 Daniel S. Harvie1,2,3*
Daniel S. Harvie1,2,3*- 1The Hopkins Centre, Menzies Health Institute Queensland, Griffith University, Gold Coast, QLD, Australia
- 2School of Allied Health Sciences, Griffith University, Gold Coast, QLD, Australia
- 3Wearable Computer Laboratory, Australian Research Centre for Interactive and Virtual Environments, University of South Australia, Adelaide, SA, Australia
Chronic conditions represent a significant twenty first century challenge. Education and self-management training are the mainstay of clinical intervention for such conditions since care is dependent on health literacy and self-management. This intervention not only imparts the necessary understanding and skills for self-management, but also helps people to overcome personal barriers to positive behavioral change, such as low self-efficacy. Moreover, education maximizes dignity, by enabling shared decision-making. A plethora of research supports the role of education and self-management training in the management of chronic conditions, whilst at the same time highlighting that not all approaches lead to meaningful behavioral change. Immersive virtual reality (VR) offers a unique set of features and tools for delivering these interventions. For example, the immersive nature focuses attention and promotes engagement; the ability to simulate authentic and interactive real-world scenarios can be used to promote the benefits of active learning; and the ability to facilitate embodiment of avatars with distinct appearance and capability can be used to bias new perceptions and behaviors in-line with the avatar's characteristics. Moreover, the ability to use VR independent of a clinician renders a potential solution to instances where significant barriers to healthcare access exist. This short perspective paper will discuss how VR may be used to host education and self-management interventions in the domain of chronic condition management. Further, it will outline considerations for developers and conclude with a call for the co-creation of new VR-based education and self-management interventions.
Introduction
Rationale
Chronic conditions are responsible for a significant burden on both individuals and society. Globally, 38 million people die from these conditions annually, while their economic burden is projected to reach USD$7 trillion by 2025 (World Health Organization, 2014). While medical treatments have advanced, most chronic conditions depend on long-term adherence to self-management strategies—typically requiring behavioral changes involving diet, rehabilitation and exercise, the correct use of prescription medications, and mitigation or elimination of risk factors such as smoking and stress (Allegrante et al., 2019). As a result, the development of interventions that can assist people in adopting and maintaining long-term self-management has significant potential for impact. Education and skills training are the mainstay of such management.
Virtual reality (VR) has been considered one of the most promising tools to promote learning in educational and work-place training contexts (Liu et al., 2017a), and hence there is much to gain from considering its potential role in providing education to people with chronic conditions. VR is a simulated experience that can be similar to, or completely different from, the real world. In immersive VR, an artificial reality is presented to the user via a Head Mounted Display (HMD), such that the user voluntarily suspends belief and accepts the digitally presented scenario. Immersive VR has been used as a medium for chronic condition interventions such as exposure therapy for phobias and post-traumatic stress, kinesthetic training for chronic neck pain, and physical rehabilitation (Gohari et al., 2019). Whilst immersive VR has been used to deliver information about the science and psychology of pain, as well as in teaching relaxation and mindfulness skills to people with chronic pain (Louw et al., 2019; Darnall et al., 2020), its application in delivering self-management programs is not yet common. Developing such interventions using this new platform is likely complex, and consideration is needed regarding how to assimilate: (1) The unique tools afforded by immersive technologies, (2) The education and training needs of people with chronic conditions, and (3) The key theoretical models that describe the underpinnings of learning and behavior change. These three domains will be now be discussed in more detail.
Unique Features of Virtual Reality for Education & Training
Studies show that simply porting computer-based interventions into VR does not necessarily improve learning, and may even have a negative impact. For example, one study compared a computer-based biology lab simulation to the same class ported directly to VR. The result was a reduction, rather than improvement, in learning outcomes (Makransky et al., 2019). In contrast, another study compared a computer-based trauma response training program to a VR training equivalent built with the features of immersive VR in mind (Coulter et al., 2007). The result was a significant improvement in learning outcomes. Thus, consideration of the unique features of VR and how they may intersect with the goal of learning (and behavior change) is likely to be essential to creating effective interventions.
Attentional Focus: Immersion, Presence, Engagement
The quality of immersion refers to the level of sensory fidelity provided by a VR system hardware and software. Presence is the subjective perception of being physically present in a non-physical world (Slater, 2003, 2018). As such, a system that is more immersive, results in greater illusory presence. With this sense of presence comes engrossment in the multisensory experience, and an exclusion of other internal and external stimuli. This intense attentional focus has been exploited by clinician's seeking temporary pain and anxiety relief during medical procedures (Chan et al., 2018; Eijlers et al., 2019). Importantly, learning depends on directing one's attention toward, and engaging with, educational content (Kolb, 1984). As such, one would predict that this immersive feature would result in better learning outcomes. However, increasing attentional focus in VR does not necessarily translate to learning performance, and paradoxically may reduce it—perhaps by over-loading cognitive resources (Krassmann et al., 2020). As such, self-management related educational content in VR should not rely on this feature alone to improve learning. Moreover, driving development resources into optimizing immersion may yield diminishing returns. Rather, developers should look to optimize other aspects of VR education and self-management training.
Interaction and Role Play
From a young age, learning is linked with movement. According to some learning scientists, the use of movement and gesture helps to off-load mental work and free cognitive resources for consolidation of learning (Goldin-Meadow, 2011). Moreover, it may aid in maintaining motivation and engagement with the educational content. By mapping real-world movement to virtual movement, interactive VR enables users to change their visual perspective, and to manipulate virtual objects using virtual hands. Combined with the ability to simulate both real and abstract scenarios, VR affords unmatched potential to create life-like interactive learning scenarios. These scenarios may relate to understanding their condition or management principles, rehearsing lifestyle or disease management skills, or overcoming personal or social barriers.
Embodiment
In VR, a digital avatar can be substituted for the participants real body and displayed from a first-person perspective. Moreover, virtual and real movement can be tethered. This visuomotor congruence results in the illusory “embodiment” of the digital avatar (Slater et al., 2010; Serino et al., 2016). This illusory ownership over a virtual body supports the sense of presence in the virtual world and may be leveraged to support the learning outcomes. That is, developers can manipulate the characteristics of the avatar to have certain capabilities in a way that biases certain perceptions or behaviors. This technique, along with example applications in the domain of chronic condition management, will be discussed further in sections related to embodied learning and the Proteus effect.
Practical Aspects
For many people with chronic conditions, access to multidisciplinary face-to-face interventions that promote self-management may be limited. This lack of access may result from geography and the lack of appropriately trained clinicians, or limitations related to disability, transportation, time, or finances. Limitations also extend to clinician time which is often focussed on immediate needs or biomedical aspects of a health condition, rather than patient empowerment. Digital health interventions can assist to overcome these structural barriers. In addition, they may also assist in overcoming individual and social access barriers. For example, cultural norms and stigma may prevent some patients seeking assistance from therapists such as psychologists and dieticians. Accessing, for example, stress management or behavioral nutrition training in VR may bypass this barrier, particularly if it is couched within a broader biopsychosocial intervention.
A fact of VR that is rapidly increasing its feasibility, is its diminishing cost and increasing portability. For example, the Oculus Quest costs USD$299 and does not require a separate computer to operate. As such, it is possible to post it out to clients, for example as part of a telehealth intervention. These practical features of VR should not be underestimated and give meaningful direction to where the technology may be best placed.
Chronic Condition Education and Training Needs
Historical Perspective
The historical biomedical approach to healthcare involved training practitioners to treat conditions, without close consideration of the psychosocial context (Allegrante et al., 2019). Factors such as the individual's knowledge, motivation, capacity and resources for carrying out the necessary action were not prioritized (Allegrante et al., 2019). Over the years, chronic condition education has evolved from a compliance-oriented approach, toward an empowerment- and self-management-oriented approach (Allegrante et al., 2019). Whilst health knowledge correlates with outcomes (Camerini et al., 2012), improvements in health behaviors are greater when education is combined with empowerment and self-management training (Allegrante et al., 2019). While these interventions show consistent efficacy, their benefit is often modest, suggesting scope for improvement (Allegrante et al., 2019; Safari et al., 2020) (Hermanns et al., 2020).
The Insufficiency of Knowledge
As mentioned, knowledge acquisition is often insufficient to improve self-management (Ockene et al., 2002). That is, knowledge does not directly translate to new health behaviors unless coupled with: an intention to change, a belief that one has the capacity to change, and the skills to action that change. In this light, VR training programs for chronic conditions should be developed with close attention to learning and behavior change models, such as the Theory of Planned Behavior (Ajzen, 1991). Notably, individual models of behavior change have significant limitations (Rich et al., 2015), and considering additional models such as the PRIME Theory of Human Motivation (West and Brown, 2013), may yield additional insight for development.
Beliefs, Attitudes, Motivations
Knowledge acquisition is impotent if it does not alter beliefs. Likewise, altering a belief is impotent without altering attitude toward a behavior and provoking an intention to change. As such, information must be not only informative, but persuasive. It may be useful to view intention to change along a spectrum, where the central point is a state of ambivalence—characterized by inaction underpinned by unresolved internal ideas about change. Motivational techniques can aid in resolving ambivalence by highlighting personal motivations for change (as well as motivations for inaction) (Engle and Arkowitz, 2006). In VR, engaging, highly visual, and interactive tasks that highlight the benefits of change. Inspiration for such experiences may be drawn from other fields. For example, VR has been used to motivate change in perpetrators of domestic violence, by virtually placing them in the role of victim (Ventura et al., 2020). Salient experiences highlighting the consequences (non)change, and aim to resolve ambivalence, may be one motivation-based application of VR in chronic disease management. Similar non-VR techniques normally facilitated by a clinician are known to aid resolution of ambivalence (Engle and Arkowitz, 2006). Moreover, VR offers ways to facilitate such a task remotely and with the application of principles of learning and behavior change discussed elsewhere in this paper.
Changing Perceptions
Unhelpful social stigmas and perceptions about health and chronic condition management pervade the public sphere (e.g., Louw et al., 2019; Pandrangi et al., 2019; Halabi, 2020; Jung et al., 2020). For example, the belief that health is something managed by health care providers and not something that must be self-managed is still widespread. This aspect is referred to as the subjective norm in the Theory of Planned Behavior (Ajzen, 1991). As such, interventions aiming to improve self-management should consider addressing these perceptions and extol the benefits of patient-led care. Perceptions about management can also be augmented through positive peer support and modeling. The inclusion of a social element within a VR intervention is currently challenging, although Multiple User Virtual Environments have been used (Pillen et al., 2020).
Self-Efficacy: Improving Perceived Control
According to the Theory of Planned Behavior, any intention to change must be complimented by: 1. The perception that one can change, and 2. The actual skills needed to execute the new behavior(s) (Ajzen, 1991). Here, perceptions are a focus, because adopting new self-management behaviors requires patients to accept that improved health is within their power (locus of control) and that they have the capacity (self-efficacy) to execute the necessary change. As such, educational self-management interventions should seek to directly target perceptions of control. With well-designed applications, VR is well-placed to assist in this way. Here, rehearsal of new skills in realistic simulations and with the provision of positive feedback, a user is likely to build a sense of agency and control through experience.
Self-Efficacy: Improving Actual Control
The type of skill building required for effective chronic condition management or rehabilitation will be specific to that condition. For example, the skills required to manage chronic pain may include pacing and graded activity skills; stress-management techniques such as cognitive diffusion or meditation; problem-solving and goal-setting skills; and sleep management schemes. Managing diabetes on the other hand, may focus skills related to weight loss such as meal planning and blood glucose monitoring. Such skills may be acquired and rehearsed in interactive VR scenarios, and made effective through the implementation of gamification, task progression, feedback and reward schemes. One example of a simple implementation of skills training in VR for chronic pain is relaxation training for stress management (Darnall et al., 2020). Here, training to self-induce a relaxed state can be made easier by overlaying relaxing audio-visual contexts and breath detection and feedback techniques (Darnall et al., 2020). Notably, such interventions may have implications beyond improving perceived capacity to manage stress. That is, meditation has also been shown to impact cognitive control (Waller and Bates, 1992). Cognitive control refers to our ability to inhibit automatic responses. Cognitive control relates to skills needed when attempting behavior change, such as self-discipline and ability to delay gratification (Waller and Bates, 1992; O'hea et al., 2005).
Theoretical Models of Learning and Behavior Change in VR
The interplay between learning theory and the affordances of VR have been thoroughly reviewed (Pillen et al., 2020). Here we consider key aspects of learning theory in the context of VR-based education and training interventions for chronic conditions and the specific goal of positive behavior change. As suggested by the Theory of Planned Behavior, the targets of behavior change interventions should consider beliefs and attitudes, perceptions about best and normal care, perceptions of self-efficacy, and skills-based knowledge (Ajzen, 1991). Understanding learning theory represents an opportunity for developers seeking to create effective intervention.
Constructivism
Constructivism is an empirically supported theory where understanding is constructed actively through experiences, and reflections on those experiences (Petrie et al., 1995). The VR toolkit includes features that give it distinct capacity to mediate salient experiences where participants learn through interacting with content, and in a way that either intentionally or naturally stimulates reflection. These features include the ability to simulate abstract scenarios, to simulate numerous real-world scenarios without having to change locations or use physical equipment, the ability to provide real-time feedback, reinforcement and reflective prompts, to apply gamification, and to induce a state of presence that may foster greater engagement and curiosity (Liu et al., 2017b). Constructivist principles are best satisfied in content creation when the participant has greater capacity to constructs his or her own learning experience within the learning environment (Colzato et al., 2015; Pillen et al., 2020). That is, the degree to which constructivist principles are satisfied, can be visualized on a scale of passive consumption of information, through to producers of information (see Figure 1, including example VR activities).
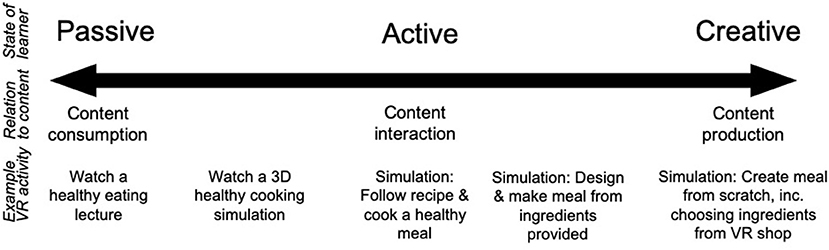
Figure 1. A scale of relating to the learning theory of constructivism.
Embodied Cognition and Embodied Learning
Embodied cognition is a theory of cognition based on the premise that the brain and body are intrinsically coupled by virtue of their co-evolution (Fox, 2001; Inzlicht et al., 2015). In this theory which supports the constructivist paradigm, the body—along with its sensorimotor capabilities and brain-held representations—provide the neural architecture for human cognitive processes. Health education programs are typically mentalistic—learners sit, watch, and listen, with little engagement of the body. Like other cognitive processes, learning co-evolved with the body. As a result, better engagement of sensorimotor systems in learning has significant potential to enhance education. To this aim, the potential for engagement of the body through interaction, gives VR unique capacity to employ embodied learning principles in a manner that is more scalable than real-world simulated learning.
Narrative-Based Learning
Narrative-based learning is a learning model grounded in the theory that humans define their experiences within the context of narratives—which serve as cognitive structures and a means of communication, as well as aiding people in framing and understanding their perceptions of the world (Fox, 2001). Narrative is also an important motivational component of learning. At the core of the narrative learning approach, is a problem that must be solved by constructing and applying knowledge.
The Proteus Effect
Remarkably, the occupant of a virtual avatar can express new behaviors and attitudes reflective of the character of the avatar (Mahon, 2015; Jacobson, 2017). For example, after flying above a virtual city as a superhero, participants are more likely to help an experimenter pick up a jar of “accidentally” spilled pens than if they flew in a virtual helicopter (Ziemke, 2016). Participants have even been shown to perform better on cognitive tasks when embodying Einstein (Bruner, 1991). This close relationship between mind and (perceived) body has been described as embodied cognition (Fox, 2001; Inzlicht et al., 2015). One recent clinical application of this idea was in a case report with a person with Chronic low back pain (LBP) (Slater and Sanchez-Vives, 2014). Here, the patient's presentation included negative body-related attitudes and perceptions, such as low physical self-confidence and perceptions of physical vulnerability that may have contributed to his presentation and level of disability. When the patient embodied avatars that had high-physical capability and athletic physical-appearance, the patient displayed more positive self-perceptions—such as greater perceptions of strength and confidence with physical activity.
Generalization
The concept of generalization is well-known in the learning sciences (Slater, 2017). Generalization denotes that learning in one context, does not necessarily fully translate to another context (Rosenberg et al., 2013; Slater, 2017). As such, VR education programs should consider intermediate steps to facilitate real-world translation. In the case of VR relaxation training for example, a “transfer phase” could be included that introduces relaxation techniques into real-world routines. Transfer may also be aided by a debriefing session, between the clinician and client, following the simulation.
Examples From the Literature
While existing examples in the literature are scant, most do not capitalize on the features of virtual reality or leverage education science principles. For example, a recent VR-based education and rehabilitation for chronic lung disease delivered education simply as 2D videos in a 3D environment (Banakou et al., 2018). Others use 3D content simply to view anatomical pathology, and aid understanding of a disease state (e.g., Harvie et al., 2020). Some applications have used experiential learning techniques. For example, one application uses a virtual lion to induce fear—presumably to show how our defensive response systems (e.g., fear and pain) respond to the perception of danger, rather than danger itself. This is likely to persuade patients that their pain is not necessarily a sign of damage, and that re-engaging in activity is safe (Banich and Caccamise, 2011). Moreover, meditation-based games that interact with the user's breath, have been used in applications that teach stress-management skills (Darnall et al., 2020). Educational techniques that align with the imaginative and creative mandate of the constructivist paradigm are difficult to find in the health context but may be found elsewhere (e.g., Sharkey and Sharkey, 1993).
Conclusion
Immersive VR has opened up a world of possibilities in healthcare and beyond, most of which are currently untapped. Whilst not exhaustive, this review has described many of the important features of VR that make it a potentially transformative tool for facilitating education and self-management interventions for people with chronic conditions. Moreover, it has outlined some of the key learning theories that intersect with the features of VR that may assist in effective program development (see Table 1 for a summary table of key points for developing education and self-management interventions in VR). While developer tools such as visual scripting and large repositories of pre-modeled assets reduce the resources and time required to develop new applications, the effort needed to create high-quality experiences should not be underestimated. Indeed, the effectiveness of a VR intervention will rely on the design and production quality, as much as the educational content itself. As such, progress in this space will require support from funders of health research and industry, as well as transdisciplinary collaboration. This co-design process may include: (1) Narrative designers, specialized health communication experts and educationalists, (2) Health and behavioral psychology experts from academic, clinician and patient perspectives, (3) Visual and sound content developers and software programmers, and 4. Experts in human computer interaction and gamification. Key points for developing education and self-management strategies are summarized in Table 1. Given the potential upside of improved self-management in the growing problem of chronic conditions, leveraging tools with strong potential is imperative.

Table 1. Key points for developing education and self-management interventions in virtual reality.
Author Contributions
This manuscript was conceived and implemented by DH.
Funding
DH was supported by an Early Career Research Fellowship from the National Health and Medical Research Council of Australia (GNT2204950). This paper was the result of projects supported by a Hopkins Centre seeding grant and an Australian Centre for Interactive and Virtual Environments seeding grant.
Conflict of Interest
The author is involved with developing a VR education and self-management training intervention for people with chronic pain.
References
Ajzen, I. (1991). The theory of planned behavior. Organ. Behav. Hum. Decis. Process 50, 179–211. doi: 10.1016/0749-5978(91)90020-T
Allegrante, J. P., Wells, M. T., and Peterson, J. C. (2019). Interventions to support behavioral self-management of chronic diseases. Annu. Rev. Public Health 40, 127–146. doi: 10.1146/annurev-publhealth-040218-044008
Banakou, D., Kishore, S., and Slater, M. (2018). Virtually being Einstein results in an improvement in cognitive Task performance and a decrease in age bias. Front. Psychol. 9:917. doi: 10.3389/fpsyg.2018.00917
Banich, M. T., and Caccamise, D. (2011). Generalization of Knowledge: Multidisciplinary Perspectives. New York, NY: Psychology Press.
Camerini, L., Schulz, P. J., and Nakamoto, K. (2012). Differential effects of health knowledge and health empowerment over patients' self-management and health outcomes: a cross-sectional evaluation. Patient Educ. Couns. 89, 337–344. doi: 10.1016/j.pec.2012.08.005
Chan, E., Foster, S., Sambell, R., and Leong, P. (2018). Clinical efficacy of virtual reality for acute procedural pain management: a systematic review and meta-analysis. PLoS ONE 13:e0200987. doi: 10.1371/journal.pone.0200987
Colzato, L. S., Sellaro, R., Samara, I., and Hommel, B. (2015). Meditation-induced cognitive-control states regulate response-conflict adaptation: evidence from trial-to-trial adjustments in the Simon task. Conscious. Cogn. 35, 110–114. doi: 10.1016/j.concog.2015.04.012
Coulter, R., Saland, L., Caudell, T., Goldsmith, T. E., and Alverson, D. (2007). “The effect of degree of immersion upon learning performance in virtual reality simulations for medical education,” in Medicine Meets Virtual Reality 15: In Vivo, in Vitro, in Silico: Designing the Next in Medicine, ed J. D. Westwood (Amsterdam: IOS Press), 155.
Darnall, B. D., Krishnamurthy, P., Tsuei, J., and Minor, J. D. (2020). Self-administered skills-based virtual reality intervention for chronic pain: randomized controlled pilot study. JMIR Form. Res. 4:e17293. doi: 10.2196/17293
Eijlers, R., Utens, E. M., Staals, L. M., de Nijs, P. F., Berghmans, J. M., Wijnen, R. M., et al. (2019). Meta-analysis: systematic review and meta-analysis of virtual reality in pediatrics: effects on pain and anxiety. Anesth. Analg. 129:1344. doi: 10.1213/ANE.0000000000004165
Engle, D. E., and Arkowitz, H. (2006). Ambivalence in Psychotherapy: Facilitating Readiness to Change: New York, NY: Guilford Press.
Gohari, S. H., Gozali, E., and Kalhori, S. R. N. (2019). Virtual reality applications for chronic conditions management: a review. Med. J. Islam. Repub. Iran 33:67. doi: 10.34171/mjiri.33.67
Goldin-Meadow, S. (2011). Learning through gesture. Wiley Interdisc. Rev. Cogn. Sci. 2, 595–607. doi: 10.1002/wcs.132
Halabi, O. (2020). Immersive virtual reality to enforce teaching in engineering education. Multimedia Tools Appl. 79, 2987–3004. doi: 10.1007/s11042-019-08214-8
Harvie, D. S., Rio, E., Smith, R. T., Olthof, N., and Coppieters, M. W. (2020). Virtual reality body image training for chronic low back pain: a single case report. Front. Virtual Real. 1:13. doi: 10.3389/frvir.2020.00013
Hermanns, N., Ehrmann, D., Finke-Groene, K., and Kulzer, B. (2020). Trends in diabetes self-management education: where are we coming from and where are we going? A narrative review. Diabet. Med. 37, 436–447. doi: 10.1111/dme.14256
Inzlicht, M., Bartholow, B. D., and Hirsh, J. B. (2015). Emotional foundations of cognitive control. Trends Cogn. Sci. 19, 126–132. doi: 10.1016/j.tics.2015.01.004
Jacobson, J. (2017). “Authenticity in immersive design for education,” in Virtual, Augmented, and Mixed Realities in Education, eds D. Lieu, C. Dede, R. Juang, and J. Richards (Singapore: Springer), 35–54.
Jung, T., Moorhouse, N., Shi, X., and Amin, M. F. (2020). A virtual reality–supported intervention for pulmonary rehabilitation of patients with chronic obstructive pulmonary disease: mixed methods study. J. Med. Internet Res. 22:e14178. doi: 10.2196/14178
Kolb, D. A. (1984). Experience as the Source of Learning and Development. Upper Sadle River, NJ: Prentice Hall
Krassmann, A. L., Herpich, F., Tarouco, L. M. R., and Bercht, M. (2020). “Investigating the relation between sense of presence, attention, and performance: virtual reality versus web 2020,” in International Conference on Human-Computer Interaction (Cham: Springer).
Liu, D., Bhagat, K. K., Gao, Y., Chang, T. W., and Huang, R. (2017a). “The potentials and trends of virtual reality in education,” Virtual, Augmented, and Mixed Realities in Education, eds D. Lieu, C. Dede, R. Juang, and J. Richards (Singapore: Springer), 105–130.
Liu, D., Dede, C., Huang, R., and Richards, J. (2017b). Virtual, Augmented, and Mixed Realities in Education. Singapore: Springer.
Louw, A., Louw, C., and Flynn, T. (2019). Case report: pain neuroscience education using virtual reality. Pain Rehabil. J. Physiother. Pain Assoc. 2019, 4–7.
Mahon, B. Z. (2015). What is embodied about cognition? Lang. Cogn. Neurosci. 30, 420–429. doi: 10.1080/23273798.2014.987791
Makransky, G., Terkildsen, T. S., and Mayer, R. E. (2019). Adding immersive virtual reality to a science lab simulation causes more presence but less learning. Learn. Instruct. 60, 225–236. doi: 10.1016/j.learninstruc.2017.12.007
Ockene, I. S., Hayman, L. L., Pasternak, R. C., Schron, E., and Dunbar-Jacob, J. (2002). Task force# 4—adherence issues and behavior changes: achieving a long-term solution. J. Am. Coll. Cardiol. 40, 630–640. doi: 10.1016/S0735-1097(02)02078-8
O'hea, E. L., Grothe, K. B., Bodenlos, J. S., Boudreaux, E. D., White, M. A., and Brantley, P. J. (2005). Predicting medical regimen adherence: the interactions of health locus of control beliefs. J. Health Psychol. 10, 705–717. doi: 10.1177/1359105305055330
Pandrangi, V. C., Gaston, B., Appelbaum, N. P., Albuquerque Jr, F. C., Levy, M. M., and Larson, R. A. (2019). The application of virtual reality in patient education. Ann. Vasc. Surg. 59, 184–189. doi: 10.1016/j.avsg.2019.01.015
Petrie, K., Moss-Morris, R., and Weinman, J. (1995). The impact of catastrophic beliefs on functioning in chronic fatigue syndrome. J. Psychosom. Res. 39, 31–37. doi: 10.1016/0022-3999(94)00071-C
Pillen, H., McNaughton, D., and Ward, P. R. (2020). A review of critical pedagogies in health and social care: findings from a ‘best fit'framework synthesis. Crit. Public Health 30, 468–486. doi: 10.1080/09581596.2019.1591613
Rich, A., Brandes, K., Mullan, B., and Hagger, M. S. (2015). Theory of planned behavior and adherence in chronic illness: a meta-analysis. J. Behav. Med. 38, 673–688. doi: 10.1007/s10865-015-9644-3
Rosenberg, R. S., Baughman, S. L., and Bailenson, J. N. (2013). Virtual superheroes: using superpowers in virtual reality to encourage prosocial behavior. PLoS ONE 8:e55003. doi: 10.1371/journal.pone.0055003
Safari, R., Jackson, J., and Sheffield, D. (2020). Digital self-management interventions for people with osteoarthritis: systematic review with meta-analysis. J. Med. Internet Res. 22:e15365. doi: 10.2196/15365
Serino, S., Pedroli, E., Keizer, A., Triberti, S., Dakanalis, A., Pallavicini, F., et al. (2016). Virtual reality body swapping: a tool for modifying the allocentric memory of the body. Cyberpsychol. Behav. Soc. Netw. 19, 127–133. doi: 10.1089/cyber.2015.0229
Sharkey, N. E., and Sharkey, A. J. (1993). Adaptive generalisation. Artificial Intell. Rev. 7, 313–328. doi: 10.1007/BF00849058
Slater, M. (2017). “Implicit learning through embodiment in immersive virtual reality,” in Virtual, Augmented, and Mixed Realities in Education, eds D. Lieu, C. Dede, R. Juang, and J. Richards (Singapore: Springer), 19–33.
Slater, M. (2018). Immersion and the illusion of presence in virtual reality. Br. J. Psychol. 109, 431–433. doi: 10.1111/bjop.12305
Slater, M., and Sanchez-Vives, M. V. (2014). Transcending the self in immersive virtual reality. Computer 47, 24–30. doi: 10.1109/MC.2014.198
Slater, M., Spanlang, B., Sanchez-Vives, M. V., and Blanke, O. (2010). First person experience of body transfer in virtual reality. PloS ONE 5:e10564. doi: 10.1371/journal.pone.0010564
Ventura, S., Badenes-Ribera, L., Herrero, R., Cebolla, A., Galiana, L., and Baños, R. (2020). Virtual reality as a medium to elicit empathy: a meta-analysis. Cyberpsychol. Behav. Soc. Netw. 23, 667–676. doi: 10.1089/cyber.2019.0681
Waller, K. V., and Bates, R. C. (1992). Health locus of control and self-efficacy beliefs in a healthy elderly sample. Am. J. Health Promot. 6, 302–309. doi: 10.4278/0890-1171-6.4.302
World Health Organization (2014). Global Status Report on Noncommunicable Diseases 2014. World Health Organization.
Keywords: virtual reality, chronic condition, chronic disease, self-management, health education (MeSH)
Citation: Harvie DS (2021) Immersive Education for Chronic Condition Self-Management. Front. Virtual Real. 2:657761. doi: 10.3389/frvir.2021.657761
Received: 23 January 2021; Accepted: 18 March 2021;
Published: 13 April 2021.
Edited by:
Danielle Levac, Northeastern University, United StatesReviewed by:
Deborah Richards, Macquarie University, AustraliaVangelis Lympouridis, University of Southern California, United States
Copyright © 2021 Harvie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel S. Harvie, ZC5oYXJ2aWVAZ3JpZmZpdGguZWR1LmF1