 A. Arnautovic1,†
A. Arnautovic1,† H. Dalyanoglu2,†
H. Dalyanoglu2,† L. J. Vallejo Castano2,†
L. J. Vallejo Castano2,† W. Garabet1
W. Garabet1 J. Mulorz1
J. Mulorz1 A. Knapsis1S. Düsing3I. N. Schellinger4,5H. Schelzig1
A. Knapsis1S. Düsing3I. N. Schellinger4,5H. Schelzig1 U. Raaz4,5M. Duran6
U. Raaz4,5M. Duran6 M. U. Wagenhäuser1*
M. U. Wagenhäuser1*
- 1Department of Vascular and Endovascular Surgery, Medical Faculty and University Hospital Duesseldorf, Heinrich-Heine-University, Duesseldorf, Germany
- 2Department of Cardiac Surgery, Medical Faculty and University Hospital Duesseldorf, Heinrich-Heine-University, Duesseldorf, Germany
- 3Department of Angiology, University Medical Center Leipzig, Leipzig University, Leipzig, Germany
- 4Molecular and Translational Vascular Medicine, Department of Cardiology and Pneumology, Heart Center at the University Medical Center Göttingen, Göttingen, Germany
- 5Partner Site Göttingen, German Center for Cardiovascular Research e.V., Göttingen, Germany
- 6Department of Vascular and Endovascular Surgery, Marienhospital Gelsenkirchen, Teaching Hospital of Ruhr-University Bochum, Gelsenkirchen, Germany
Background: Abdominal aortic aneurysm (AAA) is a dynamic disease characterized by a continuous diameter progression. AAA may therefore be categorized in early-stage disease (small diameter AAA) and late-stage disease (large diameter AAA). To date, there is no effective therapy for patients in early stages, resulting in disease-specific stressors. This study was designed to quantify these stressors using a specifically designed questionnaire.
Methods: A self-designed 17-item questionnaire with categorical response options was distributed to patients with small AAA. The aim of the approach was to gain a deeper understanding of patients' quality of life (QoL), psychological state and attitudes towards hypothetical future treatment options.
Results: 122 patients were contacted, 63 of whom consented to participate in the study. The study cohort was predominantly older than 65 years, 84% were male and 56% had been diagnosed with small-size AAA less than 1 year ago. In summary, the AAA diagnosis has a significant impact on all aspects of personal health perception, including physical, social and mental health. The overall QoL was found to be impaired compared to the situation before the AAA diagnosis for most of the respondents, and the current treatment options were considered unsatisfactory. The majority of small AAA patients surveyed would be open to new (invasive) therapies to stop disease progression.
Conclusion: The diagnosis of AAA leads to a reduction in QoL, which impairs the physical, social and mental health, particularly affecting mental health. Patients would welcome treatment options in early stages of their disease.
Introduction
Abdominal aortic aneurysm (AAA) is defined by a dilation of the aorta that is greater than 3 cm or an increase in diameter exceeding 50% compared to the aortic diameter at the level of the diaphragm (1). The prevalence of the disease in individuals over the age of 50 is estimated to be as high as 7.9% in men and 1.3% in women which symbolizes a significant health burden worldwide (2, 3). AAA are commonly classified by size into early- and late-stage disease, with early-stage referring to small aneurysms measuring less than 50 mm in women and less than 55 mm in men.). As of today, there is no treatment available at early stages of the disease which effectively prevents the diameter progression. Late-stage disease is characterized by larger aneurysms exceeding these sex-specific thresholds, for which elective surgical repair is generally recommended in asymptomatic patients due to the markedly increased risk of rupture (4). In case of rupture, high mortality rates are observed and even postintervention mortality is significant (5).
There are different therapeutic options available: endovascular aortic repair (EVAR) and open surgical repair (OSR). EVAR now demonstrates high procedural quality and improved outcomes due to continuous technical and technological advancements, making it the most commonly used therapeutic option for AAA (6). However, despite significant improvements in patient safety, the long-term complication rate following EVAR is estimated to range between 16% and 30%. Here, the most common complications include both endograft device-related and systemic complications (7). Among them, different types of endoleak (EL) may occur, which may warrant re-interventions exposing affected patients to the risk of recurrent endovascular procedures.
AAA represents a dynamic pathological condition that remains asymptomatic during its early stages. The annual expansion rate of the aneurysm varies between 0.09 cm and 0.46 cm, contingent upon the initial aneurysm size and other contributory risk factors (6). The recommended intervals for follow-up ultrasound—widely regarded as the modality of choice for AAA surveillance due to its safety, accessibility, and cost-effectiveness—are informed by these clinical considerations and range from 6 months to several years, depending on the current aneurysm diameter (4). Such fact heightens patient awareness, marked by specific stress factors, particularly related to the anticipated enlargement of the AAA diameter. Quality of life (QoL), as well as changes within its individual dimensions following a diagnosis of AAA, appear to be subject to disease-specific alterations, likely attributable to the initially asymptomatic course of the condition. That being said, the recent literature has indicated a reduction in overall health status among patients with AAA; however, the validated questionnaires employed neither comprehensively capture all individual dimensions of health nor are they specifically designed to address potential disease-specific stressors associated with AAA (8–12). Furthermore, it has been shown that the impact on QoL in AAA patients under surveillance (up to 90% of all incidentally detected AAA) is highly individual, with a notable influence on emotional parameters (13).
This study seeks to contribute to the existing body of knowledge by identifying disease-specific stressors in the early stages of AAA through the administration of a custom-designed, AAA-specific questionnaire to patients with small aneurysms who do not yet meet the criteria for therapeutic intervention. Additionally, it seeks to evaluate the potential readiness of AAA patients for treatment during the initial phase of the disease.
Methods
Building upon the Short-Form Health Survey (SF-8), a newly developed 17-item questionnaire specifically designed to assess AAA-related stressors was administered to patients diagnosed with small abdominal aortic aneurysms not yet requiring intervention. Recruitment took place at the Clinic for Cardiac Surgery and the Clinic for Vascular and Endovascular Surgery at University Hospital Düsseldorf, Germany, as well as at the Clinic for Vascular and Endovascular Surgery at Sankt Marien-Hospital Buer and Marienhospital Gelsenkirchen, Gelsenkirchen, Germany (see Supplementary Figure 1). Here, all patients who were diagnosed with a small AAA between January 1, 2023, and June 1, 2024, were included in the study. The timeframe was chosen to keep the potential recall period for patients within a reasonable and reliable timeframe. No exclusion criteria applied. Patients were mailed the survey form together with an unmarked return envelope.
The questionnaire was divided into three sections: a demographic part, a health-specific part, and a part directed to the standard of care. Patients completed the questions independently, without external assistance. The analysis was conducted anonymously. The questionnaire aimed to address three key questions for patients with small AAAs, as follows:
1. How do patients feel about being diagnosed with small-size AAA at an early stage, particularly considering the current lack of treatment options at this stage?
2. To what extent does the diagnosis of a small AAA affect the patient's daily life? Are there any restrictions or changes in everyday life since the diagnosis?
3. How would patients react to the hypothetical possibility of an early, minimally invasive treatment for AAA? Would they opt for such treatment if it was available?
The study was approved by the ethic Committee of the Medical Faculty at the Heinrich-Heine-University Düsseldorf (study number: 2024-2815). As this study was fully anonymous, informed consent was waived.
Categorical data in a pre-diagnosis vs. post-diagnosis comparison were analyzed using Fisher's exact test to evaluate shifts resulting from the AAA diagnosis. The level of significance was set to p < 0.05.
Results
A total of 122 patients with small AAAs were contacted, with 63 patients ultimately participating, resulting in a response rate of 52%. The standardized Cronbach's alpha for the QoL–related items of the questionnaire was 0.84, indicating a high level of internal consistency (see Supplementary Figure 1).
The first three questions assessed demographic data of the study cohort. The majority of patients were older than 65 years, male, smokers and were diagnosed with a small AAA less than one year ago (Table 1).
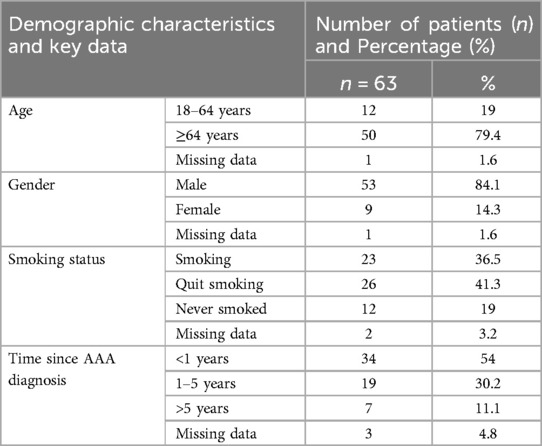
Table 1. Patient demographic characteristics and key data. Data are presented as absolute and relative frequencies, n (%), for categorical variables within the study cohort, including age, gender, smoking status, and time since AAA diagnosis. (n = 63).
The first question of the health-related section addressed personal well-being before and after receiving the diagnosis. Here, the diagnosis of a small AAA was associated with a statistically significant decline in personal well-being (Figure 1A and Table 2) (p < 0.05). Specifically, the ratio of patients with good and very good personal well-being dropped from 71% before to 43% after diagnosis. Conversely, the proportion of individuals who rated their personal well-being as bad or very bad almost quadrupled, rising from 5% to 19% after the diagnosis of an AAA (Figure 1A and Table 2). The decline in personal well-being also translated in corresponding findings in the quality of life (QoL) assessment. Here, 54% of the patients would find their quality of life at least somewhat better without AAA diagnosis (Figure 1B and Table 2).
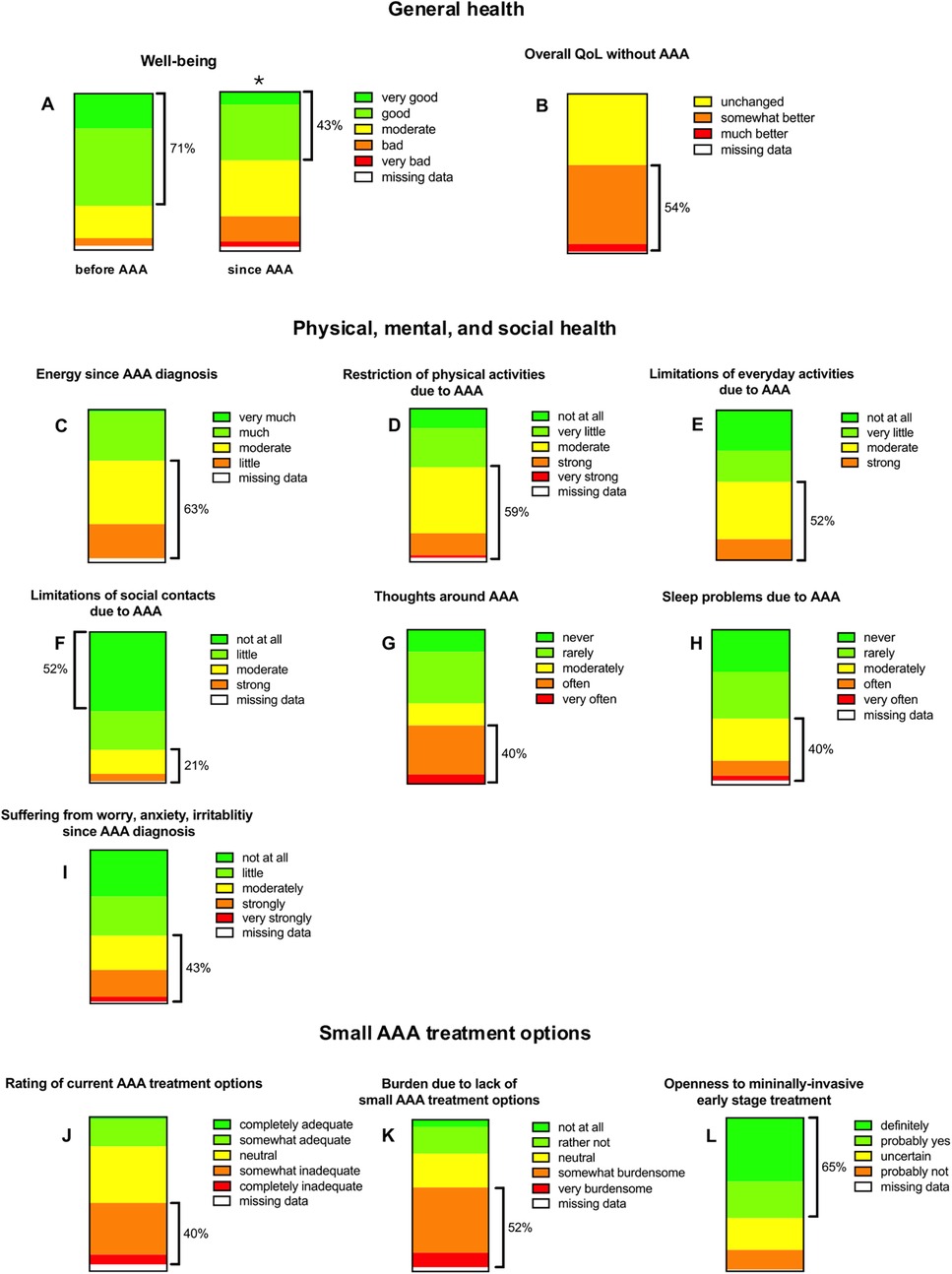
Figure 1. Patient-reported outcomes (charts A–L) regarding general health (A–B), physical, mental, and social well-being (C–I), and perspectives on treatment options for small abdominal aortic aneurysms (AAA) (J–L). Each chart reflects response distributions across ordinal scales (e.g., from very good to very bad). Responses reflect perceived well-being, energy levels, activity limitations, psychological burden, and openness to future treatments. While 43% of participants reported improved well-being since diagnosis, 65% expressed willingness to consider minimally invasive early-stage interventions. *Indicates p < 0.05 vs. well-being status before AAA.
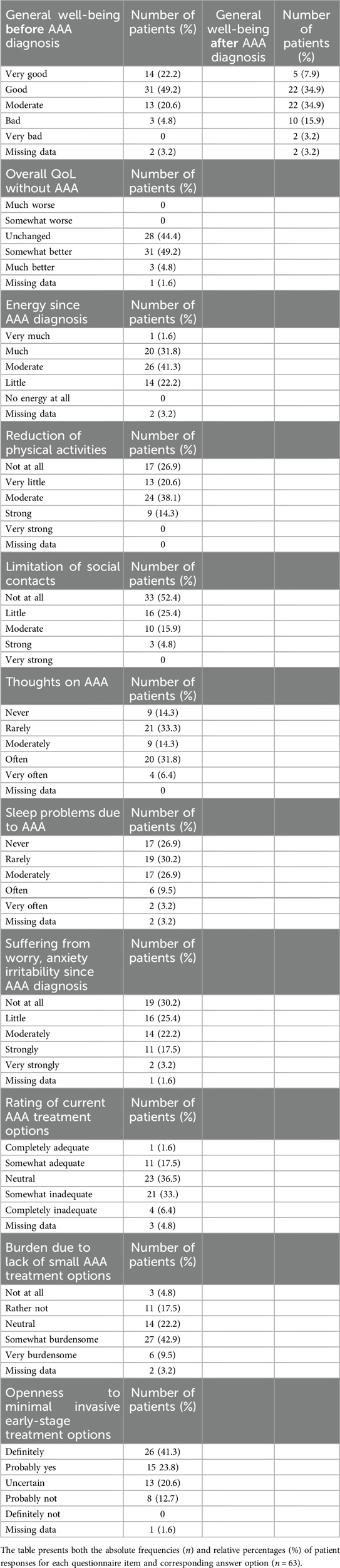
Table 2. Absolute and relative frequencies.
To identify specific factors driving QoL deterioration, we analyzed items of physical, mental and social health. 63% of the patients reported on self-perceived energy levels that were moderate and worse since AAA diagnosis (Figure 1C and Table 2). Also, the majority of patients reported at least moderately restricted physical activities since diagnosis (Figures 1D,E and Table 2). Specifically, 59% of the patients reduced sports at least moderately (Figure 1D and Table 2), and 52% patients reduced everyday activities (e.g., household tasks, shopping, etc.) to an at least to a moderate extent (Figure 1E and Table 2). Interestingly, for most patients (52%) there were no restrictions in contact with family members. Yet, 21% of the patients reported at least moderate limitation regarding social contacts (Figure 1F and Table 2). When examining mental health, we observed that most patients' thoughts are frequently centered on their illness. Interestingly, only 13% of patients reported never thinking about their AAA, while 40% stated that their thoughts often or very often revolve around the disease during the day (Figure 1G and Table 2). For many patients, the diagnosis of a small size AAA means having difficulties falling asleep: 40% of the patients experienced this issue at least moderately and in 13% of the patients this even occurred often to very often (Figure 1H and Table 2). Of note, the severity of worries and anxiety related to AAA disease exhibits a similar distribution pattern (Figure 1I and Table 2).
The final three questions addressed current treatment options and aimed to assess patients' willingness to adopt a hypothetical early-stage treatment. Notably, 40% of respondents felt that existing treatment options and therapeutic approaches are somewhat or completely inadequate (Figure 1J and Table 2). This sentiment is particularly driven by the lack of options for small AAAs, which are managed conservatively through surveillance—a method perceived as rather or very burdensome by 52% of patients (Figure 1K and Table 2). Consequently, the willingness to pursue treatment in the early stages of the disease is remarkably high. If a minimally invasive treatment capable of slowing AAA growth were available, 65% of respondents indicated they would opt for it (Figure 1L and Table 2).
Discussion
Given the limitations of a 52% response rate and a modest sample size of 63 patients, this study suggests that the diagnosis of small, early-stage AAA represents a significant and widespread health burden, adversely affecting patients' physical, social, and psychological well-being.
The World Health Organization defines quality of life (QoL) as an individual's perception of their place in life, considering the cultural and value systems they live within, as well as their personal goals, expectations, standards, and concerns (14). Given the progressive nature of AAA, which may be asymptomatic in its early stages but still exposes the patient to a constant, progressive life-threatening risk of rupture, a small AAA diagnosis impacts nearly every dimension of QoL as defined by the WHO (15, 16). In this context, the reduced QoL suggested by the findings of the present study cohort is not only logical but also understandable.
Analyzing different QoL dimensions in detail, our survey suggests a significant impact on the mental health of patients with small-size AAA. Recent qualitative studies describe the mixed emotions patients experience following an AAA disease, ranging from relief at having a diagnosis to fears about disease progression. Here, both Botero et al. and Hansson et al. found that patients valued the detection of their AAA, while the diagnosis also led to worry, uncertainty, and feelings of anxiety (17, 18). Mental health has a significant impact on the vasculature, with conditions like depression, anxiety, psychological distress, and post-traumatic stress disorder recognized as independent cardiovascular risk factors (19). Interestingly, several mechanistic associations have already been further elucidated. For instance, it has been demonstrated that mental stress can induce transient peripheral endothelial dysfunction, which is considered as an early-stage phenomenon of atherosclerosis (20). Moreover, additional cardiovascular parameters appear to be influenced by mental stress. Specifically, the impact on mean arterial pressure is believed to be mechanistically mediated by elevated levels of circulating neurotransmitters, as well as by interactions with vascular inflammation through increased concentrations of pro-inflammatory cytokines (21, 22). However, the reverse relationship, i.e., the extent to which cardiovascular diseases, or the mere knowledge of their existence, influence mental health, appears to be far less well documented. In their review of 11 studies, Ericsson et al. addressed the question to what extent the knowledge of having an aneurysm may be worrying and burdensome for affected patients. In analogy with our data, the authors found that patients diagnosed with AAA tend to have inferior QoL and health than those without such diagnosis (23). Focusing on mental health in particular, a study from Kim et al. reported an increased rate of depression rate upon AAA diagnosis predominantly at younger ages (24). In this context, individual disease perception—and its positive modification by others—as well as social support within the close social circle of the AAA patient, may serve as important protective factors. However, the presence and influence of these factors were beyond the scope of the current questionnaire-based study and may rather serve as a basis for future research initiatives aiming to improve preventive patient care. That being said, the question arises as to the clinical implications for treating physicians. In light of the present data, early psychological support for patients in the initial stages of AAA disease may prove particularly beneficial and could therefore be considered as a potential component of patient care.
In addition to mental health, an AAA diagnosis also appears to severely restrict everyday activities. Our data may suggest a substantial limitation in self-perceived energy levels as well as in the ability to perform daily activities following an AAA diagnosis. This is consistent with findings by Bath et al., who reported that physical health limitations were the most persistent restriction after an AAA diagnosis, while the impact on mental QoL was more transient (25). As a matter of fact, the loss of self-perceived energy levels cannot be directly attributed to AAA, since it is not a consumptive disease. There is likely to be a significant overlap with other dimensions of health, such as mental and social factors. This interwovenness and interdependency of the individual dimensions of health is not novel but has already been introduced to the current literature (26).
Social health is another area potentially influenced by a AAA diagnosis. It is noteworthy that the present study did not identify a significant association between AAA and restrictions in social activities. Similarly, a Swedish cross-sectional study by Damhus et al. also found that social relationships might remain relatively unaffected by an AAA diagnosis, with participants reporting no changes in their contact with family members (27). In fact, social support may play a crucial role in helping patients cope with the stress and worry associated with AAA.
Understandably, following an AAA diagnosis, many patients seek ways to positively influence the course of the disease (28). The relatively high participation rate in this study, despite the lack of direct physician involvement, underscores how deeply concerned patients are about their condition and how much it affects their lives. In this context, considerable emphasis should be placed on the findings pertaining to patients’ willingness to adopt a hypothetical therapeutic intervention, even during the early stages of abdominal aortic aneurysm (AAA) disease. In view of patients’ evident preference for minimally invasive interventions—particularly when considering factors related to procedural burden and postoperative recovery—such therapeutic modalities may prove especially appropriate and accessible for individuals in the early stages of AAA disease (29, 30). Given the hypothetical nature of the question posed to respondents in this study, the reported high willingness to undergo minimally invasive treatment should be interpreted exploratory in nature and does not warrant immediate changes in clinical treatment strategies. Should such an objective be pursued in future studies, more detailed, procedure-specific risk–benefit information would be essential to facilitate informed, individualized decision-making. Nonetheless, the reported overall willingness to consider minimally invasive therapy during this so-called ‘window of missed opportunity’ reflects the substantial burden the disease imposes on patients’ QoL across multiple dimensions. This also emphasizes to need for healthcare providers to prioritize the development and implementation of effective therapeutic strategies that help patients better manage the disease. Patients appear to recognize the critical need for intervention at this early stage.
This study is subject to several limitations. Firstly, the relatively small sample size, combined with a response rate of 52% and recruitment from a limited number of centers, may limit the representativeness of the study population and introduce a considerable risk of self-selection bias. Consequently, the generalizability of the findings to the broader population may be constrained. Therefore, the presented survey data need validation on larger cohorts in multi center settings and findings should be interpretated with caution. However, the demographic characteristics of our patient population (including sex, age, and smoking status) align with those of the general AAA population, suggesting that the sample may still be representative despite its limited size. Additionally, the questionnaire used was self-designed and has not undergone specific validation, which restricts direct comparisons with the existing literature. As a result of the custom-made design, certain aspects of AAA may not have been fully addressed. Although rigorous measures were undertaken to assess internal consistency through the calculation of Cronbach's alpha, which yielded a high level of internal consistency, the employment of a non-validated questionnaire may impinge upon the reliability and external validity of the results. Lastly an additional potential selection bias may also compromise our reported data since included patients may be more concerned with general health issues due to their AAA diagnosis.
In conclusion, although AAA is often detected at an early, asymptomatic stage, the awareness of a progressive and potentially life-threatening condition may significantly impact patients’ QoL, as well as their physical and mental health. A substantial proportion of patients with small AAA appear to harbor reservations regarding the adequacy of the current standard of care. This may, in turn, reflect a preference for earlier intervention—currently hypothetical—that aims to arrest disease progression.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The study was approved by the ethic Committee of the Medical Faculty at the Heinrich-Heine-University Düsseldorf (study number: 2024-2815). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AA: Conceptualization, Data curation, Formal analysis, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing, Methodology, Project administration, Resources, Software, Supervision. HD: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. LV: Data curation, Formal analysis, Writing – original draft. WG: Writing – review & editing, Data curation, Validation, Visualization. JM: Writing – review & editing, Data curation, Project administration, Software, Validation, Visualization. AK: Writing – review & editing, Data curation, Formal analysis, Investigation, Project administration, Validation. SD: Writing – review & editing, Data curation, Formal analysis, Visualization. IS: Writing – review & editing, Conceptualization, Supervision, Validation, Visualization. HS: Writing – review & editing, Conceptualization, Project administration, Resources, Supervision, Validation, Visualization. UR: Writing – review & editing, Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization. MD: Writing – review & editing, Conceptualization, Formal analysis, Supervision, Validation, Visualization. MW: Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was partially funded by Angiolutions GmbH, Hannover, Germany.
Conflict of interest
The authors declare that this study received funding from Angiolutions GmbH. The funder had the following involvement in the study: study design. IS and UR are founders and shareholders of Angiolutions. MUW is scientific and clinical advisor to Angiolutions. HS is member of Angiolutions' advisory board.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1600775/full#supplementary-material
Supplementary Figure 1 | Questionnaire assessing quality of life in patients with abdominal aortic aneurysm (AAA). This self-administered questionnaire consists of two sections: The first four items gather general health and demographic information (age, gender, smoking status, and time since diagnosis). The subsequent items (questions 5–17), under the heading “Questionnaire Quality of Life with Abdominal Aortic Aneurysm”, specifically assess physical, emotional, and social aspects of living with an AAA. Patients were instructed to respond solely in relation to their aneurysm, excluding other comorbidities. Responses were collected anonymously and voluntarily. For the calculation of Cronbach’s alpha, only items 5–17 were included, as they directly address disease-specific quality of life.
Supplementary Figure 2 | Correlation matrix of AAA Quality of Life (QoL)-associated questionnaire items for reliability assessment. The heatmap illustrates the pairwise Pearson correlation coefficients among questions 5–13 of the custom-made AAA questionnaire for Cronbach's alpha calculation. The color gradient reflects the magnitude and direction of the correlations, providing a graphical overview of inter-item relationships. Cronbach Alpha is .84, suggesting a high internal consistency.
References
1. Altobelli E, Rapacchietta L, Profeta VF, Fagnano R. Risk factors for abdominal aortic aneurysm in population-based studies: a systematic review and meta-analysis. Int J Environ Res Public Health. (2018) 15(12):2805. doi: 10.3390/ijerph15122805
2. Mussa FF. Screening for abdominal aortic aneurysm. J Vasc Surg. (2015) 62(3):774–8. doi: 10.1016/j.jvs.2015.05.035
3. Patil A, Conley M, Paulson C, Pompoco C, Wallace R, Swiston C, et al. Abdominal aortic aneurysm and exfoliation syndrome: a literature review comparing single site findings. Acta Ophthalmol. (2023) 101(5):478–84. doi: 10.1111/aos.15307
4. Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, et al. Editor’s choice—European Society for Vascular Surgery (ESVS) 2024 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg. (2024) 67(2):192–331. doi: 10.1016/j.ejvs.2023.11.002
5. Karthikesalingam A, Holt PJ, Vidal-Diez A, Ozdemir BA, Poloniecki JD, Hinchliffe RJ, et al. Mortality from ruptured abdominal aortic aneurysms: clinical lessons from a comparison of outcomes in England and the USA. Lancet. (2014) 383(9921):963–9. doi: 10.1016/S0140-6736(14)60109-4
6. Hornby-Foster I. Abdominal aortic aneurysm growth rates in patients undergoing local ultrasound surveillance. Ultrasound. (2023) 31(1):23–32. doi: 10.1177/1742271X221093751
7. Daye D, Walker TG. Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management. Cardiovasc Diagn Ther. (2018) 8(Suppl 1):S138–56. doi: 10.21037/cdt.2017.09.17
8. Lesjak M, Boreland F, Lyle D, Sidford J, Flecknoe-Brown S, Fletcher J. Screening for abdominal aortic aneurysm: does it affect men’s quality of life? Aust J Prim Health. (2012) 18(4):284–8. doi: 10.1071/PY11131
9. Marteau TM, Kim LG, Upton J, Thompson SG, Scott AP. Poorer self assessed health in a prospective study of men with screen detected abdominal aortic aneurysm: a predictor or a consequence of screening outcome? J Epidemiol Community Health. (2004) 58(12):1042–6. doi: 10.1136/jech.2003.019307
10. Spencer CA, Norman PE, Jamrozik K, Tuohy R, Lawrence-Brown M. Is screening for abdominal aortic aneurysm bad for your health and well-being? ANZ J Surg. (2004) 74(12):1069–75. doi: 10.1111/j.1445-1433.2004.03270.x
11. Wanhainen A, Rosén C, Rutegård J, Bergqvist D, Björck M. Low quality of life prior to screening for abdominal aortic aneurysm: a possible risk factor for negative mental effects. Ann Vasc Surg. (2004) 18(3):287–93. doi: 10.1007/s10016-004-0021-x
12. Lyttkens L, Wanhainen A, Svensjö S, Hultgren R, Björck M, Jangland E. Systematic review and meta-analysis of health related quality of life and reported experiences in patients with abdominal aortic aneurysm under ultrasound surveillance. Eur J Vasc Endovasc Surg. (2020) 59(3):420–7. doi: 10.1016/j.ejvs.2019.07.021
13. Suckow BD, Schanzer AS, Hoel AW, Wyers M, Marone LK, Veeraswamy RK, et al. A novel quality of life instrument for patients with an abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. (2019) 57(6):809–15. doi: 10.1016/j.ejvs.2019.01.018
14. The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. (1995) 41(10):1403–9. doi: 10.1016/0277-9536(95)00112-k
15. Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. (2003) 348(19):1895–901. doi: 10.1056/NEJMcp012641
16. Vardulaki KA, Prevost TC, Walker NM, Day NE, Wilmink AB, Quick CR, et al. Growth rates and risk of rupture of abdominal aortic aneurysms. Br J Surg. (1998) 85(12):1674–80. doi: 10.1046/j.1365-2168.1998.00946.x
17. Berterö C, Carlsson P, Lundgren F. Screening for abdominal aortic aneurysm, a one-year follow up: an interview study. J Vasc Nurs. (2010) 28(3):97–101. doi: 10.1016/j.jvn.2010.04.001
18. Hansson A, Brodersen J, Reventlow S, Pettersson M. Opening Pandora’s box: the experiences of having an asymptomatic aortic aneurysm under surveillance. Health Risk Soc. (2012) 14:341–59. doi: 10.1080/13698575.2012.680953
19. Sara JDS, Toya T, Ahmad A, Clark MM, Gilliam WP, Lerman LO, et al. Mental stress and its effects on vascular health. Mayo Clin Proc. (2022) 97(5):951–90. doi: 10.1016/j.mayocp.2022.02.004
20. Ghiadoni L, Donald AE, Cropley M, Mullen MJ, Oakley G, Taylor M, et al. Mental stress induces transient endothelial dysfunction in humans. Circulation. (2000) 102(20):2473–8. doi: 10.1161/01.CIR.102.20.2473
21. Freyschuss U, Hjemdahl P, Juhlin-Dannfelt A, Linde B. Cardiovascular and sympathoadrenal responses to mental stress: influence of beta-blockade. Am J Physiol. (1988) 255(6 Pt 2):H1443-51 doi: 10.1152/ajpheart.1988.255.6.H1443
22. Camell CD, Sander J, Spadaro O, Lee A, Nguyen KY, Wing A, et al. Inflammasome-driven catecholamine catabolism in macrophages blunts lipolysis during ageing. Nature. (2017) 550(7674):119–23. doi: 10.1038/nature24022
23. Ericsson A, Kumlien C, Ching S, Carlson E, Molassiotis A. Impact on quality of life of men with screening-detected abdominal aortic aneurysms attending regular follow ups: a narrative literature review. Eur J Vasc Endovasc Surg. (2019) 57(4):589–96. doi: 10.1016/j.ejvs.2018.10.012
24. Kim MH, Yoo JH, Cho HJ, Ko KJ, Jun KW, Han KD, et al. Increased depression risk in patients with abdominal aortic aneurysm: a nationwide cohort study. Ann Surg Treat Res. (2021) 101(5):291–8. doi: 10.4174/astr.2021.101.5.291
25. Bath MF, Sidloff D, Saratzis A, Bown MJ, Investigators UKAGS. Impact of abdominal aortic aneurysm screening on quality of life. Br J Surg. (2018) 105(3):203–8. doi: 10.1002/bjs.10721
26. Sowers KM, Rowe WS, Clay JR. The intersection between physical health and mental health: a global perspective. J Evid Based Soc Work. (2009) 6(1):111–26. doi: 10.1080/15433710802633734
27. Damhus CS, Siersma V, Hansson A, Bang CW, Brodersen J. Psychosocial consequences of screening-detected abdominal aortic aneurisms: a cross-sectional study. Scand J Prim Health Care. (2021) 39(4):459–65. doi: 10.1080/02813432.2021.2004713
28. Pettersson M, Hansson A, Brodersen J, Kumlien C. Experiences of the screening process and the diagnosis abdominal aortic aneurysm among 65-year-old men from invitation to a 1-year surveillance. J Vasc Nurs. (2017) 35(2):70–7. doi: 10.1016/j.jvn.2016.11.003
29. Winterborn RJ, Amin I, Lyratzopoulos G, Walker N, Varty K, Campbell WB. Preferences for endovascular (EVAR) or open surgical repair among patients with abdominal aortic aneurysms under surveillance. J Vasc Surg. (2009) 49(3):576–81.e3. doi: 10.1016/j.jvs.2008.09.012
Keywords: quality of life, abdominal aortic aneurysm, diagnosis, survey, small aortic aneurysms
Citation: Arnautovic A, Dalyanoglu H, Vallejo Castano LJ, Garabet W, Mulorz J, Knapsis A, Düsing S, Schellinger IN, Schelzig H, Raaz U, Duran M and Wagenhäuser MU (2025) General health survey in patients with small abdominal aortic aneurysm. Front. Cardiovasc. Med. 12:1600775. doi: 10.3389/fcvm.2025.1600775
Received: 31 March 2025; Accepted: 14 July 2025;
Published: 19 August 2025.
Edited by:
Nicola Mumoli, ASST Valle Olona, ItalyReviewed by:
Jiaxuan Feng, Second Military Medical University, ChinaShuqi Ren, Beihang University, China
Copyright: © 2025 Arnautovic, Dalyanoglu, Vallejo Castano, Garabet, Mulorz, Knapsis, Düsing, Schellinger, Schelzig, Raaz, Duran and Wagenhäuser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. U. Wagenhäuser, bWFya3VzLndhZ2VuaGFldXNlckBmcmVlbmV0LmRl
†These authors have contributed equally to this work