 G Tomasicchio
G Tomasicchio A Dezi
A Dezi A Picciariello
A Picciariello D. F Altomare
D. F Altomare G Martines
G Martines M De Fazio
M De Fazio M Rinaldi
M Rinaldi- Department of Precision of Regenerative Medicine and Ionian Area, University “Aldo Moro” of Bari, Italy
Introduction: Anal fissure is one of the most common anal disease characterized by intense anal pain, and deterioration of patients quality of life. Treatment is mainly based on the topical administration of calcium antagonist or nitric oxide ointments, and in cases refractory to medical treatment patients can undergo surgery. This study aims to assess the efficacy and safety of Levorag emulgel in the treatment of acute and chronic fissures using of a validated scoring system.
Material and Methods: A prospective observational study was carried out on patients with anal fissures between February and May 2022. The efficacy of the treatment was evaluated using the REALISE score, a new validated scoring system that rates VAS for pain, NSAID use, pain duration, bleeding, and quality of life (QoL), recorded after 10, 20 and 30 days from the beginning of treatment.
Results: Forty patients (median age 46 years, IQR 29–57, 70% women) with acute (22, 55%) or chronic (18, 45%) anal fissures entered the study. The median anal pain score according to the VAS scale decreased significantly from 7 (IQR 4.7–8) at baseline to 1 (IQR 0–3.2, p = 0.05) after 20 days. At the 30-day proctological examination, 22 patients (61%) were pain free (median VAS of 0, IQR 0–1.2, p < 0.05). Pain duration after defecation measured according to the REALISE score, showed a significant decrease after 10 days, from a median value of 2 (IQR 1–4) to 1 (IQR 1–1.2) (p < 0.005). The median value of the REALISE score decreased significantly, from 15 (IQR 11–19.25) at first proctological evaluation to 4 (IQR 4–6, p = 0.139) after 30 days of treatment. At day 30, complete fissure healing was achieved in 30 patients (80%). The healing rate was 82% and 78% in patients with acute and chronic anal fissures, respectively.
Conclusion: The use of Levorag® Emulgel may represent a safe and effective non-invasive first line treatment in patients affected by acute or chronic anal fissure.
Introduction
Anal fissure (AF) is one of the most common anal disease characterized by intense and prolonged anal pain after defecation, bleeding, and considerable deterioration of patient's quality of life (1). AF is often caused by the passage of hard stools or prolonged diarrhea (2). Spontaneous healing rarely occur because the reactive spastic contraction of the internal anal sphincter, decreases blood flow to the affected area (1–4). In fact, treatment strategies aim to reduce this uncontrolled spasm, using topical creams based on calcium antagonists (such as diltiazem) or nitric oxide donors (such as glycerin trinitrate) (5, 6) or by injections of botulinum toxin A (7) allowing restoration of blood flow to the anoderm (8) and to facilitate evacuation by using stool softeners.
When conservative treatments fail, surgical options including internal anal sphincterotomy, anal advancement flap, and anal stretch/dilation may be considered (9, 10).
None of these medical treatments are completely free from side effects such as headaches, migraines, and pruritus ani, while surgical approach can cause bleeding, abscesses, fistulas, and considerable risk of fecal incontinence (11–13).
This study aims to evaluate the safety and effectiveness of Levorag® Emulgel, a topical ointment which favors pain relief, microperfusion of the anoderm and the reepithelization process(11, 14), in the treatment of acute and chronic anal fissures assessed by a new validated scoring system.
Material and methods
A prospective observational study was carried out in a tertiary proctology unit on patients with anal fissures between February and May 2022. After receiving approval from the local ethics committee, patients of both sexes aged 18 to 85 years with acute or chronic anal fissures were enrolled. Exclusion criteria included previous medical or surgical treatment, perianal Crohn's disease, previous anorectal operations, prolapsed hemorrhoids, rectal prolapse, functional disorders of the defecation and continence, and pregnancy. Acute fissures were defined as recent (within 6 weeks) ulcerations of the anoderm, while chronic anal fissures persisted for more than 6 weeks, with sentinel tags and/or induration of the lateral margins of the fissure and/or exposure of the internal anal sphincter. Demographic data and detailed clinical histories were recorded, including information about anal pain intensity and duration, bowel habits, and stool consistency (using the Bristol stool scale) (15) before treatment. Patients were examined in the Sims position. The anal verge was inspected to confirm the presence of the anal fissure and to determine its location. When tolerated, digitorectal examination (DRE) to evaluate the anal sphincter tone and anoscopy were performed. Eligible patients received three boxes of Levorag® Emulgel (THD, SpA, Coreggio, RE, Italy), a topical ointment containing a Hibiscus plant extract called myoxinol with a botox-like effect, and carboxymethyl glucan, a yeast polysaccharide with immune-stimulating properties, for use in the conservative treatment of anal fissures. Each box contained twenty 3.5 ml single-dose tubes. Patients were instructed to apply the ointment twice a day (every 12 h) for 30 days using the tip of their finger. Stool softeners were administered in case of constipation. The efficacy of the treatment was evaluated using the REALISE score, a new validated scoring system that rates VAS for pain, NSAID use, pain duration, bleeding, and quality of life (QoL) (16). The score was calculated during the first clinical evaluation, at day 10 and 20 by a telephone interview (17, 18), and at day 30 by an outpatient evaluation. Side effects were recorded. The degree of re-epithelization (healing) was evaluated and scored as follows: 0 = anal fissure still present, 1 = superficial fissure, 2 = partial re-epithelization, 3 = complete re-epithelization. Patient satisfaction was rated on a scale of 0 (failure) to 5 (excellent).
Statistical analysis
Continuous parameters were reported as median and interquartile ranges. Categorical variables were recorded as numbers and percentages. Comparisons of categorical variables were performed by the Chi-square and Fisher's Exact test, where appropriate. Comparisons between groups were made by the Mann-Whitney U test. A p value < 0.05 was considered statistically significant. Statistical analysis was carried out using RStudio (R version 4.0.3 (2020-10-10) Copyright (C) 2020 The R Foundation for Statistical Computing).
Results
Forty patients (median age 46 years, IQR 29–57, 70% women) with acute (22, 55%) or chronic (18, 45%) anal fissures entered the study after giving an oral informed consent.
Thirty-six patients (12 males, median age 52 years, IQR 28–57, and 24 females, median age 45 years, IQR 29–56) completed both telephone interviews and a proctological evaluation at day 30. Four out of forty patients (10%) who did not complete the follow-up, underwent internal anal sphincterotomy (1 patient) and calcium antagonist-based ointments 10 days after the first consultation (3 patients). Previous pregnancies were reported by 14 women (58%) (Table 1). Four patients (11%) had an anterior anal fissure. digital rectal examination (DRE) was not tolerated at the first consultation by 10 patients (28%). The median anal pain score according to the visual analogue scale (VAS) was 7 (IQR 4.7–8) at baseline, and decreased to 3 (IQR 1–5, p < 0.005) 10 days later and to 1 (IQR 0–3.2, p = 0.05) after 20 days. At the 30-day proctological examination, 22 patients (61%) were pain free (median VAS of 0, IQR 0–1.2, p < 0.05). Pain duration after defecation measured according to the REALISE score, showed a significant decrease after 10 days, from a median value of 2 (IQR 1–4) to 1 (IQR 1–1.2) (p < 0.005). This score did not change after 20 and 30 days (median value 1, IQR 1–1, p = 0.23). With regard to bowel habits at the first evaluation, 8 patients (22%) had stool type 2 according to the Bristol stool scale, while 24 (67%) and 4 (11%) patients had type 3 and 6, respectively. The median value of the REALISE score at the first clinical evaluation was 15 (IQR 11–19.25) with a significant reduction at 10 days to 8 (IQR 6–11, p < 0.005). At 20 days, a median value of 6 (IQR 4.75–6.25, p < 0.05) was recorded. Between 20 and 30 days after the onset of treatment, the score decreased to 4 (IQR 4–6, p = 0.139) (Figure 1). At day 30, complete fissure healing was achieved in 30 patients (80%). One patient still had a chronic anal fissure at 30 days follow-up. Partial healing with complete symptoms remission was recorded in 5 patients. The healing rate was 82% and 78% in patients with acute and chronic anal fissures, respectively. At the last consultation, satisfaction was scored as 5 (extremely satisfied) by 25 patients, 4 (satisfied) by 7 patients, 3 (moderately satisfied) by 2 patients, 2 (not satisfied) by 1 patient and 1 (completely not satisfied) by the last one. Eight patients complained of pruritus ani during the first examination, with complete relief 20 days after. No other adverse events were recorded. All domains of the REALISE score are reported in Table 2.

Figure 1. REALISE score at the baseline, 10–20 and 30 days from the start of treatment.
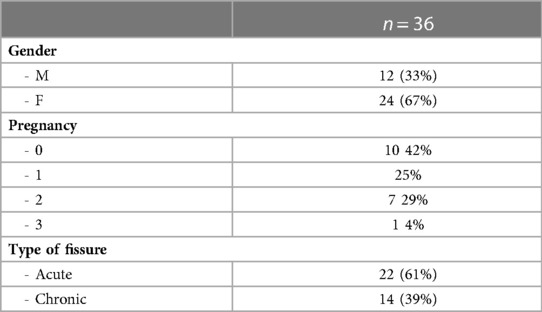
Table 1. Demographic characteristics of patients included in the study.
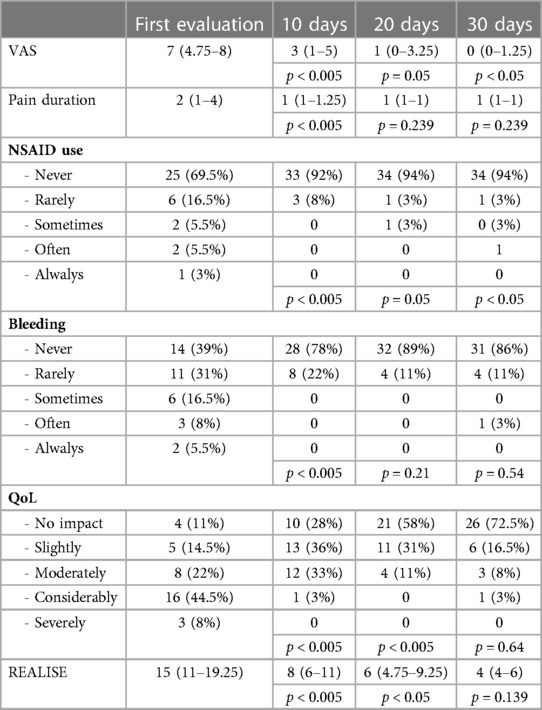
Table 2. RALISE domains at the baseline, 10-20 and 30 days from the start of treatment.
Discussion
Non-operative management is the first-line approach for treating anal fissures, as it can provide relief the associated anal spasm with pain decreases and healing of the fissure in about 60 to 80% of the cases (19).
A recent survey among gastrointestinal surgeons in the Netherlands reported that initial treatment consists of conservative measures including administration of fibers/laxatives and topical ointments (20).
In the past few decades, several topical ointments have been proposed as non-invasive treatments for anal fissures. Currently, the Association of Coloproctologists of Great Britain and Ireland recommends diltiazem as first-line treatment for chronic anal fissures (21) with a healing rate of 52.3% after 8 weeks, because of its lower side effect (22), despite the use of topical nitrate has showed a higher healing rate (63.6%). However, in a recent randomized clinical trial on patients affected by chronic anal fissures, glyceryl trinitrate ointment resulted less effective than tocopherol acetate in the reduction of anal pain and in term of healing and recurrence rate 16 weeks after finishing the treatment (23).
Botulinum toxin can also be used as conservative treatment being more effective than nitrates and calcium channel blockers even if but the local injection is painful and its effect is temporary (7).
In this study, the administration of Levorag® Emulgel, a topical ointment with natural anti-inflammatory agents, botox-like effect, and immune-stimulating properties, resulted in complete healing in 80% of patients with acute or chronic anal fissures. These results are in agreement with data published by Digennaro et al. (11) who reported an efficacy of 89.4% in acute and 62.8% in chronic anal fissures in their prospective multicenter observational trial on 265 patients.
Nordholm-Cartensen et al. (24) reported a healing rate of 52% in a randomized clinical trial of patients with chronic anal fissures, although the number of patients in the Levorag group (26 patients) was smaller than the estimated sample size and the study's power was only 70%. Furthermore, the RCT did not provide a clear definition of “fissure healing.”
A preliminary study by Giordano et al. (25) on the use of Levorag in patients with chronic anal fissures, reported a healing rate of 84% with over 85% of bleeding control after 40 days of treatment. Our study confirms these results, but the Levorag ointment was administered for only 30 days. In addition, our data showed a significant reduction of pain after 10 days of treatment (7 vs. 3 on the median VAS), with a slow but progressive pain reduction in the follow-up. Furthermore, the introduction of a validated score to assess the severity of the fissure, makes the evaluation of our results more objective and measurable.
In our analysis, the healing rate was higher than other medical treatments using topical ointments, however the small sample size and the inclusion of acute anal fissures may limit the reliability of the study. Other limitations of this study are the lack of a control group and the use of only the Bristol scale to evaluate bowel habit.
In conclusion the use of Levorag® Emulgel may represent a safe and effective non-invasive first line treatment in patients affected by acute or chronic anal fissure. Multicenter prospective randomized studies with long-term follow-up are expected to confirm our results.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comitato Etico Indipendente Azienda Ospedaliero-Universitaria consorziale Policlinico. The patients/participants provided their written informed consent to participate in this study.
Author contributions
GT, AD, MR and AP, all contributed equally to this study in terms of contributions to the conception and design of the research project; acquisition, analysis, and interpretation of data for the study; drafting and revising the project critically; final approval of the version to be published. DFA and CG contributed equally to this study Drafting the work and revising it critically for important intellectual content. MDF and GM: Substantial contributions to the conception and design of the study; acquisition, analysis, and interpretation of data for the work; Final approval of the version to be published. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sit M, Yilmaz EE, Canan F, Yildirim O, Cetin MM. Health-related quality of life in patients with anal fissure: effect of type D personality. Prz Gastroenterol. (2014) 9(2):93–8. doi: 10.5114/pg.2014.42504
2. Lund JN, Scholefield JH. Aetiology and treatment of anal fissure. Br J Surg. (1996) 83(10):1335–44. doi: 10.1002/bjs.1800831006
3. Lund JN, Binch C, McGrath J, Sparrow RA, Scholefield JH. Topographical distribution of blood supply to the anal canal. Br J Surg. (1999) 86(4):496–8. doi: 10.1046/j.1365-2168.1999.01026.x
4. Schouten WR, Briel JW, Auwerda JJ. Relationship between anal pressure and anodermal blood flow. The vascular pathogenesis of anal fissures. Dis Colon Rectum. (1994) 37(7):664–9. doi: 10.1007/BF02054409
5. Tarasconi A, Perrone G, Davies J, Coimbra R, Moore E, Azzaroli F, et al. Anorectal emergencies: WSES-AAST guidelines. World J Emerg Surg. (2021) 16(1):48. doi: 10.1186/s13017-021-00384-x
6. Nelson RL, Manuel D, Gumienny C, Spencer B, Patel K, Schmitt K, et al. A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol. (2017) 21(8):605–25. doi: 10.1007/s10151-017-1664-2
7. Altomare DF, Binda GA, Canuti S, Landolfi V, Trompetto M, Villani RD. The management of patients with primary chronic anal fissure: a position paper. Tech Coloproctol. (2011) 15(2):135–41. doi: 10.1007/s10151-011-0683-7
8. Altomare DF, Rinaldi M, Milito G, Arcana F, Spinelli F, Nardelli N, et al. Glyceryl trinitrate for chronic anal fissure–healing or headache? Results of a multicenter, randomized, placebo-controled, double-blind trial. Dis Colon Rectum. (2000) 43(2):174–9. discussion 9-81. doi: 10.1007/BF02236977
10. Gallo G, Stratta E, Realis Luc A, Clerico G, Trompetto M. A tailored rhomboid mucocutaneous advancement flap to treat anal stenosis. Colorectal Dis. (2020) 22(10):1388–95. doi: 10.1111/codi.15118
11. Digennaro R, Pecorella G, La Manna S, Alderisio A, Alderisio A Jr., De Pascalis B, et al. Prospective multicenter observational trial on the safety and efficacy of LEVORAG(R) Emulgel in the treatment of acute and chronic anal fissure. Tech Coloproctol. (2015) 19(5):287–92. doi: 10.1007/s10151-015-1289-2
12. Levin A, Cohen MJ, Mindrul V, Lysy J. Delayed fecal incontinence following surgery for anal fissure. Int J Colorectal Dis. (2011) 26(12):1595–9. doi: 10.1007/s00384-011-1284-7
13. Al-Thoubaity F. Safety and efficacy of the treatment of chronic anal fissure by lateral internal sphincterotomy: a retrospective cohort study. Ann Med Surg (Lond). (2020) 57:291–4. doi: 10.1016/j.amsu.2020.08.010
14. Di Trapani B, Gagliardo CM, Bargiggia C, Tomasini S, Molinelli B, Feo M, et al. Antinflammatory effect of levorag(R) (THD) emulgel on radiation proctocolitis around a colo-anal anastomosis. Minerva Chir. (2020) 75(5):373–4. doi: 10.23736/S0026-4733.20.08321-2
15. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. (1997) 32(9):920–4. doi: 10.3109/00365529709011203
16. Picciariello A, Lobascio P, Spazzafumo L, Rinaldi M, Dibra R, Trigiante G, et al. The REALISE score: a new statistically validated scoring system to assess the severity of anal fissures. Tech Coloproctol. (2021) 25(8):935–40. doi: 10.1007/s10151-021-02459-y
17. Gallo G, Picciariello A, Di Tanna GL, Santoro GA, Perinotti R. Telemedicine in colorectal surgery Italian working Group; Grossi U. E-consensus on telemedicine in colorectal surgery: a RAND/UCLA-modified study. Updates Surg. (2022) 74(1):163–70. doi: 10.1007/s13304-021-01139-8
18. Gallo G, Grossi U, Sturiale A, Di Tanna GL, Picciariello A, Pillon S, et al. E-consensus on telemedicine in proctology: a RAND/UCLA-modified study. Surgery. (2021) 170(2):405–11. doi: 10.1016/j.surg.2021.01.049
19. Jin JZ, Hardy MO, Unasa H, Mauiliu-Wallis M, Weston M, Connolly A, et al. A systematic review and meta-analysis of the efficacy of topical sphincterotomy treatments for anal fissure. Int J Colorectal Dis. (2022) 37(1):1–15. doi: 10.1007/s00384-021-04040-3
20. van Reijn-Baggen DA, Dekker L, Elzevier HW, Pelger RCM, Han-Geurts IJM. Management of chronic anal fissure: results of a national survey among gastrointestinal surgeons in the Netherlands. Int J Colorectal Dis. (2022) 37(4):973–8. doi: 10.1007/s00384-022-04115-9
21. Cross KL, Massey EJ, Fowler AL, Monson JR. The management of anal fissure: ACPGBI position statement. Colorectal Dis. (2008) 10(Suppl 3):1–7. doi: 10.1111/j.1463-1318.2008.01681.x
22. Boland PA, Kelly ME, Donlon NE, Bolger JC, Larkin JO, Mehigan BJ, et al. Management options for chronic anal fissure: a systematic review of randomised controlled trials. Int J Colorectal Dis. (2020) 35(10):1807–15. doi: 10.1007/s00384-020-03699-4
23. Ruiz-Tovar J, Llavero C. Perianal application of glyceryl trinitrate ointment versus tocopherol acetate ointment in the treatment of chronic anal fissure: a randomized clinical trial. Dis Colon Rectum. (2022) 65(3):406–12. doi: 10.1097/DCR.0000000000002120
24. Nordholm-Carstensen A, Perregaard H, Wahlstrom KL, Hagen KB, Hougaard HT, Krarup PM. Treatment of chronic anal fissure: a feasibility study on Levorag(R) Emulgel versus Diltiazem gel 2. Int J Colorectal Dis. (2020) 35(4):615–21. doi: 10.1007/s00384-020-03515-z
Keywords: anal fissure, topical treatment, anal pain, scoring system, healing
Citation: Tomasicchio G, Dezi A, Picciariello A, Altomare D. F, Giove C, Martines G, De Fazio M and Rinaldi M (2023) Safety and efficacy of Levorag emulgel in the treatment of anal fissures using a validated scoring system. Front. Surg. 10:1145170. doi: 10.3389/fsurg.2023.1145170
Received: 15 January 2023; Accepted: 8 March 2023;
Published: 22 March 2023.
Edited by:
Alberto Realis Luc, Clinica Santa Rita, ItalyReviewed by:
Carlo Alberto Manzo, University of Milan, ItalyNaciye Cigdem Arslan, Istanbul Medipol University, Türkiye
Giuseppe Pentassuglia, Azienda Sanitaria Locale "Città di Torino", Italy
© 2023 Tomasicchio, Dezi, Picciariello, Altomare, Giove, Martines, De Fazio and Rinaldi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: A Picciariello YXJjYW5nZWxvcGljY2lhcmllbGxvQGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery