 Ana Belén Jiménez-Jiménez1,2*
Ana Belén Jiménez-Jiménez1,2* Javier Muñoz-Paz1,2Diana Ladera-Santos1,3Ángela Heredia-Torres1,2
Javier Muñoz-Paz1,2Diana Ladera-Santos1,3Ángela Heredia-Torres1,2 Javier Caballero-Villarraso1,4Fernando Mayordomo-Riera1,2
Javier Caballero-Villarraso1,4Fernando Mayordomo-Riera1,2
- 1GC-28 Group, Maimonides Biomedical Research Institute of Cordoba (IMIBIC), Córdoba, Spain
- 2Department of Physical Medicine and Rehabilitation, Reina Sofía University Hospital, Córdoba, Spain
- 3Department of Cardiology, Reina Sofía University Hospital, Córdoba, Spain
- 4Department of Clinical Analysis, Reina Sofía University Hospital, Córdoba, Spain
Takotsubo syndrome (TTS) is an acute cardiac condition characterized by transient regional left ventricular systolic dysfunction. Traditionally, it has been associated with physical or psychological stressors. Clinically, the onset of TTS is similar to acute coronary syndrome, requiring appropriate differential diagnosis to distinguish between the two clinical entities. Its treatment is usually conservative, and the prognosis is generally favorable. We report the case of a 57-year-old woman who was referred to the Department of Rehabilitation after suffering a non-ST-segment elevation myocardial infarction. During her eighth physical rehabilitation session, she developed palpitations and hypertension. Initial telemetry monitoring showed ventricular bigeminy with extrasystoles, tachycardia episodes, and ST-segment elevation. She was admitted to the Department of Cardiology, and cardiac catheterization and subsequent coronary angiography were performed, revealing no incidence of coronary lesions. However, ventriculography demonstrated severe left ventricular dysfunction in the systolic phase, characterized by akinesia of the mid-apical segments. These findings were suggestive of Takotsubo syndrome, which was subsequently confirmed by cardiac magnetic resonance imaging.
Introduction
Takotsubo syndrome (TTS), also known as “broken heart syndrome” or “stress-induced cardiomyopathy,” is a rare clinical entity. Its prevalence is estimated to be 1%–2% in patients presenting with suspected acute coronary syndrome (ACS) (1). Keeping in mind certain contexts in which this disease can appear is essential to facilitate early and accurate diagnosis and ensure proper treatment.
Takotsubo syndrome is a nonischemic heart disease that usually affects postmenopausal women. It has traditionally been associated with emotional or physical stressors, such as an intense emotional reaction, typically occurring within 5 days prior to symptom onset. Although the etiological mechanisms remain unknown, it is believed that sympathetic discharge plays a key role. This sympathetic discharge can lead to myocardial contraction, microvascular dysfunction, myocardial infarction, and systolic dysfunction (2).
Its clinical manifestations and electrocardiogram abnormalities often mimic those of ACS, especially in the early phase. Often reported symptoms are chest discomfort, electrocardiogram abnormalities such as ST-segment elevation or depression, and cardiac rhythm abnormalities on ECG. In some cases, however, the ECG may appear normal. Blood tests usually show high serum levels of troponin. Therefore, an accurate differential diagnosis is important between the two diseases (3, 4). Nevertheless, TTS manifests as wall motion abnormalities in the absence of obstructive coronary artery disease, as confirmed by angiography.
The typical pattern of abnormal regional left ventricular motion in TTS includes apical hypokinesia, akinesia, or dyskinesia with apical ballooning, accompanied by relative basal hyperkinesia, resembling the shape of octopus traps used in Japan. Atypical forms of TTS also exist, which are characterized by mid-ventricular or basal hypokinesia. Focal stress-induced TTS is another rare form that closely mimics myocarditis or myocardial infarction, making differential diagnosis challenging. In particular, midventricular TTS is characterized by motion abnormalities in the middle portion of the left ventricle, while the apical region remains normokinetic or hyperkinetic. Atypical TTS presents with a peculiarity: ECG abnormalities often include ST-segment depression and less profound T-wave inversion in leads I and aVL. Patients with atypical TTS are usually younger than those with typical TTS, and there are usually no differences in symptoms or emotional or physical triggers (5).
Cardiac magnetic resonance (CMR) is a valuable, non-invasive diagnostic tool that facilitates the differential diagnosis between ischemic and nonischemic etiologies (acute myocarditis, Takotsubo syndrome, and other conditions) of myocardial injury (6).
TTS usually responds well to conservative treatment, with complete recovery of systolic function after several weeks or months. However, sometimes, heart rehabilitation programs may be required. Even so, its prognosis is generally favorable (7, 8).
Case description
The patient is a 57-year-old woman with a medical history of dyslipidemia managed with statins and a history of smoking (since 2 years ago) and appendectomy. She was receiving treatment with omeprazole, aspirin, ticagrelor, bisoprolol, ramipril, atorvastatin/ezetimibe, and eplerenone because of a non-ST-segment elevation myocardial infarction (NSTEMI) in June 2022.
She was referred to the Department of Rehabilitation to begin heart physical therapy 7 months after suffering an NSTEMI. The NSTEMI was caused by a total obstruction in the proximal to mid-segment of the right coronary artery, and it was treated with revascularization using a Biofreedom stent (2.5 × 22 mm). The patient had a mildly depressed left ventricular ejection fraction (LVEF 50%) because of septal and inferior hypokinesia and presented with symptoms of acute heart failure, including dyspnea, which was classified as NYHA functional class II, and orthopnea.
Before beginning rehabilitation treatment, an initial evaluation was carried out, which consisted of an ergospirometry test performed on a treadmill following an incremental Naughton ramp protocol. The test was terminated due to patient exhaustion; however, it was clinically and electrocardiographically negative for ischemic heart disease. The patient passed the test and was included in a medium cardiac risk group (score 0+).
After 5 months of starting the rehabilitation program, the patient told us of an intense emotional reaction related to a family problem that occurred 2 days before the eighth rehabilitation session. The patient said that she felt worried. During physical training, her heart rate and rhythm were monitored by electrode patches placed on her chest. The telemetry data on heart rate and rhythm were projected onto a medical computer and supervised by a doctor, allowing observation of changes in cardiac rate or rhythm while the patient walked on the treadmill.
During the eighth rehabilitation session, the patient walked on the treadmill at 4.5 km/h with no incline. She began experiencing palpitations, but she did not report dyspnea, thoracic pain, or fainting. Telemetry showed ventricular bigeminy, which is characterized by extrasystole and tachycardia episodes reaching 130–140 beats per minute (bpm), a wide QRS complex during exertion, and ST-segment elevation (Figure 1). As a result of this episode, the training session was halted. Arterial pressure was measured, and it indicated 180 mmHg (diastolic) and 120 mmHg (systolic). During the acute phase, a blood test revealed a serum level of high-sensitivity troponin of 3.012 ng/L (normal range: <0.4 ng/L). However, the cardiac rhythm and arterial pressure normalized after 30 min of rest.
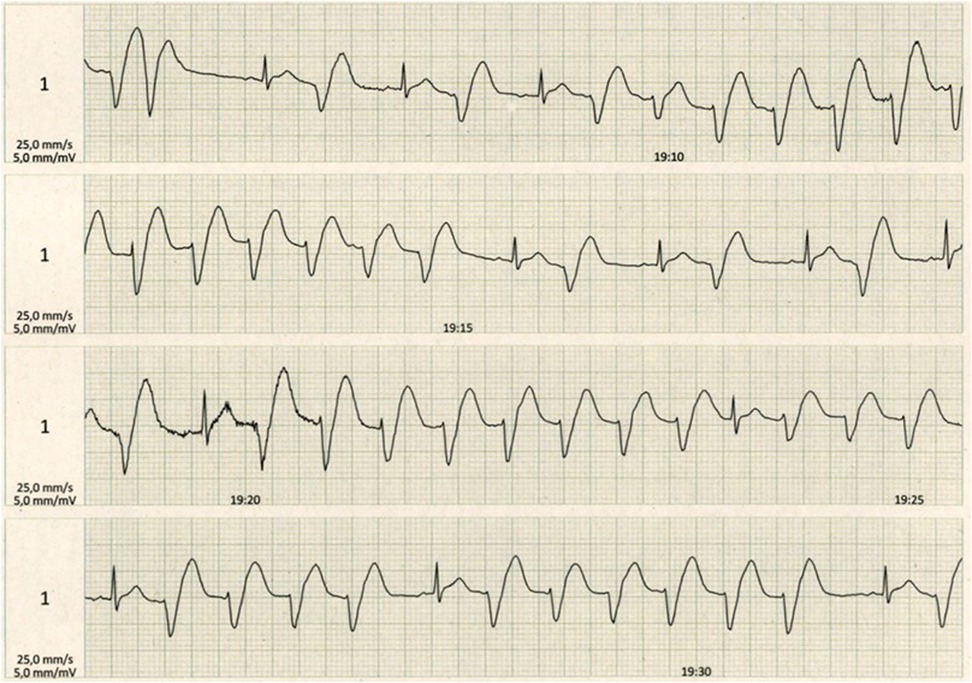
Figure 1. Telemetry during exertion in the eighth session of the heart rehabilitation program showing ventricular bigeminy with extrasystole and tachycardia with wide QRS complex episodes reaching 130–140 beats per minute and ST-segment elevation.
The patient was admitted to the Department of Cardiology. A beta-blocker dose was prescribed, and the heart rhythm was monitored. Another ECG performed after 3 h demonstrated sinus tachycardia at 100 bpm, a narrow QRS complex with inferior Q waves, slow R-to-S progression in the precordial leads, and isolated J-point elevation in lead V6 (Figure 2). The patient was then transferred to the hemodynamics unit, where catheterization and subsequent coronary angiography were performed, which did not reveal coronary artery obstruction (Figure 3A). Thus, ischemic heart disease was ruled out. Afterward, left ventriculography demonstrated akinesia and ballooning of the middle and apical segments and severe systolic dysfunction (Figure 3B), with no left ventricular contraction during the diastolic phase (Figure 3C). These findings suggested a diagnosis of TTS.
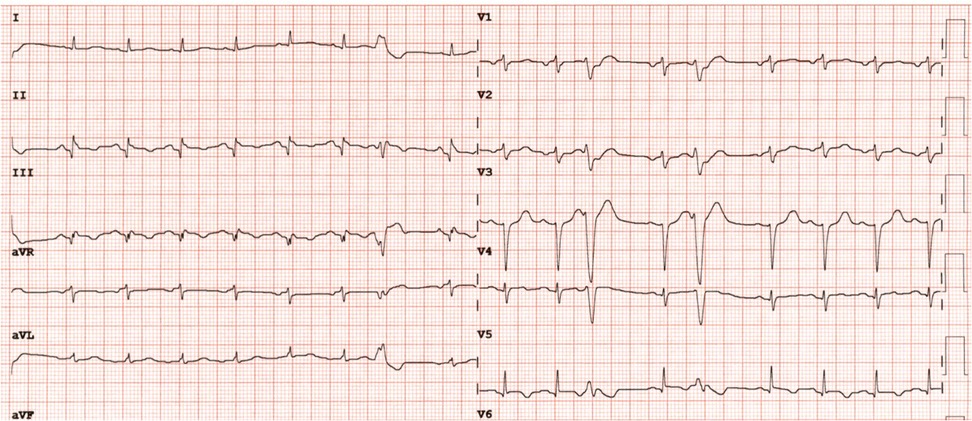
Figure 2. ECG performed in the Cardiology Department demonstrating sinus tachycardia at 100 bpm, narrow QRS complexes, inferior Q waves, slow R-to-S progression in the precordial leads, and isolated J-point elevation in lead V6.
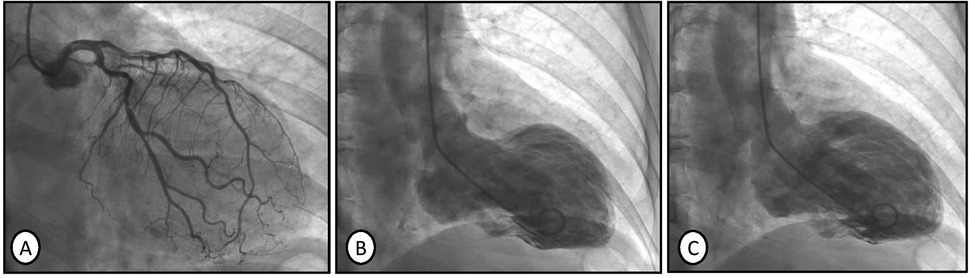
Figure 3. Coronary angiography with no evidence of coronary artery obstruction (A). Ventriculography performed in the left ventricle revealing akinesia and ballooning of the middle and apical segments , indicating severe dysfunction in the end-systolic phase (B). Normal left ventricular contraction during the end-diastolic phase (C).
During this time, the patient remained asymptomatic, except for an increase in cardiac frequency during minimal exertion, but these symptoms resolved gradually. On day 4, a CMR scan was performed, and it confirmed the diagnosis of TTS. Imaging showed a dilated, non-hypertrophic left ventricle with a moderately reduced left ventricular ejection fraction (LVEF 39%) and noticeable hypokinesia of the mid-apical segments during systole (Figure 4A), while diastolic function remained normal (Figure 4B). Additionally, the T2-STIR sequence showed a marked increase in signal intensity in the mid-apical segments, consistent with diffuse myocardial edema (Figure 4C). In addition, a previous infarction area appeared in the right coronary artery territory. No intracavitary thrombi, pericardial effusion, or pleural effusion were observed. Therefore, according to these findings, the patient was diagnosed with TTS.
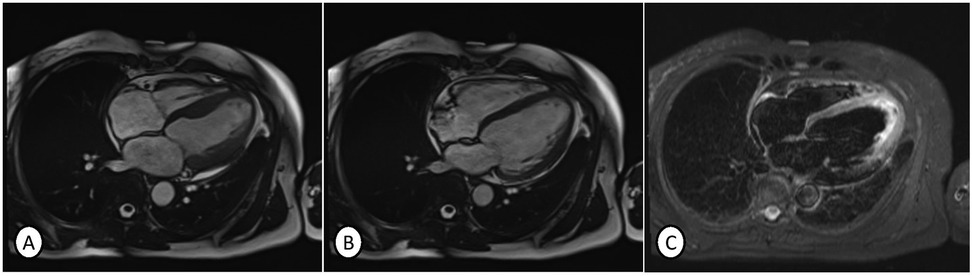
Figure 4. Cardiac magnetic resonance imaging showing a dilated, non-hypertrophic left ventricle with a moderately depressed left ventricular ejection fraction (LVEF 39%) and noticeable hypokinesia in the mid-apical segments during systole (A) and normal contraction in the diastole (B), and T2-STIR sequence showing a marked increase in signal intensity in the mid-apical segments, consistent with diffuse myocardial edema (C). No intracavitary thrombi or pericardial or pleural effusions were observed. Therefore, according to these findings, the patient was diagnosed with TTS.
Discharge recommendations included maintaining a healthy lifestyle, following the Mediterranean Diet, avoiding stressful situations and potential emotional triggers, controlling cardiovascular risk factors under the care of a primary attention physician, recognizing warning signs requiring evaluation at the Emergency Department, and continuing treatment with acetylsalicylic acid, an angiotensin-converting enzyme inhibitor, a beta-blocker, and statins.
The clinical course was uncomplicated, and the patient was included again in a heart rehabilitation program to improve her ventricular function. She completed the program without complications. After 5 months of completing the rehabilitation program, a planned transthoracic echocardiogram indicated complete recovery of left ventricular function, with normalization of global and segmental systolic function and a preserved left ventricular ejection fraction (LVEF 55%).
Discussion
TTS is a rare heart disease characterized by transient left ventricular systolic dysfunction, which usually affects the apex. The primary differential diagnosis is ACS due to similar electrical, biochemical, and clinical presentations (9). As we mentioned in the diagnosis of the reported patient, the acute phase of TTS often involves ECG abnormalities (cardiac arrhythmias, ST-segment elevation, or Q waves), clinical symptoms, and high troponin levels in blood tests—features commonly seen in both diseases, complicating the differential diagnosis (10). However, coronary angiography, ventriculography, and cardiac magnetic resonance imaging support a TTS diagnosis.
For this reason, patients undergoing a heart rehabilitation program should be monitored effectively to enable the early detection of ACS (the most frequent complication), as well as other rare diseases such as TTS.
The etiology of TTS remains unclear, although it has been reported to be associated with emotional or physical stress (11, 12). Other cases of TTS triggered by stressful physical situations (such as hypoglycemia or a traumatic amputation) have also been reported (13, 14). Although TTS is usually associated with negative emotional events (such as fear or anxiety), it can also occur in spectators experiencing intense positive emotions during stressful sporting events (15).
It has been proposed that these stressful factors are related to sympathetic discharge and elevated catecholamine levels (16). This can lead to myocardial stunning, microvascular dysfunction, myocardial microinfarction, and, consequently, typical left ventricular systolic dysfunction (4). Recent evidence suggests that TTS may be a form of ACS due to microvascular dysfunction (17, 18). In this regard, a case of TTS has been reported in a patient after a COVID-19 infection (19, 20).
This case has two peculiarities: (i) TTS onset occurred in a cardiac monothyrization setting during a training session (in the Department of Rehabilitation), which allowed for an early diagnosis; and (ii) two etiological factors were present at the same time. It should be considered that ventricular tachycardia appearance after physical training and previous emotionally stressful events could have a synergistic effect on the myocardium. These actions (especially when combined) could result in a potential adrenergic discharge and, therefore, a greater probability of the development of left ventricular dysfunction.
As with this patient, TTS treatment is usually conservative, involving expectant behavior and monitoring for arterial pressure and the possible appearance of cardiac arrhythmias. This dysfunction is generally transient, and the majority of patients recover systolic function within weeks to months. Occasionally, they require inclusion in heart rehabilitation programs (21, 22).
From the patient's perspective, she told us that verbalizing this family problem helped her feel more at peace. Furthermore, the continuous care by the nurses (monitoring blood pressure and heart rhythm) made her feel cared for and looked after, and she demonstrated a grateful attitude every time.
Conclusion
It is well-known that the risk of cardiovascular complications increases after an ACS, particularly within the first 5 years. There is a greater probability of developing TTS in the first 4 weeks after ACS (23). Despite the possibility of this heart complication, we found no other cases in the scientific literature reporting the onset of TTS in patients enrolled in a heart rehabilitation program after an ACS, particularly during therapy sessions. For this reason, we would like to emphasize the rigor of the established guidelines, algorithms, and the importance of bearing in mind this rare condition, even in unusual contexts. Undoubtedly, these diagnostic algorithms lead to an appropriate syndromic classification because they involve a correct exclusion diagnosis of ACS.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AJ-J: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Visualization. JM-P: Conceptualization, Investigation, Writing – original draft. ML: Data curation, Visualization, Writing – original draft. ÁH-T: Conceptualization, Investigation, Writing – review & editing. JC-V: Writing – original draft, Writing – review & editing. FM-R: Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by the R&D budget from the Department of Physical Medicine and Rehabilitation of Reina Sofia University Hospital, Córdoba.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1560087/full#supplementary-material
References
1. Medina de Chazal H, Del Buono MG, Keyser-Marcus L, Ma L, Moeller FG, Berrocal D, et al. Stress cardiomyopathy diagnosis and treatment: JACC state-of-the-art review. J Am Coll Cardiol. (2018) 72:1955–71. doi: 10.1016/j.jacc.2018.07.072
2. Omerovic E, Citro R, Bossone E, Redfors B, Backs J, Bruns B, et al. Pathophysiology of Takotsubo syndrome—a joint scientific statement from the heart failure association Takotsubo syndrome study group and myocardial function working group of the European Society of Cardiology—part 1: overview and the central role for catecholamines and sympathetic nervous system. Eur J Heart Fail. (2022) 24:257–73. doi: 10.1002/ejhf.2400
3. Moady G, Vons S, Atar S. A comparative retrospective study of patients with Takotsubo syndrome and acute coronary syndrome. Isr Med Assoc J. (2021) 23(2):107–10.33595216
4. Crea F, Iannaccone G, La Vecchia G, Montone RA. An update on the mechanisms of Takotsubo syndrome: “at the end an acute coronary syndrome”. J Mol Cell Cardiol. (2024) 191:1–6. doi: 10.1016/j.yjmcc.2024.04.009
5. Padilla-Lopez M, Duran-Cambra A, Belmar-Cliville D, Soriano-Amores M, Arakama-Goikoetxea S, Vila-Perales M, et al. Comparative electrocardiographic analysis of midventricular and typical Takotsubo syndrome. Front Cardiovasc Med. (2023) 10:1286975. doi: 10.3389/fcvm.2023.1286975
6. Liang K, Nakou E, Del Buono MG, Montone RA, D'Amario D, Bucciarelli-Ducci C. The role of cardiac magnetic resonance in myocardial infarction and non-obstructive coronary arteries. Front Cardiovasc Med. (2022) 8:821067. doi: 10.3389/fcvm.2021.821067
7. Assad J, Femia G, Pender P, Badie T, Rajaratnam R. Takotsubo syndrome: a review of presentation, diagnosis and management. Clin Med Insights Cardiol. (2022) 16:82. doi: 10.1177/11795468211065782
8. Matta A, Delmas C, Campelo-Parada F, Lhermusier T, Bouisset F, Elbaz M, et al. Takotsubo cardiomyopathy. Rev Cardiovasc Med. (2022) 23(1):38. doi: 10.31083/j.rcm2301038
9. Lau C, Chiu S, Nayak R, Lin B, Lee MS. Survival and risk of recurrence of Takotsubo syndrome. Heart. (2021) 107(14):1160–6. doi: 10.1136/heartjnl-2020318028
10. Colantonio M, Awad M, Liriano MM, Santer M, Murshid A, Haleem A. An unlikely cause of chest pain: recurrent Takotsubo cardiomyopathy. J Community Hosp Intern Med Perspect. (2024) 14(5):114–9. doi: 10.55729/2000-9666.1394
11. Bader M, Mubarak M, Ali S, Hasan Z, Alsudairy N. A case of Takotsubo cardiomyopathy in a 65-year-old woman triggered by emotional stress. Cureus. (2024) 16(11):e73533. doi: 10.7759/cureus.73533
12. Wei Juan L, Kaisbain N. Emotional stress induced broken heart syndrome: a case report. Cureus. (2022) 14(12):e32384. doi: 10.7759/cureus.32384
13. Xia P, Zhang Y, Sun Y, Wang J. Case report: Takotsubo syndrome induced by severe hypoglycemia. Front Cardiovasc Med. (2022) 9:1059638. doi: 10.3389/fcvm.2022.1059638
14. Bacro-Duverger BH, Thorburn AQ, Denney BD, Gullett JP, Thompson MA, Pigott DC. Takotsubo cardiomyopathy following traumatic hand amputation: a case report. Clin Pract Cases Emerg Med. (2022) 6(3):225–28. doi: 10.5811/cpcem.2022.2.55463
15. Polimeni A, Spaccarotella C, Ielapi J, Esposito G, Ravera A, Martuscelli E, et al. The impact of UEFA Euro 2020 football championship on Takotsubo syndrome: results of a multicenter national registry. Front Cardiovasc Med. (2022) 9:951882. doi: 10.3389/fcvm.2022.951882
16. Ruiz P, Gabarre P, Chenevier-Gobeaux C, François H, Kerneis M, Cidlowski JA, et al. Case report: changes in the levels of stress hormones during Takotsubo syndrome. Front Cardiovasc Med. (2022) 9:931054. doi: 10.3389/fcvm.2022.931054
17. Dong F, Yin L, Sisakian H, Hakobyan T, Jeong LS, Joshi H, et al. Takotsubo syndrome is a coronary microvascular disease: experimental evidence. Eur Heart J. (2023) 44(24):2244–53. doi: 10.1093/eurheartj/ehad274
18. Alim S, Shah H, Zahera SM, Rahmatova J, Irfan M, Mahmood Z, et al. An update on Takotsubo syndrome. J Cardiovasc Med. (2023) 24(10):691–9. doi: 10.2459/JCM.0000000000001528
19. Li P, Wang Y, Liang J, Zuo X, Li Q, Sherif AA, et al. Takotsubo syndrome and respiratory diseases: a systematic review. Eur Heart J Open. (2022) 2(2):oeac009. doi: 10.1093/ehjopen/oeac009
20. Dall'Ara G, Compagnone M, Carletti R, Piciucchi S, Gardini E, Galvani M. Case report: asymptomatic SARS-COV2 infection triggering recurrent Takotsubo syndrome. Front Cardiovasc Med. (2024) 11:1418316. doi: 10.3389/fcvm.2024.1418316
21. Bairashevskaia AV, Belogubova SY, Kondratiuk MR, Rudnova DS, Sologova SS, Tereshkina OI, et al. Update of Takotsubo cardiomyopathy: present experience and outlook for the future. Int J Cardiol Heart Vasc. (2022) 39:100990. doi: 10.1016/j.ijcha.2022.100990
22. Gobeil K, White K, Bhat A, Szalai H, Lagu TC, Pack QR. Cardiac rehabilitation in Takotsubo cardiomyopathy: predictors of utilization and effects of exercise training. Heart Lung. (2021) 50(2):230–4. doi: 10.1016/j.hrtlng.2020.12.006
Keywords: Takotsubo, broken heart syndrome, stress-induced cardiomyopathy, atypical onset, heart rehabilitation
Citation: Jiménez-Jiménez AB, Muñoz-Paz J, Ladera-Santos D, Heredia-Torres Á, Caballero-Villarraso J and Mayordomo-Riera F (2025) Case Report: Onset of Takotsubo syndrome during a heart rehabilitation session. Front. Cardiovasc. Med. 12:1560087. doi: 10.3389/fcvm.2025.1560087
Received: 13 January 2025; Accepted: 28 May 2025;
Published: 24 June 2025.
Edited by:
Junjie Xiao, Shanghai University, ChinaReviewed by:
Giulia Iannaccone, Catholic University of the Sacred Heart, ItalyFulvio Cacciapuoti, Hospital Antonio Cardarelli, Italy
Copyright: © 2025 Jiménez-Jiménez, Muñoz-Paz, Ladera-Santos, Heredia-Torres, Caballero-Villarraso and Mayordomo-Riera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Belén Jiménez-Jiménez, YW5hYi5qaW1lbmV6LmppbWVuZXouc3NwYUBqdW50YWRlYW5kYWx1Y2lhLmVz