Abstract
Background:
The clinical application value of cardiopulmonary exercise test (CPET) has increasingly attracted attention, and related research has been increasing yearly. However, there is no summary analysis of the existing CPET literature. This is the first bibliometric analysis of publications in the CPET.
Methods:
CPET-related articles published between 2002 and 2021 were retrieved from the Web of Science Core Collection database. The search was limited to Articles and Reviews in English. CiteSpace software was used to conduct collaborative network analysis of countries/regions, institutions, authors, the co-occurrence of subject categories and keywords, and co-citation analysis of authors, journals, and references.
Results:
A total of 4,426 publications were identified. During the study period, the number of published articles increased yearly. Developed countries from the Americas and Europe led the field. The University of Milan was the most prolific institution, with Ross Arena and Wasserman K being the most prolific and co-cited authors in the field, respectively. Cardiovascular System & Cardiology and Respiratory System were the main areas involved. Moreover, heart failure, oxygen uptake, and prognostic value were the central themes.
Conclusions:
CPET had attracted widespread attention, and the number of publications will increase substantially according to the current growth trends. In the future, CPET is expected to be further adopted in large-scale clinical studies as a means of assessing the functional ability of patients to verify the efficacy of related interventions. High-quality evidence-based medical CPET-related indicators is expected to be used in clinical diseases risk prediction.
Introduction
Exercise testing have many modalities to be utilized in different clinical situations, the widely used ones include 6-minute walk test, exercise-induced bronchospasm test, stair climbing, shuttle test and cardiopulmonary exercise test (1). Cardiopulmonary exercise test (CPET) is an exercise test that objectively and quantitatively assesses cardiopulmonary fitness (CRF) by measuring breathing gas metabolic parameters simultaneously (e.g., oxygen uptake, carbon dioxide excretion) during exercise (2). At present, CPET is the internationally recognized gold standard for evaluating CRF (3), which is defined as the ability of the circulatory and respiratory systems to provide oxygen to skeletal muscle during continuous physical activity. It is a comprehensive reflection of the body's exercise capacity (4), assessed by the quantifiable index of maximum oxygen uptake (VO2max). Many studies have shown that CRF is a strong independent predictor of chronic diseases, such as cardiovascular disease (5) and cancer (6), and a modifiable risk factor which is influenced by lifestyle and physical activity. Relevant studies have shown that, compared with traditional clinical risk factors for cardiovascular disease, CRF can better predict the health status and possible adverse events (7, 8). Previously, CPET was mainly performed by cardiopulmonary physiologists for physiological scientific research, but in recent years, more studies have found that CRF-related indicators have an important predictive role in disease prognosis (9–12), which has led to the extensive use of CPET in clinical practice (13). In 2016, the American Heart Association proposed in a scientific statement that CRF should be categorized as a clinical vital sign and routinely assessed in clinical practice (14).
Bibliometrics is a scientific research method that quantitatively analyzes all knowledge carriers (journal articles, books, etc.) through mathematical or statistical methods (15), and it can be applied to any discipline to quantitatively analyze the historical development and evolution trends of a specific research field. With the development of information technology, a series of knowledge mapping software based on bibliometric research methods have emerged, which can present complex knowledge entities and their interrelationships in the form of visual graphics and facilitates understanding of the knowledge structure system of a research field. The medical field is a major field of bibliometric methods application, and bibliometric studies on cardiovascular (16), respiratory (17), dermatology (18), oncology (19), infectious diseases (20) have been recognized. The literature search reveals that the number of bibliometric-related documents shows a trend of increasing yearly.
As the use of CPET in clinical practice has become more widespread, more research based on CPET have been conducted. Although traditional literature reviews can summarize and analyze CPET, it is still mainly limited to a specific topic that the author is concerned about and cannot provide a comprehensive analysis of the CPET field which can help the other researchers quickly understand the key research team, research results and related progress. This problem can be effectively solved by introducing a bibliometric approach to compile and analyze the published documents about CPET from the past 20 years. We found that no bibliometric study on CPET has been conducted, which prompted us to conduct this study.
Methods
Data acquisition and search strategy
The Web of Science (WoS, Clarivate Analytics, Philadelphia, PA, USA) database collected more than 12,000 international academic journals and is one of the most comprehensive and authoritative database platforms for the assessment of global academic resources (21). In addition, it has the function of citation index search, which is a necessary condition for bibliometric co-citation analysis. Therefore, the WoS database was selected as the data source for our study.
All literature was retrieved and exported from the Web of Science Core Collection (WoSCC) database with the search formula TS (Topic) = (“cardiopulmonary exercise test*”). The indices we searched include Science Citation Index Expanded (SCI-EXPANDED), Social Sciences Citation Index (SSCI), Arts & Humanities Citation Index (AHCI), Conference Proceedings Citation Index–Science (CPCI-S), Conference Proceedings Citation Index–Social Science & Humanities (CPCI-SSH), Emerging Sources Citation Index (ESCI), Current Chemical Reactions (CCR-EXPANDED), Index Chemicus (IC). The preliminary search yielded 6,270 records, and a total of 4,426 records were obtained. The data analysis set through the results refinement function of WoSCC database, with the setting of language: English, document type: Articles, Review Articles, and the time span from January 1, 2002, to December 31, 2021. 4,426 records were selected with “Full record with cited references,” exported in “the plain text file format,” and renamed in the form of “download*.txt" to ensure that they can be read correctly by CiteSpace software (22).
Data extraction
A total of 4,426 documents were imported into CiteSpace (5.8.R3) software to remove duplicates. The acquired documents were then manually reviewed by two independent researchers to ensure relevance to the CPET research topic. When there is a dispute between two researchers, they need to read the original article together to reach a final agreement.
Data analysis
Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA, USA) software was used for the graphs of the number of publications per year. The analysis of knowledge mapping visualization was performed by the CiteSpace software, which is one of the most popular software for bibliometric analysis. It was developed by Prof. Chaomei Chen based on the Java programming language and can carry out collaborative network analysis, co-occurrence analysis, and co-citation analysis to reveal the collaborative networks of countries, institutions and authors, the distribution of subject areas, high-frequency keywords and core literature in a particular research area in the form of visual graphs or tables.
Results
Annual quantitative distribution of publications
The annual number of publications revealed the development trends of research in this field. As was shown in Figure 1, from 2002 to 2021, the number of publications related to CPET had been steadily increasing. A slow growth trend was observed from 2002 to 2017. In contrast, it had achieved a rapid increase from 2017 (323) to 2021 (594), which indicated that the CPET had received increasing attention in the last 5 years.
Figure 1
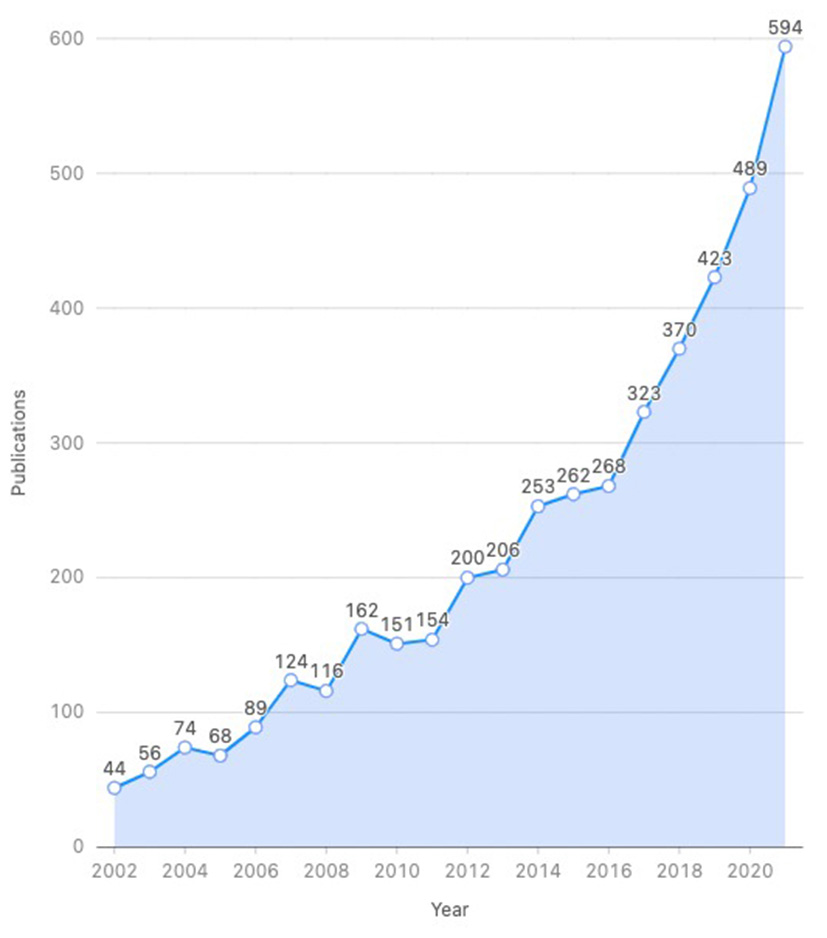
Annual number of publications about CPET.
The 4,426 documents contain 4,180 articles and 246 reviews. Articles accounted for approximately 95% of the document type, indicating a greater focus on original research such as clinical trials or case reports.
Collaborative network analysis
Country
Researchers from 104 countries published CPET-related articles, with the United States (1,135), England (513), Italy (475), Brazil (422), and Germany (339) being the top 5 countries (Table 1). It is worth noting that the total number of publications from the United States was more than twice that from England, which ranks second. At the same time, the United States had a high BC (betweenness centrality) value (BC = 0.62).
Table 1
| Rank | Country | Count | BC | Year |
|---|---|---|---|---|
| 1 | USA | 1,135 | 0.62 | 2002 |
| 2 | England | 513 | 0.19 | 2007 |
| 3 | Italy | 475 | 0.00 | 2007 |
| 4 | Brazil | 422 | 0.00 | 2007 |
| 5 | Germany | 339 | 0.00 | 2007 |
| 6 | Canada | 253 | 0.88 | 2008 |
| 7 | Japan | 243 | 0.00 | 2007 |
| 8 | Netherlands | 197 | 0.24 | 2008 |
| 9 | France | 170 | 0.78 | 2008 |
| 10 | Belgium | 160 | 0.10 | 2007 |
Top 10 countries in terms of number of published CPET articles.
BC, betweenness centrality.
Figure 2 showed that each node represents a country, the node size is positively correlated with the frequency of co-occurrence in different country. The line between two nodes represents the co-occurrence relationship between two countries, and the thickness of the line indicates the strength of the relationship. The color of the rings and lines around the node indicate the year in which the country or relationship first appeared. The purple circles around some nodes indicate betweenness centrality (BC), which shows the importance of a node in the whole network. Nodes with a BC value ≥0.1 are marked in the network with a purple ring. The thickness of the purple ring is proportional to its BC value. The first year of appearance of the United States was 2002. It is 4–5 years earlier than the other countries in the top 10, indicating that the United States had taken the lead in CPET-related research on a global scale and the research interest was very high. The research results from the United States played an important role in the global collaborative research network. In addition, Canada (BC = 0.88) and France (BC = 0.78) also had a high BC value, indicating strong collaborative relationships with other countries. Italy, Brazil, Germany and Japan had low BC values, indicating that these countries have weaker cooperative relations with other countries, as shown in Figure 2 that they were located on the edge of the network structure. However, they were ranked in top 10 in terms of the number of publications, which reflects the great contributions these countries had made in this research field.
Figure 2
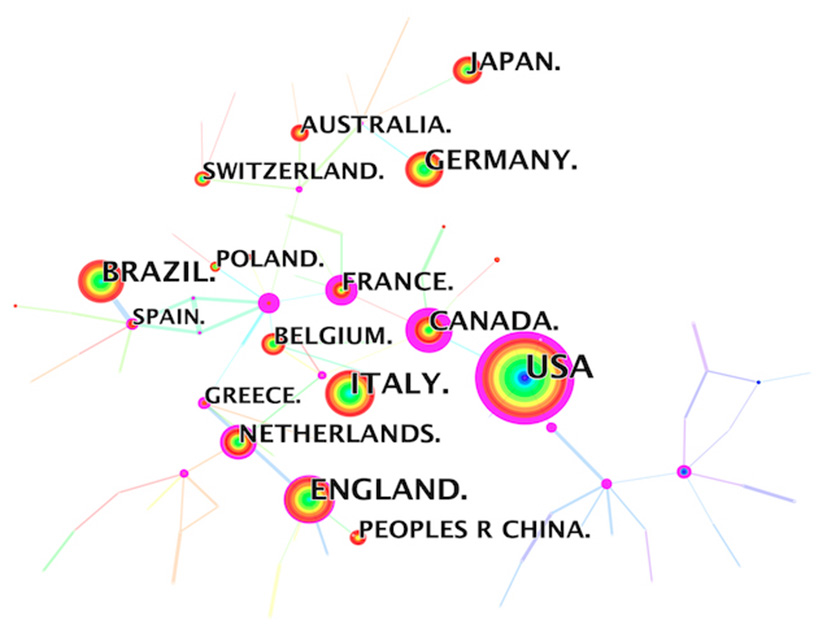
Country collaborative network analysis.
Institutions
CPET-related research involved 480 institutions worldwide, and six of the top 10 institutions in terms of number of articles published were from the United States, which once again highlight the strong influence of the United States in this field. The top three institutions were the University of Milan (191, Italy), Stanford University (114, USA), and the University of São Paulo (105, Brazil) (Table 2).
Table 2
| Rank | Institution | Count | BC | Country | Year |
|---|---|---|---|---|---|
| 1 | University of Milan | 191 | 0.10 | Italy | 2002 |
| 2 | Stanford University | 114 | 0.05 | USA | 2004 |
| 3 | University of São Paulo | 105 | 0.00 | Brazil | 2002 |
| 4 | Mayo Clinic | 90 | 0.02 | USA | 2002 |
| 5 | University of Illinois | 90 | 0.05 | USA | 2013 |
| 6 | Istituto di Ricovero e Cura a Carattere Scientifico | 85 | 0.22 | Italy | 2002 |
| 7 | Brigham and Women's Hospital | 73 | 0.27 | USA | 2005 |
| 8 | Technical University of Munich | 70 | 0.01 | Germany | 2005 |
| 9 | Virginia Commonwealth University | 70 | 0.19 | USA | 2004 |
| 10 | Duke University | 68 | 0.28 | USA | 2002 |
Top 10 institutions based on the number of CPET publications.
BC, betweenness centrality.
The 1st ranked University of Milan had almost 80 more articles than the 2nd ranked Stanford University, indicating a huge lead. Interestingly, none of the top five institutions had a BC value >0.1, indicating that the cooperation between the top research institutions was not close, and they mainly conducted CPET-related research independently (Figure 3).
Figure 3
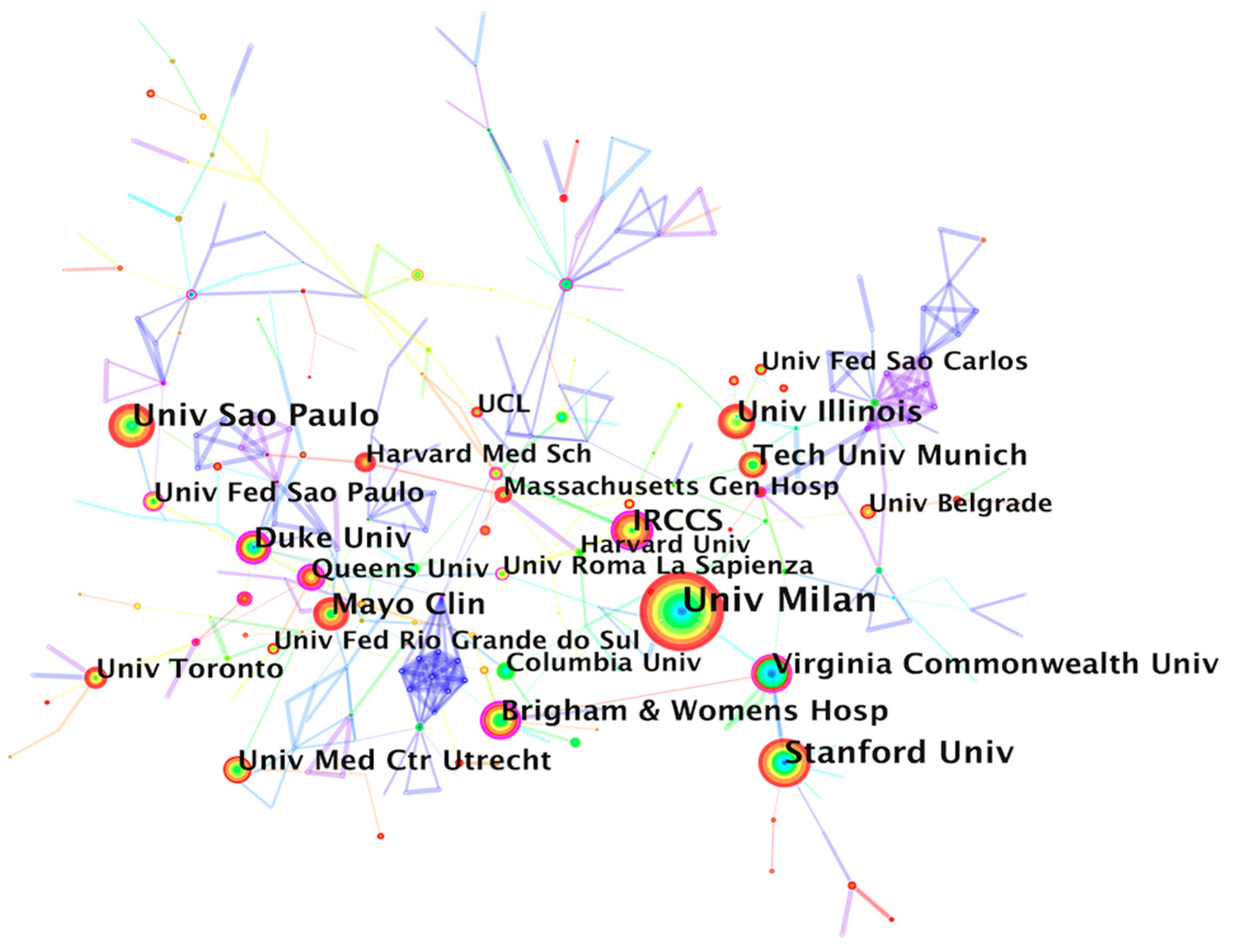
Institution collaborative network analysis.
Authors
The analysis of the author collaborative network showed that Ross Arena (142) had the most published articles, followed by Jonathan Myers (110), Marco Guazzi (96), and Piergiuseppe Agostoni (92) (Table 3), and the number of articles per capita had reached over 90, which was the highest ranking. The 5th to 10th authors had more than twice the number of published papers per capita and constitute the most representative high-yield author team in the CPET field. Further, the BC values of the top 10 authors were not high, which once again confirmed that the research cooperation relationship related to CPET was not strong. In Figure 4, each node represent an author. Nodes with usage bursts are visualized by red rings, indicating that the author appeared at a high frequency during a certain period. Most of the top 10 authors had high burst values, suggesting that their research directions were well correlated with CPET topics.
Table 3
| Rank | Author | Count | Burst | BC | Year |
|---|---|---|---|---|---|
| 1 | Ross Arena | 142 | – | 0.03 | 2006 |
| 2 | Jonathan Myers | 110 | 3.91 | 0.04 | 2006 |
| 3 | Marco Guazzi | 96 | 3.18 | 0.10 | 2006 |
| 4 | Piergiuseppe Agostoni | 92 | 8.91 | 0.01 | 2008 |
| 5 | Ugo Corra | 45 | – | 0.03 | 2006 |
| 6 | Alfred Hager | 41 | 4.33 | 0.00 | 2008 |
| 7 | Damiano Magri | 39 | 4.88 | 0.05 | 2008 |
| 8 | Elisabetta Salvioni | 39 | 6.21 | 0.07 | 2012 |
| 9 | J Alberto Neder | 37 | 12.01 | 0.02 | 2016 |
| 10 | Gregory D Lewis | 36 | 5.83 | 0.00 | 2010 |
Top 10 authors based on the number of CPET publications.
BC, betweenness centrality.
Figure 4
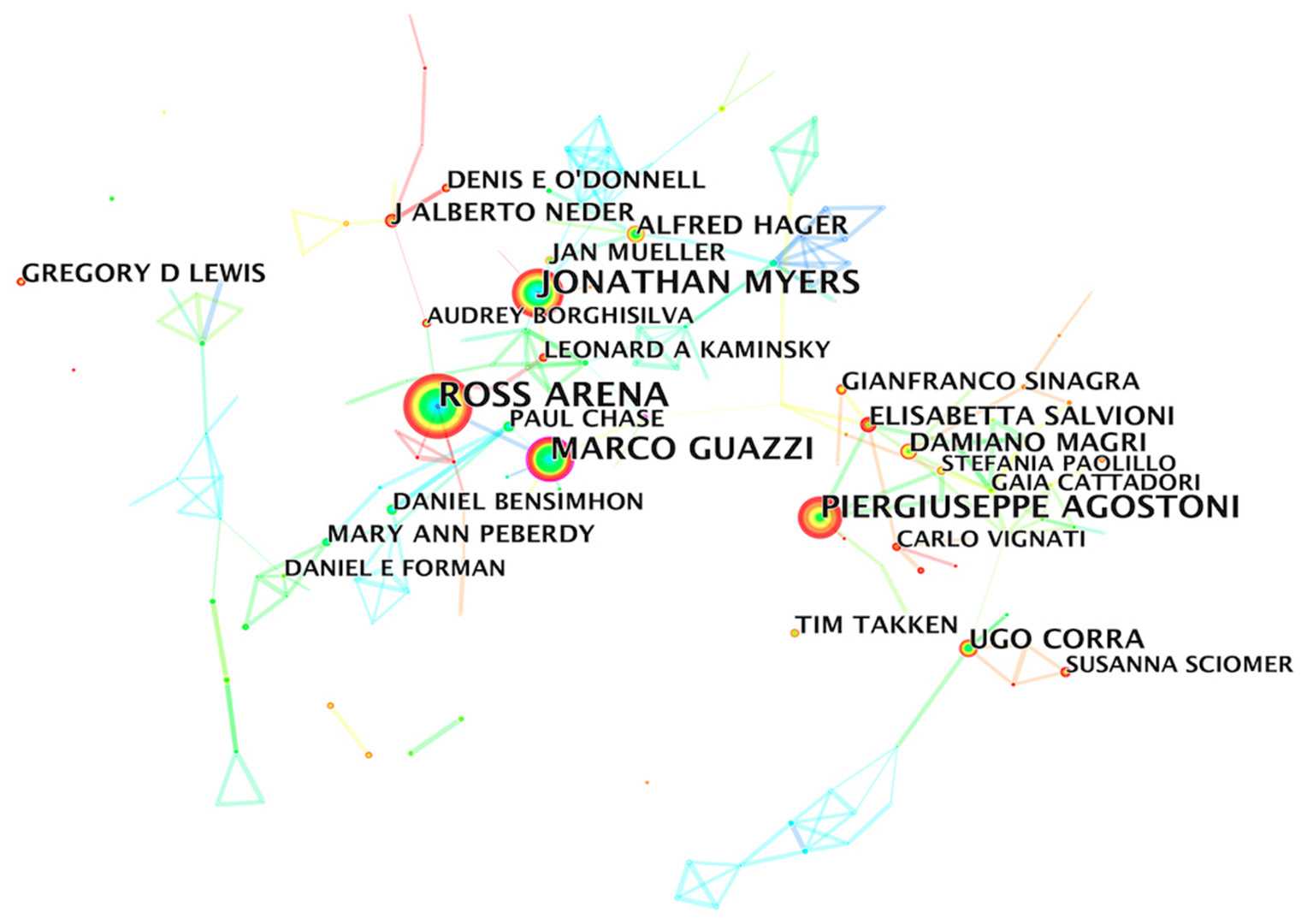
Author collaborative network analysis.
Co-occurrence analysis
Subject categories
Supplementary Table 1 showed that Cardiovascular System & Cardiology (1948) was a key discipline in the CPET field, and the number of publications under this discipline category far exceeded that of other disciplines. Respiratory System (776), and General & Internal Medicine (404) were ranked 2nd and 3rd respectively. In addition, Sport Sciences, Physiology, Surgery, Pediatrics, Rehabilitation, Research & Experimental Medicine, and Critical Care Medicine were also applied subjects of CPET in clinical practice.
It is worth pointing out that Critical Care Medicine had a significantly high BC value (BC=0.92), suggesting that it was the connection between other sub-subject categories (Supplementary Figure 1).
Keywords
Keywords are the highly refined content of the full text, which reflects the article topic. Table 4 showed the top 20 keywords with co-occurrence frequency in CPET field. Among them, heart failure, exercise capacity, quality of life, oxygen uptake all co-occurred more than 300 times, and the BC values of keywords such as morality, physical activity, survival, risk, oxygen consumption, adult, anaerobic threshold, and gas exchange were all ≥0.1, indicating that they played an important role in connecting other keywords in the whole keyword network.
Table 4
| Rank | Keywords | Count | BC | Rank | Keywords | Count | BC |
|---|---|---|---|---|---|---|---|
| 1 | Heart failure | 805 | 0.07 | 11 | performance | 323 | 0.03 |
| 2 | Capacity | 644 | 0.09 | 12 | association | 313 | 0.02 |
| 3 | Exercise | 623 | 0.03 | 13 | survival | 287 | 0.38 |
| 4 | Mortality | 566 | 0.15 | 14 | risk | 271 | 0.11 |
| 5 | Cardiopulmonary exercise testing | 554 | 0.08 | 15 | oxygen consumption | 268 | 0.18 |
| 6 | Exercise capacity | 474 | 0.03 | 16 | adult | 268 | 0.24 |
| 7 | Disease | 389 | 0.03 | 17 | anaerobic threshold | 262 | 0.31 |
| 8 | Physical activity | 369 | 0.14 | 18 | gas exchange | 250 | 0.29 |
| 9 | Quality of life | 358 | 0.04 | 19 | recommendation | 242 | 0.00 |
| 10 | Oxygen uptake | 328 | 0.10 | 20 | children | 242 | 0.03 |
Top 20 keywords on CPET.
BC, betweenness centrality.
To further determine the relationships among keywords, we used the log-likelihood rate (LLR) algorithm model to perform a cluster analysis and extracted the top 10 cluster labels based on the keyword fields. Modularity Q=0.7894, Silhouettes S=0.9455, indicating that the structure of the clusters was significant, and the clustering relationship was highly credible. Smaller values of the cluster labels indicate a larger number of keywords within the cluster. The top 10 clustering labels were: oxygen consumption (#0), exercise capacity (#1), pulmonary hypertension (#2), chronic heart failure (#3), exercise test (#4), oxygen uptake (#5), cardiopulmonary exercise testing (#6), heart failure (#7), congenital heart disease (#8), and mortality (#9). The cluster labels generally reflected three major aspects: the clinical significance of CPET, the evaluation indicators and the diseases in which it is mainly applied in clinical practice (Figure 5).
Figure 5
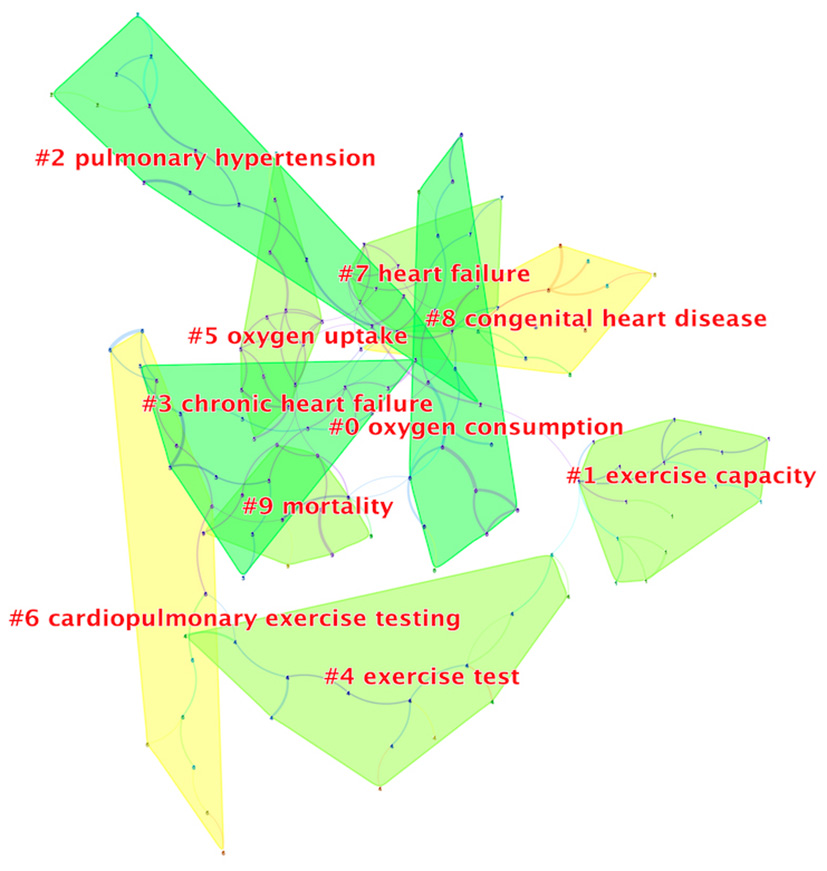
Keyword cluster analysis.
Keywords burst analysis refers to a surge in the frequency of a keyword in a certain period, indicating that the keyword had received high attention from researchers in that period. The burst strength represents the intensity of the rapid growth of a keyword. Based on the keywords burst analysis, research hotspots in different periods during the development of CPET can be discovered. As shown in Figure 6, between 2002 and 2009, congenital heart disease, BNP and heart failure, and myocardial infarction were the main research hotspots, and peak oxygen uptake was the main evaluation indication of CPET. Between 2004 and 2014, many studies focused on the evaluation of other indications provided by CPET, such as the index of ventilation efficiency over the min ventilation-carbon dioxide production (VE/VCO2) slope. In the last 5 years, the concept of CRF had been introduced and attracted continuous and widespread attention, CPET had been widely recommended by clinical guidelines for cardiovascular diseases. Cardiovascular diseases were still the main application area of CPET and this continues to be a main research interest.
Figure 6
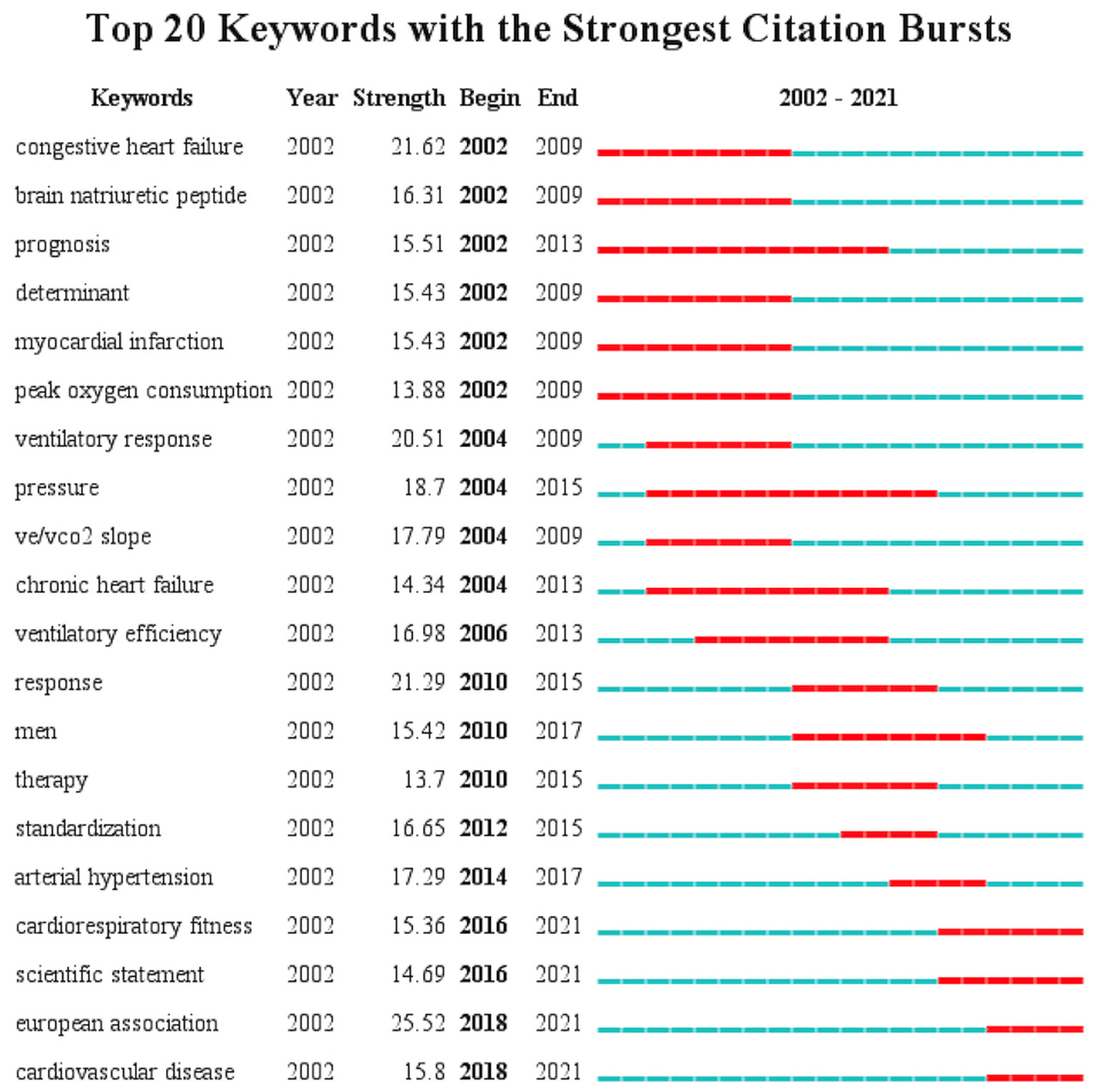
Top 20 keywords in burst analysis.
Co-citation analysis
Author
When two authors' papers are simultaneously cited by a third author's papers, it indicates that there is a co-citation relationship between these two authors. Table 5 showed the top 10 authors by co-citation frequency. Wasseman K had an absolute lead in co-citation frequency (1,078) and a high BC value (0.91), indicating that his research had a great influence in the CPET field. The second was the American Thoracic Society rather than an independent author because CiteSpace software only extracts the first author by default when conducting author co-citation analysis. The high citation frequency was mainly related to the clinical guidelines it published as the author. It is worth pointing out that the authors ranked 3rd to 5th: Guazzi M, Myers J, Arena R were also the top three authors in the author co-occurrence analysis, indicating that they had a steady contribution to the CPET field. It should also be noted that the 6th ranked author Beaver WL had a high BC value (1.00), suggesting that his research was widely cited throughout the co-citation network (Figure 7).
Table 5
| Rank | Co-cited author | Co-cited frequency | BC |
|---|---|---|---|
| 1 | Wasserman K | 1,078 | 0.91 |
| 2 | American Thoracic Society | 789 | 0.04 |
| 3 | Guazzi M | 716 | 0.13 |
| 4 | Myers J | 669 | 0.28 |
| 5 | Arena R | 637 | 0.09 |
| 6 | Beaver WL | 595 | 1.00 |
| 7 | Balady GJ | 490 | 0.00 |
| 8 | Mancini DM | 415 | 0.39 |
| 9 | Crapo RO | 385 | 0.07 |
| 10 | Whipp BJ | 365 | 0.26 |
Top 10 authors ranked by co-cited frequency on CPET publications.
BC, betweenness centrality.
Figure 7
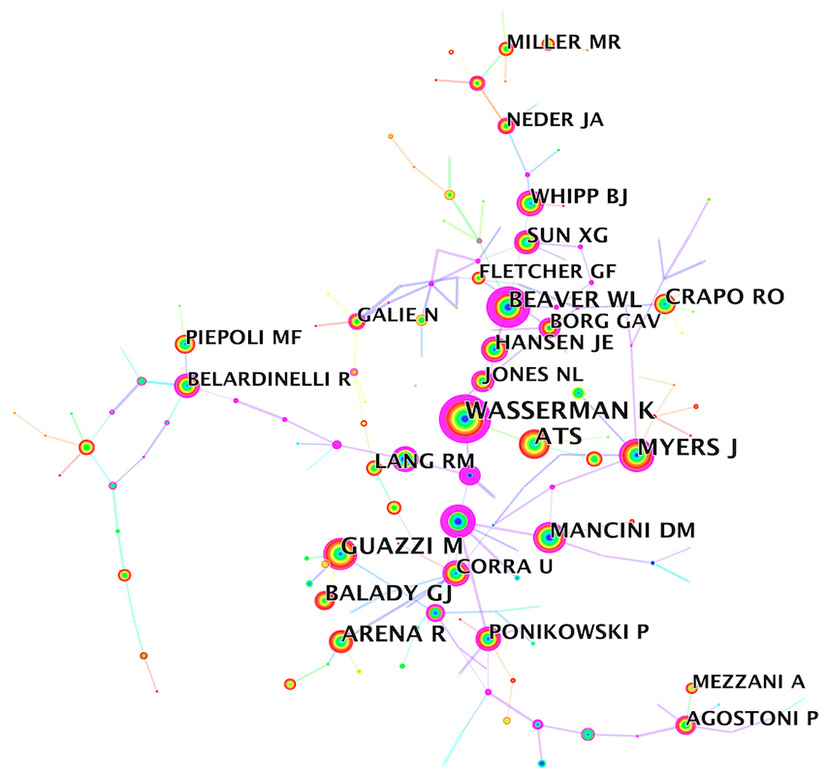
Author co-cited analysis.
Journal
It can be seen from Table 6 that 50% of the top 10 journals ranked by co-cited frequency were professional journals in the cardiovascular field, and the rest of the journals categories included general internal medicine, physiology, sport sciences, and critical care medicine. Half of the journals had an impact factor of ≥10, and 90% are JCR Q1 or Q2.
Table 6
| Rank | Journal | Co-cited frequency | BC | Impact factor (2020) | Category | Quartile in category (JCR) |
|---|---|---|---|---|---|---|
| 1 | Circulation | 3,191 | 1.15 | 29.690 | Cardiac and Cardiovascular Systems | Q1 |
| 2 | Journal of the American College of Cardiology | 2,617 | 0.81 | 24.093 | Cardiac and Cardiovascular Systems | Q1 |
| 3 | Chest | 2,057 | 0.71 | 9.410 | Critical Care Medicine | Q1 |
| 4 | European Heart Journal | 2,035 | 0.36 | 29.983 | Cardiac and Cardiovascular Systems | Q1 |
| 5 | American Journal of Cardiology | 1,920 | 0.32 | 2.778 | Cardiac and Cardiovascular Systems | Q3 |
| 6 | Journal of Applied Physiology | 1,871 | 0.31 | 3.532 | Physiology | Q2 |
| 7 | American Journal of Respiratory and Critical Care Medicine | 1,801 | 0.46 | 21.405 | Critical Care Medicine | Q1 |
| 8 | The New England Journal of Medicine | 1664 | 0.11 | 91.253 | Medicine, General and Internal | Q1 |
| 9 | Medicine and Science in Sports and Exercise | 1,622 | 0.18 | 5.411 | Sport Sciences | Q1 |
| 10 | American Heart Journal | 1,521 | 0.18 | 4.749 | Cardiac and Cardiovascular Systems | Q2 |
Top 10 journals ranked by co-cited frequency on CPET publications.
BC, betweenness centrality.
In addition, the BC value of 10 journals were all ≥0.1 (Supplementary Figure 2). All these findings indicated that the clinical application of CPET was a prominent research topic, and the CPET-related papers published in these high-level journals also provided sufficient theoretical and data for the clinical application of CPET.
References
As was shown in Table 7, the top 10 most co-cited documents were clinical guidelines, scientific statements, or reviews. These documents were published after 2010, indicating that CPET had been gradually included in clinical guidelines and recommended for use in related diseases since 2010. It also reflected that researchers had gradually recognized the value of CPET in clinical auxiliary diagnosis and risk assessment. At the same time, relevant societies had formulated standard operating procedures for CPET in adults and introduced standardized guidance documents for the interpretation of CPET indications in specific populations, to further promote CPET's clinical application.
Table 7
| Rank | Title | Reference type | Co-cited frequency | Year | BC | Impact factor (2020) | Quartile in category (JCR) |
|---|---|---|---|---|---|---|---|
| 1 | 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC (23) | Practice Guideline | 143 | 2016 | 0.08 | 29.983 | Q1 |
| 2 | Clinician's Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association (24) | Review | 124 | 2010 | 0.23 | 29.690 | Q1 |
| 3 | 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations (25) | Scientific Statements | 113 | 2016 | 0.01 | 29.983 | Q1 |
| 4 | Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association (14) | Review | 102 | 2016 | 0.10 | 29.690 | Q1 |
| 5 | 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Pediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) (26) | Practice Guideline | 96 | 2016 | 0.03 | 29.983 | Q1 |
| 6 | Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging (27) | Review | 74 | 2015 | 0.00 | 5.251 | Q2 |
| 7 | EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations (28) | Practice Guideline | 69 | 2012 | 0.03 | 29.690 | Q1 |
| 8 | Cardiopulmonary Exercise Testing: What Is its Value (29) | Review | 69 | 2017 | 0.00 | 24.093 | Q1 |
| 9 | Cardiopulmonary Exercise Testing in Heart Failure (30) | Review | 64 | 2016 | 0.19 | 12.035 | Q1 |
| 10 | ATS/ACCP Statement on cardiopulmonary exercise testing (31) | Review | 61 | 2003 | 0.02 | 21.405 | Q1 |
Top 10 references ranked by co-cited frequency on CPET.
BC, betweenness centrality.
Discussion
The number of articles published each year represents the level of activity in the development of a particular research field. The significant surge in the number of publications on the topic of CPET since 2017 indicated growing interest in the field. Clinicians gradually realized that CPET can provide important clinical auxiliary diagnostic information (29), so they were becoming more willing to perform CPET as part of a routine clinical examination. In addition, it may also because that CPET is gradually moving worldwide, and all regions of the world are vigorously promoting CPET-related research.
The country collaboration network showed that countries with strong comprehensive economic strength in North America and Europe dominated the CPET research field, followed by China, Japan, and Australia, but African countries had fewer publications, revealing the current uneven global development trends in the CPET field. This may be related to the higher national health awareness in developed countries such as American, England, and Italy. It is worth noting that the CPET instruments commonly used in clinical practice are also mainly manufactured by European and North American countries.
Almost all top 10 research institutions in terms of collaborative publications were the top 10 universities or their affiliated medical institutions in Europe countries and the United States, which indicated that top research and medical talents from these countries were driving the development in the CPET field. However, there were no institutions from Asia, Australia, or Africa among the top 10 institutions, indicating that the institutional partnership between Europe and the United States and other regional countries was not strong, which may be due to language factors or different health awareness among people in different countries. Tongji University from China ranked 30th, with a frequency of 31. In recent years, its number of publications had increased rapidly, showing a great development trend, which is expected to become a bridge for cross-regional cooperation with institutions of European and American countries.
Author collaboration network analysis suggested a non-tight collaboration among the core authors. Jonathan Myers, Marco Guazzi, and Ross Arena were the core researchers in the CPET field because of their high number and citations of published papers. However, it should also be noted that although Wasserman K did not have a huge number of publications, they ranked first in number of citations. He was an American physiologist, the founder of the Wasserman 9-Panel Plot (32) (the current standard layout for the presentation of CPET gas metabolism data), and one of the first people to propose the use of exercise tests to detect the coordination of cardiorespiratory metabolism (33, 34). He was also the first person to propose the determination of anaerobic thresholds to measure health risk by detecting changes in the composition of exhaled gas during exercise (35, 36).
Subject co-occurrence analysis showed that cardiovascular, respiratory, and other traditional medical system diseases were the main applied subjects of CPET. Sport sciences and physiology were interdisciplinary subjects involved in CPET, because the operation of CPET (treadmill or ergometry bicycle) and the interpretation of the results require the participation of sports scientists and cardiopulmonary physiologists. They can evaluate patients' exercise ability according to CPET results and formulate corresponding exercise programs to guide patients' rehabilitation outside the hospital (37–39).
Keywords co-occurrence and cluster analysis revealed the research status and hotspots of CPET. Heart failure was a major application area of CPET (40–42). CPET was always used to determine the maximum heart rate during exercise to guide the patient's daily physical activity and to assess the impact of drugs or interventions on the patient's exercise capacity (43, 44). Indicators from CPET had an independent predictive effect on prognosis in patients with heart failure, whether used alone or in combination with other non-CPET indicators. However, the establishment of CPET-related prognostic indicators had undergone many years of development and optimization. The early proposed VO2 peak had been widely recognized for its predictive role in prognosis and was the gold standard for evaluating functional ability (45–47). Subsequently, to exclude the effects of obesity and β-blockers on VO2, the VE/VCO2 slope was also proved to have a good predictive effect (48–50). Furthermore, to exclude the influence of subjective motility of patients, related studies had proposed using log OUES (oxygen uptake efficiency slope) as the predictor of mortality (51–54), and some studies had proposed that excessive ventilation assessed over the first 3 min should be taken for prognostic stratification to patients unable to perform maximal CPET (55). What's more, peak circulatory power, the combined application of AT and VE/VCO2 slope, VO2 peak and VE/VCO2 had proven to be strong predictors of heart failure mortality risk (56, 57). The combination application of %VO2 and BNP can further optimize the risk stratification in patients with chronic heart failure (58, 59). In addition to heart failure, the routine application of CPET in clinical practice had expanded to other patient populations, including those with coronary artery disease (60), congenital heart disease (61), and pulmonary hypertension (62, 63).
Co-citation analysis of references showed three publications with BC>0.1, revealing three important turning points in CPET development. The first turning point occurred in 2010 (24) when the American Heart Association issued a scientific statement indicating that CPET can provide more clinical information than other standard exercise tests, especially in diagnosingcardiopulmonary system diseases. More importantly, the document clearly specified the calibration of instruments and analysis systems, the selection principles of different CPET protocols, quality control and supervision during the test and results interpretation in clinical practice. Thus, it provided direct and detailed guidance to clinicians, pioneered a standardized test protocol for CPET, and laid a good foundation for its wider application in different patient populations. The remaining two turning points both occurred in 2016. The first reviewed the predictive role of CPET indicators on heart failure prognosis, how to use CPET indicators for the risk stratification management of heart failure, and summarized the available studies related to CPET in heart failure (30). The second was a scientific statement from the American Heart Association that analyzed a series of research findings showing the association between CRF and health outcomes and recommends CRF as a predictor of health status (14). It also highlighted the importance of CRF in predicting cardiovascular mortality and its role in pre-surgical risk assessment and risk stratification for heart failure and stroke, and it is now widely used in the construction of disease risk prediction models. In addition to cardiovascular diseases, CPET also played an important role in metabolic diseases such as diabetes and cancer. In conclusion, these three key references can be seen as landmark events in CPET field, which had a profound impact on promoting the application of CPET in cardiovascular and other diseases.
It is worth noting that the top 10 references in the co-citation analysis were all clinical guidelines or reviews, indicating that highly co-cited original articles about CPET were still relatively lacking. High-quality clinical research using CPET as the main efficacy evaluation index in cardiovascular system disease is expected to become a promising direction for future development. In addition, how to further popularize the theoretical basis of CPET among clinicians and clarify its clinical benefits should also be studied.
Limitation
Although this is the first bibliometric analysis on a CPET topic, there are some potential limitations in this study. Like other bibliometric analyses, the search results obtained in this study were limited by the selected database. To meet the format requirements of CiteSpace software for analysis, only the WoSCC database was used in this study, so some literature related to this topic may not be included. The timespan of publication for the included literature is: 2002 to 2021, which will also result in earlier papers not being included in the analysis, we limit the language to English, which may lead to these literatures published in other languages being ignored. With the publication of relevant scientific research results, the results of bibliometric analysis in this topic may change in the future, but a summary analysis of 20 years of related results in this field is also helpful for later researchers to understand the development overview of this field in a specific period.
Conclusion
To the best of our knowledge, this is the first bibliometric study to summarize the results of the last 20 years of research on CPET in the WoSCC database, using the CiteSpace software. The results of this study can help new researchers to understand the major research institutions, famous researchers, classic articles, and development trends in this field. The CPET field is in a period of vigorous development, and relevant research results are emerging. The annual number of publications is expected to further increase. Ross Arena had published the most literature in this field, and Wasserman K was the author with the highest co-citation frequency, indicating that his research results had greatly contributed to the development of this field. The literature published in top international journals in the cardiovascular field had made an important contribution to advancing the development of CPET field, indicating that CPET had attracted widespread attention from the academic community. At present, the main clinical application of CPET is cardiovascular diseases, mainly heart failure, and its main roles include objective and quantitative assessment of patients' CRF and guidance of patients' functional exercise. High-quality clinical studies with large samples using cardiopulmonary exercise testing as the main efficacy evaluation index are promising directions for future research.
Funding
This study was supported by National Key Research and Development Program of China (No. 2019YFC0840608), Major research project of scientific and technological innovation project of Chinese Academy of Chinese Medicine Sciences (No. CI2021A00913), and Innovation Team and Talents Cultivation Program of National Administration of Traditional Chinese Medicine (No. ZYYCXTD-C-202007).
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
DS and MX conceived the study and reviewed and revised the manuscript. LS collected the data and wrote the manuscript. HQ and JL re-examined the data. LS, WW, and LZ analyzed the data. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to give thanks to Prof. Chaomei Chen for developing the CiteSpace software and making it freely available to the public, and to all the reviewers for their valuable suggestions that allowed us to further improve our manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.982351/full#supplementary-material
Supplementary Figure 1Subject categories co-occurrence analysis network.
Supplementary Figure 2Journal co-cited analysis.
References
1.
Weisman IM Zeballos RJ . Clinical exercise testing. Clin Chest Med. (2001) 22:679–701. 10.1016/S0272-5231(05)70060-5
2.
DeCato TW Haverkamp H Hegewald MJ . Cardiopulmonary exercise testing (CPET). Am J Respir Crit Care Med. (2020) 201:P1–P2. 10.1164/rccm.2011P1
3.
Ross RM . ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. (2003) 167:1451. 10.1164/ajrccm.167.10.950
4.
Raghuveer G Hartz J Lubans DR Takken T Wiltz JL Mietus-Snyder M et al . Cardiorespiratory fitness in youth: an important marker of health: a scientific statement from the American Heart Association. Circulation. (2020) 142:e101–18. 10.1161/CIR.0000000000000866
5.
Ezzatvar Y Izquierdo M Núñez J Calatayud J Ramírez-Vélez R García-Hermoso A . Cardiorespiratory fitness measured with cardiopulmonary exercise testing and mortality in patients with cardiovascular disease: a systematic review and meta-analysis. J Sport Health Sci. (2021) 10:609–19. 10.1016/j.jshs.2021.06.004
6.
Chmelo J Khaw RA Sinclair RCF Navidi M Phillips AW . Does cardiopulmonary testing help predict long-term survival after esophagectomy?Ann Surg Oncol. (2021) 28:7291–7. 10.1245/s10434-021-10136-5
7.
Mandsager K Harb S Cremer P Phelan D Nissen SE Jaber W . Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. (2018) 1:e183605. 10.1001/jamanetworkopen.2018.3605
8.
Myers J de Souza E . Silva CG, Arena R, Kaminsky L, Christle JW, Busque V, et al. Comparison of the FRIEND and Wasserman-Hansen equations in predicting outcomes in heart failure. J Am Heart Assoc. (2021) 10:e021246. 10.1161/JAHA.121.021246
9.
Belardinelli R Lacalaprice F Carle F Minnucci A Cianci G Perna G et al . Exercise-induced myocardial ischaemia detected by cardiopulmonary exercise testing. Eur Heart J. (2003) 24:1304–13. 10.1016/S0195-668X(03)00210-0
10.
Letnes JM Dalen H Vesterbekkmo EK Wisløff U Nes BM . Peak oxygen uptake and incident coronary heart disease in a healthy population: the HUNT Fitness Study. Eur Heart J. (2019) 40:1633–9. 10.1093/eurheartj/ehy708
11.
Inuzuka R Diller G-P Borgia F Benson L Tay ELW Alonso-Gonzalez R ., et al. Comprehensive use of cardiopulmonary exercise testing identifies adults with congenital heart disease at increased mortality risk in the medium term. Circulation. (2012) 125:250–9. 10.1161/CIRCULATIONAHA.111.058719
12.
Snowden CP Prentis JM Anderson HL Roberts DR Randles D Renton M et al . Submaximal cardiopulmonary exercise testing predicts complications and hospital length of stay in patients undergoing major elective surgery. Ann Surg. (2010) 251:535–41. 10.1097/SLA.0b013e3181cf811d
13.
Richter Larsen K Svendsen UG Milman N Brenøe J Petersen BN . Exercise testing in the preoperative evaluation of patients with bronchogenic carcinoma. Eur Respir J. (1997) 10:1559–65. 10.1183/09031936.97.10071559
14.
Ross R Blair SN Arena R Church TS Després J-P Franklin BA et al . Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation. (2016) 134:e653–99. 10.1161/CIR.0000000000000461
15.
Ninkov A Frank JR Maggio LA . Bibliometrics: methods for studying academic publishing. Perspect Med Edu. (2021) 11:173–610.1007/s40037-021-00695-4
16.
Devos P Ménard J . Trends in worldwide research in hypertension over the period 1999-2018: a bibliometric study. Hypertension. (2020) 76:1649–55. 10.1161/HYPERTENSIONAHA.120.15711
17.
Xavier-Santos D Padilha M Fabiano GA Vinderola G Gomes Cruz A Sivieri K et al . Evidences and perspectives of the use of probiotics, prebiotics, synbiotics, and postbiotics as adjuvants for prevention and treatment of COVID-19: A bibliometric analysis and systematic review. Trends Food Sci Technol. (2022) 120:174–92. 10.1016/j.tifs.2021.12.033
18.
Maymone MBC Laughter M Vashi NA Jones JD Hugh J Dunnick CA et al . The most cited articles and authors in dermatology: a bibliometric analysis of 1974-2019. J Am Acad Dermatol. (2020) 83:201–5. 10.1016/j.jaad.2019.06.1308
19.
Stout NL Alfano CM Belter CW Nitkin R Cernich A Lohmann Siegel K et al . Bibliometric analysis of the landscape of cancer rehabilitation research (1992-2016). J Natl Cancer Inst. (2018) 110:815–24. 10.1093/jnci/djy108
20.
Deng Z Chen J Wang T . Bibliometric and visualization analysis of human coronaviruses: prospects and implications for COVID-19 research. Front Cell Infect Microbiol. (2020) 10:581404. 10.3389/fcimb.2020.581404
21.
Falagas ME Pitsouni EI Malietzis GA Pappas G . Comparison of PubMed, Scopus, Web of Science, and Google Scholar: strengths and weaknesses. FASEB J. (2008) 22:338–42. 10.1096/fj.07-9492LSF
22.
Chen C . CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci. (2006) 57:359–77. 10.1002/asi.20317
23.
Ponikowski P Voors AA Anker SD Bueno H Cleland JGF Coats AJS et al . 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. 10.1093/eurheartj/ehw128
24.
Balady GJ Arena R Sietsema K Myers J Coke L Fletcher GF et al . Clinician's guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation. (2010) 122:191–225. 10.1161/CIR.0b013e3181e52e69
25.
Guazzi M Arena R Halle M Piepoli MF Myers J Lavie CJ . 2016 focused update: clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur Heart J. (2018) 39:1144–61. 10.1093/eurheartj/ehw180
26.
Galiè N Humbert M Vachiery J-L Gibbs S Lang I Torbicki A et al . 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. (2016) 37:67–119. 10.1093/eurheartj/ehv317
27.
Lang RM Badano LP Mor-Avi V Afilalo J Armstrong A Ernande L et al . Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. (2015) 28:1–39.e14.10.1016/j.echo.2014.10.003
28.
Guazzi M Adams V Conraads V Halle M Mezzani A Vanhees L et al . EACPR/AHA scientific statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation. (2012) 126:2261–74. 10.1161/CIR.0b013e31826fb946
29.
Guazzi M Bandera F Ozemek C Systrom D Arena R . Cardiopulmonary exercise testing: what is its value?J Am Coll Cardiol. (2017) 70:1618–36. 10.1016/j.jacc.2017.08.012
30.
Malhotra R Bakken K D'Elia E Lewis GD . Cardiopulmonary exercise testing in heart failure. JACC Heart Fail. (2016) 4:607–16. 10.1016/j.jchf.2016.03.022
31.
American Thoracic Society American American College of Chest Physicians . ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. (2003) 167:211–77. 10.1164/rccm.167.2.211
32.
Glaab T Taube C . Practical guide to cardiopulmonary exercise testing in adults. Respir Res. (2022) 23:9. 10.1186/s12931-021-01895-6
33.
Wasserman K . Breathing during exercise. N Engl J Med. (1978) 298:780–5. 10.1056/NEJM197804062981408
34.
Wasserman K . The Dickinson W. Richards lecture. New concepts in assessing cardiovascular function. Circulation. (1988) 78:1060–71. 10.1161/01.CIR.78.4.1060
35.
Wasserman K Beaver WL Whipp BJ . Gas exchange theory and the lactic acidosis (anaerobic) threshold. Circulation. (1990) 81:II14–30.
36.
Wasserman K . Determinants and detection of anaerobic threshold and consequences of exercise above it. Circulation. (1987) 76:VI29–39.
37.
Marzolini S Oh P McIlroy W Brooks D . The feasibility of cardiopulmonary exercise testing for prescribing exercise to people after stroke. Stroke. (2012) 43:1075–81. 10.1161/STROKEAHA.111.635128
38.
Pymer S Nichols S Prosser J Birkett S Carroll S Ingle L . Does exercise prescription based on estimated heart rate training zones exceed the ventilatory anaerobic threshold in patients with coronary heart disease undergoing usual-care cardiovascular rehabilitation? A United Kingdom perspective. Eur J Prev Cardiol. (2020) 27:579–89. 10.1177/2047487319852711
39.
Zhu L-Y Li M-Y Li K-H Yang X Yang Y-Y Zhao X-X et al . Effect of exercise prescription implementation rate on cardiovascular events. Front Cardiovasc Med. (2021) 8:753672. 10.3389/fcvm.2021.753672
40.
Edelmann F Wachter R Schmidt AG Kraigher-Krainer E Colantonio C Kamke W et al . Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: the Aldo-DHF randomized controlled trial. JAMA. (2013) 309:781–91. 10.1001/jama.2013.905
41.
Janicki JS Weber KT McElroy PA . Use of the cardiopulmonary exercise test to evaluate the patient with chronic heart failure. Eur Heart J. (1988) 9 (Suppl H):55–8. 10.1093/eurheartj/9.suppl_H.55
42.
de Vries RJ van Veldhuisen DJ Dunselman PH van der Veer N Crijns HJ . Physiological parameters during the initial stages of cardiopulmonary exercise testing in patients with chronic heart failure. Their value in the assessment of clinical severity and prognosis. Eur Heart J. (1997) 18:1921–30. 10.1093/oxfordjournals.eurheartj.a015201
43.
Kindermann M Schwaab B Finkler N Schaller S Böhm M Fröhlig G . Defining the optimum upper heart rate limit during exercise: a study in pacemaker patients with heart failure. Eur Heart J. (2002) 23:1301–8. 10.1053/euhj.2001.3078
44.
Hirsh DS Vittorio TJ Barbarash SL Hudaihed A Tseng C-H Arwady A et al . Association of heart rate recovery and maximum oxygen consumption in patients with chronic congestive heart failure. J Heart Lung Transplant. (2006) 25:942–5. 10.1016/j.healun.2006.04.006
45.
Anker SD Coats AJ . Peak VO2 for prognosis in heart failure?J Am Coll Cardiol. (1999) 33:591–2.
46.
Swank AM Horton J Fleg JL Fonarow GC Keteyian S Goldberg L et al . Modest increase in peak VO2 is related to better clinical outcomes in chronic heart failure patients: results from heart failure and a controlled trial to investigate outcomes of exercise training. Circ Heart Fail. (2012) 5:579–85. 10.1161/CIRCHEARTFAILURE.111.965186
47.
Chiaranda G Myers J Arena R Kaminsky L Sassone B Pasanisi G et al . Prognostic comparison of the FRIEND and Wasserman/Hansen peak VO2 equations applied to a submaximal walking test in outpatients with cardiovascular disease. Eur J Prev Cardiol. (2021) 28:287–92. 10.1177/2047487319871728
48.
Chua TP Ponikowski P Harrington D Anker SD Webb-Peploe K Clark AL et al . Clinical correlates and prognostic significance of the ventilatory response to exercise in chronic heart failure. J Am Coll Cardiol. (1997) 29:1585–90. 10.1016/S0735-1097(97)00078-8
49.
Jaussaud J Douard H . Usefulness of the lowest VE/VCO2 ratio measured during exercise in heart failure. Eur J Heart Fail. (2011) 13:809. 10.1093/eurjhf/hfr065
50.
Guazzi M Myers J Arena R . Cardiopulmonary exercise testing in the clinical and prognostic assessment of diastolic heart failure. J Am Coll Cardiol. (2005) 46:1883–90. 10.1016/j.jacc.2005.07.051
51.
Davies LC Wensel R Georgiadou P Cicoira M Coats AJS Piepoli MF et al . Enhanced prognostic value from cardiopulmonary exercise testing in chronic heart failure by non-linear analysis: oxygen uptake efficiency slope. Eur Heart J. (2006) 27:684–90. 10.1093/eurheartj/ehi672
52.
Hollenberg M Tager IB . Oxygen uptake efficiency slope: an index of exercise performance and cardiopulmonary reserve requiring only submaximal exercise. J Am Coll Cardiol. (2000) 36:194–201. 10.1016/S0735-1097(00)00691-4
53.
Baba R Nagashima M Goto M Nagano Y Yokota M Tauchi N et al . Oxygen uptake efficiency slope: a new index of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. J Am Coll Cardiol. (1996) 28:1567–72. 10.1016/S0735-1097(96)00412-3
54.
Sun X-G Hansen JE Stringer WW . Oxygen uptake efficiency plateau best predicts early death in heart failure. Chest. (2012) 141:1284–94. 10.1378/chest.11-1270
55.
Jankowska EA Witkowski T Ponikowska B Reczuch K Borodulin-Nadzieja L Anker SD et al . Excessive ventilation during early phase of exercise: a new predictor of poor long-term outcome in patients with chronic heart failure. Eur J Heart Fail. (2007) 9:1024–31. 10.1016/j.ejheart.2007.07.001
56.
Cohen-Solal A Tabet JY Logeart D Bourgoin P Tokmakova M Dahan M et al . non-invasively determined surrogate of cardiac power ('circulatory power') at peak exercise is a powerful prognostic factor in chronic heart failure. Eur Heart J. (2002) 23:806–14. 10.1053/euhj.2001.2966
57.
Giardini A Specchia S Berton E Sangiorgi D Coutsoumbas G Gargiulo G et al . Strong and independent prognostic value of peak circulatory power in adults with congenital heart disease. Am Heart J. (2007) 154:441–7. 10.1016/j.ahj.2007.05.009
58.
Kato TS Collado E Khawaja T Kawano Y Kim M Farr M et al . Value of peak exercise oxygen consumption combined with B-type natriuretic peptide levels for optimal timing of cardiac transplantation. Circ Heart Fail. (2013) 6:6–14. 10.1161/CIRCHEARTFAILURE.112.968123
59.
de Groote P Dagorn J Soudan B Lamblin N McFadden E Bauters C . B-type natriuretic peptide and peak exercise oxygen consumption provide independent information for risk stratification in patients with stable congestive heart failure. J Am Coll Cardiol. (2004) 43:1584–9. 10.1016/j.jacc.2003.11.059
60.
Chaudhry S Arena RA Hansen JE Lewis GD Myers JN Sperling LS et al . The utility of cardiopulmonary exercise testing to detect and track early-stage ischemic heart disease. Mayo Clin Proc. (2010) 85:928–32. 10.4065/mcp.2010.0183
61.
Wadey CA Weston ME Dorobantu DM Pieles GE Stuart G Barker AR et al . The role of cardiopulmonary exercise testing in predicting mortality and morbidity in people with congenital heart disease: a systematic review and meta-analysis. Eur J Prev Cardiol. (2022) 29:513–33. 10.1093/eurjpc/zwab125
62.
Ruigrok D Meijboom LJ Nossent EJ Boonstra A Braams NJ van Wezenbeek J et al . Persistent exercise intolerance after pulmonary endarterectomy for chronic thromboembolic pulmonary hypertension. Eur Respir J. (2020) 55:2000109. 10.1183/13993003.00109-2020
63.
Godinas L Sattler C Lau EM Jaïs X Taniguchi Y Jevnikar M et al . Dead-space ventilation is linked to exercise capacity and survival in distal chronic thromboembolic pulmonary hypertension. J Heart Lung Transplant. (2017) 36:1234–42. 10.1016/j.healun.2017.05.024
Summary
Keywords
cardiopulmonary exercise test, bibliometric analysis, citation analysis, cardiopulmonary fitness, cardiovascular disease
Citation
Song L, Qu H, Luo J, Wang W, Zheng L, Xue M and Shi D (2022) Cardiopulmonary exercise test: A 20-year (2002-2021) bibliometric analysis. Front. Cardiovasc. Med. 9:982351. doi: 10.3389/fcvm.2022.982351
Received
30 June 2022
Accepted
28 July 2022
Published
15 August 2022
Volume
9 - 2022
Edited by
Jan Reinhardt, Sichuan University, China
Reviewed by
Andy Wai Kan Yeung, University of Hong Kong, China; Herbert Loellgen, Johannes Gutenberg University Mainz, Germany; Malcolm Koo, Tzu Chi University of Science and Technology, Taiwan
Updates
Copyright
© 2022 Song, Qu, Luo, Wang, Zheng, Xue and Shi.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mei Xue meiar@126.comDazhuo Shi shidztcm@163.com
This article was submitted to General Cardiovascular Medicine, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.