapy with docetaxel, cisplatin, and fluorouracil. World J Surg Oncol. (2016) 14:86. doi: 10.1186/s12957-016-0844-2
17. Wu L, Li C, Pan L. Nasopharyngeal carcinomas: a review of current updates. Exp Ther Med. (2018) 15:3687–92. doi: 10.3892/etm.2018.5878
18. Tota JE, Best AF, Zumsteg ZS, Gillison ML, Rosenberg PS, Chaturvedi AK. Evolution of the oropharynx cancer epidemic in the United States: moderation of increasing incidence in younger individuals and shift in the burden to older individuals. J Clin Oncol. (2019) 37:1538–47. doi: 10.1200/JCO.19.00370
19. National Comprehensive Cancer Network (NCCN). Head and Neck Cancers Version 2.2025 (2025). Available at: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (Accessed April 22, 2025).
20. National Cancer Institute. Cancer Statistics. Surveillance, Epidemiology, and End Results Program (2021). Available at: https://seer.cancer.gov/statfacts/html/oralcav.html (Accessed April 3, 2025).
21. National Cancer Institute. Surveillance, Epidemiology, End Results Program: Cancer Statistics (2025). Available at: https://seer.cancer.gov/statfacts/html/oralcav.html (Accessed February 5, 2025).
22. Gane EM, McPhail SM, Hatton AL, Panizza BJ, O’Leary SP. Predictors of health-related quality of life in patients treated with neck dissection for head and neck cancer. Eur Arch Otorhinolaryngol. (2017) 274:4183–93. doi: 10.1007/s00405-017-4754-x
23. Mascarella MA, Richardson K, Mlynarek A, Forest VI, Hier M, Sadeghi N, et al. Evaluation of a preoperative adverse event risk index for patients undergoing head and neck cancer surgery. JAMA Otolaryngol Head Neck Surg. (2019) 145:345–51. doi: 10.1001/jamaoto.2018.4513
24. Ebersole B, McCarroll L, Ridge JA, Liu JC, Bauman J, Donnelly S, et al. Identification and management of late dysfunction in survivors of head and neck cancer: implementation and outcomes of an interdisciplinary quality of life (IQOL) clinic. Head Neck. (2021) 43:2124–35. doi: 10.1002/hed.26681
25. Mason H, DeRubeis MB, Foster JC, Taylor JMG, Worden FP. Outcomes evaluation of a weekly nurse practitioner-managed symptom management clinic for patients with head and neck cancer treated with chemoradiotherapy. Oncol Nurs Forum. (2013) 40:581–6. doi: 10.1188/13.ONF.40-06AP
26. Melotek JM, Cooper BT, Koshy M, Silverman JS, Spiotto MT. Weekly versus every-three-weeks platinum-based chemoradiation regimens for head and neck cancer. J Otolaryngol Head Neck Surg. (2016) 45:62. doi: 10.1186/s40463-016-0175-x
27. Al-Mamgani A, de Ridder M, Navran A, Klop WM, de Boer JP, Tesselaar ME. The impact of cumulative dose of cisplatin on outcome of patients with head and neck squamous cell carcinoma. Eur Arch Otorhinolaryngol. (2017) 274:3757–65. doi: 10.1007/s00405-017-4687-4
28. Bauman JR, Panick JR, Galloway TJ, Ridge JA, Chwistek MA, Collins ME, et al. A pilot study of a collaborative palliative and oncology care intervention for patients with head and neck cancer. J Palliat Med. (2021) 24:1673–81. doi: 10.1089/jpm.2020.0656
29. Van Cleave JH, Fu MR, Bennett AV, Persky MS, Li Z, Jacobson AS, et al. The development, usability, and reliability of the electronic patient visit assessment (ePVA) for head and neck cancer. Mhealth. (2019) 5:21. doi: 10.21037/mhealth.2019.06.05
30. Van Cleave JH, Fu MR, Bennett AV, Concert C, Riccobene A, Tran A, et al. The usefulness of the electronic patient visit assessment (ePVA)© as a clinical support tool for real-time interventions in head and neck cancer. Mhealth. (2021) 7:7. doi: 10.21037/mhealth-19-250
31. Van Cleave J. Implementing the NYU electronic patient visit assessment (ePVA) to improve patient outcomes in head and neck cancer. Oncol Nurs Forum. (2023) 50:e43–4. doi: 10.1188/23.ONF.E3
32. Bowden A, Fox-Rushby JA. A systematic and critical review of the process of translation and adaptation of generic health-related quality of life measures in Africa, Asia, Eastern Europe, the Middle East, South America. Soc Sci Med. (2003) 57:1289–306. doi: 10.1016/S0277-9536(02)00503-8
33. Moslimani M, Lopez MH, Noe-Bustamante L. 11 Facts About Hispanic Origin Groups in the U.S. Immigration & Migration (2023). Available at: https://www.pewresearch.org/short-reads/2023/08/16/11-facts-about-hispanic-origin-groups-in-the-us/#:∼:text=Additional%20information%20about%20all%20U.S.,in%20Latin%20America%20and%20Spain (Accessed April 19, 2025).
34. Lynn MR. Determination and quantification of content validity. Nurs Res. (1986) 35:382–5. doi: 10.1097/00006199-198611000-00017
35. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. (2006) 29:489–97. doi: 10.1002/nur.20147
36. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. (2007) 30:459–67. doi: 10.1002/nur.20199
37. Squires A, Aiken LH, van den Heede K, Sermeus W, Bruyneel L, Lindqvist R, et al. A systematic survey instrument translation process for multi-country, comparative health workforce studies. Int J Nurs Stud. (2013) 50:264–73. doi: 10.1016/j.ijnurstu.2012.02.015
38. Stromseng Sjetne I, Tvedt C, Squires A. Måleinstrumentet « the nursing work index-revised »—oversettelse og utprøving av en norsk versjon. Nurs Res Norway. (2011) 6:358–65. doi: 10.4220/sykepleienf.2011.0189
39. Squires A, Bruyneel L, Aiken LH, Van den Heede K, Brzostek T, Busse R, et al. Cross-cultural evaluation of the relevance of the HCAHPS survey in five European countries. Int J Qual Health Care. (2012) 24:470–5. doi: 10.1093/intqhc/mzs040
40. Squires A, Finlayson C, Gerchow L, Cimiotti JP, Matthews A, Schwendimann R, et al. Methodological considerations when translating “burnout.”. Burn Res. (2014) 1:59–68. doi: 10.1016/j.burn.2014.07.001
41. Orts-Cortés MI, Moreno-Casbas T, Squires A, Fuentelsaz-Gallego C, Maciá-Soler L, González-María E, et al. Content validity of the Spanish version of the practice environment scale of the nursing work index. Appl Nurs Res. (2013) 26:e5–9. doi: 10.1016/j.apnr.2013.08.006
42. Alzate LCC, Bayer GLA, Squires A. Validation of a Spanish version of the practice environment scale of the nursing work index in the Colombian context. Hisp Health Care Int. (2014) 12:34–42. doi: 10.1891/1540-4153.12.1.34
43. Ambani Z, Al-Hamdan Z, Al-Touby S, Ghanim A, Al Jarameez F, Squires A. Content validation of the Arabic translation of the practice environment scale of the nursing work Index-revised. J Nurs Meas. (2019) 27:234–46. doi: 10.1891/1061-3749.27.2.234
44. Zisberg A., Lickiewicz J., Rogozinski A., Hahn S., Mabire C., Gentizon J., et al. (2022). Adapting the geriatric institutional assessment profile for different countries and languages: a multi-language translation and content validation study. Int J Nurs Stud 134. 104283. doi: 10.1016/j.ijnurstu.2022.104283
45. McKown S, Acquadro C, Anfray C, Arnold B, Eremenco S, Giroudet C, et al. Good practices for the translation, cultural adaptation, and linguistic validation of clinician-reported outcome, observer-reported outcome, and performance outcome measures. J Patient Rep Outcomes. (2020) 4:89. doi: 10.1186/s41687-020-00248-z
46. Van Cleave JH, Concert C, Kamberi M, Zahriah E, Most A, Mojica J, et al. A preliminary validation of an optimal cutpoint in total number of patient-reported symptoms in head and neck cancer for effective alignment of clinical resources with patients’ symptom burden. Cancer Care Res Online. (2024) 4:e051. doi: 10.1097/CR9.0000000000000051
47. Lenz ER, Pugh LC, Milligan RA, Gift A, Suppe F. The middle-range theory of unpleasant symptoms: an update. ANS Adv Nurs Sci. (1997) 19:14–27. doi: 10.1097/00012272-199703000-00003
48. Kuder GF, Richardson MW. The theory of the estimation of test reliability. Psychometrika. (1937) 2:151–60. doi: 10.1007/BF02288391
49. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
50. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
51. Davis LL. Instrument review: getting the most from a panel of experts. Appl Nurs Res. (1992) 5:194–7. doi: 10.1016/S0897-1897(05)80008-4
52. Knafl K, Deatrick J, Gallo A, Holcombe G, Bakitas M, Dixon J, et al. The analysis and interpretation of cognitive interviews for instrument development. Res Nurs Health. (2007) 30:224–34. doi: 10.1002/nur.20195
53. Batalove J. Frequently Requested Statistics on Immigrants and Immigration in the United States. Migration Policy Institute. (2024). March 12, 2025. Available at: https://www.migrationpolicy.org/article/frequently-requested-statistics-immigrants-and-immigration-united-states?gad_source=1&gbraid=0AAAAAD8CHmqDzeMBARXxLQHcYcnYuFECw&gclid=Cj0KCQjw_JzABhC2ARIsAPe3ynq6xIQWCucjhkKosyXajVVDE4LvgT6YDVOIfGZ0m2OaW2WQFYp7QQ4aAjPIEALw_wcB. (April 22, 2025).
54. Bullinger M, Anderson R, Cella D, Aaronson N. Developing and evaluating cross-cultural instruments from minimum requirements to optimal models. Qual Life Res. (1993) 2:451–9. doi: 10.1007/BF00422219
55. Flaherty JA, Gaviria FM, Pathak D, Mitchell T, Wintrob R, Richman JA, et al. Developing instruments for cross-cultural psychiatric research. J Nerv Ment Dis. (1988) 176:257–63. doi: 10.1097/00005053-198805000-00001
56. Sun Y-C, Yang F-Y, Liu H-J. Exploring google translate-friendly strategies for optimizing the quality of google translate in academic writing contexts. SN Soc Sci. (2022) 2:147. doi: 10.1007/s43545-022-00455-z
57. Feinstein AR. Symptoms as an index of biological behaviour and prognosis in human cancer. Nature. (1966) 209:241–5. doi: 10.1038/209241a0
58. Cleeland CS, Sloan JA. Assessing the symptoms of cancer using patient-reported outcomes (ASCPRO): searching for standards. J Pain Symptom Manage. (2010) 39:1077–85. doi: 10.1016/j.jpainsymman.2009.05.025
59. Raphael J, Ahmedzai S, Hester J, Urch C, Barrie J, Williams J, et al. Cancer pain: part 1: pathophysiology; oncological, pharmacological, and psychological treatments: a perspective from the British pain society endorsed by the UK association of palliative medicine and the royal college of general practitioners. Pain Med. (2010) 11:742–64. doi: 10.1111/j.1526-4637.2010.00840.x
60. Van Cleave JH, Egleston BL, Ercolano E, McCorkle R. Symptom distress in older adults following cancer surgery. Cancer Nurs. (2013) 36:292–300. doi: 10.1097/NCC.0b013e31826dd517
61. Reyes-Gibby CC, Anderson KO, Shete S, Bruera E, Yennurajalingam S. Early referral to supportive care specialists for symptom burden in lung cancer patients: a comparison of non-Hispanic whites, Hispanics, and non-Hispanic blacks. Cancer. (2012) 118:856–63. doi: 10.1002/cncr.26312
62. Booker SQ, Baker TA, Esiaka D, Minahan JA, Engel IJ, Banerjee K, et al. A historical review of pain disparities research: advancing toward health equity and empowerment. Nurs Outlook. (2023) 71:101965. doi: 10.1016/j.outlook.2023.101965
63. Portenoy RK, Ugarte C, Fuller I, Haas G. Population-based survey of pain in the United States: differences among white, African American, and Hispanic subjects. Journal of Pain. (2004) 5:317–28. doi: 10.1016/j.jpain.2004.05.005
64. Reyes-Gibby CC, Aday LA, Todd KH, Cleeland CS, Anderson KO. Pain in aging community-dwelling adults in the United States: non-Hispanic Whites, non-Hispanic Blacks, and Hispanics. J Pain. (2007) 8:75–84. doi: 10.1016/j.jpain.2006.06.002
65. Allar BG, Eruchalu CN, Rahman S, Mou D, Ortega G, Reich AJ, et al. Lost in translation: a qualitative analysis of facilitators and barriers to collecting patient reported outcome measures for surgical patients with limited English proficiency. Am J Surg. (2022) 224:514–21. doi: 10.1016/j.amjsurg.2022.03.005
Keywords: limited english proficiency, immigrants, patient reported outcome measures, head and neck cancer, public health
Citation: Van Cleave JH, Guerra A, Liang E, Gutiérrez C, Karni RJ, Tsikis M, Nguyen GPC and Squires AP (2025) Using content validity index methodology for cross-cultural translation of a patient-reported outcome measure for head and neck cancer. Front. Health Serv. 5:1582127. doi: 10.3389/frhs.2025.1582127
Received: 10 March 2025; Accepted: 3 June 2025;
Published: 20 June 2025.
Edited by:
Claudia Rutherford, The University of Sydney, AustraliaReviewed by:
Raman Kaur, Reed Elsevier, United StatesChindhu Shunmugasundaram, The University of Sydney, Australia
Copyright: © 2025 Van Cleave, Guerra, Liang, Gutiérrez, Karni, Tsikis, Nguyen and Squires. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Janet H. Van Cleave, amFuZXQuaC52YW5jbGVhdmVAdXRoLnRtYy5lZHU=