 Xiao-Dong Li
Xiao-Dong Li Kewei Du*
Kewei Du*
- Department of Orthopedics, Shidong Hospital Affiliated to University of Shanghai for Science and Technology, Shanghai, China
Background: This study aimed to evaluate the treatment effects of three internal fixation methods, including tension band with K-wires, tension band with cannulated screws and tension band with ring-pins on transverse fractures of the patella.
Methods: Patellar fracture patients treated in Shanghai Yangpu District Shidong Hospital from March 2016 to January 2023 were divided into three groups based on the internal fixation method: the ring-pins group (tension band with ring-pins), the K-wires group (tension band with K-wires), and the cannulated screws group (tension band with cannulated screws). Surgery duration, hemoglobin decrease, excellent rate of knee joint function evaluation at postoperative 3 months and 12 months, VAS scores before surgery and at 3 and 12 months after surgery, postoperative complication rate, and removal rate of internal fixation were compared among the three groups of patients.
Results: No significant differences were observed in operation time and the degree of hemoglobin decrease before and after operation among the three groups (P > 0.05). There was a statistical difference in the excellent and good rate of Böstman's score among the three groups of patients 3 months after surgery (P < 0.05). The excellent and good rates of knee joint scores in the ring-pins group and the cannulated screws group in 3 months after surgery were higher than in the K-wires group, and no significant differences were observed in the excellent and good rates of Böstman's score among the three groups at 12 months after surgery (P > 0.05). No significant differences were observed in VAS scores across groups before and after surgery (P > 0.05). The VAS scores at 3 months and 12 months after surgery were lower than those before surgery (P < 0.001). Significant differences were observed in the incidence of postoperative complications (P < 0.05) and hardware removal rates (P < 0.001) among the three groups. The ring-pins group and the cannulated screws group had fewer postoperative complications than the K-wires group.
Conclusion: Compared with K-wires and cannulated screws, ring-pins have the advantages of wide application range, low postoperative complication rate, and easy removal of implants. Treatment experience, low surgical complexity, and good postoperative knee joint function recovery have obvious clinical application value.
1 Introduction
The patella is an essential component of normal knee function, and fractures of the patella account for 1%–1.7% of all fractures in adults (1). These fractures are most common in patients aged 20–50 years and are often caused by falls or traffic accidents. Transverse fractures are the most common type, accounting for approximately 50% of patellar fractures, and can usually be identified through imaging. Surgical intervention is indicated when the displacement is ≥3 mm, the articular surface defect is >2 mm, or there is dysfunction in knee extension (2). Currently, tension band fixation is a commonly used surgical approach (3), with the tension band with K-wires and tension band with cannulated screws being widely used and considered classic methods. However, both techniques have notable drawbacks, such as the tendency for K-wires to back out or for cannulated screws cause iatrogenic bone damage and increased surgical complexity during removal. With advancements in materials, ring-pins combining the advantages of both classic methods while mitigating some of their shortcomings (4). This technique has been gradually adopted in clinical practice in recent years. Lee et al. demonstrated that all three fixation techniques provide adequate biomechanical stability for normal daily activities (5), Kim et al. reported that the modified technique provides dual benefits: enhanced implant stability and reduced propensity for causing soft tissue irritation (6).
This study retrospectively analyzed 101 cases of transverse patellar fractures treated at our hospital. We compared the therapeutic outcomes of three tension band fixation methods, including surgical duration, hemoglobin level decrease, knee function (Böstman scores), pain relief (VAS scores), complication rates, and implant removal rates. Our findings provide evidence-based recommendations for optimizing fixation strategies.
2 Materials and methods
2.1 Subjects of the study
Patellar fracture patients admitted to Shanghai Yangpu District Shidong Hospital from March 2016 to January 2023 were included in the present retrospective study, comparing the clinical efficacy of three different tension band internal fixation methods. Inclusion criteria were: (1) fresh transverse patellar fractures caused by trauma; (2) aged ≥18 years, without major underlying medical conditions or mental illness, and with regular postoperative follow-up. (3) Patients who were self-sufficient and had normal knee function before the fracture. Exclusion criteria were: (1) patients with major underlying medical conditions or mental illness; (2) patients with concurrent fractures in other parts of the body; (3) patients with preoperative skin abrasions or infections at the surgical site; (4) patients lost to follow-up after surgery. This study was approved by the Ethics Committee of Shanghai Yangpu District Shidong Hospital (2023-061-01).
A total of 101 patients with transverse patellar fractures treated surgically in our hospital from March 2016 to January 2023 were included in the study. The cohort consisted of 39 males and 62 females, aged 25–90 years (average age: 64.1 years). Based on the internal fixation method, patients were divided into three groups: the ring-pins group (tension band with ring-pins, 19 cases), the K-wires group (tension band with K-wires, 51 cases), and the cannulated screws group (tension band with cannulated screws, 31 cases). There were no significant differences in sex, age, or time from injury to surgery among the three groups (P > 0.05). All fractures were located in the middle or lower third of the patella, ensuring group comparability (Table 1).

Table 1. Baseline characteristics of the three groups.
2.2 Surgical methods
All patients underwent the same preoperative preparation, including elevation and immobilization of the affected knee, brace fixation, and routine preoperative examinations. Patients received either spinal or general anesthesia and were placed in the supine position. The surgical area was sterilized and draped, and the procedure was performed under C-arm fluoroscopy.
2.2.1 Preoperative examination
All patients underwent knee x-rays (anteroposterior and lateral views) and CT scans to assess the fracture type and displacement. A comprehensive evaluation of the patient's overall condition and pre-injury knee function was also conducted.
2.2.2 Surgical procedure
A longitudinal incision was made over the patella, and the fracture site and intra-articular hematoma were cleared. The fracture ends were reduced and temporarily fixed with reduction forceps. The ring-pins group: Two φ2.0 mm ring-pins were inserted from the inferior to the superior pole of the patella. A cable was passed through the pinhole in a figure-of-eight configuration. The knee was flexed and extended to ensure stable fixation, and fluoroscopy confirmed satisfactory reduction and proper positioning of the ring-pins and cable. The ends of the ring-pins were bent and cut. The K-wires group: Two φ2.0 mm K-wires were inserted from the inferior to the superior pole of the patella. A cable was used in a figure-of-eight configuration. The knee was flexed and extended to ensure stable fixation, and fluoroscopy confirmed satisfactory reduction and proper positioning of the K-wires and cable. The ends of the K-wires were bent and cut. The cannulated screws group: Two guide pins were inserted from the inferior to the superior pole of the patella. Two φ3.5 mm cannulated screws were placed over the guide pins, and a cable was used in a figure-of-eight configuration. The knee was flexed and extended to ensure stable fixation, and fluoroscopy confirmed satisfactory reduction and proper positioning of the screws and cable.
2.2.3 Postoperative management
Prophylactic antibiotics were administered within 1 h before surgery and discontinued within 24 h after the procedure. Routine pain management and anti-swelling treatments were provided. Blood biochemical tests were repeated, and functional exercises were initiated on the first postoperative day, with knee flexion ≥90° and full extension. Gradual weight-bearing and knee flexion-extension exercises were performed at 6–8 weeks postoperatively.
2.3 Evaluation criteria
All patients were followed up for 3–12 months postoperatively. Radiologic exams were conducted to assess fracture healing and knee function. The primary outcomes included: (1) Intraoperative conditions: surgery duration (from skin incision to wound closure), blood loss (hemoglobin decrease before and after surgery), and hospital stay. (2) Excellent and good rates of knee function Böstman scores at 3 and 12 months postoperatively (Böstman score (7): assessed based on knee range of motion (6 points), pain level (6 points), impact on daily activities (4 points), muscle atrophy (2 points), need for crutches (2 points), joint effusion (2 points), weakness during walking (2 points), and stair-climbing ability (2 points). A score of 20 is poor, 20–27 is good, and 28–30 is excellent. (3) Preoperative and postoperative Visual Analog Scale(VAS) scores at 3 and 12 months (8): participants mark their pain level on a continuous line, with 0 indicating no pain, 1–3 mild pain, 4–6 moderate pain, 7–9 severe pain, and 10 unbearable pain). (4) Postoperative complication rates (e.g., wire migration, soft-tissue irritation) and hardware removal rates.
2.4 Statistical analysis
Statistical analysis was performed using jamovi 2.3.28.0 software. Categorical data were expressed as percentages and analyzed using the χ2 test. Continuous data were expressed as mean ± standard deviation. The Shapiro–Wilk test was used to assess normality. Data conforming to a normal distribution were analyzed using the F-test, while non-normally distributed data were analyzed using the Kruskal–Wallis H-test. Intra-group comparisons were performed using repeated measures ANOVA. P < 0.05 was considered statistically significant.
3 Results
3.1 Surgical and postoperative recovery conditions
All patients were followed up for 12–18 months (mean: 15 months). No infections, non-unions, or internal fixation failures occurred. All wounds healed well, with no iatrogenic injuries. The average hospital stay was 10.9 days. There were no significant differences in surgery duration, hemoglobin decrease, or hospital stay among the three groups (P > 0.05) (Table 2).

Table 2. Comparison of intraoperative and postoperative conditions among three groups.
3.2 Postoperative knee function Böstman scores
There was a significant difference in the excellent and good rates of Böstman scores among the three groups at 3 months postoperatively (P < 0.05). However, there was no significant difference at 12 months postoperatively (P > 0.05) (Table 3). In the K-wires group, 4 out of 8 patients with poor functional scores at 3 months showed improvement to good after hardware removal at 12 months.

Table 3. Proportion of excellent/good outcomes of postoperative knee function Böstman scores among three groups.
3.3 Postoperative pain conditions
There were no significant differences in VAS scores before and after surgery among the three groups (P > 0.05). However, the VAS scores at 3 and 12 months postoperatively were significantly lower than preoperative scores (P < 0.001) (Table 4).

Table 4. Preoperative and postoperative VAS scores among three groups.
3.4 Postoperative complications
There were significant differences in postoperative complication rates (P < 0.05) and hardware removal rates (P < 0.001) among the three groups (Table 5). In the ring-pins group, there was 1 case of soft-tissue irritation. In the K-wires group, there were 6 cases of soft-tissue irritation and 6 cases of wire migration. In the cannulated screws group, there were 2 cases of soft-tissue irritation. The hardware removal rate was correlated with postoperative complications (P < 0.001). Considering the influence of age, we compared the incidence of postoperative complications between those >70 and ≤70 years old, both within and across groups, revealed no statistically significant differences (P > 0.05) (Table 6).
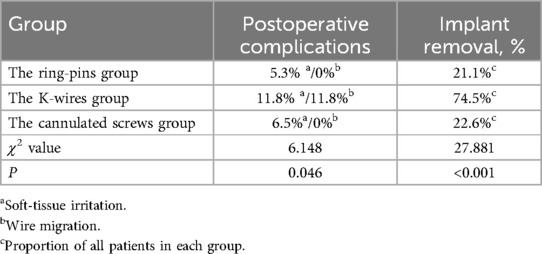
Table 5. Comparison of postoperative complications and hardware removal rates among three groups.

Table 6. Comparison of postoperative complications among the three groups with age stratification (>70 years).
Case 1: A 50-year-old female patient presented with right knee pain and limited mobility for 1 day following a fall. She was admitted with a diagnosis of right patellar fracture. Under general anesthesia with intubation, she underwent open reduction and internal fixation of the patellar fracture using a tension band with ring-pins band. Postoperatively, there were no signs of infection, wire migration, or breakage. After 15 months of follow-up, the hardware was removed, and the patient showed good fracture healing (Figure 1).

Figure 1. The ring-pins group: (A,B) preoperative anteroposterior and lateral x-rays showing significant fracture displacement. (C,D) Postoperative 3-month anteroposterior and lateral x-rays demonstrating satisfactory reduction, smooth articular surface, and no wire migration. (E,F) Postoperative 15-month anteroposterior and lateral x-rays showing blurred fracture lines. (G,H) Postoperative 15-month anteroposterior and lateral x-rays after hardware removal, showing complete fracture healing.
Case 2: A 62-year-old female patient presented with right knee pain and limited mobility for 5 days following a fall. She was admitted with a diagnosis of right patellar fracture. Under general anesthesia with intubation, she underwent open reduction and internal fixation of the patellar fracture using an Tension band with K-wires. Postoperatively, there were no signs of infection, wire migration, or breakage. After 12 months of follow-up, the hardware was removed, and the patient showed good fracture healing (Figure 2).

Figure 2. The K-wires group: (A,B) preoperative anteroposterior and lateral x-rays showing fracture displacement and angulation. (C,D) Postoperative 3-month anteroposterior and lateral x-rays demonstrating satisfactory reduction, correction of angulation, and no wire migration. (E,F) Postoperative 11-month anteroposterior and lateral x-rays showing blurred fracture lines. (G,H) Postoperative 12-month anteroposterior and lateral x-rays after hardware removal, showing complete fracture healing.
Case 3: A 59-year-old female patient presented with left knee pain and limited mobility for 1 day following a fall. She was admitted with a diagnosis of left patellar fracture. Under general anesthesia with intubation, she underwent open reduction and internal fixation of the patellar fracture using a tension band with cannulated screws. Postoperatively, there were no signs of infection, screw migration, or breakage. After 13 months of follow-up, the hardware was removed, and the patient showed good fracture healing (Figure 3).

Figure 3. The cannulated screws group: (A,B) preoperative anteroposterior and lateral x-rays showing fracture angulation. (C,D) Postoperative 3-month anteroposterior and lateral x-rays demonstrating correction of angulation, smooth articular surface, and no screw migration. (E,F) Postoperative 12-month anteroposterior and lateral x-rays showing blurred fracture lines. (G,H) Postoperative 13-month anteroposterior and lateral x-rays after hardware removal, showing complete fracture healing.
4 Discussion
Patellar fractures are common traumatic fractures in clinical practice, requiring rigid fixation and anatomical reduction to achieve early functional exercise (9), prevent knee stiffness, and restore knee extension function (10). Currently, different internal fixation methods and surgical approaches are used for different types of patellar fractures. Tension band internal fixation is the standard surgical method for patellar fractures (11), with the ring-pins, K-wires and cannulated screws being commonly used. However, there is no widespread consensus on which internal fixation method is superior. The ring-pins group, as a newer technique, combines the advantages of the tension band with K-wires and the tension band with cannulated screws and has been gradually adopted in clinical practice. This study compared the three methods in terms of several dimensions based on 101 cases of transverse patellar fractures treated surgically in our hospital, providing a reference for the selection of surgical methods in clinical practice.
This study found no significant differences in fracture healing time among the three internal fixation methods. The tension band with cannulated screws had no risk of wire slippage, as the screw and wire form a single unit that adheres closely to the bone, providing strong resistance to wire migration (12). This method is less likely to result in fixation failure or fracture displacement and is simple to perform. It is suitable for patellar fractures with large fragments and minimal comminution. However, the drilling process can cause bone damage (13); Bone ingrowth into screws may complicate removal, and cable laceration by screw threads may lead to retained hardware. The tension band with K-wires is simple to perform, cost-effective, and causes minimal bone damage, making it suitable for comminuted fractures. However, K-wires are prone to migration and loosening during and after surgery, leading to unstable fixation (14–17). As surgeons may bend both K-wires ends for stability, removal necessitates cutting a bent end through extended incisions. In this study, 6 cases of wire migration were observed. Additionally, the long ends of the K-wires can irritate the surrounding soft-tissues (18), as seen in 6 cases in this study. However, in our study, 74.5% of patients in the K-wires group underwent hardware removal after fracture healing, which imposed additional economic burdens and surgical risks on these patients. The ring-pins group is similar in surgical technique to the tension band with K-wires, but the wire passing through the ring-pins forms a single unit, which reduced the risk of migration (6, 19) and fixation failure (4, 19). The shorter ends of the K-wires cause less soft-tissue irritation, effectively alleviating postoperative knee pain and allowing for early functional rehabilitation (20). This method combines the simplicity and minimal bone damage of the tension band with K-wires with the advantages of the tension band with cannulated screws.
In this study, there were no significant differences in surgery duration, hemoglobin decrease, time from injury to surgery, or hospital stay among the three surgical methods, and the costs of surgery were similar. This indicates that the complexity of the three surgical techniques is comparable, and the financial burden on patients is similar. The ring-pins group and the K-wires group had slightly longer surgery duration than the cannulated screws group, which may be related to the additional steps of adjusting the depth of the K-wires and bending and cutting their ends. The larger diameter of the cannulated screws causes more bone damage, resulting in a greater hemoglobin decrease in the cannulated screws group compared to the other two groups. Surgeons should consider the patient's bone quality, preoperative hemoglobin levels, and overall condition when selecting the appropriate internal fixation method. The VAS scores before and after surgery showed that all three surgical methods significantly alleviated pain, achieving the surgical goals. The K-wires group had worse knee function scores at 3 months postoperatively compared to the ring-pins group and the cannulated screws group (P < 0.05). However, there was no significant difference in knee function scores at 12 months postoperatively, which may be related to the higher complication rates (e.g., wire migration, soft-tissue irritation) and higher hardware removal rates in the K-wires group. In the K-wires group, hardware removal at 12 months significantly improved knee function scores (P < 0.001), suggesting that timely hardware removal can alleviate pain and dysfunction caused by complications. The high rate of wire migration in the K-wires group may be related to the following factors: (1) The majority of patients in this study were elderly (mean age: 64.1 years), with a high prevalence of osteoporosis and poor bone quality. (2) The smooth surface of the K-wires and the bending of only one end can lead to loosening after fracture healing. (3) Repeated knee flexion and extension can cause deformation of the K-wires, leading to bone resorption due to pressure on the surrounding bone. For elderly patients with osteoporosis, the ring-pins group and the tension band with cannulated screws can reduce the risk of wire migration. Postoperative anti-osteoporosis treatment and rehabilitation should also be standardized.
The optimal fixation method for patellar fractures remains debated, with plate osteosynthesis emerging as a viable alternative to traditional tension band wiring. According to Bickel et al, tension band wiring and locked plating showed comparable 1-year functional outcomes (21). Biomechanical analyses suggest that fixed-angle plate osteosynthesis of the patella offers significantly greater stiffness and lower fracture gap dehiscence than the other fixation methods (22). Siljander et al. reported favorable outcomes with low-profile mesh plates, demonstrating lower complication rates compared to tension band wiring, which is often associated with hardware irritation and secondary surgeries (23).
5 Conclusion
Compared to the other two groups, the ring-pins group demonstrated several advantages, including a broad range of applications, low postoperative complication rates, and ease of implant removal. This method provides a superior treatment experience for patients, characterized by low surgical complexity and favorable postoperative recovery of knee function, making the ring-pins technique a preferred option for patellar fracture surgery.
However, this study has certain limitations. As a retrospective analysis, surgical outcomes may have been influenced by variations in surgeons' skill levels. Additionally, the follow-up period was relatively short, requiring further evaluation of medium- to long-term outcomes. Future studies should incorporate extended follow-up durations to better evaluate the outcomes of these techniques.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Shanghai Yangpu District Shidong Hospital (2023-061-01). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
X-DL: Formal analysis, Writing – review & editing, Methodology, Conceptualization, Writing – original draft, Investigation, Data curation, Visualization. KD: Methodology, Validation, Conceptualization, Supervision, Writing – review & editing, Project administration, Resources, Software, Funding acquisition.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by grant from the Shanghai Yangpu District Science and Technology Committee and Shanghai Yangpu District Health Committee (Grant No. YPM202307).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kim S, Mungalpara N, Wangikar R, Tarabichi M, Joseph K, Bedi A, et al. Comparative study of locking neutralization plate construct versus tension band wiring with a cannulated screw for patella fractures: experimental and finite element analysis. J Orthop Surg Res. (2024) 19:77. doi: 10.1186/s13018-024-04538-w
2. Hargett DI, Sanderson BR, Little MTM. Patella fractures: approach to treatment. J Am Acad Orthop Surg. (2021) 29:244–53. doi: 10.5435/JAAOS-D-20-00591
3. Henrichsen JL, Wilhem SK, Siljander MP, Kalma JJ, Karadsheh MS. Treatment of patella fractures. Orthopedics. (2018) 41:e747–55. doi: 10.3928/01477447-20181010-08
4. Kyung MG, Lee SH, Kim MB. Complications related to implant fixation of patellar fractures: comparison of ring pins versus bent K-wires. J Knee Surg. (2017) 30:560–4. doi: 10.1055/s-0036-1593621
5. Lee K-H, Lee Y, Lee YH, Cho BW, Kim MB, Baek GH. Biomechanical comparison of three tension band wiring techniques for transverse fracture of patella: Kirschner wires, cannulated screws, and ring pins. J Orthop Surg (Hong Kong). (2019) 27:2309499019882140. doi: 10.1177/2309499019882140
6. Kim MB, Lee YH, Shin WC, Baek GH. Locked tension band wiring using ring pins for patellar fractures: a method of minimising implant migration. Arch Orthop Trauma Surg. (2014) 134:1537–43. doi: 10.1007/s00402-014-2071-z
7. Böstman O, Kiviluoto O, Nirhamo J. Comminuted displaced fractures of the patella. Injury. (1981) 13:196–202. doi: 10.1016/0020-1383(81)90238-2
8. Aitken RC. Measurement of feelings using visual analogue scales. Proc R Soc Med. (1969) 62(10):989–93. doi: 10.1177/003591576906201005
9. Galla M, Lobenhoffer P. [Patella fractures]. Chirurg. (2005) 76:987–97; quiz 998–999. doi: 10.1007/s00104-005-1081-3
10. Steinmetz S, Brügger A, Chauveau J, Chevalley F, Borens O, Thein E. Practical guidelines for the treatment of patellar fractures in adults. Swiss Med Wkly. (2020) 150:w20165. doi: 10.4414/smw.2020.20165
11. Jirangkul P, Kosiyatrakul A. Abstaining from symptomatic implants of modified tension band wiring by nonabsorbable suture fixation for transverse patella fractures. J Orthop Surg Res. (2021) 16:367. doi: 10.1186/s13018-021-02494-3
12. Drolia N, Sinha S, Paneru SR, Kumar A, Jameel J, Kumar S, et al. Comparison of functional and radiological outcomes of transverse patellar fractures fixed with tension band fixation using cannulated screws and Kirschner wires: a prospective randomized study. Indian J Orthop. (2022) 56:369–76. doi: 10.1007/s43465-021-00498-z
13. Steiner JA, Ferguson SJ, van Lenthe GH. Screw insertion in trabecular bone causes peri-implant bone damage. Med Eng Phys. (2016) 38:417–22. doi: 10.1016/j.medengphy.2016.01.006
14. Choi H-R, Min K-D, Choi S-W, Lee B-I. Migration to the popliteal fossa of broken wires from a fixed patellar fracture. Knee. (2008) 15:491–3. doi: 10.1016/j.knee.2008.06.005
15. Lazaro LE, Wellman DS, Sauro G, Pardee NC, Berkes MB, Little MTM, et al. Outcomes after operative fixation of complete articular patellar fractures: assessment of functional impairment. J Bone Joint Surg Am. (2013) 95:e96.1–8. doi: 10.2106/JBJS.L.00012
16. Meena S, Nag HL, Kumar S, Barwar N, Mittal S, Singla A. Delayed migration of K-wire into popliteal fossa used for tension band wiring of patellar fracture. Chin J Traumatol. (2013) 16(3):186–8. doi: 10.3760/cma.j.issn.1008-1275.2013.03.012
17. Oyama H, Takegami Y, Tokutake K, Murase F, Arakawa O, Oguchi T, et al. Predictors of postoperative complications of tension band wiring techniques for patella fracture: a retrospective multicenter (TRON group) study. Injury. (2023) 54:110896. doi: 10.1016/j.injury.2023.110896
18. Hoshino CM, Tran W, Tiberi JV, Black MH, Li BH, Gold SM, et al. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Joint Surg Am. (2013) 95:653–9. doi: 10.2106/JBJS.K.01549
19. Jian Z, Jia J, Zeng L, Li D, Zhang X, Zhou J, et al. Ring-pins combined with cable cerclage for the fixation of displaced inferior patellar pole fractures. Front Surg. (2022) 9:1043822. doi: 10.3389/fsurg.2022.1043822
20. Liu J, Ge Y, Zhang G, Zheng X, Gao L, Xing E, et al. Clinical outcomes of cannulated screws versus ring pin versus K-wire with tension band fixation techniques in the treatment of transverse patellar fractures: a case-control study with minimum 2-year follow-up. Biomed Res Int. (2022) 2022:5610627. doi: 10.1155/2022/5610627
21. Bickel S, Jensen KO, Klingebiel FK-L, Teuben MPJ, Pfeifer R, Pape H-C, et al. Clinical and functional outcomes of locked plating vs. cerclage compression wiring for AO type C patellar fractures- a retrospective single-center cohort study. Eur J Trauma Emerg Surg. (2024) 50:2975–85. doi: 10.1007/s00068-024-02633-5
22. Wild M, Eichler C, Thelen S, Jungbluth P, Windolf J, Hakimi M. Fixed-angle plate osteosynthesis of the patella—an alternative to tension wiring? Clin Biomech (Bristol). (2010) 25:341–7. doi: 10.1016/j.clinbiomech.2009.12.010
Keywords: tension band with ring-pins, cannulated screws, transverse fractures of the patella, internal fixation, fractures abstract, surgery
Citation: Li X-D and Du K (2025) Comparison of the therapeutic effects of three internal fixation methods for transverse fractures of the patella. Front. Surg. 12:1633670. doi: 10.3389/fsurg.2025.1633670
Received: 23 May 2025; Accepted: 17 July 2025;
Published: 30 July 2025.
Edited by:
Kyun-Ho Shin, Nanoori Hospital, Republic of KoreaReviewed by:
Erwin Kollig, Zentralkrankenhaus der Bundeswehr, GermanySherwan Hamawandi, Hawler Medical University, Iraq
Copyright: © 2025 Li and Du. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kewei Du, ZHVrZXdlaUB1c3N0LmVkdS5jbg==