 Maria Jose Cabada-Garcia1,2
Maria Jose Cabada-Garcia1,2 Jahir Rodriguez-Rivera1
Jahir Rodriguez-Rivera1 Carlos Jerjes-Sanchez1,3*
Carlos Jerjes-Sanchez1,3* Mauricio Castillo-Perez1
Mauricio Castillo-Perez1 Paola Gutierrez-Gallegos1
Paola Gutierrez-Gallegos1 Ana Lucia Martinez-Rodriguez1Enrique Paredes-Gutierrez1Renata Claudia Quevedo-Salazar1Humberto De Leon-Gutierrez1
Ana Lucia Martinez-Rodriguez1Enrique Paredes-Gutierrez1Renata Claudia Quevedo-Salazar1Humberto De Leon-Gutierrez1 Oscar David Lopez-Cortes1Jathniel Panneflek1,3Raul Monjaras-Alvarado1Jesus Antonio Moron-Mosso1Jaime Guillermo Gonzalez-Medina1
Oscar David Lopez-Cortes1Jathniel Panneflek1,3Raul Monjaras-Alvarado1Jesus Antonio Moron-Mosso1Jaime Guillermo Gonzalez-Medina1
- 1Tecnológico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Monterrey, Nuevo León, México
- 2Fellow of the General Directorate of Quality and Health Education, Ministry of Health, Mexico City, México
- 3Instituto de Cardiología y Medicina Vascular, TecSalud, Escuela de Medicina y Ciencias de la Salud, Tecnológico de Monterrey, San Pedro Garza García, Nuevo León, México
Introduction: Controversy persists regarding the use of pericardial effusion drainage in patients with pulmonary arterial hypertension (PAH), as several studies report high rates of post-procedure morbidity and mortality.
Methods: We conducted a systematic review to evaluate the safety of pericardiocentesis (PC) in patients with PAH and a large or hemodynamically significant pericardial effusion. We focused on studies involving patients with PAH who presented with a large or hemodynamically significant pericardial effusion and underwent PH. Our primary objective was to evaluate the incidence of major periprocedural complications, and our secondary objectives were to identify the clinical presentation and echocardiographic findings.
Results: We identified 35 patients across 16 studies. Connective tissue disease was the most common etiology of PAH. Drainage strategies during PC differed across studies. The overall mortality rate was 20%, and we identified pericardial decompression syndrome in 14% of patients. Dyspnea and peripheral edema dominated the clinical presentation. Echocardiographic findings of cardiac tamponade, particularly left-sided chamber collapse, appeared more frequently.
Discussion: PC in patients with PAH carries a heightened risk of pericardial decompression syndrome and mortality. However, careful patient selection, echocardiographic guidance, gradual decompression, and continuous hemodynamic monitoring during the procedure may help improve outcomes.
Systematic Review Registration: PROSPERO 585310.
Introduction
Pulmonary arterial hypertension (PAH) is a vascular disease characterized by a progressive increase in pulmonary vascular resistance and pulmonary arterial pressure, leading to right ventricular (RV) dysfunction, heart failure phenotypes, and premature death (1). Pericardial effusion (PE) occurs in up to 25%–29% of patients with PAH (1–3), with higher rates observed in PAH related to connective tissue disease (CTD) (4, 5). The Mexican REMEHIP registry (1) identified a 10% prevalence of PE in patients with PAH, and the REVEAL (6) and REHAP (7) registries associated PE with an increased risk of death in this subgroup. PE may occur due to the disruption of lymphatic and venous drainage around the heart secondary to the increased right atrial (RA) pressure seen in PAH. However, serositis may also cause PE independently, especially in CTDs. Recently, myocardial edema has been experimentally identified as a stage preceding the development of PE, reflecting hemodynamic deterioration prior to the clinical onset of PE (8). PE is independently associated with worse prognosis (9) and increased mortality (2, 10–13), regardless of the presence of other risk factors. Additionally, it is a poor prognostic factor in the three-strata risk-assessment model in patients with PAH (2). A direct proportional relationship has been observed between the severity of PE and the risk of mortality, underscoring its importance as a poor prognostic factor and a predictor of more intensive treatment.
Although the clinical significance of PE is clear, guidelines for managing this specific population remain poorly defined. An enlarged PE induces significant hemodynamic instability without treatment, particularly when associated with RV dysfunction. Paradoxically, relieving the effusion may result in a sudden increase in venous return and transmural pressure, leading to RV decompensation and circulatory collapse attributed to pericardial decompression syndrome (PDS) (14, 15). Existing evidence regarding the safety and risk-benefit ratio of pericardiocentesis (PC) in patients with PAH remains controversial, complicating clinical decision-making (13, 14, 16–18). The only available systematic review addressing the role of pulmonary hypertension (PH) in the development of cardiac tamponade does not explicitly assess the outcomes of PC (15). Given the lack of conclusive evidence (10, 14), we conducted the first systematic review to evaluate the safety of PC in patients with PAH associated with large or hemodynamically significant PE.
Methods
Systematic review protocol and study design
We conducted a systematic review adhering to the PRISMA statement (19) and registered the protocol in PROSPERO under ID number 585310. The primary objective of this study was to evaluate the safety of PC in patients with PAH presenting with a large or hemodynamically significant PE by assessing the incidence of major periprocedural complications. The secondary objective was to identify the clinical and echocardiographic findings associated with large or hemodynamically significant PE in patients with PAH.
Search strategy and data sources
We conducted an electronic search of PubMed, Scopus, Web of Science, OpenGrey, and Google Scholar for case reports, case series, case-control studies, randomized clinical trials, registries, and prospective and retrospective studies published until July 2024 (Supplementary Appendix S1). The team simplified the final search strategy to refine the scope of studies using keywords and MeSH terms (Supplementary Appendix S2). We employed snowball sampling to minimize lost reports and utilized controlled vocabulary (Supplementary Appendix S3). We collected the articles using the Zotero reference manager software.
Eligibility criteria
We included studies involving patients with PAH associated with a large or hemodynamically significant PE who underwent PC. The diagnosis of PAH required confirmation through right heart catheterization. We excluded systematic reviews and studies, including groups 2, 3, 4, or 5 PH; those that did not report patients' clinical course; studies with patients under 18 years of age; those primarily focused on trivial or small PE; and cases where PE was due to malignancy, trauma, or recent cardiac surgery.
Study selection and data extraction
Two investigators performed the search strategy and initial screening using the Rayyan software (22). Our team consisted of cardiologists, residents, and medical students who underwent proper training regarding PAH from a cardiologist with extensive expertise in the field. After eliminating duplicates, investigators independently identified potentially eligible studies by examining the titles and abstracts, and subsequently obtained full articles to assess adherence to eligibility criteria. A third researcher with experience in the field resolved any disagreement regarding study inclusion. The investigators then independently extracted and analyzed data through a double-data extraction process into an online collaborative database with controlled access, which was constructed to consider the variables of interest (Supplementary Appendix S4).
Risk of bias
We reviewed various databases, including the grey literature. We used hand-searching and snowballing methods (23) to ensure broad study coverage. There were no language restrictions. Two researchers independently performed the screening, eligibility analysis, and data extraction. We held regular discussions to review the extracted data, resolve disagreements through consensus, and systematically enter the data into the database. Based on the CONSORT guidelines and the Newcastle-Ottawa Quality Assessment Form for Cohort Studies, we designed a data quality strategy to evaluate the included studies.
Data synthesis and analysis
We conducted a formal narrative synthesis of the demographic, clinical, echocardiographic, right heart catheterization, and periprocedural complications information of the included studies. We used summary statistics for continuous and categorical variables according to their types and distributions. We obtained the reported frequency and percentage for continuous variables, as well as the weighted average and standard deviation for continuous variables, in studies with more than one patient.
Definitions
PAH: mean pulmonary arterial pressure (mPAP) ≥20 mmHg at rest, measured by right heart catheterization, pulmonary artery wedge pressure ≤15 mmHg, and pulmonary vascular resistance >2 Wood units (20).
PE: an abnormal accumulation of pericardial fluid in the pericardial cavity (trivial: seen only in systole, corresponding to <50 ml of pericardial fluid; small: <10 mm, corresponding to 50–100 ml; moderate: 10–20 mm, corresponding to 100–500 ml; large: >20 mm, corresponding to >500 ml; very large: >25 mm, corresponding to >700 ml) (21).
Cardiac tamponade: cardiac compression due to fluid accumulation within the pericardial sac, resulting in impaired diastolic filling of the ventricles associated with clinical instability (hypotension, respiratory distress, etc.) (24).
PDS: acute hemodynamic deterioration and/or pulmonary edema resulting from sudden ventricular dysfunction that occurs following an otherwise uncomplicated PC (25, 26).
Mayor periprocedural complication: death, major bleeding, traumatic injury to cardiac structures, injury to surrounding structures, significant hemodynamic compromise, or circulatory collapse requiring cardiopulmonary resuscitation, intraprocedurally or up to 30 days post-procedure (16).
See the Supplementary Material (Appendix S3) for additional definitions.
Results
We systematically reviewed PubMed, Scopus, OpenGrey, Google Scholar, and Web of Science on September 12, 2024. Figure 1 shows the PRISMA Flow Diagram. The initial search yielded 1,003 articles, of which 885 remained after duplicates were removed. Two investigators independently screened the titles and abstracts, eliminating 833 articles. The two investigators analyzed 52 articles through full-text screening and included 13 studies that met the inclusion criteria. We contacted the authors of seven additional articles during full-text screening because of the unclear diagnostic methods for establishing PAH. Three authors confirmed the diagnosis of PAH using right heart catheterization (17, 27, 28). We performed double-data extraction of the 16 included articles (13, 14, 16–18, 27–37) (Supplementary Table S1–S7). The included articles are one prospective cohort, three retrospective cohorts, two case series, six case reports, and four abstracts. The risk of bias assessment identified all studies except one (13) as of poor quality, primarily due to the study design (Table 1). 62.5% of the studies included patients <55 years, and most were female. The most common PAH group was associated with CTD, mainly systemic sclerosis (SSc). Most studies included patients receiving PAH therapy. Dyspnea was the predominant clinical presentation reported across most studies, followed by peripheral edema (Table 2).
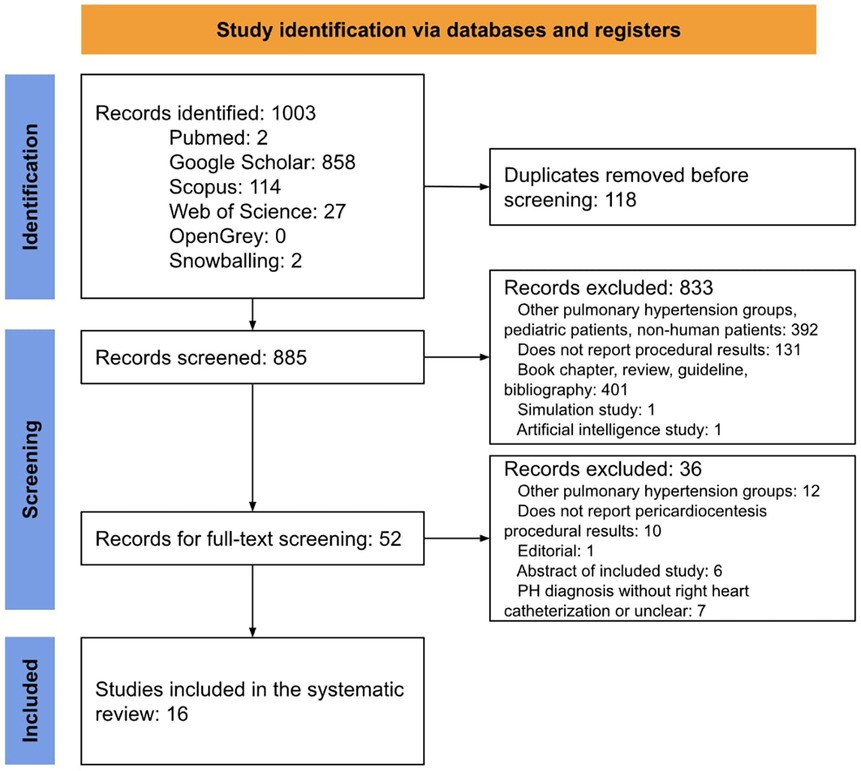
Figure 1. PRISMA flow diagram.
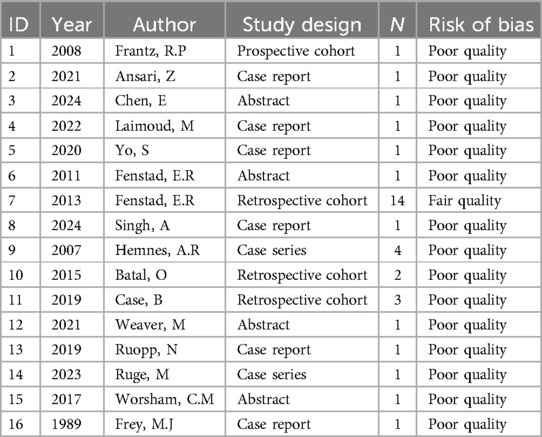
Table 1. Quality assessment.

Table 2. Study design and patient characteristics of studies on PAH patients who underwent pericardiocentesis.
Studies qualitatively classified the effusion size. Various studies performed echocardiography-guided PC (13, 14, 16, 18, 27, 33) and PC with real-time invasive hemodynamic monitoring (14, 18, 35). The total amount of pericardial fluid drained across the studies ranged from 80 to 2400 ml. The drainage strategy differed, with most studies performing gradual drainage over several hours or days (Table 3). Nine studies reported pre- and/or post-PC right heart catheterization data (Table 4), describing significant decreases in RA pressure, mean pulmonary artery pressure, pulmonary vascular resistance, intrapericardial pressure, and higher cardiac index values following the procedure. PDS was noted when studies reported PDS, hemodynamic instability, hypotension, shock, circulatory collapse requiring cardiopulmonary resuscitation, or vasopressor requirement following uncomplicated PC. PDS was the most frequent complication in five (14%) patients (17, 27, 30, 31, 34). Two case reports (27, 30), one abstract (31), one retrospective cohort (13), and one case series (17) (Table 5) reported 30-day all-cause mortality after the intervention. The remaining studies reported marked improvement in clinical status or discharge without complications. Six studies (13, 16, 17, 29, 34, 36) included patients who met the inclusion criteria from within a larger cohort. In these cases, we extracted data from the included patients for our review, and the Supplementary Table shows the study results for all patients in that study (Supplementary Table S8).
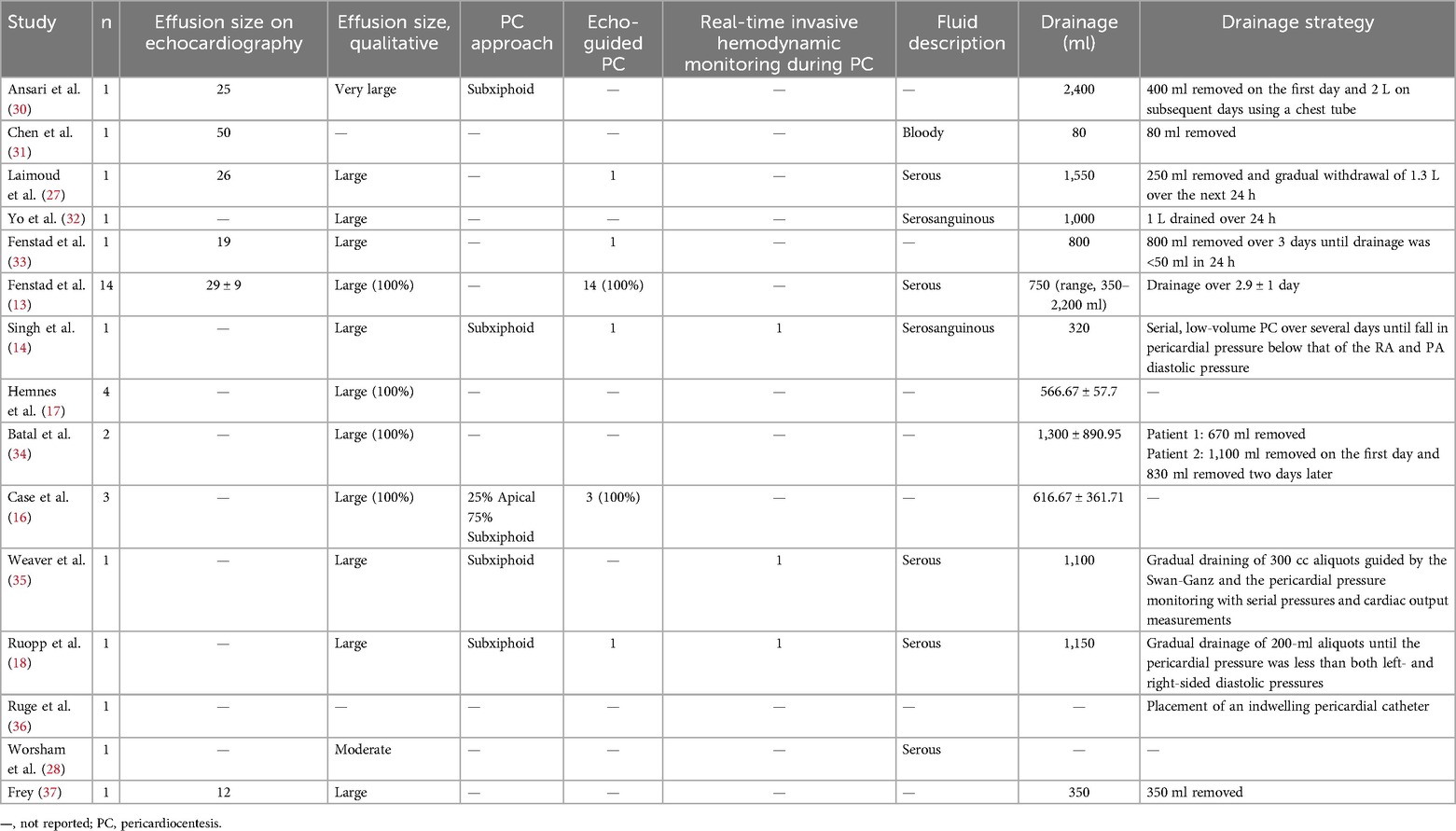
Table 3. Pericardial effusion and pericardiocentesis characteristics in PAH patients.
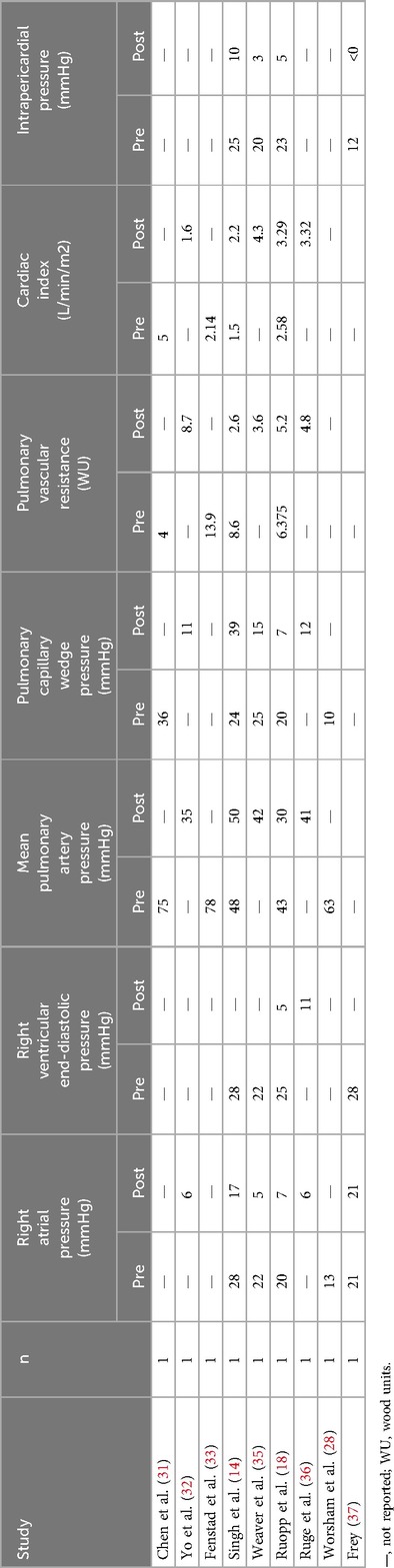
Table 4. Hemodynamic data in PAH patients pre and post-pericardiocentesis.
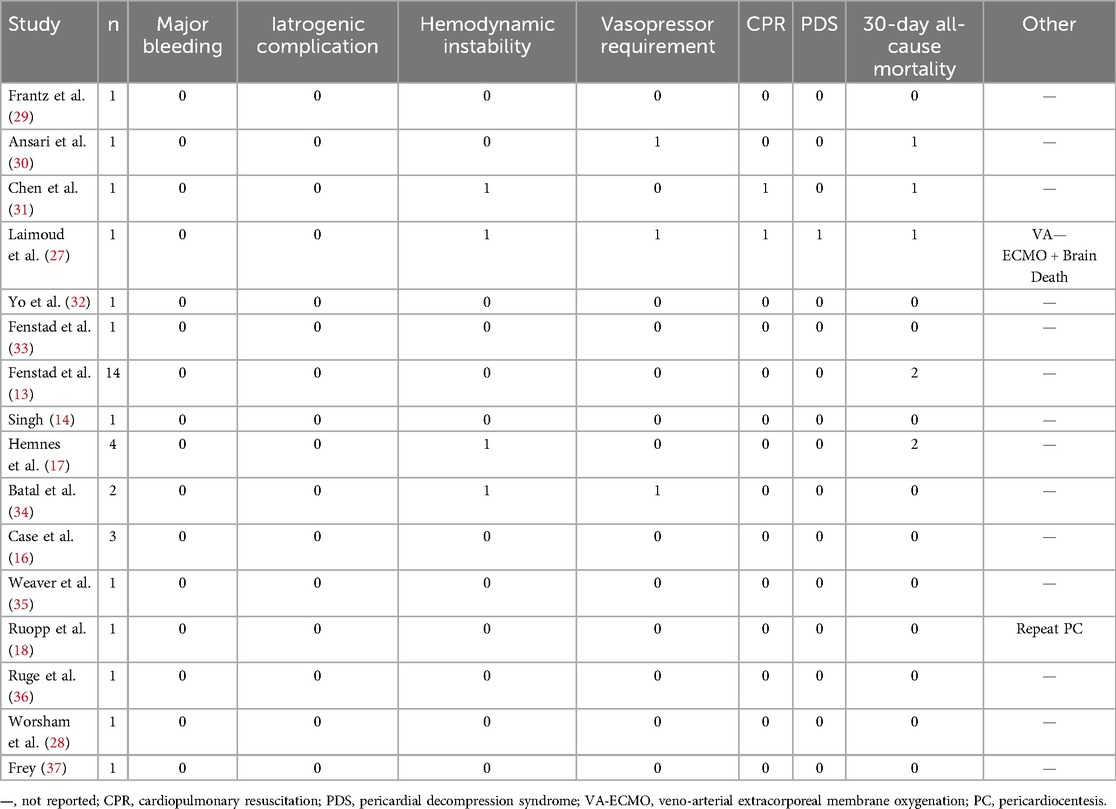
Table 5. 30-day peri-procedural complications and all-cause mortality.
The echocardiographic characteristics reported in patients with PAH and large PE include moderate or more significant RV enlargement and dysfunction, likely related to the underlying PAH. Additionally, studies reported RA collapse (13, 18, 32, 36), RV collapse (14, 18, 32), left atrial (LA) collapse (13, 30, 33), left ventricular (LV) collapse (17, 28, 30, 37), diastolic hepatic vein flow reversal (13, 14, 33), >25% variation in mitral inflow (13, 14, 17, 33), interventricular septum shift (18, 27, 32, 33, 37), and inferior vena cava (IVC) plethora (30) (Table 6).
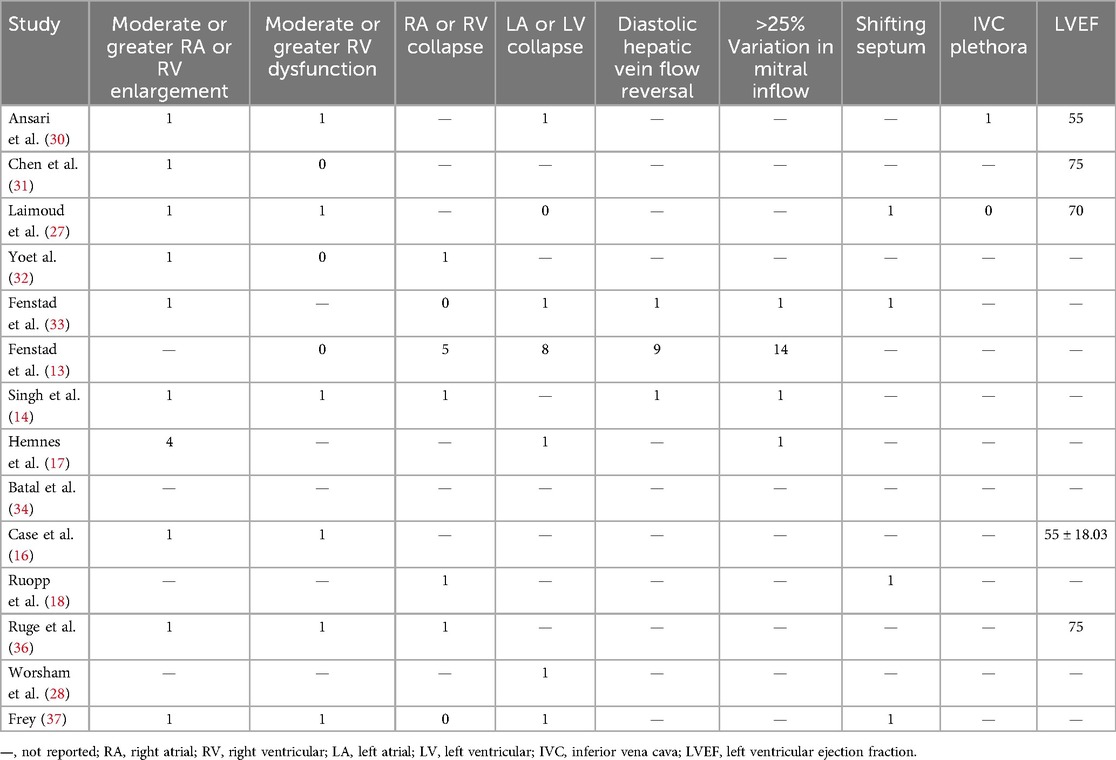
Table 6. Echocardiographic findings in patients with PAH and cardiac tamponade.
Discussion
This is the first systematic review that examines PC safety in patients with PAH presenting with large or hemodynamically significant PE. Our findings are as follows: (1) the most common phenotype consisted of young female patients with CTD-associated PAH; (2) the compiled mortality was 20% (7 of 35 patients), lower than what has been previously reported for PAH patients receiving PC; (3) post-procedure hemodynamic instability, including PDS, was the most frequent periprocedural complication across studies; (4) PC strategies varied, with most patients undergoing gradual drainage over hours or days; (5) most patients presented acutely with dyspnea and peripheral edema; and (6) the most common echocardiographic finding was left-sided chamber diastolic collapse, as opposed to the right-chamber collapse usually observed in cardiac tamponade.
Data regarding mortality rates associated with PC in patients with PAH is controversial, and its safety remains uncertain. Our study observed a 20% overall mortality rate following PC, with a range of 0% to 100%. Similarly, retrospective data from the National Inpatient Sample Database found a 25% unadjusted mortality rate in patients with PAH undergoing PC, which remained elevated after adjusting for confounders (38). Likewise, previous evidence has reported high post-PC mortality (50%) in patients with PAH (12, 17), supporting the use of alternative and more conservative treatment strategies. Conversely, several case reports have demonstrated favorable outcomes following PC in PAH when drainage is performed gradually (10, 14, 33). Differences in mortality rates may be partly explained by clinical heterogeneity within studies, PAH severity, underlying patient comorbidities, effusion size, drainage method, and timing of intervention. In contrast, among non-PAH populations, the complication rates associated with PC are significantly lower, ranging from 4% to 10%, depending on the clinical setting, type of monitoring, and operator skills (39).
Nevertheless, studies examining the outcomes of PC among patients with PAH are limited and do not provide definitive conclusions. Despite these discrepancies, the mortality rate associated with PC in patients with PAH is approximately four times higher than that observed in the general population (40–44). This observation may arise from the diagnostic challenges encountered in this population, where the absence of typical clinical and imaging findings often results in delayed treatment (13, 15, 45). Furthermore, the underlying heart disease may predispose these patients to an increased risk of complications (16, 46), such as PDS, as shown in our study. Additionally, it is essential to note that PE alone is an independent marker of mortality in patients with PAH (2, 10–13). These findings emphasize the importance of careful patient selection and risk assessment in patients with PAH undergoing PC.
Acute hemodynamic deterioration and/or pulmonary edema following PC characterizes PDS, although its definition remains inconsistent and lacks uniform application in clinical settings. Our study identified PDS in 14% of the patients, which differs from the reported general incidence of <5% (47). This discrepancy may be attributed to the underrecognition of the syndrome in the current literature. Nonetheless, studies involving patients with PAH have shown concerning mortality rates, potentially reflecting a less effective hemodynamic response in these patients (17). However, the exact mechanism by which PDS affects patients with PAH is unclear. Vandyke et al. (48) suggested that the sudden return of venous circulation and rapid re-expansion of the right chambers may lead to acute left-sided heart failure as a result of ventricular interdependence.
Additionally, a study evaluating RV changes following PC in patients with and without PH found no improvement in RV function in the PH group, in contrast to the enhanced function observed in patients without PH (49). In this context, RV decompression can lead to massive volume overload, which cannot be offset because of the persistently impaired ventricular function in these patients. An alternative hypothesis is that overdistention of the RV after PC may reduce coronary perfusion, causing RV ischemia. Furthermore, it has been proposed that large PE predominantly occurs in end-stage severe right heart failure in advanced PAH, where the right heart is unable to withstand additional stress due to its already deteriorated condition, even after PC. Further studies are needed to better understand the mechanisms underlying PDS in patients with PAH.
Case reports have recommended gradual decompression during PC in the presence of significant PH to prevent PDS (10, 14, 33). Echocardiography guidance during PC enables the identification of the proper site and the active monitoring of RV dynamics and cardiac output, allowing for the prompt delivery of hemodynamic support if needed. However, only 37.5% of the included studies reported echocardiography-guided PC. Moreover, real-time hemodynamic monitoring during PC allows drainage to continue until the pericardial pressure is below the bi-atrial diastolic pressures while preserving RV structural support to prevent an acute decompensation (18). It also enables the rapid identification of hemodynamic decline and informs the use of vasoactive therapies and more advanced interventions. The included studies that performed PC with a real-time Swan-Ganz and an intrapericardial pressure catheter reported no periprocedural complications. However, although we identified an overall improvement in cardiac hemodynamics after PC, more evidence is needed to identify a possible correlation. Recent evidence suggests that patients with PAH and large PE should undergo a right heart catheterization to evaluate hemodynamics before a pericardial procedure is contemplated (12, 50). Conversely, others propose hemodynamic monitoring immediately after PC for the early identification of impaired tissue perfusion and the need for cardiopulmonary support (27). Additionally, several studies suggest that the immediate use or initiation of PAH-specific therapy may contribute to successful post-drainage outcomes (4, 12). Although our findings suggest that hemodynamic monitoring may improve outcomes, it is essential to emphasize that these data are limited and somewhat anecdotal. This highlights the need for controlled studies that can support this proposal.
Cardiac tamponade typically presents a distinctive clinical presentation characterized by Beck's triad: hypotension due to reduced cardiac output, muffled heart sounds from PE, and jugular venous distention due to impaired venous return (51). In patients with PAH, the presentation of tamponade may differ. Adrian et al. (15) suggest that PAH may initially be a protective factor against cardiac tamponade. The increased pressures in the pulmonary system and RV enable the pericardium to hold a low fluid volume without causing right-chamber collapse. This results in a delayed presentation and rapid progression of symptoms that severely impact cardiac output once the protective effect wanes. Common signs and symptoms include dyspnea, tachycardia, peripheral edema, altered consciousness, and oxygen desaturation (52). Pulsus paradoxus is rarer because of the incapacity of the noncompliant RV to alter its filling volumes in response to the respiratory cycle. Hypotension may also be absent because of the compensatory increase in systemic vascular resistance (11). In our review, dyspnea and peripheral edema were the most frequently reported symptoms. However, these are nonspecific and are often misdiagnosed as right heart failure. As both conditions can present with similar clinical features, cardiac tamponade should be considered in the differential diagnosis of patients with right heart overload symptoms, and a bedside echocardiogram would be essential to rule out the possibility of PE. Early diagnosis is crucial in ensuring timely intervention and improving patient outcomes.
Typical echocardiographic signs of tamponade may be absent in the PAH population because of the increased right-sided pressures that “protect” against the rising pericardial pressure and maintain the RV output (53), concealing the classic presentation of cardiac tamponade. Limited evidence suggests that cardiac tamponade may occur in the absence of right-sided collapse and instead present with isolated effects on left-sided chambers. Signs like systolic RA collapse, RV diastolic collapse, IVC plethora, and reductions in blood flow velocities >25% across the mitral valve during inspiration are more infrequent. Accordingly, LV diastolic collapse occurred in several patients in our review, which is highly unusual and usually only develops in patients with loculated PE or severe PH (54). We also documented LA collapse and >25% variation in mitral flow more often than RA collapse and variation in tricuspid flow, respectively, suggesting a more evident effect of PE on the left heart. In a previous systematic review (15), 82% of patients with PAH had at least one unusual echocardiographic tamponade sign (IVC plethora, increased transvalvular respiratory variation, LA collapse, and LV collapse), and only 10.5% had both RA and RV collapse. This suggests that an echocardiographic evaluation in patients with PAH and a large PE should include a thorough assessment of the LA and LV for early echocardiographic tamponade identification.
Our systematic review has several significant limitations. This retrospective series of reported cases in the current literature has inherent selection and information biases. We included only articles that diagnosed PAH through right-heart catheterization, excluding several studies based on echocardiography diagnoses. While this approach ensured diagnostic accuracy and consistency across studies, it inevitably reduced the overall sample size. As a result, our findings should be interpreted with caution, as the limited number of cases restricts the generalizability of our conclusions. Furthermore, most of the included studies were case reports or small case series, which increases the potential for reporting bias, along with the inclusion of grey literature. The studies exhibited significant heterogeneity due to variations in study design, patient populations, and PC techniques, which complicated the generalization of findings and may have influenced our conclusions. Moreover, the broad definition of PDS may have further contributed to this variability, potentially leading to an overestimation of our findings and limiting comparability across studies. In addition, complete data could not be retrieved from all studies. Some of the conclusions drawn, notably the suggested association between hemodynamic monitoring and improved clinical outcomes, were not clearly supported by specific evidence; prospective, controlled data are needed. The absence of robust data underpinning this claim weakens the overall strength of the clinical recommendations derived from the literature. Also, there was ambiguity regarding the use and reporting of echocardiographic guidance. While echocardiography is regarded as essential in guiding pericardial interventions, only 37% of the studies explicitly reported its use. Whether the remaining studies omitted this technique or failed to report its utilization remains unclear. This inconsistency complicates the interpretation of outcomes and prevents definitive conclusions about the role of echocardiographic guidance in patient management. The heterogeneity among patients with connective tissue disease was not adequately addressed. Specifically, the studies did not differentiate the management strategy between inflammatory pericardial effusions and those associated with advanced right heart failure, two distinct clinical entities with potentially different therapies and prognoses. The lack of subgroup analysis limits the applicability of the findings to these diverse patient populations. Most included studies lacked control groups. This means that causal inferences should be drawn with caution. Finally, as with many systematic reviews, variations in study design, reporting quality, and potential publication bias across the included studies may have influenced the results. These limitations should be considered when interpreting the findings of this review Causal inferences should be drawn with caution.
A significant strength of this systematic review is that it is the first to provide evidence on the safety of PC in patients with PAH associated with tamponade or significant PE. We also employed a comprehensive and methodical approach to evidence collection and data extraction, utilizing multiple major databases and grey literature sources, alongside independent dual-reviewer screening and data extraction processes. Including studies across diverse designs (retrospective cohorts, case series, and case reports) provided a broad perspective on clinical presentations, management strategies, and outcomes of PC in patients with PAH and PE. Additionally, we contacted authors directly to confirm the diagnosis of PAH using right heart catheterization when it was unclear. We included case reports to capture real-world scenarios more effectively and improve the generalizability of our study, which we consider appropriate given the rarity of the studied condition. Despite the overall low quality of the included studies, the review's systematic and exhaustive nature allows for valuable insights into procedural approaches, hemodynamic changes, and potential complications, such as PDS.
Our findings suggest that PC in the setting of large or hemodynamically significant PE in patients with PAH is linked to a high mortality rate (20%) and PDS, particularly among young women with CTD-associated PAH. However, these rates are lower than those previously reported. The clinical presentation often mimics right heart failure, and typical imaging findings may be absent. Therefore, clinicians should prioritize evaluating LV and LA diastolic collapse in the presence of significant PE in patients with PAH. Echocardiography-guided and gradual decompression during PC, with or without real-time hemodynamic monitoring, shows potential for improved outcomes, although further research is needed to confirm these findings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MC-G: Data curation, Visualization, Formal analysis, Methodology, Validation, Supervision, Investigation, Writing – review & editing, Writing – original draft. JR-R: Investigation, Data curation, Writing – original draft, Visualization, Writing – review & editing, Validation, Formal analysis, Supervision, Methodology. CJ-S: Writing – original draft, Methodology, Supervision, Investigation, Visualization, Conceptualization, Funding acquisition, Writing – review & editing, Validation, Formal analysis. MC-P: Visualization, Writing – original draft, Formal analysis, Data curation, Methodology, Investigation, Validation, Writing – review & editing. PG-G: Methodology, Data curation, Writing – original draft, Visualization, Investigation, Validation, Writing – review & editing, Formal analysis. AM-R: Writing – review & editing, Investigation, Validation, Writing – original draft, Methodology, Visualization, Data curation, Formal analysis. EP-G: Investigation, Writing – original draft, Formal analysis, Visualization, Validation, Methodology, Data curation, Writing – review & editing. RQ-S: Formal analysis, Data curation, Visualization, Methodology, Validation, Investigation, Writing – review & editing, Writing – original draft. HD-G: Formal analysis, Data curation, Writing – original draft, Visualization, Investigation, Writing – review & editing, Validation, Methodology. OL-C: Visualization, Methodology, Formal analysis, Investigation, Data curation, Writing – original draft, Writing – review & editing, Validation. JP: Writing – review & editing, Formal analysis, Methodology, Writing – original draft, Validation, Data curation, Investigation, Visualization. RM-A: Formal analysis, Writing – original draft, Visualization, Methodology, Data curation, Writing – review & editing, Validation, Investigation. JM-M: Writing – original draft, Formal analysis, Writing – review & editing, Investigation, Data curation, Methodology, Visualization, Validation. JG-M: Methodology, Formal analysis, Visualization, Writing – review & editing, Writing – original draft, Data curation, Investigation, Validation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1610419/full#supplementary-material
Abbreviations
CTD, connective tissue disease; JVD, jugular venous distension; LA, left atrium/left atrial; LV, left ventricle/left ventricular; PAH, pulmonary arterial hypertension; PC, pericardiocentesis; PDS, pericardial decompression syndrome; PE, pericardial effusion; PH, pulmonary hypertension; RA, right atrium/right atrial; RV, right ventricle/right ventricular; SSc, systemic sclerosis.
References
1. Jerjes-Sánchez C, Ramírez-Rivera A, Hernandez NZ, Cueto Robledo G, García-Aguilar H, Gutiérrez-Fajardo P, et al. Demographic, hemodynamic characteristics, and therapeutic trends of pulmonary hypertension patients: the pulmonary hypertension Mexican registry (REMEHIP). Pulm Circ. (2024) 14(2):e12395. doi: 10.1002/pul2.12395
2. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. (2023) 61(1):2200879. doi: 10.1183/13993003.00879-2022
3. Shimony A, Fox BD, Langleben D, Rudski LG. Incidence and significance of pericardial effusion in patients with pulmonary arterial hypertension. Can J Cardiol. (2013) 29(6):678–82. doi: 10.1016/j.cjca.2012.04.009
4. Honeycutt GR, Safdar Z. Pulmonary hypertension complicated by pericardial effusion: a single center experience. Ther Adv Respir Dis. (2013) 7(3):151–9. doi: 10.1177/1753465812471416
5. Fisher MR, Mathai SC, Champion HC, Girgis RE, Housten-Harris T, Hummers L, et al. Clinical differences between idiopathic and scleroderma-related pulmonary hypertension. Arthritis Rheum. (2006) 54(9):3043–50. doi: 10.1002/art.22069
6. McGoon MD, Miller DP. REVEAL: a contemporary US pulmonary arterial hypertension registry. Eur Respir Rev. (2012) 21(123):8–18. doi: 10.1183/09059180.00008211
7. Escribano-Subias P, Blanco I, López-Meseguer M, Lopez-Guarch CJ, Roman A, Morales P, et al. Survival in pulmonary hypertension in Spain: insights from the Spanish registry. Eur Respir J. (2012) 40(3):596–603. doi: 10.1183/09031936.00101211
8. Stewart RH, Cox CS, Allen SJ, Laine GA. Myocardial edema provides a link between pulmonary arterial hypertension and pericardial effusion. Circulation. (2022) 145(11):793–5. doi: 10.1161/CIRCULATIONAHA.121.057666
9. Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, et al. Predicting survival in pulmonary arterial hypertension: insights from the registry to evaluate early and long-term pulmonary arterial hypertension disease management (REVEAL). Circulation. (2010) 122(2):164–72. doi: 10.1161/CIRCULATIONAHA.109.898122
10. Vallabhajosyula S, Sundaragiri PR. Atypical cardiac tamponade in severe pulmonary hypertension. BMJ Case Rep. (2015) 2015:bcr2014209187. doi: 10.1136/bcr-2014-209187
11. Sahay S, Tonelli AR. Pericardial effusion in pulmonary arterial hypertension. Pulm Circ. (2013) 3(3):467–77. doi: 10.1086/674302
12. Dunne JV, Chou JP, Viswanathan M, Wilcox P, Huang SH. Cardiac tamponade and large pericardial effusions in systemic sclerosis: a report of four cases and a review of the literature. Clin Rheumatol. (2011) 30(3):433–8. doi: 10.1007/s10067-010-1667-0
13. Fenstad ER, Le RJ, Sinak LJ, Maradit-Kremers H, Ammash NM, Ayalew AM, et al. Pericardial effusions in pulmonary arterial hypertension. Chest. (2013) 144(5):1530–8. doi: 10.1378/chest.12-3033
14. Singh A, Mosarla R, Carroll K, Sulica R, Pashun R, Bangalore S, et al. Pericardiocentesis in severe pulmonary arterial hypertension guided by a pulmonary artery catheter. JACC Case Rep. (2024) 29(12):102339. doi: 10.1016/j.jaccas.2024.102339
15. Adrian RJ, Alerhand S, Liteplo A, Shokoohi H. Is pulmonary hypertension protective against cardiac tamponade? A systematic review. Intern Emerg Med. (2024) 19(7):1987–2003. doi: 10.1007/s11739-024-03566-y
16. Case BC, Yang M, Kagan CM, Yerasi C, Forrestal BJ, Tariq MU, et al. Safety and feasibility of performing pericardiocentesis on patients with significant pulmonary hypertension. Cardiovasc Revasc Med. (2019) 20(12):1090–5. doi: 10.1016/j.carrev.2019.09.022
17. Hemnes AR, Gaine SP, Wiener CM. Poor outcomes associated with drainage of pericardial effusions in patients with pulmonary arterial hypertension. South Med J. (2008) 101(5):490–4. doi: 10.1097/SMJ.0b013e31816c0169
18. Ruopp N, Schoenberg N, Farber H. Swan-Ganz and pericardial pressure-guided pericardiocentesis in pulmonary arterial hypertension-associated cardiac tamponade. Ann Am Thorac Soc. (2019) 16(9):1189–91. doi: 10.1513/AnnalsATS.201902-127CC
19. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
20. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. (2022) 43(38):3618–731. doi: 10.1093/eurheartj/ehac237
21. Weitzman LB, Tinker WP, Kronzon I, Cohen ML, Glassman E, Spencer FC. The incidence and natural history of pericardial effusion after cardiac surgery–an echocardiographic study. Circulation. (1984) 69(3):506–11. doi: 10.1161/01.CIR.69.3.506
22. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5(1):210. doi: 10.1186/s13643-016-0384-4
23. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. Br Med J. (2005) 331(7524):1064–5. doi: 10.1136/bmj.38636.593461.68
24. Fowler NO. Cardiac tamponade. A clinical or an echocardiographic diagnosis? Circulation. (1993) 87(5):1738–41. doi: 10.1161/01.CIR.87.5.1738
25. Pradhan R, Okabe T, Yoshida K, Angouras DC, DeCaro MV, Marhefka GD. Patient characteristics and predictors of mortality associated with pericardial decompression syndrome: a comprehensive analysis of published cases. Eur Heart J Acute Cardiovasc Care. (2015) 4(2):113–20. doi: 10.1177/2048872614547975
26. Prabhakar Y, Goyal A, Khalid N, Sharma N, Nayyar R, Spodick DH, et al. Pericardial decompression syndrome: a comprehensive review. WJC. (2019) 11(12):282–91. doi: 10.4330/wjc.v11.i12.282
27. Laimoud M, Machado P, Zadra AR, Maghirang M, Alenazy A. Emergency veno-arterial extracorporeal membrane oxygenation for pericardial decompression syndrome. Case Rep Cardiol. (2022) 2022:1–7. doi: 10.1155/2022/5440635
28. Worsham CM, Lel J, Klings ES. Worsening dyspnea in a patient with connective tissue disease and pulmonary arterial hypertension. Am J Respir Crit Care Med. (2017) 195:A6195. https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2017.195.1_MeetingAbstracts.A6195?role=tab
29. Frantz RP, Kjellstrom B, McGoon M. Ambulatory hemodynamic monitoring in pulmonary arterial hypertension. Adv Pulm Hypertens. (2008) 7(4):405–10. doi: 10.21693/1933-088X-7.4.405
30. Ansari Aval Z, Mirhosseini SM, Jafari Naeini S. Atypical presentation of cardiac tamponade in pulmonary hypertension: a case report and review of the literature. Clin Case Rep. (2021) 9(12):e05218. doi: 10.1002/ccr3.5218
31. Chen E, Wu G, Killu K, Ganesh S. Cardiac arrest after a diagnostic pericardiocentesis in a patient with severe pulmonary arterial hypertension. A60 Reaching for New (Sherman) Heights: Interesting Cases in Pulmonary Thromboembolic Disease; American Thoracic Society (2024). p. A2230. Available online at: https://www.atsjournals.org/doi/10.1164/ajrccm-conference.2024.209.1_MeetingAbstracts.A2230 (Accessed 2024 November 6).
32. Yo S, Thenganatt J, Lipton J, Granton J. Incident pulmonary arterial hypertension associated with bosutinib. Pulm Circ. (2020) 10(3):1–4. doi: 10.1177/2045894020936913
33. Fenstad ER, Kane GC, Frantz RP. 505 pericardial effusion in a patient with pulmonary arterial hypertension. J Heart Lung Transplant. (2011) 30(4):S171. doi: 10.1016/j.healun.2011.01.516
34. Batal O, Dardari Z, Costabile C, Gorcsan J, Arena VC, Mathier MA. Prognostic value of pericardial effusion on serial echocardiograms in pulmonary arterial hypertension. Echocardiography. (2015) 32(10):1471–6. doi: 10.1111/echo.12909
35. Weaver M, Taylor M, El-Kersh K. Swan-Ganz and intra-pericardial pressure guided pericardiocentesis in scleroderma-associated pah. Chest. (2021) 160(4):A2210–1. doi: 10.1016/j.chest.2021.07.1949
36. Ruge M, Fischman DL, Rajapreyar I, Brailovsky Y. The value of right heart catheterization. JACC Case Rep. (2023) 21:101959. doi: 10.1016/j.jaccas.2023.101959
37. Frey MJ. Recognition of cardiac tamponade in the presence of severe pulmonary hypertension. Ann Intern Med. (1989) 111(7):615. doi: 10.7326/0003-4819-111-7-615
38. Vasquez MA, Iskander M, Mustafa M, Quintero-Martinez JA, Luna A, Mintz J, et al. Pericardiocentesis outcomes in patients with pulmonary hypertension: a nationwide analysis from the United States. Am J Cardiol. (2024) 210:232–40. doi: 10.1016/j.amjcard.2023.10.047
39. Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. (2015) 36(42):2921–64. doi: 10.1093/eurheartj/ehv318
40. Kumar R, Sinha A, Lin M, Uchino R, Butryn T, O′Mara MS, et al. Complications of pericardiocentesis: a clinical synopsis. Int J Crit Illn Inj Sci. 2015;5(3):206. doi: 10.4103/2229-5151.165007
41. Tsang TSM, Enriquez-Sarano M, Freeman WK, Barnes ME, Sinak LJ, Gersh BJ, et al. Consecutive 1127 therapeutic echocardiographically guided pericardiocenteses: clinical profile, practice patterns, and outcomes spanning 21 years. Mayo Clin Proc. (2002) 77(5):429–36. doi: 10.1016/S0025-6196(11)62211-8
42. Ball JB, Morrison WL. Cardiac tamponade. Postgrad Med J. (1997) 73(857):141–5. doi: 10.1136/pgmj.73.857.141
43. Callahan JA, Seward JB, Nishimura RA, Miller FA, Reeder GS, Shub C, et al. Two-dimensional echocardiographically guided pericardiocentesis: experience in 117 consecutive patients. Am J Cardiol. (1985) 55(4):476–9. doi: 10.1016/0002-9149(85)90397-2
44. Wybraniec MT, Kampka Z, Drabczyk M, Zielonka M, Urbaniec P, Wypych G, et al. Clinical characteristics and risk factors of in-hospital mortality among patients undergoing percutaneous pericardiocentesis. Front Cardiovasc Med. (2023) 10:1252525. doi: 10.3389/fcvm.2023.1252525
45. Adams JR, Tonelli AR, Rokadia HK, Duggal A. Cardiac tamponade in severe pulmonary hypertension. A therapeutic challenge revisited. Annals ATS. (2015) 12(3):455–60. doi: 10.1513/AnnalsATS.201410-453CC
46. Champion HC. The heart in Scleroderma. Rheum Dis Clin N Am. (2008) 34(1):181–90. doi: 10.1016/j.rdc.2007.12.002
47. Dosios T, Theakos N, Angouras D, Asimacopoulos P. Risk factors affecting the survival of patients with pericardial effusion submitted to subxiphoid pericardiostomy. Chest. (2003) 124(1):242–6. doi: 10.1378/chest.124.1.242
48. Vandyke WH, Cure J, Chakko CS, Gheorghiade M. Pulmonary edema after pericardiocentesis for cardiac tamponade. N Engl J Med. (1983) 309(10):595–6. doi: 10.1056/NEJM198309083091006
49. Alnsasra H, Case BC, Yang M, Rogers T, Satler LF, Asch FM, et al. Pericardiocentesis induced right ventricular changes in patients with and without pulmonary hypertension. Echocardiography. (2021) 38(5):752–9. doi: 10.1111/echo.15046
50. Hosoya H, Derk CT. Clinically symptomatic pericardial effusions in hospitalized systemic sclerosis patients: demographics and management. BioMed Res Int. (2018) 2018:1–6. doi: 10.1155/2018/6812082
51. Sternbach G. Claude beck: cardiac compression triads. J Emerg Med. (1988) 6(5):417–9. doi: 10.1016/0736-4679(88)90017-0
52. Imazio M, De Ferrari GM. Cardiac tamponade: an educational review. Eur Heart J Acute Cardiovasc Care. (2021) 10(1):102–9. doi: 10.1177/2048872620939341
53. Topyła-Putowska W, Tomaszewski M, Wysokiński A, Tomaszewski A. Echocardiography in pulmonary arterial hypertension: comprehensive evaluation and technical considerations. JCM. (2021) 10(15):3229. doi: 10.3390/jcm10153229
Keywords: pulmonary hypertension, pulmonary arterial hypertension, pericardial tamponade, pericardial effusion, pericardial decompression syndrome, mortality
Citation: Cabada-Garcia MJ, Rodriguez-Rivera J, Jerjes-Sanchez C, Castillo-Perez M, Gutierrez-Gallegos P, Martinez-Rodriguez AL, Paredes-Gutierrez E, Quevedo-Salazar RC, De Leon-Gutierrez H, Lopez-Cortes OD, Panneflek J, Monjaras-Alvarado R, Moron-Mosso JA and Gonzalez-Medina JG (2025) Safety of pericardiocentesis in pulmonary arterial hypertension: a systematic review. Front. Cardiovasc. Med. 12:1610419. doi: 10.3389/fcvm.2025.1610419
Received: 12 April 2025; Accepted: 30 July 2025;
Published: 18 August 2025.
Edited by:
Maryanne Caruana, University of Malta, MaltaReviewed by:
Stefano Albani, Azienda USL della Valle d'Aosta, ItalyMohamed Laimoud, Cairo University, Egypt
Copyright: © 2025 Cabada-Garcia, Rodriguez-Rivera, Jerjes-Sanchez, Castillo-Perez, Gutierrez-Gallegos, Martinez-Rodriguez, Paredes-Gutierrez, Quevedo-Salazar, De Leon-Gutierrez, Lopez-Cortes, Panneflek, Monjaras-Alvarado, Moron-Mosso and Gonzalez-Medina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Jerjes-Sanchez, Y2FybG9zLmplcmplc0B1ZGljZW0ub3Jn;Y2FybG9zamVyamVzQHRlYy5teA==