 Hendrik T. Tevaearai Stahel1*
Hendrik T. Tevaearai Stahel1* Gabriel Weiss2,3Peter Landowski2,3Sandra Folkmann2,3Marieluise Harrer2,3Bernard Voet4Martin Grabenwöger2,3,5
Gabriel Weiss2,3Peter Landowski2,3Sandra Folkmann2,3Marieluise Harrer2,3Bernard Voet4Martin Grabenwöger2,3,5
- 1Cardiovascular Department, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
- 2Department of Cardiovascular Surgery, Clinic Floridsdorf, Vienna, Austria
- 3Karl Landsteiner Institute of Cardiovascular Research, Vienna, Austria
- 4Voet Consulting, Berlin, Germany
- 5Medical Faculty, Sigmund Freud Private University, Vienna, Austria
Objectives: Effective and reliable cardioplegic cardiac arrest is crucial for maximizing myocardial protection and preserving postoperative contractile function. Aim of this study was to demonstrate, in line with an ongoing European registration procedure, the efficacy and safety of the new Cardioplexol™ solution.
Methods: Single-centre, single-blind, randomized, active-controlled phase-3 non-inferiority trial comparing Cardioplexol™ and Buckberg solutions during cardiac surgery. Patients planed for elective CABG, valve surgery and/or aortic root surgery, were considered eligible after meeting all inclusion and exclusion criteria. Peak troponin-T (TnT) during the first 24 h post-reperfusion was defined as primary endpoint. Intraoperative and ICU-related secondary endpoints were also evaluated, as were safety endpoints.
Results: Out of 248 operated patients, 226 (100 Cardioplexol™, 126 Buckberg) were considered for per-protocol analysis. Peak-TnT was similar in both groups (0.77 vs. 0.78 ng/ml) and non-inferiority of Cardioplexol™ was confirmed. Delay before complete cardiac arrest (11 vs. 71 s, p < 0.001) and cross-clamp time (51.2 vs. 60.7 min, p < 0.001) were shorter after Cardioplexol™. The defibrillation rate was also significantly reduced (10% vs. 52%, p < 0.001). Although not statistically significant, cumulative dose of catecholamines within 24 h postreperfusion (6,202 vs. 7,170 µg/kg, p = 0.07), and ICU stay (38.1 vs. 44.0 h, p = 0.110) also appeared reduced after Cardioplexol™. Mortality was lower after Cardioplexol™ (1 pt. vs. 5 pts.). Safety parameters were comparable in both groups.
Conclusion: Efficacy and safety of Cardioplexol™ were demonstrated.
Clinical Trial Registration: https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-004198-10/results, Eudra CT-No: 2011-004198-10.
Introduction
Most cardiac surgery procedures require efficient and reliable cardiac arrest to ensure heart inactivity, while guaranteeing maximal myocardial protection to preserve post-operative contractile function. Several cardioplegic solutions were developed over the last 50 years, such as Buckberg, St-Thomas or Bretschneider solutions (1), most of them being still considered as standard (2–4). Surprisingly, only a handful of cardioplegic solutions are approved by regulatory authorities in some countries. In addition, several centers modify standard solutions or manufacture a customized cardioplegia (5–7). Therefore, even if numerous studies have reported on clinical results obtained with these various solutions, only very few reach a sufficient level of evidence (8).
Cardioplexol™ is a ready-to-use new cardioplegic solution combining four well characterized chemical ingredients at pharmacologically compatible doses. With its low volume (100 ml), the solution was originally conceived to match with the concept of Minimal invasive Extra Corporeal Circulation (MiECC) which consists of a closed circuit operating at reduced and constant volume (9). With experience, it appeared valuable in regular procedures as well. At the time of study preparation, Cardioplexol™ had been used in Bern, Switzerland, in ∼5,000 patients, demonstrating several advantages and no noticeable sideeffect (9–11).
The aim of this pivotal study was therefore to demonstrate, in the context of a European registration procedure, the safety and efficacy of Cardioplexol™.
Patients and methods
Study design
Single-centre, single-blind, randomized, active-controlled phase-3 noninferiority trial investigating the safety and efficacy of Cardioplexol™ during cardiac surgeries performed with a heart-lung machine. The study is part of a national registration procedure in Switzerland and a decentralized procedure (DCP) in Europe (RMS: Austria), and was conducted at the Hospital Hietzing, Vienna, between May-2012 and July-2015.
Study protocol was approved by the Ethics Committee of the City of Vienna (EK-11-191-1011, February 17, 2012) and the Austrian regulatory agencies BASG and AGES. Each patient provided written informed consent preoperatively.
Investigational drug
Cardioplexol™ is a two-component system: vial-A (95 ml) and syringe-B (5 ml). The final 100 ml solution, obtained by injecting the syringe content into the vial, contains potassium-chloride (10.0 mmol), magnesium-sulfate-heptahydrate (16.2 mmol), xylitol (29.6 mmol) and procaine-hydrochloride (1.1 mmol), is hypertonic (850 mosmol) and slightly acidic (pH ∼ 6.0).
Boxes of Cardioplexol™ are kept refrigerated (2–8°C) before use. The final solution is prepared short before use and kept in 2 sterile 50ml-syringes on ice on the instruments' table, ready for injection.
The initial dose of Cardioplexol™ is administered immediately after aortic crossclamping. The surgeon connects the first 50 ml syringe to the cardioplegia cannula, gently aspirates a few ml of blood to check the connection and complete venting of the cannula, then rapidly injects the entire content (5–7 s) into the aortic root. The procedure is immediately repeated with the second syringe. In situations where aortic cross-clamping is likely to last longer than 60 min, a second dose of Cardioplexol™ (50–100 ml) must be administered between 45 and maximal 60 min of cross-clamping. Similarly, if aortic clamping is likely to last longer than 90 respectively 120 min, a third respectively fourth dose (50–100 ml) must be administered after 75 (maximal 90) respectively 105 (maximal 120) minutes of clamping.
Comparative medicine
After consulting Austrian and German drug registration authorities, it was decided to compare Cardioplexol™ with Buckberg blood cardioplegia (12), considered a benchmark (13, 14). Buckberg was supplied by Dr. Franz Köhler Chemie GmbH (Alsbach-Hähnlein, Germany).
Study populations and randomization
Every patient, aged 18–80, with indication for elective CABG and/or valve replacement/repair and/or aortic root surgery, planned to be performed under with ECC, was considered eligible for enrollment. Exclusion criteria: preoperative LVEF < 30%, IABP, catecholamine support, myocardial infarction within 7 days, previous cardiac surgery including pace-maker or ICD, active myocarditis and/or endocarditis, aortic valve insufficiency (severity grade >1), history of atrial fibrillation or neurologic event, known carotid artery disease, HIT, dialysis or pre-operative creatinine >2.0 mg/dl, anti-vitamin K treatment or known hematologic disorder, patient is pregnant or lactating, intravenous drug users, alcohol abusers, prisoners, patients institutionalized or unable to give informed consent.
Following informed consent, at least 24 h prior to surgery, eligible patients were randomly assigned to Cardioplexol™ or Buckberg cardioplegia in a 1:1 ratio. Allocation sequence was correctly concealed using web-based central unrestricted randomization (WebSpirit, 2 mt Inc. Ulm, Germany), stratified according to surgical indication.
Surgical procedure
After usual cardiac exposure and cannulation, a cardioplegia cannula was inserted into the aorta, connected to a three-way valve and de-aired. CPB was started and increased to 100% flow. The ascending aorta was then clamped after checking that cardiac chambers are adequately unloaded. Cardioplegic solution was administered, and the intervention proceeded as usual.
Study endpoints
Post-operative troponin-T (TnT) is considered a suitable parameter that adequately reflects myocardial preservation and effectiveness of cardioplegia (15–17). Therefore, peak value of TnT during the first 24 h following myocardial reperfusion was set as primary endpoint. Values were assessed at 6, 12 and 24 h post reperfusion. Secondary endpoints are listed in Table 1. Safety endpoints included serious and non-serious adverse events and laboratory values.
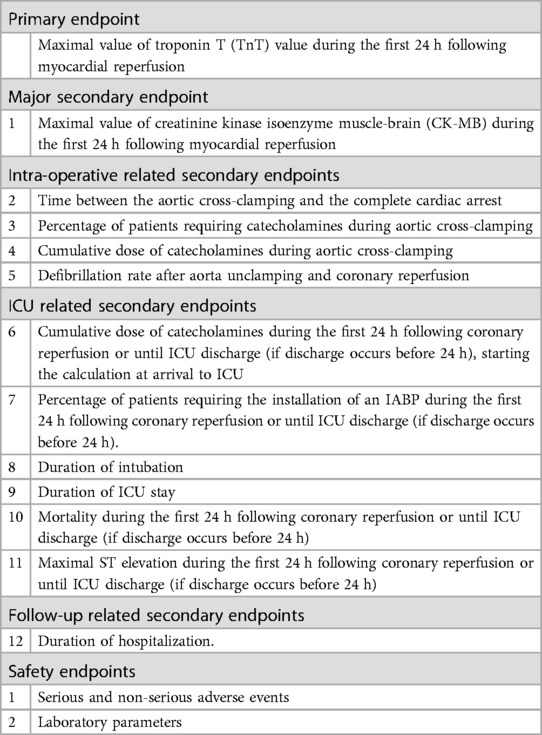
Table 1. Description of primary and secondary endpoints.
Sample size calculation and statistical analysis
Based on a similar population analysis, it was estimated that 260 patients would be required to achieve 240 completed patients. Non-inferiority margin was set at 20% above the value reported for Buckberg solution. The sample size of 120 in each group was sufficient with a 1:1 allocation, a power of 80% and a twosided 95% CI. Cardioplexol™ was considered as non-inferior to Buckberg if the upper boundary of the two-sided 95% CI for the ratio of TnT values was below this margin.
Descriptive statistics are expressed as mean, standard deviation, median and ranges for continuous variables, and frequencies and percentages for categorical variables. All statistical tests were two-sided, and a p-value of <0.05 was considered significant. Log-transformed TnT and CK-MB values were used for statistical analyses. Both groups were assessed using t-test for continuous variables and Fisher's exact test for dichotomous variables.
Analysis sets
- Screening population: All patients who gave informed consent.
- Full-Analysis-Set (FAS): All eligible patients who were operated and received the study treatment.
- Safety population: All patients of the FAS-population.
- Per-Protocol-Set (PPS): All subjects of the FAS-population with non-missing max. TnT values and without protocol deviations.
- Modified-Per-Protocol-Set (mod-PPS): PPS-population with protocol deviations considered clinically irrelevant.
Results
Patient disposition, demographic and pre-operative characteristics
Overall, 280 patients were screened. Fifteen were excluded before randomization (Figure 1): in-/exclusion criteria (n = 13), patient's refusal (n = 1), surgeon's decision to exclude (n = 1).
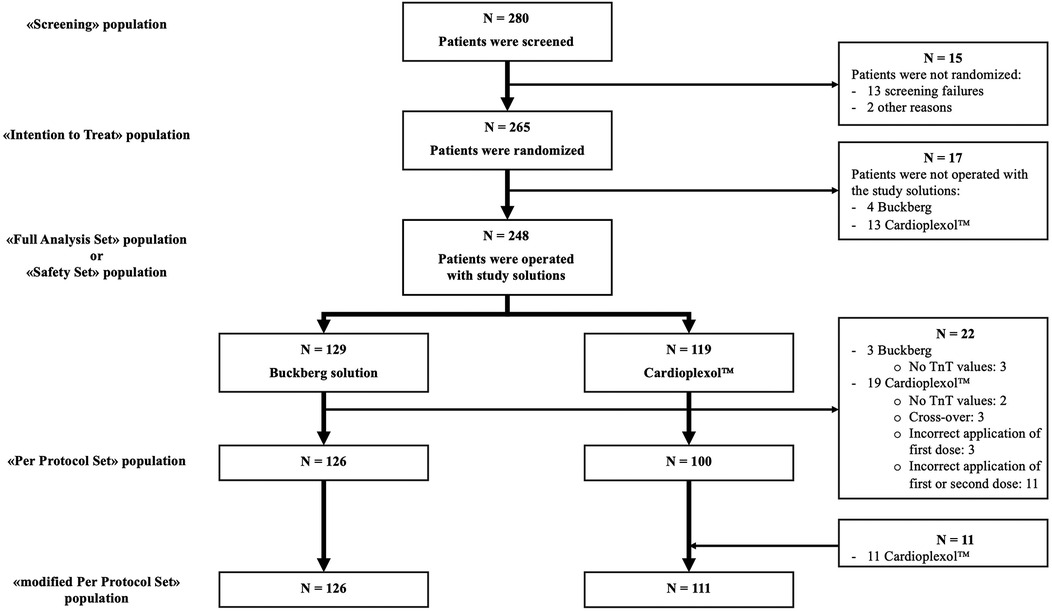
Figure 1. Patients disposition.
Of 265 randomized patients, 17 were not operated (4 Buckberg, 13 Cardioplexol™; Supplementary Appendix 1). Therefore, 248 patients (FAS), were operated and received either Buckberg (n = 129) or Cardioplexol™ (n = 119). Baseline profiles are summarized in Table 2.
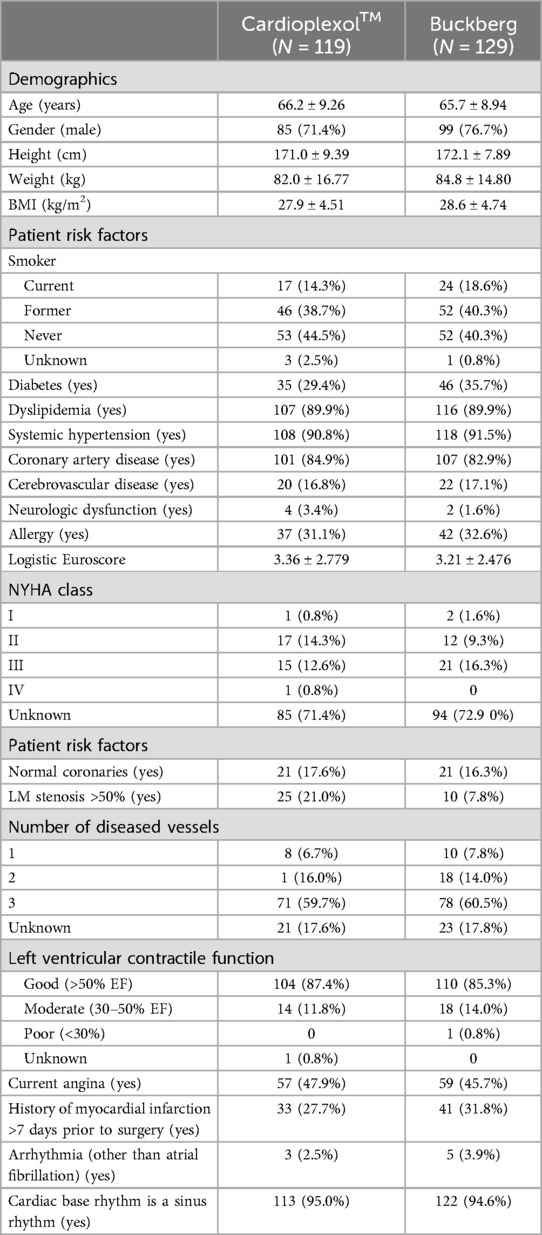
Table 2. Patients’ demographic and pre-operative characteristics (FAS 604 population).
Of these FAS patients, another 22 (3 Buckberg, 19 Cardioplexol™) had to be excluded (5 patients without post-operative TnT value, 3 who received Buckberg's solution in addition to Cardioplexol™, and 14 for whom Cardioplexol™ was not administered according to protocol, Supplementary Appendix 2), resulting in a PPS-population of 226 patients (126 Buckberg, 100 Cardioplexol™).
Modified-PPS-population
The large number of Cardioplexol™ patients excluded from the PPS-population was mainly due to a strict interpretation of the administration protocol, which states that second and third doses of Cardioplexol™ must be administered within a 60- and 90-minute time limit respectively. In nine cases, clamping time exceeded 60 min, without a second dose being administered. Careful analysis (Supplementary Appendix 3) shows, however, that this limit was exceeded by less than 3 min in 5 patients, and less than 10 min in 2 others. For the first 5 patients, corresponding post-operative max.-TnT values were all below 1.0 ng/ml. For longer procedures, TnT values increased progressively. In two other cases, clamping time extended beyond 90 min without a third dose. In a real-life setting, surgeons might regard these times as indicative rather than strict, and minimal deviations would be considered uncritical. Consequently, the 11 patients for whom timing of second or third dose administration was not strictly adhered to were re-entered in a newly defined “mod-PPS” population, thus minimizing differences in patient numbers between Cardioplexol™ (n = 111) and Buckberg (n = 126) groups. Eventually, only eight Cardioplexol™ patients were excluded from mod-PPS: major administration problem (n = 3), cross-over to Buckberg (n = 3), no postoperative TnT values (n = 2).
Surgical characteristics
Types of procedures and surgical caracteristics were comparable between the groups (Table 3). However, ECC- and cross-clamp times were shortened by 67 min among Cardioplexol™ patients and 63% required a single dose. Conversely, Buckberg patients required up to 7 doses. Duration (18.6 ± 19.5 vs. 250.6 ± 78.5 s for the first dose, and 9.9 ± 8.6 vs. 123.6 ± 30.2 s for the second dose) and volume of injections (102.8 ± 13.6 vs. 271.4 ± 73.7 ml for the first dose, and 63.6 ± 22.5 vs. 123.3 ± 42.4 ml for the second dose) were also markedly reduced after Cardioplexol™.
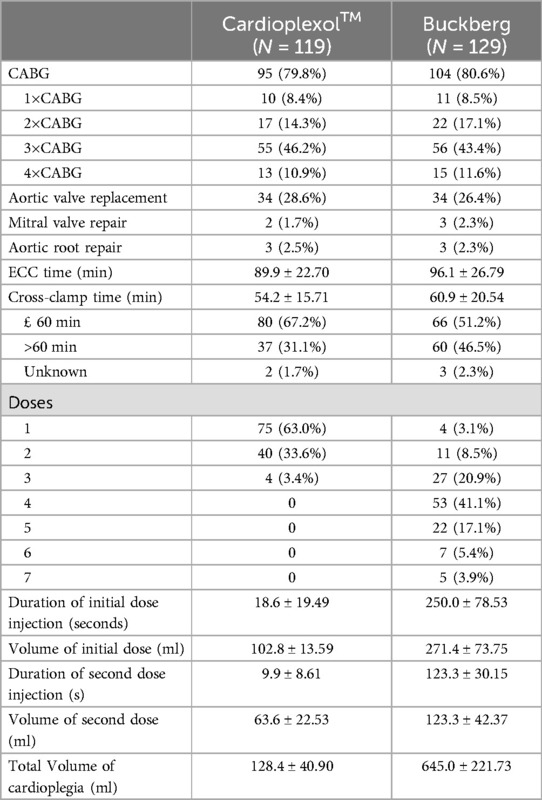
Table 3. Patients’ operative characteristics (FAS population).
Surgeon's influence
Each surgeon included comparable numbers of patients in both groups, except for two who included only 3, respectively 1 patient. Five surgeons included at least 20 patients, whereas 7 including less than 20 (Table 4). Excluded cases and administration errors were equally distributed between participating surgeons.
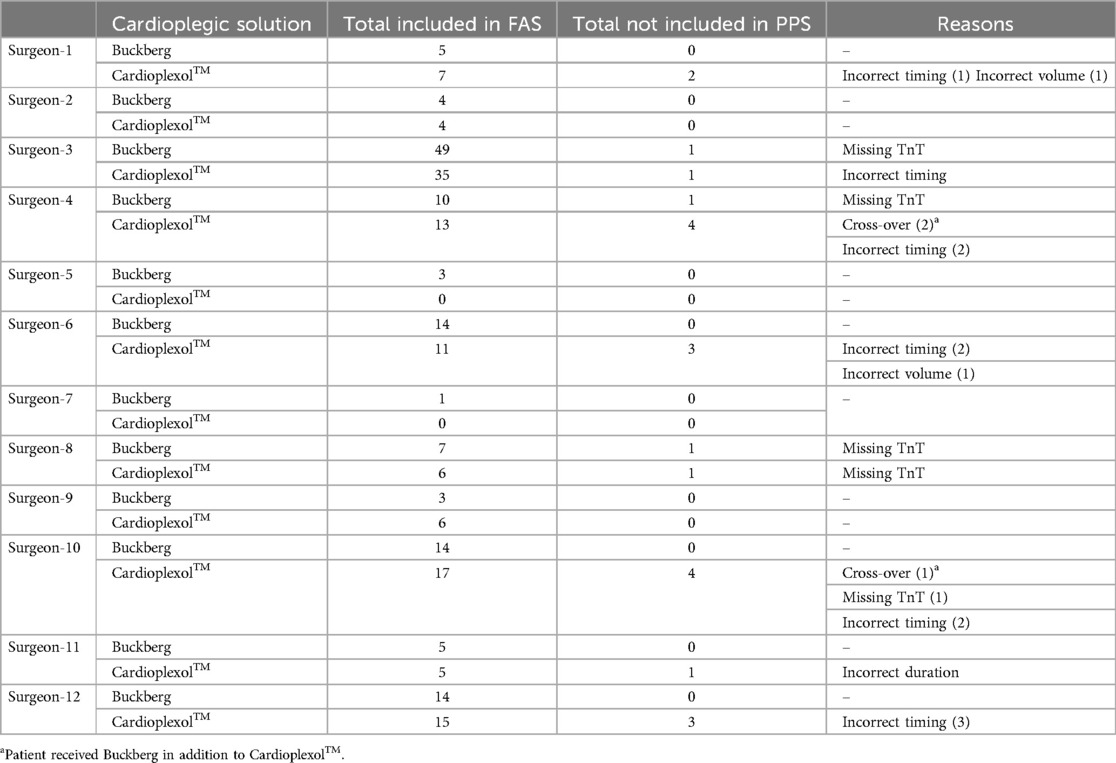
Table 4. Summary of numbers of cases included and excluded by 613 participating surgeons (FAS population).
Of 10 surgeons who operated with both cardioplegia, 5 had lower TnT results with Cardioplexol™, while the other had lower TnT results with Buckberg (Table 5).
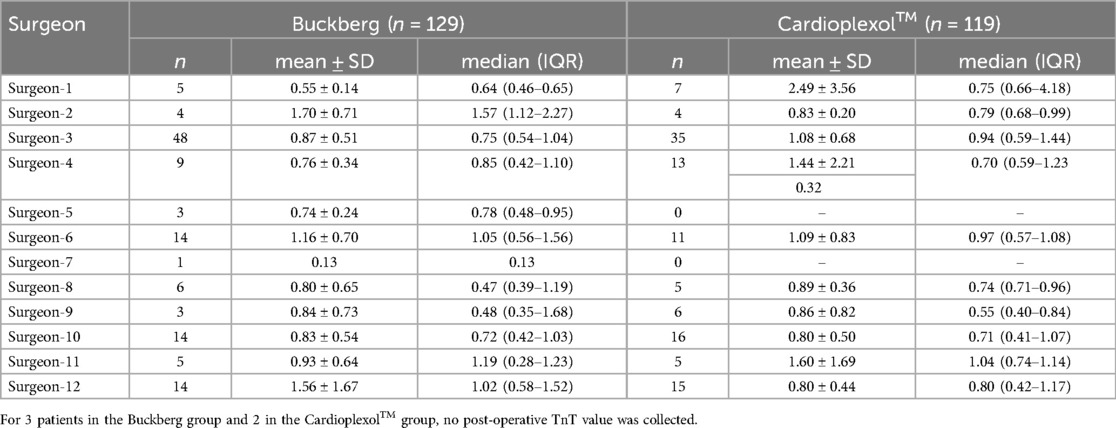
Table 5. Comparison of max. TnT values (ng/ml) obtained by the 12 participating surgeons (FAS population).
Primary endpoint
Results of max.-TnT values are presented in Table 6.1 for FAS-, PPS- and mod-PPS-populations. Values after 6 h of myocardial reperfusion are presented in Table 6.2.
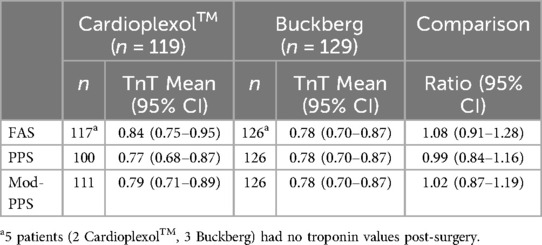
Table 6.1. Non-inferiority analysis of max.-TnT results (ng/ml).
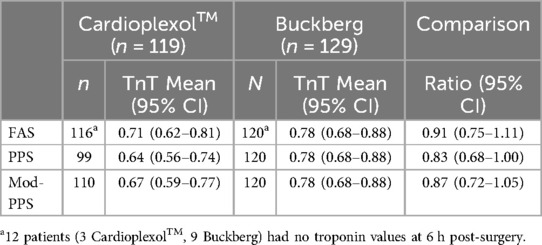
Table 6.2. Non-inferiority analysis of TnT results at 6 h post-reperfusion (ng/ml).
Subgroups were analyzed separately for possible differences by age category (Table 7), gender (Table 8) or type of surgery (Table 9).
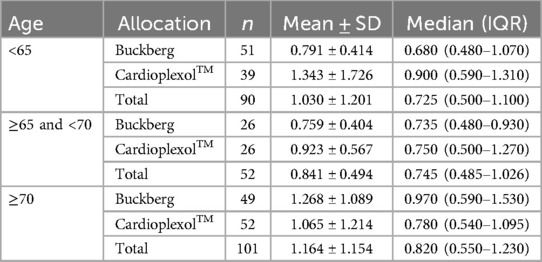
Table 7.1. Comparison of max. TnT values (ng/ml) in various age groups: FAS population.
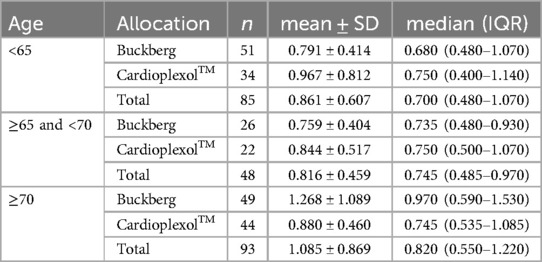
Table 7.2. Comparison of max. TnT values (ng/ml) in various age groups: PPS population.
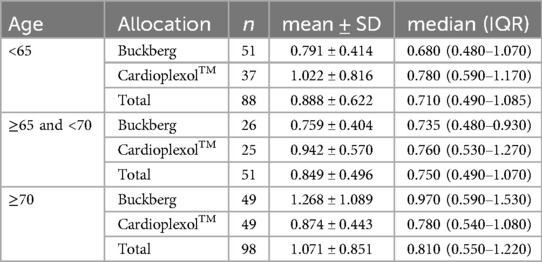
Table 7.3. Comparison of max. TnT values (ng/ml) in various age groups: mod-PPS population.
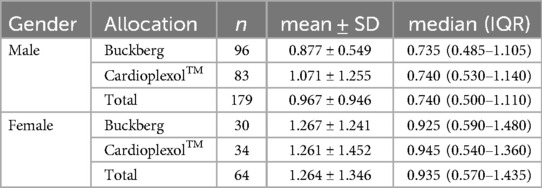
Table 8.1. Comparison of max. TnT values (ng/ml) between genders: FAS population.
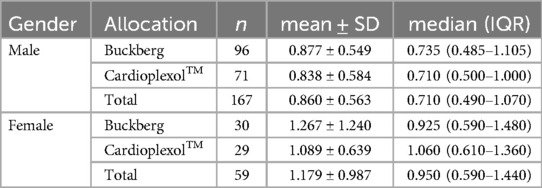
Table 8.2. Comparison of max. TnT values (ng/ml) between genders: PPS population.
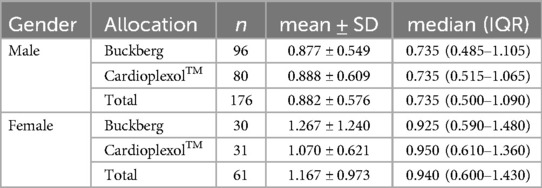
Table 8.3. Comparison of max. TnT values (ng/ml) between genders: mod-PPS population.
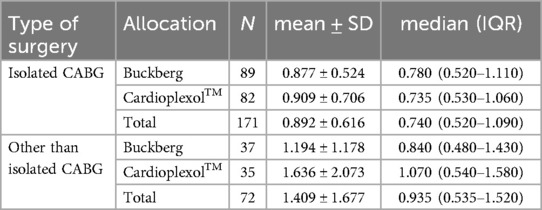
Table 9.1. Comparison of max. TnT values (ng/ml) between types of surgery: FAS population.
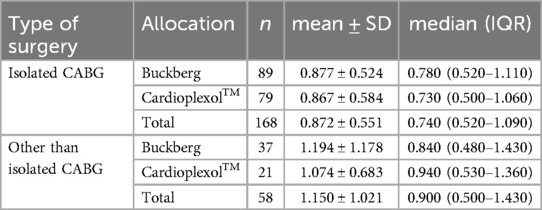
Table 9.2. Comparison of max. TnT values (ng/ml) between types of surgery: PPS population.
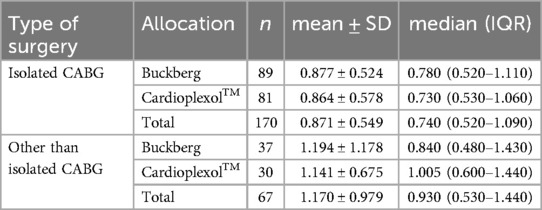
Table 9.3. Comparison of max. TnT values (ng/ml) between types of surgery: mod-PPS population.
Secondary efficacy endpoints
CK-MB results were very similar to those observed for TnT (Table 10). Time between aortic cross-clamping and cardiac arrest was significantly shorter after Cardioplexol™ (p < 0.001). Although not an endpoint, cross-clamp time was shorter after Cardioplexol™ vs. Buckberg (51.2, 95% CI: 24.2–87.2 min vs. 60.7, 95% CI: 18.8–130.0 min; p < 0.001). Other favorable effects of Cardioplexol™: lower rate of defibrillation (10% vs. 52%, p < 0.001), reduced post-operative inotropic support (p < 0.001), and reduction in ICU stay (38.1 vs. 44.0 h, p = 0.110).
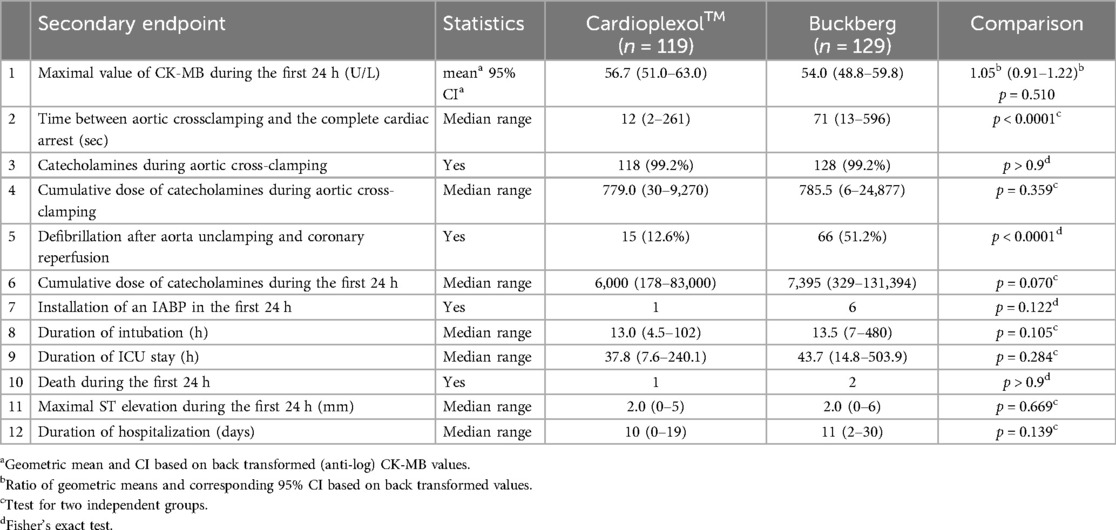
Table 10.1. Results of secondary endpoints: FAS population.
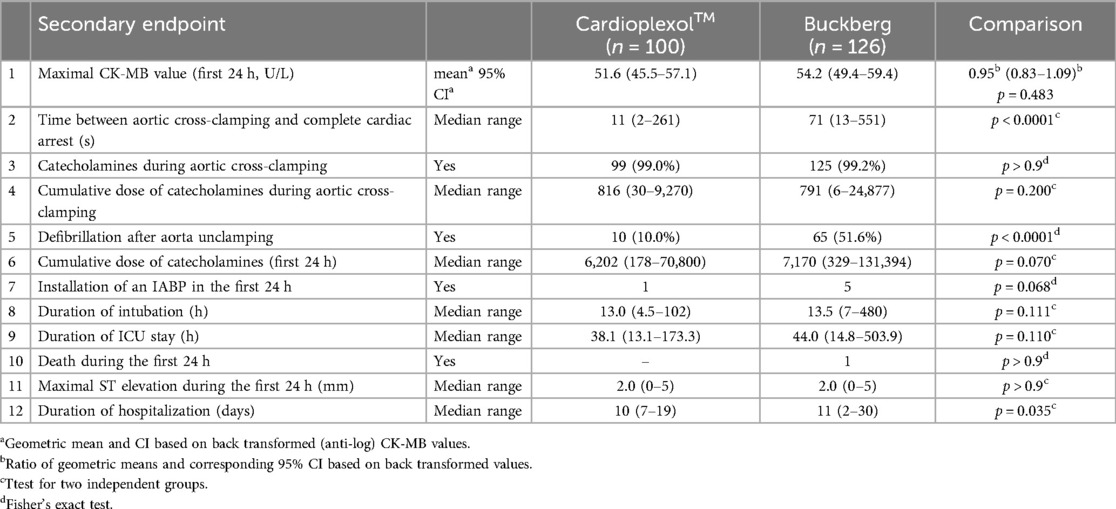
Table 10.2. Results of secondary endpoints: PPS population.
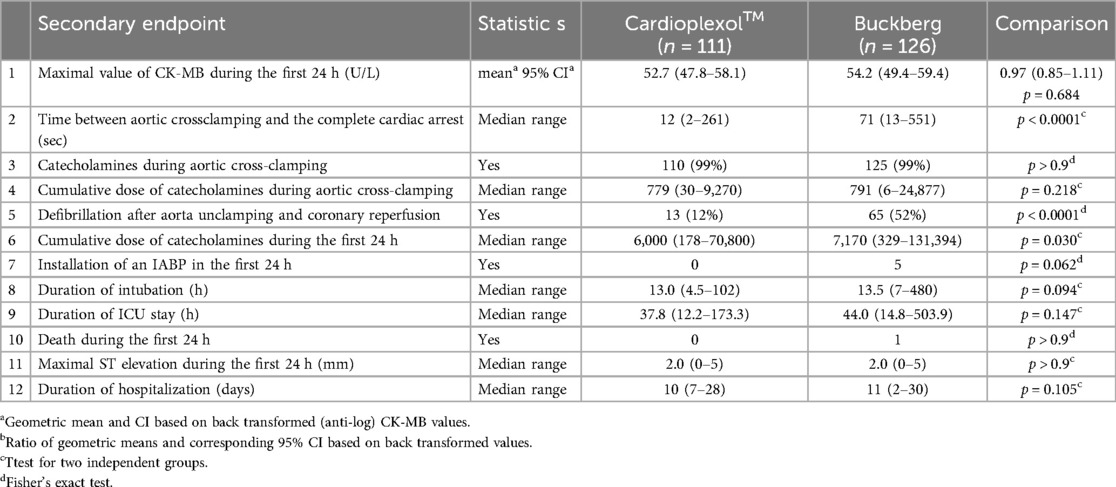
Table 10.3. Results of secondary endpoints: mod-PPS population.
Secondary safety endpoints
Follow-up results at 30 days were comparable between the groups (Table 11) except for mortality (1 Cardioplexol™ vs. 5 Buckberg patients). Adverse events, severity grade and causality are summarized in Supplementary Appendices 4, 5. Number of patients with adverse events was similar in both groups. Number of adverse events was however slightly lower in the Cardioplexol™ group.
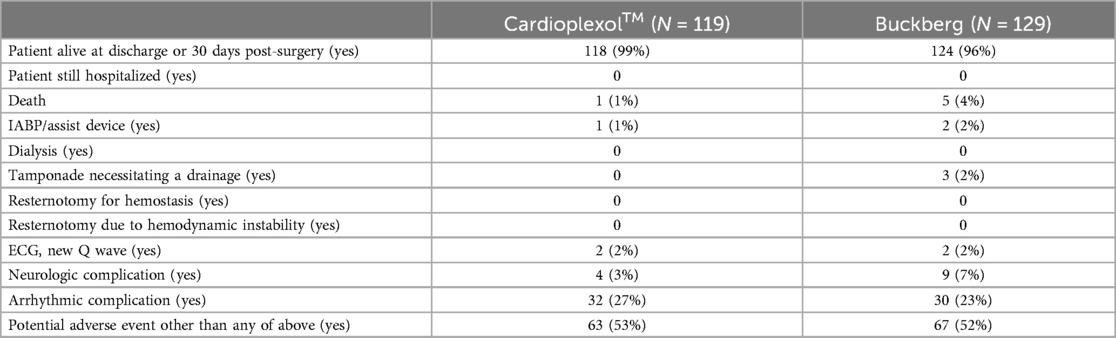
Table 11. Follow-up results at 30 days post-surgery (safety population).
In both groups, pH, lactate, haematocrit, potassium, sodium and calcium values remained in normal ranges during the entire procedure (Table 12). Blood transfusion was deemed necessary in 22% of patients operated on with Cardioplexol™ and 29% of patients operated on with Buckberg.
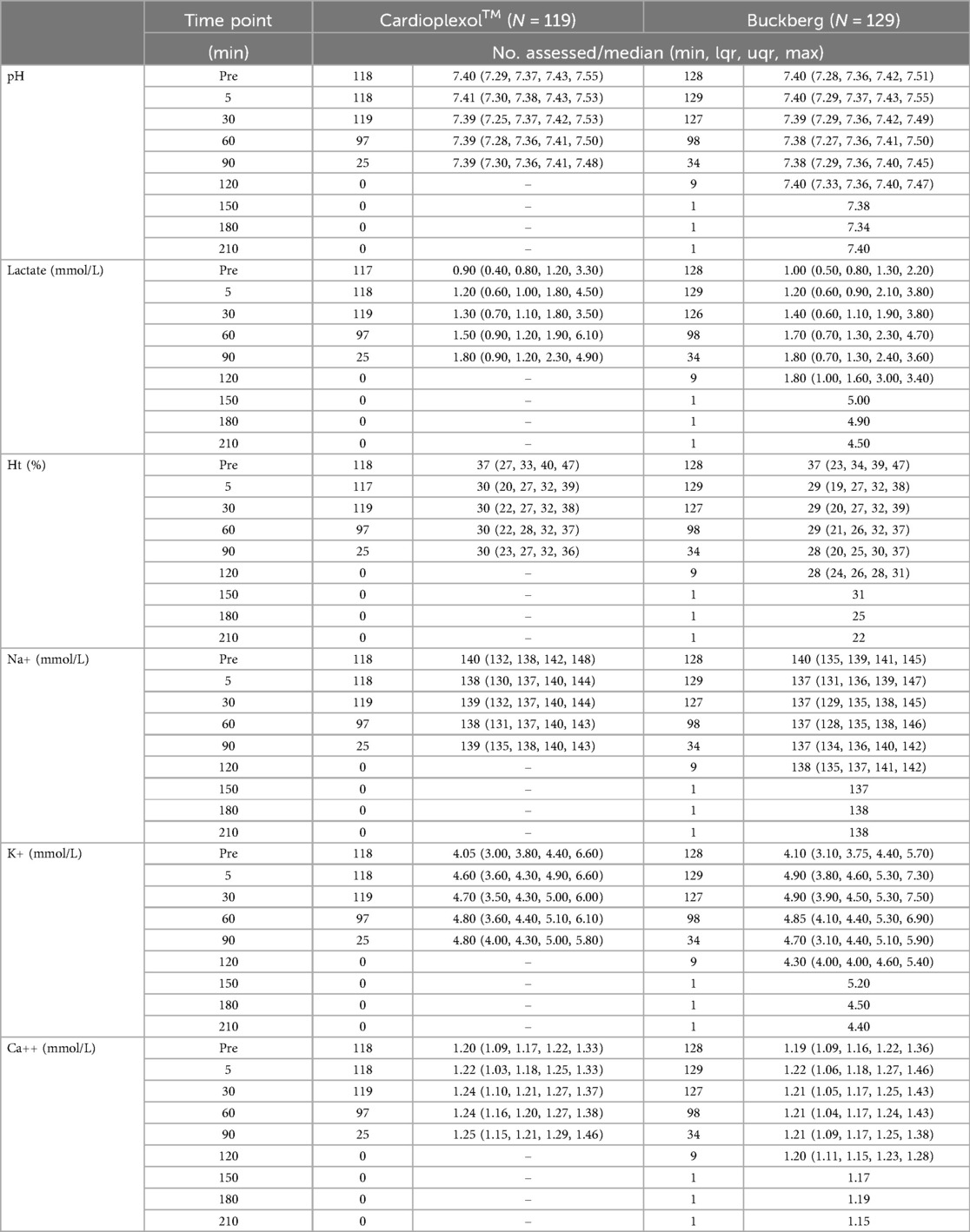
Table 12. Intraoperative blood gas analysis at the specified time after termination of initial cardioplegic infusion/injection (safety population).
Discussion
The current pivotal study aimed at demonstrating the safety and efficacy of Cardioplexol™, a new low volume cardioplegic solution which showed several advantages in previous reports (11, 18). Maximal post-operative TnT values were similar in both the PPS- and mod-PPS-populations, with a non-inferiority margin not exceeding 20% of the Buckberg solution values. In addition, results for all 12 secondary endpoints showed a clear benefit of Cardioplexol™, especially regarding the time between aortic cross-clamping and cardiac arrest, the defibrillation rate following aortic unclamping, the cumulative dose of catecholamines within 24 h, post-operative ICU stay, and length of hospital stay. The study also demonstrated the safety of Cardioplexol™ when used as recommended.
Non-inferiority analysis
From a strictly regulatory standpoint, the recommended approach for noninferiority trials is to perform both FAS and PPS analyses, and to conclude noninferiority only if both give the same results. Since a relevant number of patients had to be excluded, making the PPS-population possibly different from the original FAS-populations, the regulatory authorities argued that a potential bias could have been introduced with consequences on the overall interpretation. However, conditions in the current study need to be put into perspective. Indeed, it is important to carefully assess the relevance of protocol deviations likely to occur in such a trial. Clearly, a population that excludes non-compliant patients (PPS-population), and that properly addresses the impact of these data, is more likely to provide reliable non-inferiority results. Conversely, a population that better matches daily-life scenario (mod-PPS-population), will better reflect clinical reality to be expected once the drug is commercially available. In a real-life scenario, surgeons decide on an individual basis which strategy is most appropriate. This is particularly true for a study such as this one, where a well-established treatment is compared to a new one with which surgeons have no experience so far. For that reason, it was reasonable to expect only minor deviations in the Buckberg group, without effect on the primary endpoint. Accordingly, Buckberg administration was not strictly monitored but left to the surgeon's discretion. In contrast, Cardioplexol™ administration was strictly formulated, and all surgeons received some theoretical training. Protocol violations were recorded in 19 cases. Some may be considered “mild” (missing postoperative TnT values, n = 2; delayed administration of the second/third dose, n = 11), with only little influence on primary endpoint. For 6 patients, reasons for exclusion were more serious with potential major impact on primary endpoint: 3 patients also received Buckberg (cross-over), and 3 patients had serious administration errors: volume too low (85 ml), volume too high (>200 ml), injection too slow (197 s). The mod-PPS population excluded only these later 6 patients.
Primary endpoint
Several studies indicate that postoperative TnT profile correlates well with short-, medium- and even long-term prognosis (16, 19–21). Timing of peak occurrence may reflect different clinical scenarios (22). It typically occurs around 6–8 h post myocardial reperfusion in uncomplicated cardiac surgery procedures (22–30). Conversely, in cases of acute coronary syndrome without coronary reperfusion, the increase in TnT typically extends over 24 h (31). Therefore, post-operative TnT values that keep increasing after 12 or 24 h likely correspond to an event that was not resolved by reperfusion. This might be cardioplegia-related but could also reflect an independent issue (coronary artery occlusion, graft thrombosis, kinking or twist).
Maximum and 6 h reperfusion values seem thus to best reflect quality of cardioplegic protection. Both values are clearly non-inferior as compared to those observed in the Buckberg group.
Secondary endpoints
Although less specific and sensitive than TnT, CK-MB remains a traditional biomarker used to evaluate cardioplegic solutions (32–34). In the present study, CK-MB values appeared similar in both groups.
Other secondary endpoints were selected according to their direct or indirect relationship with clinical outcome. For instance, a rapid cardiac arrest critically limits the metabolic demands of non-perfused heart (35–38) and improves myocardial integrity during the ischemic period. In the present study, cardiac arrest occurred much faster after Cardioplexol™ and the positive consequences was reflected by a significant reduction of ventricular fibrillation after reperfusion, easier conversion (less electrical energy and fewer shocks required; data not shown) and reduced need for post-operative inotropic support. These benefits ultimately led to a reduction in overall ICU length of stay.
The quantity of vasoactive drugs required during the clamping period may reflect hemodynamic changes possibly induced by the cardioplegic solution (32, 34, 39). In present study, an advantage was observed after Cardioplexol™ and can be explained by the small volume, confined to the coronary system. Mortality was assessed at 24 h to better evaluate a possible effect of cardioplegia. Mortality, however, is more commonly assessed at day 30 (4, 33). In present study, only one (Buckberg) patient died within 24 h of surgery (Table 10). At 30-day mortality markedly increased in Buckberg patients but remained low after Cardioplexol™ (Table 11).
Safety aspects
Distribution and severity of adverse events were homogeneous in both groups. Mortality was however lower after Cardioplexol™. Although Cardioplexol™ contains high equivalent of potassium, serum values remained within a normal range. In fact, they were slightly lower than values in the Buckberg group, probably because the low volume of Cardioplexol™ doses remain confined to the coronary system.
A major deviation from the administration protocol was observed in 6 patients, raising questions about the safety of Cardioplexol™ administration. In principle, administration of Cardioplexol™ is straightforward. However, it differs from standard solutions in its limited volume, rapid direct injection by the surgeon himself, immediate cardiac arrest and no need to repeat administration every 20 min. This prompted a complementary clinical study, aimed at validating a clearly structured training program for surgeons with no prior experience of using Cardioplexol™ (40).
Limitations
The present study was monocentric and therefore cannot exclude the possibility of it being non-replicable in other centers. Although most confounding factors were well balanced between study groups, confirmation of findings in other centers would be welcome. Furthermore, surgical indications were varied, and essentially included isolated CABGs, valves procedures or a combination of the two, these accounting for the vast majority of current cardiac surgeries. It is known that the benefit of cardioplegia is not always the same in all cases. In addition, post-operative TnT values are known to slightly differ after CABG vs. valve replacement. However, the aim of this pivotal study was to verify that Cardioplexol™ is generally effective, whatever the indication. An initial sub-analysis confirmed the differences in post-operative TnT max values after isolated CABG vs. any operation other than isolated CABG. However, these results remain similar irrespective of the cardioplegia solution adopted (Table 9). Similarly, there were no notable differences across genders or age groups (Tables 7, 8).
Finally, given that the recruitment period extended to 2015, the presentation of the results of this study appears to be relatively delayed. The data analysis was in fact carried out upon completion of the study and submitted to the registration authorities. The data had also been published on the EU clinical trials register website: https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-004198-10/results. The authorities, however, requested that a new study be conducted before the results of this first study could be validated. Indeed, although it considered that the Cardioplexol™ solution was in itself effective and safe, its administration remained a critical point and an administration error could be harmful. In this context, it was requested that a training protocol for surgeons new to the use of Cardioplexol™ be tested in a new phase 3 study, which would therefore be considered complementary to the present study and would enable a final decision to be made regarding marketing authorization. This study has been carried out (40) and confirms that specific training for surgeons who do not yet have experience with the use of Cardioplexol™ helps to avoid administration errors and consequently increases the safety of this medication.
Conclusion
Safety and efficacy of Cardioplexol™ were confirmed in this pivotal singlecentre, single-blind, randomized Phase-3, non-Inferiority study. Together with the data presented in the supplementary study (40), the results presented here constituted a key part of the European registration dossier. Cardioplexol™ received marketing authorization in Switzerland in September 2023 and in 10 European countries in April 2024.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The studies involving humans were approved by Ethics Committee of the City of Vienna (EK-11-191-1011, February 17, 2012). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HT: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. GW: Data curation, Investigation, Writing – review & editing. PL: Data curation, Project administration, Supervision, Writing – review & editing. SF: Data curation, Investigation, Writing – review & editing. MH: Data curation, Investigation, Writing – review & editing. BV: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – original draft. MG: Investigation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Swiss Cardio Technologies AG.
Acknowledgments
The authors are deeply thankful to Mrs Christiane Chène and team Regenold GmbH (regulatory-related aspects), Mrs Katharina Glaninger and team S2-ScienceSolutions GmbH (monitoring), Mr Joseph Merges and team MITGesundheit GmbH (Pharmacovigilance and Safety aspects), and the Clinical Trial Unit, Bern University. Authors acknowledge the commitment of all participating surgeons, not mentioned as author: Drs. M. Gorlitzer, Heine, R. Moidl, H. Pisarik, P. Poslussny, M. Thalmann, F. Veit, F. Waldenberger. Finally, the authors gratefully acknowledge the contribution of Professors Thierry Carrel and Jürg Schmidli, who provided expert guidance throughout the development phases of Cardioplexol™ and the present study.
Conflict of interest
HTT is inventor of Cardioplexol™, co-founder, and consultant for Swiss-Cardio Technologies AG. BV is statistical consultant for Swiss-Cardio-Technologies AG.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1587713/full#supplementary-material
References
1. Cordell AR. Milestones in the development of cardioplegia. Ann Thorac Surg. (1995) 60:793–6. doi: 10.1016/0003-4975(95)00570-B
2. Ali JM, Miles LF, Abu-Omar Y, Galhardo C, Falter F. Global cardioplegia practices: results from the global cardiopulmonary bypass survey. J Extra Corpor Technol. (2018) 50:83–93. doi: 10.1051/ject/201850083
3. Lohbusch B, Olson K, Magowan B, Cherichella R, Wolverton J, Dell'aiera L, et al. Adult clinical perfusion practice survey: 2020 results. J Extra Corpor Technol. (2023) 55:3–22. doi: 10.1051/ject/2023002
4. Guru V, Omura J, Alghamdi AA, Weisel R, Fremes SE. Is blood superior to crystalloid cardioplegia? A meta-analysis of randomized clinical trials. Circulation. (2006) 114:I-331. doi: 10.1161/CIRCULATIONAHA.105.001644
5. Harvey B, Shann KG, Fitzgerald D, Mejak B, Likosky DS, Puis L, et al. International pediatric perfusion practice: 2011 survey results. J Extra Corpor Technol. (2012) 44:186–93. doi: 10.1051/ject/201244186
6. Kotani Y, Tweddell J, Gruber P, Pizarro C, Austin EH, Woods RK, et al. Current cardioplegia practice in pediatric cardiac surgery: a North American multiinstitutional survey. Ann Thorac Surg. (2013) 96:923–9. doi: 10.1016/j.athoracsur.2013.05.052
7. Drury NE, Horsburgh A, Bi R, Willetts RG, Jones TJ. Cardioplegia practice in paediatric cardiac surgery: a UK & Ireland survey. Perfusion. (2019) 34:125–9. doi: 10.1177/0267659118794343
8. Wahba A, Milojevic M, Boer C, De Domer FMJJ, Gudbajarsson T, van den Goor J, et al. 2019 EACTS/EACTA/EBCP guideline on cardiopulmonary bypass in adult cardiac surgery. Eur J Cardiothorac Surg. (2019) 123:713–57. doi: 10.1093/ejcts/ezz267
9. Immer FF, Ackermann A, Gygax E, Stalder M, Englberger L, Eckstein FS, et al. Minimal extracorporeal circulation is a promising technique for coronary artery bypass grafting. Ann Thorac Surg. (2007) 84:1515–20. doi: 10.1016/j.athoracsur.2007.05.069
10. Goeber V, Hohl A, Gahl B, Dick F, Eigenmann V, Carrel TP, et al. Early troponin T and prediction of potentially correctable in-hospital complications after coronary artery bypass grafting surgery. PLoS One. (2013) 8:e74241. doi: 10.1371/journal.pone.0074241
11. Matt P, Arbeleaz E, Schwirtz G, Doebele T, Eckstein F. Lowvolume, single-shot crystalloid cardioplegia is safe for isolated aortic valve replacement. Thorac Cardiovasc Surg. (2012) 60:360–2. doi: 10.1055/s-00311295565
12. Buckberg GD, Dyson CW, Emerson RC. Techniques for administering blood cardioplegia: blood cardioplegia. In: Engelman RM, Levitsky S, editors. Textbook of Clinical Cardioplegia. Mt. Kisko: Futura (1982). p. 305–16.
13. Robinson LA, Schwarz D, Goddard DB, Fleming WH, Galbraith TA. Myocardial protection for acquired heart disease surgery: results of a national survey. Ann Thorac Surg. (1995) 59:361–72. doi: 10.1016/00034975(94)00869-9
14. Karthik S, Grayson AD, Oo AY, Fabri BM. A survey of current myocardial protection practices during coronary artery bypass grafting. Ann R Coll Surg Engl. (2004) 86:413–5. doi: 10.1308/147870804669
15. Baggish AL, MacGillivray TE, Hoffman W, Newll JB, Lewandrowski KB, Lee-Lewandrowski E, et al. Postoperative troponin-T predicts prolonged intensive care unit length of stay following cardiac surgery. Crit Care Med. (2004) 32:1866–71. doi: 10.1097/01.ccm.0000139692.19371.7c
16. Buse GAL, Koller MT, Grapow M, Bolliger D, Seeberger M, Filipovic M. The prognostic value of troponin release after adult cardiac surgery—a meta-analysis. Eur J Cardiothorac Surg. (2009) 37:399–406. doi: 10.1016/j.ejcts.2009.05.054
17. Mohammed AA, Agnihotri AK, van Kimmenade RRJ, Martinez-Rumayor A, Green SM, UIroz R, et al. Prospective, comprehensive assessment of cardiac troponin T testing after coronary artery bypass graft surgery. Circulation. (2009) 120:843–50. doi: 10.1161/CIRCULATIONAHA.108.837278
18. Stahel HT, Barandun S, Kaufmann E, Gahl B, Englberger L, Jenni H, et al. Single-center experience with the combination of Cardioplexol™ cardioplegia and MiECC for isolated coronary artery bypass graft procedures. J Thorac Dis. (2019) 11:S1471–9. doi: 10.21037/jtd.2019.04.47
19. Domanski MJ, Mahaffey K, Hasselblad V, Brener SJ, Smith PK, Hillis G, et al. Association of myocardial enzyme elevation and survival following coronary artery bypass graft surgery. JAMA. (2011) 305:585–91. doi: 10.1001/jama.2011.99
20. Soraas CL, Friis C, Tunheim Engebretsen KV, Sandvik L, Kjeldsen SE, Tonnessen T. Troponin T is a better predictor than creatinin kinaseMB of long-term mortality after coronary artery bypass graft surgery. Am Heart J. (2012) 164:779–85. doi: 10.1016/j.ahj.2012.05.027
21. Nellipudi JA, Baker RA, Dykes L, Krieg BM, Bennetts JS. Prognostic value of high-sensitivity troponin T after on-pump coronary artery bypass graft surgery. Heart Lung Circ. (2021) 30:1562–9. doi: 10.1016/j.hlc.2021.03.272
22. Tevaearai Stahel HT, Do PD, Klaus JB, Gahl B, Locca D, Goeber V, et al. Clinical relevance of troponin T profile following cardiac surgery. Front Cardiovasc Med. (2018) 5:182. doi: 10.3389/fcvm.2018.00182
23. Carrier M, Pellerin M, Perrault LP, Solymoss BC, Pelletier LC. Troponin levels in patients with myocardial infarction after coronary artery bypass grafting. Ann Thorac Surg. (2000) 69:435–40. doi: 10.1016/s00034975(99)01294-1
24. Lehrke S, Steen H, Sievers HH, Peters H, Optiz A, Müller-Bardorff M, et al. Cardiac troponin T for prediction of short- and long-term morbidity and mortality after elective open heart surgery. Clin Chem. (2004) 50:1560–67. doi: 10.1373/clinchem.2004.031468
25. Januzzi JL, Lewandrowski K, MacGillivray TE, Newell JB, Kathiresan S, Servoss SJ, et al. A comparison of cardiac troponin T and creatine kinase-MB for patient evaluation after cardiac surgery. J Am Coll Cardiol. (2002) 39:1518–23. doi: 10.1016/s0735-1097(02)01789-8
26. van Beek D, van Zaane B, Looije M, Peelen L, van Klei W. Typical rise and fall of troponin in (peri-procedural) myocardial infarction: a systematic review. World J Cardiol. (2016) 8:293–301. doi: 10.4330/wjc.v8.i3.293
27. Cubero-Gallego H, Lorenzo M, Heredia M, Gomez I, Tamayo E. Diagnosis of perioperative myocardial infarction after heart valve surgery with new cut-off point of high-sensitivity troponin T and new electrocardiogram or echocardiogram changes. J Thorac Cardiovasc Surg. (2017) 154:895–903. doi: 10.1016/j.jtcvs.2017.02.013
28. Markman PL, Tantiongco JP, Bennetts JS, Baker RA. Highsensitivity troponin release profile after cardiac surgery. Heart Lung Circ. (2017) 26:833–9. doi: 10.1016/j.hlc.2016.09.017
29. Gahl B, Göber V, Odutayo A, Tevaearai Stahel HT, da Costa BR, Jakob SM, et al. Prognostic value of early postoperative troponin T in patients undergoing coronary artery bypass grafting. J Am Heart Assoc. (2018) 7(5):e007743. doi: 10.1161/JAHA.117.007743
30. Omran H, Deutsch MA, Groezinger E, Zittermann A, Renner A, Neumann JT, et al. High-sensitivity cardiac troponin I after coronary artery bypass grafting for post-operative decision-making. Eur Heart J. (2022) 43:2388–403. doi: 10.1093/eurheartj/ehab918
31. Thielmann M, Massoudy P, Schmermund A, Neuhäuser M, Marggraf G, Kamler M, et al. Diagnostic discrimination between graft-related and non-graft-related perioperative myocardial infarction with cardiac troponin I after coronary artery bypass surgery. Eur Heart J. (2005) 26:2440–7. doi: 10.1093/eurheartj/ehi437
32. Demmy TL, Molina JE, Ward HB, Gorton ME, Kouchoukos NT, Schmaltz RA, et al. Custodiol versus plegisol: a phase 3 multicentre myocardial protection study. Int Angiol. (2008) 17:149–53. doi: 10.1055/s-00311278300
33. Fan Y, Zhang AM, Xiao YB, Weng YG, Hetzer R. Warm versus cold cardioplegia for heart surgery: a meta-analysis. Eur J Cardiothorac Surg. (2010) 37:912–9. doi: 10.1016/j.ejcts.2009.09.030
34. Braathen B, Tønnessen T. Cold blood cardioplegia reduces the increase in cardiac enzyme levels compared with cold crystalloid cardioplegia in patients undergoing aortic valve replacement for isolated aortic stenosis. J Thorac Cardiovasc Surg. (2010) 139:874–80. doi: 10.1016/j.jtcvs.2009.05.036
35. Jennings RB, Murry CE, Steenbergen C, Reimer KA. Development of cell injury in sustained acute ischemia. Circulation. (1990) 82:II2-12.2394018
36. Jennings RB, Reimer KA. The cell biology of acute myocardial ischemia. Annu Rev Med. (1991) 42:225–46. doi: 10.1146/annurev.me.42.020191.001301
37. Dunn RB, Griggs DM. Transmural gradients in ventricular tissue metabolites produced by stopping coronary blood flow in the dog. Circ Res. (1975) 37:438–45. doi: 10.1161/01.res.37.4.438
38. Freedman BM, Pasque MK, Pellom GL, Deaton DW, Frame JR, Wechsler AS. Effects of delay in administration of potassium cardioplegia to the isolated rat heart. Ann Thor Surg. (1984) 37:309–13. doi: 10.1016/s00034975(10)60736-9
39. Minatoya K, Okabayashi H, Shimada I, Tanabe A, Nishina T, Nandate K, et al. Intermittent antegrade warm blood cardioplegia for CABG: extended interval of cardioplegia. Ann Thorac Surg. (2000) 69:74–6. doi: 10.1016/s0003-4975(99)01384-3
Keywords: cardiac surgery, cardioplegic solution, cardioplegia, myocardial protection, extracorporeal circulation, randomized controlled trial
Citation: Tevaearai Stahel HT, Weiss G, Landowski P, Folkmann S, Harrer M, Voet B and Grabenwöger M (2025) Single-centre, single-blind, randomized, active-controlled phase-3 non-inferiority study to investigate the safety and efficacy of the cardioplegic solution Cardioplexol™. Front. Cardiovasc. Med. 12:1587713. doi: 10.3389/fcvm.2025.1587713
Received: 4 March 2025; Accepted: 15 April 2025;
Published: 15 May 2025.
Edited by:
Gianni Angelini, University of Bristol, United KingdomReviewed by:
Suguru Ohira, Westchester Medical Center, United StatesPierpaolo Chivasso, Ospedali Riuniti San Giovanni di Dio e Ruggi d'Aragona, Italy
Copyright: © 2025 Tevaearai Stahel, Weiss, Landowski, Folkmann, Harrer, Voet and Grabenwöger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hendrik T. Tevaearai Stahel, aGVuZHJpay50ZXZhZWFyYWlAZ21haWwuY29t