 Thomas Lustenberger
Thomas Lustenberger Philipp Störmann
Philipp Störmann Kathrin Eichler2
Kathrin Eichler2 Ingo Marzi
Ingo Marzi- 1Department of Trauma, Hand and Reconstructive Surgery, Hospital of the Goethe University Frankfurt am Main, Frankfurt, Germany
- 2Institute for Diagnostic and Interventional Radiology, Hospital of the Goethe University Frankfurt am Main, Frankfurt, Germany
Introduction: In patients with severe pelvic ring injuries, exsanguination still is the leading cause of death in the early post-injury phase. While mechanical pelvic ring stabilization and pre-peritoneal pelvic packing are mainly addressing venous bleeding, angio-embolization aims to control arterial bleeding. The goal of the present study was to evaluate the rate of postoperative angio-embolization after mechanical pelvic ring injury stabilization and pre-peritoneal pelvic packing. Bleeding sources detected in the angiography and the patient's outcome were investigated.
Patients and Methods: Retrospective observational cohort study at a single academic level I trauma center, reviewing all patients with pelvic ring injuries admitted from 01/2010 to 12/2019. Patients with emergent mechanical pelvic ring stabilization (supraacetabular external fixator and/or pelvic C-clamp) and direct pre-peritoneal pelvic packing were further analyzed. Patients that underwent postoperative angio-embolization were compared with those that did not. All postoperative angio-embolizations were evaluated with regards to bleeding sources and type of embolization.
Results: During the study period, a total of 39 patients required immediate mechanical pelvic stabilization and direct pre-peritoneal pelvic packing. Of these, 12 patients (30.8%) underwent a postoperative angio-embolization. The following vessels were identified as bleeding sources: superior gluteal artery (n = 6), obturator artery (n = 2), internal pudendal artery (n = 2), unnamed branches of the internal iliac artery (n = 3). A selective embolization was successful in 11 patients; in 1 patient, an unilateral complete occlusion of the internal iliac artery was performed to control the bleeding. Mean time from hospital admission to the surgical procedure was 52.8 ± 14.7 min and the mean time from admission to angio-embolization was 189.1 ± 55.5 min. The in-hospital mortality rate of patients with angio-embolization was 25.0% (n = 3). Of these, 2 patients died due to multiple organ failure and 1 patient due to severe head injury.
Conclusion: Secondary angio-embolization after external pelvic fixation and pre-peritoneal pelvic packing was effective in controlling ongoing bleeding. The most frequently detected bleeding vessel was the superior gluteal artery, which is difficult to surgically address, further highlighting the importance of angio-embolization in the management algorithm.
Introduction
Severe fractures of the pelvic ring pose significant challenges to the entire trauma team in terms of life-threat and functional outcome. Management algorithms focusing on volume resuscitation, mechanical stabilization of the pelvic ring injury, and coagulation management have improved over the last years and have resulted in significant achievements in the treatment of these usually polytraumatized patients (1). Nevertheless, the overall mortality rate in these patients remains high, ranging from 5 to 10% for patients with any type of pelvic fracture (2–4), up to 60–70% for hemodynamically compromised pelvic fracture patients or patients with open pelvic ring injuries (5–8).
In the past years, many different approaches to effectively manage the hemodynamically unstable patient with pelvic ring injury have been suggested and have been lively and controversially discussed in the contemporary literature (2, 9–25). These controversies have their origin—among other reasons—in different trauma system developments comparing European countries and North America and therefore have resulted in different favored pathways in the treatment of these highly challenging injuries. In the Anglo-American area, arteriography has become increasingly available over the last decade and has subsequently been implemented as the first line treatment even in the hemodynamically unstable pelvic trauma patient. In European countries, however, many trauma surgeons were trained in orthopedic surgery and are therefore highly familiar with early pelvic stabilization techniques which can easily be combined with pelvic packing in the initial phase. Therefore, two different fundamental treatment modalities have been suggested to manage patients with significant pelvic ring injuries and ongoing hemodynamic instability: Angio-embolization addressing arterial bleeding vs. pelvic packing, mainly controlling venous hemorrhage and bleeding from the spongious pelvic fracture site.
Our group previously pointed out that these two treatment modalities “are not antagonistic but rather should be seen as complementary modalities” (26, 27). In our own experience, signs of ongoing hemorrhage after mechanical pelvic stabilization and pre-peritoneal pelvic packing indicate the requirement for a postoperative pelvic angiography. Embolization of remaining arterial bleeding can then be performed on the way from the operating room to the Intensive Care Unit (ICU) in a patient with a more stabilized hemodynamic status. This concept of pre-peritoneal pelvic packing, external fixation of the pelvic ring injury and secondary angio-embolization is not new and has previously been described. Burlew et al. (28) reported on 75 patients with severe pelvic fractures and life-threatening hemorrhage, which underwent pelvic packing and external pelvic fixation. After surgery, a total of 10 patients (13%) successfully underwent angio-embolization; none of these patients died due to pelvic bleeding. The authors concluded that “angio-embolization should be seen as a complementary procedure for life-threatening hemorrhage control” following surgical pelvic packing and external fixation.
The goal of the present analysis is to assess the incidence of the need of postoperative angio-embolization after mechanical stabilization of the pelvic ring injury and direct pre-peritoneal pelvic packing. The sources of ongoing hemorrhage after surgical pelvic intervention and the patient's outcome are evaluated. We hypothesized that a secondary angio-embolization is effective in controlling persistent pelvic bleeding and will be required in a minority of patients following surgical damage control procedures.
Methods
After approval by the Institutional Review Board, we performed a single center, retrospective observational cohort study, reviewing all severely injured trauma patients with pelvic ring injuries which were admitted to our level I trauma center from January 1, 2010 to December 31, 2019. As part of our participation in the German Trauma Registry DGU® and as previously described (29, 30), all data was prospectively documented using a computer-based online documentation tool. Patients with pelvic ring injuries were identified using the Abbreviated Injury Scale (AIS) code 8561xx. Patients requiring immediate mechanical stabilization of their pelvic ring injury and pre-peritoneal pelvic packing were further analyzed. Other inclusion criteria were blunt trauma, primary admission and age ≥ 18 years. Patients were excluded if they died in the shock room or if they did not receive any type of damage control procedure (supra-acetabular external fixator, pelvic C-clamp, pre-peritoneal pelvic packing) for their pelvic ring injury.
The following variables were extracted from our database and from the patient's electronic file [X-rays and computed tomography (CT) scan, operation report, discharge summary]: pelvic fracture pattern (AO classification), Injury Severity Score (ISS), AIS score for each body region (head, chest, abdomen, extremity), acute management of the pelvic ring injury on day 0, age, gender, first values of blood pressure and pulse rate on admission, and outcome (blood transfusion requirement, ICU length of stay, mortality).
Further variables abstracted included time to surgical intervention (mechanical pelvic stabilization and pelvic packing), time to postoperative angio-embolization and the time required for angio-embolization. The bleeding sources noted during the angio-embolization were extracted from the procedure report of the interventional radiologist.
Our emergency department treatment algorithm for patients with severe pelvic fractures has been extensively described previously (26, 27, 31). In brief, immediately after arrival, a mechanical stabilization of the pelvic ring injury is performed using a pelvic binder if it has not been done in the pre-hospital setting. Patients with a systolic blood pressure of <90 mmHg despite volume management and transfusion of packed red blood cells (PRBC) are classified as “non-responder.” In these patients, urgent surgical exploration, direct pre-peritoneal pelvic packing and mechanical stabilization of the pelvis using a pelvic C-clamp and/or an anterior supra-acetabular external fixator are carried out; diagnostic procedures including a polytrauma CT scan are postponed until hemodynamic stability has been achieved. During direct pre-peritoneal pelvic packing, associated intraabdominal, thoracic, and extremity injuries are simultaneously assessed and are treated according to damage control principles.
Direct pre-peritoneal pelvic packing is performed via a midline incision from the symphysis pubis extending cranially. The bladder is retracted laterally, the pelvic brim is palpated and a total of three laparotomy packs are placed below the pelvic brim. The first is placed as posteriorly as possible just below the sacroiliac joint, the second is placed just anterior to the first, and the third sponge is placed in the retropubic space deep lateral to the bladder. Afterwards, the contralateral side is packed identically. A second look procedure with removal or change of the pelvic packs is carried out 24–48 h after the initial surgery.
In case of clinical and/or laboratory signs of ongoing bleeding, such as a persistent requirement of volume resuscitation and PRBC transfusion, increasing lactate or base deficit values noted on blood gas analysis, an angiography is done, ideally before ICU admission. If contrast extravasation is seen in the angiography, a selective embolization of the bleeding vessels, using coils or foam, is directly undertaken. Any evidence of vessel spasm or an abrupt cut-off of a vessel are considered as signs of vascular injury and an embolization is likewise carried out. To assess the success of the angio-embolization procedure, the interventional radiologist routinely performs an additional contrast run after the final embolization to ensure complete hemostasis. If hemodynamic stability is achieved following angio-embolization, the diagnostic work-up, including CT scans and plain radiographs of extremity injuries, is completed if it has not been done before the emergency surgery. Thereafter, the patient is transferred to the ICU for further resuscitation.
For the present analysis, the patient cohort was divided into two groups: patients with angio-embolization following mechanical pelvic ring stabilization and direct pre-peritoneal pelvic packing and patients without angio-embolization after emergency surgery. Primary outcome parameters included transfusion requirement [amount of PRBC/fresh frozen plasma (FFP) from emergency department admission to ICU admission, total amount transfused during hospital stay], and in-hospital mortality rate.
Statistical Analysis
Demographic and clinical characteristics comparing the two groups were evaluated using bivariate analysis. P-values for categorical variables were derived from the 2-sided Fisher's exact test and for continuous variables from the Mann–Whitney U test. Values are reported as mean ± standard deviation (SD) for continuous variables and as percentages for categorical variables. All analysis were performed using the Statistical Package for Social Sciences (SPSS for Mac), version 24.0 (SPSS Inc., Chicago, IL).
Results
During the 10 year study period, a total of 293 patients with pelvic ring injuries were admitted. Of these, 39 patients (13.3%) required immediate mechanical pelvic stabilization and direct pre-peritoneal pelvic packing. A total of 12 patients (30.8% of the 39 patients) subsequently underwent postoperative angio-embolization due to persistent signs of ongoing bleeding (Figure 1).
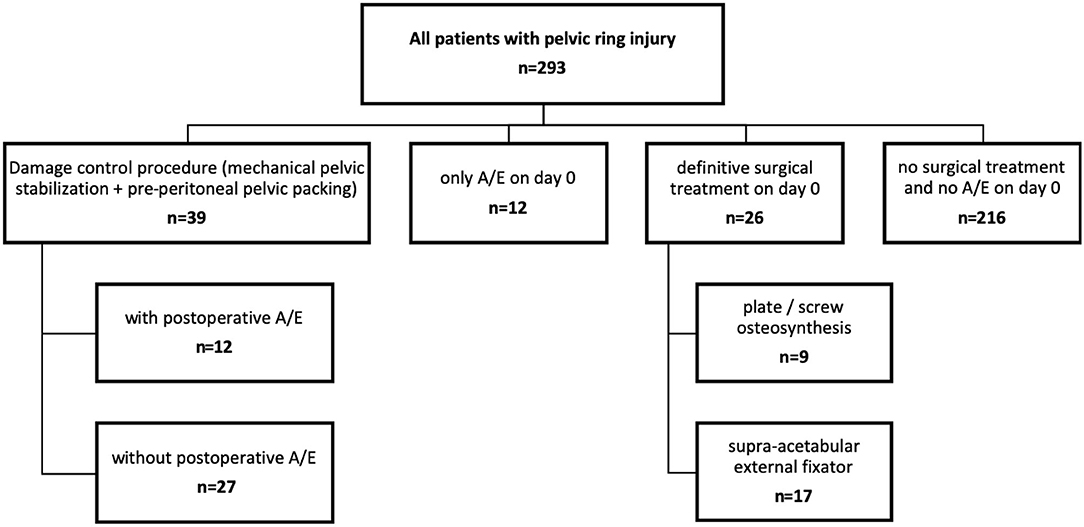
Figure 1. Flow chart demonstrating acute management of the pelvic ring injury on the day of admission. A/E, angio-embolization.
Table 1 compares patients with and without angio-embolization following mechanical stabilization of the pelvic ring injury and direct pre-peritoneal pelvic packing. Patients which underwent postoperative angio-embolization had a significantly lower systolic blood pressure on admission, a higher ISS with a higher rate of severe head injuries (AIS head ≥3), received more PRBC and more FFP transfusion until ICU admission, and demonstrated a significantly higher lactate value on admission. The overall mortality rate, however, did not differ statistically significant between the two groups (without vs. with angio-embolization, 14.8 vs. 25.0%, p = 0.654).
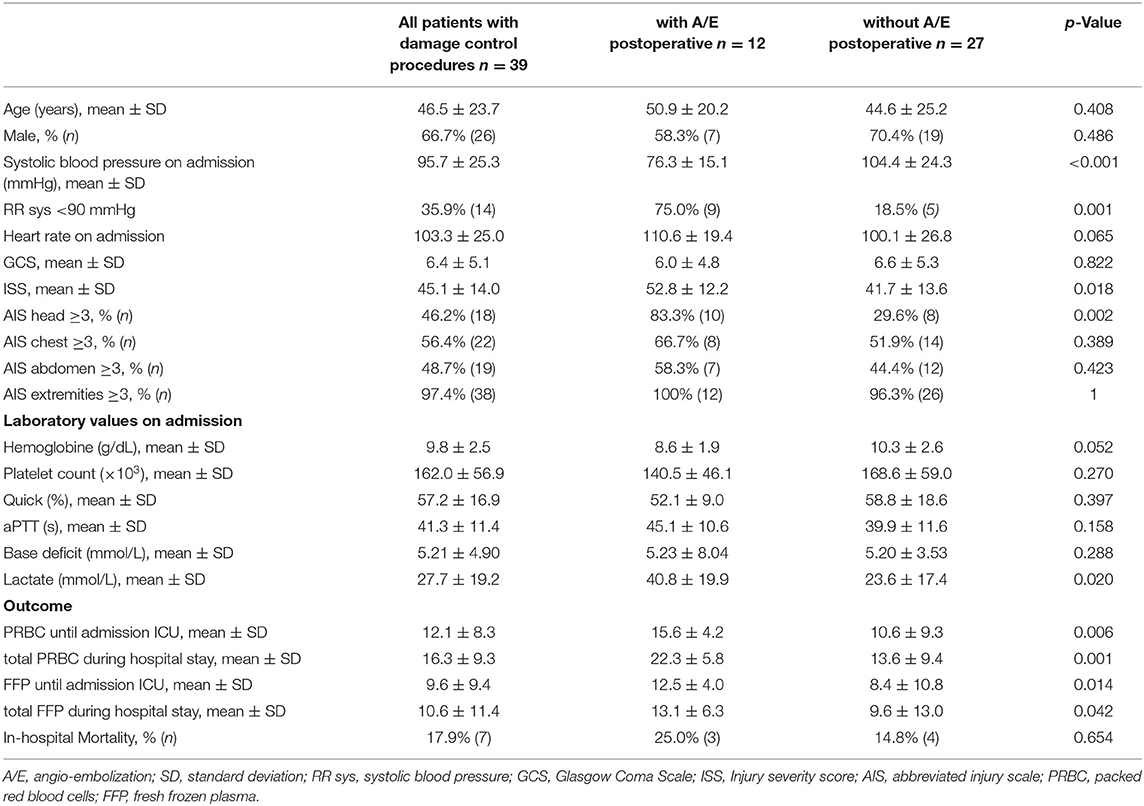
Table 1. Characteristics and outcome of patients with and without postoperative angio-embolization.
Of the 12 patients with postoperative angio-embolization, 3 patients suffered a type B2 and 9 patients a type C pelvic ring injury (C1, n = 3; C2 n = 2; C4, n = 4).
The mean time from admission to surgical intervention was 52.8 ± 14.7 min (range 34–76 min). All 12 patients underwent mechanical pelvic stabilization (supra-acetabular external fixator, n = 12; pelvic C-clamp, n = 3) and direct pre-peritoneal pelvic packing (n = 12). A total of 10 patients required further damage control procedures including external fixators of extremities (n = 10), laparotomy to address intra-abdominal associated injuries (n = 5) and intracranial pressure monitoring and/or craniotomies or craniectomies for the traumatic brain injury (n = 7). The mean time from hospital admission to postoperative angio-embolization was 189.1 ± 55.5 min (range 111–289 min) and the mean time required for the angio-embolization procedure was 52.3 ± 28.3 min (range 21–124 min).
Table 2 describes the angiographically identified bleeding sources and the type of embolization performed. In one patients, two bleeding vessels were identified during angiography. While in 11 patients a selective embolization of the bleeding vessels was undertaken, in 1 patient an unilateral complete occlusion of the internal iliac artery had to be performed. The superior gluteal artery was the most often identified bleeding source (n = 6, 42.6%). In all 12 patients, the angio-embolization procedure was successfully performed achieving complete hemostasis in the pelvic region. No complications associated with the embolization, such as necrosis or ischemia of tissues occurred during the hospital stay.
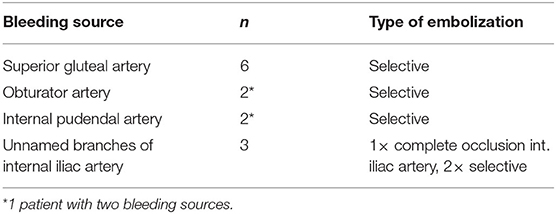
Table 2. Bleeding sources and type of embolization in patients treated with mechanical pelvic stabilization and pelvic packing followed by angio-embolization.
The mean transfusion requirement of packed red blood cells until angio-embolization was 15.6 ± 4.2 (range 9–21 packs). After angio-embolization until 48 h after admission, a mean of 5.1 ± 2.1 packs of red blood cells (range 2–9 packs) had to be transfused. The second look procedure was performed within 27.9 ± 8.6 h after the first operation. In two patients the pelvis was repacked due to persistent oozing. No complications related to the packing, such as pelvic space infection, were observed.
The mean ICU length of stay was 17.9 ± 10.7 days (range 3–42 days). Overall, three patients died in the further hospital course; two patients due to multiple organ failure (days 7 and 12, respectively) and one patient due to the traumatic brain injury (day 3).
Discussion
In the present study analyzing a 10-year period, approximately 13% of patients with pelvic ring injuries required emergent mechanical pelvic ring stabilization and direct pre-peritoneal pelvic packing due to hemodynamic instability. Of these patients, approximately 30% underwent post-operative angio-embolization to address ongoing arterial bleeders. The main finding is, that—by following the presented treatment algorithm—none of these highly unstable and critically injured pelvic ring injury patients (mean ISS of 53 points) died due to hemorrhage. Furthermore, we noted that the most often found bleeding artery after pelvic packing was the superior gluteal artery, which is difficult to surgically address.
In severe pelvic ring injuries, the bleeding source is more frequently of venous than arterial origin (90 vs. 10%). However, in pelvic trauma patients with hemodynamic instability, these numbers significantly change and a higher rate of arterial extravasation is observed in these cases. In the study by Eastridge et al. (7), 58.7% of patients with a severely unstable pelvic ring injuries and ongoing hemodynamic instability demonstrated an arterial vascular lesion. Similarly, Miller and colleagues reported a 67.9% rate of arterial bleeding in patients with ongoing hemodynamic compromise (12). However, although angio-embolization is clearly the treatment of choice in pelvic ring injury patients with arterial hemorrhage, numerous downsides of this procedure need to be considered, which—in our opinion—limit its safe use in the hemodynamically compromised trauma patient. First, angiography is known to possibly be a time-consuming procedure and simultaneous diagnostic or therapeutic interventions are not or only very limited possible in the angiography suite. Second, it necessitates the timely (24/7) availability of a highly skilled and trained interventional radiologist, but also associated technical assistants. Furthermore, the entire procedure needs to be set up quickly and without significant delay between end of the shock room treatment and start of angiography. This time and availability requirement has been shown to be one, if not the most important drawback of this procedure in critical situation with hemodynamically unstable patients. Numerous studies have highlighted that considerable time delays, ranging from 50 min up to 5.5 h, exist in performing the angiography procedure, what might obviously not be tolerated by a patient with hemodynamic instability (4, 10, 13). In a multicenter study, including 11 major trauma center in Australia and New Zealand and describing the treatment practice in hemodynamically compromised patients with severe pelvic ring injuries, only 14.7% of the angiography procedures were started within 90 min of hospital admission (32). Considering the time interval between admission and start of surgical procedure in our patients, a mean time to surgery of 52.8 ± 14.7 min, ranging from 34 to 76 min, was found, which accurately reflects the importance of achieving fast hemorrhage control.
Identifying whether venous or arterial bleeding is the major source responsible for the hemodynamic instability is not possible in the acute resuscitation phase. Venous bleeding from the fractured bony surface and from the pre-sacral and pre-vesical plexus is almost always present in significant pelvic ring injuries. Therefore, considering the previously listed drawbacks of angiography, mechanical stabilization of the pelvic fracture and pelvic packing is the first line of treatment in our management algorithm. Simultaneously, other necessary damage control techniques for concomitant head, chest, abdominal, and/or extremity injuries are applied. In case of ongoing hypotension and/or ongoing transfusion requirement following mechanical pelvic stabilization and pelvic packing, angiography and embolization of persistent arterial bleeders is performed. The intention by following this sequence of treatment modalities (surgery as first line, angio-embolization as second line of treatment) in these highly unstable patient, is to have a hemodynamically at least transient stable patient in the angiography suite. Additionally, surgery as first line procedure may “buy” time for setting up the emergent pelvic angiography. Our management algorithm is in line with previously reported protocols for patients with pelvic ring injuries (22, 28, 33–35). In the study by Burlew and coauthors, 13% of the patients underwent secondary angio-embolization. The mortality rate in this high-risk patient group was 21% with only 2% (n = 3) death cases due to acute bleeding (33). Magnone et al. (22) recently published a prospective validation of a pre-peritoneal pelvic packing protocol for hemodynamically unstable pelvic trauma patients. Similar to the previously mentioned study, the authors concluded that pelvic packing was a quick and effective method in the treatment of these severely injured patients. However, in contrast to our study, not all patients received a mechanical stabilization of the pelvic ring injury, which—in our opinion—is essential in order to provide sufficient abutment for the pelvic packs. Lastly, hybrid operating room systems have to be mentioned. In multiple studies, hybrid operating rooms have been shown to improve the management and workflow in patients with severe pelvic ring injuries (36–38). Ito and colleagues recently demonstrated that the time from admission to angio-embolization was significantly shorter in the hybrid operating room group. At our institution (and likely in the vast majority of trauma centers worldwide), hybrid operating room systems are currently not available, however, it would clearly pose a significant advantage in the management of these patients (38).
The most commonly reported arteries that require embolization in patients with pelvic ring injuries are the internal iliac artery in approximately 67%, unnamed branches of the internal iliac artery (17%), the superior gluteal artery (4%), the obturator artery (4%), and the internal pudendal artery (3%) (39). Multiple studies have addressed the association between pelvic fracture pattern and hemorrhage (10, 40–42). Due to the proximity, the superior gluteal artery is at risk in fractures involving the sciatic notch (39). Fractures of the pubic rami are associated with obturator vessel laceration and disruption of the sacroiliac joint with hemorrhage from gluteal and hypogastric branches (43, 44). To the best of our knowledge, the present study is one of the few investigations that specifically evaluates the angiographically identified sources of arterial bleeding following mechanical stabilization and surgical exploration and packing of the pelvic ring injury. In almost half of the cases, the superior gluteal artery was identified as the ongoing bleeder, which is, due to its anatomic course, difficult to surgically address. Contrary to the other branches of the internal iliac artery, the superior gluteal artery exits the small pelvis through the greater sciatic foramen. Therefore, and due to its dorsal position outside the pelvis, it is highly challenging—if not impossible—to perform surgical hemostasis or to pack the artery sufficiently. Its course outside the pelvis likewise exposes the superior gluteal artery to the risk of laceration when a percutaneous sacroiliac screw insertion is performed (45, 46). The obturator artery, on the other hand, which was found in 2 cases as the bleeding source, may be more accessible for surgical hemostasis. However, retraction of the vessel stump or vasospasm may complicate the identification of its laceration. Embolization was in all but one case performed in a selective way. A complete unilateral occlusion of the internal iliac artery was necessary in one case to achieve sufficient hemostasis; however, no complications associated with the complete occlusion were observed in the further hospital course.
The present study has several limitations, the most important being the retrospective study design. Furthermore, only a very selected group of pelvic ring injury patients was examined in this investigation. Patients not receiving damage control interventions for their pelvic ring injury on the day of admission and deaths in the shockroom were excluded from the analysis, introducing a selection bias. As a consequence, the reported mortality rate in the present study cannot be compared with mortality rates from studies looking at all patients with severe pelvic ring injuries. Additionally, due to our strict inclusion criteria, the number of patients analyzed in our study is low. However, it is important to notice, that these patients are a highly critical and severely injured subgroup of pelvic ring injury patients (mean ISS of 53 points), that are—even in high-volume trauma centers as ours—not frequently seen. Finally, the study periods spans over 10 years, in which changes and improvements in volume and transfusion management have occurred. However, with regards to our management algorithm for patients with severe pelvic ring injuries, no significant changes were introduced in our clinic during the study period. As we previously published, interventional emergency embolization for severe pelvic ring fractures with arterial bleeding is an integral part in our treatment algorithm since many years (13).
Conclusion
According to our management protocol, all hemodynamically unstable patients with severe pelvic ring injuries were directly transferred to the operating room, where mechanical stabilization of the pelvic ring, direct pre-peritoneal pelvic packing, and, in approximately one third of the patients, a subsequent angio-embolization was carried out. This sequence of treatment modalities resulted in a complete hemostasis of the pelvic hemorrhage in all of the examined cases. The superior gluteal artery, which is—due to its position and course in the pelvis—difficult to access, was the most often found ongoing arterial bleeder following surgical exploration and pelvic packing, further highlighting the importance of the secondary angio-embolization.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Institutional Review Board University Hospital Frankfurt. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
TL, PS, KE, and IM participated in research design, data analysis and wrote the paper. CN and MJ participated in research design and data analysis. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This paper was partly presented at the 18th European Congress of Trauma and Emergency Surgery, May 7-9, 2017; Bucharest, Romania. The abstract was previously published (47).
References
1. Scalea TM, Stein DM, O'Toole RV. Pelvic Fractures. In: Feliciano DV, Mattox KL, Moore EE, editors, Trauma. 6th ed. McGraw Hill Medical (2008). p. 759–88.
2. Biffl WL, Smith WR, Moore EE, Gonzalez RJ, Morgan SJ, Hennessey T, et al. Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg. (2001) 233:843–50. doi: 10.1097/00000658-200106000-00015
3. Starr AJ, Griffin DR, Reinert CM, Frawley WH, Walker J, Whitlock SN, et al. Pelvic ring disruptions: prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J Orthop Trauma. (2002) 16:553–61. doi: 10.1097/00005131-200209000-00003
4. Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. (2009) 40:343–53. doi: 10.1016/j.injury.2008.12.006
5. Cothren CC, Osborn PM, Moore EE, Morgan SJ, Johnson JL, Smith WR. Preperitonal pelvic packing for hemodynamically unstable pelvic fractures: a paradigm shift. J Trauma. (2007) 62:834–9. discussion: 9–42. doi: 10.1097/TA.0b013e31803c7632
6. Osborn PM, Smith WR, Moore EE, Cothren CC, Morgan SJ, Williams AE, et al. Direct retroperitoneal pelvic packing versus pelvic angiography: a comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury. (2009) 40:54–60. doi: 10.1016/j.injury.2008.08.038
7. Eastridge BJ, Starr A, Minei JP, O'Keefe GE, Scalea TM. The importance of fracture pattern in guiding therapeutic decision-making in patients with hemorrhagic shock and pelvic ring disruptions. J Trauma. (2002) 53:446–50. discussion: 50–1. doi: 10.1097/00005373-200209000-00009
8. Grotz MR, Allami MK, Harwood P, Pape HC, Krettek C, Giannoudis PV. Open pelvic fractures: epidemiology, current concepts of management and outcome. Injury. (2005) 36:1–13. doi: 10.1016/j.injury.2004.05.029
9. Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF III. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma. (1997) 43:395–9. doi: 10.1097/00005373-199709000-00001
10. Cook RE, Keating JF, Gillespie I. The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg Br. (2002) 84:178–82. doi: 10.1302/0301-620X.84B2.0840178
11. Croce MA, Magnotti LJ, Savage SA, Wood GW II, Fabian TC. Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg. (2007) 204:935–9. discussion: 40–2. doi: 10.1016/j.jamcollsurg.2007.01.059
12. Miller PR, Moore PS, Mansell E, Meredith JW, Chang MC. External fixation or arteriogram in bleeding pelvic fracture: initial therapy guided by markers of arterial hemorrhage. J Trauma. (2003) 54:437–43. doi: 10.1097/01.TA.0000053397.33827.DD
13. Westhoff J, Laurer H, Wutzler S, Wyen H, Mack M, Maier B, et al. Interventional emergency embolization for severe pelvic ring fractures with arterial bleeding. Integration into the early clinical treatment algorithm. Unfallchirurg. (2008) 111:821–8. doi: 10.1007/s00113-008-1479-8
14. Ertel W, Eid K, Keel M, Trentz O. Therapeutical strategies and outcome of polytraumatized patients with pelvic injuries. Eur J Trauma Emerg Surg. (2000) 26:278–86. doi: 10.1007/PL00002452
15. Ertel W, Keel M, Eid K, Platz A, Trentz O. Control of severe hemorrhage using C-clamp and pelvic packing in multiply injured patients with pelvic ring disruption. J Orthop Trauma. (2001) 15:468–74. doi: 10.1097/00005131-200109000-00002
16. Velmahos GC, Chahwan S, Falabella A, Hanks SE, Demetriades D. Angiographic embolization for intraperitoneal and retroperitoneal injuries. World J Surg. (2000) 24:539–45. doi: 10.1007/s002689910087
17. Giannoudis PV, Pape HC. Damage control orthopaedics in unstable pelvic ring injuries. Injury. (2004) 35:671–7. doi: 10.1016/j.injury.2004.03.003
18. Sarin EL, Moore JB, Moore EE, Shannon MR, Ray CE, Morgan SJ, et al. Pelvic fracture pattern does not always predict the need for urgent embolization. J Trauma. (2005) 58:973–7. doi: 10.1097/01.TA.0000171985.33322.b4
19. Lindahl J, Handolin L, Söderlund T, Porras M, Hirvensalo E. Angiographic embolization in the treatment of arterial pelvic hemorrhage: evaluation of prognostic mortality-related factors. Eur J Trauma Emerg Surg. (2013) 39:57–63. doi: 10.1007/s00068-012-0242-6
20. ten Broek RPG, Bezemer J, Timmer FA, Mollen RMHG, Boekhoudt FD. Massive haemorrhage following minimally displaced pubic ramus fractures. Eur J Trauma Emerg Surg. (2014) 40:323–30. doi: 10.1007/s00068-013-0361-8
21. Rommens PM, Wagner D, Hofmann A. Surgical management of osteoporotic pelvic fractures: a new challenge. Eur J Trauma Emerg Surg. (2012) 38:499–509. doi: 10.1007/s00068-012-0224-8
22. Magnone S, Allievi N, Ceresoli M, Coccolini F, Pisano M, Ansaloni L. Prospective validation of a new protocol with preperitoneal pelvic packing as the mainstay for the treatment of hemodynamically unstable pelvic trauma: a 5-year experience. Eur J Trauma Emerg Surg. (2019). doi: 10.1007/s00068-019-01115-3. [Epub ahead of print].
23. Jang JY, Shim H, Kwon HY, Chung H, Jung PY, Kim S, et al. Improvement of outcomes in patients with pelvic fractures and hemodynamic instability after the establishment of a Korean regional trauma center. Eur J Trauma Emerg Surg. (2019) 45:107–13. doi: 10.1007/s00068-017-0886-3
24. Lee MA, Yu B, Lee J, Park JJ, Lee GJ, Choi KK, et al. Effects of the establishment of a trauma center and a new protocol on patients with hemodynamically unstable pelvic fractures at a single institution in Korea. Eur J Trauma Emerg Surg. (2019) 45:273–9. doi: 10.1007/s00068-017-0899-y
25. Polytrauma Guideline Update G. Level 3 guideline on the treatment of patients with severe/multiple injuries : AWMF Register-Nr. 012/019. Eur J Trauma Emerg Surg. (2018) 44(Suppl. 1):3-271. doi: 10.1007/s00068-018-0922-y
26. Marzi I, Lustenberger T. Management of bleeding pelvic fractures. Scand J Surg. (2014) 103:104-11. doi: 10.1177/1457496914525604
27. Lustenberger T, Wutzler S, Stormann P, Laurer H, Marzi I. The role of angio-embolization in the acute treatment concept of severe pelvic ring injuries. Injury. (2015) 46(Suppl. 4):S33–8. doi: 10.1016/S0020-1383(15)30016-4
28. Burlew CC, Moore EE, Smith WR, Johnson JL, Biffl WL, Barnett CC, et al. Preperitoneal pelvic packing/external fixation with secondary angioembolization: optimal care for life-threatening hemorrhage from unstable pelvic fractures. J Am Coll Surg. (2011) 212:628–35. discussion: 35–7. doi: 10.1016/j.jamcollsurg.2010.12.020
29. Wyen H, Wutzler S, Rüsseler M, Mack M, Walcher F, Marzi I. Five years experience of trauma care in a German urban level I university trauma center. Eur J Trauma Emerg Surg. (2009) 35:448–54. doi: 10.1007/s00068-009-9140-y
30. Helm M, Kulla M, Fischer S, Lampl L. TraumaWatch—Ein modulares Konzept zur innerklinischen Traumadokumentation. Notfall und Rettungsmedizin. (2004) 7:328–35. doi: 10.1007/s10049-004-0667-5
31. Lustenberger T, Wutzler S, Störmann P, Marzi I. The role of pelvic packing for hemodynamically unstable pelvic ring injuries. Clin Med Insights Trauma Intens Med. (2015) 6:1–8. doi: 10.4137/CMTIM.S12257
32. Verbeek D, Sugrue M, Balogh Z, Cass D, Civil I, Harris I, et al. Acute management of hemodynamically unstable pelvic trauma patients: time for a change? Multicenter review of recent practice. World J Surg. (2008) 32:1874–82. doi: 10.1007/s00268-008-9591-z
33. Burlew CC, Moore EE, Stahel PF, Geddes AE, Wagenaar AE, Pieracci FM, et al. Preperitoneal pelvic packing reduces mortality in patients with life-threatening hemorrhage due to unstable pelvic fractures. J Trauma Acute Care Surg. (2017) 82:233–42. doi: 10.1097/TA.0000000000001324
34. Coccolini F, Stahel PF, Montori G, Biffl W, Horer TM, Catena F, et al. Pelvic trauma: WSES classification and guidelines. World J Emerg Surg. (2017) 12:5. doi: 10.1186/s13017-017-0117-6
35. Stahel PF, Burlew CC, Moore EE. Current trends in the management of hemodynamically unstable pelvic ring injuries. Curr Opin Crit Care. (2017) 23:511–9. doi: 10.1097/MCC.0000000000000454
36. Jang JY, Oh J, Shim H, Kim S, Jung PY, Kim S, et al. The need for a rapid transfer to a hybrid operating theatre: Do we lose benefit with poor efficiency? Injury. (2020) 51:1987–93. doi: 10.1016/j.injury.2020.04.029
37. Jang JY, Shim H, Jung PY, Kim S, Bae KS. Preperitoneal pelvic packing in patients with hemodynamic instability due to severe pelvic fracture: early experience in a Korean trauma center. Scand J Trauma Resusc Emerg Med. (2016) 24:3. doi: 10.1186/s13049-016-0196-5
38. Ito K, Nagao T, Tsunoyama T, Kono K, Tomonaga A, Nakazawa K, et al. Hybrid emergency room system improves timeliness of angioembolization for pelvic fracture. J Trauma Acute Care Surg. (2020) 88:314–9. doi: 10.1097/TA.0000000000002544
39. Vaidya R, Waldron J, Scott A, Nasr K. Angiography and embolization in the management of bleeding pelvic fractures. J Am Acad Orthop Surg. (2018) 26:e68–76. doi: 10.5435/JAAOS-D-16-00600
40. Costantini TW, Bosarge PL, Fortlage D, Bansal V, Coimbra R. Arterial embolization for pelvic fractures after blunt trauma: are we all talk? Am J Surg. (2010) 200:752–7. discussion: 7–8. doi: 10.1016/j.amjsurg.2010.06.006
41. Hauschild O, Aghayev E, von Heyden J, Strohm PC, Culemann U, Pohlemann T, et al. Angioembolization for pelvic hemorrhage control: results from the German pelvic injury register. J Trauma Acute Care Surg. (2012) 73:679–84. doi: 10.1097/TA.0b013e318253b5ba
42. Gilliland MG, Ward RE, Flynn TC, Miller PW, Ben-Menachem Y, Duke JH Jr. Peritoneal lavage and angiography in the management of patients with pelvic fractures. Am J Surg. (1982) 144:744–7. doi: 10.1016/0002-9610(82)90562-1
43. Metz CM, Hak DJ, Goulet JA, Williams D. Pelvic fracture patterns and their corresponding angiographic sources of hemorrhage. Orthop Clin North Am. (2004) 35:431–7, v. doi: 10.1016/j.ocl.2004.06.002
44. Hak DJ. The role of pelvic angiography in evaluation and management of pelvic trauma. Orthop Clin North Am. (2004) 35:439–43, v. doi: 10.1016/j.ocl.2004.06.001
45. Berger-Groch J, Lueers M, Rueger JM, Lehmann W, Thiesen D, Kolb JP, et al. Accuracy of navigated and conventional iliosacral screw placement in B- and C-type pelvic ring fractures. Eur J Trauma Emerg Surg. (2020) 46:107–13. doi: 10.1007/s00068-018-0990-z
46. Rommens PM, Nolte EM, Hopf J, Wagner D, Hofmann A, Hessmann M. Safety and efficacy of 2D-fluoroscopy-based iliosacral screw osteosynthesis: results of a retrospective monocentric study. Eur J Trauma Emerg Surg. (2020). doi: 10.1007/s00068-020-01362-9. [Epub ahead of print].
Keywords: pelvic ring fracture, management, hemodynamic instability, pelvic packing, angiography, embolization, external fixation
Citation: Lustenberger T, Störmann P, Eichler K, Nau C, Janko M and Marzi I (2020) Secondary Angio-Embolization After Emergent Pelvic Stabilization and Pelvic Packing Is a Safe Option for Patients With Persistent Hemorrhage From Unstable Pelvic Ring Injuries. Front. Surg. 7:601140. doi: 10.3389/fsurg.2020.601140
Received: 31 August 2020; Accepted: 30 November 2020;
Published: 17 December 2020.
Edited by:
Zsolt J. Balogh, The University of Newcastle, AustraliaReviewed by:
Philip Frank Stahel, Rocky Vista University, United StatesLaszlo Toth, Leeds Teaching Hospitals NHS Trust, United Kingdom
John Holcomb, University of Alabama at Birmingham, United States
Copyright © 2020 Lustenberger, Störmann, Eichler, Nau, Janko and Marzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thomas Lustenberger, bHVzdGVuYmVyZ2VyQHRyYXVtYS51bmktZnJhbmtmdXJ0LmRl