 Kamilla Pedersen
Kamilla Pedersen Peter Musaeus
Peter Musaeus- 1Centre for Educational Development, Aarhus Universitet, Aarhus, Denmark
- 2Psychosis Research Unit, Aarhus University Hospital Psychiatry, Aarhus, Denmark
Virtual Reality has emerged as a valuable tool in medical education, primarily for teaching basic sciences and procedural skills. However, its potential in clinical psychiatry, particularly in comprehending the subjective experiences of individuals with mental illness, remains largely untapped. This paper aims to address this gap by proposing a phenomenological-driven approach to the design of virtual reality in psychiatry education. Insights into psychopathology, which involves the systematic study of abnormal experiences as well as self-awareness on behalf of the clinician, demands training. The clinician must develop sensitivity, observational skills, and an understanding of patients’ subjective experiences. While integrating the subjective perspective and promoting emotional self-awareness in psychiatry education have been recommended, further research is necessary to effectively harness virtual reality for this purpose. Drawing from the convergence of virtual reality, phenomenological approaches to grasping subjectivity and psychopathology, this paper aims to advance teachings in psychopathology. It underscores the importance of integrating biomedical knowledge with the lived experiences of psychiatric patients to offer learners a comprehensive understanding of clinical psychiatry. This approach is deeply rooted in the theories of three influential figures: Karl Jaspers, a German psychiatrist and philosopher, who emphasized the role of phenomenology in clinical psychiatry; Ludwig Binswanger, a Swiss psychiatrist and psychotherapist, known for his work on existential analysis; and Medard Boss, a Swiss psychiatrist and psychoanalyst, who introduced Daseinsanalysis, focusing on the individual’s existence in the world. To facilitate learning in acute psychiatry, a virtual reality scenario was developed. This scenario offers two perspectives: one from the patient’s viewpoint, simulating a severe psychotic incident, and the other from the perspective of junior doctors, exposing them to the challenges of communication, decision-making, and stress in a clinical setting. This paper argues that these phenomenological approaches are valuable in helping inform the didactical considerations in the design of the virtual reality scenario, enhancing the learning experience in psychiatry education. It highlights the potential of virtual reality to deepen understanding in the teaching of clinical psychiatry and provides practical insights into its application in an educational context.
1 Introduction
The interaction between a novice clinician and a distressed psychotic patient is anything but virtual reality. It embodies a genuine convergence of two individuals, each immersed within their distinctive realm of reality. This encounter manifests as deeply significant while simultaneously evoking a sense of profound disquietude. The clinician can easily become overwhelmed by the patient who is trapped in delusional perceptions and burdened by a profound sense of alienation. The patient’s behavior may appear irrational, as if it lacks meaningful responses to human interaction, whether it be therapeutic efforts or simple acts of compassion like smiling or comforting gestures (Qureshi et al., 2017). Preparing clinicians for the complexities of acute psychiatric care involves a dual focus: meticulous attention to the clinical environment and the whole range of embodied cognitions that make up the encounter of the clinician and patient. Learning technology holds the potential to serve not only as a window into the patient’s perspectives but also as a mediating force, effectively bridging the gap between the clinician’s clinical gaze and the fragmented worldview of individuals experiencing psychosis. Learning technology acts as a medium to facilitate a deeper understanding of the patient’s unique perspective within their complex world. Gaining an insight into how symptoms influence a psychiatric patient’s behavior is crucial for making informed decisions and engaging with patients as a professional helper entrusted with another person’s care.
Psychopathology is an integral part of clinical psychiatry, which is defined as the systematic study of patients’ abnormal experiences, cognition, and clinical observation of behavior (Sanati, 2020). Thus, psychiatry, as a field of study and practice, indeed involves both objective and subjective aspects. Advancing opportunities made possible by progressive imaging techniques and genetic testing continually add to improving the field of psychiatry, entailing a push toward objectivism in diagnostic testing and physiological measurement (Parnas et al., 2013). However, the emphasis on objectivist criteria reflected in psychiatry education of health professionals fails to situate psychiatry within the interpersonal and subjective realm which conditions the complexities of clinical practices where the patient is truly met (Goldberg et al., 2008). Navigating this interrelatedness may be particularly essential in psychiatry where it is fundamental that the clinicians exercise a fertile patient approach to obtain access to explore their subjective experience by communication to identify, and exclude, symptoms (Nordgaard and Parnas, 2013). Furthermore, the clinicians must develop self-awareness and an understanding of their own emotions, preconceptions, and reactions which could potentially bias their clinical judgment (Baron et al., 2009).
This necessitates different approaches to teaching clinical psychiatry compared to more tangible medical fields as it involves grasping not only “visible” biomedical knowledge but also the methods for assessing, gathering, and documenting subjective findings. Recognizing this, there is a growing acknowledgment that psychiatry education should blend biomedicine with an exploration of the subjective perspective and emotional self-awareness to enhance students’ learning in psychopathology (Yakeley et al., 2014; Baniasadi et al., 2020). However, there is limited guidance on how to integrate these elements effectively into clinical teaching (Jensen et al., 2023).
The hypothesis we develop in this paper is that phenomenology as a guiding compass to the development of virtual reality has the means to advance health professionals learning the epistemological convergences of biomedical facts, the subjective experience of patients, and self-awareness in clinical psychiatry as an inseparable whole (Irarrázaval and Kalawski, 2022).
We believe this approach will enable learning experiences to engage learners in the tacit complexities of clinical psychiatry scenarios and thus provide them with a deepened understanding of clinical psychiatry (Jaspers, 1997; Fuchs, 2013).
1.1 Virtual reality in medical education as applied to psychiatry education
The idea of using virtual reality for educational purposes has been implemented since the inception of the virtual reality era (Makhkamova et al., 2019). Over the past two decades, virtual reality has firmly established itself as a prominent training technology in medical education, finding prominence in the fields of medicine, surgery, and psychiatry education. In the realm of psychiatry education, virtual reality remains relatively new and unexplored. The use of virtual reality in medical education encompasses diverse designs, with various formats, applications, and focuses, depending on the target audience and clinical context. These formats include text descriptions, video materials, simulated patients, and computer-based multimedia. Some patient cases emphasize theory to impart knowledge about diseases and treatments, while others require a practical approach, emphasizing skill development in communication, teamwork, and decision-making (Pomata, 2014). Training technologies in surgery and medicine often target specific practice domains, concentrating on procedural skills and transferring cognitive knowledge (Courteille, 2008; Cheung et al., 2018). One such example is serious gaming, where game technology is utilized to recreate work and decision-making scenarios, providing an immersive environment for interactive clinical learning (Lam et al., 2019). A crucial element in serious gaming depends on interactions where learners can engage with the physical layout of the ward, manipulate medical equipment, and have the freedom to make choices and respond to a wide range of interactions with virtual patients and healthcare professionals (Kampa et al., 2016). These virtual environments are meticulously crafted to replicate real-world hospital settings, offering learners a realistic training experience with varying levels of interactivity and graphics (Graafland et al., 2012).
Virtual reality has the potential to place the person in context at the center of the simulated cases so that the model represents the patient as well as the immediate context of the patient’s life, both as active participants in the virtual environment and as bystanders (Ho and Ng, 2022). The embodied experience represents the user’s body in a different human or even non-human form, for example, through avatars or simulated actors, as extensions of the user’s physical presence in the virtual space (Sora-Domenjó, 2022). The physical presence may refer to either embodied cognition aspects, which consider the user’s conceptualization of reality, or embodied interaction, which reflects considering the user’s body as the sensing and interacting instrument potentially facilitated by virtual reality devices (Regenbrecht and Schubert, 2023). Such cases provide a unique opportunity for learners to experience a sense of presence, allowing them to observe patients from different perspectives—not only spatially as typical clinicians but also socially, feeling together with the patient or even co-existing, being next to the patient in the same space (Bula, 2012). Presence is yet fundamentally an individual feeling arising from subconscious processes being immediate, and philosophically, as not being objectively verifiable (Slater et al., 2009). This illusory sense of presence in virtual reality has displayed the capability of nurturing empathetic comprehension by enabling clinicians to envision situations from another individual’s standpoint via perspective-taking (Ventura et al., 2020).
The influence on empathy by perspective-taking in virtual reality was explored in a pilot study by Wijma et al. (2018) who introduced a virtual reality environment to experience living with dementia with the purpose of reducing psychological distress in caregivers of individuals with dementia. Similarly, Formosa et al. (2018) investigated the impact of a virtual environment on increasing empathy for individuals with a schizophrenic spectrum disorder, showcasing the daily activities of those with schizophrenia. Both studies found measurable improvement in empathy. Empathic attributes in clinicians are positive for building meaningful relationships and achieving effective patient communication in clinical practice (Scholl et al., 2014). It is, however, worth noting that feelings of empathy someone might develop within a virtual reality environment do not necessarily elicit behavioral change (Ramirez et al., 2021). Empathy and emotions in learning play distinct yet interconnected roles in the educational process. Empathy involves understanding and sharing the feelings and perspectives of others.
Emotions in this context refer to the personal feelings and reactions evoked by the learning experience. Emotions can influence engagement, motivation, and memory retention. Libera et al. (2021) introduced a method for assessing paranoia, emphasizing the capability of 360° immersive videos to elicit emotions like fear, anxiety, anger, confidence, and curiosity. These videos simulate experiences of feeling paranoia in different public places, involving perspective-taking. The study also revealed cognitive reactions linked to paranoia, showing promising results in the validity of the method as an assessment tool. It is also important to distinguish between the concepts of presence and emotional content as they are separate but intertwined. Emotion is an integral part of the response to a virtual environment, raising the question of whether these reactions mirror what one would expect in a real-life situation (Slater et al., 2009). Consequently, the incorporation of virtual environments into medical education needs to ensure not only the learning of problem-solving clinical skills in virtual clinical scenarios but also the transferability of acquired skills into the complex reality characterizing clinical settings (Gerup et al., 2020). A concern regarding clinical transferability from virtual environments has been raised about the impersonal and anonymous nature of virtual patient systems, as well as the isolated learning experience characterizing self-directed learning (Urresti-Gundlach et al., 2017). Despite technological advancements and the improved realism of avatars in virtual scenarios, these technologies still face challenges in achieving genuine human relatability. One notable limitation is the absence of mimicry and emotional responses in avatars, which are fundamental aspects of human communication. Mimicry, encompassing facial expressions and body language, plays a vital role in conveying emotions and establishing a sense of authenticity in interpersonal interactions (Pedersen et al., 2021). The lack of subtle cues in avatars can impede the learner’s experience of authenticity, making it difficult to empathize with the virtual characters (Sora-Domenjó, 2022; Rapuano et al., 2023). Furthermore, the presence of the uncanny valley effect adds another obstacle to achieving genuine human relatability in avatars. This phenomenon occurs when humanoid figures closely resemble humans but fall slightly short, leading to feelings of unease or discomfort (Mori, 1970). Despite the best intentions to create realistic avatars, the lack of nuanced emotional responses and the uncanny valley effect can create a disconnect between learners and the virtual environment (Kegel et al., 2020). In many virtual reality systems, the haptic aspect is underdeveloped, especially when it comes to simulating actions like caressing, patting on the shoulder, or running fingers through hair. These limitations are crucial in clinical teaching, where genuine human interaction and empathy are essential for patient care. Capturing the nuances, subtleties, and expressions that define the psychic phenomena of subjective experiences and embodied sense of self in unique patients requires a high level of sensitivity, a solid understanding of mental phenomena, and familiarization with common symptoms, as well as adept communication and observational skills (Jaspers, 1968; Fuchs and Schlimme, 2009). The inability of avatars to completely replicate human relatability can impede the development of essential clinical skills in psychiatry; specifically the ability to observe authentic human facial and bodily expressions and to focus on non-verbal communication and responses enriched with human-like emotions holds significant importance (Kenny et al., 2008; Edelbring et al., 2011).
An additional consideration, especially when considering the acquisition of new skills within a secure and self-directed learning setting, is the potential of immersive virtual reality to provide deeply meaningful experiences for learners unfettered by the bounds of reality. However, despite its engaging nature, immersive virtual reality may not necessarily result in better learning outcomes for basic science compared to traditional methods such as PowerPoint presentations (Parong and Mayer, 2018). Yet another challenge posed by immersive virtual reality experiences is the potential for learners to resort to escapism. Instead of confronting life’s challenges and uncertainties head-on, individuals might seek solace through avenues like excessive immersion in virtual realms (Siricharoen, 2019). This detachment from authentic existence risks ensnaring them within the artificial confines of a virtual environment, deterring them from one’s authentic being-in-the-world, which risks trapping the individual in the safe confines of a virtual world (Haj-bolouri, 2023). Immersive virtual environments may offer an alternate world without time constraints and become a compelling escape from the demands and complexities of a meaningful clinical encounter.
Taxonomy serves as a fundamental tool in any scientific discipline, including education, by facilitating the organization and understanding of concepts within the field (Anderson et al., 2001). It plays a vital role in promoting effective learning and the systematic categorization of knowledge within a given discipline. In general, there is a demand for guidelines and established best practices in the design of virtual learning applications to explore questions such as which supportive technologies are more suitable for distinct target audiences and instructional methods for diverse instructional activities and desired learning outcomes (Makhkamova et al., 2019). The designated teacher functions as guides and facilitators of learning in the critical moments of transformation during students’ educational experiences (Meyer and Land, 2005). To deliver a complete meaningful virtual reality learning experience, one has to think about not just what goes on inside the simulation, story, visuals, and audio but also what transpires around the framework that surrounds and supports it. Medical students need an intellectual and emotional space to reflect on their inexorable transition from lay to professional status, as well as validation from their mentors about that process (Goldberg et al., 2008). Learning how to navigate clinical psychiatry requires a higher level of taxonomy as this field involves intricate cognitive processes that demand a greater degree of abstraction and conceptualization, particularly in the assessment of individualized and nuanced cases, such as those involving psychotic patients (Arseneault, 2021). Thus, teachers play an essential role in scaffolding of virtual reality to provide support and structure to students as they learn and develop new skills at a higher taxonomy level, whereas the educators play a significant role in guiding and prompting student reflection and critical thinking, gradually reducing support as their understanding and proficiency grow (Woolley and Jarvis, 2007). The intention must be to enable a shared simulated learning experience with the ability to address a flexible range of clinical domains and learning taxonomies to enrich the intuitive and analytical skills required in the field of psychopathology (Stanghellini, 2017).
While medical education researchers have acknowledged the effectiveness of virtual reality, their attention has been predominantly centered on cognitive aspects and procedural skills. This focus has potentially led to a lack of emphasis on the specific skills unique to clinical psychiatry practices (Piot et al., 2020).
1.2 Navigating the depths of acute psychiatry
In medical education, the transition to psychiatry clinical training is considered stressful as students must cope with new responsibilities and expectancies (Belitsky and Kenny, 1995; Tazakori et al., 2008). Medical training in the assessment of somatic illness does not fully address the specific aspects of communicating with psychiatric patients to assess psychiatric symptoms (Kurtz et al., 2003; Priebe et al., 2011; Engel et al., 2022). Encountering a transgressive patient with psychosis as a junior doctor can be a taxing and potentially overwhelming experience. Psychosis refers to a loss of contact with reality, leading to hallucinations, delusions, and disorganized thinking and behavior. In addition, stigma regarding psychiatry and psychiatric patients is known to add to insecurity, which may negatively affect clinical communication and diagnostic accuracy. Thus, navigating psychiatry represents a challenge, particularly for junior doctors who are often anxious about how to meet psychiatric patients in acute distress (Gask et al., 2011; Lewis, 2013).
Acute psychiatry refers to the branch of psychiatry that focuses on the diagnosis, assessment, and treatment of individuals experiencing severe and acute mental health crises (Bowers et al., 2005). It involves providing immediate care and intervention to patients who are in distress or experiencing psychiatric emergencies (Nicholls et al., 2011). However, acute incidents also occur in somatic (non-psychiatric) wards as medical conditions, such as certain neurological or endocrine disorders, which can manifest with psychiatric symptoms (Foster et al., 2007). Without a basic understanding of symptoms, medical professionals may struggle to recognize and appropriately manage these cases (Nordt et al., 2006).
Phenomenology plays a significant role in psychiatry by focusing on the assessment of abnormal mental phenomena, which is the core of psychiatric skills (Parnas et al., 2013). Phenomenology offers insights into patients’ mental experiences by bridging the gap between everyday clinical encounters and abstract concepts. This phenomenological approach helps us understand and describe the fundamental aspects of patients’ experiences, making the classification process clearer (Kräupl Taylor, 1967). Healthcare professionals across all specialties must possess the competences and skills to manage acute incidents, including those with psychiatric components (Kallivayalil, 2012). Gaining an insight and skill training into the phenomenological approach that characterizes practices in clinical psychiatry is therefore fundamental in psychiatric education. Although the phenomenological approach may seem contradictory to a taxonomic approach in science, it has been suggested that taxonomy for psychopathology must soundly summarize clinical information but without losing fine-grained details that are relevant for research and treatment (Arseneault, 2021). This ability is difficult to represent or, rather, embody in teaching (Nordgaard et al., 2013).
Embodiment is evolving into a significant paradigm of psychopathology. Furthermore, embodied concepts of mental illness underscore the interconnected interplay among modified subjective experiences, disrupted social interactions, and neurobiological dysfunctions in the progression of the illness (Fuchs and Schlimme, 2009). Role-taking activities involve those who position their bodies in a space and time specific to the psychopathological clinical context. This is evident in its ability to stimulate interactive behavior regulation rooted in social roles, as exemplified by the dynamic between a client and a doctor (Shibuya, 2020). Notably, taking on roles extends to simulation training, where learners immerse themselves in the roles of psychiatric patients or healthcare professionals. This approach has been found to offer a multifaceted understanding of various perspectives within clinical situations, thereby contributing to the embodiment concept (Qureshi et al., 2017). Although there is a growing interest in using virtual reality for educational purposes in psychiatry, there is currently a general lack of evidence supporting which specific virtual reality designs may be effective in supporting taxonomies within psychopathology (Bateman et al., 2013; Kiesewetter et al., 2020). A recent systematic review of virtual patients, including virtual reality, in psychiatry education found that their design primarily focused on specific behavioral learning goals (Jensen et al., 2023). Although these goals included enhancing diagnostic accuracy, developing advisory skills, and promoting positive attitudes toward oneself (such as self-efficacy), they were often fragmented. These studies typically separated learning objectives into knowledge, skills, and attitudes, rather than integrating them into a comprehensive learning scenario. Although having defined learning objectives aligned with specific learning outcomes in virtual patient cases is not inherently problematic, it limits their application in terms of phenomenological sensitivity.
If psychiatry education is to adopt virtual reality as a learning tool, the content must be both scientifically and didactically sound to enrich the intuitive and analytical skills required in the field of psychopathology (Qureshi et al., 2017; Stanghellini, 2017). Furthermore, it must provide depth and perspective to the portrayal of patients to understand their subjective experiences related to their symptoms (Urresti-Gundlach et al., 2017) and stimulate emotional self-awareness to advance students’ learning in the assessment of psychopathology. The phenomenological approach in psychiatry blends natural and social science methodologies, offering a comprehensive understanding of users’ psychological aspects and experiences in clinical, social, and cultural contexts (De Leon, 2014). This perspective has implications for developing virtual reality scenarios by considering individual users’ unique psychological attributes and experiences in conjunction with the clinical, social, and cultural factors that shape them.
In light of this, we propose to adopt a phenomenology-driven approach to the design of virtual reality scenarios for psychiatry education. This approach draws insights from interconnected phenomenologists, directly inspiring the technical and practical aspects of the design. It aims to enhance the intuitive and analytical skills necessary in psychopathology by thoughtfully integrating various facets of mental health and experiences within the virtual reality scenarios. We believe that the integration not only aligns with the theoretical underpinnings but also ensures a holistic and immersive learning experience that resonates with the complex nature of psychiatric practice.
The remainder of the paper is organized as follows: Section 2 begins by exploring the theoretical origins of phenomenology in clinical psychiatry and its potential impact on designing virtual reality applications for improved learning. In Section 3, we present a case study that details how phenomenological considerations influenced the development of a virtual reality scenario, guiding design choices and technical execution. In Section 4, we discuss the practical implementation of this scenario in a classroom setting, using ethnographic observations to highlight its efficient integration. Finally, we thoroughly examine the potential of the scenario in shaping students’ learning experiences, setting the stage for their educational journey in acute psychiatry expertise.
2 Phenomenological insights into psychopathology
The basis of the phenomenological approach presented stems from the theories of three interrelated theorists. First, Karl Jaspers, a German psychiatrist and philosopher, emphasized the role of phenomenology in clinical psychiatry as a hybrid scientific discipline that must combine natural and social science methods with the capacity to understand another person’s thoughts, feelings, and experiences from the first person’s perspective (Jaspers, 1997). Second, Medard Boss, a Swiss psychiatrist and psychoanalyst, developed a form of psychotherapy called “Daseinsanalysis” or analysis of “being there” that aims to help the patient come to an understanding of thrownness (German word: Geworfenheit) into existence (Boss, 1990). Third, Ludwig Binswanger, a Swiss psychiatrist and psychotherapist, developed the concept of “existential analysis” as a method for understanding and treating mental illness. Emphasizing the importance of understanding the patient’s subjective experience, he believed that mental illness should be comprehended within the framework of the individual’s existence (Binswanger, 1958).
2.1 Embodied protagonist: an immersive exploration
Karl Jaspers described clinical psychiatry as the study of inner experience in which the psychiatrist is obliged to recreate and capture the patient’s experience through a process of imaginative variation (Kräupl Taylor, 1967). He addressed various disorders, explaining commonalities in mental illnesses through a flexible approach, recognizing each patient’s uniqueness within their social and cultural context (Jaspers, 1997; De Leon, 2014). Jaspers noted the unique nature of human psychic illness, which introduces a new dimension where the incompleteness, vulnerability, freedom, and infinite possibilities of human beings themselves become causes of illness.
Jaspers’ concept, inspired by the work of the philosopher Edmund Husserl, emphasizes imaginative variation to uncover conscious experience structures (Lindseth and Norberg, 2004). Consciousness, intricately tied to the body and environment, forms a holistic experience (Miron, 2012). Jaspers highlighted three consciousness aspects: being awake, intentional directedness toward objects, and reflective self-awareness (Parnas et al., 2013).
Imaginative variation is crucial in psychiatric education. It enables clinicians to identify universal characteristics by exploring diverse patient realities. Jaspers emphasized that mere observation is insufficient. To grasp the full spectrum of psychic reality, phenomenological interviewers must apply extensive knowledge of normal and abnormal psychology, understanding people’s experiences and their nuances (Jaspers, 1968). However, novices struggle to anticipate patient perspectives, lacking firsthand insight.
In virtual reality, Jaspers’ interconnectedness with the body and subjective perspectives aligns with users’ immersive experiences. Yet, perception of reality is not solely based on laws of physics or objective logics; it is influenced by culture and history (both individual or biographical and societal history), including art and media (Jaspers, 1968). Designing virtual reality scenarios must consider this interplay to capture patients’ subjective realities accurately.
Intertwining Jaspers’ imaginative variation with cinematic and narrative approaches may inspire immersive experiences that depict subjective realities, enriching learners’ understanding of psychopathology. The analogical link between film and dreams has existed since the inception of cinema (Dickson, 2017). Jaspers’ imaginative variation and dreaming share an element of iteration (Zippel, 2016). Film, as a medium, evokes emotions, engages the senses, and creates immersive environments, fostering empathy and connection with characters (Johansen, 2010). Narrative elements in film resonate with personal experiences, creating relatable connections and evoking emotions (Ballon and Molyn, 2007). Narrative structures guide clinical scenario development, exemplified by theories on plot progression (Aristotle, 1987). Cinematic techniques convey meaning and elicit emotional responses (Bordwell, 2006). These techniques could enhance the emotional impact of virtual reality experiences (Pirker and Dengel, 2021), enhancing the portrayal of psychopathological nuances in virtual reality. The authenticity of video captures patient experiences and symptoms more effectively than text or animation-based representations, fostering learner engagement and presence (Courteille, 2008). Contemporary film genres amplify protagonist traits and provide shared experiences, fostering community engagement (Boler, 1999).
Jaspers’ cultural interconnectedness aligns with the communal nature of cinema. Exploring cinematic and narrative elements in a phenomenological approach may inspire immersive learning designs. In virtual reality scenarios, learners should embody the protagonist’s persona, experiencing situations in an embodied way, mirroring the protagonist’s perceptions (Dickson, 2017). Unlike passive film observation, virtual scenarios engage learners’ senses and bodies. Traditional filmmaking often uses over-the-shoulder shots to show a character’s point of view. In virtual reality, the concept of a fixed “point of view” is more complex since viewers have their own perspectives. Learners do not just watch; they experience scenarios intimately from the mind of the “other,” offering an understanding beyond the capabilities of contemporary films.
2.2 Reflecting Dasein through a protagonist’s mind
Medard Boss was concerned with human experience as it is lived. Boss emphasized that being-in-the-world fundamentally establishes knowing as a mode of Dasein, or human existence. The focus is on illuminating details and seemingly trivial aspects within the experience that may be taken for granted in our lives to create meaning and achieve a sense of understanding (Boss, 1990). This emphasis leans on the historicity of not only conceptual understanding but also being situated in the world. Historicity, a person’s history or background, is interwoven with the culture a person is enculturated in and is at hand and handed down, thus presenting ways of understanding the world (Laverty, 2003). Boss’s concept of “thrownness”—the shaping conditions of one’s being—can guide the design of a virtual reality scenario in psychiatry. Daseinsanalysis, delving into individual existence, aligns with the immersive nature of virtual reality. Visual and auditory cues in virtual reality scenarios present the protagonist’s perspective, enhanced with light, movement, and color to focus attention (Vindenes and Wasson, 2021). Integrating sensory elements into virtual reality can enhance Boss’s analysis of “being there,” deepening learners’ connection to others’ experiences. By immersing learners in the protagonist’s “thrownness,” they can gain a deeper connection to the subjective experiences of others. “Virtual Dasein” draws upon the philosophical framework of phenomenology and refers to the concept of virtual existence or being-in-the-world within the context of virtual reality. It emphasizes user agency and exploration, allowing individuals to reflect on their own existence, perception, and engagement within the virtual world, where users can embody themselves within a virtual world in interactive and immersive environments (Varisco, 2007). However, this immersive engagement must be harnessed effectively within a learning context that necessitates reflection and guided learning. To ensure the effectiveness of the learning experience, it is crucial to provide a guiding taxonomy and educational facilitation. In the context of developing new skills within a safe environment, there is a concern that immersive virtual reality can offer users a highly meaningful experience unfettered by the bounds of reality. This detachment from one’s authentic being-in-the-world risks trapping the individual in the safe confines of a virtual world (Haj-bolouri, 2023).
Existential analysis warns against excessive escapism, a risk posed by immersive virtual reality (Siricharoen, 2019). According to existential analysis, escapism can be viewed as a way of evading responsibility, and arguably, this can hit the learner, clinician, and patient. By indulging in distractions or fantasies, individuals avoid acknowledging and confronting their existential anxieties and challenges. Instead of engaging with their authentic selves and exploring their fears, anxieties, and possibilities, they retreat into a comfortable but ultimately unfulfilling state of avoidance (Miron, 2012). This escape may lead individuals to disconnect from their authentic being-in-the-world, hindering their willingness to engage with genuine challenges and impeding their personal growth opportunities. Virtual reality scenarios must carefully balance immersion and authenticity to prevent learners from retreating into a detached virtual world. This educator’s role is essential to not only steer learners away from escapism but also channel their immersive experiences toward constructive reflection and meaningful learning outcomes.
2.3 Scaffolding learning experiences
Ludwig Binswanger and Medard Boss, psychotherapists working in clinical practice, unraveled existential themes in the context of being a person in general and having mental health problems in particular. However, their ideas and concepts could be applied in education and learning contexts by drawing parallels and adapting their insights with implications for educational practices that aim to foster a deeper understanding of oneself and others. Daseinsanalysis, developed by Boss (1977), views the patient’s emotions as integral to the authentic interpersonal relationship with the analyst. This therapeutic method encourages individuals to explore their past, present, and future, scrutinizing the multifaceted influences shaping their lives.
The concept of “antecedent interpretation” involves attributing meaning to an event based on preceding factors. It entails analyzing the context preceding a situation to comprehend it (Needleman, 1963). Phenomenological reduction, through bracketing, suspends preconceived beliefs for a clearer understanding (Tufford and Newman, 2012). It encompasses examining the “lived experience” via intentionality, essence, and phenomenological reduction (Husserl, 2017). Intentionality refers to conscious focus on objects or content, which aligns with the focus of the virtual reality experience. Essences depict relationships with real, remembered, or imagined elements. In Daseinsanalysis, Boss encouraged individuals to explore their being-in-the-world, to engage in self-reflection and interpretation, and to uncover the profound connections between their existence, knowledge, and the world they inhabit.
Scaffolding plays a pivotal role in consolidating students’ understanding of domains which they have previously only encountered through reading or hearing, melding symptomatology and psychopathology knowledge (Hansen et al., 2020; Vercuil et al., 2018). A crucial balance must be struck in utilizing virtual reality as a controlled environment for skill development while encouraging genuine self-confrontation and responsibility in the clinic. Binswanger’s insights guide the creation of psychiatry education scenarios in virtual reality, aiming for a delicate equilibrium between challenging learners’ knowledge, attitudes, and professional identities, without overwhelming them or causing disengagement (Allen Moore and Russell Smith, 2012).
The objective is to prevent an uncontrolled retreat from immersive self-embodiment. The clinical teacher can guide the learner through a structured time framework with a predefined narrative structure in virtual clinical scenarios. This approach enables learners to transition between various modes of presence, fostering a vivid sense of immersion within the unfolding narrative, aligning with the main character’s “Dasein.”
Mirroring the existential analyst’s use of open-ended questions, educators employ similar inquiries to encourage introspection and critical thoughts. Open-ended questions intentionally offer teachers flexibility in addressing various levels of learning taxonomy (Moore and Smith, 2012; Brame, 2015). Just as analysts delve into a patient’s subjective reality, educators unravel students’ perspectives, emotions, and thoughts. These open-ended questions stimulate deep reflection, broaden empathy, and cultivate self-awareness. They also encourage a consideration of societal and contextual influences on personal perspectives.
2.4 Modeling the virtual reality case
In 2020, a group of six teachers in clinical psychiatry, including the first author, recognized the need to better prepare medical students and junior doctors in handling acute psychiatric issues. They envisioned that a virtual reality patient case could offer a learning experience with dual objectives: 1) developing clinical competencies in acute psychiatry and 2) reducing stress and uncertainty when navigating acute psychiatric situations. To describe the clinical scenario, we formulated a set of learning objectives encompassing psychopathology knowledge, clinical reasoning, communication, decision-making, and self-awareness of emotions and reactions.
The virtual reality scenario encompasses two separate scenarios in an acute situation in a psychiatric hospital context highlighting the main characters in each. The first is from the perspective of being a patient with the simulated experience of having a severe psychotic incident, and the second is from the perspective of being a junior doctor, feeling the stress of navigating communication with the patient and staff and insecurity of clinical decision-making.
Our patient, Martin, is a law student who sought to enhance his academic performance by clandestinely using his friend’s attention-deficit/hyperactivity disorder (ADHD) medication. Medications prescribed for ADHD target brain chemicals to improve focus, reduce impulsivity, and increase attention span. On the other hand, we have Cecilie, a doctor in her inaugural year of specialization in general medicine. It is on her very first shift at the psychiatric hospital that our clinical scenario unfolds within the walls of the psychiatric ward. Martin was admitted to the facility after he was found in the children’s room of an unfamiliar apartment, necessitating a police response. He exhibited perplexing behavior that, fortunately, has not harmed anyone. These two unique perspectives converge upon the experience of psychosis, delving deep into the emotions and thoughts that accompany the role of both a doctor and an individual navigating the demanding and often unpredictable clinical situations inherent to treating patients grappling with a psychotic episode (See Figure 1).
FIGURE 1. Protagonist perspectives on the acute event.
The acute psychiatry scenario was carefully crafted to immerse medical professionals and students in a narrative-based learning experience, focusing on a patient in a severe psychotic state. The script followed a narrative structure, embracing a phenomenological approach and cinematic principles. Our aim was to explore the complex experiences and emotions associated with these conditions, providing an insight into the profound challenges of mental illness for both learners and clinicians. Gustav Freytag, a renowned German novelist and dramaturg theoretician, expanded upon Aristotle’s ideas on dramatic plot structure, particularly in tragedy (Aristotle, 1987). Freytag identified five key stages: 1) exposition, 2) rising action, 3) climax, 4) falling action, and 5) resolution (Bucher, 2018). Both Aristotle and Freytag recognized that tragedy explores profound aspects of human existence, often delving into suffering, conflict, and emotional turmoil. In the context of psychiatry, severe psychotic conditions that affect individuals resemble modern-day tragedies, mirroring the emotional and psychological struggles depicted in tragic narratives. Freytag’s five-act structure guided the narrative development of the virtual reality script for the acute clinical scenario (See Figure 2).

FIGURE 2. Narrative scenario structure.
Creating the script scenario was an intricate process within the teacher group. User groups were consulted to fill in gaps in knowledge and add subtle nuances. The script underwent multiple iterations, with the authoring team actively instructing during scenario execution and closely collaborating in post-production. This meticulous approach was instrumental in crafting and utilizing scenarios that not only met but exceeded educational objectives.
2.5 Technical execution
The scenarios were designed to create a 3D effect in high resolution and consistent high framerate, allowing the learner to perceive depth within the scenario. To achieve this effect, two slightly different images were used for each eye. Stitching was employed to seamlessly combine the camera angles, providing a panoramic view that complemented the 180-degree perspective. The decision to limit the scenario to a 180-degree environment served multiple purposes. First, it aimed to keep the engaged learner’s attention focused on specific angles, ensuring a consistent body position in line with the protagonist. This allowed users to turn their heads naturally from side to side to explore the surroundings and points of interest. Furthermore, from a perspective standpoint, the use of a 180-degree environment with “fade-to-black” transitions for each scene served to address the common challenges related to motion sickness-related issues, like dizziness and nausea, often associated with abrupt scene transitions in virtual reality experiences. The virtual reality scenarios were implemented on Pico G2 4K virtual reality headsets, providing “look and choose” selections using side buttons, eliminating the need for controllers and configuring controller functionality.
To provide users with the sensation of inhabiting a body, the actor was filmed in a manner that allowed users to perceive their own virtual body. This encompassed capturing details such as the clothing worn by the characters and their arm and hand movements, thus creating a compelling sense of embodiment. This approach led to a departure from the typical vignette, which often refers to a darker area at the bottom of the user’s field of view where the camera or tripod was positioned during filming to avoid revealing equipment in the shot. In our case, this vignette was pushed further into the background and meticulously adjusted during the stitching process to ensure that the panoramic view remained consistent. The film recordings were entrusted to a specialized firm with expertise in immersive virtual reality storytelling. Their contributions to the production encompassed various crucial roles, including the director, camera operator, lighting director, lighting assistant, sound engineer, runner, and director of imagery. In the post-production phase, they managed special effects, titles, and more. This collaboration was pivotal in bringing the script to life within the confines of our project resources. Filming in an authentic hospital surrounding required significant coordination with the management, staff, and patients in a large hospital building covering four psychiatric specialties and related hospital bed units with approximately 140 beds and outpatient treatment facilities. Certain areas of the hospital, such as hallways and patient wards, needed to be cordoned off for filming. The clinical teachers helped solve this logistical challenge.
Given the extensive setup and intricate effects involved in our production, it was essential to enlist professional actors to ensure the highest level of performance quality. The casting process for key characters, including doctors, patients, and simulating hospital staff, underwent rigorous selection. Eight clinical hospital staff members were also recruited as actors. The resident staff actors, dealing with these situations daily, greatly enhanced the authenticity of the alarm scenarios in the virtual reality experience.
2.6 Special effects in protagonist perception
To achieve the desired stimulus, to fix the learners’ attention and experiences to important story elements, the scenario involved a variety of visual, sound, and 2D animation effects involving sound cues, motion, and visual storytelling to guide the viewer’s gaze and focus on key narrative elements. We placed significant emphasis on spatial audio mixing, which involves creating a 3D sound experience where sounds come from specific directions. We focused on incorporating the protagonist’s own thoughts by using their own voice and slightly dampening background noises when they were thinking or reflecting on the situation. The voice in their thoughts also reflected their state of mind. For instance, when they were feeling fearful or uncertain, their inner voice might manifest in variations in the tempo or pitch of their thoughts, which could differ from the way they communicated with their surroundings. In scenarios where the protagonist’s reactions needed to be highlighted, such as in the case of Martin’s auditory hallucinations, we closely adhered to psychopathological validated definitions (Wing, 2016). We assessed whether it was Martin’s own voice, an external voice, and whether it sounded human or mechanical. Additionally, we worked with auditory hallucinations such as knocking sounds, cat meowing, and camera flashes to emphasize a paranoid state. Martin’s hallucinations were portrayed in line with psychopathological descriptions of how they manifest in acute psychosis. For instance, a loud metallic crash occurred as a graphic set of bars fell down on the hospital window. Martin then saw a menacing demon crawling toward him. The actor playing the demon wore an all-black costume with long black fingers. In post-production, visual effects were added to make the demon appear to move unnaturally, with varying speeds up and down. Furthermore, a trailing haze of smoke and faded black streaks followed its movements.
From the doctor’s perspective, we introduced an innovative “eye-tracking” feature that played a role in a decision-making moment. When users, in the role of Cecilie, focused on specific documents or information in the electronic patient journal interface, a small red dot acted as a cursor linked to their eye movements in which the selected document became more readable. This red dot served as a timer, simulating the time needed to make a selection. This created akin to a real-life scenario where doctors must choose information while interacting with patients. Although the outcome remained unchanged, this interactive element provided users with a sense of control and the illusion of making informed decisions based on available information.
2.7 The didactical utilization
The didactical design was carefully crafted to integrate virtual reality education into a standard curriculum, making it an integral part of learning rather than just an add-on. In practice, our approach aimed to effortlessly fit into a traditional classroom. Since the scenarios did not demand physical control, students could remain seated, just like in a regular classroom session. We aimed for a plug-and-play setup that required minimal technical introduction and did not rely on the internet to avoid connectivity issues. We opted for a linear narrative without branching and physical interactions, eliminating the need for controllers. The videos were directly installed on the headset, and users could access them with just three clicks using the headset’s side button.
Students naturally formed their customary horseshoe arrangement, a common sight in their familiar surroundings. Before each session, virtual reality headsets were neatly prepared and placed at each student’s designated seat as they entered the room. Each session, lasting 2 hours, split evenly between the doctor’s perspective and the patient’s perspective. We accommodated up to 30 students by carefully calculating the number of available headsets. Junior doctors, undergoing specialized psychiatry training, guided the students through this immersive experience.
The instructors began with a quick tutorial on wearing the Pico G2 4K virtual reality headsets and adjusting them for comfort. They provided students an overview of the topic and explained that after each of the five scenes in the virtual scenarios, they would pause for group discussions. During these discussions, students would remove their headsets for reflective conversations. Then, everyone would put their headsets on together to continue the virtual reality journey as a class. The framework deliberately avoided predefined questions, instead encouraging students to share their impressions, experiences, and thoughts and summarize key takeaways. Sample questions included “First impressions?” “What did you experience?” and “What are your thoughts?” This adaptable approach facilitated the exploration of various topics, summarizing key takeaways relevant to acute psychiatry, psychosis, and psychiatry in general.
2.8 Personifying thrownness: unveiling the contextual dimensions
The narrative device was inspired by Gustav Freytag’s notions of narratives applied to the life trajectory of the patient, Martin, and the doctor, Cecilie. Their trajectories lead to the pivotal moment at the psychiatric hospital, captivating the audience as they delve into the trials faced by either the patient or the doctor. Guided by this immersive experience, learners embark on a path of simulated problem-solving, gaining insights into the main character’s world, where themes of suffering, hope, taboo, and meaning intertwine seamlessly.
To provide a concise overview of the main character, the opening scene in scene 1 unfolds through a captivating vignette. Through a series of evocative images narrated by the protagonist, the past and present amalgamate, personifying their journey. Personifying the main characters’ use of photos of their past and current situation, we deliberately wanted to promote the Dasein concept of thrownness, based on the factual information constituting their “being-in-the-world,” meaning that they find themselves in a particular situation or context without having chosen it for themselves (Seinfeld et al., 2022). This is exemplified in the exposition scene drawn from the patient, Martin.
2.9 Psychotic onset
In the patient exposition scene 1, Martin’s ethereal encounters, akin to dreams, play a pivotal role. His aspiration to become a lawyer, encapsulated within his symbolic “dream,” serves to illuminate his motives, immediate circumstances, and, most importantly, his Dasein—his very existence—thus laying the groundwork for the events that follow (See Table 1). In the continuation of scene 1, learners find themselves as Martin sitting in his dormitory in front of his laptop. He appears to be in the writing process of an assignment under the influence of study drugs revealed by the pill blisters on his table. Furthermore, there is what appears to be a snorting trail on the framed picture of his girlfriend Emma, holding a cat. His surroundings appear messy and dirty, and he scratches his skin, seeming to sweep something off his arm. Then he starts exploring Instagram and the account belonging to his former girlfriend, Emma. She smiles in the pictures. Gradually, he experiences the onset of psychosis symptoms in the form of visual hallucinations where his girlfriend suddenly appears visually and out of context walking past the window in a neon yellow dress and his hands becoming more transparent. His reactions and experiences to these symptoms are articulated in his voice appearing as an inner thought that expresses confusion and anxiety and autonomous symptoms accompanied by the sound of increased heartbeat and panting (See Figure 3).
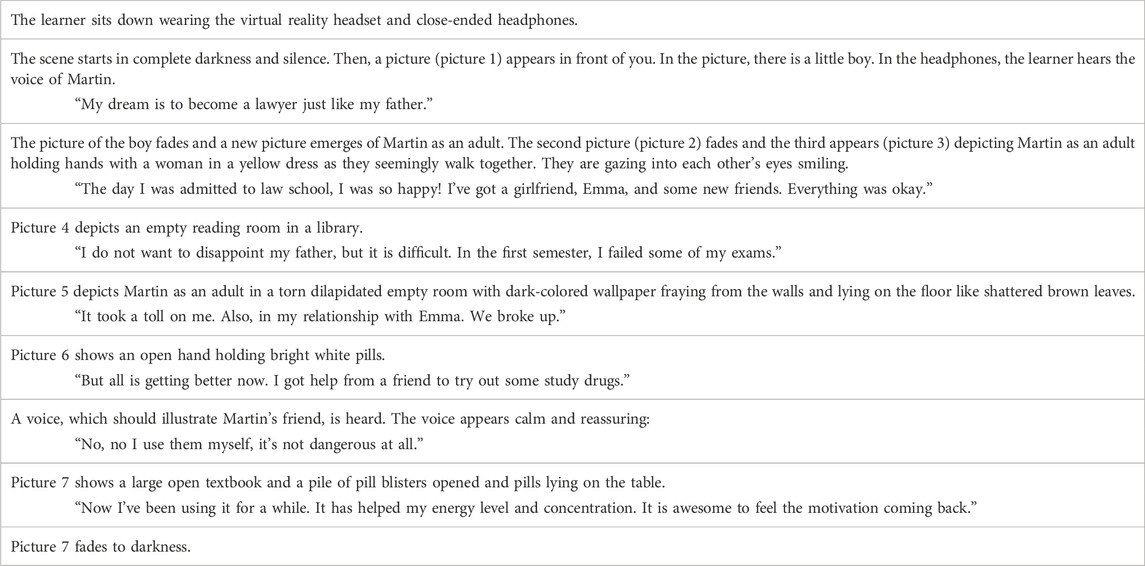
TABLE 1. Excerpt from scene 1, part I.
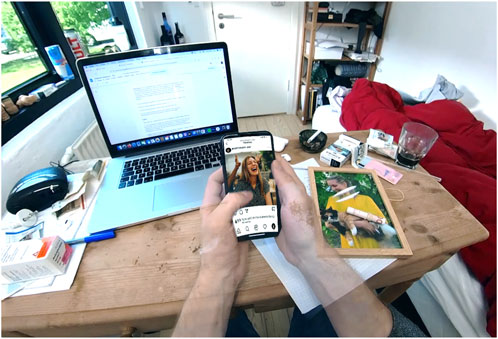
FIGURE 3. Transparent hand hallucination.
2.10 De-realization
As the exposition scene 1 unfolds in, a realization dawns upon the learner—Martin has ventured beyond the confines of his room. A captivating photo collage emerges, depicting his journey along an enigmatic trail through the bustling heart of the city. Amidst the collage, fragmented sounds, images, voices, and disorienting impressions intertwine, mirroring Martin’s profound disorientation in time and space. Images rapidly cut in, propelled by an escalating soundscape—the haunting meow of a cat, an insistent knocking, and the distant wail of a siren—culminating in a crescendo of chaos. Within this visual symphony, two final pictures emerge—a child displaying a wounded spirit, not abused, and the presence of a police car. This evocative sequence captures the kaleidoscope of psychopathologies intertwined with Martin’s psychotic onset, unraveling the complexities of his psychotic experiences.
The visual portrayal of Martin’s escalating psychotic symptoms in this scene draws inspiration from the music video “Smack My Bitch Up” by the English rave group The Prodigy, released in November 1997. Filmed entirely from a first-person’s perspective, the video immerses viewers in a drug-and-alcohol-fueled night out, offering a glimpse into the protagonist’s altered state of mind through various camera movements. This artistic influence adds a captivating dimension to Martin’s journey, further heightening the intensity and authenticity of his distorted perceptions (Vernallis, 2007). First-person narratives can tend toward a stream of consciousness in which the person appears anonymous, as visualized in this scene. However, different from the “Smack My Bitch Up” video, we already knew Martin’s “Dasein” from the prehistory vignette.
In the continuation of scene 2, part III, Martin finds himself admitted at the hospital and experiences a variety of severe psychotic symptoms (See Table 2).
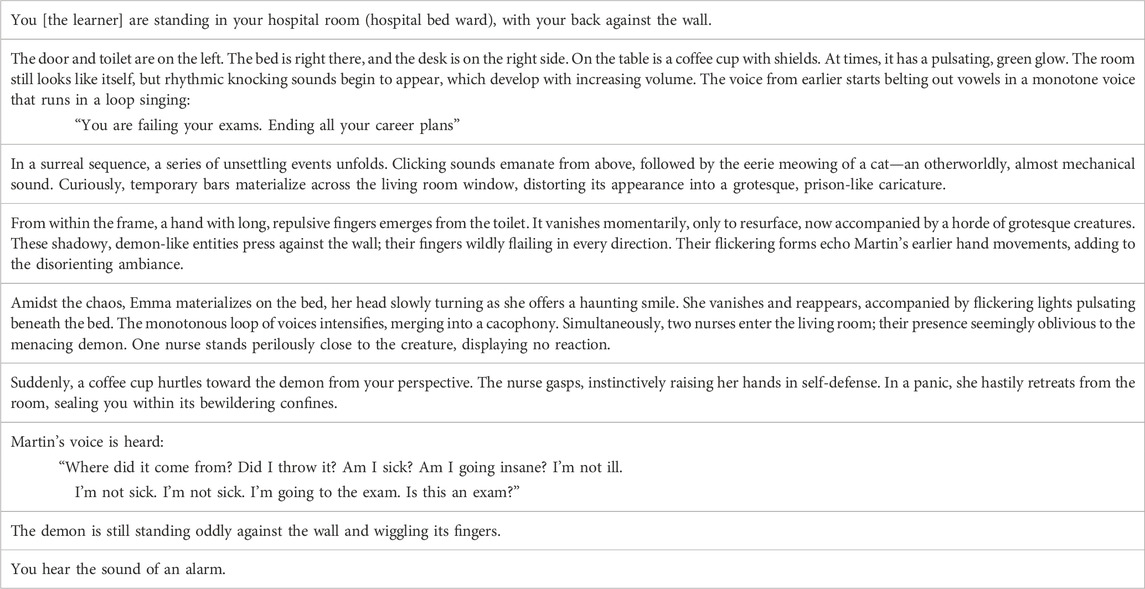
TABLE 2. Excerpt from scene 2, part I.
2.11 Tunnel vision
In the doctor’s exposition scene 1, the student and would-be doctor delves into the world of Dr. Cecilie. Following the photo vignette that provides glimpses into her background—a childhood dream of becoming a doctor, a meaningful experience abroad in a third-world country, and her first shift at the psychiatric hospital—the learners now find themselves experiencing the world through Cecilie’s perspective.
The viewer or aspiring doctor accompanies Dr. Cecilie as she takes a seat on her bed in the hospital’s on-call room. This room serves as a sanctuary for doctors during their shifts, offering a place to rest, recharge, and retreat when not attending to patients. Cecilie’s room is neat and tidy, reflecting both the clinical standards of the hospital and Cecilie’s own psychological needs. It contains the essentials—a bed, a desk, and a computer for documentation.
Suddenly, her alarm jolts her into action. She reads the text message indicating an alarm location, and her reactions and reflections unfold through her internal voice, simulating her anxious attempts to recall previous locations. Overlaying this internal narrative is a visual representation as Cecilie tries to recall the hospital’s layout, mentally mapping out the paths she needs to take, accompanied by automated symptoms such as the sound of her heartbeat rising and panting. The scene fades with the sounds of her rising heartbeat to the next scene in which Cecilie runs down a hospital main hallway.
Cecilie observes the personal staff swiftly passing by her on both sides, their movements appearing faster than her own movements. The main hall stretches out; its dimensions expand as the light and colors morph, blending with the blaring alarm and the rhythmic cadence of staff footsteps (See Figure 4).

FIGURE 4. Portraying the doctor’s tunnel vision.
We visualized the scene from the classic horror film “The Shining” directed by Stanley Kubrick, where the little boy named Danny rides his tricycle through long, empty corridors (Cocks, 2022). The repetitive sound of the running personnel and Cecilie’s panting and heartbeat contribute to the atmosphere of isolation and impending danger, and the use of symmetry and long takes in the scene creates a sense of claustrophobia and disorientation, heightening the viewer’s sense of unease.
2.12 Clash of realities
In the climax action of scene 3, the patient experiences severe distress due to his hallucinations and delusions expressed. This distress is manifested during his interaction with the doctor and the in-ward staff (See Figure 5).

FIGURE 5. Patient and doctor perspective of the climax scene.
We visualized the climax of Martin’s psychotic symptoms, taking inspiration from scenes in the film “Village of the Damned” (1995), a science fiction–horror movie directed by John Carpenter. In the film, blonde-haired children with glowing eyes, of uncertain parentage, possess terrifying powers. The main characters are involuntarily thrust into a quest due to a sudden life-threatening circumstance, where they try to gather information on the incomprehensible and inexplicable. The discovery of the “fiery hypnotic eyes” that can cause harm becomes pivotal to the story. The intense and distressing state that patients may experience during a severe psychotic episode has been likened to the emotions evoked by screen techniques in horror films. Viewers often identify narrative elements that resonate with their personal life experiences and cultural factors depicted in the film, which can induce varying levels of stress or even act as a traumatic experience (Ballon and Molyn, 2007). As Carpenter noted on augmenting terror in his screen techniques, the grotesque manifestations in horror films disregard the impenetrable surface that confines and limits the body as a separate and self-contained entity. The grotesque imagery portrays not only the external appearance but also the inner features of the body, often merging them into a unified whole (Craig, 2005).
In summary, Table 3 captures the intertwining narratives of Martin’s thoughts and the reassuring voice that creates a sense of tension.
TABLE 3. Excerpt from scene 3, part I.
2.13 Turning point
In the culmination of virtual reality scenarios scenes 4 (falling action) and 5 (resolution), a pivotal moment emerges where the patient, once in the throes of severe distress from hallucinations and delusions, appears to reach a state of relative calmness. The voice hallucinations seem more like a silenced whisper, gently just calling the patient’s name “Martin” in the voice of his ex-girlfriend, with no demands. The doctor Cecilie’s assurance that the patient must stay, coupled with the gentle reminder of the potential use of coercion, seems to serve as a turning point. Now, the nursing team takes over, offering the patient an invitation to step outside for a cigarette in the garden. It is a deliberate inconclusive ending, leaving learners with unanswered questions. This calmed transformation may seem evident to rely solely on the clinical intervention. It may involve the empathetic approach from the doctor and the in-ward staff.
While the acute state seems to have resolved, doubts linger regarding the broader clinical context. Which of the underlying issues have truly been solved? What role did the doctor play in this transformation, if any? This open-ended conclusion was designed to encourage learners to reflect on the manifestation of psychosis in patients as well as their role in complex clinical scenarios with the nuances of patient care, where solutions may be elusive and outcomes uncertain.
2.14 Field notes of the teaching sessions
During the introduction to clinical rotations in psychiatry, the virtual reality scenarios were tested in group teaching sessions with fourth-semester medical master students who were in the initial stages of their clerkship rotation at a psychiatric hospital.
The method for data collection was ethnographic observation supplemented by written jottings and notes as inspired by the way of short-term engagement in the field of research exploring cultural norms and phenomena (Andreassen et al., 2020). This approach was preferred over audio recording or video filming as it allowed for a comprehensive understanding of the dynamic interactions taking place within the classroom. Audio recordings could have potentially inhibited students’ willingness to discuss sensitive topics related to their own personal experiences, assumptions, and emotions. Similarly, video recordings may have created a sense of self-consciousness among the participants, impacting the authenticity of their reflections and inhibiting their willingness to openly share, in the otherwise naturally occurring settings and ordinary activities (Hammersley, 2018).
3 Results and responses
A total of 104 students and two teachers participated in the observed sessions.
The utilization of virtual reality technology appeared to work with the straightforward setup. Occasional difficulties in aligning the headset properly were attributed to technical glitches in the devices, which was why an extra 2–3 headsets were available to account for such issues.
The duration of the virtual scenarios was 8 min each, 16 min in total, with the introduction segments of approximately 5 min and left time from the mandatory 2 hours to explore the content, in the shared classroom discussions.
After the instructors had piloted the virtual reality format, they discovered that the most intuitive way to present the scenarios was by initially displaying the doctor’s perspective. The teachers reflected that this order served a dual purpose as many students were potentially entering a psychiatric hospital for the first time. The portrayal of hospital settings helped demystify the surroundings for the students related to preconceptions. Moreover, the initial focus on the doctor’s role with patient observation seemed to prime the students better for the patient scenario and was constructive in advancing taxonomies reflected in discussions. This consideration stemmed from the understanding that students experienced the patient scenario as dramatic and more emotionally charged than the doctor’s scenario, with the potential to overshadow the highlighted professional aspects of psychopathology.
The subsequent sections provide a glimpse into the observed pedagogical influences achieved through this approach. These selected excerpts from the ethnographic notes distinctly illustrate the ways in which the augmented scenes influenced students’ engagement, reflecting their discussion in the classroom session context.
3.1 Dasein in the doctor’s and patient’s mind
Quotes drawn from classroom discussions on the initial exposition scenes leading up to the psychotic onset in Martin’s scenario:
Student: I mirror myself in him. I find that worth remembering. Before they had a normal function.
Student: One can identify with him. He’s like us, going through studies. Exams. Study drugs. All the mess. His study room is quite stereotypical for that.
Student: He also seems self-destructive. He goes on Instagram and looks at her. That must worsen the situation.
Student: I noticed he scratched his skin. Like there is some tactile.
Teacher: We call it coke bugs—slang for tactile hallucinations. The patient feels and maybe sees bugs crawling on his skin.
Quotes drawn from classroom discussions on the initial exposition and rising action scene in Cecilie’s scenario with the transition from the on-call room premises to running though the hallway:
Student: She seemed very nervous. How will she be able to handle the pressure in such a situation when she’s already feeling like that?
Teacher: Being nervous on the first shift can be very natural, regardless of the medical specialty and department.
Student: We did not think she seemed nervous. However, we wondered why she was walking so slowly while everyone else was running.
Student: We’ve learned that the doctor should walk briskly.
Student: Could one perhaps use a running wheel?
Teacher: Yes, that could be an option. However, the doctor has the legal responsibility and needs to lead. One can use the walk to think. One needs to be calm. However, in my first shift as a junior doctor, I admit I also rushed.
3.2 Full range of psychic reality
Quotes drawn from classroom discussions on the climax scenes from the Martin’s and Cecilie’s perspective:
Student: It felt like when you dream, the freaky feeling I recognize that you can’t flee. However, we can close our eyes [in the virtual reality headset]. He cannot.
Student: I thought that when he threw the cup he felt like—it is not me who threw it.
Teachers: What do you think about this?
Student: He asks himself, is this real? It must be so real for him that he is actually in doubt.
Student: I think he was somewhat aware he did it but did not intend it. Must be replacement of will?
Teacher: What does he think about the staff?
Student: Maybe he doesn't even realize they are staff.
Student: I felt it deep in my gut. Seeing Martin from the doctor’s perspective, it looked like he was irrational and aggressive towards me as a doctor, but now I understand that it makes total sense to react the way he does.
Student: Yeah, now it seems awkward the way the staff entered his room and asked: how are you doing, when there’s a fucking spider [reference to the Demon] sitting there.
3.3 Revising antecedent interpretations
Quotes drawn from classroom discussions from the falling action and resolution scenes from the Martin’s and Cecilie’s perspective:
Student: Just before [in the time-experience of the doctor] I thought I would take control of the situation leading him back to his bedroom to talk quietly. But this, including closing the curtains in to shield him from stimuli now seems meaningless.
Teacher: How would you communicate with him?
Student: Maybe ask him what he sees/hears.
Student: But maybe he can't put it into words?
Teacher: We just need to know if he is psychotic. Why is it important for a doctor to know?
Student: Because we are the ones who have to use coercion.
Teacher: Yes, it is us as doctors who must decide and have the legal responsibility if coercion is to be exercised by hospital staff.
4 Discussion
The phenomenology-derived approach to developing patient cases in virtual reality invited us to consider three key elements: transforming clinical data into personalized narratives, creating embodied cinematic experiences, and using existential analysis for scaffolding scenarios.
4.1 Demonized hallucinations
Medard Boss argued that dreams create their own messages. For instance, if someone feels trapped in their waking life, they might experience their feet being locked or immobilized in their dreams (Boss, 1977). This can be understood as an embodied expression of existential dimensions. When someone dreams of being trapped, it can reflect their unconscious anxieties, conflicts, and unresolved issues. It becomes a metaphorical representation of their sense of constraint or limitation in their everyday existence.
Framing Martin’s perspective and including elements that mirror his aspirations and feelings of being trapped, whether by his father’s expectations, the loss of his girlfriend, or the loss of control of his hands, aims to prompt students to contemplate and discuss the factors triggering Martin’s psychotic state. This includes examining the influences that contribute to their clinical reasoning skills.
Students naturally make observations, noting the messy room and Martin’s upcoming exams. However, they go beyond mere observation and interpret the disruption in Martin’s Dasein, not solely attributing it to study drugs (biomedical causality). They give meaning to their observations by considering the impact of exam pressure (sociocultural perspective) and his emotional state following his breakup with his girlfriend (existential perspective). Prescription stimulants, also referred to as “study drugs,” are known to be used by students to help them focus or stay awake to enhance academic performance, with a risk of negative side effects on physical and mental health, including psychosis (Abelman, 2017). Contemporary failings of prohibitionist policies to reduce consumption in students are reflected in the voice of Martin’s friend, justifying the use of study drugs being harmless (Desantis and Hane, 2010). According to Boss, Dasein events are crucial moments that can disrupt an individual’s everyday existence, profoundly impacting their subjective experience and understanding of themselves and the world. In the case of Martin, the disruption of his Dasein due to the onset of psychosis is designed to actively engage students in learning experiences that challenge their existing hypotheses. Martin’s drug use is not explicitly presented as the clear trigger for the psychotic event. The aim is to encourage critical reflection rather than establish a predefined clinical causal explanation for his experiences. While there might be an apparent connection, leaving it open for interpretation and discussion allows for a more comprehensive exploration. Understanding their own preconceptions enables learners to project insights into aspects of Martin’s “Dasein,” encouraging critical reflection on their own assumptions that might otherwise remain implicit.
Students were found to refer to psychopathology, not by the abstracted clinical definition, but in context to the patients’ concrete experience. For example, replacement of will refers to a psychopathological explanation of a psychotic experience that one’s movements or actions are imposed by a foreign will, as Martin experienced when a coffee cup is thrown encountering a demon during his hallucinatory state. This demonstrates for the students that Martin’s psychotic symptoms are part of his Dasein and cannot be excluded from his subjective experience of his present situation as a whole.
4.2 Disturbance of tidiness
Taking a phenomenological perspective, we hypothesize that learners’ perception of the orderly surroundings in the doctor’s scenario evokes an underlying sense of eeriness, reflecting psychological disturbance. The tidy environment sets the stage for an unconscious expectation of disruption. Simulating the doctor’s heightened senses draws her into a state of “tunnel vision,” amplifying her focus and anticipation for the unknown ahead, fueled by adrenaline. Both Jaspers and Boss explored the significance of tidiness in relation to patients’ psychology, potentially signaling underlying disturbances with existential implications (Miron, 2012). Learners may unconsciously reflect on witnessing the tidiness and subsequent alarm, examining the motives and fears behind these events. Boss guided learners to delve into existential themes, like their relationship with the environment, feelings of security, and existential anxieties triggered by a disrupted calm setting. This contrast between order and sudden alarm aims to stimulate anticipation or anxiety, encouraging learners to explore deeper emotional responses. Structuring a narrative where clinicians’ actions are deliberately portrayed as less than optimal, contradictory, or even incorrect challenges and encourages students to think, reflect, and discuss (Turner, 1966; Priyadharshini, 2012).
Constructing an enriched narrative centered on the physical presence of the patient and clinician, with Cecilie’s actions deliberately depicted as suboptimal, contradictory, or even incorrect, aims to puzzle or even provoke the students intentionally, with the purpose of challenging and motivating them to think, reflect, and engage in discussions (Turner, 1966; Priyadharshini, 2012).
From Jaspers’ perspective, the visual and auditory hallucinations experienced by Martin are crucial for understanding his condition and would emphasize the need to explore Martin’s subjective experience further to gain a deeper understanding of his condition. However, as the teachers note, in acute situations, the optimal approach is to prioritize calming the patient in order to prevent further escalation of the situation. A calm demeanor, use of clear language, and sustained eye contact can effectively de-escalate the situation and alleviate the patient’s anxiety or aggression (Bowers et al., 2015). The teacher emphasizes that, in the acute situation, the priority is not to thoroughly examine and map the patient’s psychotic symptoms in their tormented state. Instead, the focus is on confirming their presence and making an informed clinical decision, which may involve coercion for the safety of both the patient and staff.
We found that Daseinsanalysis offers a valuable framework for shaping the professional identity of aspiring therapists, psychiatrists, and other mental health practitioners by exploring how trainees balance their presence in the hospital with their knowledge of psychiatry. The patient’s distress and alienation affect both the novice clinician and the patient themselves, making it crucial to understand the patient’s unique perspective and the reasons behind their behavior, with virtual reality aiding in this understanding. Through this reflection and curious questioning in a dynamic discussion with the teacher, the teacher can draw on his or her experience to provide the student with a deeper understanding of the potential impact of stress on their future practice. This experience immerses the learners in Cecilie’s mindset, allowing them to understand the challenges and complexities she faces as she navigates her duties in the hospital. By reflecting on how the scene affected them personally, students can gain self-awareness of their own reactions and coping mechanisms in stressful situations.
The virtual scenario in this study helped students recognize that the patient’s apparent lack of response or their seemingly irrational thoughts are manifestations of their internal struggles. This may involve employing alternative modes of communication or exploring creative therapeutic approaches to establish a connection (Scholl et al., 2014). The teachers’ didactic scaffolding of the virtual scenarios is vital to create a safe space, providing guidance and support for students to express their experiences in understanding and grappling with these learning experiences (Davis and Weeden, 2009). The variation in experiences during clerkship, influenced by factors such as hospital department and access to supervisor resources, highlights the importance of teacher guidance in group sessions (Liljedahl, 2009). The phenomenological approach to design and scaffold virtual reality as such complements the unique experiences encountered by medical students during their clerkship.
In our phenomenological approach, we adapted film-inspired visuals as a mean to bridge the gap between theoretical knowledge and experiential understanding, fostering empathy and facilitating discussions on the complexities of psychotic symptoms within the framework of Daseinsanalysis. Our intention in integrating visual techniques was to capture the feelings of despair, danger, and the distorted perception of reality often associated with individuals in severe psychotic states (Ballon and Molyn, 2007). These scenes provided deeper insights, encouraging students to consider various factors contributing to a patient’s condition. This approach aligns with Jasper’s emphasis on understanding subjective patient perspectives, promoting empathy, and facilitating discussions about the intricate nature of psychotic symptoms, all within the framework of Daseinsanalysis by Boss or existential analysis by Binswanger. The cinematic techniques served as a valuable tool for deepening the comprehension of psychosis within the educational context. By leveraging the techniques and principles of art, educators can craft virtual reality experiences that are not only engaging but also profoundly impactful in enhancing the learning process.
Such an approach invites us to explore the relationship between our holding on, letting go, and building of a new relationship with the physical as well as social environment. Virtual reality becomes the foreground to the background or contexts in which we provide care. By immersing ourselves in virtual environments that simulate clinical scenarios, we can deepen our understanding of the subjective experiences of patients and gain insights into their struggles and aspirations. This approach not only enriches our professional identity but also enables us to connect with patients on a deeper level, facilitating meaningful therapeutic engagements.
4.3 Practical implications
The influence on students’ professional learning within the scope of our virtual reality scenarios is a critical aspect to consider. In clinical training, fostering independence and clinical responsibility is deemed important for students’ competency development (Sher and New, 2016; Gentles, 2017). However, understanding how students perceive and interpret contradictions in their learning process is a complex internal process. Teachers must actively elicit information about students’ existing conceptions and viewpoints, recognizing that a challenge only exists if students perceive it as a contradiction (Davis and Weeden, 2009).
In virtual reality scenarios, clinical educators can tap into the expressive power of not only perceptive elements such as visuals and sound but also human storytelling. This is more than techniques and contributes to an environment laden with choices and dilemmas of whether they are successfully solved, foster emotional engagement, and enhance the overall educational impact. However, in the context of psychiatry education, educators must carefully choose content and cinematic effects to align with learning objectives and evoke appropriate emotions without veering off track (Pedersen, 2021).
We believe that the cinematic techniques adapted to the didactic framework in virtual reality allow students to augment Jasper’s attentiveness to the subjective patient perspectives, facilitating discussions on the complexities of psychopathology and bridging the exiting gaps between biomedical, sociocultural, and existential perspectives in psychiatry education. In the context of virtual reality for education, careful arguments must be made for the artistic selection and de-selection of cinematic effects. It is crucial to ensure that these artistic choices do not derail or misconstrue the intended learning objectives. Instead, they should be thoughtfully integrated to enhance the educational content and evoke appropriate emotional responses that deepen the learning experience.
5 Limitations and future perspectives
While the method of observing group sessions offered valuable insights into the students’ engagement with the virtual reality scenarios and their subsequent reflections, it is important to recognize the limitations inherent in solely relying on this approach. One notable limitation was the absence of interviews or direct interactions with the participants. By conducting interviews, we could have delved deeper into the students’ individual experiences, thoughts, and emotions pertaining to the virtual reality scenarios and their comprehension of Dasein and existential analysis. However, it is crucial to note that the primary objective of the study was not to collect detailed individual accounts or subjective perspectives, but rather to speculate on the broader impact of the virtual reality scenarios on students’ reflections and understanding within a group setting. The observation aimed to explore the virtual reality format’s capacity to facilitate collective learning experiences and influence classroom dynamics, rather than focusing on individual interviews or personal accounts.
Nonetheless, future research endeavors could consider integrating interviews or other qualitative methods to complement the observations and obtain a more comprehensive understanding of the students’ individual experiences and perspectives. This would enable a more nuanced exploration of the influence of the virtual reality scenarios on their learning and reflections, specifically in relation to Dasein and existential analysis in psychiatry.
We also acknowledge the limitations of our method as we employed a convenience sample of students. Therefore, in terms of external validity, we cannot ascertain the extent to which our study findings would apply to other settings. The detailed description of our considerations in the virtual reality design enables the reader to assess the potential transferability of our hypothesis. Although the project’s original goal was to support medical education, the phenomenological approach framework that guided the virtual reality design is relevant to psychiatry education and training across various professions regardless of experience and educational level. This opens up avenues for further research on our virtual reality format beyond medical education.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any identifiable images or data included in this article.
Author contributions
KP: conceptualization, formal analysis, investigation, methodology, visualization, writing–original draft, and writing–review and editing. PM: conceptualization, formal analysis, methodology, visualization, writing–original draft, and writing–review and editing.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abelman, D. D. (2017). Mitigating risks of students use of study drugs through understanding motivations for use and applying harm reduction theory: A literature review. Harm Reduct. J. 14, 68–77. doi:10.1186/s12954-017-0194-6
Allen Moore, W., and Russell Smith, A. (2012). Effects of video podcasting on psychomotor and cognitive performance, attitudes and study behaviour of student physical therapists. Innovations Educ. Teach. Int. 49 (4), 401–414. doi:10.1080/14703297.2012.728876
Anderson, L. W., et al. (2001). A taxonomy for learning, teaching and assessing. 1st edn., New York, NY, USA: Longman.
Andreassen, P., Christensen, M. K., and Møller, J. E. (2020). Focused ethnography as an approach in medical education research’, Medical Education 54 (4), 296–302. doi:10.1111/medu.14045
Aristotle, (1987). “Poetics,” in R. Janko. Indianapolis. 3rd edn. (Cambridge, UK: Hackett Publishing Company).
Arseneault, L. (2021). Taxonomy of psychopathology: A work in progress and a call for interdisciplinary research. World Psychiatry 20 (1), 73–74. doi:10.1002/wps.20817
Ballon, B., and Molyn, L. (2007). Horror films: tales to master terror or shapers of trauma? Am. J. Psychotherapy 61 (2), 211–230. doi:10.1176/appi.psychotherapy.2007.61.2.211
Baniasadi, T., Ayyoubzadeh, S. M., and Mohammadzadeh, N. (2020). Challenges and practical considerations in applying virtual reality in medical education and treatment. Oman Med. J. 35 (3), 1255–e210. doi:10.5001/omj.2020.43
Baron, D., et al. (2009). “Healing and the physician,” in Psychiatry and behavioral science - an introduction and study guide for medical students (Philadelphia, PA, USA: Temple University Press), 191–263.
Bateman, J., Allen, M., Samani, D., Kidd, J., and Davies, D. (2013). Virtual patient design: exploring what works and why. a grounded theory study. Med. Educ. 47 (6), 595–606. doi:10.1111/medu.12151
Belitsky, C., and Kenny, S. H. (1995). Transition to psychiatric residency: unique stresses; unique rewards. Jefferson J. Psychiatry 12 (2), 37–46. doi:10.29046/jjp.012.2.004
Binswanger, L. (1958). “The existential analysis school of thought,” in Existence: A new dimension in psychiatry and psychology. Editor E. Angel (New York, NY, USA: Brill), 191–213. doi:10.1037/11321-007
Bordwell, D. (2006). The way hollywood tells it. 1st edn., California, CA, USA: University of California Press.
Boss, M. (1990). Daseinsanalytische bemerkungen zum wesen der Freudschen psychoanalyse. Daseinsanalyse 7, 167–173. doi:10.1159/000456301
Boss, M. (1977). Dreaming and the dreamed in the daseinsanalytical way of seeing. Sound. Interdiscip. J. 60 (3), 235–263.
Bowers, L., James, K., Quirk, A., Simpson, A., Stewart, D., and Hodsoll, J. (2015). Reducing conflict and containment rates on acute psychiatric wards: the safewards cluster randomised controlled trial. Int. J. Nurs. Stud. 52 (9), 1412–1422. doi:10.1016/j.ijnurstu.2015.05.001
Bowers, L., Simpson, A., Alexander, J., Hackney, D., Nijman, H., Grange, A., et al. (2005). The nature and purpose of acute psychiatric wards: the tompkins acute ward study. J. Ment. Health 14 (6), 625–635. doi:10.1080/09638230500389105
Bucher, J. (2018). Methods and princliples for crafting immersive narratives. 1st edn., New York, NY, USA: Taylor & Francis.Storytelling for virtual reality
Bula, T. (2012). Place presence, social presence, co-presence, and satisfaction in virtual worlds. Comput. Educ. 58 (1), 154–161. doi:10.1016/j.compedu.2011.08.024
Cheung, J. J. H., Kulasegaram, K. M., Woods, N. N., Moulton, C. a., Ringsted, C. V., and Brydges, R. (2018). Knowing how and knowing why: testing the effect of instruction designed for cognitive integration on procedural skills transfer. Adv. Health Sci. Educ. 23 (1), 61–74. doi:10.1007/s10459-017-9774-1
Cocks, G. (2022) ‘Stanley kubrick’s magic mountain: fiction as history in the shining’, Cent. Eur. Hist., 55(4), pp. 528–550. doi:10.1017/S0008938921001448
Courteille, O. (2008). Computer simulations of the clinical encounter. Perceptions and emotional aspects. Solna, Sweden: Karolinska Institutet.
Craig, J. R. (2005). The cinema of John carpenter: The technique of terror. New York, NY, USA: Wallflower Press.
Davis, K. W., and Weeden, S. R. (2009). Teacher as trickster on the learner’s journey. J. Scholarsh. Teach. Learn. 9 (2), 70–81.
De Leon, J. (2014). One hundred years of limited impact of jaspers’ general psychopathology on us psychiatry. J. Nerv. Ment. Dis. 202 (2), 79–87. doi:10.1097/NMD.0000000000000092
Desantis, A. D., and Hane, A. C. (2010). “Adderall is definitely not a drug”: justifications for the illegal use of ADHD stimulants. Subst. Use \& Misuse 45 (1–2), 31–46. doi:10.3109/10826080902858334
Dickson, S. (2017). The oneiric film: Refocusing the film–dream analogy from an existential phenomenological perspective. MA Thesis. London, England: University of London.
Edelbring, S., Dastmalchi, M., Hult, H., Lundberg, I. E., and Dahlgren, L. O. (2011). Experiencing virtual patients in clinical learning: A phenomenological study. Adv. Health Sci. Educ. 16 (3), 331–345. doi:10.1007/s10459-010-9265-0
Engel, K. G., Pedersen, K., Johansen, M. D., Schoennemann, K. R., Kjaer, L. B., and Nayahangan, L. J. (2022). Consensus on communication curriculum content in Danish undergraduate medical education: A delphi study. Med. Teach. 44 (11), 1221–1227. doi:10.1080/0142159X.2022.2072280
Formosa, N. J., Morrison, B. W., Hill, G., and Stone, D. (2018). Testing the efficacy of a virtual reality-based simulation in enhancing users’ knowledge, attitudes, and empathy relating to psychosis. Aust. J. Psychol. 70 (1), 57–65. doi:10.1111/ajpy.12167
Foster, C., Bowers, L., and Nijman, H. (2007). Aggressive behaviour on acute psychiatric wards: prevalence, severity and management. J. Adv. Nurs. 58 (2), 140–149. doi:10.1111/j.1365-2648.2007.04169.x
Fuchs, T. (2013). One century of Karl Jaspers psychopathology. (Oxford, England: Oxford University Press). doi:10.1093/med/9780199609253.001.0001
Fuchs, T., and Schlimme, J. E. (2009). Embodiment and psychopathology: A phenomenological perspective. Curr. Opin. Psychiatry 22 (6), 570–575. doi:10.1097/YCO.0b013e3283318e5c
Gask, L., Coskun, B., and Baron, D. A. (2011). Teaching psychiatry: Putting theory into practice. Oxford, England: John Wiley & Sons.
Gerup, J., Soerensen, C. B., and Dieckmann, P. (2020). Augmented reality and mixed reality for healthcare education beyond surgery: an integrative review. Int. J. Med. Educ. 11, 1–18. doi:10.5116/ijme.5e01.eb1a
Goldberg, J. L., McKeever, P., and Abbey, S. (2008). Humanism or professionalism? The white coat ceremony and medical education. Acad. Med. J. Assoc. Am. Med. Coll. 83 (8), 715–722. doi:10.1097/ACM.0b013e31817eba30
Graafland, M., Schraagen, J. M., and Schijven, M. P. (2012). Systematic review of serious games for medical education and surgical skills training. Br. J. Surg. 99 (10), 1322–1330. doi:10.1002/bjs.8819
Haj-bolouri, A. (2023). The experience of immersive virtual reality: A phenomenology inspired inquiry. Commun. Assoc. Inf. Syst. 52, 782–814. doi:10.17705/1cais.05238
Hammersley, M. (2018). What is ethnography? Can it survive? Should it? Ethnogr. Educ. 13 (1), 1–17. doi:10.1080/17457823.2017.1298458
Ho, J. C. F., and Ng, R. (2022). Perspective-taking of non-player characters in prosocial virtual reality games: effects on closeness, empathy, and game immersion. Behav. Inf. Technol. 41 (6), 1185–1198. doi:10.1080/0144929X.2020.1864018
Irarrázaval, L., and Kalawski, J. P. (2022). Phenomenological considerations on empathy and emotions in psychotherapy. Front. Psychol. 13, 1000059–9. doi:10.3389/fpsyg.2022.1000059
Jaspers, K. (1997). General psychopathology. 1st edn., Baltimore, Maryland, United States: Johns Hopkins University Press.
Jaspers, K. (1968). The phenomenological approach in psychopathology. Br. J. psychiatry J. Ment. Sci. 114 (516), 1313–1323. doi:10.1192/bjp.114.516.1313
Jensen, R. A. A., Musaeus, P., and Pedersen, K. (2023). Virtual patients in undergraduate psychiatry education: A systematic review and synthesis. Adv. health Sci. Educ. theory Pract., 0123456789. doi:10.1007/s10459-023-10247-6
Johansen, J. D. (2010). Feelings in literature. Integr. Psychol. Behav. Sci. 44 (3), 185–196. doi:10.1007/s12124-009-9112-0
Kallivayalil, R. (2012). The importance of psychiatry in undergraduate medical education in India. Indian J. Psychiatry 54 (3), 208. doi:10.4103/0019-5545.102336
Kampa, A., Burelli, P., and Haake, S. (2016) ‘Storytelling in serious games’, in R. Dörner, S. Göbel, M. Kickmeier-Rust, M. Masuch, and K. Zweig Entertainment computing and serious games. 1st edn. Springer, Berlin, Germany, doi:10.1007/978-3-319-46152-6
Kegel, L. C., Brugger, P., Frühholz, S., Grunwald, T., Hilfiker, P., Kohnen, O., et al. (2020). Dynamic human and avatar facial expressions elicit differential brain responses. Soc. Cognitive Affect. Neurosci. 15 (3), 303–317. doi:10.1093/scan/nsaa039
Kenny, P., et al. (2008). Virtual justina: A PTSD virtual patient for clinical classroom training. Annu. Rev. CyberTherapy Telemedicine 6 (1), 113–118. doi:10.1007/978-3-540-85483-8_40
Kiesewetter, J., Sailer, M., Jung, V. M., Schönberger, R., Bauer, E., Zottmann, J. M., et al. (2020). Learning clinical reasoning: how virtual patient case format and prior knowledge interact. BMC Med. Educ. 20, 73–10. doi:10.1186/s12909-020-1987-y
Kräupl Taylor, F. (1967). The role of phenomenology in psychiatry. Br. J. psychiatry J. Ment. Sci. 113 (500), 765–770. doi:10.1192/bjp.113.500.765
Kurtz, S., Silverman, J., Benson, J., and Draper, J. (2003). Marrying content and process in clinical method teaching: enhancing the calgary-cambridge guides. Acad. Med. J. Assoc. Am. Med. Coll. 78 (8), 802–809. doi:10.1097/00001888-200308000-00011
Lam, J. T., Gutierrez, M. A., Goad, J. A., Odessky, L., and Bock, J. (2019). Use of virtual games for interactive learning in a pharmacy curriculum. Curr. Pharm. Teach. Learn. 11 (1), 51–57. doi:10.1016/j.cptl.2018.09.012
Laverty, S. M. (2003). Hermeneutic phenomenology and phenomenology: A comparison of historical and methodological considerations. Int. J. Qual. Methods 2 (3), 21–35. doi:10.1177/160940690300200303
Lewis, A. (2013). The state of psychiatry (psychology revivals): Essays and addresses. London: Routledge.
Libera, C. D., et al. (2021). Using 360 ° immersive videos to assess paranoia in a non-clinical population clinical population. Boca Raton, Florida, United States: Taylor & Francis. doi:10.1080/13546805.2021.1956885
Liljedahl, M. (2009). Learning in the clinical environment. Med. Teach., doi:10.1080/01421590902744936
Lindseth, A., and Norberg, A. (2004). A phenomenological hermeneutical method for researching lived experience. Scand. J. Caring Sci. 18, 145–153. doi:10.1111/j.1471-6712.2004.00258.x
Makhkamova, A., (2019). “Towards a taxonomy of virtual reality usage in education: A systematic review,” in Augmented reality and virtual reality Changing realities in a dynamic world, (Berlin, Germany, Springer)
Meyer, J. H. F., and Land, R. (2005). Threshold concepts and troublesome knowledge (2): epistemological considerations and a conceptual framework for teaching and learning. High. Educ. 49 (3), 373–388. doi:10.1007/s10734-004-6779-5
Miron, R. (2012). Karl Jaspers: From selfhood to being. Leiden, Netherlands: Brill. doi:10.1163/9789401208062
Nicholls, D., Gaynor, N., Shafiei, T., Bosanac, P., and Farrell, G. (2011). Mental health nursing in emergency departments: the case for a nurse practitioner role. J. Clin. Nurs. 20, 530–536. doi:10.1111/j.1365-2702.2010.03504.x
Nordgaard, J., and Parnas, J. (2013). A haunting that never stops: psychiatry’s problem of description. Acta Psychiatr. Scand. 127 (6), 434–435. doi:10.1111/acps.12092
Nordgaard, J., Sass, L. A., and Parnas, J. (2013). The psychiatric interview: validity, structure, and subjectivity. Eur. archives psychiatry Clin. Neurosci. 263 (4), 353–364. doi:10.1007/s00406-012-0366-z
Nordt, C., Rössler, W., and Lauber, C. (2006). Attitudes of mental health professionals toward people with schizophrenia and major depression. Schizophr. Bull. 32 (4), 709–714. doi:10.1093/schbul/sbj065
Parnas, J., Sass, L. A., and Zahavi, D. (2013). Rediscovering psychopathology: the epistemology and phenomenology of the psychiatric object. Schizophr. Bull. 39 (2), 270–277. doi:10.1093/schbul/sbs153
Parong, J., and Mayer, R. E. (2018). Learning science in immersive virtual reality. J. Educ. Psychol. 110 (6), 785–797. doi:10.1037/edu0000241
Pedersen, K., Moercke, A. M., Paltved, C., Mors, O., and Ringsted, C. (2021). Video cases as tricksters, in medical students´ transition to psychiatric clerkship. A liminal perspective. MedEdPublish 10 (1), 1–15. doi:10.15694/mep.2021.000095.1
Pedersen, K. (2021). Psychiatric lecture ignited by (electro) shocks. Humanist. Psychiatry 9 (2), 2325–9485.
Pirker, J., and Dengel, A. (2021). The potential of 360° virtual reality videos and real VR for education - a literature review. IEEE Comput. Graph. Appl. 41, 76–89. doi:10.1109/MCG.2021.3067999
Pomata, G. (2014). The medical case narrative: distant reading of an epistemic genre. Literature Med. 32 (1), 1–23. doi:10.1353/lm.2014.0010
Priebe, S., Dimic, S., Wildgrube, C., Jankovic, J., Cushing, A., and McCabe, R. (2011). Good communication in psychiatry – A conceptual review. Eur. Psychiatry 26 (7), 403–407. doi:10.1016/j.eurpsy.2010.07.010
Priyadharshini, E. (2012). Thinking with trickster: sporadic illuminations for educational research. Camb. J. Educ. 42 (4), 547–561. doi:10.1080/0305764X.2012.733344
Qureshi, A., Kwok, Y., Chaudhary, Z., Leung, F. H., Mylopoulos, M., and Sockalingam, S. (2017). A simulation to teach integrated care in undergraduate medical education: the getting to know patients system of care (GPS-CARE) experience. Acad. Psychiatry 41 (4), 533–537. doi:10.1007/s40596-016-0657-1
Ramirez, E. J., Elliott, M., and Milam, P. E. (2021). What it’s like to be a _____: why it’s (often) unethical to use VR as an empathy nudging tool. Ethics Inf. Technol. 23 (3), 527–542. doi:10.1007/s10676-021-09594-y
Rapuano, M., Iachini, T., and Ruggiero, G. (2023). Interaction with virtual humans and effect of emotional expressions: anger matters. J. Clin. Med. 12 (4), 1339. doi:10.3390/jcm12041339
Regenbrecht, H., and Schubert, T. (2023). Designing for presence: Embodied interaction in computer-mediated realities. doi:10.31234/osf.io/cyw23
Sanati, A. (2020). An exploration of psychopathology for clinical practice. BJPsych Adv. 26 (5), 296–298. doi:10.1192/bja.2020.37
Scholl, I., Zill, J. M., Härter, M., and Dirmaier, J. (2014). An integrative model of patient-centeredness – a systematic review and concept analysis. PLoS ONE 9 (9), e107828. doi:10.1371/journal.pone.0107828
Seinfeld, S., Hasler, B. S., Banakou, D., and Levy, J. (2022). Editorial: virtual reality and empathy. Front. Psychol. 21. doi:10.3389/fpsyg.2022.1089006
Shibuya, K. (2020). Digital transformation of identity in the age of artificial intelligence. Berlin, Germany: Springer. doi:10.1007/978-981-15-2248-2
Siricharoen, W. V. (2019). The effect of virtual reality as a form of escapism. Available at: https://aisel.aisnet.org/confirm2019.
Slater, M., et al. (2009). How we experience immersive virtual environments: the concept of presence and its measurement *. Anu. Psicol. 40 (2), 193–210.
Sora-Domenjó, C. (2022). Disrupting the “empathy machine”: the power and perils of virtual reality in addressing social issues. Front. Psychol. 13, 814565–814613. doi:10.3389/fpsyg.2022.814565
Stanghellini, G. (2017). Lost in dialogue: Anthropology, psychopathology, and care (international perspectives in philosophy and psychiatry). 1st edn., Oxford, England: Oxford University Press.
Tazakori, Z., Hashempour, Z., Molavi, P., and Karimollahi, M. (2008). Unexpected stressful experiences in transition from medical student to junior doctor in Ardabil medical sciences university centers and affiliated hospitals 2005. Ann. General Psychiatry 7 (1), S309. doi:10.1186/1744-859X-7-S1-S309
Tufford, L., and Newman, P. (2012). Bracketing in qualitative research. Qual. Soc. Work 11 (1), 80–96. doi:10.1177/1473325010368316
Turner, V. (1966). The ritual process, the ritual process: Structure and antistructure. Ithaca, New York, NY, USA: Cornell University Press.
Urresti-Gundlach, M., Tolks, D., Kiessling, C., Wagner-Menghin, M., Härtl, A., and Hege, I. (2017). Do virtual patients prepare medical students for the real world? Development and application of a framework to compare a virtual patient collection with population data. BMC Med. Educ. 17 (1), 174–177. doi:10.1186/s12909-017-1013-1
Varisco, D. (2007). Virtual Dasein: ethnography in cyberspace. CyberOrient 2 (1), 26–45. doi:10.1002/j.cyo2.20100201.0002
Ventura, S., Badenes-Ribera, L., Herrero, R., Cebolla, A., Galiana, L., and Baños, R. (2020). Virtual reality as a medium to elicit empathy: A meta-analysis. Cyberpsychology, Behav. Soc. Netw. 23 (10), 667–676. doi:10.1089/cyber.2019.0681
Vernallis, C. (2007). “Strange people, weird objects,” in Medium cool. Editors R. Beebe, and J. Middleton (Durham, North Carolina, United States: Duke University Press Music Videos from Soundies to Cellphones), 111–151. doi:10.2307/j.ctv123x5x2.8
Vindenes, J., and Wasson, B. (2021). A postphenomenological framework for studying user experience of immersive virtual reality. Front. Virtual Real. 2, 1–15. doi:10.3389/frvir.2021.656423
Wijma, E. M., Veerbeek, M. A., Prins, M., Pot, A. M., and Willemse, B. M. (2018). A virtual reality intervention to improve the understanding and empathy for people with dementia in informal caregivers: results of a pilot study. Aging Ment. Health 22 (9), 1121–1129. doi:10.1080/13607863.2017.1348470
Wing, J. K. (2016). The SCAN Glossary and principles of the interview. Diagnosis Clin. Meas. Psychiatry, 36–43. doi:10.1017/cbo9780511666445.005
Woolley, N. N., and Jarvis, Y. (2007). Situated cognition and cognitive apprenticeship: A model for teaching and learning clinical skills in a technologically rich and authentic learning environment. Nurse Educ. Today 27 (1), 73–79. doi:10.1016/j.nedt.2006.02.010
Yakeley, J., Hale, R., Johnston, J., Kirtchuk, G., and Shoenberg, P. (2014). Psychiatry, subjectivity and emotion - deepening the medical model. psychiatric Bull. 38 (3), 97–101. doi:10.1192/pb.bp.113.045260
Keywords: virtual reality, phenomenology, psychiatry education, psychosis, psychopathology
Citation: Pedersen K and Musaeus P (2023) A phenomenological approach to virtual reality in psychiatry education. Front. Virtual Real. 4:1259263. doi: 10.3389/frvir.2023.1259263
Received: 15 July 2023; Accepted: 25 September 2023;
Published: 19 October 2023.
Edited by:
Sameer Kishore, Middlesex University Dubai, United Arab EmiratesReviewed by:
Heide Karen Lukosch, Human Interface Technology Lab New Zealand (HIT Lab NZ), New ZealandStefan Marks, Auckland University of Technology, New Zealand
Copyright © 2023 Pedersen and Musaeus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kamilla Pedersen, S2FtaWxsYUBhdS5kaw==