 Pablo Díez-Villanueva1*†
Pablo Díez-Villanueva1*† César Jiménez-Méndez1†
César Jiménez-Méndez1† Clara Bonanad2
Clara Bonanad2 Carolina Ortiz-Cortés3
Carolina Ortiz-Cortés3 Eduardo Barge-Caballero4,5Josebe Goirigolzarri6
Eduardo Barge-Caballero4,5Josebe Goirigolzarri6 Alberto Esteban-Fernández7
Alberto Esteban-Fernández7 Angel Pérez-Rivera8
Angel Pérez-Rivera8 Marta Cobo5,9
Marta Cobo5,9 Ancor Sanz-García10
Ancor Sanz-García10 Francesc Formiga11
Francesc Formiga11 Albert Ariza-Solé12
Albert Ariza-Solé12 Manuel Martínez-Sellés13‡
Manuel Martínez-Sellés13‡ Fernando Alfonso1‡
Fernando Alfonso1‡- 1Cardiology Department, Hospital Universitario de la Princesa, Universidad Autónoma de Madrid, CIBERCV, IIS-IP, Madrid, Spain
- 2Cardiology Department, Hospital Clínico Universitario de Valencia, Instituto de Investigación Sanitaria (INCLIVA), Valencia, Spain
- 3Cardiology Department, Hospital Universitario San Pedro de Alcántara, Cáceres, Spain
- 4Cardiology Department, Complejo Hospitalario Universitario de a Coruña, A Coruña, Spain
- 5Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Madrid, Spain
- 6Cardiology Department, Hospital Clínico Universitario San Carlos, Madrid, Spain
- 7Cardiology Department, Hospital Universitario Severo Ochoa, Leganés, Spain
- 8Cardiology Department, Hospital Universitario de Burgos, Universidad Isabel I, Burgos, Spain
- 9Cardiology Department, Hospital Universitario Puerta de Hierro, Madrid, Spain
- 10Unidad de Análisis de Datos, Instituto de Investigación Sanitaria del Hospital Universitario de la Princesa, Madrid, Spain
- 11Servicio de Medicina Interna, Hospital Bellvitge, L'Hospitalet de Llobregat, Barcelona, Spain
- 12Cardiology Department, Hospital Universitario de Bellvitge, L'Hospitalet de Llobregat, Barcelona, Spain
- 13Cardiology Department, Hospital Universitario Gregorio Marañón, CIBERCV, Universidad Europea, Universidad Complutense, Madrid, Spain
Introduction: Frailty is common among patients with heart failure (HF). Our aim was to address the role of frailty in the management and prognosis of elderly men and women with HF.
Methods and results: Prospective multicenter registry that included 499 HF outpatients ≥75 years old. Mean age was 81.4 ± 4.3 years, and 193 (38%) were women. Compared with men, women were older (81.9 ± 4.3 vs. 81.0 ± 4.2 years, p = 0.03) and had higher left ventricular ejection fraction (46 vs. 40%, p < 0.001) and less ischemic heart disease (30 vs. 57%, p < 0.001). Women had a higher prevalence of frailty (22 vs. 10% with Clinical Frailty Scale, 34 vs. 15% with FRAIL, and 67% vs. 46% with the mobility visual scale, all p-values < 0.001) and other geriatric conditions (Barthel index ≤90: 14.9 vs. 6.2%, p = 0.003; malnutrition according to Mini Nutritional Assessment Short Formulary ≤11: 55% vs. 42%, p = 0.007; Pfeiffer cognitive test's errors: 1.6 ± 1.7 vs. 1.0 ± 1.6, p < 0.001; depression according to Yesavage test; p < 0.001) and lower comorbidity (Charlson index ≥4: 14.1% vs. 22.1%, p = 0.038). Women also showed worse self-reported quality of life (6.5 ± 2.1 vs. 6.9 ± 1.9, on a scale from 0 to 10, p = 0.012). In the univariate analysis, frailty was an independent predictor of mortality in men [Hazard ratio (HR) 3.18, 95% confidence interval (CI) 1.29–7.83, p = 0.012; HR 4.53, 95% CI 2.08–9.89, p < 0.001; and HR 2.61, 95% CI 1.23–5.43, p = 0.010, according to FRAIL, Clinical Frailty Scale, and visual mobility scale, respectively], but not in women. In the multivariable analysis, frailty identified by the visual mobility scale was an independent predictor of mortality (HR 1.95, 95% CI 1.04–3.67, p = 0.03) and mortality/readmission (HR 2.06, 95% CI 1.05–4.04, p = 0.03) in men.
Conclusions: In elderly outpatients with HF frailty is more common in women than in men. However, frailty is only associated with mortality in men.
Introduction
Heart failure (HF) is one of the main causes of morbimortality in older patients (1). Both its incidence and prevalence are increasing due, in part, to population aging (2, 3). However, elderly patients are still frequently underrepresented in clinical trials (4), and a better understanding of the clinical factors associated with prognosis in this population is needed (5). Frailty, which is common in elderly patients with HF, is an age-associated clinical syndrome characterized by a decrease in physiological reserve that entails an increased vulnerability to stressors (6–8). As such, frailty should be adequately both identified and addressed in HF patients (9).
Besides, sex-related differences in men and women with HF have been identified, not only from a pathophysiological point of view, but also regarding the different impact of traditional risk factors, together with specific sex-related factors and different prognosis in men and women (10, 11).
Our aim was to address the role of frailty and sex differences in the management and prognosis of elderly outpatients with HF.
Methods
The FRAGIC registry (impacto de la FRAGilidad y otros síndromes Geriátricos en el manejo clínico y pronóstico del paciente anciano ambulatorio con Insuficiencia Cardíaca) is an prospective observational multicenter study. The rationale of this study has been previously reported (12). Briefly, ambulatory patients ≥75 years with chronic HF treated according to current guidelines (13) were prospectively included between March and September 2019. Baseline clinical characteristics and laboratory and echocardiographic parameters were collected. Functional status and functional class as well as comorbidity and a systematic and comprehensive geriatric evaluation were registered in all patients at the first visit. Medical treatment was optimized according to clinical practice guidelines recommendations in all patients. Follow-up was carried out via clinical visit, electronic medical records review and/or telephone contacts at 1 year follow up. Total mortality and the need for hospitalization for any cause (duration >24 h) were recorded. The ethics committee of Hospital Universitario de La Princesa (Madrid, Spain) approved the study and the protocol was redacted according to the Declaration of Helsinki. All patients included in this study willingly completed the informed consent.
Statistical analysis
For the purpose of this analysis, patients were divided by sex. Percentages were used to represent categorical variables, and the mean and standard deviation were used for continuous variables. The univariate comparison between each independent variable and sex, was assessed by Log-Rank test, from which p-values and Hazard ratios (HR) were obtained. Next, a predictive model was fitted using Cox Regression (multivariate analysis) by selecting those variables from the univariate analysis (p < 0.05 for women, and p < 0.001 for men, this difference is due to the high number of statistically significant variables in univariate analysis in men); this analysis was performed separately for women and men by considering as outcome mortality or the combination of mortality and readmission. Disease-specific survival or the cumulative event of readmission for any cause and mortality was obtained using the Kaplan-Meier method. Comparison of survival distributions was performed using a Log-Rank test. Data were analyzed using our own codes and basic functions in R, version 4.0.3 (http://www.R-project.org; the R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics and geriatric syndromes according to sex
A total of 499 ambulatory patients with chronic HF were included. Mean age was 81.4 ± 4.3 years, and 38% were women. Compared with men, women were older (81.9 ± 4.3 vs. 81.0 ± 4.2 years, p = 0.03) and had significantly higher left ventricular ejection fraction as well as less previous ischemic heart disease. Baseline variables are depicted in Table 1. Comorbidity prevalence was higher in men. Women had a higher prevalence of frailty and other geriatric conditions. Frailty was always more common in women irrespective of the scale (all p values< 0.001). Physical status according to short physical performance battery (SSPB) was also lower in women, in whom malnutrition and depression, as well as worse self-reported quality of life, were also more frequent (Table 1).

Table 1. Baseline characteristics.
Clinical outcomes during follow-up according to sex
During a mean follow up of 371 (361–387) days, 58 patients (11.6%) died (32 men and 26 women). The leading cause of mortality was non-cardiovascular mortality (58%). Table 2 shows the variables associated with 1-year mortality according to sex in univariate analysis. In men, lower values of hemoglobin, lymphocytes, albumin and sodium, as well as urea and renal dysfunction were associated with mortality, whilst a lower platelet count was associated with prognosis in women. Data related to more advanced HF were associated with worse prognosis in women. Higher doses of diuretics, higher levels of natriuretic peptides and reduced right ventricular function were the only parameters independently associated with mortality in men and women. Frailty was associated with mortality only in men, although a trend toward higher mortality was observed in women according to some scales. Figure 1 shows the differential impact of frailty according to sex in mortality
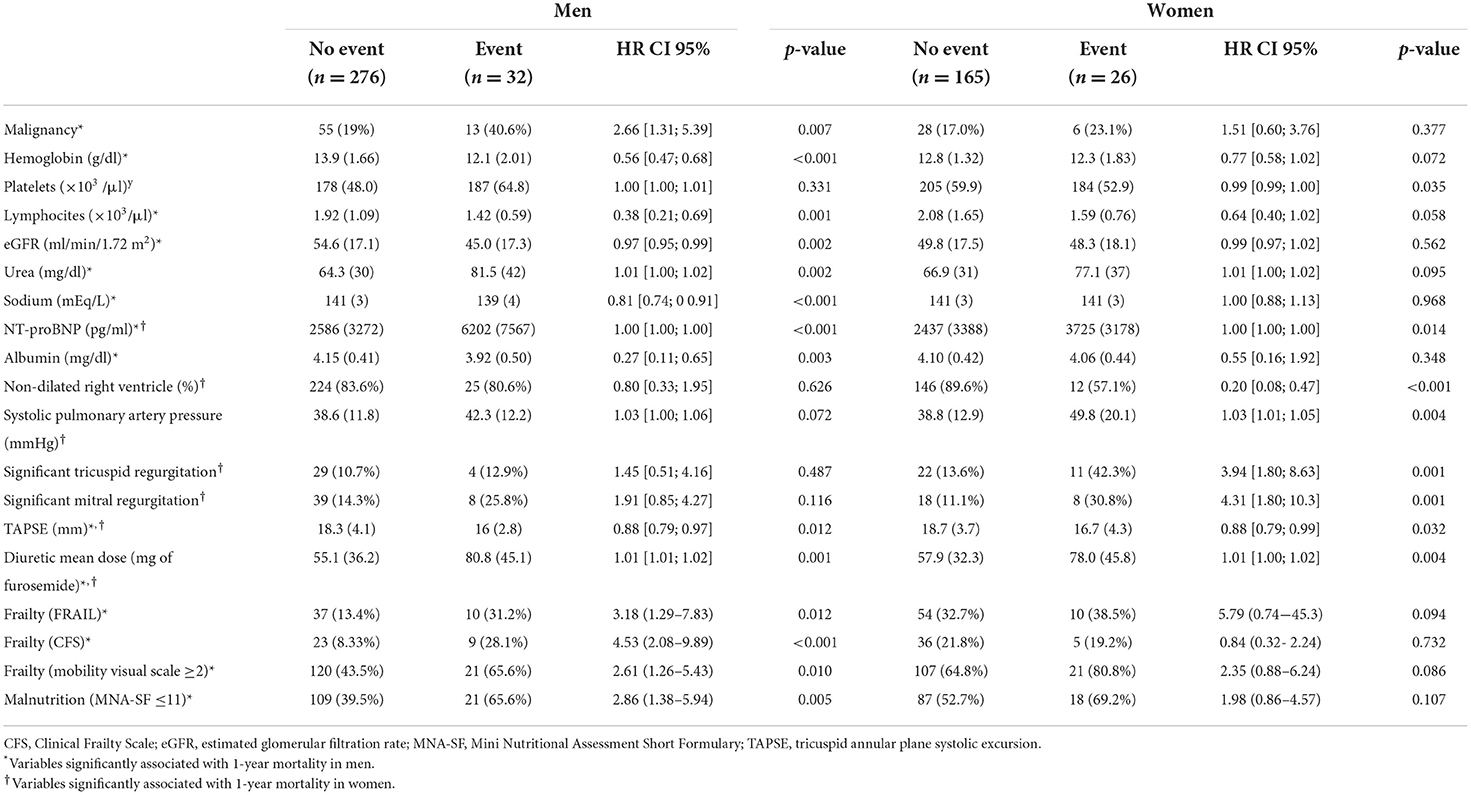
Table 2. Variables significantly associated with 1-year mortality according to sex.
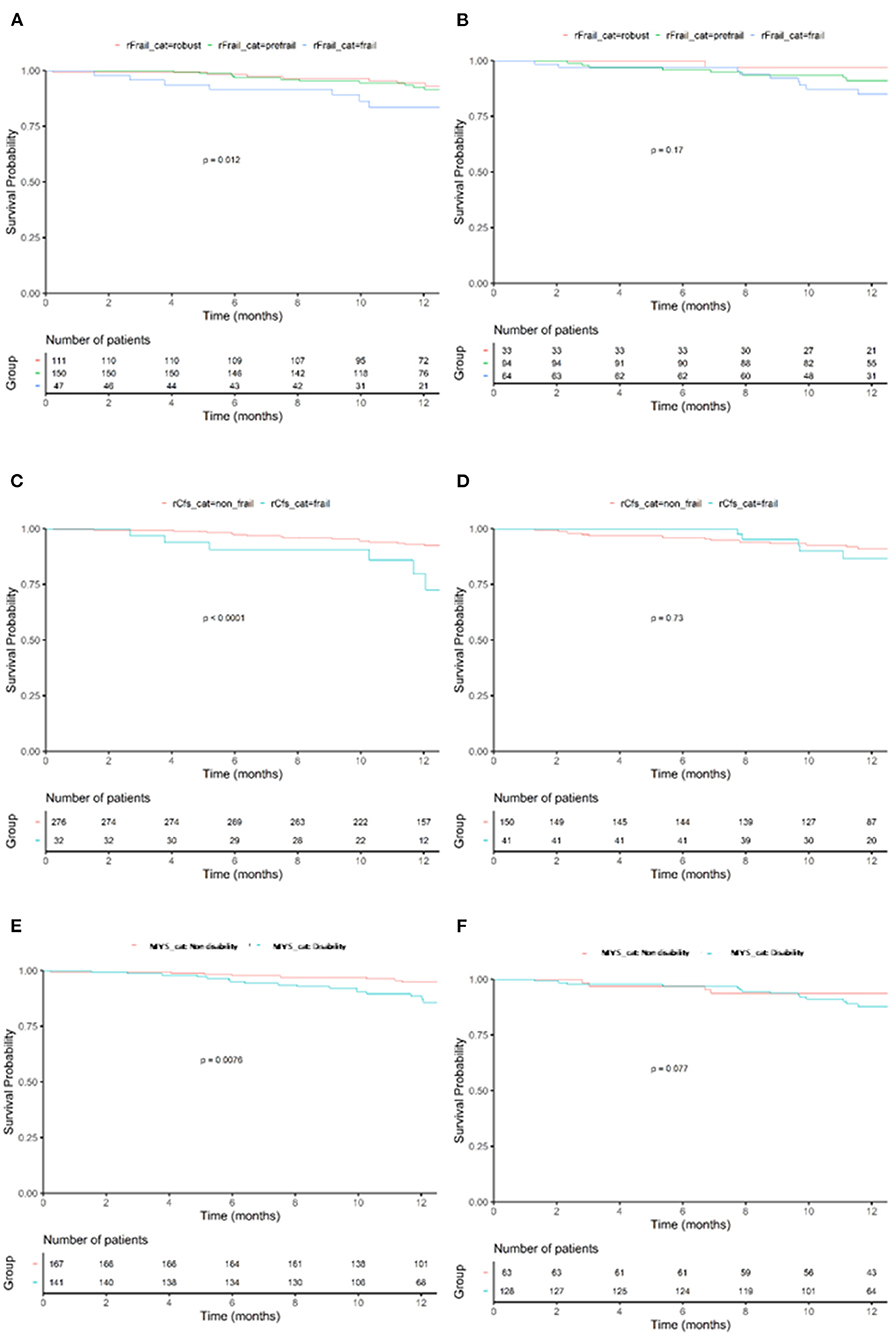
Figure 1. Kaplan–Meyer for 1-year mortality according to frailty category. Effects of frailty (FRAIL scale) in mortality in men (A) and women (B). Effects of frailty (Clinical Frailty scale) in mortality in men (C) and women (D). Effects of frailty (mobility visual scale) in mortality in men (E) and women (F). p-value shows comparison by Log-Rank.
During follow up, 202 patients (40%) fulfilled the 1-year composite endpoint of mortality and readmission for any cause:117 (38%) men and 85 (44.5%) women. Table 3 shows the variables associated with this endpoint according to sex in univariate analysis. Atrial fibrillation, physical signs of congestion, lower hemoglobin or lymphocytes levels, and a more advanced HF, were associated with mortality and readmission in men and women. Comorbidity and geriatric syndromes, were associated with worse prognosis in men, but not in women (except frailty estimated by Clinical Frailty Scale). Figure 2 shows the different impact of frailty in men and women in the composite endpoint.
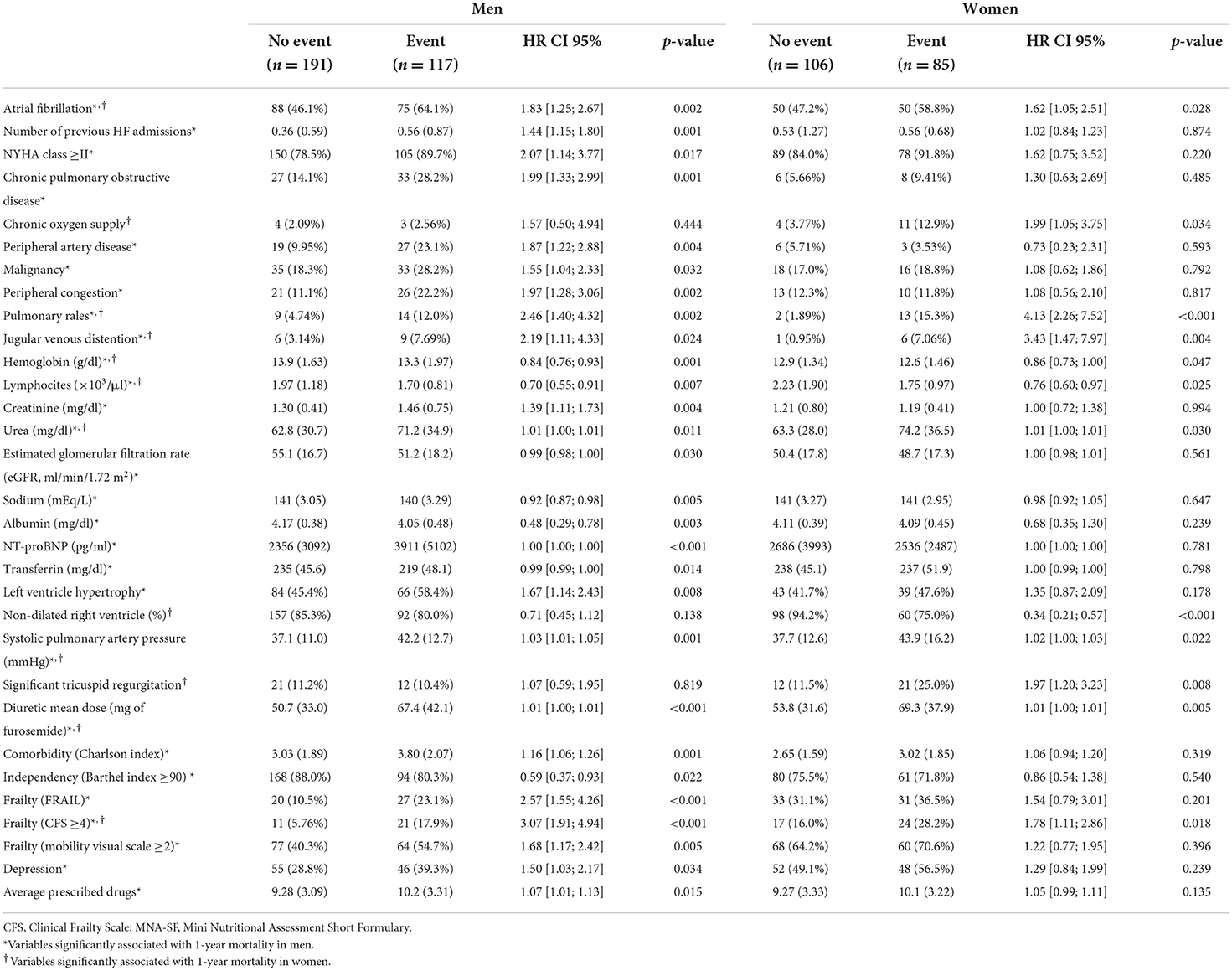
Table 3. Variables significantly associated with 1-year mortality or readmission according to sex.
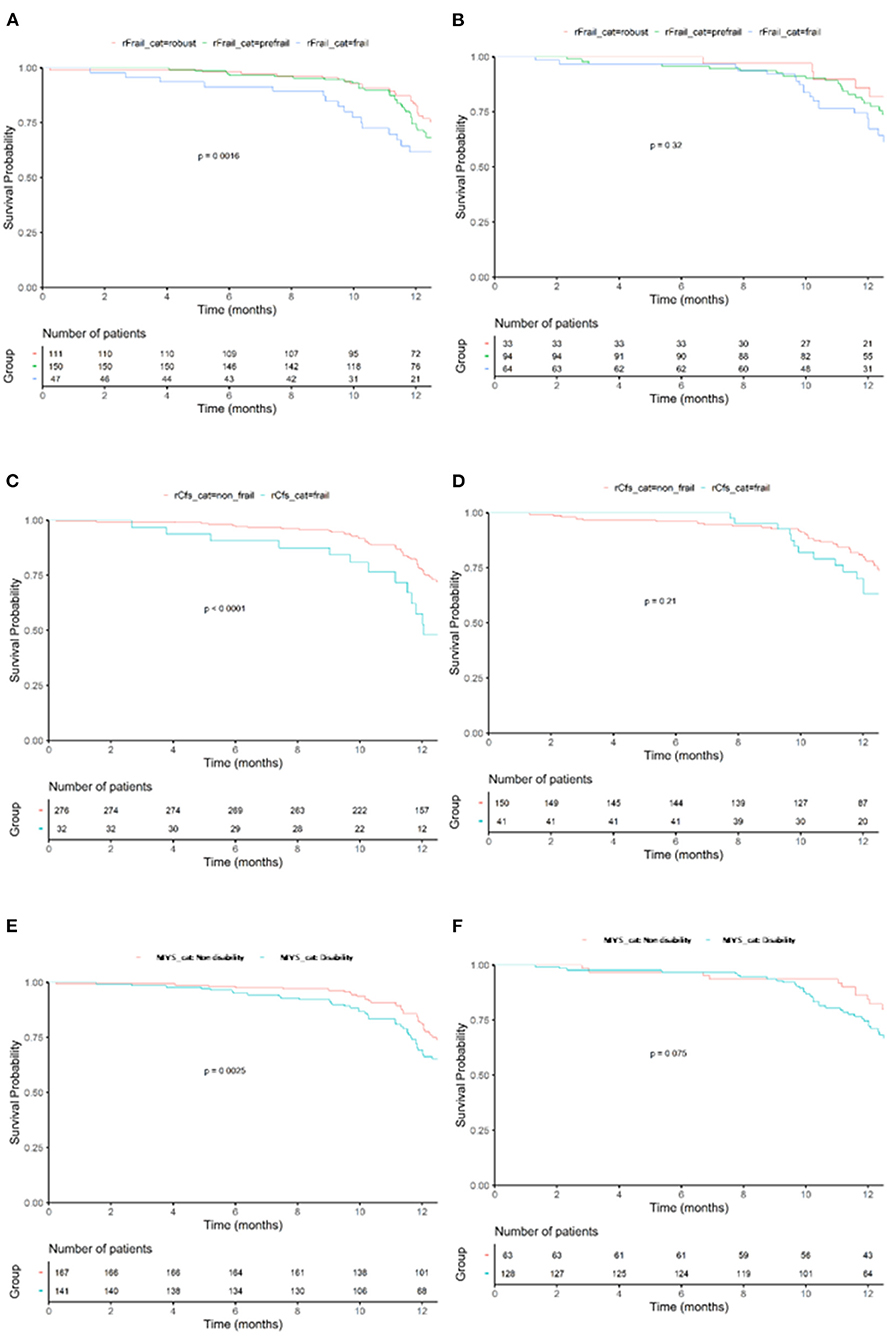
Figure 2. Kaplan–Meyer for 1-year mortality or readmission according to frailty category. Effects of frailty (FRAIL scale) in mortality or readmission in men (A) and women (B) Effects of frailty (Clinical Frailty scale) in mortality or readmission in men (C) and women (D). Effects of frailty (mobility visual scale) in mortality or readmission in men (E) and women (F). p-value shows comparison by Log-Rank.
In the multivariable analysis, frailty identified by the visual mobility scale was an independent predictor of mortality (HR 1.95, 95% CI 1.04–3.67, p = 0.03) and mortality/readmission (HR 2.06, 95% CI 1.05–4.04, p = 0.03) in men (Tables 4, 5). In women, higher doses of diuretics and higher levels of natriuretic peptides were the only factors significantly associated with mortality, while hemoglobin, right ventricular dilatation and higher diuretic doses were independently associated with mortality/readmission during follow-up (Tables 6, 7).
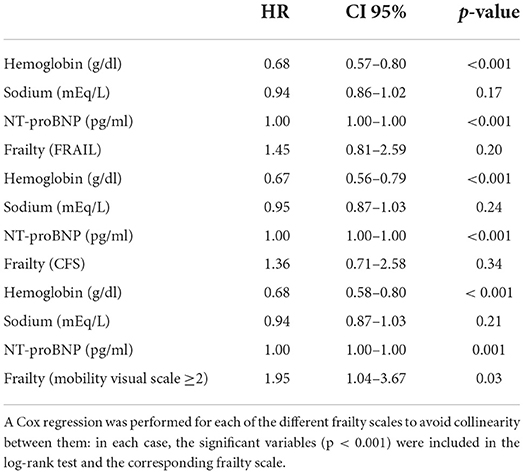
Table 4. Independent predictors of 1-year mortality in men.
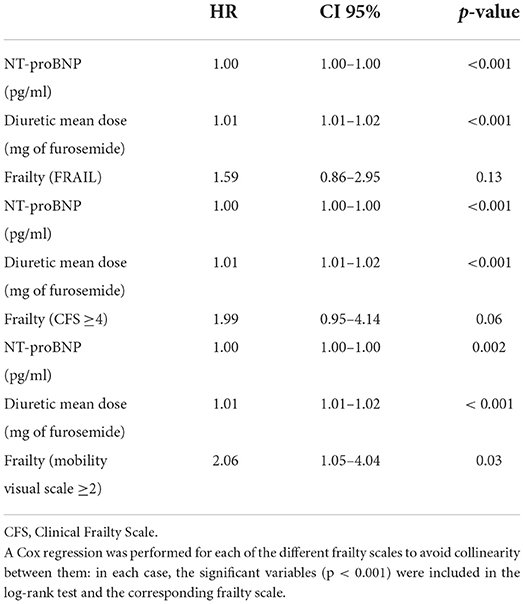
Table 5. Independent predictors of 1-year mortality and readmission in men.

Table 6. Independent predictors of 1-year mortality in women.
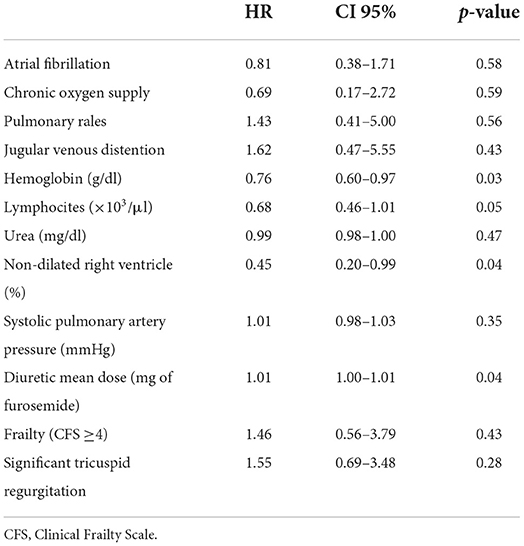
Table 7. Independent predictors of 1-year mortality and readmission in women.
Discussion
To the best of our knowledge, this is the first study addressing sex differences in the impact of frailty in elderly ambulatory patients with chronic HF followed by cardiologists. Main findings of our study are: (1) elderly men and women with chronic HF show a different baseline and clinical profile; (2) frailty and other geriatric syndromes are more common in women, although they only associate worse prognosis in men; (3) some parameters common in advanced stages of HF entail worse prognosis in men and women, but differ between them.
There are several sex differences in patients with HF previously reported, as traditional risk factors, pathophysiology and response to treatment differs between men and women (10, 11, 14, 15). In a large multicentre study, including >80,000 hospitalized patients, Hsich et al. described, more than a decade ago, that women with HF were usually older than men, more likely to have hypertension and depression and less likely to have coronary or peripheral artery disease. However, in-hospital mortality rates were similar irrespective of sex (16). Our study showed similar results, since HF women were older, and had less frequently a previous history of coronary or peripheral artery disease. However, patients included in our study were all ambulatory patients with chronic HF (i.e., not hospitalized), and mean age was much higher. Besides, our study adds novel evidence with valuable data from the late clinical follow up, unlike the study by Hsich et al.
In FRAGIC study, women presented with better LVEF compared with men, as previously reported (10). Such differences regarding the subtype of HF have been suggested to be partially explained due to inherent physiological distinctions between men and women (17, 18). Regarding clinical presentation, some studies suggest women usually present with worse functional class and more advanced symptoms (10, 11, 14). Interestingly, in our study key issues like NTproBNP levels or NYHA functional class did not differ at baseline between men and women, unlike other previous studies, in which female sex had been associated with worse functional class and even higher NTproBNP levels regardless of LVEF (14, 19). In FRAGIC study, higher levels of natriuretic peptides and diuretics doses were significantly associated with higher mortality in women at 1 year follow-up. On the other hand, lower hemoglobin and sodium levels and higher NTproBNP levels independently associated poorer prognosis in men, together with the presence of frailty identified by the visual mobility scale.
Regarding geriatric conditions, HF commonly coexists with frailty, especially in the elder population, yet the prevalence of frailty varies according to the scale used. Both conditions when present together lead to worse outcomes (3, 20). Thus, it is recommended to properly assess its presence (9, 21), since the greater accumulation of deficits in frailty domains, the greater the mortality (22). Notably, frailty affects women significantly more than men in HF, as demonstrated in a recent meta-analysis including 29 studies, in which the relative risk of frailty was found to be 26% higher in women compared with men (23). As expected, the relative risk of frailty in women was higher when defined with a physical approach. In this regard, Denfeld et al. performed a small prospective single-center study (including 115 patients, mean age 63.6 ± 15.7 years, 49% women) aimed to characterize sex differences in physical frailty in HF. Authors found that women with HF were significantly more likely to be physically frail than men. Frailty was related with higher overall comorbidity burden in both men and women although frail women had a worse symptom profile (24). However, such population was significantly younger than that in our study (mean age 63.6 vs. 81.4 years) and had different baseline characteristics: 71% had reduced LVEF and almost 50% had NYHA III-IV functional status (which may, in part, explain the discrepant findings). In our study, women were more commonly frail than men, irrespective of the scale. Hence, it could be hypothesized that these differences may rely on the fact that frailty scales might not adequately identify (or even overestimate) the presence of frailty in women. However, the FRAIL scale was developed in a cohort of 4,000 patients, 50% women and this scale was later validated in a mostly-women community population (25, 26). FRAIL scale has been also validated in a sample of 703 patients, 40% women (27), whereas the CFS was developed in a prospective cohort of 2305 patients, 61% women, from the Canadian Study of Health and Aging (CSHA) (28). Interestingly, in our study, women showed significantly worse self-reported quality of life. This finding has been previously reported in some studies, closely related to HF status (10), though it has also been found to be higher in frail patients (Souza).
Concerning the prognosis of frailty in HF patients, a recent metanalysis showed it was associated with an approximately 1.5-fold increase risk of death and hospitalization in HF patients, although differences between men and women were not explored (29). However, results of this study should be taken with caution, since the sample had high heterogeneity, with some studies including patients during an acute HF episode, and frailty was not uniformly defined. On the other hand, in a recent study including nearly 600 patients admitted with decompensated HF (mean age 76.6 years, 45% women), patients with higher CFS score showed a worse clinical profile and had higher probability of all-cause death and rehospitalisation in both men and women (30). Besides, it is recommended to assess frailty in an ambulatory fashion, and not in the setting of an acute HF event, as in those studies (9). In our study, frailty identified by the mobility visual scale was independently associated with mortality/readmission in men.
Recently, St Sauver et al. (31), demonstrated the negative relationship between inflammation, multi-morbidity and biologic aging, in such a way that men and elderly people, especially with higher comorbidity, had significantly higher levels of inflammatory biomarkers. This, in turn, has been linked with the concept of “inflammaging,” key component of the aging process. Soysal et al. (32) have associated this concept with the development of cardiovascular disease and frailty. Thus, although the prevalence of frailty was lower in men in our study, it could be hypothesized that a greater proinflammatory state might explain, at least in part, why it had a greater prognostic impact in older men with heart failure.
Our study, despite its prospective design, has some limitations that merit discussion. First, it is an observational study so we cannot rule out the possibility of selection bias. On the other hand, the sample size was modest, and the percentage of women included lower than that in other similar studies. Also, the 1-year event rate was relatively low, therefore results should be extrapolated with caution, particularly to other settings, since our study only included elderly ambulatory patients with chronic HF followed by cardiologists. In spite of these limitations, we think that this study provides new and interesting information on gender differences in the impact of frail in older patients from a large cohort of consecutive unselected elderly HF patients. Further studies will be required to elucidate the underlying reasons explaining a distinct effect of frailty according to gender.
Conclusion
Elderly women with HF present frailty and other geriatric conditions more often than men, although frailty is only associated with worse prognosis in men.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by CEIm Hospital Universitario de La Princesa, Madrid, Spain. The patients/participants provided their written informed consent to participate in this study.
Author contributions
PD-V and CJ-M prepared the first draft of the manuscript. All authors improved the manuscript with relevant content, contributed to the article, and approved the submitted version.
Acknowledgments
To the Geriatric Section of the Spanish Society of Cardiology, for its support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. (2018) 391:572–80. doi: 10.1016/S0140-6736(17)32520-5
2. McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42:3599–726. doi: 10.1093/eurheartj/ehab368
3. Heckman GA, McKelvie RS, Rockwood K. Individualizing the care of older heart failure patients. Curr Opin Cardiol. (2018) 33:208–16. doi: 10.1097/HCO.0000000000000489
4. Cherubini A, Oristrell J, Pla X, Ruggiero C, Ferretti R, Diestre G et al. The persistent exclusion of older patients from ongoing clinical trials regarding heart failure. Arch Intern Med. (2011) 171:550–6. doi: 10.1001/archinternmed.2011.31
5. Díez-Villanueva P, Jiménez-Méndez C, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol. (2021) 18:219–32. doi: 10.11909/j.issn.1671-5411.2021.03.009
6. Rodríguez-Mañas L, Féart C, Mann G, Viña J, Chatterji S, Chodzko-Zajko W, et al. Searching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition-consensus conference project. J Gerontol A Biol Sci Med Sci. (2013) 68:62–7. doi: 10.1093/gerona/gls119
7. Chaudhry SI, McAvay G, Chen S, Whitson H, Newman AB, Krumholz HM, et al. Risk factors for hospital admission among older persons with newly diagnosed heart failure: findings from the Cardiovascular Health Study. J Am Coll Cardiol. (2013) 61:635–42. doi: 10.1016/j.jacc.2012.11.027
8. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
9. Díez-Villanueva P, Arizá-Solé A, Vidán MT, Bonanad C, Formiga F, Sanchis J, et al. Recommendations of the geriatric cardiology section of the spanish society of cardiology for the assessment of frailty in elderly patients with heart disease. Rev Esp Cardiol. (2019) 72:63–71. doi: 10.1016/j.rec.2018.06.035
10. Lala A, Tayal U, Hamo CE, Youmans Q, Al-Khatib SM, Bozkurt B, et al. Sex differences in heart failure. J Card Fail. (2022) 28:477–98. doi: 10.1016/j.cardfail.2021.10.006
11. Postigo A, Martínez-Sellés M. Sex influence on heart failure prognosis. Front Cardiovasc Med. (2020) 7:616273. doi: 10.3389/fcvm.2020.616273
12. Díez-Villanueva P, Salamanca J, Ariza-Solé A, Formiga F, Martín-Sánchez FJ, Bonanad Lozano C, et al. Impacto de la FRAgilidad y otros síndromes Geriátricos en el manejo clínico y pronóstico del paciente anciano ambulatorio con Insuficiencia Cardiaca (FRAGIC). Estudio prospectivo y multicéntrico. Rev Esp Geriatr Gerontol. (2020) 55:29–33. doi: 10.1016/j.regg.2019.08.005
13. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
14. Dewan P, Rørth R, Raparelli V, Campbell RT, Shen L, Jhund PS, et al. Sex-related differences in heart failure with preserved ejection fraction. Circ Heart Fail. (2019) 12:e006539. doi: 10.1161/CIRCHEARTFAILURE.119.006539
15. Vicent L, Guerra J, Vazquez-García R, Gonzalez-Juanatey JR, Dolz LM, Segovia J, et al. Ischemic etiology and prognosis in men and women with acute heart failure. J Clin Med. (2021) 10:1713. doi: 10.3390/jcm10081713
16. Hsich EM, Grau-Sepulveda MV, Hernandez AF, Peterson ED, Schwamm LH, Bhatt DL, et al. Sex differences in in-hospital mortality in acute decompensated heart failure with reduced and preserved ejection fraction. Am Heart J. (2012) 163:430–7, 437.e1–3. doi: 10.1016/j.ahj.2011.12.013
17. Ravera A, Santema BT, de Boer RA, Anker SD, Samani NJ, Lang CC, et al. Distinct pathophysiological pathways in women and men with heart failure. Eur J Heart Fail. (2022). doi: 10.1002/ejhf.2534. [Epub ahead of print].
18. Beale AL, Meyer P, Marwick TH, Lam CSP, Kaye DM. Sex differences in cardiovascular pathophysiology: why women are overrepresented in heart failure with preserved ejection fraction. Circulation. (2018) 138:198–205. doi: 10.1161/CIRCULATIONAHA.118.034271
19. Stolfo D, Uijl A, Vedin O, Strömberg A, Faxén UL, Rosano GMC, et al. Sex-based differences in heart failure across the ejection fraction spectrum: phenotyping, and prognostic and therapeutic implications. JACC Heart Fail. (2019) 7:505–15. doi: 10.1016/j.jchf.2019.03.011
20. Pandey A, Kitzman D, Reeves G. Frailty is intertwined with heart failure: mechanisms, prevalence, prognosis, assessment, and management. JACC Heart Fail. (2019) 7:1001–101. doi: 10.1016/j.jchf.2019.10.005
21. Vitale C, Jankowska E, Hill L, Piepoli M, Doehner W, Anker SD, et al. Heart Failure Association/European Society of Cardiology position paper on frailty in patients with heart failure. Eur J Heart Fail. (2019) 21:1299–305. doi: 10.1002/ejhf.1611
22. Kleipool EEF, Wiersinga JHI, Trappenburg MC, Rossum AC, Dam CS, Liem SS, et al. The relevance of a multidomain geriatric assessment in older patients with heart failure. ESC Heart Fail. (2020) 7:1264–72. doi: 10.1002/ehf2.12651
23. Davis MR, Lee CS, Corcoran A, Gupta N, Uchmanowicz I, Denfeld QE. Gender differences in the prevalence of frailty in heart failure: a systematic review and meta-analysis. Int J Cardiol. (2021) 333:133–40. doi: 10.1016/j.ijcard.2021.02.062
24. Denfeld QE, Habecker BA, Camacho SA, Roberts Davis M, Gupta N, Hiatt SO, et al. Characterizing sex differences in physical frailty phenotypes in heart failure. Circ Heart Fail. (2021) 14:e008076. doi: 10.1161/CIRCHEARTFAILURE.120.008076
25. Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J Am Geriatr Soc. (2012) 1478–86. doi: 10.1111/j.1532-5415.2012.04074.x
26. Woo J, Yu R, Wong M, Yeung F, Wong M, Lum C. Frailty screening in the community using the FRAIL Scale. J Am Med Dir Assoc. (2015) 16:412–9. doi: 10.1016/j.jamda.2015.01.087
27. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. (2012) 16:601–8. doi: 10.1007/s12603-012-0084-2
28. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1503/cmaj.050051
29. Yang X, Lupón J, Vidán MT, Ferguson C, Gastelurrutia P, Newton PJ, et al. Impact of frailty on mortality and hospitalization in chronic heart failure: a systematic review and meta-analysis. J Am Heart Assoc. (2018) 7:e008251. doi: 10.1161/JAHA.117.008251
30. Kanenawa K, Isotani A, Yamaji K, Nakamura M, Tanaka Y, Hirose-Inui K, et al. The impact of frailty according to Clinical Frailty Scale on clinical outcome in patients with heart failure. ESC Heart Fail. (2021) 8:1552–61. doi: 10.1002/ehf2.13254
31. St Sauver J, Rocca W, LeBrasseur N, Chamberlain A, Olson J, Jacobson D, et al. Inflammatory biomarkers, multi-morbidity, and biologic aging. J Int Med Res. (2022) 50:3000605221109393. doi: 10.1177/03000605221109393
Keywords: frailty, heart failure, elderly, sex, prognosis
Citation: Díez-Villanueva P, Jiménez-Méndez C, Bonanad C, Ortiz-Cortés C, Barge-Caballero E, Goirigolzarri J, Esteban-Fernández A, Pérez-Rivera A, Cobo M, Sanz-García A, Formiga F, Ariza-Solé A, Martínez-Sellés M and Alfonso F (2022) Sex differences in the impact of frailty in elderly outpatients with heart failure. Front. Cardiovasc. Med. 9:1000700. doi: 10.3389/fcvm.2022.1000700
Received: 22 July 2022; Accepted: 26 August 2022;
Published: 12 September 2022.
Edited by:
Matteo Pagnesi, ASST Spedali Civili di Brescia, ItalyReviewed by:
Dario Cani, ASST Spedali Civili, ItalyDeirdre M. Mooney, Maine Medical Center, United States
Copyright © 2022 Díez-Villanueva, Jiménez-Méndez, Bonanad, Ortiz-Cortés, Barge-Caballero, Goirigolzarri, Esteban-Fernández, Pérez-Rivera, Cobo, Sanz-García, Formiga, Ariza-Solé, Martínez-Sellés and Alfonso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Díez-Villanueva, cGFibG9fZGllel92aWxsYW51ZXZhQGhvdG1haWwuY29t
†These authors share first authorship
‡These authors share last authorship