 Yingtian Yang1,†
Yingtian Yang1,† Qianyu Lv1,†
Qianyu Lv1,† Xinzheng Hou1
Xinzheng Hou1 Yanfei Lv2Xirui Zhang3
Yanfei Lv2Xirui Zhang3 Qian Wu1
Qian Wu1 Xuejiao Ye1
Xuejiao Ye1 Chenyan Yang1Mingyu Huang1
Chenyan Yang1Mingyu Huang1 Shihan Wang1*
Shihan Wang1*
- 1Department of Cardiovascular Internal Medicine, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China
- 2School of Management, Fudan University, Shanghai, China
- 3Department of Geriatrics, Baogang Hospital of Inner Mongolia, Baotou, China
Objective: To evaluate the relative impacts of various exercise protocols on blood pressure (BP) and endothelial function in prehypertension individuals.
Methods: In this systematic review and network meta-analysis (NMA), PubMed, Cochrane Library, Web of Science, Embase, CINAHL, SPORTDiscus, and Rehabilitation & Sports Medicine databases were searched until September 12, 2024. Randomized controlled trials that examined the effectiveness of exercise treatments on people with prehypertension compared to a non-exercise control group or other exercise modes were included. A Bayesian NMA were applied to examine SBP, DBP, flow-mediated dilation (FMD), and pulse wave velocity (PWV). The surface underneath the cumulative ranking curve data was utilized to rate interventions. Confidence was evaluated using the CINeMA framework.
Results: A total of 18 articles with 2,592 individuals were included in the NMA. Tai Chi demonstrated the greatest decrease in SBP of −8.67 mm Hg [95% credible interval (CI): −17.29 to −0.05], while isometric exercise training (IET) exhibited the most substantial enhancement in DBP of −4.61 mm Hg (95% CI: −8.11 to −1.11) and PWV of −0.82 m/s (95% CI: −1.58 to −0.06). Moderate-intensity continuous training yielded the largest improvement in FMD at 5.82% (95% CI: 5.41–6.22).
Conclusion: Diverse exercise modalities can enhance BP and vascular function in prehypertensive patients. Overall, Tai Chi and IET are the most productive exercises for reducing BP, with IET being particularly effective in diminishing arterial stiffness. MICT stands out in enhancing endothelial function. Nevertheless, further comprehensive studies encompassing more diverse exercise treatments are necessary to ascertain the best exercise patterns and dosing strategies.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=614765, identifier: CRD42024614765.
1 Introduction
Hypertension (HTN) represents a key risk factor for cardiovascular events, causing damage to multiple organs (1). Currently, the primary management of HTN remains long-term pharmacological treatment, which is associated with poor adherence, high long-term economic burden, and potential drug-related adverse effects (2). Therefore, advancing the frontline of HTN prevention and control is particularly crucial for disease prevention and prognosis improvement (3). The 7th Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) in 2003 first proposed the concept of prehypertension (PHT), characterized by systolic blood pressure (SBP) of 120–139 mm Hg and/or diastolic blood pressure (DBP) of 80–89 mm Hg (4). The 2018 China Hypertension Survey reported (5) that approximately 41.3% of adults were in a PHT state, with an estimated national PHT population of 435 million. As a transitional phase between normative blood pressure (BP) and clinical HTN, PHT is more likely to progress to HTN and cardiovascular diseases than those with normal BP (6, 7).
Endothelial dysfunction and vascular remodeling are critical characteristics of HTN and preliminary indications of atherosclerosis (8). Retrospective research of 1375 HTN individuals indicated that flow-mediated dilation (FMD) and pulse wave velocity (PWV) are independent risk factors for predicting the occurrence of coronary heart disease in hypertensive populations (9). FMD, a non-intrusive measurement of endothelial function, is regarded as the gold standard for evaluating vascular endothelial function in clinical research. FMD is an independent predictor of cardiovascular outcomes and can be utilized to identify subjects at increased risk for future cardiovascular events (10). Simultaneously, diminished FMD is significantly linked to the onset of HTN (11). PWV is an essential parameter to evaluate arterial stiffness. PWV levels over 10 m/s can forecast detrimental hemodynamic alterations, independently increasing cardiovascular risk (12, 13). Additionally, PWV may serve as a reliable marker for detecting target organ damage in patients with PHT (14). Consequently, efficient monitoring of vascular function in PHT patients offers a thorough insight into vascular health and the related risks of HTN. This is crucial for identifying high-risk individuals early, evaluating therapeutic outcomes, and formulating personalized treatment strategies.
Increasing evidence suggests that exercise interventions can effectively lower blood pressure in HTN and PHT patients (15, 16). Relevant guidelines also prioritize exercise as a management and treatment strategy for PHT people. This is because exercise not only offers potential cost-effectiveness compared to antihypertensive medications but also modifies the lifestyle of PHT patients, providing lifelong benefits (17, 18). A previous network meta-analysis on effective antihypertensive strategies for PHT patients confirmed that exercise is the most effective intervention (19). Moreover, recent research has demonstrated that exercise can significantly improve endothelial function in HTN and PHT patients, including enhancing FMD and reducing PWV (20, 21). Despite these benefits, there remains a lack of comprehensive evaluations assessing the impact of various exercise modalities on PHT individuals, particularly for improving vascular function indicators like FMD and PWV.
Network meta-analysis (NMA) expands upon pairwise meta-analysis (22), utilizing direct and indirect evidence to improve effect estimation and treatment ranking, even when specific interventions have never been compared in randomized controlled trials (RCTs) (23). This study aims to assess the effectiveness of various exercise protocols on BP and endothelial function in adults with PHT based on a comprehensive systematic review and network meta-analysis. Evidence-based guidance will help refine treatment strategies for PHT and optimize clinical management.
2 Methods
2.1 Study design and registration
Our review was conducted in alignment with the Cochrane Collaboration Handbook (24) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (25) as well as the extension statement for network meta-analyses (PRISMA-NMA) (26) reporting guidelines (Supplementary Table S1). A priori protocol has been registered in PROSPERO (registration number: CRD42024614765).
2.2 Search strategy
A complete search was conducted from PubMed (MEDLINE), Cochrane Library, Web of Science, Embase, CINAHL, SPORTDiscus, and Rehabilitation & Sports Medicine Source databases from inception until September 12, 2024. With the assistance of a research librarian proficient in scientific databases, we executed a search strategy utilizing a combination of medical subject heading (MeSH) terms and keywords pertinent to exercise, physical activity, prehypertension, and randomized controlled trials. Manual searches of the reference lists from prior and analogous systematic reviews and meta-analyses were conducted to uncover additional papers not found in the initial search. The comprehensive search procedures are outlined in Supplementary Table S2.
2.3 Inclusion and exclusion criteria
Eligibility criteria were developed according to the PICOS framework (Population, Intervention, Comparator, Outcomes, and Study design). Inclusion criteria: Participants were adults (aged ≥18 years) exhibiting BP within the PHT range, defined as SBP between 120 and 139 mm Hg and/or DBP between 80 and 89 mm Hg (27). The intervention encompassed any mode of exercise training. Exercise interventions were classified into the following categories: aerobic exercise training [low-intensity training (LIT), moderate-intensity continuous training (MICT), and high-intensity interval training (HIIT)], isometric exercise training (IET), resistance training (RT), yoga, Tai Chi, or a combination of two or more of the above exercise forms. Supplementary Table S3 presents the detailed definitions of exercise types (3). Comparators included additional exercise modes or a non-exercise control group (usual care/health education) (4). The primary outcomes encompassed both SBP and DBP. Blood pressure can be measured using auscultatory, automatic, or 24-h ambulatory monitoring methods. FMD and PWV were utilized as outcomes for assessing endothelial function. Studies were required to incorporate measurements taken before and after the intervention (5). The study design was confined to RCTs, and the published language was restricted to English.
Exclusion criteria: (1) Non-randomized design; (2) Subjects with psychiatric disorders, cognitive impairment, pregnancy, cardiovascular diseases (e.g., heart failure, stroke, myocardial infarction), cancer, and pulmonary hypertension. People diagnosed with HTN, unless they included people with PHT whose results could be independently extracted. (3) Participants were receiving concurrent co-interventions attached to exercise (e.g., medication or dietary supplementation); (4) No detailed definition of the modalities of exercise; (5) Studies focusing exclusively on the acute assessment of BP; (6) For data derived from the same study population or duplicate published RCTs, we only included the one with the larger sample sizes and more comprehensive data; (7) The full text of the study or sufficient data [means and standard deviations (SD)] were unavailable through relevant databases and other sources, and the authors did not respond to our data requests; (8) Duplicate publications, reviews, systematic reviews, meta-analyses, conference abstracts, academic theses, letters, protocols, case reports, dissertations, and animal studies were excluded.
2.4 Eligibility assessment and data extraction
Search results were imported into NoteExpress software (version 3.7.0), where duplicates were removed. Two assessors independently examined the titles and abstracts to identify possibly relevant papers. If at least one investigator considered the paper eligible, a further full-text evaluation for final eligibility was obtained. Articles meeting the inclusion criteria after full-text screening were included in the NMA. Two investigators extracted the following data from each eligible article using a standardized form: article details (title, first author, publication year, country), characteristics of the study population (sample size, age, sex, disease status, treatment), outcome metrics (mean and SD at baseline and post-exercise or change values), specifics of exercise interventions (frequency, length, and duration), comparisons, and additional information. Origin 2024 was employed to extract the underlying numerical data from the graphical representation. Data consistency was verified through cross-checking of records following extraction. Discrepancies were addressed through discussion and, when necessary, the engagement of a third researcher.
2.5 Risk of bias assessment
Two researchers separately assessed the risk of bias for the included RCTs utilizing the updated Cochrane risk of bias assessment for randomized trials (RoB 2) (28–30). The criteria for evaluating bias across five areas: (1) randomized process, (2) allocation concealment, (3) missing outcome data, (4) assessment of outcomes, and (5) selection of the reported result. The risk of bias for each area and overall was categorized as low, some concerns, or high. Any disputes were settled through discussion or consultation with a third reviewer.
2.6 Data analysis
2.6.1 Pairwise meta-analysis
Continuous data were synthesized as Mean Difference (MD) ± SD to evaluate and derive effect sizes for the interventions. Due to the clinical heterogeneity of the included trials, randomized pairwise meta-analyses were conducted utilizing the “meta” R package.
2.6.2 Network meta-analysis
The Bayesian statistical model was developed with JAGS software version 4.3.1, incorporating the “gemtc” and “BUGSnet” packages (Rstudio, Boston, MA, USA). The results were analyzed using four Markov chains, each producing 50,000 iterations and burn-in at a step size of 20,000 pre-iterations. Network diagrams were generated by Stata SE 18.0 (StataCorp, College Station, Texas, USA). The convergence of the iterations was monitored using the Brooks-Gelman-Rubin approach, which analyzed within-chain and between-chain variation to calculate the Potential Scale Reduction Factor (PSRF). A PSRF close to 1 suggests that approximate convergence was achieved (23). We also compared and ranked the intervention types applying Surface Under the Cumulative Ranking curve (SUCRA) plots; an SUCRA value closer to 100% implies greater efficacy of the exercise (31). The I2 test was employed to evaluate statistical heterogeneity, with I2 values below 25% signifying low heterogeneity, values between 25% and 75% suggesting moderate heterogeneity, and values over 75% denoting high heterogeneity (32). We performed sensitivity analyses by eliminating articles lacking methodological rigor that exhibited a high risk of bias. In addition, the robustness of the results was evaluated by performing a meta-regression analysis with publication year, female ratio, mean age, treatment duration, and frequency as the covariates. Publication bias was assessed using comparison-adjusted funnel plots and Egger's test if ten or more trials were available for outcome comparison. Analyzes were deemed to exhibit publication bias when p < 0.05.
2.6.3 Assessment of inconsistency
Fixed-effects and random-effects models were fitted using leverage-value plots along with the corresponding Deviation Information Criterion (DIC), effective number of parameters (pD), and deviance residuals (Dres). Lower values of DIC and Dres that approximate the total number of arms in the NMA indicate a better fit. A DIC difference of ≤3 suggests no significant difference between the models (33). Given the complex structure of evidence in NMA, the presence of evidence inconsistency needed to be assessed. DIC was also used to evaluate model consistency, with a DIC difference of ≤3 between the inconsistent model and the hypothetical consistent model indicating good consistency, and a larger difference suggesting inconsistency (34). Local inconsistency across direct, indirect, and network estimates was assessed using the node-splitting method, with inconsistency identified at p < 0.05 (35).
2.7 Certainty of evidence
The certainty of evidence for each outcome in the NMA was evaluated using the Confidence in Network Meta-Analysis (CINeMA) framework, which relies on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology (36, 37). The assessment encompassed six domains: (1) within-study bias, (2) reporting bias, (3) indirectness, (4) imprecision, (5) heterogeneity, and (6) incoherence. Each domain was judged as having no, some, or major concerns. Similarly, being identical to the GRADE method, our confidence in the quality of evidence was rated as high, moderate, low, or very low for each relative intervention effect (38, 39).
2.8 Patient and public involvement
No patients were directly involved in this study's design, performance, measuring, and reporting. The findings from the NMA assessing physical activity will help inform the development of new exercise guidelines for PHT to prevent hypertension and associated illnesses.
3 Results
3.1 Literature screening process
A total of 2,716 records were initially obtained through database searches, and an additional 56 entries were identified by reviewing reference lists. After eliminating duplicate records using NoteExpress, 2,133 articles were screened based on their titles and abstracts, and 2,033 records were discarded. The remaining 100 studies were downloaded for full-text evaluation. Among these, 3 articles were not RCTs, 3 studies reported unrelated outcomes, and 4 studies were duplicate publications. Additionally, 1 paper was in a foreign language, 7 studies were conference abstracts, 1 was an academic thesis, 8 trials focused on acute blood pressure assessment, 8 studies involved ineligible interventions, 40 studies included ineligible subjects, 1 study had incomplete data, and 6 studies were study protocols. The excluded full-text articles for reasons are presented in the Supplementary Table S4. Ultimately, 18 studies involving 2,538 subjects were included in this NMA. Figure 1 displays the PRISMA flow diagram for the literature selection process.
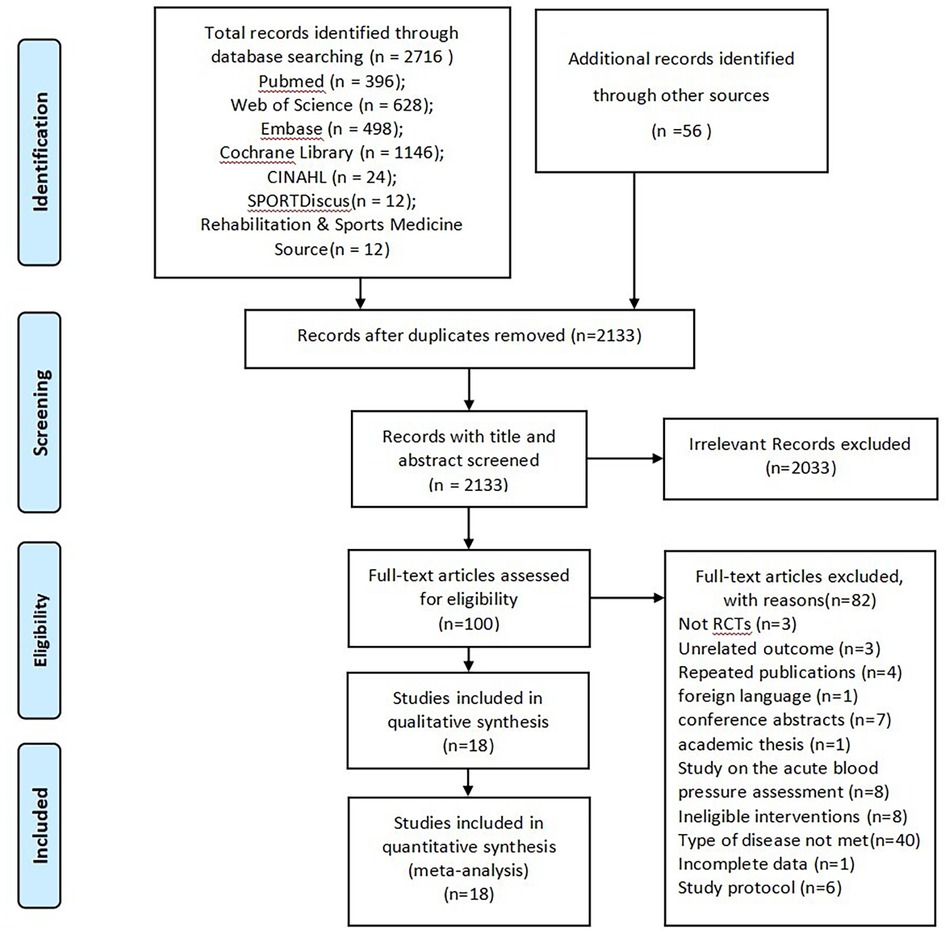
Figure 1. Flowchart of literature selection.
3.2 Study characteristics
Overall, 18 trials (21, 40–56) were eligible and included in our NMA. A total of 2,592 subjects were allocated to the control group (n = 830) and one or more of the following groups: 860 patients underwent aerobic exercise training (comprising 75 patients receiving LIT, 773 patients engaged in MICT, and 12 patients participating in HIIT), IET (n = 226), RT (n = 130), Yoga (n = 250), Tai Chi (n = 173), and a combination of aerobic exercise with RT (n = 123). The patients' ages varied from 19.0 to 67.3 years. Regarding publishing locations, 5 studies were conducted in the USA (41, 42, 45, 49, 56); 4 studies in India (44, 48, 53, 55); 2 studies in Thailand (52, 54); and 1 research each in China (46); Nigeria (51); UK (50); Kenya (47); Malaysia (43); Iran (40); and Chile (21). The exercise duration spanned from 24 days to 1 year, the frequency ranged from 3 to 7 times per week, and the duration of a single session ranged from 15 to 60 min. AT mainly consists of treadmill, cycling, walking, and swimming. Tai Chi is represented by 24-form Yang-style Tai Chi. IET consists of isometric handgrip and wall squat exercise training, with intensity measured by 30% maximum voluntary contraction or 95% heart rate peak. RT intensity ranged from 20 to 80% one-repetition maximum.The outcome of SBP was reported in 17 trials (40–56), DBP in 17, FMD in 5 (21, 40–42, 49), and PWV in 5 (21, 41, 49, 54, 56). More details of the publications included are summarized Table 1.
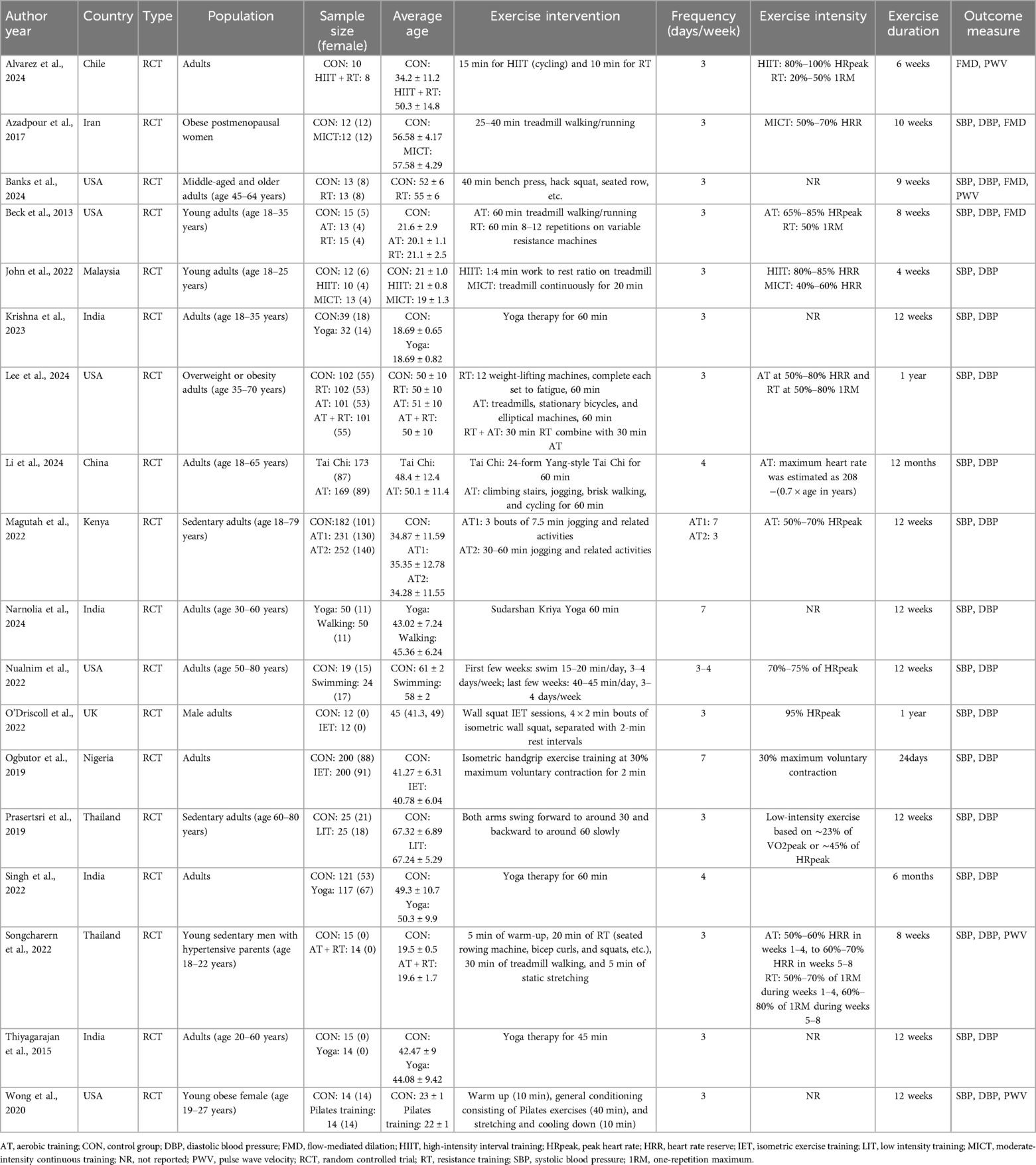
Table 1. Characteristics of included studies.
3.3 Risk of bias
Figure 2 summarizes the results of the risk of bias according to ROB2. Of 18 included RCTs, 5 trials (27.8%) were rated low risk (45–47, 51, 56), 11 trials (61.1%) were judged to have some concerns (40–44, 48–50, 52–54), and 2 (11.1%) study at high risk (21, 55). The high risk of bias is mainly attributed to the unbalanced randomization process and bias from missing outcome data. Among all the studies, 16 trials (88.9%) reported on the randomization process (21, 40–43, 45–48, 50–56) while only 6 trials (33.3%) adequately concealed the intervention allocation (45–47, 51, 55, 56). Owing to the characteristics of exercise therapies, blinding patients and researchers prove challenging, with only 4 (22.2%) reporting outcome assessor blinding (40, 45, 46, 55). Supplementary Figure S1 presents detailed information on the ROB2 evaluation for all included studies. Future high-quality RCTs are necessary for this area and should be improved, especially at the methodological level of allocation concealment, blinding, and missing data handling, to provide a more robust evidence-based basis.
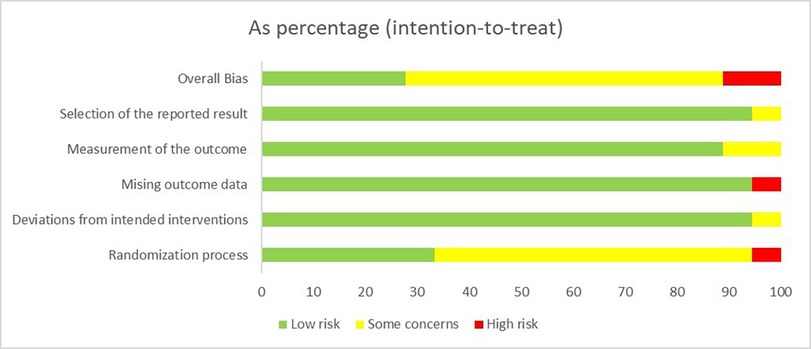
Figure 2. Summary of risk-of-bias assessment.
3.4 Network geometry
The network geometry graph displays the treatment comparisons of different exercise modalities for SBP, DBP (Figure 3A), FMD (Figure 3B), and PWV (Figure 3C). The SBP and DBP NMA (17 studies, n = 2574 patients) consisted of 9 conditions, 13 direct pairwise comparisons, and 34 indirect pairwise comparisons. The FMD NMA (5 studies, n = 154 patients) consisted of 4 conditions, 4 direct pairwise comparisons, and 5 indirect pairwise comparisons. The PWV NMA (5 studies, n = 144 patients) consisted of 5 conditions, 4 direct pairwise comparisons, and 6 indirect pairwise comparisons.
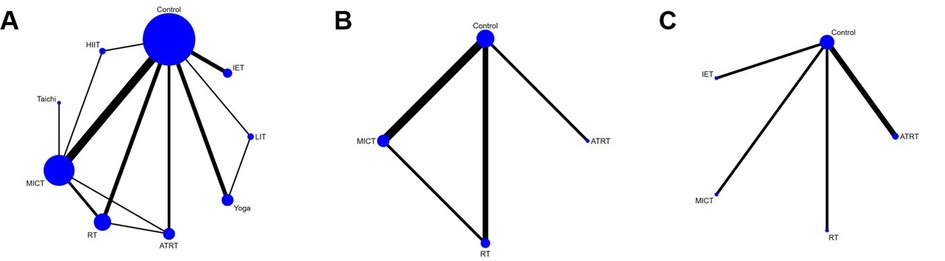
Figure 3. Network plots for (A) SBP and DBP, (B) FMD, and (C) PWV.
3.5 Systolic blood pressure
The comparative impact of any exercise prescription vs. control on SBP is illustrated in Supplementary Figure S2.1. The posterior MD for all exercise training varied from −0.38 to −8.67 mm Hg, with the most substantial network estimate attributed to Tai Chi [−8.67 mm Hg, 95% credible interval (CI) (−17.29 to −0.05, prandom = 0.04)]. Compared with control, the effect of HIIT [−6.47 mm Hg, 95% CI (−13.92–0.99), prandom = 0.09], ATRT [−5.28 mm Hg, 95% CI (−10.87–0.31), prandom = 0.06], and LIT [−0.38 mm Hg, 95% CI (−6.86–6.10), prandom = 0.91] were the comparisons that were not statistically significant.
3.6 Diastolic blood pressure
The comparative impact of any exercise prescription vs. control on DBP is shown in Supplementary Figure S2.2. The posterior MD for all exercise training varied from −0.54 to −4.61 mm Hg, with the most substantial network estimate from IET at −4.61 mm Hg (95% CI: −8.11 to −1.11, prandom = 0.01). In comparison to the control group, the effects of Tai Chi [−4.49 mm Hg, 95% CI (−10.59–1.62), prandom = 0.15], HIIT [−3.76 mm Hg, 95% CI (−9.95–2.43), prandom = 0.23], and LIT [−0.54 mm Hg, 95% CI (−5.13–4.06), prandom = 0.82] were the comparisons that were not statistically significant.
3.7 Flow-mediated dilation
The comparative impact of any exercise prescription vs. control on FMD is shown in Supplementary Figure S2.3. The posterior MD for all exercise training varied from 2.66% to 5.82%, with each exercise modality revealing a significant difference in FMD improvement. The most effective network estimates were obtained from MICT [5.82%, 95% CI (5.41–6.22), prandom < 0.01], followed by ATRT [5.60%, 95% CI (0.53–10.67), prandom = 0.03], and RT [2.66%, 95% CI (1.11–.21), prandom < 0.001].
3.8 Pulse wave velocity
The comparative impact of any exercise prescription vs. control on PWV is illustrated in Supplementary Figure S2.4. The posterior MD for all exercise training varied from −0.10 to −0.82 m/s, with the most substantial network estimates obtained from IET [−0.82 m/s, 95% CI (−1.58 to −0.06), prandom = 0.03]. Compared to the control, the effects of ATRT [−0.59 m/s, 95% CI (−1.33–0.14), prandom = 0.11], MICT [−0.25 m/s, 95% CI (−0.92–0.42), prandom = 0.46], and RT [−0.10 m/s, 95% CI (−0.88–0.68), prandom = 0.80] were statistically non-significant.
3.9 Ranking superiority and NMA estimates
We conducted a treatment rank probability analysis to ascertain the ranking of all interventions. Additionally, we produced SUCRA plots to visualize the probability percentages of ranking. Figure 4 displays the treatment rank plot and SUCRA plot for SBP, with the top three ranked exercises being Tai Chi (79%), followed by MICT (66%), and HIIT (64%). League plots (Supplementary Figure S3) were created to provide a detailed summary of the posterior MD and 95% CIs for SBP from the NMA, illustrating the significance of each exercise prescription in comparison to the control group and other interventions. Within these plots, green units indicate superior treatment efficiency compared to the comparator, whereas red units suggest inferior performance. Statistical differences at the 95% CI between interventions and their comparators are marked with (**). The primary findings for SBP showed that Tai Chi was significantly effective in reducing SBP compared to MICT [−2.40 mm Hg, 95% CI (−4.37 to −0.42)], while IET also demonstrated a significant superiority over MICT [−2.16 mm Hg, 95% CI (−2.65 to −1.69)]. Figure 5 displays the treatment rank plot and SUCRA plot for DBP, with the leading three ranked exercises being IET (71%), followed by Tai Chi (66%), and Yoga (62%). The principal findings for DBP indicated that IET was significantly more effective than Yoga [−1.44 mm Hg, 95% CI (−2.03 to −0.87)]. Comparative details regarding other exercise modalities are available in Supplementary Figure S4. For FMD, the leading three exercises ranked were MICT (84%), ATRT (77%), and RT (38%) (Supplementary Figure S5). Comparatively, MICT was significantly superior at improving FMD than RT [−3.16 mm Hg, 95% CI (−1.57 to −4.74)]. No other notable differences in FMD were observed among the various exercise therapies. The top three exercises for PWV were IET (85%), ATRT (71%), and MICT (44%) (Supplementary Figure S6). IET demonstrated significantly better efficacy in decreasing PWV compared to MICT [−0.57 mm Hg, 95% CI (−0.98 to −0.16)] and RT [−0.72 mm Hg, 95% CI (−1.29 to −0.14)]. In contrast, no significant differences in PWV were observed among the other exercise therapies.
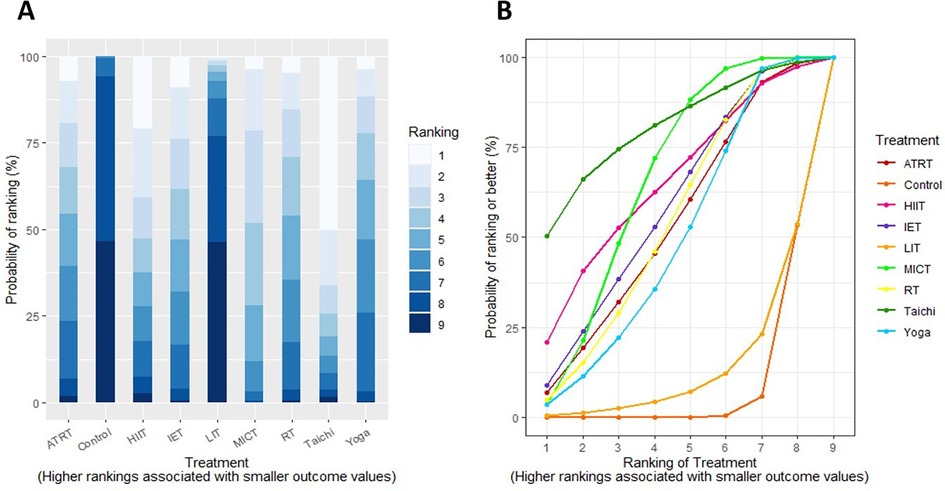
Figure 4. (A) treatment rank probabilities plot for SBP and (B) SUCRA plot for SBP.
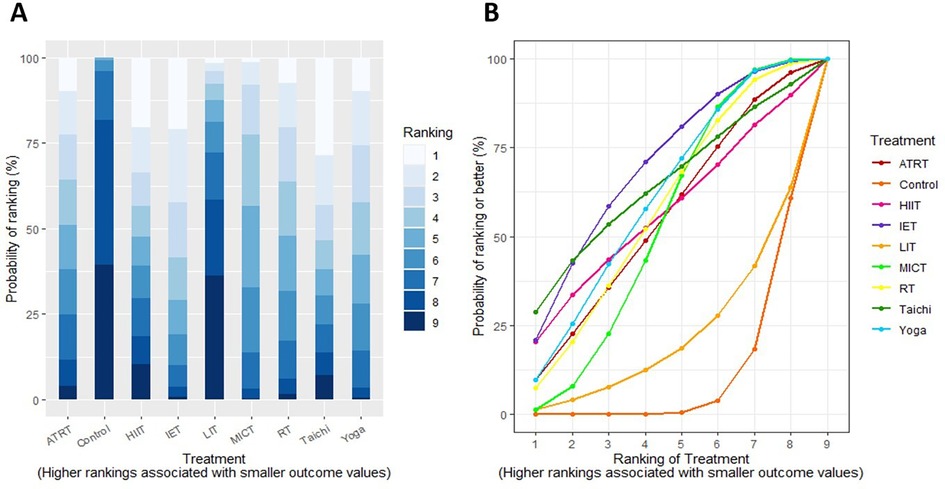
Figure 5. (A) treatment rank probabilities plot for DBP and (B) SUCRA plot for DBP. Two charts compare treatments based on ranking probability.
3.10 Model fits and network inconsistency
In terms of modeling fit, Supplementary Figure S7 provides the plots of leverage values, which show the corresponding Dres and DIC. The random effects models for SBP and DBP exhibited lower DIC, and the leverage values indicated fewer outliers, thus the random effects models were selected. No significant differences were observed across the model fit parameters for FMD and PWV. Regarding the consistency assessment, the DIC comparisons showed good agreement for SBP (DIC, 73.97 vs. 74.51), DBP (DIC, 74.12 vs. 74.87), FMD (DIC, 19.54 vs. 19.59), and PWV (DIC, 19.58 vs. 19.57). Nodal split analyses of the primary results indicated no significant differences among direct, indirect, and NMA evidence (Bayesian p > 0.05), implying no local inconsistency exists (Supplementary Figure S8). The PSRF values in all comparisons approached 1.00, suggesting that approximate convergence had been achieved.
3.11 Sensitivity analyses and meta-regressions
Sensitivity analyses were performed for the primary outcome by excluding research with a high risk of bias. The results were generally consistent following the original NMA, except that the effect of the Yoga intervention on SBP was changed to −5.96 mm Hg with 95% CI (−11.1 to −0.81) (Supplementary Figure S9). Furthermore, meta-regression analyses revealed that covariates (publication year, female ratio, mean age, treatment duration, and frequency) did not influence the results of this NMA (Supplementary Table S5).
3.12 Publication bias
Studies containing SBP and DBP outcome indicators exceeding 10 were assessed for publication bias using funnel plots (Supplementary Figure S10). The comparison-adjusted funnel plots show that all studies are predominantly distributed on either side of the zero line, indicating no significant asymmetry. Egger's test results for SBP and DBP exhibited no significant publication bias (pSBP = 0.59, pDBP = 0.79). Nevertheless, several studies remained outside the boundaries of the 95% CI, suggesting moderate to substantial heterogeneity among these studies.
3.13 Certainty of evidence
Supplementary Table S6 displays the detailed results derived from the CINeMA approach for NMA. The quality of evidence for SBP and DBP varied from moderate to very low; FMD outcomes were rated as very low, and PWV outcomes ranged from moderate to very low. For primary outcomes, the effect of Tai Chi on SBP demonstrated low certainty mainly due to imprecision, which was related to the small sample size in the included papers. The findings of IET on DBP were downgraded to moderate to very low quality primarily by heterogeneity (I2 ≥ 50%) and imprecision. The confidence of the MICT evidence on FMD was rated as very low, and all of the evidence was downgraded by within-study bias and imprecision. Evidence involving the effect of IET on PWV was rated as moderate quality.
4 Discussion
To our knowledge, this systematic review and NMA provide the most comprehensive synthesis of data on different exercise interventions in prehypertensive populations. This NMA evaluated all relevant RCTs identified through systematic searches, comprising 17 trials and 2,574 participants, to assess the efficacy and superiority of diverse exercise programs in lowering blood pressure, enhancing endothelial function, and reducing vascular stiffness. Pairwise analysis indicated that most exercise modalities significantly reduced blood pressure and FMD compared to controls, while statistical significance for PWV was observed only with IET. NMA results suggest that Tai Chi is the most efficacious exercise for reducing SBP, followed by MICT and HIIT in second and third place, respectively. For DBP, IET exhibited the most significant MD, succeeded by Tai Chi and Yoga. Regarding vascular function, IET was considered the most effective exercise for decreasing PWV, whereas MICT showed the best efficacy in improving FMD.
After excluding studies at high risk of bias, the sensitivity analysis results were generally consistent with the original NMA, demonstrating the robustness of our findings. Previous studies have found that exercise durations exceeding 12 weeks and frequency exceeding 5 times per week are associated with better blood pressure reductions (57). Younger age may lead to greater improvements in vascular function (58). A prospective study involving 412,413 U.S. adults has also revealed that women could derive greater all-cause and cardiovascular mortality risk reduction benefits from equivalent doses of physical activity compared with men (59). However, in the meta-regression of our study, no significant effect of year of publication, female ratio, mean age, intervention duration, and frequency on the outcome of the NMA has been identified, which may be related to the small number of RCTs included in this NMA, and these findings should be treated with caution. The majority of studies showed some concern regarding “within-study bias”, essentially due to flaws in the randomized concealment process and blinding by exercise interventions. “Imprecision” and “heterogeneity” were also the principal factors for downgrading in most comparisons, which partially affects the credibility of the results.
Currently, most meta-analyses examining the effects of exercise types on BP concentrate on general populations or mixed samples of hypertensive and prehypertensive individuals. A previous large-scale NMA reported that IET was the most effective approach for improving BP (60), whose results for SBP were inconsistent with our findings. This disparity may be ascribed to their inclusion of hypertensive and normotensive individuals and that our NMA incorporated more recent research. Our study focuses on the PHT population and is the first to include Tai Chi as a novel exercise modality in NMA alongside established methods like MICT, RT, and IET. Tai Chi, a traditional Chinese mind-body practice, emphasizes the combination of movement, mindfulness, and respiration (61). This holistic exercise form could further enhance its efficacy in reducing SBP by alleviating stress and improving autonomic nervous system function (62). Previous studies have confirmed that healthy lifestyle modifications (body mass index, diet, smoking, alcohol consumption, sodium excretion, and sedentary behavior) can reduce SBP by 3.5 mm Hg (63). For every 1 mm Hg decrease in SBP, the risk of cardiovascular disease declined by approximately 2%–3% (64). The mean difference in Tai Chi reduction in our NMA was up to −8.67 mm Hg, which may have clinical significance for preventing cardiovascular disease or even reducing the risk of cardiovascular events. Li et al. (46) confirmed that Tai Chi exhibits significant advantages over conventional MICT in decreasing BP load, implying a stronger capacity to reduce hypertension risk (65). Although imprecision has resulted in the effect of tai chi on SBP exhibiting low confidence of evidence, this may be attributed to the new emergence of the PHT definition in recent years and the insufficient sample size of studies conducted for this area. As far as the existing literature is concerned, the effect of tai chi on BP is unquestionable (66). A recent meta-analysis also confirmed that Tai Chi can more significantly reduce SBP in hypertensive patients compared to regular walking or aerobic exercise (67). Our investigation into the comparative effects of different exercise modalities revealed that both Tai Chi and IET surpassed MICT in lowering SBP, further supporting their potential advantages in BP reduction.
In recent years, several studies have shown that IET has a more effective antihypertensive effect than aerobic exercise (68, 69). This applies not only to hypertensive individuals but also demonstrates superior advantages in PHT individuals with lower baseline BP levels. O'Driscoll et al. (50) observed that PHT participants experienced reductions of 10.5 mm Hg in SBP and 8 mm Hg in DBP following a 1-year IET intervention. IET, characterized by sustained muscle contractions without changes in muscle length, involves highly complex mechanisms to reduce BP. Existing studies indicate that the primary mechanisms for IET's hypotensive effects are decreasing total peripheral resistance and auguring vascular compliance (70). Our NMA partially supports that perspective. Compared to the control group, IET is the only exercise modality with a significant effect on PWV, achieving the highest rank in the NMA and corroborated by moderate-quality evidence. However, more high-quality evidence is still required to support it in the future, owing to the limited number of studies.
Our findings indicate that all exercise types can effectively enhance vascular endothelial function in PHT individuals, with MICT producing the most notable benefits. A 1% rise in FMD corresponded to a 13% reduction in cardiovascular risk (71). In our NMA, MICT was associated with a mean 5.82% increase in FMD, indicating that MICT can significantly improve endothelial function in patients with PHT, potentially reducing cardiovascular events. Studies suggest that aerobic exercise improves endothelial function by elevating arterial wall shear stress via recurrent perfusion, reducing reactive oxygen species, and upregulating endothelial nitric oxide synthase (eNOS) and nitric oxide (NO) (72, 73). We obtained different ranking results in evaluating FMD outcome relative to PWV, presumably owing to inadequate trial and sample size data. Although MICT was identified as the most efficacious modality for improving FMD, the absence of IET, Tai Chi, and HIIT from this NMA prevents a comprehensive comparison of exercise options. Consequently, additional clinical studies are required and recommended to examine the antihypertensive effects of various exercise modalities mediated through vascular function, thus providing more robust scientific evidence and practical guidance for the prevention and management of PHT. This would help mitigate the prevalence of HTN and associated cardiovascular complications, improving long-term health outcomes for PHT patients.
4 Limitations
It should be acknowledged that several limitations may have impacted the results of this study. First, the risk of bias assessment revealed several methodological shortcomings in the included trials, including deficiencies in random allocation concealment, absence of blinding for exercise interventions, and missing data attributed to low adherence. Secondly, the evidence is inherently unstable due to the limited number of RCTs included in this NMA. Future research should focus on conducting high-quality, large-scale RCTs to strengthen the evidence base. Thirdly, because of data and sample size restrictions, we were unable to identify the optimal dosage parameters. Therefore, additional definitive studies are required to investigate various intensities, durations, and frequencies of effective exercise types to clarify guidelines. Fourth, the majority of evidence was evaluated as low or very low quality, with downgraded confidence levels owing to risks of bias and heterogeneity. Despite performing sensitivity analyses and meta-regressions, we could not identify the principal causes of heterogeneity. Therefore, these findings need to be interpreted with prudence.
5 Conclusion
This systematic review and NMA demonstrate the significant effect of exercise on BP and vascular function in PHT individuals. Tai Chi exhibits the greatest effectiveness in reducing SBP, whereas IET produces the most notable improvements in DBP and PWV. MICT stands out in enhancing endothelial function. These findings provide a scientific basis for developing personalized exercise prescriptions. Particularly, Tai Chi and IET, owing to their proven efficacy and practicality, merit broader adoption in clinical and public health contexts. Nevertheless, further high-quality studies encompassing diverse exercise modalities are necessary to refine optimal exercise strategies and dosing parameters, thereby enhancing guidance for PHT prevention and management.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
YY: Conceptualization, Data curation, Writing – original draft, Writing – review & editing, Formal analysis, Methodology, Software. QL: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. XH: Conceptualization, Supervision, Writing – review & editing. YL: Formal analysis, Methodology, Writing – review & editing. XZ: Conceptualization, Data curation, Formal analysis, Writing – original draft. QW: Data curation, Methodology, Software, Writing – review & editing. XY: Methodology, Writing – review & editing. CY: Formal analysis, Software, Writing – review & editing. MH: Formal analysis, Software, Writing – review & editing. SW: Conceptualization, Data curation, Funding acquisition, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by the Beijing Municipal Natural Science Foundation (7232311), the National Natural Science Foundation of China (82374421), and the Major Tackling Project of Science and Technology Innovation Project of the Chinese Academy of Traditional Chinese Medicine (CI2021A00921).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1550435/full#supplementary-material
References
1. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2162–203. doi: 10.1016/S0140-6736(24)00933-4
2. Mancia G, Cappuccio FP, Burnier M, Coca A, Persu A, Borghi C, et al. Perspectives on improving blood pressure control to reduce the clinical and economic burden of hypertension. J Intern Med. (2023) 294:251–68. doi: 10.1111/joim.13678
3. Zhang F, Bryant KB, Moran AE, Zhang Y, Cohen JB, Bress AP, et al. Effectiveness of hypertension management strategies in sprint-eligible US adults: a simulation study. J Am Heart Assoc. (2024) 13:e32370. doi: 10.1161/JAHA.123.032370
4. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JJ, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. (2003) 289:2560–72. doi: 10.1001/jama.289.19.2560
5. Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. (2018) 137:2344–56. doi: 10.1161/CIRCULATIONAHA.117.032380
6. Jin Q, Chen Y. Risk of heart disease and stroke among individuals with prehypertension or blood pressure progression: a national population-based cohort study. Blood Press Monit. (2024) 29:173–9. doi: 10.1097/MBP.0000000000000698
7. Duan W, Wu J, Liu S, Jiao Y, Zheng L, Sun Y, et al. Impact of prehypertension on the risk of major adverse cardiovascular events in a Chinese rural cohort. Am J Hypertens. (2020) 33:465–70. doi: 10.1093/ajh/hpaa019
8. Pedralli ML, Marschner RA, Kollet DP, Neto SG, Eibel B, Tanaka H, et al. Different exercise training modalities produce similar endothelial function improvements in individuals with prehypertension or hypertension: a randomized clinical trial exercise, endothelium and blood pressure. Sci Rep. (2020) 10:7628. doi: 10.1038/s41598-020-64365-x
9. Tao S, Yu L, Yang D, Huang L, Li J. Association of endothelial function and limb artery indices with coronary artery stenosis severity in patients with hypertension. Ann Med. (2024) 56:2427369. doi: 10.1080/07853890.2024.2427369
10. Thijssen D, Bruno RM, van Mil A, Holder SM, Faita F, Greyling A, et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur Heart J. (2019) 40:2534–47. doi: 10.1093/eurheartj/ehz350
11. Quyyumi AA, Patel RS. Endothelial dysfunction and hypertension: cause or effect? Hypertension. (2010) 55:1092–4. doi: 10.1161/HYPERTENSIONAHA.109.148957
12. Kim HM, Rhee TM, Kim HL. Integrated approach of brachial-ankle pulse wave velocity and cardiovascular risk scores for predicting the risk of cardiovascular events. PLoS One. (2022) 17:e267614. doi: 10.1371/journal.pone.0267614
13. Russell SL, Rahman M, Steward CJ, Harwood AE, McGregor G, Banerjee P, et al. Central pulse wave velocity and augmentation index are repeatable and reproducible measures of arterial function. Health Sci Rep. (2024) 7:e70155. doi: 10.1002/hsr2.70155
14. Wu S, Chen D, Zeng X, Wen J, Zhou C, Xiao K, et al. Arterial stiffness is associated with target organ damage in subjects with pre-hypertension. Arch Med Sci. (2018) 14:1374–80. doi: 10.5114/aoms.2017.69240
15. Punia S, Singh V, Joshi S, Malik M, Saini M. Effects of walking in individuals with prehypertension and stage 1 hypertension in India: a randomised controlled trial. Int J Ther Rehabil. (2022) 29:1–10. doi: 10.12968/ijtr.2020.0163
16. Bai Y, Burns R, Gell N, Byun W. A randomized trial to promote physical activity in adult pre-hypertensive and hypertensive patients. J Sports Sci. (2022) 40:1648–57. doi: 10.1080/02640414.2022.2099179
17. Zhou YF, Liu N, Wang P, Jeong YJ, Song XY, Pan XF, et al. Cost-effectiveness of drug treatment for Chinese patients with stage I hypertension according to the 2017 hypertension clinical practice guidelines. Hypertension. (2020) 76:750–8. doi: 10.1161/HYPERTENSIONAHA.119.14533
18. Li J, Zhao D, Cai J, Chen S, Wu S, Qi Y. Cost-effectiveness of treatment in adults with blood pressure of 130–139/80–89 mmHg and high cardiovascular risk in China: a modelling study. Lancet Reg Health West Pac. (2024) 42:100962. doi: 10.1016/j.lanwpc.2023.100962
19. Li W, Liu H, Wang X, Liu J, Xiao H, Wang C, et al. Interventions for reducing blood pressure in prehypertension: a meta-analysis. Front Public Health. (2023) 11:1139617. doi: 10.3389/fpubh.2023.1139617
20. Zhou HY, Wang SY, Zhao CT, He H. Effect of exercise on vascular function in hypertension patients: a meta-analysis of randomized controlled trials. Front Cardiovasc Med. (2022) 9:1013490. doi: 10.3389/fcvm.2022.1013490
21. Alvarez C, Peñailillo L, Ibacache-Saavedra P, Jerez-Mayorga D, Campos-Jara C, Andrade DC, et al. Six weeks of a concurrent training therapy improves endothelial function and arterial stiffness in hypertensive adults with minimum non-responders. Hipertens Riesgo Vasc. (2024) 41(4):240–50. doi: 10.1016/j.hipert.2024.07.001
22. Mills EJ, Thorlund K, Ioannidis JP. Demystifying trial networks and network meta-analysis. Br Med J. (2013) 346:f2914. doi: 10.1136/bmj.f2914
23. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. (2004) 23:3105–24. doi: 10.1002/sim.1875
24. Higgins J, GSCC. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: John Wiley & Sons Ltd (2011). p. S38.
25. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The prisma 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
26. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The prisma extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
27. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JJ, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. (2003) 42:1206–52. doi: 10.1161/01.HYP.0000107251.49515.c2
28. Sterne J, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
29. Minozzi S, Dwan K, Borrelli F, Filippini G. Reliability of the revised Cochrane risk-of-bias tool for randomised trials (rob2) improved with the use of implementation instruction. J Clin Epidemiol. (2022) 141:99–105. doi: 10.1016/j.jclinepi.2021.09.021
30. Crocker TF, Lam N, Jordao M, Brundle C, Prescott M, Forster A, et al. Risk-of-bias assessment using Cochrane’s revised tool for randomized trials (rob 2) was useful but challenging and resource-intensive: observations from a systematic review. J Clin Epidemiol. (2023) 161:39–45. doi: 10.1016/j.jclinepi.2023.06.015
31. Seitidis G, Tsokani S, Christogiannis C, Kontouli KM, Fyraridis A, Nikolakopoulos S, et al. Graphical tools for visualizing the results of network meta-analysis of multicomponent interventions. Res Synth Methods. (2023) 14:382–95. doi: 10.1002/jrsm.1617
32. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:ED142. doi: 10.1002/14651858.ED000142
33. Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. (2013) 33:607–17. doi: 10.1177/0272989X12458724
34. Dempster AP. The direct use of likelihood for significance testing. Stat Comput. (1997) 7:247–52. doi: 10.1023/A:1018598421607
35. van Valkenhoef G, Dias S, Ades AE, Welton NJ. Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res Synth Methods. (2016) 7:80–93. doi: 10.1002/jrsm.1167
36. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. Grade: an emerging consensus on rating quality of evidence and strength of recommendations. Br Med J. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
37. Puhan MA, Schunemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, et al. A grade working group approach for rating the quality of treatment effect estimates from network meta-analysis. Br Med J. (2014) 349:g5630. doi: 10.1136/bmj.g5630
38. Nikolakopoulou A, Higgins J, Papakonstantinou T, Chaimani A, Del GC, Egger M, et al. Cinema: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. (2020) 17:e1003082. doi: 10.1371/journal.pmed.1003082
39. Papakonstantinou T, Nikolakopoulou A, Higgins J, Egger M, Salanti G. Cinema: software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst Rev. (2020) 16:e1080. doi: 10.1002/cl2.1080
40. Azadpour N, Tartibian B, Koşar ŞN. Effects of aerobic exercise training on ace and adrb2 gene expression, plasma angiotensin ii level, and flow-mediated dilation: a study on obese postmenopausal women with prehypertension. Menopause. (2017) 24:269–77. doi: 10.1097/GME.0000000000000762
41. Banks NF, Rogers EM, Stanhewicz AE, Whitaker KM, Jenkins N. Resistance exercise lowers blood pressure and improves vascular endothelial function in individuals with elevated blood pressure or stage-1 hypertension. Am J Physiol Heart Circ Physiol. (2024) 326:H256–69. doi: 10.1152/ajpheart.00386.2023
42. Beck DT, Casey DP, Martin JS, Emerson BD, Braith RW. Exercise training improves endothelial function in young prehypertensives. Exp Biol Med (Maywood). (2013) 238:433–41. doi: 10.1177/1535370213477600
43. John AT, Chowdhury M, Islam MR, Mir IA, Hasan MZ, Chong CY, et al. Effectiveness of high-intensity interval training and continuous moderate-intensity training on blood pressure in physically inactive pre-hypertensive young adults. J Cardiovasc Dev Dis. (2022) 9(8):246. doi: 10.3390/jcdd9080246
44. Krishna BH, Pulaganti M, Sekhar AC, Jampala S. Exploring the effects of yoga therapy on cardiovascular risk profile, cardiac workload, and oxygen demand in individuals with prehypertension: a pilot study. Int J Acad Med Pharm. (2023) 5:1595–600. doi: 10.47009/jamp.2023.5.5.313
45. Lee DC, Brellenthin AG, Lanningham-Foster LM, Kohut ML, Li Y. Aerobic, resistance, or combined exercise training and cardiovascular risk profile in overweight or obese adults: the cardiorace trial. Eur Heart J. (2024) 45:1127–42. doi: 10.1093/eurheartj/ehad827
46. Li X, Chang P, Wu M, Jiang Y, Gao Y, Chen H, et al. Effect of tai chi vs aerobic exercise on blood pressure in patients with prehypertension: a randomized clinical trial. JAMA Netw Open. (2024) 7:e2354937. doi: 10.1001/jamanetworkopen.2023.54937
47. Magutah K, Mbuthia G, Akiruga JA, Haile D, Thairu K. Effect of fixed 7.5 min’ moderate intensity exercise bouts on body composition and blood pressure among sedentary adults with prehypertension in western-Kenya. PLoS Glob Public Health. (2022) 2:e806. doi: 10.1371/journal.pgph.0000806
48. Narnolia PK, Binawara BK, Mehra M, Sharma P, Sharma S. To study the effect of Sudarshan Kriya yoga and conventional physical exercise on blood pressure, pulse rate and quality of life in prehypertensive subjects. Int J Pharm Clin Res. (2024) 16:666–70. Available at: https://www-embase-com.edlibproxy.flysheet.com.tw:8443/records?subaction=viewrecord&rid=1&page=1&id=L2030826478
49. Nualnim N, Parkhurst K, Dhindsa M, Tarumi T, Vavrek J, Tanaka H. Effects of swimming training on blood pressure and vascular function in adults >50 years of age. Am J Cardiol. (2012) 109:1005–10. doi: 10.1016/j.amjcard.2011.11.029
50. O'Driscoll JM, Edwards JJ, Coleman DA, Taylor KA, Sharma R, Wiles JD. One year of isometric exercise training for blood pressure management in men: a prospective randomized controlled study. J Hypertens. (2022) 40:2406–12. doi: 10.1097/HJH.0000000000003269
51. Ogbutor GU, Nwangwa EK, Uyagu DD. Isometric handgrip exercise training attenuates blood pressure in prehypertensive subjects at 30% maximum voluntary contraction. Niger J Clin Pract. (2019) 22:1765–71. doi: 10.4103/njcp.njcp_240_18
52. Prasertsri P, Singsanan S, Chonanant C, Boonla O, Trongtosak P. Effects of arm swing exercise training on cardiac autonomic modulation, cardiovascular risk factors, and electrolytes in persons aged 60–80 years with prehypertension: a randomized controlled trial. J Exerc Sci Fit. (2019) 17:47–54. doi: 10.1016/j.jesf.2018.11.002
53. Singh VP, Khandelwal B. Effectiveness of yoga and lifestyle modification on prehypertensive subjects-a randomized controlled trial. Neuroquantology. (2022) 20:1323–37. doi: 10.48047/NQ.2022.20.17.NQ880167
54. Songcharern N, Ruangthai R, Tumnark P, Phoemsapthawee J. Improved arterial stiffness after combined aerobic and resistance training: correlation with heart rate variability change in prehypertensive offspring of hypertensive parents. J Exerc Rehabil. (2022) 18:395–405. doi: 10.12965/jer.2244416.208
55. Thiyagarajan R, Pal P, Pal GK, Subramanian SK, Trakroo M, Bobby Z, et al. Additional benefit of yoga to standard lifestyle modification on blood pressure in prehypertensive subjects: a randomized controlled study. Hypertens Res. (2015) 38:48–55. doi: 10.1038/hr.2014.126
56. Wong A, Figueroa A, Fischer SM, Bagheri R, Park SY. The effects of mat pilates training on vascular function and body fatness in obese young women with elevated blood pressure. Am J Hypertens. (2020) 33:563–9. doi: 10.1093/ajh/hpaa026
57. Yin Y, Yu Z, Wang J, Sun J. Effects of the different tai chi exercise cycles on patients with essential hypertension: a systematic review and meta-analysis. Front Cardiovasc Med. (2023) 10:1016629. doi: 10.3389/fcvm.2023.1016629
58. Li C, Wu S, Lei B, Zang W, Tao X, Yu L. Effect of aerobic exercise on endothelial function in hypertensive and prehypertensive patients: a systematic review and meta-analysis of randomized controlled trials. J Hypertens. (2025) 43:727–38. doi: 10.1097/HJH.0000000000003980
59. Ji H, Gulati M, Huang TY, Kwan AC, Ouyang D, Ebinger JE, et al. Sex differences in association of physical activity with all-cause and cardiovascular mortality. J Am Coll Cardiol. (2024) 83:783–93. doi: 10.1016/j.jacc.2023.12.019
60. Edwards JJ, Deenmamode A, Griffiths M, Arnold O, Cooper NJ, Wiles JD, et al. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br J Sports Med. (2023) 57:1317–26. doi: 10.1136/bjsports-2022-106503
61. Ma J, Zhang JW, Li H, Zhao LS, Guo AY, Chen ZH, et al. Safety and effectiveness of a tai chi-based cardiac rehabilitation programme for chronic coronary syndrom patients: study protocol for a randomised controlled trial. Bmj Open. (2020) 10:e36061. doi: 10.1136/bmjopen-2019-036061
62. Lu WA, Kuo CD. The effect of tai chi chuan on the autonomic nervous modulation in older persons. Med Sci Sports Exerc. (2003) 35:1972–6. doi: 10.1249/01.MSS.0000099242.10669.F7
63. Ojangba T, Boamah S, Miao Y, Guo X, Fen Y, Agboyibor C, et al. Comprehensive effects of lifestyle reform, adherence, and related factors on hypertension control: a review. J Clin Hypertens (Greenwich). (2023) 25:509–20. doi: 10.1111/jch.14653
64. Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. (2014) 2:634–47. doi: 10.1016/S2213-8587(14)70102-0
65. Filippone EJ, Foy AJ, Naccarelli GV. Controversies in hypertension I: the optimal assessment of blood pressure load and implications for treatment. Am J Med. (2022) 135:1043–50. doi: 10.1016/j.amjmed.2022.05.007
66. Chen Z, Li Q, Xu T, Zhou X, Shu Y, Guo T, et al. An updated network meta-analysis of non-pharmacological interventions for primary hypertension in adults: insights from recent studies. Syst Rev. (2024) 13:318. doi: 10.1186/s13643-024-02744-5
67. Zhang W, Wang H, Xiong Z, Li C. Efficacy of tai chi exercise in patients with hypertension: systematic review and meta-analysis. Curr Probl Cardiol. (2024) 49:102798. doi: 10.1016/j.cpcardiol.2024.102798
68. Edwards J, De Caux A, Donaldson J, Wiles J, O'Driscoll J. Isometric exercise versus high-intensity interval training for the management of blood pressure: a systematic review and meta-analysis. Br J Sports Med. (2022) 56:506–14. doi: 10.1136/bjsports-2021-104642
69. Carlson DJ, Dieberg G, Hess NC, Millar PJ, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis. Mayo Clin Proc. (2014) 89:327–34. doi: 10.1016/j.mayocp.2013.10.030
70. Edwards JJ, Coleman DA, Ritti-Dias RM, Farah BQ, Stensel DJ, Lucas S, et al. Isometric exercise training and arterial hypertension: an updated review. Sports Med. (2024) 54:1459–97. doi: 10.1007/s40279-024-02036-x
71. Inaba Y, Chen JA, Bergmann SR. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: a meta-analysis. Int J Cardiovasc Imaging. (2010) 26:631–40. doi: 10.1007/s10554-010-9616-1
72. Durand MJ, Gutterman DD. Exercise and vascular function: how much is too much? Can J Physiol Pharmacol. (2014) 92:551–7. doi: 10.1139/cjpp-2013-0486
Keywords: exercise, prehypertension, blood pressure, endothelial function, network meta-analysis
Citation: Yang Y, Lv Q, Hou X, Lv Y, Zhang X, Wu Q, Ye X, Yang C, Huang M and Wang S (2025) Effects of different exercise modalities on blood pressure and endothelial function in prehypertension individuals: a systematic review and network meta-analysis. Front. Cardiovasc. Med. 12:1550435. doi: 10.3389/fcvm.2025.1550435
Received: 27 January 2025; Accepted: 6 June 2025;
Published: 25 June 2025.
Edited by:
Lanfranco D'Elia, University of Naples Federico II, ItalyReviewed by:
R. Clinton Webb, University of South Carolina, United StatesHugo Vieira Pereira, Lusofona University, Portugal
Copyright: © 2025 Yang, Lv, Hou, Lv, Zhang, Wu, Ye, Yang, Huang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shihan Wang, d2FuZ3NoaWhhbjkxQDEyNi5jb20=
†These authors have contributed equally to this work