 Helena Baecher1*
Helena Baecher1* Bhagvat Maheta2
Bhagvat Maheta2 Lisa-Marie Lottner3
Lisa-Marie Lottner3 Adriana C. Panayi1
Adriana C. Panayi1 Samuel Knoedler4
Samuel Knoedler4 Fernando Guastaldi5
Fernando Guastaldi5 João F. Mano6
João F. Mano6 Steffen Koerdt1
Steffen Koerdt1 Carsten Rendenbach1
Carsten Rendenbach1 Max Heiland1
Max Heiland1 Leonard Knoedler1†
Leonard Knoedler1† Christian Doll1†
Christian Doll1†- 1Department of Oral and Maxillofacial Surgery, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 2California Northstate University College of Medicine, Elk Grove, CA, United States
- 3Department of Oral and Maxillofacial Surgery, University Hospital Regensburg, Regensburg, Germany
- 4Department of Plastic Surgery and Hand Surgery, Klinikum rechts der Isar, Technical University of Munich, Munich, Germany
- 5Department of Oral and Maxillofacial Surgery, Massachusetts General Hospital, Harvard School of Dental Medicine, Boston, MA, United States
- 6Department of Chemistry, CICECO – Aveiro Institute of Materials, University of Aveiro, Aveiro, Portugal
Total joint reconstruction (TJR) is essential for the management of end-stage temporomandibular joint (TMJ) disorders. Current reconstruction techniques include the use of autologous grafts, such as chondrocostal tissue or fibula, and alloplastic TMJ replacement systems. Commercially available TMJ replacement systems provide both stock and customized prostheses. Advances in computer-aided design/computer-aided manufacturing technology, three-dimensional printing, and virtual surgical planning have accelerated the trend toward individualized TMJ prostheses, enhancing anatomical adaptation, intraoperative efficiency, and postoperative outcomes. A promising alternative under preclinical investigation is TMJ tissue engineering, a regenerative approach utilizing scaffolds, stem cells, and growth factors to reconstruct specific TMJ components, including the skeletal condyle, fibrocartilaginous disc, and glenoid fossa. Bioprinting has further transformed the field by enabling the creation of complex, multi-tissue structures with cellular viability and functionality. Techniques such as integrated tissue and organ printing and volumetric printing have shown promise for enhancing graft performance by improving scaffold heterogeneity. However, these advanced approaches remain in the preclinical stage and require critical evaluation before clinical translation. Despite these advancements, challenges such as high costs, technical complexities, and the need for extensive, robust datasets persist. Continued research into novel biomaterials, advanced biofabrication techniques, and digital surgical technologies, supported by larger preclinical and in vitro studies, is imperative to address these limitations and advance clinical applicability.
Introduction
Temporomandibular disorders (TMD) affect approximately 31%–34% of the global population, with a higher prevalence among females compared to males (Zieliński et al., 2024; Valesan et al., 2021). As a significant public health concern, the true burden of TMD is likely underestimated due to undiagnosed cases (Spotts, 2017). Although robust data on the proportion of TMD patients undergoing surgery are scarce, approximately 6% receive surgical intervention (Salinas et al., 2022). In severe instances, including end-stage temporomandibular joint (TMJ) diseases, congenital abnormalities, neoplasms, or trauma, surgical reconstruction of the TMJ may become necessary (Resnick, 2018; He et al., 2011; Schmidt et al., 2022; Gonzalez-Perez et al., 2023). In 2014, 572 alloplastic TMJ prostheses were implanted in the United States; projections indicate that 902 procedures are expected by 2030 (Onoriobe et al., 2016). However, techniques for TMJ reconstruction represent an essential area of research that has undergone constant development over the last few years.
The surgical approach varies based on the extent of pathological involvement, ranging from arthroscopic techniques or targeted discectomy to resection of the mandibular condyle, or total resection of the TMJ (Breik et al., 2016; Ângelo et al., 2022; Kreutziger, 1994). A schematic illustration of the TMJ is provided in Figure 1.
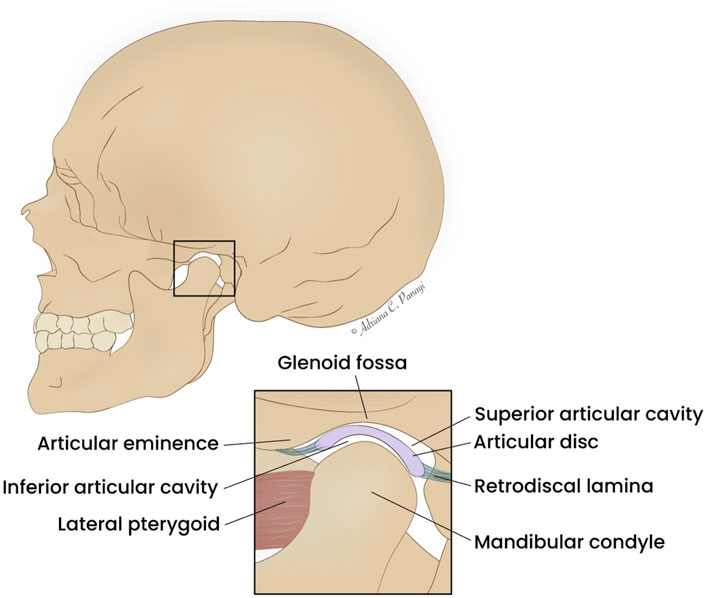
Figure 1. Schematic illustration of the TMJ. Created with Adobe Illustrator (Version 29.6, Adobe Inc., San Jose, California, United States).
Modern strategies for TMJ reconstruction integrate diverse surgical techniques, including revascularized tissue transfers, costochondral grafting, and alloplastic TMJ replacement. The choice of procedure depends on several patient-specific factors, such as age, underlying pathology, skeletal maturity, and the risk of compromising the contralateral joint’s function (Imola and Liddell, 2016). In most clinical scenarios, total TMJ replacement using alloplastic prostheses is the preferred approach. In contrast, autologous graft reconstruction is commonly chosen for growing children, patients undergoing adjuvant radiation following malignant tumor removal, and individuals in low-income settings (Pedersen et al., 2021; Borbon et al., 2023). The traditional view supports the use of autologous grafts in skeletally immature patients, emphasizing their potential to grow with the child and thereby reduce the risk of future facial asymmetry (Ko et al., 1999; Awal et al., 2018). Recent studies, however, have demonstrated the applications of customized alloplastic TMJ prostheses even in skeletally immature patients (Alba et al., 2024; Sinn et al., 2021; Hashemi et al., 2024).
Over recent decades, the development and application of alloplastic materials, along with advances in tissue-engineered solutions, have significantly expanded the options for TMJ replacement (Salash et al., 2016).
In the era of computer-aided design and manufacturing (CAD/CAM), three-dimensional (3D) printing, and virtual surgical planning (VSP), TMJ reconstruction has undergone significant advancements.
As a result, patient-specific TMJ prostheses designed through VSP have become a widely established approach, continuously undergoing refinements. Future perspectives focus on tissue engineering and bioprinting of TMJ tissues, offering the potential for biomimetic innovations. However, these technologies remain in preclinical stages and should be critically evaluated.
Furthermore, initial efforts have been made to integrate augmented reality and virtual reality into the field of TMJ surgery. These technologies provide preoperative support for condylar resection planning, prosthesis selection, and the identification of potential interferences. Additionally, they offer intraoperative real-time guidance for osteotomies, prosthesis placement, screw fixation, and occlusion verification (Niloy et al., 2024).
Despite these advancements, there remains a scarcity of comprehensive studies that condense the latest innovations in TMJ surgery. This research gap leaves untapped potential to leverage recent findings to improve TMJ patient care. To fill this research gap, this review aims to provide an encompassing overview of the recent developments in TMJ reconstruction and distill the most promising research findings.
State of the art–established techniques in TMJ reconstruction
Virtual surgical planning
Early TMJ surgery relied on manually shaping autologous grafts, such as costochondral or fibula free flaps, guided by anatomical landmarks and refined through intraoperative adjustments (Wax et al., 2000; Munro and Chir, 1980). However, this freehand shaping of the bone grafts into an accurately fitting condyle head is challenging, and inaccuracies in contouring the new TMJ can lead to mandibular dysfunction, impacting swallowing, speaking, and chewing (Wax et al., 2000). To improve outcomes, VSP integrated digital simulations and 3D models into preoperative workflows, enhancing precision (Raccampo et al., 2023). Advances in 3D printing and CAD/CAM technologies now enable tools like 3D-printed drilling guides, placement guides and patient-specific osteosynthesis plates in maxillofacial surgery, which aid in accurate graft shaping and synthesis (Myers et al., 2021; Rodby et al., 2014; Hadad et al., 2023).
In current clinical workflows, high-resolution computed tomography (CT) or cone-beam computed tomography (CBCT) scans are used to capture bony anatomy, in select cases supplemented by magnetic resonance imaging (MRI) for visualization of soft tissues and vascular structures. These datasets are imported as Digital Imaging and Communications in Medicine (DICOM) files into dedicated surgical planning software (e.g., Mimics, Materialise NV, Leuven, Belgium), where they are co-registered within a unified coordinate system to ensure accurate anatomical alignment. Using semi-automated or AI-assisted segmentation tools, individual anatomical regions, particularly the TMJ, are isolated and converted into 3D surface files (e.g., STL format). In subsequent design platforms (e.g., 3-matic, Materialise NV, Leuven, Belgium), osteotomy lines are defined, either as simple planar cuts or complex freeform curves, based on the clinical scenario. Prosthetic components are virtually designed, often in collaboration between biomedical engineers and surgeons, and adjusted according to anatomical landmarks and resection planes. Surgical guides for osteotomies and drilling are then modeled within the same planning environment and manufactured via 3D printing using biocompatible materials. These guides are typically aligned with the planned implant trajectory to ensure congruent intraoperative placement. Additionally, anatomical models of the mandible and prosthetic replicas may be printed to assist with surgical rehearsal and intraoperative reference. All components are thoroughly sterilized and quality-controlled prior to clinical use, enabling accurate, reproducible execution of the preoperative plan (Raccampo et al., 2023). A workflow of VSP and CAD/CAM-based fabrication of TMJ prostheses is represented in Figure 2.
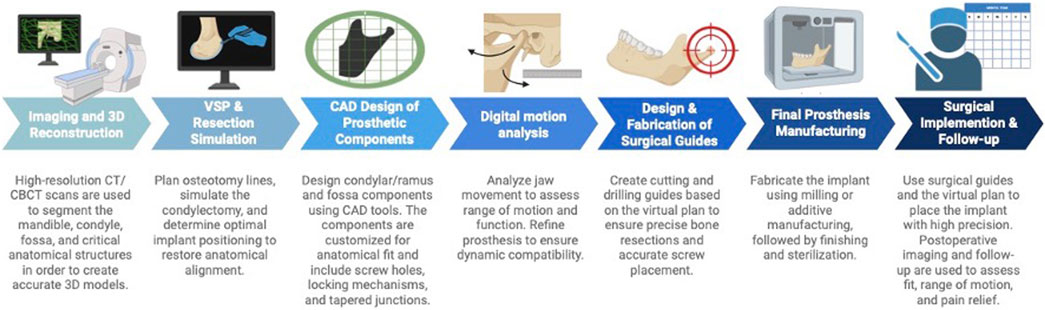
Figure 2. Workflow of VSP and CAD/CAM-based fabrication of TMJ prostheses. Created with BioRender (BioRender Inc., Toronto, Canada). Abbreviations: CAD/CAM. computer-aided design/computer-aided manufacturing, VSP: virtual surgical planning.
The integration of VSP with personalized CAD/CAM-produced devices was initially designed to enhance efficiency and support surgeons in TMJ reconstruction. This approach offers i) reduced surgical time, ii) improved accuracy through cutting and placement guides and precalculated contact surfaces, iii) enhanced aesthetic results iv) visualization of patient-specific anatomical variations before and during surgery, and v) precise margins in tumor resection scenarios prior to TMJ reconstruction (del Castillo Pardo de Vera et al., 2024; Mian et al., 2021; Dowgierd et al., 2021). With regard to alloplastic TMJ replacement, improved accuracy of the condylar position, reduced screw stress, and diminished contact stress on the condylar component remain the most significant benefits (Mian et al., 2021). Recent studies on the accuracy of TMJ prostheses implemented with VSP report highly precise positioning associated with long-term surgical success in the form of enhanced osseointegration and reduced micromovements (Neuhaus et al., 2021).
A study by Sawh-Martinez et al. evaluated the position of the condyle following mandibular reconstruction using CT imaging. The comparison between mandibular reconstructions with and without VSP demonstrated that VSP significantly improved precision, particularly by reducing superior and lateral shifts of the ipsilateral condyle, as well as minimizing changes in the condylar and condylar neck angles (Sawh-Martinez et al., 2017).
Current TMJ alloplastic replacement systems
Several commercially available TMJ replacement systems exist, including the Zimmer Biomet Microfixation System (Jacksonville, United States), patient-specific TMJ Concepts by Stryker (Ventura, United States), Materialise’s custom-made TMJ Total Arthroplasty System (Leuven, Belgium), and IPS Implants® by KLS Martin (Tuttlingen, Germany).
The Zimmer Biomet system offers both stock and customized prostheses, while the TMJ replacement systems by TMJ Concepts, Materialise, and KLS Martin are exclusively patient-specific (Kanatsios et al., 2018; Jones, 2011; Materialise, 2023; KLS Martin Group, 2024). Stock prostheses provide advantages such as immediate availability and lower costs compared to customized systems. Furthermore, preoperative planning is less time-intensive for stock prostheses (Gonzalez-Perez et al., 2016). However, these advantages are offset by the need for intraoperative adaptation, which may prolong surgical procedures (Olate et al., 2023). A significant limitation of stock prostheses is their reduced precision, as they cannot be perfectly tailored to individual patients. For instance, Abramowicz et al. reported that 23% of Biomet Microfixation stock prostheses failed to fit stereolithographic models of patients who subsequently required patient-specific joint prostheses (Abramowicz et al., 2012).
On the other hand, customized prostheses offered by all the mentioned manufacturers provide the benefits of patient-specific designs, enabling simplified intraoperative workflows, reduced bone modification, and enhanced precision in fitting (Mercuri, 2013). However, these advantages come at a higher cost, largely due to their complex manufacturing processes (Zheng et al., 2019).
All four systems are two-component designs consisting of a mandibular condyle and a glenoid fossa. The mandibular components of the Zimmer Biomet (stock/customized), TMJ Concepts, and Materialise systems comprise a cobalt-chromium-molybdenum (Co-Cr-Mo) alloy condylar head and a titanium alloy body, which is either entirely composed of titanium or features a plasma-sprayed titanium coating (Materialise, 2023; KLS Martin Group, 2024; Giannakopoulos et al., 2012; Aagaard and Thygesen, 2014). In contrast, the mandibular component of the KLS Martin system is manufactured entirely from a titanium alloy (KLS Martin Group, 2024). Remarkably, Zimmer Biomet offers a fully titanium alternative for the mandibular component in patients with verified nickel or Co-Cr allergies (Granquist et al., 2018). For all five systems, the fossa components are fabricated from ultra-high molecular weight polyethylene (UHMWPE). In the Zimmer Biomet system (stock/customized), the entire fossa component is composed of UHMWPE, whereas in the other systems, the UHMWPE articulating surface is secured to a titanium mesh backing (TMJ Concepts) or a metal base (Materialise and KLS Martin) (Materialise, 2023; KLS Martin Group, 2024; Giannakopoulos et al., 2012; Aagaard and Thygesen, 2014). Notably, all five systems provide cutting and/or positioning guides (Materialise, 2023; KLS Martin Group, 2024; Brown et al., 2016; Sembronio et al., 2021).
The stock Zimmer Biomet System received full approval by the US Food and Drug Administration (FDA) in 2005 and represents a well-established option in TMJ reconstruction, with available long-term outcomes (Giannakopoulos et al., 2012).
In contrast, the systems by Materialise and KLS Martin are relatively recent advancements. Consequently, long-term studies and robust evidence-based data for these systems are currently lacking. Notably, there exists a retrospective study on customized TMJ prostheses by Engimplan/Materialise Company (Rio Claro, Brazil), evaluating 22 patients over 2 years (Leandro et al., 2022). However, the high level of personalization offered by these prostheses, combined with insertion aids such as drilling and osteotomy guides, surgical splints, and TMJ trial implants for precise fossa component placement, provides significant advantages (Materialise, 2023; KLS Martin Group, 2024).
A summary of the materials used in alloplastic TMJ replacement systems is provided in Table 1.
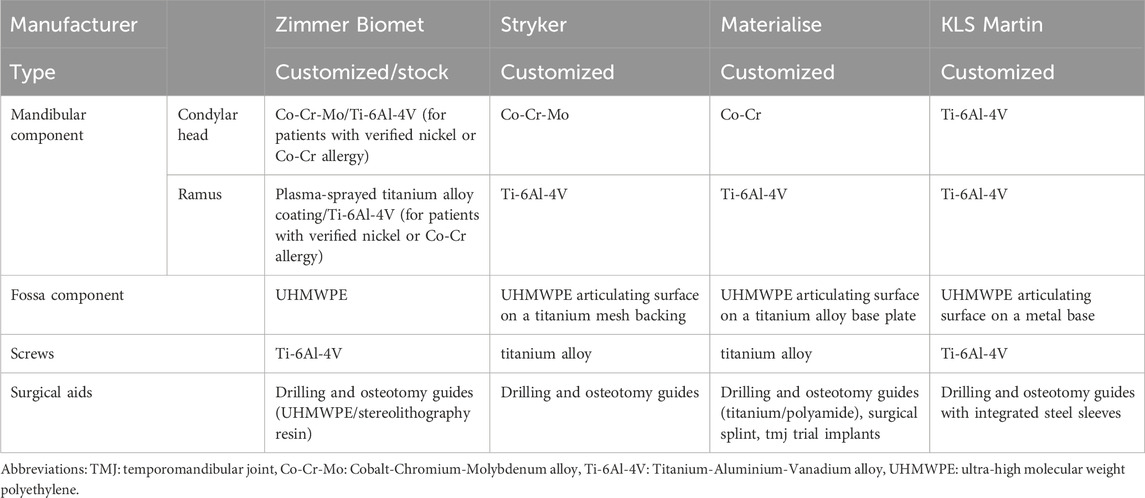
Table 1. Summary of materials used in different alloplastic TMJ replacement systems.
Alloplastic vs. autologous reconstruction
Before the advent of TMJ alloplastic replacement systems, and in cases where such implants are contraindicated, autologous TMJ reconstruction was, and continues to be, the preferred method. The most commonly used grafting tissues include costochondral grafts, sternoclavicular grafts, and free fibula grafts (Sidebottom, 2013).
Complications associated with costochondral grafts are reported in 51%–58% of patients and include infection, facial nerve weakness, malocclusion, and graft fracture due to overload. Especially, (re)ankylosis and graft overgrowth represent common issues (Awal et al., 2018; Sidebottom, 2013; Saeed et al., 2003). Revision surgery or implant removal is required in approximately 42% of cases (Saeed et al., 2003). Significant drawbacks of costochondral grafts are the unpredictable growth and the donor site morbidity, which can include chronic costochondritis pain and the risk of pleural disruption (Sidebottom, 2013; Sekhoto et al., 2019).
TMJ reconstructions using sternoclavicular grafts have been associated with complications such as joint ankylosis, foreign body giant cell reaction, graft destruction or fracture, and donor site morbidity, including clavicle fractures. Graft survival rates were 50% in patients with inflammatory TMJ pathology but reached 93% in those without inflammatory conditions or prior alloplastic TMJ reconstruction (Wolford et al., 1994).
Reconstruction of the mandibular condyle using a fibula free flap is predominantly performed in cases of mandibulectomy involving the condyle. Wax et al. reported postoperative fibular head displacement out of the fossa in 12% of cases, hypoperfusion of the graft requiring a second venous anastomosis in 6%, and asymptomatic bone exposure in 6% (Wax et al., 2000). In further studies, graft survival was reported as 100%. Preservation of the articular disc in most patients likely contributed to the absence of TMJ ankylosis (Wax et al., 2000; Gravvanis et al., 2017; Powers et al., 2022). Donor site morbidity is described in the literature as relatively low, including a limited range of motion in the ankle, ankle instability, and gait abnormalities (Rendenbach et al., 2016).
In clinical practice, alloplastic TMJ prostheses are the primary choice for TMJ replacement or reconstruction. The literature indicates low rates of removal and revision for these devices. Amarista et al. reported revision rates of 3% for patient-specific TMJ Concepts prostheses, 3% for stock Zimmer Biomet prostheses, and 2% for custom Zimmer Biomet prostheses (Amarista et al., 2020). Even in cases of extended TMJ replacement, treatment with TMJ prostheses has been demonstrated to be a safe and effective option for patients with TMJ deficits involving the mandible and/or the zygomatic arch (Gerbino et al., 2024).
Adverse events associated with alloplastic TMJ replacements include infection, nerve injuries (i.e., facial nerve, trigeminal nerve), neuropathic pain, and hearing disturbances, with an overall incidence of 5%–19% (Aagaard and Thygesen, 2014; Neff et al., 2020). A meta-analysis by Lima et al. identified the most common complications as facial nerve paresis or paralysis (8%), sensory disturbances (2%), heterotopic bone formation (1%), and infections (1%) (Peres Lima et al., 2023). Functional complications, such as hardware loosening and ankylosis, have also been reported, while multiple surgeries prior to TMJ replacement are associated with poorer outcomes (Neff et al., 2020; Rajkumar and Sidebottom, 2022; Sanovich et al., 2014; Handa et al., 2023). Notably, hypersensitivity or allergic reactions to prosthetic materials occur in approximately 11% of patients (Neff et al., 2020).
Implant survival rates are high, with a 2024 meta-analysis reporting a 97% survival rate over follow-up periods ranging from 12 months to 21 years (Lima et al., 2024). A long-term study by Wolford et al. documented a 100% implant survival with a median follow-up of 21 years (Wolford et al., 2015). A comparison of different options for TMJ reconstruction is provided in Table 2.

Table 2. Comparison of the different options for TMJ reconstruction.
TMJ replacement in children
Reconstruction of the TMJ in children presents a unique clinical challenge. The most common underlying conditions necessitating TMJ reconstruction include congenital deformities, neoplasms, ankylosis, and progressive resorptive diseases (Resnick, 2018). Early reconstruction of the mandible and TMJ has been shown to reduce the risk of facial asymmetry and growth disturbances affecting the mandible, maxilla, and midfacial skeleton. In addition, early intervention may mitigate the development of malocclusion, symptoms of CMD, obstructive sleep apnea, and psychosocial issues (Resnick, 2018). Despite early intervention, more than 50% of pediatric patients exhibit recurrent facial asymmetry by the time they reach skeletal maturity (Pluijmers et al., 2014). Traditional surgical paradigms advocate the use of autologous grafts in skeletally immature patients due to their potential for growth and remodeling, theoretically reducing the likelihood of future asymmetry (Ko et al., 1999; Awal et al., 2018). Costochondral grafts and vascularized free fibula flaps are the most established autologous options in this population. However, costochondral grafts are primarily composed of cortical bone and rely heavily on surrounding tissues for revascularization, which increases the risk of postoperative resorption compared to vascularized flaps (Resnick, 2018). Furthermore, the growth behavior of costochondral grafts is unpredictable. Reports have documented cases of overgrowth, undergrowth, and even lack of growth (Awal et al., 2018). Recent studies have explored the use of customized alloplastic TMJ prostheses in skeletally immature patients (Yang et al., 2015). Although alloplastic TMJ prostheses are considered the treatment of choice in adults, their use in growing patients remains controversial due to concerns about interference with craniofacial development and the potential need for future revision surgeries (Alba et al., 2024; Sinn et al., 2021; Hashemi et al., 2024). However, many children requiring TMJ reconstruction already exhibit severely disrupted mandibular growth patterns, and over half of autologous reconstructions eventually necessitate surgical revision (Keyser et al., 2020). A 10-year follow-up study of pediatric costochondral grafts reported revision surgery in 33% of cases due to recurrent ankylosis, in 16% due to overgrowth, and in 7% due to undergrowth (Awal et al., 2018).
A recent survey of 14 pediatric patients treated with customized alloplastic TMJ prostheses reported only two postoperative complications requiring surgical intervention: one infection and one case of heterotopic ossification. Bilateral reconstruction was performed in nine cases, and unilateral reconstruction in five. All patients demonstrated improved mandibular function, increased maximum interincisal opening (MIO), and no evidence of asymmetrical growth (Keyser et al., 2020). In a case series by Sinn et al., five pediatric TMJ reconstructions were performed using both stock and customized alloplastic devices. All cases showed improved MIO. Secondary procedures included orthodontic treatment and the use of a palatal expander in one patient, and surgical scar revision in another. Collectively, while the use of customized alloplastic TMJ prostheses in children remains controversial, emerging evidence suggests they may be a viable alternative in selected cases, particularly after failed autologous reconstruction.
Novel innovations and future perspectives
Total joint replacement
Total joint replacement is required in cases of end-stage TMJ disorders and involves the surgical replacement of the TMJ with an alloplastic prosthesis (Neff et al., 2020). The aim of total TMJ replacement is to restore both morphology and function, striving to replicate the native TMJ as closely as possible (Yadav et al., 2021). The FDA-approved materials for alloplastic joint prostheses include cobalt–chromium alloys, commercially pure titanium (cpTi), alloyed titanium (Ti6Al4V), and UHMWPE (Yadav et al., 2021).
Research is increasingly focused on optimizing accurate fitting by customized joint prostheses to restore optimal functions. A study by Ingawale et al. introduced a patient-specific TMJ prosthesis with novel features designed to enhance adaptation to each patient’s anatomic conditions. The surgeon can customize the shape and center of rotation of the condylar head, with the design being precisely adapted to the load-bearing conditions. The prosthesis incorporates perforated notches that extend into the host bone at implantation. The glenoid fossa design facilitates sufficient rotation and allows for anterior-posterior and medio-lateral translation. A modified design, featuring a rectangular slot with curved anterior and posterior edges and circumferential stabilization for the condylar head, ensures accurate fitting on the skeletal surface. Consequently, this study demonstrates that the introduced approach holds promise for stable total TMJ reconstruction, validated under both functional/normal and para-functional/worst-case TMJ loading scenarios (Ingawale and Goswami, 2022).
De Meurechy et al. developed an innovative, patient-specific 3D-printed titanium alloy TMJ replacement system designed to restore laterotrusive movements through the reinsertion of the lateral pterygoid muscle. Utilizing a sheep model, the study evaluated the efficacy of a HadSat® diamond-like carbon (H-DLC) coating for the condylar head, combined with a machined UHMWPE fossa component enriched with Vitamin E and subjected to γ-irradiation. The findings advocate for the combined use of H-DLC-coated titanium for the condyle and Vitamin E-stabilized UHMWPE for the fossa as a superior option for TMJ implant systems (De Meurechy et al., 2022).
In a sheep model, another research group investigated a novel, customized TMJ prosthesis that permits the reinsertion and integration of the lateral pterygoid muscle (LPM) into the prosthesis. This approach aimed to preserve LPM function and reduce excessive load on the contralateral joint through optimized load distribution. The methodology involved preserving the LPM enthesis and reattaching it to a scaffold at the condylar neck of the TMJ prosthesis. Again, an H-DLC coating was applied to the condylar head. Histological analysis demonstrated a functional fibrotic reintegration of the LPM onto the prosthesis, thereby successfully restoring muscle function (Mommaerts et al., 2025).
Tissue engineering–the future of TMJ reconstruction?
Tissue engineering for TMJ reconstruction focuses on three components: i) the skeletal condyle, ii) the fibrocartilaginous disc, and iii) the glenoid fossa and articular eminence (Aryaei et al., 2016; Acri et al., 2019). This process combines scaffolds, cells, and growth factors, but optimizing these elements for each anatomical component of the TMJ remains challenging (Acri et al., 2019).
Biological scaffolds which can be used for the reconstruction of the articular disc include decellularized extracellular matrix (ECM) sheets, fibrin, collagen, and chitosan (Acri et al., 2019). Synthetic scaffolds include PLA, PCL, polyglycolic acid (PGA), poly-L-lactic acid (PLLA), poly-L-lactic-co-glycolic acid (PLGA), and photopolymerized hydrogel polyethylene glycol diacrylate (PEGDA) (Singh et al., 2022). Notably, ongoing research also explores scaffold-free, self-assembling approaches for bioengineering articular discs (Vapniarsky et al., 2018).
Various cell types can be used to seed these scaffolds, comprising stem cells, induced pluripotent stem cells (iPSCs), and differentiated chondrocytes (Acri et al., 2019; Zhao et al., 2024).
Growth factors prominently used in articular disc engineering include transforming growth factor-β1 (TGF-β1), fibroblast growth factor (FGF), and insulin-like growth factor (IGF) (Johns and Athanasiou, 2008; Kalpakci et al., 2011).
In an in vitro study, Yi et al. investigated 3D-printed polymer scaffolds coated with polydopamine (PDA) and combined with decellularized extracellular matrix (dECM) hydrogel for TMJ disc reconstruction, reporting promising outcomes in promoting chondrogenesis and fibrogenesis (Yi et al., 2021).
For mandibular condyle engineering, scaffolds can include the mentioned synthetic materials but also mineralized components like hydroxyapatite (HA) (Ciocca et al., 2013; Konopnicki and Troulis, 2015). While synthetic materials offer the advantages of an unlimited supply and straightforward manufacturing, mineralized scaffolds closely mimic the native bone structure, provide enhanced mechanical strength, and exhibit osteoconductive properties (Acri et al., 2019; Howlader et al., 2017). A combination of MSCs and growth factors, such as TGF-β1, FGF, and BMP-2, can be used to bioengineer the skeletal condyle (Konopnicki and Troulis, 2015; Grayson et al., 2010).
Engineering the glenoid fossa poses significant challenges due to its complex morphology and cartilage-bone interface. Notably, only few studies have addressed this aspect (Aryaei et al., 2016). A 2019 review by Acri et al. proposed combining MSCs with calcium phosphate, HA, or PCL scaffolds and BMP-2, SOX9, and VEGF for the skeletal part. For cartilage engineering, they recommended using MSCs with PLA, PCL, or alginate scaffolds and growth factors like BMP-2, TGF-β1, or IGF-1 (Acri et al., 2019).
A summary of materials for tissue engineering is presented in Table 3, providing an updated version of the work by Acri et al. (2019).
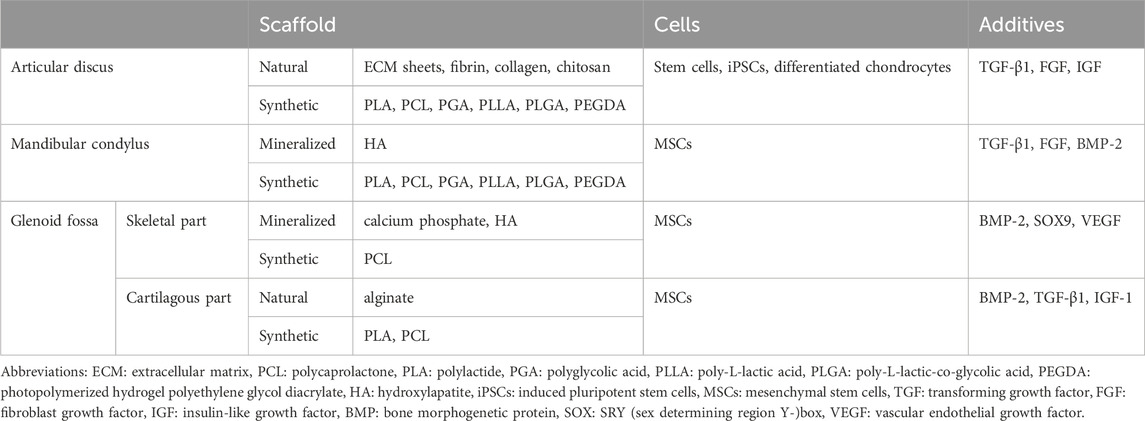
Table 3. Summary of materials for tissue engineering different parts of the TMJ.
Regenerative treatments using stem cells have demonstrated promising outcomes in the management of degenerative TMJ disorders, showing significant chondrogenic regenerative potential (De et al., 2019). This was exemplified in an animal study by Köhnke et al., where histological analysis revealed a substantial increase in cartilage thickness in stromal-cell-treated groups compared to untreated controls (Köhnke et al., 2021). These findings provide a valuable foundation for ongoing research in bioengineering and regenerative medicine. However, these regenerative approaches are primarily effective in early to moderate disease stages and require further validation in human trials (Matheus et al., 2022; Zhang et al., 2015).
Recent advancements in 3D printing
Bioprinting represents a cutting-edge development in tissue engineering, advancing the scope of reconstructive surgery by enabling the production of intricate, multi-tissue structures with cellular viability intact. Rooted in the principles of three-dimensional printing, bioprinting integrates living cells, biomaterials, and bioactive compounds into precise, layer-by-layer arrangements to mimic native anatomical tissues (Ramadan and Zourob, 2021). The foundation of bioprinting lies in data derived from advanced imaging modalities such as CT and MRI, which are converted into CAD-models for custom tissue fabrication. Techniques such as inkjet, extrusion, laser-assisted bioprinting (LAB), and stereolithography utilize these models to create patient-specific grafts tailored to the complex structures of the TMJ (Bishop et al., 2017).
Other more sophisticated biofabrication techniques, permitting a fast processing in volume and permitting the use of hydrogel-precursors with undesirable rheological properties to be extruded, should be considered in the future to produce such kind of complex structures, including digital-light processing or volumetric 3D printing (Li et al., 2023; Rodríguez-Pombo et al., 2022).
Reconstruction of the TMJ is challenging due to the structural diversity and biomechanical demands. Bioprinting offers a promising approach, enabling precise customization of each TMJ component to address these complexities effectively. Particularly, bioprinting of fibrocartilaginous tissue for the TMJ holds promising future prospects, driven by ongoing research into cartilage bioprinting techniques, including scaffold-based, scaffold-free, and in situ bioprinting approaches (Wu et al., 2021). While a substantial body of literature exists on cartilage bioprinting in fields such as bioprinting of the meniscus, intervertebral disc, ear, and nose, research specifically focused on bioprinting TMJ fibrocartilaginous tissue remains limited (Hu et al., 2023; Perera et al., 2021).
Helgeland et al. explored the use of genipin-crosslinked 3D-printed gelatin scaffolds as a promising platform for regenerating TMJ cartilage. Their findings highlighted the ability of these bioprinted scaffolds to enhance the attachment, survival, and chondrogenic differentiation of human bone marrow-derived mesenchymal stem cells (hBMSCs). This demonstrates the scaffolds’ potential for supporting cartilage tissue engineering in TMJ repair and regeneration applications (Helgeland et al., 2021).
Advanced printing methods, such as integrated tissue and organ printing (ITOP), allow for the simultaneous deposition of multiple bioinks (i.e., a combination of hydrogels, cellular components, and bioactive additives) to create composite tissues (Gungor-Ozkerim et al., 2018; Park et al., 2022; Kang et al., 2016). Additionally, the use of 3D-printed surgical guides facilitates accurate graft placement during implantation, further enhancing clinical outcomes (Park et al., 2022).
Despite its potential, bioprinting for TMJ reconstruction remains in a translational phase, with limited clinical application and minimal progress in animal models. Currently, only a few bioprinted tissues, such as dermal, skeletal, cartilagous, or hepatical tissue, have been successfully transplanted into animals (Yang et al., 2021; Di Bella et al., 2018; Alawi et al., 2023). Ongoing research focuses on optimizing scaffold materials, improving bioink formulations, and understanding cellular behavior within engineered tissues. While animal models have demonstrated promising outcomes, significant challenges remain in achieving long-term stability, integration, and functionality of bioprinted TMJ components (Hu et al., 2023; Salah et al., 2020). As bone tissue engineering using LAB and cartilage bioprinting have been explored in isolated studies involving mice, small animal models, such as mice and further rabbits, represent a logical next step in the translational advancement of bioprinting (Keriquel et al., 2017; Apelgren et al., 2019). Future perspectives in biomaterials and manufacturing techniques are summarized in a graphical abstract, as presented in Figure 3.
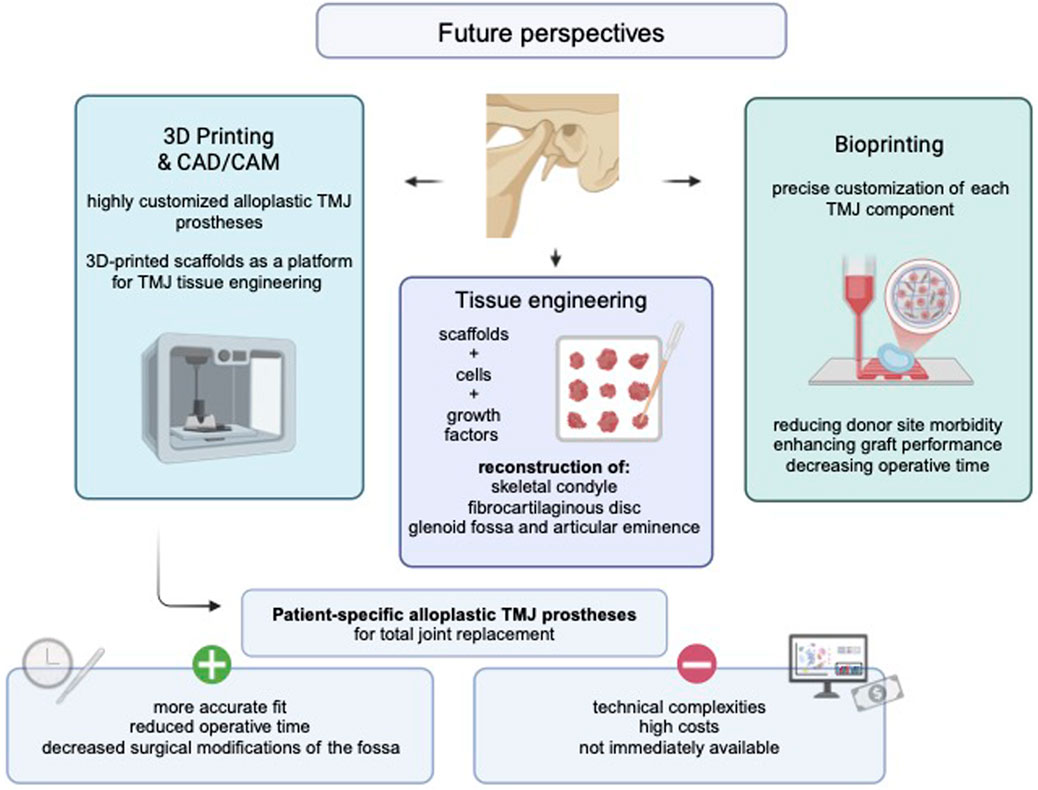
Figure 3. Graphical abstract presenting future perspectives in TMJ surgery. Created with BioRender (BioRender Inc., Toronto, Canada). Abbreviations: CAD/CAM. computer-aided design/computer-aided manufacturing, TMJ: temporomandibular joint.
Tissue-engineered TMJ components in the growing patient
As a forward-looking approach, tissue-engineered TMJ components represent a promising biological alternative, particularly in pediatric patients. Several studies have demonstrated the successful implantation of tissue-engineered organs in growing children. For example, in 2012, Elliott et al. reported the implantation of a tissue-engineered trachea in a 12-year-old patient, which remained functional and demonstrated growth compatibility over a 2-year follow-up period (Elliott et al., 2012). Similarly, tissue-engineered vascular grafts have been successfully used in children with congenital heart disease, showing favorable safety profiles and long-term feasibility (Sugiura et al., 2018). Notably, children may benefit even more than adults from engineered tissues that integrate fully with the host organism and adapt to somatic growth. Growth-adaptive grafts are capable of accommodating the dynamic anatomical changes of the developing craniofacial skeleton and promoting host-mediated remodeling. Moreover, long-term durability is a critical consideration in pediatric patients due to their extended life expectancy and the cumulative mechanical demands placed on reconstructive materials (Ott, 2012). Although tissue-engineered TMJ components remain in the preclinical stage, their future clinical translation holds particular promise for growing patients.
Approval pathways and ethical challenges
The FDA approval process for alloplastic TMJ devices follows the medical device regulatory pathway, typically requiring premarket approval (PMA) due to their classification as Class III devices, which involves rigorous evaluation of safety, efficacy, and long-term performance through clinical trials. Manufacturers must submit extensive data, including biocompatibility, mechanical testing, and clinical study outcomes (FDA, 2021). In contrast, tissue-engineered TMJ components fall under the category of combination products, involving both biologics and devices, and are regulated through a coordinated approach involving the Center for Devices and Radiological Health (CDRH) and the Center for Biologics Evaluation and Research (CBER) (NIH SEED, 2023). These constructs must undergo preclinical studies demonstrating functional integration, followed by Investigational New Drug (IND) applications and phased clinical trials before Biologics License Application (BLA) approval, making their translational pathway considerably more complex and time-intensive (Nordberg et al., 2022).
The use of alloplastic and tissue-engineered TMJ reconstruction in pediatric patients raises ethical concerns related to growth compatibility, long-term safety, and consent. Alloplastic devices may require multiple revision surgeries over a lifetime, while tissue-engineered constructs remain experimental with limited longitudinal data (Laventhal et al., 2012). Clinical studies involving children also face higher regulatory and ethical hurdles compared to adults, including stricter risk-benefit evaluations, assent requirements, and logistical challenges, which often result in fewer pediatric trials and delayed innovation (PREP, 2024). Key ethical issues include proxy decision-making, irreversible interventions, and the preservation of future treatment options.
Discussion
Recent advances in digital simulation and additive manufacturing have catalyzed a paradigm shift in TMJ reconstruction. Customized alloplastic prostheses, enabled by VSP, have markedly improved both functional and aesthetic outcomes, while emerging regenerative strategies such as tissue engineering and bioprinting offer promising new directions. However, the benefits, limitations, and current challenges associated with these innovations must be critically evaluated.
The integration of VSP has significantly advanced TMJ reconstruction by shifting from conventional freehand techniques to precise, patient-specific approaches. Digital simulations and 3D-printed guides have streamlined operative procedures and enhanced the accuracy of graft shaping and prosthetic placement, thereby improving both functional and aesthetic outcomes (del Castillo Pardo de Vera et al., 2024; Mian et al., 2021; Dowgierd et al., 2021). Notably, the surgical approach in open TMJ procedures presents a significant challenge due to the close anatomical proximity to the branches of the facial nerve. To minimize the risk of injury to motor branches and the occurrence of neuropathic pain, thorough preoperative and intraoperative anatomical planning is essential (Esmaeelinejad and Sohrabi, 2015). Although various replacement systems are commercially available, ongoing innovations increasingly favor patient-specific devices. In clinical practice, maxillofacial surgeons must carefully balance the benefits and limitations of each system to determine the most appropriate intervention for individual patients.
While all four of the mentioned TMJ replacement systems (i.e., Zimmer Biomet, TMJ Concepts, KLS Martin, and Materialise) offer customized devices with similar components and materials, subtle differences persist (Materialise, 2023; KLS Martin Group, 2024; Giannakopoulos et al., 2012; Aagaard and Thygesen, 2014). Additionally, it is important to note that there is currently a paucity of published work on the systems developed by Materialise and KLS Martin.
Historically, autologous reconstruction was the mainstay for TMJ replacement. However, the significant complications and donor site morbidity associated with autologous grafts have driven the shift toward alloplastic prostheses, which generally exhibit lower complication and revision rates along with high survival outcomes (Wax et al., 2000; Sidebottom, 2013; Saeed et al., 2003; Amarista et al., 2020). Consequently, alloplastic TMJ reconstruction has been widely adopted despite certain contraindications, including its use in growing children and in patients undergoing adjuvant therapy for tumors (Pedersen et al., 2021; Borbon et al., 2023).
Recent advances in additive manufacturing have further refined these alloplastic TMJ replacement devices. For instance, approximately 27% of metal TMJ components are now produced using 3D printing, with this technology poised to dominate the future of patient-specific devices (Mercuri et al., 2022). Ongoing research is focused on developing increasingly individualized systems that better replicate native joint biomechanics and enhance functional outcomes. Nevertheless, challenges such as warping, deformation, and porosity, arising from heat transfer and rapid cooling during metal 3D printing, persist (Mercuri et al., 2022). Addressing these issues will require advanced methods, such as hot isostatic pressing and improved surface processing, to enhance durability and fracture resistance under masticatory forces (Leuders et al., 2015; Tammas-Williams et al., 2017). Despite challenges such as high costs, technical complexities, and the requirement for extensive and robust datasets, VSP and customized alloplastic TMJ reconstruction devices mark a paradigm shift in TMD management.
Innovative regenerative strategies have further broadened the scope of TMJ reconstruction. Tissue engineering offers a promising alternative to conventional options by leveraging advanced scaffolds, diverse cell types, and growth factors to replicate native anatomical structures and restore function (Acri et al., 2019). However, significant challenges remain in optimizing materials and methods for the TMJ’s complex components. Key hurdles include scaling up constructs in size and thickness, refining mechanical properties to enhance biomimetic performance, and thoroughly evaluating local and systemic biological responses to tissue-engineered components in vivo (Donahue et al., 2019). Moreover, new biomaterials, such as protein-based matrices derived from human blood or perinatal tissues, exhibit excellent biological responses and warrant consideration for TMJ reconstruction applications (Santos et al., 2018; Deus et al., 2020).
In this context, bioprinting naturally emerges as a complementary extension of tissue-engineered approaches, offering the capacity to precisely position cells, biomaterials, and bioactive compounds within three-dimensional constructs. The integration of bioprinting into TMJ reconstruction holds the potential to revolutionize maxillofacial surgery by reducing donor site morbidity, decreasing operative time, and enhancing graft performance (Salah et al., 2020). Considering the distinct structural organization and cellular composition of the TMJ, promising strategies include i) bottom-up tissue-engineered approaches, that permit to start with small scale elements that could be arranged hierarchically and with special control up to the macroscale, and ii) the combination of different biofabrication techniques to produce heterogeneous and complex structures, including the combination of extrusion and volumetric bioprinting, extrusion-based bioprinting, melt electrowriting, 3D-printing, and electrospinning (Gaspar et al., 2020; Ribezzi et al., 2023; Ainsworth et al., 2023; Ejiohuo, 2023). Despite their innovative potential, these regenerative strategies remain in the early stages of development, with most studies limited to in vitro experiments or small animal models. Although a few methods may eventually be integrated into clinical practice, many are likely to be abandoned as challenges related to scaling, mechanical stability, and biological integration are addressed. Consequently, real-world clinical outcome data on tissue engineering in TMJ reconstruction are currently unavailable. In contrast, population-based studies on alloplastic TMJ prostheses have demonstrated excellent survival rates (Amarista et al., 2020; Gerbino et al., 2024). Although evidence on long-term outcomes is still limited, several authors have reported favorable 10-year results for both patient-specific and stock prostheses with respect to functional improvement and pain reduction (Rajkumar and Sidebottom, 2022; Leandro et al., 2013). Implant survival at 10 years has been reported as 94.7% (Rajkumar and Sidebottom, 2022). To our knowledge, only one study has evaluated TMJ devices with a follow-up exceeding 20 years (Wolford et al., 2015).
TMJ reconstruction has seen transformative advancements through digital technologies such as VSP and additive manufacturing, enabling highly accurate, patient-specific alloplastic prostheses. However, three major challenges remain: the lack of growth adaptability in pediatric patients, material and mechanical limitations in 3D-printed implants, and the translational barriers facing regenerative strategies. Emerging technologies, such as 4D bioprinting, gene therapy, and bottom-up tissue engineering, offer promising solutions by enabling dynamic, biologically integrated constructs that can better replicate the complexity of the native joint. To realize these innovations clinically, interdisciplinary collaboration between engineers, surgeons, and biologists is essential, alongside rigorous preclinical testing and ethically sound clinical trials, especially in pediatric populations.
Author contributions
HB: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Writing – original draft. BM: Data curation, Investigation, Writing – original draft. L-ML: Formal Analysis, Investigation, Methodology, Software, Visualization, Writing – review and editing. AP: Visualization, Writing – review and editing. SaK: Formal Analysis, Project administration, Resources, Software, Validation, Writing – review and editing. FG: Project administration, Resources, Supervision, Validation, Writing – review and editing. JM: Investigation, Methodology, Writing – review and editing. StK: Conceptualization, Supervision, Validation, Writing – review and editing. CR: Resources, Supervision, Writing – review and editing. MH: Supervision, Writing – review and editing. LK: Writing – original draft. CD: Conceptualization, Resources, Software, Supervision, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article.
Acknowledgments
The authors wish to acknowledge the European Union's Horizon 2020 research and innovation program under the scope of the InterLynk project (grant agreement No. 953169). JFM acknowledges also the project CICECO-Aveiro Institute of Materials, UIDB/50011/2020 (DOI 10.54499/UIDB/50011/2020), UIDP/50011/2020 (DOI 10.54499/UIDP/50011/2020) & LA/P/0006/2020 (DOI 10.54499/LA/P/0006/2020), financed by national funds through the FCT/MCTES (PIDDAC).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Acri, T. M., Shin, K., Seol, D., Laird, N. Z., Song, I., Geary, S. M., et al. (2019). Tissue engineering for the temporomandibular joint. Adv. Healthc. Mater. 8, e1801236. doi:10.1002/adhm.201801236
Aagaard, E., and Thygesen, T. (2014). A prospective, single-centre study on patient outcomes following temporomandibular joint replacement using a custom-made biomet TMJ prosthesis. Int. J. Oral Maxillofac. Surg. 43, 1229–1235. doi:10.1016/j.ijom.2014.05.019
Abramowicz, S., Barbick, M., Rose, S. P., and Dolwick, M. F. (2012). Adaptability of stock TMJ prosthesis to joints that were previously treated with custom joint prosthesis. Int. J. Oral Maxillofac. Surg. 41, 518–520. doi:10.1016/j.ijom.2011.09.024
Ainsworth, M. J., Chirico, N., de Ruijter, M., Hrynevich, A., Dokter, I., Sluijter, J. P. G., et al. (2023). Convergence of melt electrowriting and extrusion-based bioprinting for vascular patterning of a myocardial construct. Biofabrication 15, 035025. doi:10.1088/1758-5090/ace07f
Alawi, S. A., Matschke, J., Muallah, D., Gelinksy, M., and Dragu, A. (2023). 3D bioprinting in plastic and reconstructive surgery: current concepts, progress, and clinical application. Eur. J. Plastic Surg. 46, 833–843. doi:10.1007/s00238-023-02108-7
Alba, B., Harmon, K. A., La-Anyane, O., Jones, K., Figueroa, A., and Tragos, C. (2024). Bilateral temporomandibular joint reconstruction with custom alloplastic implants for pediatric ankylosis. J. Craniofacial Surg. 35, 1502–1506. doi:10.1097/scs.0000000000010250
Amarista, F. J., Mercuri, L. G., and Perez, D. (2020). Temporomandibular joint prosthesis revision and/or replacement survey and review of the literature. J. Oral Maxillofac. Surg. 78, 1692–1703. doi:10.1016/j.joms.2020.05.021
Ângelo, D. F., Sanz, D., and Cardoso, H. J. (2022). Unilateral temporomandibular joint discectomy without interposal material in patients with disc perforation or fragmentation: a prospective study. J. Oral Maxillofac. Surg. Med. Pathology 34, 375–380. doi:10.1016/j.ajoms.2021.12.005
Apelgren, P., Karabulut, E., Amoroso, M., Mantas, A., Martínez Ávila, H., Kölby, L., et al. (2019). In vivo human cartilage formation in three-dimensional bioprinted constructs with a novel bacterial nanocellulose bioink. ACS Biomaterials Sci. Eng. 5, 2482–2490. doi:10.1021/acsbiomaterials.9b00157
Aryaei, A., Vapniarsky, N., Hu, J. C., and Athanasiou, K. A. (2016). Recent tissue engineering advances for the treatment of temporomandibular joint disorders. Curr. Osteoporos. Rep. 14, 269–279. doi:10.1007/s11914-016-0327-y
Awal, D. H., Jaffer, M., Charan, G., Ball, R., Kennedy, G., Thomas, S., et al. (2018). Costochondral grafting for paediatric temporomandibular joint reconstruction: 10-year outcomes in 55 cases. Int. J. Oral Maxillofac. Surg. 47, 1433–1438. doi:10.1016/j.ijom.2018.06.004
Bishop, E. S., Mostafa, S., Pakvasa, M., Luu, H. H., Lee, M. J., Wolf, J. M., et al. (2017). 3-D bioprinting technologies in tissue engineering and regenerative medicine: current and future trends. Genes Dis. 4, 185–195. doi:10.1016/j.gendis.2017.10.002
Borbon, C., Zavattero, E., Ramieri, G., and Gerbino, G. (2023). Management of failed autogenous tissues temporomandibular joint reconstruction: case series and literature review. Front. Oral Maxillofac. Med. 5, 40. doi:10.21037/fomm-22-28
Breik, O., Devrukhkar, V., and Dimitroulis, G. (2016). Temporomandibular joint (TMJ) arthroscopic lysis and lavage: outcomes and rate of progression to open surgery. J. Cranio-Maxillofacial Surg. 44, 1988–1995. doi:10.1016/j.jcms.2016.09.017
Brown, E., Wilson, M. H., and Revington, P. (2016). Single-stage temporomandibular joint arthroplasty in a patient with complete bony ankylosis and previous extradural haematoma. BMJ Case Rep. 2016, bcr2015213917. doi:10.1136/bcr-2015-213917
Ciocca, L., Donati, D., Fantini, M., Landi, E., Piattelli, A., Iezzi, G., et al. (2013). CAD–CAM-generated hydroxyapatite scaffold to replace the mandibular condyle in sheep: preliminary results. J. Biomaterials Appl. 28, 207–218. doi:10.1177/0885328212443296
De, R. G., Vaira, L. A., Carta, E., Meloni, S. M., Sembronio, S., and Robiony, M. (2019). Bone marrow nucleated cell concentrate autograft in temporomandibular joint degenerative disorders: 1-year results of a randomized clinical trial. J. Cranio-Maxillofacial Surg. 47, 1728–1738. doi:10.1016/j.jcms.2018.11.025
De Meurechy, N., Aktan, M. K., Boeckmans, B., Huys, S., Verwilghen, D. R., Braem, A., et al. (2022). Surface wear in a custom manufactured temporomandibular joint prosthesis. J. Biomed. Mater. Res. - Part B Appl. Biomaterials 110, 1425–1438. doi:10.1002/jbm.b.35010
del Castillo Pardo de Vera, J. L., Cebrián Carretero, J. L., Aragón Niño, Í., Pampín Martínez, M. M., Borjas Gómez, J. T., Navarro Cuéllar, I., et al. (2024). Virtual surgical planning for temporomandibular joint reconstruction with stock TMJ prostheses: pilot study. Medicina 60, 339. doi:10.3390/medicina60020339
Deus, I. A., Mano, J. F., and Custódio, C. A. (2020). Perinatal tissues and cells in tissue engineering and regenerative medicine. Acta Biomater. 110, 1–14. doi:10.1016/j.actbio.2020.04.035
Di Bella, C., Duchi, S., O'Connell, C. D., Blanchard, R., Augustine, C., Yue, Z., et al. (2018). In situ handheld three-dimensional bioprinting for cartilage regeneration. J. Tissue Eng. Regen. Med. 12, 611–621. doi:10.1002/term.2476
Donahue, R. P., Hu, J. C., and Athanasiou, K. A. (2019). Remaining hurdles for tissue-engineering the temporomandibular joint disc. Trends Mol. Med. 25, 241–256. doi:10.1016/j.molmed.2018.12.007
Dowgierd, K., Pokrowiecki, R., Borowiec, M., Kozakiewicz, M., Smyczek, D., and Krakowczyk, Ł. (2021). A protocol for the use of a combined microvascular free flap with custom-made 3D-Printed total temporomandibular joint (TMJ) prosthesis for mandible reconstruction in children. Appl. Sci. 11, 2176. doi:10.3390/app11052176
Ejiohuo, O. (2023). A perspective on the synergistic use of 3D printing and electrospinning to improve nanomaterials for biomedical applications. Nano Trends 4, 100025. doi:10.1016/j.nwnano.2023.100025
Elliott, M. J., De Coppi, P., Speggiorin, S., Roebuck, D., Butler, C. R., Samuel, E., et al. (2012). Stem-cell-based, tissue engineered tracheal replacement in a child: a 2-year follow-up study. Lancet 380, 994–1000. doi:10.1016/s0140-6736(12)60737-5
Esmaeelinejad, M., and Sohrabi, M. (2015). “Surgical approaches to the temporomandibular joint,” in Atlas of temporomandibular joint surgery, 31–55.
FDA (2021). FDA’s role in approving TMJ implants and monitoring their safety. Available online at: https://www.fda.gov/medical-devices/temporomandibular-disorders-tmd-devices/fdas-role-approving-tmj-implants-and-monitoring-their-safety?utm_source=chatgpt.com (Accessed July 07, 2025).
Gaspar, V. M., Lavrador, P., Borges, J., Oliveira, M. B., and Mano, J. F. (2020). Advanced Bottom-Up engineering of living architectures. Adv. Mater. 32, e1903975. doi:10.1002/adma.201903975
Gerbino, G., Sobrero, F., Poelaert, R., Borbon, C., Ramieri, G., and Mommaerts, M. (2024). Extended temporomandibular joint prostheses: a retrospective analysis of feasibility, outcomes, and complications. Int. J. Oral Maxillofac. Surg. 54, 438–447. doi:10.1016/j.ijom.2024.10.007
Giannakopoulos, H. E., Sinn, D. P., and Quinn, P. D. (2012). Biomet microfixation temporomandibular joint replacement system: a 3-year follow-up study of patients treated during 1995 to 2005. J. Oral Maxillofac. Surg. 70, 787–794. doi:10.1016/j.joms.2011.09.031
Gonzalez-Perez, L. M., Gonzalez-Perez-Somarriba, B., Centeno, G., Vallellano, C., and Montes-Carmona, J. F. (2016). Evaluation of total alloplastic temporo-mandibular joint replacement with two different types of prostheses: a three-year prospective study. Med. Oral Patol. Oral Cirugia Bucal 21, e766–e775. doi:10.4317/medoral.21189
Gonzalez-Perez, L. M., Montes-Carmona, J. F., Torres-Carranza, E., and Infante-Cossio, P. (2023). Total joint replacement for immediate reconstruction following ablative surgery for primary tumors of the temporo-mandibular joint. J. Pers. Med. 13, 1021. doi:10.3390/jpm13071021
Granquist, E. J., Bouloux, G. F., Sinn, D., Dattilo, D., McCain, J., Louis, P., et al. (2018). Outcomes and survivorship of a titanium-on-polyethylene device: results from an FDA study of the biomet microfixation total TMJ replacement system. J. Oral Maxillofac. Surg. 76, e77–e78. doi:10.1016/j.joms.2018.06.162
Gravvanis, A., Anterriotis, D., and Kakagia, D. (2017). Mandibular condyle reconstruction with fibula free-tissue transfer: the role of the masseter muscle. J. Craniofacial Surg. 28, 1955–1959. doi:10.1097/scs.0000000000003998
Grayson, W. L., Fröhlich, M., Yeager, K., Bhumiratana, S., Chan, M. E., Cannizzaro, C., et al. (2010). Engineering anatomically shaped human bone grafts. Proc. Natl. Acad. Sci. 107, 3299–3304. doi:10.1073/pnas.0905439106
Gungor-Ozkerim, P. S., Inci, I., Zhang, Y. S., Khademhosseini, A., and Dokmeci, M. R. (2018). Bioinks for 3D bioprinting: an overview. Biomaterials Sci. 6, 915–946. doi:10.1039/c7bm00765e
Hadad, H., Boos Lima, FBDJ, Shirinbak, I., Porto, T. S., Chen, J. E., and Guastaldi, F. P. (2023). The impact of 3D printing on oral and maxillofacial surgery. J. 3D Print. Med. 7, 3DP007. doi:10.2217/3dp-2022-0025
Handa, S., Guastaldi, F. P. S., Violette, L., Abou-Ezzi, J., Rosén, A., and Keith, D. (2023). Which comorbid conditions and risk factors affect the outcome of and progression to total temporomandibular joint replacement? Int. J. Oral Maxillofac. Surg. 52, 1265–1271. doi:10.1016/j.ijom.2023.05.011
Hashemi, H., Cardemil, C., and Farzad, P. (2024). Bilateral alloplastic total temporomandibular joint reconstruction in a five-year-old child: a case report and a review of the literature. Oral Maxillofac. Surg. Cases 10, 100365. doi:10.1016/j.omsc.2024.100365
He, D., Yang, C., Chen, M., Zhang, X., Qiu, Y., Yang, X., et al. (2011). Traumatic temporomandibular joint ankylosis: our classification and treatment experience. J. Oral Maxillofac. Surg. 69, 1600–1607. doi:10.1016/j.joms.2010.07.070
Helgeland, E., Mohamed-Ahmed, S., Shanbhag, S., Pedersen, T. O., Rosén, A., Mustafa, K., et al. (2021). 3D printed gelatin-genipin scaffolds for temporomandibular joint cartilage regeneration. Biomed. Phys. Eng. Express 7, 055025. doi:10.1088/2057-1976/ac1e68
Howlader, D., Vignesh, U., Bhutia, D. P., Pandey, R., Kumar, S., Chandra, T., et al. (2017). Hydroxyapatite collagen scaffold with autologous bone marrow aspirate for mandibular condylar reconstruction. J. Cranio-Maxillofacial Surg. 45, 1566–1572. doi:10.1016/j.jcms.2017.06.022
Hu, S., Yi, Y., Ye, C., Liu, J., and Wang, J. (2023). Advances in 3D printing techniques for cartilage regeneration of temporomandibular joint disc and mandibular condyle. Int. J. Bioprinting 9, 761. doi:10.18063/ijb.761
Imola, M. J., and Liddell, A. (2016). Temporomandibular joint reconstruction. Curr. Opin. Otolaryngology–Head Neck Surg. 24, 336–342. doi:10.1097/moo.0000000000000282
Ingawale, S. M., and Goswami, T. (2022). Design and finite element analysis of patient-specific total temporomandibular joint implants. Materials 15, 4342. doi:10.3390/ma15124342
Johns, D., and Athanasiou, K. (2008). Growth factor effects on costal chondrocytes for tissue engineering fibrocartilage. Cell Tissue Res. 333, 439–447. doi:10.1007/s00441-008-0652-2
Jones, R. (2011). Temporomandibular joint reconstruction with total alloplastic joint replacement. Aust. Dent. J. 56, 85–91. doi:10.1111/j.1834-7819.2010.01288.x
Kalpakci, K. N., Kim, E. J., and Athanasiou, K. A. (2011). Assessment of growth factor treatment on fibrochondrocyte and chondrocyte co-cultures for TMJ fibrocartilage engineering. Acta Biomater. 7, 1710–1718. doi:10.1016/j.actbio.2010.12.015
Kanatsios, S., Breik, O., and Dimitroulis, G. (2018). Biomet stock temporomandibular joint prosthesis: long-term outcomes of the use of titanium condyles secured with four or five condylar fixation screws. J. Cranio-Maxillofacial Surg. 46, 1697–1702. doi:10.1016/j.jcms.2018.07.002
Kang, H.-W., Lee, S. J., Ko, I. K., Kengla, C., Yoo, J. J., and Atala, A. (2016). A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nat. Biotechnol. 34, 312–319. doi:10.1038/nbt.3413
Keriquel, V., Oliveira, H., Rémy, M., Ziane, S., Delmond, S., Rousseau, B., et al. (2017). In situ printing of mesenchymal stromal cells, by laser-assisted bioprinting, for in vivo bone regeneration applications. Sci. Rep. 7, 1778. doi:10.1038/s41598-017-01914-x
Keyser, B. R., Banda, A. K., Mercuri, L. G., Warburton, G., and Sullivan, S. M. (2020). Alloplastic total temporomandibular joint replacement in skeletally immature patients: a pilot survey. Int. J. Oral Maxillofac. Surg. 49, 1202–1209. doi:10.1016/j.ijom.2020.02.001
KLS Martin Group (2024). Instructions for use - IPS implants TMJ prosthesis. Available online at: https://www.klsmartin.com/mediathek/91-350-46-02_IPS_Implants_TMJ_Prosthesis.pdf (Accessed February 02, 2025).
Ko, E. W.-C., Huang, C.-S., and Chen, Y.-R. (1999). Temporomandibular joint reconstruction in children using costochondral grafts. J. Oral Maxillofac. Surg. 57, 789–798. doi:10.1016/s0278-2391(99)90816-9
Köhnke, R., Ahlers, M. O., Birkelbach, M. A., Ewald, F., Krueger, M., Fiedler, I., et al. (2021). Temporomandibular joint osteoarthritis: regenerative treatment by a stem cell containing advanced therapy medicinal product (ATMP)—An in vivo animal trial. Int. J. Mol. Sci. 22, 443. doi:10.3390/ijms22010443
Konopnicki, S., and Troulis, M. J. (2015). Mandibular tissue engineering: past, present, future. J. Oral Maxillofac. Surg. 73, S136–S146. doi:10.1016/j.joms.2015.05.037
Kreutziger, K. L. (1994). Surgical management of the temporomandibular joint in resection of regional tumors. South. Med. J. 87, 215–224. doi:10.1097/00007611-199402000-00014
Laventhal, N., Tarini, B. A., and Lantos, J. (2012). Ethical issues in neonatal and pediatric clinical trials. Pediatr. Clin. North Am. 59, 1205–1220. doi:10.1016/j.pcl.2012.07.007
Leandro, L. F. L., Ono, H. Y., de Souza Loureiro, C. C., Marinho, K., and Garcia Guevara, H. A. (2013). A ten-year experience and follow-up of three hundred patients fitted with the biomet/lorenz microfixation TMJ replacement system. Int. J. Oral Maxillofac. Surg. 42, 1007–1013. doi:10.1016/j.ijom.2013.04.018
Leandro, L. F., Marine, K. C., Omizzolo, G., Lopes, A., Houthoofd, W., and Ornellas, F. M. (2022). Retrospective study of patients submitted to reconstruction with customized temporomandibular joint prostheses. Eur. J. Oral Maxillofac. Surg. 6, 122–127. doi:10.23736/s2532-3466.22.00297-1
Leuders, S., Vollmer, M., Brenne, F., Tröster, T., and Niendorf, T. (2015). Fatigue strength prediction for titanium alloy TiAl6V4 manufactured by selective laser melting. Metallurgical Mater. Trans. A 46, 3816–3823. doi:10.1007/s11661-015-2864-x
Li, H., Dai, J., Wang, Z., Zheng, H., Li, W., Wang, M., et al. (2023). Digital light processing (DLP)-based (bio)printing strategies for tissue modeling and regeneration. Aggregate 4, e270. doi:10.1002/agt2.270
Lima, F., Rios, L. G. C., Paranhos, L. R., Vieira, W. A., and Zanetta-Barbosa, D. (2024). Survival of temporomandibular total joint replacement: a systematic review and meta-analysis. J. Oral Rehabilitation 51, 775–784. doi:10.1111/joor.13635
Materialise (2023). Instructions for use - materialise TMJ total arthroplasty system. Available online at: https://assets-eu-01.kc-usercontent.com/8ff24b0e-57a3-0157-62d1-fa4ac9734eb5/cddfb1bb-8fec-4afa-8431-7bfb70bc7a50/IFU%20Materialise%20TMJ%20Total%20Arthroplasty%20Sytem%20-%20Materialise%20Standard%2B%20Solutions%20Screws%20-%20Europe%20-%20Multi-language%20-%20L-101684-04.pdf (Accessed February 02, 2025).
Matheus, H. R., Özdemir, Ş. D., and Guastaldi, F. P. S. (2022). Stem cell-based therapies for temporomandibular joint osteoarthritis and regeneration of cartilage/osteochondral defects: a systematic review of preclinical experiments. Osteoarthr. Cartil. 30, 1174–1185. doi:10.1016/j.joca.2022.05.006
Mercuri, L. G. (2013). The role of custom-made prosthesis for temporomandibular joint replacement. Rev. Española Cirugía Oral Maxilofac. 35, 1–10. doi:10.1016/j.maxilo.2012.02.003
Mercuri, L. G., Neto, M. Q., and Pourzal, R. (2022). Alloplastic temporomandibular joint replacement: present status and future perspectives of the elements of embodiment. Int. J. Oral Maxillofac. Surg. 51, 1573–1578. doi:10.1016/j.ijom.2022.05.015
Mian, M., Ackland, D., Fink, S., Wang, N., and Dimitroulis, G. (2021). Accuracy of custom temporomandibular joint replacement surgery using a virtual surgical planning protocol. Oral Maxillofac. Surg. 25, 367–371. doi:10.1007/s10006-020-00928-6
Mommaerts, M. Y., Deman, F., Verwilghen, D., and De Meurechy, N. (2025). Lateral pterygoid muscle enthesis reconstruction in alloplastic total temporomandibular joint replacement: an animal experiment with histological verification. J. Cranio-Maxillofacial Surg. 53, 476–483. doi:10.1016/j.jcms.2025.01.022
Munro, I. R., and Chir, B. (1980). One-stage reconstruction of the temporomandibular joint in hemifacial microsomia. Plastic Reconstr. Surg. – Glob. Open 66, 699–710. doi:10.1097/00006534-198011000-00005
Myers, P. L., Nelson, J. A., Rosen, E. B., Allen, R. J., Disa, J. J., and Matros, E. (2021). Virtual surgical planning for oncologic mandibular and maxillary reconstruction. Plastic Reconstr. Surg. - Glob. Open 9, e3672. doi:10.1097/gox.0000000000003672
Neff, A., Ahlers, O., Eger, T., Feurer, I., Giannakopoulos, N., Hell, B., et al. (2020). S3-Leitlinie: totaler alloplastischer kiefergelenkersatz: awmf-register-nr. 007-106. Langversion. Available online at: http://www.awmf.org/uploads/tx_szleitlinien/007-106l_S3_Totaler_alloplastischer_Kiefergelenkersatz_2020-04.pdf (Accessed January 01, 2025).
Neuhaus, M. T., Zeller, A. N., Bartella, A. K., Sander, A. K., Lethaus, B., and Zimmerer, R. M. (2021). Accuracy of guided surgery and real-time navigation in temporomandibular joint replacement surgery. Dent. J. 9, 87. doi:10.3390/dj9080087
NIH SEED (2023). Regulatory knowledge guide for combination products NIH SEED innovator support team. Available online at: https://seed.nih.gov/sites/default/files/2024-04/Regulatory-Knowledge-Guide-for-Combination-Products.pdf?utm_source=chatgpt.com (Accessed July 07, 2025).
Niloy, I., Liu, R. H., Pham, N. M., and Yim, C. M. R. (2024). Novel use of virtual reality and augmented reality in temporomandibular total joint replacement using stock prosthesis. J. Oral Maxillofac. Surg. 82, 632–640. doi:10.1016/j.joms.2024.02.010
Nordberg, R. C., Otarola, G. A., Wang, D., Hu, J. C., and Athanasiou, K. A. (2022). Navigating regulatory pathways for translation of biologic cartilage repair products. Sci. Transl. Med. 14, eabp8163. doi:10.1126/scitranslmed.abp8163
Olate, S., Ravelo, V., Huentequeo, C., Parra, M., and Unibazo, A. (2023). An overview of clinical conditions and a systematic review of personalized TMJ replacement. J. Personalized Med. 13, 533. doi:10.3390/jpm13030533
Onoriobe, U., Miloro, M., Sukotjo, C., Mercuri, L. G., Lotesto, A., and Eke, R. (2016). How many temporomandibular joint total joint alloplastic implants will be placed in the United States in 2030? J. Oral Maxillofac. Surg. 74, 1531–1538. doi:10.1016/j.joms.2016.04.011
Ott, H. C. (2012). Engineering tissues for children: building grafts that grow. Lancet 380, 957–958. doi:10.1016/s0140-6736(12)60951-9
Park, H. I., Lee, J. H., and Lee, S. J. (2022). The comprehensive on-demand 3D bio-printing for composite reconstruction of mandibular defects. Maxillofac. Plastic Reconstr. Surg. 44, 31. doi:10.1186/s40902-022-00361-7
Pedersen, T., Lybak, S., Lund, B., and Løes, S. (2021). Temporomandibular joint prosthesis in cancer reconstruction preceding radiation therapy. Clin. Case Rep. 9, 1438–1441. doi:10.1002/ccr3.3794
Perera, K., Ivone, R., Natekin, E., Wilga, C. A., Shen, J., and Menon, J. U. (2021). 3D bioprinted implants for cartilage repair in intervertebral discs and knee menisci. Front. Bioeng. Biotechnol. 9, 754113. doi:10.3389/fbioe.2021.754113
Peres Lima, F. G. G., Rios, L. G. C., Bianchi, J., Gonçalves, J., Paranhos, L., Vieira, W., et al. (2023). Complications of total temporomandibular joint replacement: a systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 52, 584–594. doi:10.1016/j.ijom.2022.10.009
Pluijmers, B. I., Caron, CJJM, Dunaway, D. J., Wolvius, E. B., and Koudstaal, M. J. (2014). Mandibular reconstruction in the growing patient with unilateral craniofacial microsomia: a systematic review. Int. J. Oral Maxillofac. Surg. 43, 286–295. doi:10.1016/j.ijom.2013.11.001
Powers, D., Breeze, J., and Erdmann, D. (2022). Vascularized fibula TMJ reconstruction: a report of five cases featuring computerized patient-specific surgical planning. Plastic Reconstr. Surg. - Glob. Open 10, e4465. doi:10.1097/gox.0000000000004465
PREP (2024). Ethical inclusion of children in research. Available online at: https://www.cc.nih.gov/sites/default/files/bioethics/bioethics-files/courses/pdf/2024/session3_shah.pdf (Accessed July 07, 2025).
Raccampo, L., Sembronio, S., Tel, A., and Robiony, M. (2023). Extended complex temporomandibular joint reconstructions exploiting virtual surgical planning, navigation assistance, and custom-made prosthesis: a comprehensive protocol and workflow. J. Personalized Med. 13, 931. doi:10.3390/jpm13060931
Rajkumar, A., and Sidebottom, A. J. (2022). Prospective study of the long-term outcomes and complications after total temporomandibular joint replacement: analysis at 10 years. Int. J. Oral Maxillofac. Surg. 51, 665–668. doi:10.1016/j.ijom.2021.07.021
Ramadan, Q., and Zourob, M. (2021). 3D bioprinting at the frontier of regenerative medicine, pharmaceutical, and food industries. Front. Med. Technol. 2, 607648. doi:10.3389/fmedt.2020.607648
Rendenbach, C., Kohlmeier, C., Suling, A., Assaf, A. T., Catala-Lehnen, P., Amling, M., et al. (2016). Prospective biomechanical analysis of donor-site morbidity after fibula free flap. J. Cranio-Maxillofacial Surg. 44, 155–159. doi:10.1016/j.jcms.2015.10.027
Resnick, C. M. (2018). Temporomandibular joint reconstruction in the growing child. Oral Maxillofac. Surg. Clin. N. Am. 30, 109–121. doi:10.1016/j.coms.2017.08.006
Ribezzi, D., Gueye, M., Florczak, S., Dusi, F., de Vos, D., Manente, F., et al. (2023). Shaping synthetic multicellular and complex multimaterial tissues via embedded extrusion-volumetric printing of microgels. Adv. Mater. 35, 2301673. doi:10.1002/adma.202301673
Rodby, K. A., Turin, S., Jacobs, R. J., Cruz, J. F., Hassid, V. J., Kolokythas, A., et al. (2014). Advances in oncologic head and neck reconstruction: systematic review and future considerations of virtual surgical planning and computer aided design/computer aided modeling. J. Plastic, Reconstr. Aesthetic Surg. 67, 1171–1185. doi:10.1016/j.bjps.2014.04.038
Rodríguez-Pombo, L., Xu, X., Seijo-Rabina, A., Ong, J. J., Alvarez-Lorenzo, C., Rial, C., et al. (2022). Volumetric 3D printing for rapid production of medicines. Addit. Manuf. 52, 102673. doi:10.1016/j.addma.2022.102673
Saeed, N. R., and Kent, J. N. (2003). A retrospective study of the costochondral graft in TMJ reconstruction. Int. J. Oral Maxillofac. Surg. 32, 606–609. doi:10.1054/ijom.2003.0418
Salah, M., Tayebi, L., Moharamzadeh, K., and Naini, F. B. (2020). Three-dimensional bio-printing and bone tissue engineering: technical innovations and potential applications in maxillofacial reconstructive surgery. Maxillofac. Plastic Reconstr. Surg. 42, 18. doi:10.1186/s40902-020-00263-6
Salash, J. R., Hossameldin, R. H., Almarza, A. J., Chou, J. C., McCain, J. P., Mercuri, L. G., et al. (2016). Potential indications for tissue engineering in temporomandibular joint surgery. J. Oral Maxillofac. Surg. 74, 705–711. doi:10.1016/j.joms.2015.11.008
Salinas, F. A., Krüger Weiner, C., Adami, J., Rosén, A., Lund, B., Hedenberg-Magnusson, B., et al. (2022). Sick leave and disability pension in a cohort of TMD-patients - the Swedish national registry studies for surgically treated TMD (SWEREG-TMD). BMC Public Health 22, 916. doi:10.1186/s12889-022-13329-z
Sanovich, R., Mehta, U., Abramowicz, S., Widmer, C., and Dolwick, M. F. (2014). Total alloplastic temporomandibular joint reconstruction using biomet stock prostheses: the university of Florida experience. Int. J. Oral Maxillofac. Surg. 43, 1091–1095. doi:10.1016/j.ijom.2014.04.008
Santos, S., Sigurjonsson, Ó. E., Custódio, C. A., and Mano, J. (2018). Blood plasma derivatives for tissue engineering and regenerative medicine therapies. Tissue Eng. Part B, Rev. 24, 454–462. doi:10.1089/ten.teb.2018.0008
Sawh-Martinez, R., Parsaei, Y., Wu, R., Lin, A., Metzler, P., DeSesa, C., et al. (2017). Improved temporomandibular joint position after 3-Dimensional planned mandibular reconstruction. J. Oral Maxillofac. Surg. 75, 197–206. doi:10.1016/j.joms.2016.07.032
Schmidt, C., Ertel, T., Arbogast, M., Hügle, B., Kalle, T. v., Neff, A., et al. (2022). The diagnosis and treatment of rheumatoid and juvenile idiopathic arthritis of the temporomandibular joint. Dtsch. Arzteblatt Int. 119, 47–54. doi:10.3238/arztebl.m2021.0388
Sekhoto, M. G., Rikhotso, R. E., and Rajendran, S. (2019). Management of unpredictable outcomes of costochondral grafts. Int. J. Surg. Case Rep. 62, 144–149. doi:10.1016/j.ijscr.2019.07.074
Sembronio, S., Tel, A., and Robiony, M. (2021). The use of cutting/positioning devices for custom-fitted temporomandibular joint alloplastic reconstruction: current knowledge and development of a new system. Int. J. Oral Maxillofac. Surg. 50, 530–537. doi:10.1016/j.ijom.2020.09.016
Sidebottom, A. J. (2013). Alloplastic or autogenous reconstruction of the TMJ. J. Oral Biol. Craniofacial Res. 3, 135–139. doi:10.1016/j.jobcr.2013.07.003
Singh, A. K., Khanal, N., and Chaulagain, R. (2022). Advances in tissue engineering of the temporomandibular joint disc: an overview of current status and future directions. Int. J. Dent. 2022, 9696378. doi:10.1155/2022/9696378
Sinn, D. P., Tandon, R., and Tiwana, P. S. (2021). Can alloplastic total temporomandibular joint reconstruction be used in the growing patient? A preliminary report. J. Oral Maxillofac. Surg. 79, 2267. e1–2267.e16. doi:10.1016/j.joms.2021.06.022
Spotts, P. H. (2017). Temporomandibular disorder: an underdiagnosed cause of headache, sinus pain, and ear pain. Am. Fam. Physician 95, 142–42.
Sugiura, T., Matsumura, G., Miyamoto, S., Miyachi, H., Breuer, C. K., and Shinoka, T. (2018). Tissue-engineered vascular grafts in children with congenital heart disease: intermediate term Follow-up. Seminars Thorac. Cardiovasc. Surg. 30, 175–179. doi:10.1053/j.semtcvs.2018.02.002
Tammas-Williams, S., Withers, P. J., Todd, I., and Prangnell, P. (2017). The influence of porosity on fatigue crack initiation in additively manufactured titanium components. Sci. Rep. 7, 7308. doi:10.1038/s41598-017-06504-5
Valesan, L. F., Da-Cas, C. D., Réus, J. C., Denardin, A. C. S., Garanhani, R. R., Bonotto, D., et al. (2021). Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin. Oral Investig. 25, 441–453. doi:10.1007/s00784-020-03710-w
Vapniarsky, N., Huwe, L. W., Arzi, B., Houghton, M. K., Wong, M. E., Wilson, J. W., et al. (2018). Tissue engineering toward temporomandibular joint disc regeneration. Sci. Transl. Med. 10, eaaq1802. doi:10.1126/scitranslmed.aaq1802
Wax, M. K., Winslow, C. P., Hansen, J., MacKenzie, D., Cohen, J., Andersen, P., et al. (2000). A retrospective analysis of temporomandibular joint reconstruction with free fibula microvascular flap. Laryngoscope 110, 977–981. doi:10.1097/00005537-200006000-00018
Wolford, L. M., Cottrell, D. A., and Henry, C. (1994). Sternoclavicular grafts for temporomandibular joint reconstruction. J. Oral Maxillofac. Surg. 52, 119–128. doi:10.1016/0278-2391(94)90391-3
Wolford, L. M., Mercuri, L. G., Schneiderman, E. D., Movahed, R., and Allen, W. (2015). Twenty-year Follow-up study on a patient-fitted temporomandibular joint prosthesis: the Techmedica/TMJ concepts device. J. Oral Maxillofac. Surg. 73, 952–960. doi:10.1016/j.joms.2014.10.032
Wu, Y., Kennedy, P., Bonazza, N., Yu, Y., Dhawan, A., and Ozbolat, I. (2021). Three-dimensional bioprinting of articular cartilage: a systematic review. Cartilage 12, 76–92. doi:10.1177/1947603518809410
Yadav, P., Roychoudhury, A., Kumar, R. D., Bhutia, O., Bhutia, T., and Aggarwal, B. (2021). Total alloplastic temporomandibular joint replacement. J. Maxillofac. Oral Surg. 20, 515–526. doi:10.1007/s12663-021-01628-8
Yang, S., Fan, H., Du, W., Li, J., Hu, J., and Luo, E. (2015). Overgrowth of costochondral grafts in craniomaxillofacial reconstruction: rare complication and literature review. J. Cranio-Maxillo-Facial Surg. 43, 803–812. doi:10.1016/j.jcms.2015.03.041
Yang, H., Sun, L., Pang, Y., Hu, D., Xu, H., Mao, S., et al. (2021). Three-dimensional bioprinted hepatorganoids prolong survival of mice with liver failure. Gut 70, 567–574. doi:10.1136/gutjnl-2019-319960
Yi, P., Liang, J., Huang, F., Zhao, Z., Zhou, X., Gao, Q., et al. (2021). Composite system of 3D-Printed polymer and acellular matrix hydrogel to repair temporomandibular joint disc. Front. Mater. 8, 621416. doi:10.3389/fmats.2021.621416
Zhang, S., Yap, A. U. J., and Toh, W. S. (2015). Stem cells for temporomandibular joint repair and regeneration. Stem Cell Rev. Rep. 11, 728–742. doi:10.1007/s12015-015-9604-x
Zhao, Y., Li, C., Hu, S., Wang, C., Bian, X., Kang, H., et al. (2024). In vitro differentiation of human induced pluripotent stem cells into temporomandibular joint disc like cells. Heliyon 10, e23937. doi:10.1016/j.heliyon.2023.e23937
Zheng, J., Chen, X., Jiang, W., Zhang, S., Chen, M., and Yang, C. (2019). An innovative total temporomandibular joint prosthesis with customized design and 3D printing additive fabrication: a prospective clinical study. J. Transl. Med. 17, 4. doi:10.1186/s12967-018-1759-1
Keywords: temporomandibular joint reconstruction, TMJ replacement, tissue engineering, bioprinting, 3D printing, computer-aided design, computer-aided manufacturing, CAD/CAM
Citation: Baecher H, Maheta B, Lottner L-M, Panayi AC, Knoedler S, Guastaldi F, Mano JF, Koerdt S, Rendenbach C, Heiland M, Knoedler L and Doll C (2025) Current clinical and translational challenges in temporomandibular joint reconstruction. Front. Bioeng. Biotechnol. 13:1590021. doi: 10.3389/fbioe.2025.1590021
Received: 08 March 2025; Accepted: 26 August 2025;
Published: 18 September 2025.
Edited by:
Dinesh Rokaya, Ajman University, United Arab EmiratesReviewed by:
Tomislav Badel, University of Zagreb, CroatiaShantanu Dixit, Walailak University, Thailand
Copyright © 2025 Baecher, Maheta, Lottner, Panayi, Knoedler, Guastaldi, Mano, Koerdt, Rendenbach, Heiland, Knoedler and Doll. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Baecher, aGVsZW5hLmJhZWNoZXJAY2hhcml0ZS5kZQ==
†These authors have contributed equally to this work