 Cássia da Luz Goulart1,2*
Cássia da Luz Goulart1,2* Vinícius Maldaner3,4Carla Cristina de Araújo Alves1Mauricio Milani1,5,6Juliana Milani1,4Ana Clara Gonçalves da Costa1,3Marcela Lopes Alves1,3Robson Fernando Borges1Claudia Cristina Conde Holanda Sobral1,3Letícia de Araújo Moraes1Jean Carlos Coutinho4Nádia Oliveira Gomes4Leandro Tolfo Franzoni7Filipe Ferrari7Audrey Borghi-Silva2Lawrence P. Cahalin8Graziella França B. Cipriano1,3,8Gerson Cipriano Junior1,4,8Ricardo Stein7,9*
Vinícius Maldaner3,4Carla Cristina de Araújo Alves1Mauricio Milani1,5,6Juliana Milani1,4Ana Clara Gonçalves da Costa1,3Marcela Lopes Alves1,3Robson Fernando Borges1Claudia Cristina Conde Holanda Sobral1,3Letícia de Araújo Moraes1Jean Carlos Coutinho4Nádia Oliveira Gomes4Leandro Tolfo Franzoni7Filipe Ferrari7Audrey Borghi-Silva2Lawrence P. Cahalin8Graziella França B. Cipriano1,3,8Gerson Cipriano Junior1,4,8Ricardo Stein7,9*
- 1Health Sciences and Technologies Post Graduate Program, University of Brasilia (UnB), Brasilia, Brazil
- 2Cardiopulmonary Physiotherapy Laboratory, Physiotherapy Department, Federal University of Sao Carlos, UFSCar, Sao Carlos, Brazil
- 3Rehabilitation Sciences Post Graduate Program, University of Brasilia (UnB), Brasilia, Brazil
- 4Graduate Program in Human Movement and Rehabilitation, Evangelical University of Goias, Hasselt, Brazil
- 5Rehabilitation Research Center (REVAL), Faculty of Rehabilitation Sciences, Hasselt University, Hasselt, Belgium
- 6Department of Cardiology, Heart Centre Hasselt, Jessa Hospital, Hasselt, Belgium
- 7Department of Clinical Medicine, Federal University of Rio Grande do Sul, Porto Alegre, Brazil
- 8Department of Physical Therapy, Miller School of Medicine, University of Miami, Miami, FL, United States
- 9Postgraduate Program in Health Science, Cardiology and Cardiovascular Sciences, Hospital de Clinicas, Porto Alegre, Brazil
Introduction and aim: Long COVID, characterized by persistent symptoms after acute infection, poses a major public health challenge. Understanding its long-term effects is crucial, particularly in relation to cardiorespiratory recovery. This study aimed to assess changes in cardiorespiratory fitness (CRF) and pulmonary function (PF) over 12 months following acute COVID-19, addressing a significant gap in current knowledge about the disease's lasting impact.
Methods: This prospective cohort study included 29 individuals previously diagnosed with post-acute COVID-19. The baseline data were collected during the acute phase of infection. Participants underwent clinical evaluation, cardiopulmonary exercise testing (CPET), spirometry, and maximal inspiratory pressure (MIP) measurement at baseline and again after 12 months.
Results: After one-year, significant improvements were observed across several CPET parameters, including VE/MVV ratio (Cohen's D = 0.66), peak oxygen uptake (VO2peak) in both absolute and relative terms (ml/min: d = 0.67; and ml/kg/min: d = 0.45), oxygen uptake efficiency slope (OUES; D = 0.47) and a reduction in VE/VCO2 slope (D = 0.80). Pulmonary function improved with increases in % predicted forced expiratory volume in 1 s (FEV1; d = 0.67) and forced vital capacity (FVC; D = 0.67). MIP improved significantly (D = 0.67), and the prevalence of inspiratory muscle weakness decreased from 20.7% at baseline to 3.5% at follow-up.
Conclusion: Despite the severity of their initial illness, patients demonstrated substantial recovery in CRF, PF, and inspiratory muscle strength over 12 months.
Introduction
Post-acute COVID-19 syndrome, or long COVID, is a complex, multisystem condition affecting approximately 39%–46% of individuals who recover from acute SARS-CoV-2 infection (1, 2). Characterized by persistent symptoms such as fatigue, dyspnea, muscle weakness, and exercise intolerance, these manifestations can last for 12 weeks or more, significantly impairing quality of life and placing a substantial burden of healthcare systems (3–6). The heterogeneous nature of long COVID presents significant challenges for healthcare providers, as symptoms can persist or emerge months after the initial infection, regardless of the severity of the acute illness (3, 4).
Among its many effects, long COVID has been associated with reductions in cardiorespiratory fitness (CRF), a well-established indicator of overall health (7–9). Even individuals without prior comorbidities may experience decreased exercise capacity and endurance months after infection, often resulting from combined cardiovascular, pulmonary, and peripheral limitations (3, 4). However, the underlying mechanisms contributing to these persistent functional impairments remain incompletely understood, particularly regarding the specific contributions of respiratory muscle dysfunction and pulmonary function abnormalities.
In addition, respiratory muscle dysfunction – particularly inspiratory muscle weakness – had been identified as a key contributor to reduce exercise tolerance in long COVID. Studies have shown that even patients with mild acute illness may exhibit decreased maximum inspiratory pressure (MIP) and phrenic nerve dysfunction, despite the absence of overt (5, 6). The prevalence of pulmonary function abnormalities varies considerably across studies, with reports indicating that 26% of long COVID patients present evidence of reduced pulmonary function. A significant proportion of COVID-19 survivors continue to experience reduced diffusion capacity three and twelve months after discharge, highlighting the persistent nature of these impairments (10). These findings underscore the critical need for comprehensive pulmonary function assessment in long COVID patients, as traditional spirometric measures may not capture the full extent of respiratory impairment (11).
Given the high prevalence and multifactorial nature of long COVID (3, 12), this study, therefore, aimed to evaluate changes in cardiorespiratory fitness, pulmonary function, and respiratory muscle strength over a 12-month period following acute COVID-19 infection.
Methods
Study design and settings
This prospective cohort study was conducted in accordance with the STROBE statement (13) and involved a 12-month follow-up period of individuals previously infected with COVID-19. The patients were evaluated at baseline (during the acute phase of infection in 2020) and 12 months later post the acute phase of infection. Data were collected between 2020 and 2021 at the Laboratory of Clinical Exercise Physiology, University of Brasilia.
Eligible patients were referred for outpatient evaluation and underwent standardized assessment as part of their clinical follow-up. The study protocol was approved by the Medical Ethics Committee of the University of Brasilia (CAAE: 35706720.4.0000.8093), and all procedures adhered to national and international ethical guidelines for human research.
Participants
Adults aged ≥18 years with a confirmed history of symptomatic COVID-19 – diagnosed via reverse transcription-polymerase chain reaction (RT-PCR) – were eligible for inclusion. Participants with pre-existing cardiovascular or pulmonary diseases, clinical instability or conditions that could compromise functional test performance were excluded.
All participants underwent a comprehensive medical evaluation, and COVID-19-specific clinical data were collected through standardized assessments. The severity of the acute illness was classified according to the World Health Organization (WHO) provisional clinical guidance (14).
Recruitment strategy and participant inclusion
Participants were recruited through targeted outreach on social media platforms and via contacts from related studies. Eligible individuals were invited to undergo a series of standardized clinical assessments, including cardiopulmonary exercise testing (CPET), spirometry, and evaluation of inspiratory muscle strength.
Clinical assessments
Collected data included detailed history of COVID-19 infection, hospitalization and discharge information, severity of the acute illness, medical history, and existing comorbidities. These evaluations provided the basis for participant characterization and stratification in subsequent analyses.
Cardiopulmonary exercise testing
After a familiarization session, participants underwent CPET during their first visit laboratory using an electronically braked cycle ergometer (Corival 400, Lode, The Netherlands). A ramp-incremental exercise protocol (5–15 W/min) was employed at a constant cadence of 60 rpm, following a 2-minute warm-up period at 0 W.
Oxygen uptake (VO2) and carbon dioxide production (VCO2) in ml/min, minute ventilation (VE, L/min), and the oxygen uptake efficiency slope (OUES) were measured using a breath-by-breath gas analysis system (Quark CPET, Cosmed, Italy), accompanied by continuous 12-lead electrocardiogram monitoring for heart rate (HR, bpm) (15).
The ventilatory threshold was identified visually using the V-slope method by examining the inflection point on the VCO2 vs. VO2 plot. Maximal effort was confirmed based on the highest 30 sec averaged VO2 and a peak respiratory exchange ratio (RER) ≥ 1.10 (16).
Predicted values for VO2peak (17) and OUES (18) were calculated using reference equations specific to the Brazilian population. Indirect maximal voluntary ventilation (MVV) was estimated as FEV1 × 40. Breathing reserve (%) was calculated using the following formula: breathing Reserve (%) = [(MVV − VE/MVV) × 100 (8).
Lung function by spirometry
Spirometry was performed using a MicroQuark spirometer (Cosmed, Milan, Italy) in accordance with the American Thoracic Society (ATS) guidelines (19). The following variables were assessed: forced expiratory volume at the first second (FEV1), forced vital capacity (FVC), and the FEV1/FVC ratio. Predicted values were based on reference equations for the Brazilian population (20). To ensure safety and prevent cross-contamination between participants and equipment, specific disposable antibacterial/antiviral filters were used during testing.
Respiratory muscle strength by manovacuometry
Inspiratory muscle strength was assessed using a digital manovacuometer (MVD300-U, Globalmed®, Brazil) to measure MIP, following the recommendations of the ATS/European Respiratory Society (21). Predicted MIP values were derived from Sclauser Pessoa et al. (22), and the criteria for identifying inspiratory muscle weakness (IMW) were defined according to Rodrigues et al. (23).
Statistical analysis
Data are presented as mean ± standard deviation (SD), median with interquartile range (IQR), percentages, and 95% confidence intervals (Cis), as appropriate. Normality of the data was assessed using the Shapiro–Wilk test. For within-group comparisons, paired t-tests or Wilcoxon signed-rank tests were applied, depending on data distribution. Categorical variables were analyzed using the McNemar Test. Effects size were calculated using Cohen's D and interpreted as small (0.2–0.49), medium (0.5–0.79), and large (≥0.8) (24). All analyses were conducted using SigmaPlot (Systat Software, Chicago, USA), IBM SPSS Statistics for Mac (version 24.0), and GraphPad Prism (version 7.0, USA).
Results
We initially recruited 45 patients diagnosed with acute COVID-19. However, due to stringent inclusion criteria, 11 patients were excluded: 6 did not meet the eligibility criteria, 3 declined participation, and 2 who were lost to follow-up. This resulted in a final cohort of 34 patients, of whom 29 successfully completed all assessments, as illustrated in Figure 1.
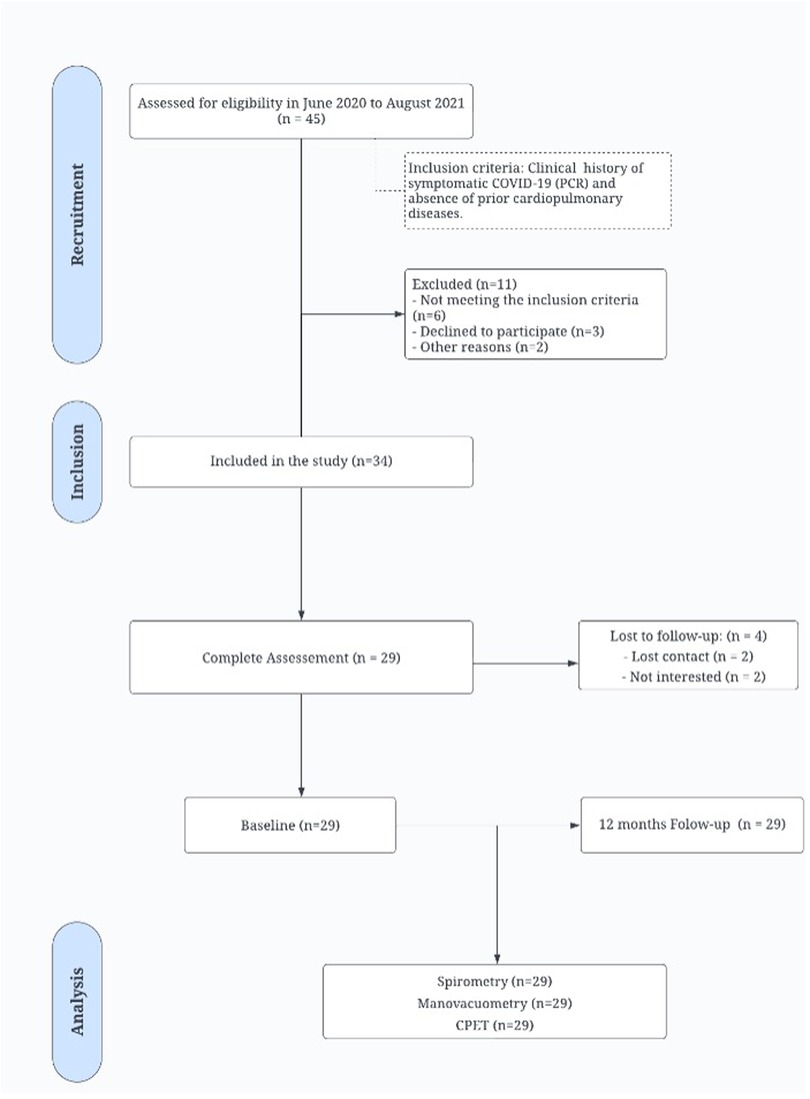
Figure 1. STROBE flow chart. This chart illustrates the patient identification, inclusion, follow-up, and analysis process in the study. CPET, Cardiopulmonary exercise testing.
A follow-up evaluation conducted 12 months after the initial assessment revealed that most patients had experienced severe illness during the acute phase of COVID-19, with hypertension being the most prevalent comorbidity. Comparisons between baseline and follow-up revealed no significant differences in demographic characteristics (p > 0.05), as detailed in Table 1.
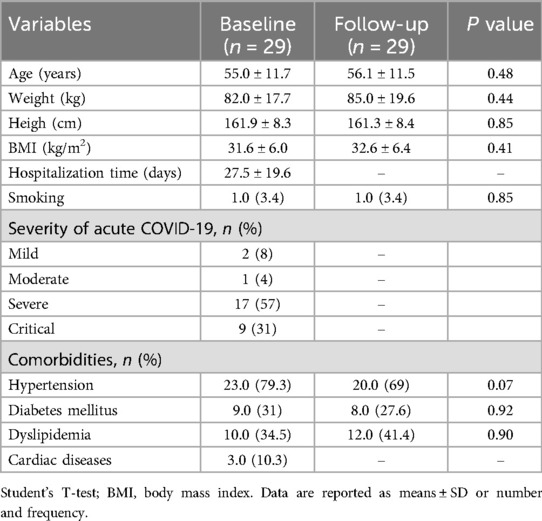
Table 1. Baseline characteristics of the study participants.
As shown in Table 2, CRF analyses at the 12-month follow-up revealed significant improvements in several measures, including an increase in the VE/MVV (Cohen's D = 0.66; p = 0.001), VO2peak in both ml/min and ml/kg/min (p = 0.002, Cohen's D = 0.67 p = 0.037, Cohen's D 0.45), and the OUES (p = 0.032, Cohen's D = 0.47). Additionally, there was a reduction in the VE/VCO2 slope (p = 0.001, Cohen's D = 0.80) (Table 2).
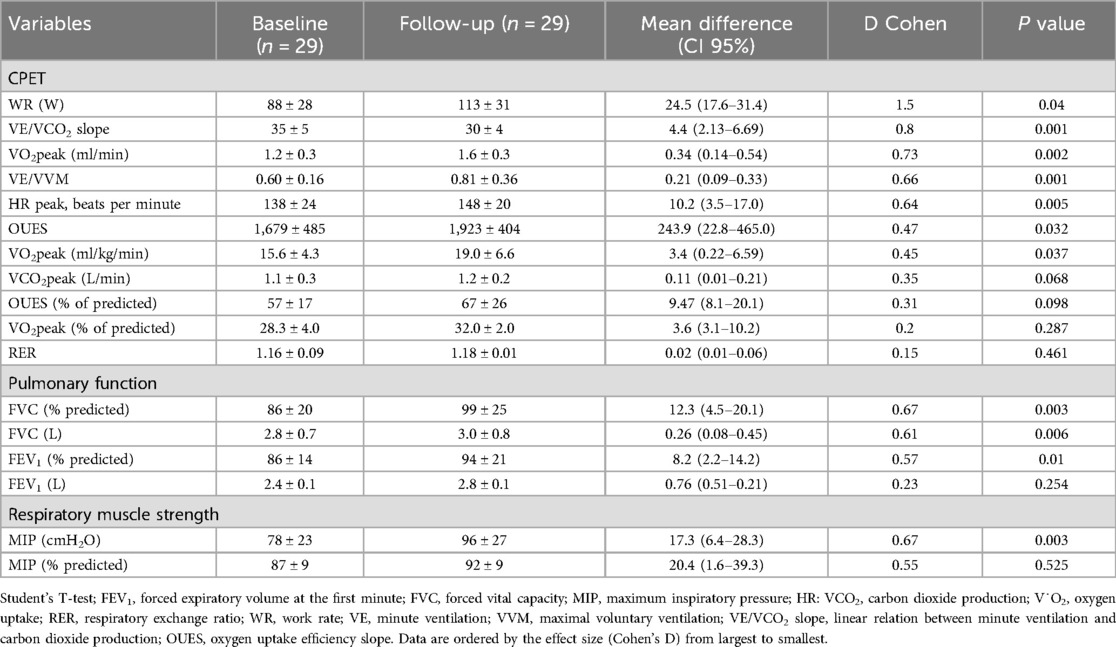
Table 2. Pulmonary function, respiratory muscle strength, and cardiopulmonary exercise testing (CPET) at baseline and follow-up.
Significant improvements were also observed in the % of predicted FEV1 and % of predicted FVC (p = 0.010, Cohen's D = 0.57 and p = 0.003, Cohen's D = 0.67, respectively) (Table 2).
Table 2 shows that MIP increased significantly from 78 ± 23 to 96 ± 27 cmH2O (p < 0.05, Cohen's D = 0.67). Figure 2 illustrates the prevalence of IMW (22, 23) and reduced inspiratory muscle strength (RIMS) at baseline and 12-months post-COVID. IMW decreased significantly from 20.69% at baseline to 3.45% at follow-up (p = 0.007), while RIMS also decreased, approaching significance, from 17.64% at baseline to 3.45% at follow-up (p = 0.084).
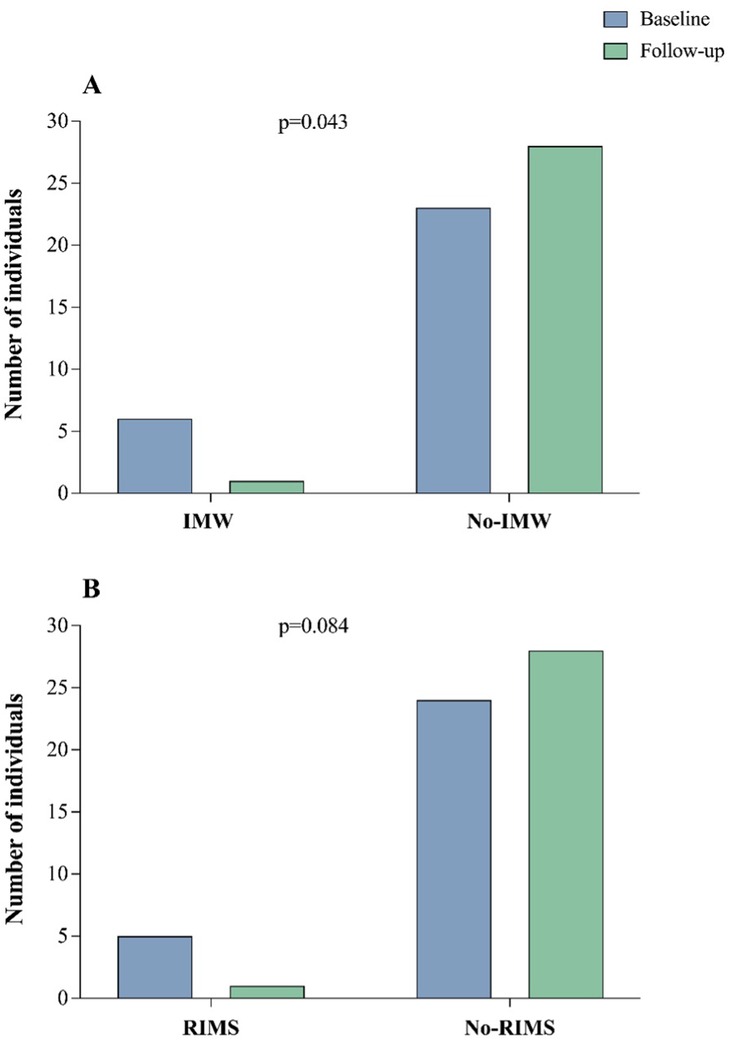
Figure 2. Comparison of inspiratory muscle weakness and reduced inspiratory muscle strength between baseline and follow-up. This figure illustrates in (A): the changes in the prevalence of inspiratory muscle weakness (IMW) and in (B): reduced inspiratory muscle strength (RIMS) from baseline to 12-month follow-up. Statistical analysis was performed using the Chi-square test to evaluate differences between the two-time points.
Figure 3 provides individual and average responses of key ventilatory, hemodynamic, gas exchange, and oxygen consumption variables after 12 months, highlighting marked improvements in all assessed parameters (p < 0.005). These findings underscore the substantial recovery in CRF, pulmonary function, and inspiratory muscle strength in patients following acute COVID-19 infection.
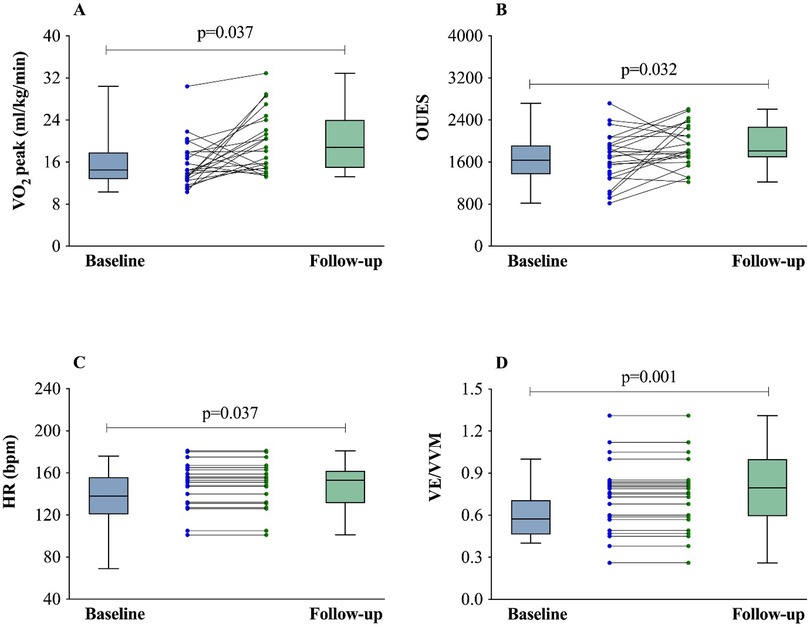
Figure 3. (A–D) Comparison between baseline and follow-up of VO2 (L/kg/min), OUES, HR peak (bpm), and VE/VVM. OUES, oxygen uptake efficiency slope; VO2, oxygen uptake; VE, minute ventilation; VVM, maximal voluntary ventilation; HR: heart rate. Student's T-test.
Discussion
This study thoroughly assessed the long-term effects of COVID-19 survivors, with a specific focus on CRF, pulmonary function, and RIMS over a 12-month period following infection. The results demonstrated significant improvements in these domains, signaling a notable recovery in patients who had experienced acute COVID-19. The main findings of this study were significant improvements in VO2 peak, VE/VVM, and OUES, with a reduction in the VE/VCO2 slope, which were associated with significant improvements in MIP, FEV1, and FVC. Additionally, a decrease in the frequency of IMW from baseline to follow-up was also observed and likely contributed to many of the above findings.
CPET is a comprehensive diagnostic tool that assesses the integration of the cardiovascular, pulmonary, and metabolic systems during physical exercise (25). CPET provides valuable information about functional capacity and the underlying mechanisms of exercise intolerance in different populations, including patients affected by COVID-19 (26). Previous studies have demonstrated changes in pulmonary function, reduced exercise capacity, and abnormalities in the cardiopulmonary response in post-COVID patients, suggesting a lasting and limiting impact of the infection (26).
One of the key findings was the improvement in VO2 peak, as it is a fundamental measure of aerobic capacity and a crucial determinant of overall health and functionality (27, 28). The increase in VO2 peak, alongside the reduction in the VE/VCO2 slope, suggests an enhanced ventilatory efficiency during exercise, possibly reflecting better pulmonary gas exchange and reduced ventilatory demand during exercise (29). Additionally, the improvement in OUES further supports greater cardiovascular and respiratory efficiency, which is likely to result in better outcomes for patients with long COVID (18).
The study also documented significant improvements in FEV1 and FVC, indicating greater lung volume and flow in patients who experienced mostly severe COVID-19 and restrictive lung defects commonly observed following severe viral infections. The improvements in these parameters suggest a potential reversal of such defects, which is a positive outcome for patients experiencing prolonged effects from long COVID. Recent studies have demonstrated that post-infection COVID-19 patients frequently show impaired lung function, with the diffusion capacity for carbon monoxide (DLCO) being the most consistently affected parameter (30). While our study did not specifically assess DLCO, the improvements in FEV1 and FVC suggest that the restrictive patterns commonly observed in post-COVID patients may be more reversible than initially anticipated.
Improvement in RMS was another critical observation, marked by increased MIP and a reduced frequency of IMW. These enhancements reflect strengthened respiratory muscles, essential for reducing the risk of future respiratory complications and enhancing patients' ability to perform daily activities, there enhancing their quality of life (31). The improvement in ventilatory efficiency, demonstrated by the increase in VE/MVV, indicates better management of ventilatory capacity and reduced hyperinflation (8). This is particularly relevant for long COVID-19 patients, who often face issues with air trapping and lung stiffness.
The observed improvements across various metrics suggest potential benefits from monitoring and supporting natural recovery in COVID-19 survivors. While the data indicate that patients may experience significant enhancements in CRF, pulmonary function, and respiratory muscle strength, caution must be exercised before attributing these outcomes to specific rehabilitation interventions due to the observational nature of this study.
Strengths and limitations
The limitations of this study include the absence of a control group, which restricts our ability to distinguish the specific impacts attributable solely to COVID-19 from those due to natural recovery processes or other interventions. Additionally, the single-center design may limit the generalizability of the results across different populations and settings. Future research should extend the follow-up period beyond the current 12-month timeframe to deepen our understanding of long COVID. Incorporating additional follow-up assessments at 18, 24 months, and beyond would offer valuable insights into the long-term progression or resolution of symptoms and functional impairments associated with COVID-19. Furthermore, future studies could explore the effectiveness of specific rehabilitation interventions, such as aerobic exercise programs or respiratory muscle training, in improving long-term outcomes in COVID-19 survivors.
Conclusion
This 12-month observational study highlights both the persistent challenges and the significant potential for recovery in individuals with long COVID. Our findings demonstrate substantial improvements in CRF, pulmonary function, and RIMS. The reduction in inspiratory muscle weakness prevalence from 20.69% to 3.45%, accompanied by significant improvements in MIP, FEV1, and FVC, demonstrates that meaningful recovery is possible even in patients who experienced severe acute illness.
These results underscore the possibility of considerable physiological recovery over time, emphasizing the importance of ongoing monitoring and personalized rehabilitation strategies to optimize outcomes in the management of long COVID. The relationship between respiratory muscle strength and overall functional capacity highlights the critical importance of comprehensive respiratory muscle assessment. Future research should extend the follow-up period beyond the current 12-month timeframe to deepen our understanding of long COVID recovery patterns and explore the effectiveness of specific rehabilitation interventions in improving long-term outcomes in COVID-19 survivors.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Brasilia (CAAE: 35706720.4.0000.8093). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
CG: Project administration, Conceptualization, Methodology, Writing – original draft, Writing – review & editing. VM: Writing – review & editing, Project administration, Writing – original draft. CA: Writing – original draft, Writing – review & editing. MM: Methodology, Writing – review & editing, Investigation, Writing – original draft. JM: Investigation, Writing – original draft, Writing – review & editing. AG: Writing – original draft, Writing – review & editing, Investigation. MA: Writing – review & editing, Writing – original draft. RB: Writing – review & editing, Writing – original draft, Conceptualization. CS: Investigation, Writing – original draft, Writing – review & editing. LM: Writing – original draft, Writing – review & editing. JC: Writing – review & editing, Conceptualization, Writing – original draft. NG: Writing – review & editing, Writing – original draft. LT: Writing – review & editing, Writing – original draft. FF: Investigation, Writing – review & editing, Writing – original draft. AB-S: Writing – original draft, Writing – review & editing, Investigation. LC: Writing – original draft, Investigation, Writing – review & editing. GFBC: Writing – original draft, Conceptualization, Writing – review & editing. GCJ: Methodology, Writing – original draft, Visualization, Investigation, Project administration, Writing – review & editing. RS: Investigation, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. National Council for Scientific and Technological Development/Ministry of Science, Technology, and Innovation (CNPq/MCTI) (Grant number: 444823/2023/9) and the Research Incentive Fund of Hospital de Clínicas de Porto Alegre (FIPE-HCPA), Porto Alegre, Brazil.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. López-León S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. SSRN Electron J. (2021) 9;11(1):16144. doi: 10.2139/ssrn.3769978
2. Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global prevalence of post-coronavirus disease 2019 (COVID-19) condition or long COVID: a meta-analysis and systematic review. J Infect Dis. (2022) 226:1593–607. doi: 10.1093/infdis/jiac136
3. Ngamsutham T, Chaiwong W, Dacha S, Sitilertpisan P, Pothirat C, Duangjit P, et al. Pulmonary function, functional capacity, respiratory, and locomotor muscle strength after severe to critically ill COVID-19: a long-term study. Tuberc Respir Dis (Seoul). (2024) 87:532–42. doi: 10.4046/trd.2024.0044
4. Tanriverdi A, Savci S, Kahraman BO, Ozpelit E. Extrapulmonary features of post-COVID-19 patients: muscle function, physical activity, mood, and sleep quality. Ir J Med Sci. (2022) 191:969–75. doi: 10.1007/s11845-021-02667-3
5. Vonbank K, Nics H, Zwick RH, Maasz J, Sabic B, Potzmann M, et al. Decreased phrenic nerve compound muscle action potential, inspiratory muscle strength, and exercise capacity after COVID-19. Front Neurol. (2024) 14. doi: 10.3389/fneur.2023.1308443
6. Hennigs JK, Huwe M, Hennigs A, Oqueka T, Simon M, Harbaum L, et al. Respiratory muscle dysfunction in long-COVID patients. Infection. (2022) 50:1391–7. doi: 10.1007/s15010-022-01840-9
7. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021) 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
8. Goulart C da L, Arêas GPT, Milani M, Borges FF dos R, Magalhães JR, Back GD, et al. Sex-based differences in pulmonary function and cardiopulmonary response 30 months post-COVID-19: a Brazilian multicentric study. Int J Environ Res Public Health. (2024) 21:1293. doi: 10.3390/ijerph21101293
9. Güneş M, Yana M, Güçlü MB. Physical activity levels respiratory and peripheral muscle strength and pulmonary function in young post-COVID-19 patients. Wien Klin Wochenschr. (2023) 135:251–9. doi: 10.1007/s00508-023-02204-5
10. Torres-Castro R, Vasconcello-Castillo L, Alsina-Restoy X, Solis-Navarro L, Burgos F, Puppo H, et al. Respiratory function in patients post-infection by COVID-19: a systematic review and meta-analysis. Pulmonology. (2021) 27:328–37. doi: 10.1016/j.pulmoe.2020.10.013
11. Kavalcı Kol B, Boşnak Güçlü M, Baytok E, Yılmaz Demirci N. Comparison of the muscle oxygenation during submaximal and maximal exercise tests in patients post-coronavirus disease 2019 syndrome with pulmonary involvement. Physiother Theory Pract. (2025) 41:275–88. doi: 10.1080/09593985.2024.2327534
12. Karaarslan F, Güneri FD, Kardeş S. Long COVID: rheumatologic/musculoskeletal symptoms in hospitalized COVID-19 survivors at 3 and 6 months. Clin Rheumatol. (2022) 41:289–96. doi: 10.1007/s10067-021-05942-x
13. Malta M, Cardoso LO, Bastos FI, Magnanini MMF, da Silva CMFP. STROBE initiative: guidelines on. Rev Saúde Pública. (2010) 44:1–5. Available online at: doi: 10.1590/s0034-89102010000300021
14. Diaz J, Appiah J, Askie L, Baller A, Banerjee A, Barkley S. The Severity of the Acute Illness was Defined by the Provisional Clinical Guidance of the World Health Organization (WHO). New York, NY: World Health Organization. (2021). Available online at: https://iris.who.int/bitstream/handle/10665/349321/WHO-2019-nCoV-clinical-2021.2-eng.pdf
15. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol. (1986) 60:2020–7. doi: 10.1152/jappl.1986.60.6.2020
16. Guazzi M, Adams V, Conraads V, Halle M, Mezzani A, Vanhees L, et al. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur Heart J. (2012) 33:2917–27. doi: 10.1093/eurheartj/ehs221
17. Milani M, Milani JGPO, Cipriano GFB, de Castro I, Cipriano Junior G. Reference standards for cardiorespiratory fitness in Brazil. J Cardiopulm Rehabil Prev. (2022) 42:366–72. doi: 10.1097/HCR.0000000000000690
18. Milani JGPO, Milani M, Cipriano GFB, de Castro I, Hansen D, Cipriano Junior G. Oxygen uptake efficiency slope in south American healthy adults. J Cardiopulm Rehabil Prev. (2023) 43:290–300. doi: 10.1097/HCR.0000000000000778
19. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. ATS/ERS task force: standardisation of lung function testing. Eur Respir J. (2005) 26:319–38. doi: 10.1183/09031936.05.00034805
20. Alberto C, Pereira DC, Sato T. New reference values for forced spirometry in white adults in Brazil *. J Bras Pneumol. (2007) 33(4):397–406. doi: 10.1590/s1806-37132007000400008
21. Gibson GJ, Whitelaw W, Siafakas N, Supinski GS, Fitting JW, Bellemare F, et al. ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med. (2002) 166:518–624. doi: 10.1164/rccm.166.4.518
22. Pessoa IMS, Parreira VF, Fregonezi GA, Sheel AW, Chung F, Reid WD. Reference values for maximal inspiratory pressure: a systematic review. Can Respir J. (2014) 21:43–50. doi: 10.1155/2014/982374
23. Rodrigues A, Da Silva ML, Berton DC, Cipriano G, Pitta F, O’Donnell DE, et al. Maximal inspiratory pressure. Chest. (2017) 152:32–9. doi: 10.1016/j.chest.2016.11.045
24. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New York, NY: Lawrence Erlbaum Associates (1988). Available online at: https://doi.org/10.4324/9780203771587
25. Herdy AH, Ritt LEF, Stein R, Araújo CGS, Milani M, Meneghelo RS, et al. Cardiopulmonary exercise test: fundamentals, applicability and interpretation. Arq Bras Cardiol. (2016) 107(5):467–81. doi: 10.5935/abc.20160171
26. Durstenfeld MS, Sun K, Tahir P, Peluso MJ, Deeks SG, Aras MA, et al. Use of cardiopulmonary exercise testing to evaluate long COVID-19 symptoms in adults: a systematic review and meta-analysis. JAMA Netw Open. (2022) 5:E2236057. doi: 10.1001/JAMANETWORKOPEN.2022.36057
27. Norweg A, Yao L, Barbuto S, Nordvig AS, Tarpey T, Collins E, et al. Exercise intolerance associated with impaired oxygen extraction in patients with long COVID. Respir Physiol Neurobiol. (2023) 313:104062. doi: 10.1016/j.resp.2023.104062
28. Jamieson A, Al Saikhan L, Alghamdi L, Hamill Howes L, Purcell H, Hillman T, et al. Mechanisms underlying exercise intolerance in long COVID: an accumulation of multisystem dysfunction. Physiol Rep. (2024) 12. doi: 10.14814/phy2.15940
29. Arena R, Humphrey R, Peberdy MA. Prognostic ability of VE/VCO 2 slope calculations using different exercise test time intervals in subjects with heart failure. Eur J Cardiovasc Prev Rehabil. (2003) 10:463–8. doi: 10.1097/01.hjr.0000102817.74402.5b
30. Fortini A, Rosso A, Cecchini P, Torrigiani A, Lo Forte A, Carrai P, et al. One-year evolution of DLCO changes and respiratory symptoms in patients with post COVID-19 respiratory syndrome. Infection. (2022) 50:513–7. doi: 10.1007/s15010-022-01755-5
Keywords: COVID-19, CPET, lung function, functional capacity, recovery
Citation: Goulart CdL, Maldaner V, Alves CCdA, Milani M, Milani J, Gonçalves da Costa AC, Alves ML, Borges RF, Sobral CCCH, Moraes LdA, Coutinho JC, Gomes NO, Tolfo Franzoni L, Ferrari F, Borghi-Silva A, Cahalin LP, Cipriano GFB, Cipriano Junior G and Stein R (2025) Recovery from COVID-19: a 12-month follow-up study on cardiorespiratory fitness and pulmonary function. Front. Cardiovasc. Med. 12:1638317. doi: 10.3389/fcvm.2025.1638317
Received: 30 May 2025; Accepted: 25 July 2025;
Published: 12 August 2025.
Edited by:
Diana C. Sanchez-Ramirez, University of Manitoba, CanadaReviewed by:
Warawut Chaiwong, Chiang Mai University, ThailandMusa Gunes, Karabük University, Türkiye
Copyright: © 2025 Goulart, Maldaner, Alves, Milani, Milani, Gonçalves da Costa, Alves, Borges, Sobral, Moraes, Coutinho, Gomes, Tolfo Franzoni, Ferrari, Borghi-Silva, Cahalin, Cipriano, Cipriano Junior and Stein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cássia da Luz Goulart, bHV6LmNhc3NpYUBob3RtYWlsLmNvbQ==; Ricardo Stein, cnN0ZWluQGNhcmRpb2wuYnI=