 Thadzia Maria de Brito Ramos
Thadzia Maria de Brito Ramos José Gildo de Moura Monteiro Júnior*Veridiana Câmara FurtadoDário Celestino Sobral Filho
José Gildo de Moura Monteiro Júnior*Veridiana Câmara FurtadoDário Celestino Sobral Filho
- Pernambuco Cardiac Emergency Hospital, University of Pernambuco (PROCAPE, UPE), Recife, Brazil
Atherosclerosis is the most important etiology of acute myocardial infarction, which is considered an inflammatory disease with specific cellular and molecular responses. Recent research has linked hematological variables as biomarkers of the severity of coronary artery disease. Studies suggest that nucleated red blood cells (NRBCs), neutrophil to lymphocyte ratio (NLR), and mean platelet volume (MPV) may serve as components of a laboratory model or hematological scoring system for in-hospital surveillance. Atherosclerotic plaques can be graded using scoring systems, such as the SYNTAX score which is used to evaluate the complexity of coronary artery disease. However, there is an open field for research to explain the complex inflammatory mechanism of these plaques. Research has shown that inflammatory processes, such as those seen in coronary atherosclerotic disease, stimulate the bone marrow to release young and immature cells into the systemic circulation, which actively aggregate and, consequently, form thrombotic plaques. This mini review article aims to demonstrate the relationship between hematological parameters and coronary angiographic findings as potential in-hospital prognostic tools for patients with acute myocardial infarction. This expressive relationship between these hematological biomarkers and coronary atherosclerotic plaques may be a target, in addition to prognostic scores, of future therapeutic interventions.
1 Introduction
Atherosclerosis is mainly a systemic inflammatory disease, and inflammation plays an important role in the pathophysiology of acute coronary syndrome (1). The inflammatory and hypoxemic etiology of cardiovascular diseases stimulates the bone marrow, leading to an increased production of certain hematological cells or determining the appearance of immature cells (2). Previous works have shown hematological parameters as potential tools for in-hospital follow-up and prognosis of patients with acute myocardial infarction (AMI) (1–3).
In this approach, all major blood count variables were represented: erythroblasts or nucleated red blood cell (NRBC) (red blood cells), neutrophil to lymphocyte ratio (NLR) (white blood cells), and mean platelet volume (MPV) (platelets) to evaluate the role relationship with coronary angiographic lesions (SYNTAX score) (Figure 1).
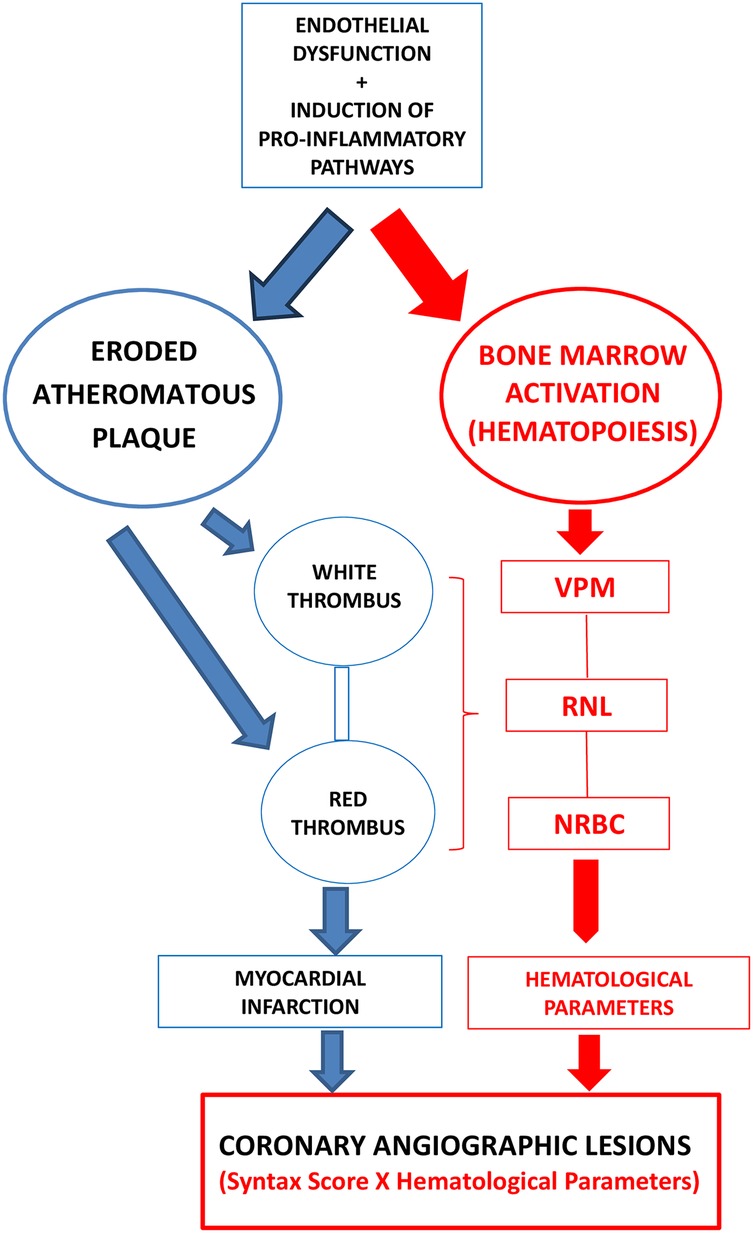
Figure 1. The relationship between atherosclerotic plaque and hematological parameters.
The SYNTAX score is used to verify the extent and severity of coronary artery disease (CAD) and has proven to be a good long-term prognostic marker in different scenarios of coronary artery disease, including patients with acute coronary syndromes (ACS) (4).
The relationship between hematological parameters and anatomical lesions provides new possibilities for hospital monitoring and prognosis of patients with AMI.
2 Hematological parameters
Atherosclerosis is a chronic inflammatory disease involving immune system activation that leads to endothelial dysfunction (5). It is mediated by lipids that induce numerous pro-inflammatory pathways and, together with bone marrow activation, induce myeloid changes, such as synthesis of nucleated red blood cells (NRBCs) and increased neutrophil to lymphocyte ratio (NLR) and mean platelet volume (MPV) in systemic circulation, further contributing to immune cell mobilization and plaque progression (2, 6). Thrombosis superimposed on an eroded or ruptured atherosclerotic plaque is responsible for life-threatening conditions such as acute coronary syndrome and stroke (7). The red thrombus is characterized by a lipid core, plaque rupture, necrotic core, neovascularization, intraplaque hemorrhage, and obstruction (8). Both types of thrombi include platelets and fibrin (9).
Bone marrow produces blood cells, a process called hematopoiesis, which is responsible for the production of red blood cells, leukocytes, and platelets. A single progenitor cell called a stem cell gives rise to all these cells when stimulated by erythropoietin, a glycoprotein produced in 90% of the kidneys, the rest in the liver. Blood exposure to low oxygen concentrations over a long time results in differentiation and increased production of red blood cells (3, 10). Research has shown that hypoxemia and infection trigger differentiation processes into distinct hematological cell lineages (10, 11).
2.1 Nucleated red blood cells
Nucleated red blood cells (NRBCs) are immature erythrocyte cells found in the bone marrow, normally in the peripheral blood of newborns for a few days, but not in adults. Its continuity in the peripheral circulation for children and adults is related to severe hypoxemia and/or infection when hematological diseases, cancer, congestive heart failure, acute and chronic anemias are excluded (12, 13). The presence of NRBCs in the peripheral circulation is associated with high concentrations of erythropoietin, interleukin-3, and interleukin-6 and a worse prognosis (12). Several studies suggest that the detection of NRBCs in hospitalized patients indicates an increased risk of mortality (14).
2.2 Neutrophil to lymphocyte ratio
The neutrophil to lymphocyte ratio (NLR) is composed of two independent markers of inflammation (15). Lymphocytes play an important role in the inflammatory response. Lymphopenia has been linked to progressive atherosclerosis in clinical studies (16). Research has shown an association between NLR and the severity and extent of coronary disease (17, 18). However, studies have disclosed a strong predictor of short- and long-term mortality in stable and unstable coronary diseases. Azab et al. (19) demonstrated that patients with non-ST-segment elevation myocardial infarction (NSTEMI) with NLR > 4.7 have a mortality rate of 29.8% compared with those with NLR < 3, with a mortality rate of 8.4% (p < 0.001).
Studies have shown that higher NLRs are related to a higher SYNTAX score in patients with non-ST-segment elevation acute coronary syndrome and higher numbers of involved coronaries (20, 21). In patients with unstable angina pectoris, NLR proved to be an independent predictor of cardiovascular mortality (22). Kaplangoray et al. (23) published that coronary thrombotic burden correlates with the neutrophil to lymphocyte ratio (r = 0.335, p < 0.001) and SYNTAX score (r = 0.351, p = 0.001).
Individuals with drug-eluting stent restenosis (ISR) are more likely to experience serious adverse cardiac events. Patients with higher NLR had higher SYNTAX scores II and greater proportions of vulnerable components of atherosclerotic plaques, demonstrating that NLR is a risk factor for in-stent restenosis (ISR) (24).
2.3 Mean platelet volume
The mean platelet volume (MPV) represents large platelets, which are metabolically and enzymatically more active than small platelets, with an important role in the extension of intravascular thrombus (25). Uysal et al. (26) showed in their study that the value of the MPV above 10.4 is a predictor of severe atherosclerosis with a sensitivity of 39% and specificity of 90% (ROC curve: 0.631, 95% CI: 0.549–0.708, p = 0.003). Therefore, MPV has been appointed as an independent risk factor for acute myocardial infarction in patients with coronary artery disease (27, 28). Studies have shown a positive correlation between VPM and SYNTAX score (29, 30).
2.4 Hematological score
The hematological score is composed of nucleated red blood cells (NRBC), mean platelet volume (MPV), and neutrophil to lymphocyte ratio (NLR), which represent the constituents of the blood count and whose changes are associated with all causes of hypoxemia and inflammation during hospitalization of patients with acute myocardial infarction. This scoring system was developed to monitor these variables, serving as a prognostic parameter. This hematological score, on a scale ranging from 0 to 49, has been shown to be associated with an increased risk of mortality (sensitivity of 89.1%, specificity 67.2%, negative predictive value of 97.9%, positive predictive value of 26.8% and area under the ROC curve of 86.8%). This work was published in 2020 by our research group, but still needs validation (2).
3 Angiographic lesions
The coronary angiographic lesions are classified by considering a scoring system, which is a tool for grading the complexity of coronary artery disease (31, 32). It specifies information on location, characteristics, tortuosity, and other factors for each lesion, which allowed the online calculator and a Kaplan–Meier curve to show what the cumulative event rate would have been for a patient at a similar risk level in the SYNTAX trial (33, 34). This score classifies coronary lesions into low SYNTAX score (0–22 points), intermediate (23–32 points), and high (≥33 points). Patients with low scores are ideal for percutaneous coronary intervention (PCI), while those with an intermediate or high SYNTAX score are preferentially eligible for surgery (34). Özmen et al. (35) demonstrated a significant relationship between the SYNTAX score and patients with diabetes mellitus.
3.1 SYNTAX score
The SYNTAX score originated from the work published by Patrick Serruys's group in 2009, which compared surgical revascularization with angioplasty using the first-generation Taxus drug-eluting stent (Boston Scientific, USA) in patients with a multi-arterial lesion pattern. The study was non-inferiority, and what was seen is that the primary outcome (death from any cause, stroke, myocardial infarction, or repeated revascularization) was more common in the angioplasty group (17.8% × 12.4%, p = 0.002). Mortality and infarction were similar in 1 year, and the surgical group experienced a higher incidence of stroke. Therefore, the SYNTAX score is an angiographic severity score of coronary lesions, assessing the difficulty and chance of success of the percutaneous intervention (PCI) (31).
3.2 SYNTAX score II
However, a second version (SYNTAX score II) was shown by Bo Xu's group in 2014, which consisted of adding clinical variables, which enlarged its performance in predicting mortality. The study examined 1,528 patients who underwent angioplasty of the unprotected left main coronary artery. The primary outcome was the ability of SYNTAX score II to predict mortality. Patients were divided into three tertiles: ≤21 points with 508 patients, >21 and ≤28 points with 480 patients, and >28 points with 540 patients. Those in the highest tertile were older, were more likely to be female, had a higher prevalence of prior heart attack and stroke, lower ejection fraction, reduced creatinine clearance, and more extensive coronary disease with complex lesions involving two or three vessels. At the 4-year follow-up, the rates of death, cardiac death, myocardial infarction, and target vessel revascularization were 4.4%, 5%, 7.5%, and 9.5%, respectively, which were significantly higher in the highest and intermediate tertiles. In the multivariate analysis, the SYNTAX score II was associated with an increased mortality rate (HR = 1.76, 95% CI: 1.1–2.82, p = 0.02) in patients receiving angioplasty in the unprotected main left coronary artery. The results suggest that SYNTAX score II has greater power to predict mortality compared with the classic SYNTAX angiographic score (36).
4 Hematological parameters and angiographic lesions
The relationship between hematological parameters and angiographic lesions is quite evident in studies published in the literature, especially the neutrophil to lymphocyte ratio and mean platelet volume (Table 1). However, there are still no studies evaluating the relationship between erythroblasts and angiographic lesions.
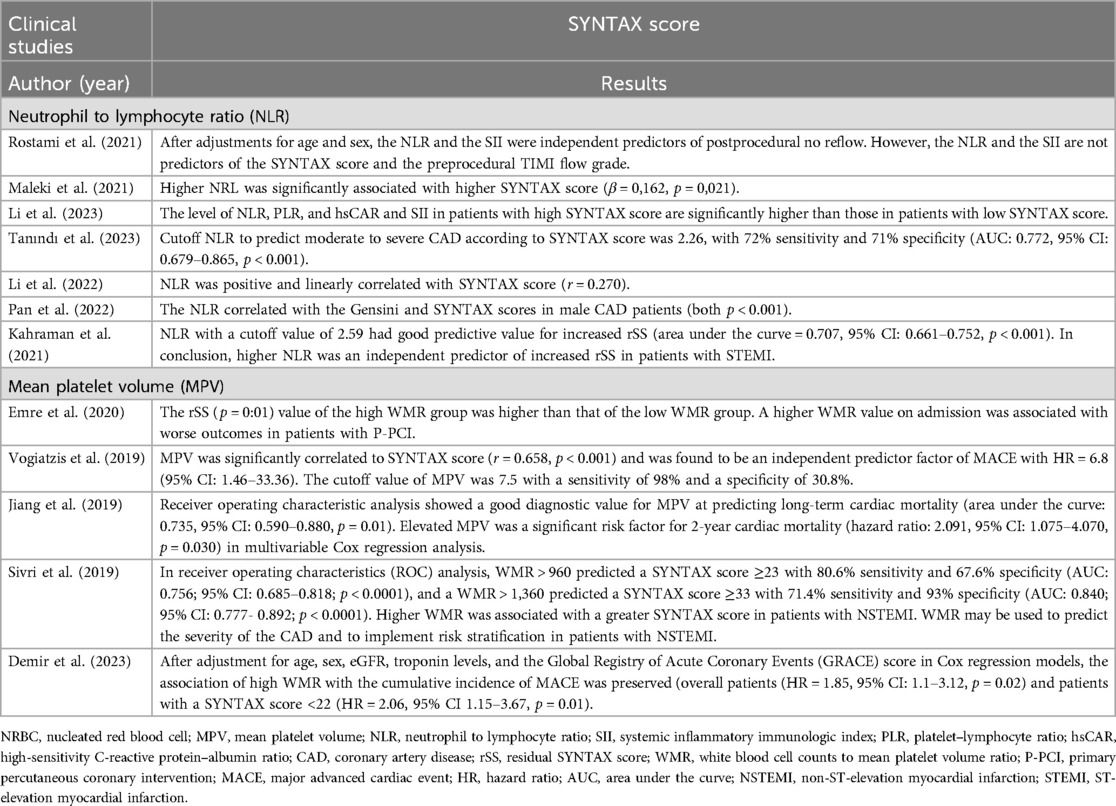
Table 1. Hematological parameters and SYNTAX score in clinical studies.
Prospective cohort study by Rostami et al. (37) included the SYNTAX score and the TIMI flow grade before and after primary percutaneous coronary intervention (pPCI), describing the NLR as an independent predictor of postprocedural no reflow, but not a predictor of the SYNTAX score and the preprocedural TIMI flow grade in patients with ST-segment elevation myocardial infarction (STEMI). However, Maleki et al. (20) demonstrated that higher NLR was significantly associated with higher SYNTAX score (β = 0.162, p = 0.021), and with the same conclusion, Li et al' (22) described that the level of NLR, among other variables, in patients with high SYNTAX score is significantly higher than that in patients with the low SYNTAX score. Zuin et al. (38) demonstrated that the NLR significantly correlated with SYNTAX score with 1-year cardiovascular mortality in patients with ST-segment elevation myocardial infarction (STEMI) or non-ST-segment elevation myocardial infarction (NSTEMI) treated with percutaneous coronary intervention (PCI) within 24 h (OR = 2.85, 95% CI: 1.54–5.26, p = 0.001 and OR = 2.57, 95% CI: 1.62–4.07, p < 0.0001 for STEMI and NSTEMI, respectively). Kurtul et al. (39) demonstrated that NLR was significantly lower in patients with a low SYNTAX score compared with that in patients with an intermediate or high SYNTAX score (3.7 ± 4–4.6 ± 2 and 7.9 ± 4, p < 0.001), and linear regression analysis revealed that NLR (coefficient β = 0.380, 95% CI: 1.165–1.917, p < 0.001) was significantly associated with the SYNTAX score in patients with NSTEMI.
The residual SYNTAX score (rSS) is used to determine the severity of obstructive coronary atherosclerosis after initial PCI, and in multivariate logistic regression analysis, the NLR was an independent predictor of high rSS (OR = 3.933; 95% CI: 2.419–6.393; p < 0.001) (40). Highly sensitive troponin T and NLR were significantly correlated with angiographic severity of acute coronary syndromes (ACS) assessed by SYNTAX score (41). Therefore, many studies have demonstrated the relationship between NLR and the severity of coronary angiographic lesions represented by the SYNTAX score (42–49).
Previous studies have demonstrated the importance of the participation of mean platelet volume (MPV) as a biomarker of coronary atherosclerotic plaque instability and, consequently, in the relationship with angiographic lesions (SYNTAX score). Vogiatzis et al. (29) described that mean platelet volume (MPV) is a primary indicator of platelet activation. It was significantly correlated to SYNTAX score (r = 0.658, p < 0.001) and was found to be an independent predictor factor of major advanced cardiac event (MACE) with HR = 6.8 (95% CI: 1.46–33.36). Sahin et al. (50) demonstrated that the association with the extent and complexity of coronary artery disease in diabetic patients with ST-elevation myocardial infarction (STEMI) was stronger than that in non-diabetic STEMI patients (r = 0.473, p < 0.001 vs. r = 0.129, p = 0.001). A recent study by Abalı et al. (51) described the relationship between MVP and the severity of coronary atherosclerosis in patients with diabetes mellitus, and they found that MPV has a positive correlation with the SYNTAX score. Ekici et al. (52) were quite categorical in clarifying that a positive correlation between MPV and SYNTAX score (p < 0.001, r = 0.504).
Therefore, numerous studies have explored the relationship between these hematological variables (NLR and MPV) with the SYNTAX score (53–55). However, there is limited research examining the nucleated red blood cells (NRBC) with a biomarker in relation to the SYNTAX score. These biomarkers may have great applicability in clinical practice.
5 Discussion
Hematological variables (NRBC, NLR, and MPV), representing the entire spectrum of blood counts in the peripheral circulation, are associated with inflammation and hypoxemia. Coronary angiographic lesions have eminently inflammatory and hematological components, suggesting a likely association between the severity of coronary atherosclerotic plaques (SYNTAX score) and hematological variables. There is substantial evidence in the literature supporting the relationship between mean platelet volume and neutrophil to lymphocyte ratio with coronary angiographic lesions (SYNTAX score), which has not yet been demonstrated with the nucleated red blood cells (NRBC).
These hematological parameters (NRBC, MPV, NLR) have shown potential as valuable tools for in-hospital surveillance of all-cause mortality in patients hospitalized with acute myocardial infarction. However, there is a need for further studies to demonstrate the relationship between these hematological variables and coronary angiographic lesions. In addition to being easy to measure and low-cost, they could serve as useful components of a prognostic scoring system.
Author contributions
TR: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. JM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. VF: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. DS: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de nível Superior (CAPES), Brasil.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Babes EE, Zaha DC, Tit DM, Nechifor AC, Bungau S, Andronie-Cioara FL, et al. Value of hematological and coagulation parameters as prognostic factors in acute coronary syndromes. Diagnostics (Basel). (2021) 11(5):850. doi: 10.3390/diagnostics11050858
2. Monteiro Junior JGM, Torres DOC, Silva MCFC, Príncipe TRN, Vasconcelos RB, Brito MEC, et al. Performance of a hematological scoring system in predicting all-cause mortality in patients with acute myocardial infarction. Int J Cardiovasc Sci. (2020) 33(4):380–8. doi: 10.36660/ijcs.20190094
3. Monteiro Junior JGM, Torres DOC, Filho SD. Hematological parameters as prognostic biomarkers in patients with cardiovascular diseases. Curr Cardiol Rev. (2019) 15(4):274–82. doi: 10.2174/1573403X15666190225123544
4. Viana MS, Correia VCA, Ferreira FM, Lacerda YF, Bragano GO, Fonseca LL, et al. Competência prognóstica distinta entre modelo clínico e anatômico em síndromes coronarianas agudas: comparação por tipo de desfecho. Arq Bras de Cardiol. (2020) 115(2):226–8. doi: 10.36660/abc.20190062
5. Libby P, Buring JE, Badimon L, Hansson GK, Deanfield J, Bittencourt MS. Atherosclerosis. Nat Rev Dis Prim. (2019) 5:56. doi: 10.1038/s41572-019-0106-z
6. Kraaijenhof JM, Hovingh GK, Stroes ES, Kroon J. The iterative lipid impact on inflammation in atherosclerosis. Curr Opin Lipidol. (2021) 32(5):286–92. doi: 10.1097/MOL.0000000000000779
7. Chiorescu RM, Mocan M, Inceu AI, Buda AP, Blendea D, Vlaicu SI. Vulnerable atherosclerotic plaque: is there a molecular signature? Int J Mol Sci. (2022) 23(21):13638. doi: 10.3390/ijms232113638
8. Tosun H, Kamışlı S, Tecellioğlu M, Alan S, Tecellioğlu FS, Öztanır MN, et al. Red and white thrombus characteristics in patients undergoing carotid endarterectomy. J Stroke Cerebrovasc Dis. (2021) 30(2):105451. doi: 10.1016/j.jstrokecerebrovasdis.2020.105451
9. Asada Y, Yamashita A, Sato Y, Hatakeyama K. Pathophysiology of atherothrombosis: mechanisms of thrombus formation on disrupted atherosclerotic plaques. Pathol Int. (2020) 70(6):309–22. doi: 10.1111/pin.12921
10. Guyton AC, Hall JE. Textbook of Medical Physiology. 11th ed. Rio de Janeiro: Elsevier Editora Ltda (2006). ISBN 978-85-352-1641-7; 32: 419-28; 33: 429-38; 36: 457- 68.
11. Monteiro Junior JGM, Sobral Filho DC. Potential role of hematological parameters in patients with acute myocardial infarction: viewpoint. Int J Cardiovasc Sci. (2020) 33(5):586–8. doi: 10.36660/ijcs.20200108
12. Stachon A, Sebbers E, Holland-Letz T, Kempf R, Herinf S, Krieg M. Nucleated red blood cells in the blood of medical intensive care patients indicate increased mortality risk: a prospective cohort study. Crit Care. (2007) 11(3):R62. doi: 10.1186/cc5932
13. Kuert S, Holland-Letz T, Friese J, Stachon A. Association of nucleated red blood cells in blood and arterial oxygen partial tension. Clin Chem Lab Med. (2011) 49(2):257–63. doi: 10.1515/CCLM.2011.041
14. Desai S, Jones SL, Turner KL, Hall J, Moore LJ. Nucleated red blood cells are associated with a higher mortality rate in patients with surgical sepsis. Surg Infect (Larchmt). (2012) 13(6):360–5. doi: 10.1089/sur.2011.089
15. Yalcinkaya E, Yuksel UC, Celik M, Kabul HK, Barcin C, Gokoglan Y, et al. Relationship between the neutrophil/lymphocyte ratio and electrocardiographic ischemia grade in the STEMI. Arq Bras Cardiol. (2015) 104(2):112–9. doi: 10.5935/abc.20140179
16. Núñez J, Núñez E, Bodí V, Sanchis J, Mainar L, Miñana G, et al. Low lymphocyte count in acute phase of ST-segment elevation myocardial infarction predicts long-term recurrent myocardial infarction. Coronary Artery Dis. (2010) 21:1–7. doi: 10.1097/mca.0b013e328332ee15
17. Kaya H, Ertaş F, İslamoğlu Y, Kaya Z, Atılgan ZA, Çil H, et al. Association between neutrophil to lymphocyte ratio and severity of coronary artery disease. Clin Appl Thromb Hemost. (2014) 20(1):50–4. doi: 10.1177/1076029613499821
18. Verdoia M, Barbieri L, Di Giovine G, Marino P, Suryapranata H, De Luca G. Neutrophil to lymphocyte ratio and the extent of coronary artery disease: results from a large cohort study. Angiology. (2016) 67(1):75–82. doi: 10.1177/0003319715577529
19. Azab B, Zaher M, Weiserbs KF, Torbey E, Lacossiere K, Gaddam S, et al. Usefulness of neutrophil to lymphocyte ratio in predicting short and long-term mortality after non-ST elevation myocardial infarction. Am J Cardiol. (2010) 106(4):470–6. doi: 10.1016/j.amjcard.2010.03.06
20. Maleki M, Tajlil A, Separham A, Sohrabi B, Pourafkari L, Roshanravan N, et al. Association of neutrophil to lymphocyte ratio (NLR) with angiographic SYNTAX score in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS). J Cardiovasc Thorac Res. (2021) 13(3):216–21. doi: 10.34172/jcvtr.2021.40
21. Shahsanaei F, Abbaszadeh S, Behrooj S, Rahimi Petrudi N, Ramezani B. The value of neutrophil-to-lymphocyte ratio in predicting severity of coronary involvement and long-term outcome of percutaneous coronary intervention in patients with acute coronary syndrome: a systematic review and meta-analysis. Egypt Heart J. (2024) 76(1):39. doi: 10.1186/s43044-024-00469-3
22. Li S, Chen H, Zhou L, Cui H, Liang S, Li H. Neutrophil-to-lymphocyte ratio predicts coronary artery lesion severity and long-term cardiovascular mortality in patients with unstable angina pectoris. Acta Cardiol. (2022) 77(8):708–15. doi: 10.1080/00015385.2021.1963564
23. Kaplangoray M, Toprak K, Aslan R, Deveci E, Gunes A, Ardahanli İ. High CRP-albumin ratio is associated with high thrombus burden in patients with newly diagnosed STEMI. Medicine (Baltimore). (2023) 102(41):e35363. doi: 10.1097/MD.0000000000035363
24. Yu M, Wang Y, Yang S, Mei J, Liu Z, Zhang L, et al. Elucidating the relationship between neutrophil-lymphocyte ratio and plaque composition in patients with drug-eluting stent restenosis by virtual histology-intravascular ultrasound. J Cardiovasc Dev Dis. (2024) 11(7):211. doi: 10.3390/jcdd11070211
25. Wendland AE, Farias MG, Manfroi WC. Volume plaquetário médio e doenca cardiovascular. J Bras Patol Med Lab. (2009) 45(5):371–8. doi: 10.1590/S1676-24442009000500005
26. Uysal HB, Dağlı B, Akgüllü C, Avcil M, Zencir C, Ayhan M, et al. Blood count parameters can predict the severity of coronary artery disease. Korean J Intern Med. (2016) 31:1093–100. doi: 10.3904/kjim.2015.199
27. Murat SN, Duran M, Kalay N, Gunebakmaz O, Akpek M, Doger C, et al. Relation between mean platelet volume and severity of atherosclerosis in patients with acute coronary syndromes. Angiology. (2013) 64(2):131–6. doi: 10.1177/0003319711436247
28. Klovaite J, Benn M, Yazdanyar S, Nordestgaard BG. High platelet volume and increased risk of myocardial infarction: 39,531 participants from the general population. J Thromb Hemost. (2011) 9(1):49–56. doi: 10.1111/j.1538-7836.2010.04110.x
29. Vogiatzis I, Samaras A, Grigoriadis S, Sdogkos E, Koutsampasopoulos K, Bostanitis I. The mean platelet volume in the prognosis of coronary artery disease severity and risk stratification of acute coronary syndromes. Med Arch. (2019) 73(2):76–80. doi: 10.5455/medarh.2019.73.76-80
30. Vukicevic P, Klisic A, Neskovic V, Babic L, Mikic A, Bogavac-Stanojevic N, et al. New markers of platelet activation and reactivity and oxidative stress parameters in patients undergoing coronary artery bypass grafting. Oxid Med Cell Longev. (2021) 2021:8915253. doi: 10.1155/2021/8915253
31. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. (2009) 360(10):961–72. doi: 10.1056/NEJMoa0804626
32. Chakrabarti AK, Gibson CM. The SYNTAX score: usefulness, limitations, and future directions. J Invasive Cardiol. (2011) 23(12):511–2. https://www.hmpgloballearningnetwork.com/site/jic/articles/syntax-score-usefulness-limitations-and-future-directions22147398
33. Wood S. Syntax Tool Unvieled at EuroPCR: Now the Trick is to Use It. Available online at: https://www.theheart.org/article/973297.do (May 22, 2009).
34. Bundhun PK, Sookharee Y, Bholee A, Huang F. Application of the SYNTAX score in interventional cardiology: a systematic review and meta-analysis. Medicine (Baltimore). (2017) 96(28):e7410. doi: 10.1097/MD.0000000000007410
35. Özmen M, Arikan E, Ozel F, Ardahanlı I. Triglyceride-glucose index: evaluation as a potential new risk marker for SYNTAX score in acute coronary syndrome. Int J Cardiovasc Sci. (2024) 37:e20240096. doi: 10.36660/ijcs.20240096
36. Xu B, Généreux P, Yang Y, Leon MB, Xu L, Qiao S, et al. Validation and comparison of the long-term prognostic capability of the SYNTAX score-II among 1,528 consecutive patients who underwent left main percutaneous coronary intervention. JACC Cardiovasc Interv. (2014) 7(10):1128–37. doi: 10.1016/j.jcin.2014.05.018
37. Rostami A, Tajlil A, Separham A, Sohrabi B, Pourafkari L, Roshanravan N, et al. Association between neutrophil-to-lymphocyte ratio and the systemic inflammatory immunologic index and the angiographic SYNTAX score and the TIMI flow grade in acute STEMI: a cohort study. J Tehran Heart Cent. (2021) 16(4):147–55. doi: 10.18502/jthc.v16i4.8600
38. Zuin M, Rigatelli G, Picariello C, dell'Avvocata F, Marcantoni L, Pastore G, et al. Correlation and prognostic role of neutrophil to lymphocyte ratio and SYNTAX score in patients with acute myocardial infarction treated with percutaneous coronary intervention: a six-year experience. Cardiovasc Revasc Med. (2017) 18(8):565–71. doi: 10.1016/j.carrev.2017.05.007
39. Kurtul S, Sarli B, Baktir AO, Demirbas M, Saglam H, Doğan Y, et al. Neutrophil to lymphocyte ratio predicts SYNTAX score in patients with non-ST segment elevation myocardial infarction. Int Heart J. (2015) 56(1):18–21. doi: 10.1536/ihj.14-175
40. Kahraman S, Agus HZ, Avci Y, Serbest NG, Guner A, Erturk M. The neutrophil to lymphocyte ratio (NLR) is associated with residual syntax score in patients with ST-segment elevation myocardial infarction. Angiology. (2021) 72(2):166–73. doi: 10.1177/0003319720958556
41. Altun B, Turkon H, Tasolar H, Beggı H, Altun M, Temız A, et al. The relationship between high-sensitive troponin T, neutrophil lymphocyte ratio and SYNTAX score. Scand J Clin Lab Invest. (2014) 74(2):108–15. doi: 10.3109/00365513.2013.860619
42. Pan Q, Zhang W, Li X, Chen Z, Yang Y, Wang G. Sex difference in the association between neutrophil to lymphocyte ratio and severity of coronary artery disease. Angiology. (2022) 73(5):470–7. doi: 10.1177/00033197211070884
43. Demir K, Avci A, Altunkeser BB, Yilmaz A, Keles F, Ersecgin A. The relation between neutrophil-to-lymphocyte ratio and coronary chronic total occlusions. BMC Cardiovasc Disord. (2014) 14:130. doi: 10.1186/1471-2261-14-130
44. Soylu K, Gedikli Ö, Dagasan G, Aydin E, Aksan G, Nar G, et al. Neutrophil-to-lymphocyte ratio predicts coronary artery lesion complexity and mortality after non-ST-segment elevation acute coronary syndrome. Rev Port Cardiol. (2015) 34(7-8):465–71. doi: 10.1016/j.repc.2015.01.013
45. Kaya A, Kurt M, Tanboga IH, Işık T, Günaydın ZY, Kaya Y, et al. Relation of neutrophil to lymphocyte ratio with the presence and severity of stable coronary artery disease. Clin Appl Thromb Hemost. (2014) 20(5):473–7. doi: 10.1177/1076029612473517
46. Sönmez O, Ertaş G, Bacaksız A, Tasal A, Erdoğan E, Asoğlu E, et al. Relation of neutrophil-to-lymphocyte ratio with the presence and complexity of coronary artery disease: an observational study. Anadolu Kardiyol Derg. (2013) 13(7):662–7. doi: 10.5152/akd.2013.188
47. Sari I, Sunbul M, Mammadov C, Durmus E, Bozbay M, Kivrak T, et al. Relation of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio with coronary artery disease severity in patients undergoing coronary angiography. Kardiol Pol. (2015) 73(12):1310–6. doi: 10.5603/KP.a2015.0098
48. Sahin DY, Elbasan Z, Gür M, Yildiz A, Akpinar O, Icen YK, et al. Neutrophil to lymphocyte ratio is associated with the severity of coronary artery disease in patients with ST-segment elevation myocardial infarction. Angiology. (2013) 64(6):423–9. doi: 10.1177/0003319712453305
49. Tanındı A, Erkan AF, Ekici B, Alhan A, Töre HF. Neutrophil to lymphocyte ratio is associated with more extensive, severe and complex coronary artery disease and impaired myocardial perfusion. Turk Kardiyol Dern Ars. (2014) 42(2):125–30. doi: 10.5543/tkda.2014.18949
50. Sahin DY, Gür M, Elbasan Z, Özdoğru I, Uysal OK, Kivrak A, et al. Mean platelet volume and extent and complexity of coronary artery disease in diabetic and nondiabetic patients with ST elevation myocardial infarction. Angiology. (2013) 64(7):505–11. doi: 10.1177/0003319712460423
51. Abalı G, Akpınar O, Söylemez N. Correlation of the coronary severity scores and mean platelet volume in diabetes mellitus. Adv Ther. (2014) 31(1):140–8. doi: 10.1007/s12325-013-0081-9
52. Ekici B, Erkan AF, Alhan A, Sayın I, Aylı M, Töre HF. Is mean platelet volume associated with the angiographic severity of coronary artery disease? Kardiol Pol. (2013) 71(8):832–8. doi: 10.5603/KP.2013.0195
53. Sivri S, Sokmen E, Celik M, Ozbek SC, Yildirim A, Boduroglu Y. Usefulness of white blood cell count to mean platelet volume ratio in the prediction of SYNTAX score in patients with non-ST elevation myocardial infarction. Pak J Med Sci. (2019) 35(3):824–9. doi: 10.12669/pjms.35.3.1017
54. Emre AR, Yasar KA, Atakan Y, Orhan C, Murathan K. Relationship between white blood count to mean platelet volume ratio and clinical outcomes and severity of coronary artery disease in patients undergoing primary percutaneous coronary intervention. Cardiovasc Ther. (2020) 2020:9625181. doi: 10.1155/2020/9625181
Keywords: hematological parameters, nucleated red blood cells, neutrophil to lymphocyte ratio, mean platelet volume, coronary angiographic lesions, SYNTAX score, prognostic
Citation: Ramos TMB, Monteiro Júnior JGM, Furtado VC and Sobral Filho DC (2025) The relationship between hematological parameters and coronary angiographic lesions. Front. Cardiovasc. Med. 12:1589121. doi: 10.3389/fcvm.2025.1589121
Received: 6 March 2025; Accepted: 1 August 2025;
Published: 21 August 2025.
Edited by:
Tommaso Gori, Johannes Gutenberg University Mainz, GermanyReviewed by:
İsa Ardahanlı, Bilecik Şeyh Edebali University, TurkeyCopyright: © 2025 Ramos, Monteiro Júnior, Furtado and Sobral Filho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Gildo de Moura Monteiro Júnior, Z2lsZG8ubW9udGVpcm9AdXBlLmJy