 Jasmina Burdzovic Andreas
Jasmina Burdzovic Andreas Anne Line Bretteville-Jensen
Anne Line Bretteville-Jensen- Department of Alcohol, Tobacco, and Drugs, Norwegian Institute of Public Health, Oslo, Norway
Objective: Adolescents who refrained from using cannabis despite having opportunities to do so represent an increasingly relevant group amid concerns about growing cannabis availability. We identified such cannabis-resilient adolescents and examined how they may differ from other youth especially in terms of prevention-relevant characteristics such as cannabis-specific contexts and cognitions.
Methods: Based on their self-reported cannabis use and direct use opportunities (i.e., use offers), we identified three groups from a nationally-representative cross-sectional sample of Norwegian high school students (N = 3,425; 47.8% boys, Mage = 18.2 ± 1.05): cannabis-naïve (no use/no offers; 59%), cannabis-resilient (no use despite the offers; 20.6%), and cannabis-using (20.3%). Multinomial regression models examined these three groups in relation to multiple socio-demographic, individual-level, and cannabis-related characteristics, focusing on cannabis-specific contexts (e.g., indirect use opportunities, access to cannabis) and cognitions [e.g., descriptive norms, perceived risks from trying cannabis, health knowledge, motivations for (non)use].
Findings: Overall, cannabis-specific contexts but not cannabis-specific cognitions differentiated cannabis-resilient and cannabis-naive students, whereas cannabis-specific cognitions but not cannabis-specific contexts differentiated cannabis-resilient and cannabis-using students. Among other factors, more accurate cannabis descriptive norms, health knowledge and risk perceptions, as well as more legal and personal reasons for non-use were significantly associated with cannabis resilience vs. use.
Conclusion: Use opportunities represent necessary but not sufficient conditions for cannabis use, as cannabis-specific cognitions differentiated cannabis-resilient from cannabis-using students notwithstanding shared exposures. Consideration of these potentially modifiable protective factors—cannabis-related knowledge and (non)use motives in particular—may be vital for person-centered initiatives across social contexts increasingly marked by cannabis availability and accessibility.
Introduction
Given its well-documented associations with multiple adverse health and psychosocial outcomes, cannabis use poses a significant, yet preventable risk for adolescent health and development (1–5). The nature of this risk is rapidly evolving, as reflected in the prolific selection of novel and more potent cannabis products readily available through the emerging legal and decriminalized markets (6–9). These structural changes involving greater physical availability and accessibility of cannabis are of particular concern as drug exposures and use opportunities—tangible situations where drugs such as cannabis are available and can easily be used if so desired—represent both the necessary conditions for cannabis initiation (10–17) and putative risks for more hazardous use patterns (9, 18, 19). Indeed, legal frameworks outlawing cannabis largely operate at this contextual level by aiming to reduce availability of the drug, the ensuing exposures and use opportunities, and ultimately, the use itself. However, the illegal status of cannabis—and its thereby presumed limited availability—can no longer serve as a prevention cornerstone. Given these legislative and structural shifts, there is a growing need for evidence-based research of relevance to novel person-centered prevention strategies.
One way to inform such strategies may be to focus on understanding adolescents' reasoning behind the decision whether to engage in cannabis use given an opportunity to do so (20–22). Specifically, those who decided against cannabis use despite use opportunities may be a highly relevant and informative group amid concerns of growing physical availability and social legitimacy of cannabis. Such adolescents may be understood within resilience framework (23–25), as they remained cannabis-free despite encountering the necessary risk conditions (i.e., physical opportunities) for initiation. Understanding factors that may differentiate these youth from their cannabis-using peers with whom they shared identical drug exposures can indeed provide valuable prevention-relevant insights.
These questions were addressed in an emerging international literature (17, 26), which identified a set of risk and protective factors—including socio-demographic characteristics, parental substance use and monitoring, and adolescents' behavioral and temperamental traits—associated with (non)resilience in face of cannabis use opportunities. While providing the significant initial steps in understanding differences between cannabis-resilient and cannabis-using youth, many of these characteristics remain of limited prevention utility given their hardly modifiable nature. And even though both of these international studies (17, 26) also pointed at the importance of risk perceptions, knowledge, and attitudes, we still know relatively little about such cannabis-specific cognitions that may be underlying resilience processes among youth faced with direct opportunities to use cannabis.
This study extends the current literature by examining adolescents' responses to direct opportunities to use cannabis in relation to their cannabis-specific contexts and cognitions. Specifically, as recent research underscored the role of cognitions in underage cannabis use (27)—including health beliefs (28, 29), risk perceptions and knowledge (30, 31), and motives and reasons for both use and non-use (20, 32, 33)—we explored these characteristics among youth who remained drug-free despite having received concrete offers to use cannabis. We did so while accounting for a range of additional factors relevant to substance use among young people, reflecting socio-demographic characteristics of both adolescents and their families (34–37), adolescents' individual-level characteristics reflecting their temperament, health, and use of other substances (38–42), and finally, adolescents' cannabis-specific contexts reflecting their additional exposures to cannabis.
Specifically, in this exploratory report based on a large nationally representative sample of Norwegian high school students we aimed to:
1. Identify and classify adolescents according to their cannabis involvement, reflecting not only their cannabis use but also their direct opportunities to do so. Based on prior literature, we expected to identify three core groups of adolescents: cannabis-using; cannabis-naïve (no use/no direct use opportunity), and—most importantly—cannabis-resilient (no use despite direct use opportunities).
2. Compare these three cannabis-involvement groups on a range of prevention-relevant characteristics, focusing on cannabis-specific contexts and—most importantly—cannabis-specific cognitions of the resilient group.
Closer exploration of these resilient youth and the putatively protective cognitions that contribute to their decision-making can prove informative for the development of education and public health strategies during periods characterized by increasing availability and accessibility of cannabis.
Materials and methods
Participants
We analyzed data from CANN2021 study, which recruited students from 34 high schools from across Norway to obtain a nationally representative sample of this adolescent population (43, 44). Because the school enrollment procedures in Norway are primarily based on the birth cohort year, majority of adolescents (97.7%) enter the 3-year academic or the 4-year vocational high school program at the age of 16 (45), translating to ages 16–17 in the first year (i.e., Grade 11), ages 17–18 in the second year (i.e., Grade 12) and ages 18–19 in the third year (i.e., Grade 13) of high school. Our targeted CANN2021 sample size was designated to be in close alignment with other key regional monitoring efforts, specifically the European School Survey Project on Alcohol and Other Drugs (ESPAD) for Norway, Sweden, and Finland (46, 47).
Student participants anonymously completed e-questionnaires focusing on their cannabis involvement and experiences broadly defined as part of a regular school hour between February 25 and April 10, 2021. All 34 participating schools thus completed data collection within the designed time-window during the 2021 Spring semester. Out of 4,122 initially eligible students from 236 classrooms, a total of 3,490 students (48.4% boys) from 210 classrooms completed e-questionnaires corresponding to 89% classroom, and 84.7% individual student participation rate. Our analytical sample for this report consisted of 3,425 students (47.8% boys, Mage = 18.2 ± 1.05) who provided valid data on their cannabis involvement, including any life history of cannabis use and/or encountered offers to use cannabis.
The study received IRB approval by the Norwegian Institute of Public Health (P-360: 21/11430-1). Because the core e-survey was anonymous and students were 16 years old or older, no parental consent was required, and the students themselves consented through participation after having received both written and oral information about the study. Study design, including detailed sampling, recruitment, and reimbursement procedures were described in detail previously (43, 44).
Measures
Cannabis involvement groups
Participants reported if they ever (a) used cannabis and (b) encountered direct use opportunities in the form of cannabis offers, but haven't used the drug. These two questions were used to classify students into three groups reflective of their cannabis involvement: (1) students who reported neither cannabis use nor receiving use offers (i.e., cannabis-naïve group); (2) students who reported no cannabis use despite receiving at least one offer to use cannabis (i.e., cannabis-resilient group), and (3) students who reported any lifetime cannabis use (i.e., cannabis-using group).
Socio-demographic characteristics
These characteristics were known either from the sampling and data-collection procedures, or were reported by the participants. These include the participants' gender (coded as “Boy” vs. “Rest”); school type (Vocational/Academic) and grade (11th, 12th, or 13th, corresponding to ages 16–19 in Norway); family structure (re-coded into “Non-intact biological family” vs. “Rest”); parental education (re-coded into three categories of either Both/At least one/Neither parent with a college degree); immigrant background based on country of birth for themselves and their parents (re-coded into “Immigrant background” vs. “Rest” following the official Statistics Norway definitions); and community of residence (Urban/Rural).
Individual-level characteristics
Participants' reports of their Norwegian, English, and math GPA were recoded to indicate whether they were failing at least one subject in school (Yes/No). Sensation seeking was assessed with a 4-item short Zuckerman Sensation Seeking scale specifically developed to tap into temperamental domains associated with adolescent substance use (40, 41); students' responses on a 5-point Likert scale were averaged such that the greater scale scores indicated greater sensation seeking (Cronbach's alpha = .79). Impulsivity was assessed with four items selected from the longer 8-item Barrat Impulsivity Scale (42); students' responses on a 4-point Likert scale were recoded and averaged such that the greater scale scores indicated greater impulsivity (Cronbach's alpha = .61). The participants' ratings of their mental and physical health on a 5-point Likert scale were dichotomized to reflect poor physical health and poor mental health respectively (coded as “Very poor/Poor” vs. “Rest”). Participants' reports of their lifetime tobacco and alcohol use histories were recoded to reflect mutually exclusive tobacco use categories of either “None”, “Cigarettes only”, “Snus only”, or “Both cigarettes and snus” and alcohol use categories of either “None”, “Alcohol use without blackouts history”, or “Alcohol use with blackouts history”.
Cannabis-specific contexts and cognitions
Participants' reports of situations where others were using cannabis but they themselves did not were recoded to reflect any indirect exposure to cannabis use opportunities (“Yes” vs. “Rest”) whereas their affirmative responses to the question asking if it would be easy for them to obtain cannabis were recoded to reflect easy access to cannabis (“Easy access” vs. “Rest”).
In addition to these two measures of their cannabis-specific contexts, students completed a module assessing their cannabis-specific cognitions. Participants' beliefs about how many of their classmates tried cannabis reflected their cannabis descriptive norms (48) and were recoded into “None/Don't know”, “Some to up to half”, “Half or more” response categories. Participants' non-affirmative responses on six items assessing their perceptions of health, social, and other risks from trying cannabis (46, 49, 50) were summed up to create a 0–6 index reflecting the extent of their perceptions of no risks from trying cannabis. Participants' erroneous responses on five items assessing possible negative health consequences of cannabis use (31, 49) were summed up to create a 0–5 index reflecting the extent of their cannabis health misconceptions. Participants motivations for and expectations from cannabis use were assessed with the 6-item Marijuana Motives Measure (MMM) (51, 52), composed of the two top-loading items each from the Social Motives (Cronbach's alpha = .87), Coping Motives (Cronbach's alpha = .76), and Conformity Motives (Cronbach's alpha = .81) subscales. The original 3-point responses (“Disagree”/“Neither Agree nor Disagree”/“Agree”) were averaged to create the corresponding Social, Coping, and Conformity motivations for cannabis use such that the greater scores reflected greater endorsement of a given motivation. Finally, participants endorsements of any of the three health (e.g., “Cannabis can harm my health.”), two legal (e.g., “I do not want to do anything illegal.”), and one personal reason (e.g., “Using cannabis is against my beliefs.”) for not using (more) cannabis (20, 32) were summed up to create corresponding indices for various reasons for cannabis non-use.
Analyses
Based on their self-reported histories of cannabis use and cannabis offers, all student participants were classified into three cannabis involvement groups: cannabis-naïve, cannabis-resilient, and cannabis-users. Then, crude and fully adjusted multinomial regression models were used to examine the associations between these three groups and multiple risk and protective factors, including (a) socio-demographic characteristics (i.e., gender, school grade, school type, family structure, parental education, immigrant background, and urbanity), (b) individual-level characteristics (i.e., school subject failure, sensation seeking, impulsivity, self-rated physical and mental health, and extensive histories of tobacco and alcohol use), and (c) cannabis-specific contexts (i.e., indirect use opportunities, easy access to cannabis) and cognitions (i.e., beliefs about others' use, perceived risks from cannabis use, misconceptions about health effects of cannabis use, motivations for cannabis use and non-use).
No weighting procedures were utilized because the sample was representative of the Norwegian high school students in terms of key sampling indicators, and closely aligned with the general population of Norwegian 17–19 year olds (44). Similarly, no missing data procedures were utilized to account for 65 participants who did not respond to the question assessing cannabis use history. Missingness on the remaining variables was low, and whenever possible, missing values were conservatively recoded into the “Rest” or “No risk” categories during dichotomization/categorization procedures.
We reported how we determined our sample size, all data exclusions (if any), all manipulations, and all measures in the study, and we follow JARS (53). All analyses were performed in Stata v. 18 (54). The main multinomial regression model addressing our key research questions was estimated with Stata's -mlogit command while accounting for clustering at the school level with the -vce (cluster school-variable) option. The resulting estimates were reported as the adjusted Relative Risk Ratios (aRRR)—commonly interpreted as Odd Ratios (OR)—with corresponding 95% CI. The data that support the findings of this study are not publicly available due to ethical reasons and privacy conditions imposed by the consent procedures. The study design and analyses were not pre-registered, and the results should therefore be considered exploratory.
Results
Cannabis involvement groups
A total of 695 (20.3%) participants reported having used cannabis at least once during lifetime. Among students who never used cannabis, 707 (or 20.6% of the entire sample) reported at least one direct use opportunity (i.e., at least one cannabis offer) and were classified as cannabis-resilient, while the remaining 2,023 participants (or 59.1% of the entire sample) reported no exposure to direct use opportunities and were thus classified as cannabis-naïve. Socio-demographic, individual-level, and cannabis-related characteristics of our analytical sample across these three cannabis-involvement groups are shown in Table 1. Crude associations between these variables and the three cannabis-involvement groups show a general dose-response pattern such that the lowest risk categories tended to be associated with the cannabis-naïve group whereas the greatest risk categories tended to be associated with the cannabis-using group.
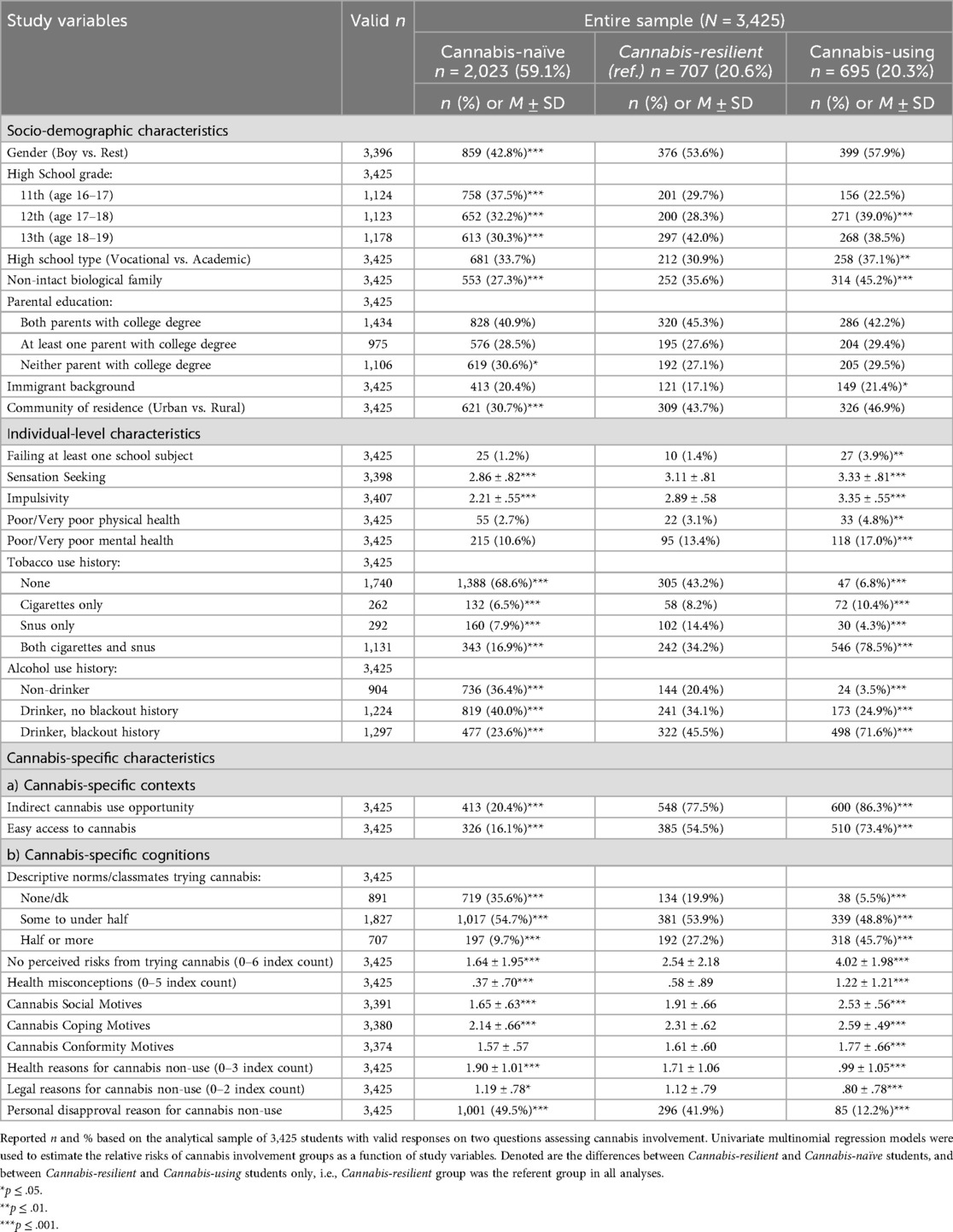
Table 1. Sample characteristics and study variables by cannabis involvement groups.
Cannabis involvement as a function of cannabis-specific contexts and cognitions
Cannabis-resilient vs. cannabis-naïve group
Results from the adjusted multinomial examining associations between all study variables and the three cannabis-involvement groups are shown in Table 2. Specifically, the profiles of cannabis-resilient and cannabis-naïve students were almost identical in terms of their socio-demographic and individual-level characteristics, such that—save for gender, family structure, urban residence, and tobacco use history—there were no significant differences in the associations between the school grade, school type, parental education, immigrant background, subject failure, sensation seeking, impulsivity, and self-rated physical and mental health across these two groups. However, significantly greater cannabis-specific contexts—such as indirect cannabis use opportunities and easy access to cannabis—were differentiating cannabis-resilient from the cannabis-naïve students. Students with beliefs that half or more of their classmates tried cannabis already and students with greater misconceptions concerning negative health effects of cannabis use were also significantly more likely to be in the cannabis-resilient than in the cannabis-naïve group, as were the students with greater endorsement of social motives but lower endorsement of conformity motives for cannabis use. Finally, there were no significant differences in the associations between the remaining cannabis-specific cognitions—including perceived risks from trying cannabis; coping motives/expectations of cannabis use; and health, legal, and personal reasons for cannabis non-use—and these two groups of high school students who never used cannabis.
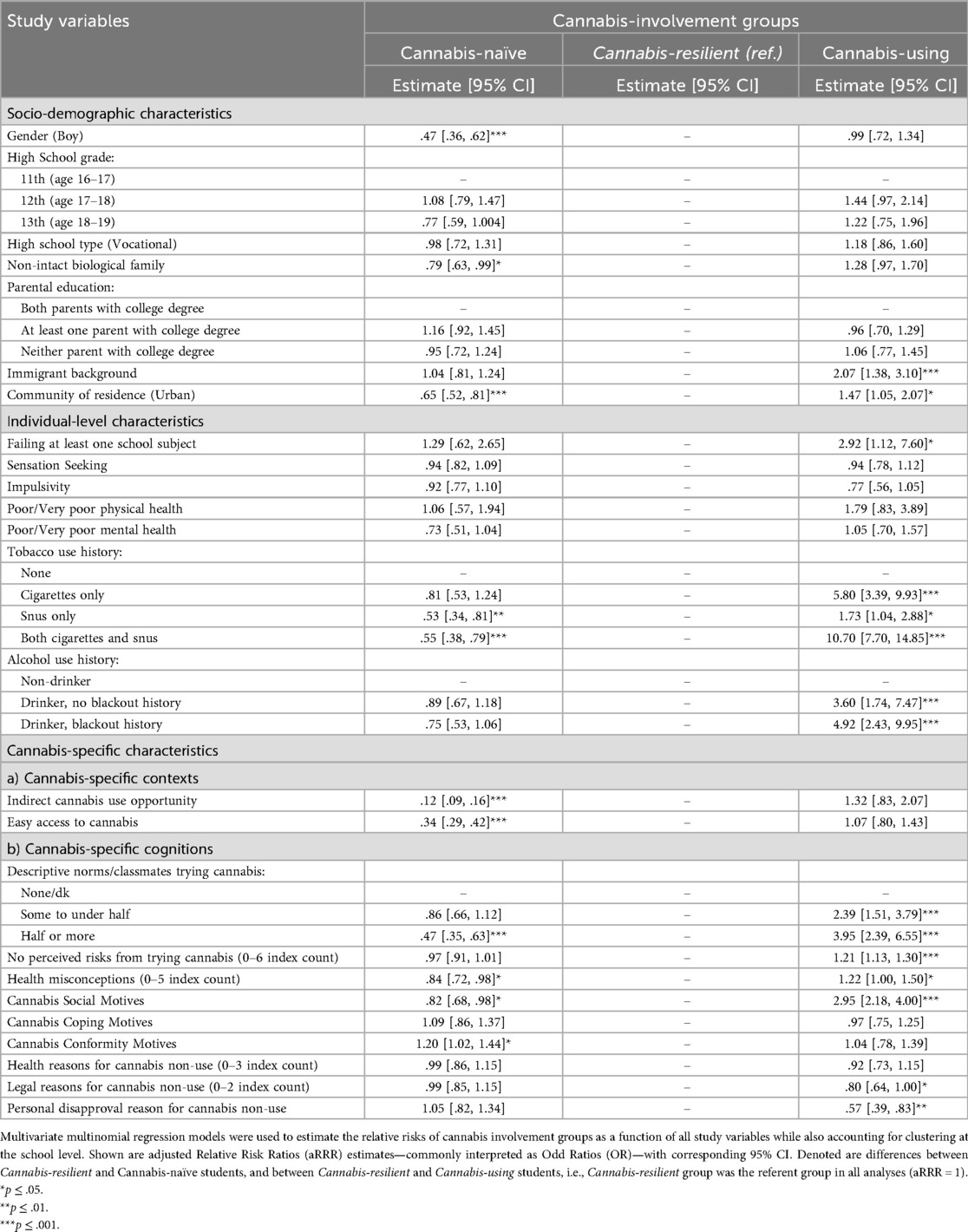
Table 2. Likelihood of cannabis involvement in a particular group as a function of adolescent's socio-demographic, individual-level, and cannabis-specific characteristics, n = 3,313.
Cannabis-resilient vs. cannabis-using group
In contrast, cannabis-resilient and cannabis-using groups diverged to a greater extent in terms of their socio-demographic and individual-level characteristics, such that students from urban communities, students from immigrant-background families, students failing at least one subject, and students with more extensive tobacco and alcohol use histories were significantly less likely to be in the cannabis-resilient than in the cannabis-using group. However, cannabis-specific contexts—such as passive cannabis use opportunities and easy access to cannabis—were not differentiating cannabis-resilient from the cannabis-using students, suggesting that these two groups shared similar cannabis-laden environments and related physical exposures. Most importantly, there were significant differences in the associations between cannabis-specific cognitions and these two groups of high school students exposed to direct cannabis use opportunities, suggesting that that such cognitions may have served as protective factors to buffer against heavier cannabis-specific contexts encountered by these youth. Specifically, students who did not believe some or most of their classmates tried cannabis; students who did not perceive trying cannabis as a no risk activity across multiple domains; students who had lower cannabis health misconceptions; students who endorsed lower social motives for cannabis use; and students who listed more legal and personal reasons for not using cannabis were all more likely to associated with the cannabis-resilient vs. cannabis-using group.
Sensitivity analyses
Our cannabis-involvement groups were conservatively based on the direct cannabis use opportunities in the form of cannabis offers, whereas indirect use opportunities were accounted for as a covariate. To consider these broader and more common cannabis exposures, we conducted a sensitivity analysis where such cases were also considered in our classification of resilience. Thus, the questions about both direct (i.e., offers) and indirect (i.e., settings where cannabis was used) use opportunities were used to classify students into three groups reflective of their cannabis involvement: (1) students who reported neither cannabis use nor any exposure to cannabis use opportunities (i.e., cannabis-naïve group); (2) students who reported no cannabis use despite direct and/or indirect use opportunities (i.e., cannabis-resilient group), and (3) students who reported any lifetime cannabis use (i.e., cannabis-using group). As in the main analyses, multinomial regression models were used to examine the associations between these three groups and all study variables, with the exception of indirect cannabis use opportunity.
These procedures again identified three groups of students: cannabis-naïve (no use/no cannabis exposure of any kind; n = 1,606 or 46.9%), cannabis-resilient (no use despite exposure; n = 1,124 or 32.8%), and cannabis-using (n = 695 or 20.3%). The results from our multinomial regression model using these groups substantively aligned with our main results, especially in terms of cannabis-specific cognitions as a protective factor against both direct and indirect cannabis use opportunities. Specifically, students who did not believe some or most of their classmates tried cannabis (aRRR = .42, 95% CI = .27–.64, and aRRR = .22, 95% CI = .14–.36, respectively); students who did not perceive trying cannabis as a no risk activity across multiple domains (aRRR = .83, 95% CI = .78–.89); students who had lower cannabis health misconceptions (aRRR = .75, 95% CI = .61–.91); students who endorsed lower Social Motives for cannabis use (aRRR = .33, 95% CI = .25–.44); and students who listed more legal and personal reasons for not using (more) cannabis (aRRR = 1.25, 95% CI = 1.02–1.53; aRRR = 1.71, 95% CI = 1.21–2.42) were all more likely to be associated with this alternative cannabis-resilient vs. cannabis-using group.
Discussion
Because cannabis use is predicated on its physical availability and accessibility, understanding adolescent cannabis use remains incomplete without consideration of such cannabis-specific contexts, associated exposures and use opportunities (12–16). Yet, understanding cannabis non-use within rapidly expanding cannabis contexts (6–9) may be more informative for prevention strategies that can no longer lean on the illegal status of the drug. That is, adolescents who resist direct cannabis use opportunities are ever more relevant group amid concerns about growing availability and legitimacy of cannabis. Using a nationally-representative sample of Norwegian high school students, we extended the extant literature by identifying such cannabis-resilient adolescents (17, 26), and by exploring cannabis-specific contexts and cognitions potentially differentiating them from other—both cannabis-using and non-using—youth.
Our results show that cannabis use was relatively common in this population: in line with recent Norwegian reports on cannabis use among adolescents (34, 55), one in five high school students (20.3%) from our nationally representative sample reported having used cannabis at least once. More importantly, just as many students (20.6%) reported that they have encountered but resisted direct use opportunities in the form of cannabis offers. Between these cannabis-using and cannabis-resilient adolescents, a total of four in ten high school students from Norway encountered at least one opportunity to use cannabis—a rather high rate in a cultural and legal setting characterized by relatively low prevalence of underage use and stricter cannabis policies (56, 57). If all of these adolescents availed themselves of received offers, the estimated lifetime prevalence of cannabis use in this population would have doubled from 20.3% to 41%.
What are the characteristics of these resilient youth, and how may they compare with youth without any cannabis involvement and with youth who yielded to cannabis use opportunities? The results from our multinomial regressions provide a useful profile of this group, both in terms of its associated risk and protective factors. Overall, cannabis-resilient and cannabis-naive youth were different mainly in terms of their riskier cannabis contexts but similar in terms of multiple protective factors, while cannabis-resilient and cannabis-using youth were similar in terms of their riskier cannabis contexts but different mainly in terms of multiple protective factors. Not surprisingly, cannabis-naïve youth were by definition not exposed to any direct cannabis offers, and contextual risk factors such as urban residence, indirect use opportunities, easy access to cannabis, and beliefs that their classmates are cannabis-users were significantly associated with the exposed, yet resilient group. More importantly, potentially protective cannabis-specific cognitions—save for cannabis health misconceptions and beliefs about why young people use cannabis—did not significantly differentiate cannabis-resilient from cannabis-naïve youth. Such pattern of results indicates that these two groups were alike on a range of cognitive characteristics including their perceptions of greater risks associated with trying cannabis; their lower endorsement of coping motives/expectations from cannabis use; and their greater health, legal, and personal disapproval reasons for cannabis non-use.
In contrast, cannabis-resilient and cannabis-using youth were both by definition exposed to cannabis use opportunities, and contextual risk factors such as indirect use opportunities and easy access to cannabis were not significantly differentiating these two groups. Nevertheless, immigrant background, urban residence, and beliefs that all of their classmates are cannabis-users were significantly associated with the cannabis-using group—perhaps suggesting an additional level of contextual risks. More importantly, potentially protective cannabis-specific cognitions—save for coping and conformity motivations/expectations from cannabis use, and health-related reasons for non-use—did significantly differentiate cannabis-resilient from cannabis-using youth. Such pattern of results indicates that these two groups were different on a range of cognitive characteristics including their perceptions of risks associated with even trying cannabis; misconceptions about the health effects of cannabis use; social motives/expectations from cannabis use; and legal and personal disapproval reasons for cannabis non-use.
The entirety of our findings extends the limited literature on cannabis use opportunities (10–17) and underscores the value of understanding such cannabis-resilient youth in prevention frameworks (17, 26, 58). These results provide an initial set of cannabis-involvement profiles relevant to public health and prevention strategies in multiple ways. First, our profiles aid in screening of at-risk groups, as they distinguish a number of structural (e.g., urban communities), familial (e.g., parental separation or immigrant background), and individual-level characteristics (e.g., boys, students with academic or substance use problems) associated with greater odds of cannabis involvement among youth. In addition to addressing cannabis-specific contexts to reduce adolescents' physical exposures to cannabis (which may be increasingly challenging in the global deregulation trends), relevant person-centered strategies may be informed by these results both in terms of resources allocation (e.g., to urban communities) and in terms of tailored and targeted deliveries (e.g., targeting students experiencing school or substance use problems). Second, our results aid in identification of possible avenues for prevention, as they also distinguish a number of cannabis-specific cognitions associated with greater odds of cannabis resilience among cannabis-exposed youth. As these cognitions are potentially modifiable, they could be addressed through information or education campaigns for example.
Indeed, our results reiterate the role of cannabis-specific risk perceptions and health beliefs/knowledge (28–31) but in the narrower context of resilience against direct cannabis offers. Specifically, our students characterized by greater perceptions of even trying cannabis as risky and students with greater health knowledge were more likely to be cannabis-resilient than cannabis-using despite their shared use opportunities. Even though our findings are based on a cross-sectional sample, they nevertheless point at the public health relevance of facts-based cannabis education among youth. As a recent review (31) noted, “(…) strategies that seek to increase knowledge among youth about the potential health harms of cannabis use should continue and be prioritized.”
Further, not surprisingly, students with lower social motives for cannabis use were more likely to be in the cannabis-resilient vs. cannabis-using group. These results again align with known risk and protective factors for cannabis use among young people, where social reasons such as having fun with friends are often the most common motivations for trying and using cannabis (51, 52, 59). Finally, students with greater legal and personal reasons for not using (more) cannabis were also more likely to be in the cannabis-resilient vs. cannabis-using group. Without engaging the debate on the deterring role of drugs prohibition among youth (60, 61), these results underscore the value of personal disapproval of illegal activities and drug use—an often overlooked dimension in understanding of drug use (62, 63) that needs to be conceptually separated from stigmatization (64).
In conclusion, although fairly common in our national sample of Norwegian high school students, cannabis use opportunities represent necessary but not sufficient conditions for use, as multiple cannabis-specific cognitions differentiated cannabis-resilient from cannabis-using youth notwithstanding shared direct exposures.
Limitations
This study's strong features such as a nationally representative sample of high school students and a large sample size notwithstanding, several caveats are warranted. First, the cross-sectional study design precludes any causal inferences. For example, the key questions concerning the causal association between perceived risks from substance use and substance use itself (65) could not be feasibly addressed in our study. And while it is possible that the cannabis-using youth lowered their risk evaluations once they started using cannabis, such trends do not necessarily negate the protective role of greater risk perceptions among the non-using, resilient youth.
Second, the veracity and reliability of students' self-reports are well-known limitations of survey methodology, and this may be especially relevant in the reporting of still illegal behaviors such as cannabis use. Such biases could result in under-estimates of use and possibly misclassification of our three cannabis-involvement groups of students. Indeed, our approach was rather conservative as we narrowly focused on the most salient form of use opportunities, that is, on cannabis offers (15, 17). Yet, the results from our sensitivity analyses where we considered both direct and indirect cannabis exposures entirely aligned with our main results and identified protective cognitions. It is also worth mentioning that if all students who were offered cannabis and/or witnessed others' use also joined in such activities, the lifetime prevalence of cannabis use among Norwegian high school students would have more than doubled. That is, in the absence of self-restraining cognitions and other protective factors, more than half of this population could have easily at least tried cannabis if not progressed into heavier use patterns.
Third, we did not utilize any advanced missing data procedures, and a handful of cases were deleted from analyses due to the non-responses on key outcome variables such as cannabis use history. It is unknown whether such non-responders imparted any bias.
Finally, the nature and additional characteristics of the examined cannabis offers were not known. We do not know if these offers entailed sales or sharing situations; if they were made in intimate or public settings; or if they were extended by close friends, romantic partners, or third parties. We also did not consider the frequency of either these offers or of actual cannabis use in our classification and regression models. All of these factors could have meaningfully shaped the participants' decisions whether or not to use cannabis and their ensuing cannabis use trajectories. Similarly, in this report we did not explore the role of gender, of socio-economic status, or of other relevant characteristics beyond including them in our regression models as covariates. Future research on cannabis use opportunities should aim to better integrate these important aspects and thoroughly explore their associations with the abstinence from, transitions into, and progressions of cannabis use among young people.
Conclusion
Using a nationally-representative sample of Norwegian high school students, we identified and examined three groups of adolescents in relation to their cannabis involvement: those who neither used cannabis nor had any direct opportunities to do so (i.e., cannabis-naïve); those who never used cannabis despite encountering at least one direct use opportunity in the form of cannabis offer (i.e., cannabis-resilient), and those who have used cannabis at least once (i.e., cannabis-using). Cannabis use opportunities were fairly common and experienced in some form by roughly four in ten students; half of which successfully resisted a direct use offer to remain non-users. Such cannabis-resilient students shared more risky cannabis-specific contexts with cannabis-using, and more protective cannabis-specific cognitions with cannabis-naïve students. Consideration of these protective cognitions common to all non-using youth—cannabis-related beliefs, knowledge, and use motives in particular—may be essential in initiatives targeting underage cannabis use across social contexts increasingly marked by cannabis availability, accessibility, and use opportunities.
Data availability statement
The dataset used in this article is not readily available because the data that support the findings of this study are not publicly available due to privacy and ethical reasons imposed by the consent procedures. Requests to access the dataset should be directed toYW5uZS5saW5lLmJyZXR0ZXZpbGxlLWplbnNlbkBmaGkubm8=.
Ethics statement
The study involving human subjects was approved by the Norwegian Institute of Public Health (P-360: 21/11430-1). The study was conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because the core e-survey was anonymous and students were 16 years old or older and legal adults for the purposes of research participation according to the Norwegian law. Therefore, no parental consent was required, and the students themselves consented through survey participation after having received both written and oral information about the study.
Author contributions
JBA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. ALB-J: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Data collection was partially supported by the Norwegian Health Directorate (Hdir), which had no role in study design; in the collection, analysis, or interpretation of the data; or in writing and submission of the manuscript for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gobbi G, Atkin T, Zytynski T, Wang S, Askari S, Boruff J, et al. Association of cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood: a systematic review and meta-analysis. JAMA Psychiatry. (2019) 76(4):426–34. doi: 10.1001/jamapsychiatry.2018.4500
2. Lorenzetti V, Hoch E, Hall W. Adolescent cannabis use, cognition, brain health and educational outcomes: a review of the evidence. Eur Neuropsychopharmacol. (2020) 36:169–80. doi: 10.1016/j.euroneuro.2020.03.012
3. Scheier LM, Griffin KW. Youth marijuana use: a review of causes and consequences. Curr Opin Psychol. (2021) 38:11–8. doi: 10.1016/j.copsyc.2020.06.007
4. Hall W, Leung J, Lynskey M. The effects of cannabis use on the development of adolescents and young adults. Annu Rev Dev Psychol. (2020) 2(1):461–83. doi: 10.1146/annurev-devpsych-040320-084904
5. Tuvel AL, Winiger EA, Ross JM. A review of the effects of adolescent cannabis use on physical health. Child Adolesc Psychiatr Clin N Am. (2023) 32(1):85–105. doi: 10.1016/j.chc.2022.07.005
6. Spindle TR, Bonn-Miller MO, Vandrey R. Changing landscape of cannabis: novel products, formulations, and methods of administration. Curr Opin Psychol. (2019) 30:98–102. doi: 10.1016/j.copsyc.2019.04.002
7. Freeman TP, Groshkova T, Cunningham A, Sedefov R, Griffiths P, Lynskey MT. Increasing potency and price of cannabis in Europe, 2006-16. Addiction. (2019) 114(6):1015–23. doi: 10.1111/add.14525
8. Wilson J, Freeman TP, Mackie CJ. Effects of increasing cannabis potency on adolescent health. Lancet Child Adolesc Health. (2019) 3(2):121–8. doi: 10.1016/S2352-4642(18)30342-0
9. Manthey J, Jacobsen B, Hayer T, Kalke J, López-Pelayo H, Pons-Cabrera MT, et al. The impact of legal cannabis availability on cannabis use and health outcomes: a systematic review. Int J Drug Policy. (2023) 116:104039. doi: 10.1016/j.drugpo.2023.104039
10. Wagner FA, Anthony JC. Into the world of illegal drug use: exposure opportunity and other mechanisms linking the use of alcohol, tobacco, marijuana, and cocaine. Am J Epidemiol. (2002) 155(10):918–25. doi: 10.1093/aje/155.10.918
11. Gillespie NA, Neale MC, Kendler KS. Pathways to cannabis abuse: a multi-stage model from cannabis availability, cannabis initiation and progression to abuse. Addiction. (2009) 104(3):430–8. doi: 10.1111/j.1360-0443.2008.02456.x
12. Burdzovic Andreas J, Bretteville-Jensen AL. Ready, willing, and able: the role of cannabis use opportunities in understanding adolescent cannabis use. Addiction. (2017) 112(11):1973–82. doi: 10.1111/add.13901
13. Hines LA, Morley KI, Strang J, Agrawal A, Nelson EC, Statham D, et al. Onset of opportunity to use cannabis and progression from opportunity to dependence: are influences consistent across transitions? Drug Alcohol Depend. (2016) 160:57–64. doi: 10.1016/j.drugalcdep.2015.12.032
14. Siegel JT, Tan CN, Navarro MA, Alvaro EM, Crano WD. The power of the proposition: frequency of marijuana offers, parental knowledge, and adolescent marijuana use. Drug Alcohol Depend. (2014) 148:34–9. doi: 10.1016/j.drugalcdep.2014.11.035
15. Burdzovic Andreas J, Pape H. Who receives cannabis use offers: a general population study of adolescents. Drug Alcohol Depend. (2015) 156:150–6. doi: 10.1016/j.drugalcdep.2015.09.009
16. Van Etten ML, Neumark YD, Anthony JC. Initial opportunity to use marijuana and the transition to first use: United States, 1979-1994. Drug Alcohol Depend. (1997) 49(1):1–7. doi: 10.1016/S0376-8716(97)00127-0
17. Burdzovic Andreas J, Pape H, Bretteville-Jensen AL. Who are the adolescents saying “no” to cannabis offers. Drug Alcohol Depend. (2016) 163:64–70. doi: 10.1016/j.drugalcdep.2016.03.025
18. Cantor N, Silverman M, Gaudreault A, Hutton B, Brown C, Elton-Marshall T, et al. The association between physical availability of cannabis retail outlets and frequent cannabis use and related health harms: a systematic review. Lancet Reg Health Am. (2024) 32:100708. doi: 10.1016/j.lana.2024.100708
19. Myran DT, Imtiaz S, Konikoff L, Douglas L, Elton-Marshall T. Changes in health harms due to cannabis following legalisation of non-medical cannabis in Canada in context of cannabis commercialisation: a scoping review. Drug Alcohol Rev. (2023) 42(2):277–98. doi: 10.1111/dar.13546
20. Terry-McElrath YM, O'Malley PM, Johnston LD. Saying no to marijuana: why American youth report quitting or abstaining. J Stud Alcohol Drugs. (2008) 69(6):796–805. doi: 10.15288/jsad.2008.69.796
21. Patrick ME, Evans-Polce RJ, Kloska DD, Maggs JL. Reasons high school students use marijuana: prevalence and correlations with use across four decades. J Stud Alcohol Drugs. (2019) 80(1):15–25. doi: 10.15288/jsad.2019.80.15
22. Hecht ML, Warren JR, Wagstaff DA, Elek E. Substance use, resistance skills, decision making, and refusal efficacy among Mexican and Mexican American preadolescents. Health Commun. (2008) 23(4):349–57. doi: 10.1080/10410230802229720
23. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. (2000) 71(3):543–62. doi: 10.1111/1467-8624.00164
24. Masten AS, Hubbard JJ, Gest SD, Tellegen A, Garmezy N, Ramirez M. Competence in the context of adversity: pathways to resilience and maladaptation from childhood to late adolescence. Dev Psychopathol. (1999) 11(1):143–69. doi: 10.1017/S0954579499001996
25. Egeland B, Carlson E, Sroufe LA. Resilience as process. Dev Psychopathol. (1993) 5(4):517–28. doi: 10.1017/S0954579400006131
26. Lopez-Quintero C, Neumark Y. Prevalence and determinants of resistance to use drugs among adolescents who had an opportunity to use drugs. Drug Alcohol Depend. (2015) 149:55–62. doi: 10.1016/j.drugalcdep.2015.01.015
27. Foster DW, Ye F, Chung T, Hipwell AE, Sartor CE. Longitudinal associations between marijuana-related cognitions and marijuana use in African-American and European-American girls from early to late adolescence. Psychol Addict Behav. (2018) 32(1):104–14. doi: 10.1037/adb0000323
28. Bolts OL, Prince MA, Noel NE. Latent profiles of cannabis use, protective behavioral strategies, and health beliefs in college students. Addict Behav. (2023) 144:107747. doi: 10.1016/j.addbeh.2023.107747
29. Chadi N, Levy S, Weitzman ER. Moving beyond perceived riskiness: marijuana-related beliefs and marijuana use in adolescents. Subst Abus. (2020) 41(3):297–300. doi: 10.1080/08897077.2019.1635972
30. Terry-McElrath YM, O'Malley PM, Patrick ME, Miech RA. Risk is still relevant: time-varying associations between perceived risk and marijuana use among US 12th grade students from 1991 to 2016. Addict Behav. (2017) 74:13–9. doi: 10.1016/j.addbeh.2017.05.026
31. Harrison ME, Kanbur N, Canton K, Desai TS, Lim-Reinders S, Groulx C, et al. Adolescents’ cannabis knowledge and risk perception: a systematic review. J Adolesc Health. (2024) 74(3):402–40. doi: 10.1016/j.jadohealth.2023.09.014
32. Martz ME, Schulenberg JE, Patrick ME. Passing on pot: high school seniors’ reasons for not using marijuana as predictors of future use. J Stud Alcohol Drugs. (2018) 79(5):761–9. doi: 10.15288/jsad.2018.79.761
33. Anderson KG, Sitney M, White HR. Marijuana motivations across adolescence: impacts on use and consequences. Subst Use Misuse. (2015) 50(3):292–301. doi: 10.3109/10826084.2014.977396
34. Mæland R, Lien L, Leonhardt M. Association between cannabis use and physical health problems in Norwegian adolescents: a cross-sectional study from the youth survey Ungdata. BMC Public Health. (2022) 22(1):661. doi: 10.1186/s12889-022-13136-6
35. Khlat M, Van Cleemput O, Bricard D, Legleye S. Use of tobacco, alcohol and cannabis in late adolescence: roles of family living arrangement and socioeconomic group. BMC Public Health. (2020) 20(1):1356. doi: 10.1186/s12889-020-09476-w
36. Hemovich V, Crano WD. Family structure and adolescent drug use: an exploration of single-parent families. Subst Use Misuse. (2009) 44(14):2099–113. doi: 10.3109/10826080902858375
37. Steinhoff A, Bechtiger L, Birchler K, Ribeaud D, Eisner M, Quednow BB, et al. Cannabis use from early adolescence to the mid-twenties in children of immigrant and nonimmigrant parents: findings from a prospective longitudinal cohort study. Int J Ment Health Addict. (2024). doi: 10.1007/s11469-024-01359-0
38. Chan O, Daudi A, Ji D, Wang M, Steen JP, Parnian P, et al. Cannabis use during adolescence and young adulthood and academic achievement: a systematic review and meta-analysis. JAMA Pediatr. (2024) 178(12):1280–9. doi: 10.1001/jamapediatrics.2024.3674
39. Hammond CJ, Chaney A, Hendrickson B, Sharma P. Cannabis use among U.S. adolescents in the era of marijuana legalization: a review of changing use patterns, comorbidity, and health correlates. Int Rev Psychiatry. (2020) 32(3):221–34. doi: 10.1080/09540261.2020.1713056
40. Sargent JD, Tanski S, Stoolmiller M, Hanewinkel R. Using sensation seeking to target adolescents for substance use interventions. Addiction. (2010) 105(3):506–14. doi: 10.1111/j.1360-0443.2009.02782.x
41. Zuckerman M. Behavioral Expressions and Biosocial Bases of Sensation Seeking. New York, NY: Cambridge University Press (1994).
42. Steinberg L, Sharp C, Stanford MS, Tharp AT. New tricks for an old measure: the development of the Barratt impulsiveness scale–brief (BIS-brief). Psychol Assess. (2013) 25(1):216–26. doi: 10.1037/a0030550
43. Bretteville-Jensen AL, Burdzovic Andreas J. CANN2021 survey and registry-linkages cohort on cannabis involvement among Norwegian high school students: design, measures, and sample characteristics. BMJ Open. (2025) 15:e092475. doi: 10.1136/bmjopen-2024-092475
44. Bretteville-Jensen AL, Burdzovic Andreas J, Dahl SL, Heider Hov D. CANN2021: En studie om cannabiserfaringer, kunnskap og holdninger blant elever på videregående skoler (CANN2021: a study on cannabis-related experinces, knowledge, and attitudes among high school students). Oslo, Norway: Folkehelseinstituttet; (2022).
45. Statistics Norway Division for Education and Culture Statistics. Facts about education in Norway 2021 – key figures 2019. Statistics Norway; Division for Education and Culture Statistics; (2019).
46. ESPAD Group. ESPAD Report 2019: Results from the European School Survey Project on Alcohol and Other Drugs, Publications Office of the European Union. Luxembourg: EMCDDA Joint Publications (2020).
47. Raitasalo K, Kraus L, Bye EK, Karlsson P, Tigerstedt C, Törrönen J, et al. Similar countries, similar factors? Studying the decline of heavy episodic drinking in adolescents in Finland, Norway and Sweden. Addiction. (2021) 116(1):62–71. doi: 10.1111/add.15089
48. Mbaba M, AuBuchon KE, Dodge T. The influence of descriptive and injunctive norms on U.S. adolescent marijuana use: a systematic review of the literature. J Stud Alcohol Drugs. (2022) 83(3):312–22. doi: 10.15288/jsad.2022.83.312
49. Leos-Toro C, Fong GT, Meyer SB, Hammond D. Cannabis health knowledge and risk perceptions among Canadian youth and young adults. Harm Reduct J. (2020) 17(1):54. doi: 10.1186/s12954-020-00397-w
50. Balneaves LG, Hammond D, Turner S, Nickel N, Woodgate RL, Watling CZ. Youth and young adults’ knowledge and perceptions of risks and benefits regarding cannabis products: a cross-sectional analysis of over 1,700 individuals. J Psychoact Drugs. (2025) 57(3):347–56. doi: 10.1080/02791072.2024.2371028
51. Simons J, Correia CJ, Carey KB, Borsari BE. Validating a five-factor marijuana motives measure: relations with use, problems, and alcohol motives. J Couns Psychol. (1998) 45(3):265–73. doi: 10.1037/0022-0167.45.3.265
52. Zvolensky MJ, Vujanovic AA, Bernstein A, Bonn-Miller MO, Marshall EC, Leyro TM. Marijuana use motives: a confirmatory test and evaluation among young adult marijuana users. Addict Behav. (2007) 32(12):3122–30. doi: 10.1016/j.addbeh.2007.06.010
53. Kazak AE. Editorial: journal article reporting standards. Am Psychol. (2018) 73(1):1–2. doi: 10.1037/amp0000263
56. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). (2019). Norway, Country Drug Report 2019.
57. Egnell S, Villman E, Obstbaum-Federley YC. Cannabis policy and legislation in the Nordic countries: a report on the control of cannabis use and possession in the Nordic legal systems. Stockholm: Nordic Welfare Centre (2019). p. 146.
58. Neumark Y, Lopez-Quintero C, Bobashev G. Drug use opportunities as opportunities for drug use prevention: Bogota, Colombia a case in point. Drug Alcohol Depend. (2012) 122(1–2):127–34. doi: 10.1016/j.drugalcdep.2011.09.022
59. Lee CM, Neighbors C, Woods BA. Marijuana motives: young adults’ reasons for using marijuana. Addict Behav. (2007) 32(7):1384–94. doi: 10.1016/j.addbeh.2006.09.010
60. Smyth BP, Davey A, Keenan E. Deterrence effect of penalties upon adolescent cannabis use. Ir J Psychol Med. (2023):1–6. doi: 10.1017/ipm.2023.5
61. Smyth BP, James P, Cullen W, Darker C. “So prohibition can work?” Changes in use of novel psychoactive substances among adolescents attending a drug and alcohol treatment service following a legislative ban. Int J Drug Policy. (2015) 26(9):887–9. doi: 10.1016/j.drugpo.2015.05.021
62. Palamar JJ. Predictors of disapproval toward “hard drug” use among high school seniors in the US. Prev Sci. (2014) 15(5):725–35. doi: 10.1007/s11121-013-0436-0
63. Salas-Wright CP, Vaughn MG, Todic J, Córdova D, Perron BE. Trends in the disapproval and use of marijuana among adolescents and young adults in the United States: 2002-2013. Am J Drug Alcohol Abuse. (2015) 41(5):392–404. doi: 10.3109/00952990.2015.1049493
64. Vanyukov MM. Stigmata that are desired: contradictions in addiction. Addict Res Theory. (2024) 32(2):83–92. doi: 10.1080/16066359.2023.2238603
Keywords: cannabis (marijuana), adolescents, cannabis exposure, resilience, cognition, contexts
Citation: Burdzovic Andreas J and Bretteville-Jensen AL (2025) Adolescents' resilience in the face of cannabis use offers: the role of cannabis-specific contexts and cognitions. Front. Adolesc. Med. 3:1653788. doi: 10.3389/fradm.2025.1653788
Received: 25 June 2025; Accepted: 29 September 2025;
Published: 23 October 2025.
Edited by:
Sheryl Ryan, Penn State Milton S. Hershey Medical Center, United StatesReviewed by:
Tammy Chung, Rutgers, The State University of New Jersey, United StatesElitsa Dimitrova, Institute for Population and Human Studies - Bulgarian Academy of Sciences, Bulgaria
Copyright: © 2025 Burdzovic Andreas and Bretteville-Jensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jasmina Burdzovic Andreas, amFidUBmaGkubm8=