Abstract
Mirror-image dextrocardia combined with absence of the hepatic segment of the inferior vena cava (IVC) and continuation of the azygos vein represents an extremely rare dual anatomical variation that significantly increases the technical complexity of leadless pacemaker (LP) implantation. This paper presents a 28-year-old male patient who required permanent pacing therapy due to third-degree atrioventricular block. Preoperative computed tomography angiography (CTA) clearly identified the aforementioned malformations. A Micra AV leadless pacemaker was subsequently implanted successfully via the left internal jugular vein. During the procedure, image mirroring technology was employed to assist the operation, ensuring precise deployment and stable parameters. This case marks the world's first successful LP implantation via the internal jugular vein in a patient with such complex anatomical variations, offering a novel, safe, and feasible approach for similar patients.
Introduction
Mirror-image dextrocardia is a rare congenital malformation, with an incidence of approximately 0.01%, is characterized by the heart's location in the right thoracic cavity and a mirror-image arrangement of the atria, ventricles, and great vessels relative to their normal anatomic positions.
It is frequently associated with other cardiovascular anomalies, which notably increases the difficulty of interventional procedures (1, 2). LPs have emerged as a preferred option for certain patients because they obviate the need for leads and pockets (3). However, when accompanied by the absence of the hepatic segment of the IVC and continuation of the azygos vein (incidence of around 0.6%), the conventional femoral vein approach often fails due to pronounced tortuosity and angulation (4, 5). Although some studies have explored alternative routes via the azygos vein or internal jugular vein (2, 4, 5), there have been no reports of LP implantation via the internal jugular vein in the context of mirror-image dextrocardia. In this case, preoperative CTA precisely identified the dual anatomical variations. The successful implantation of a Micra AV device via the left internal jugular vein, assisted by image mirroring technology during the procedure, resulted in optimal pacing parameters. This marks the world's first such case and provides a novel strategy for patients with complex anatomical conditions.
Case report
A 28-year-old male, Eighteen years prior, he was diagnosed at an outside hospital with ventricular septal defect (VSD) combined with mirror-image dextrocardia and absence of the hepatic segment of the IVC.And he underwent surgical repair for VSD. Postoperatively, he developed third-degree atrioventricular block (AVB), which was not treated further. On admission, physical examination revealed no significant abnormalities, and all laboratory test results were within normal limits.
Echocardiography revealed mirror-image dextrocardia, a post-VSD repair status, and no evidence of ventricular-level shunting. Electrocardiography (performed with left and right hand electrodes reversed) demonstrated sinus rhythm, third-degree AVB, junctional escape rhythm, and complete right bundle branch block (Figure 1A). Chest radiography confirmed mirror-image dextrocardia (Figure 1B). CTA of the great vessels showed that the IVC was located on the left side of the aorta, with absence of its hepatic segment. The IVC ascended and connected to the right superior vena cava via a dilated azygos vein. The suprarenal portion of the IVC exhibited luminal stenosis, with the narrowest diameter measuring approximately 8.5 mm, while the hepatic veins drained directly into the right atrium (Figure 2). The patient fulfilled the Class I indication for pacemaker implantation (6). However, he declined a conventional lead-based pacing system and instead opted for leadless pacemaker implantation.
Figure 1
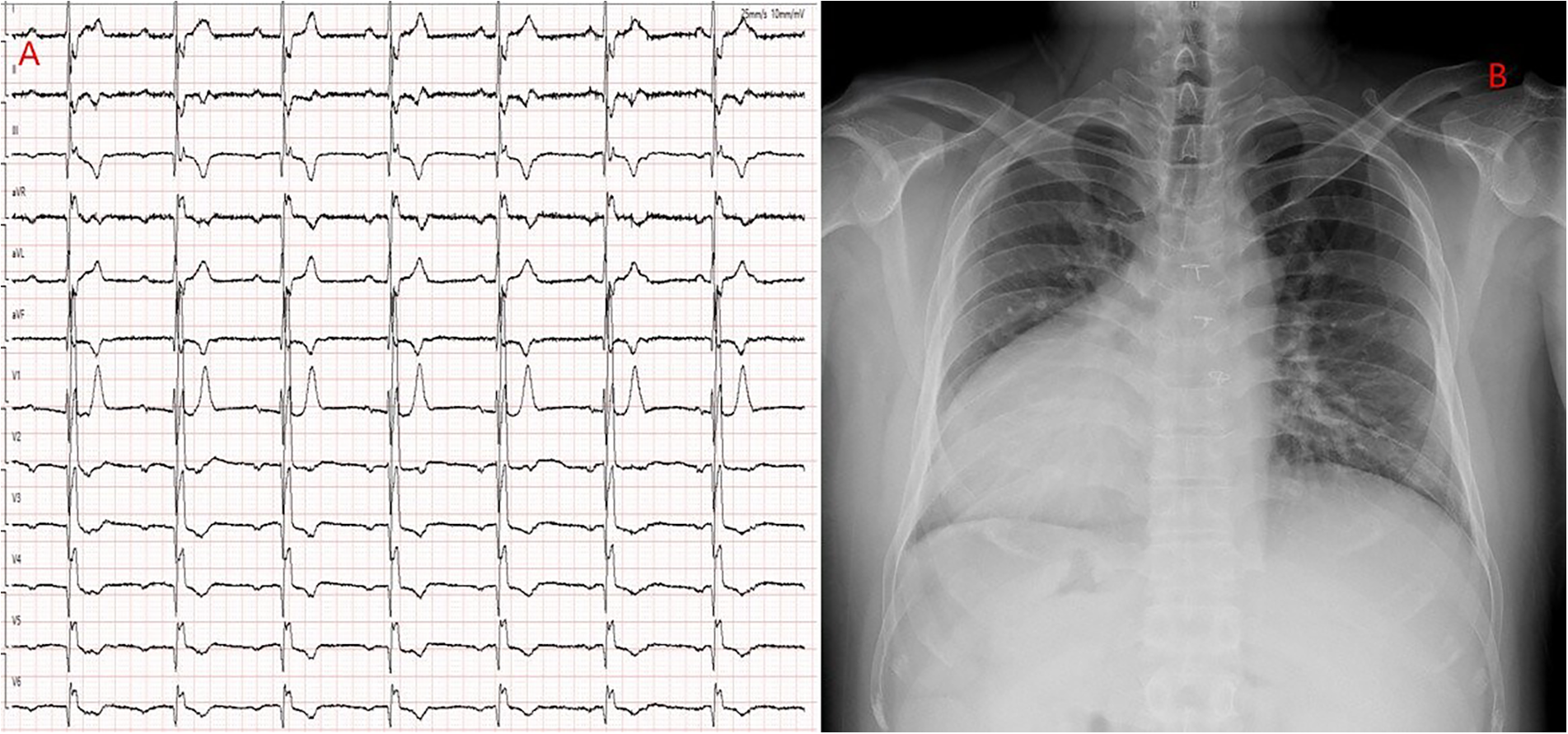
(A) ECG with reversed limb leads: Shows third-degree atrioventricular block and complete right bundle branch block. (B) Chest x-ray: Demonstrates a mirrored right-sided heart.
Figure 2
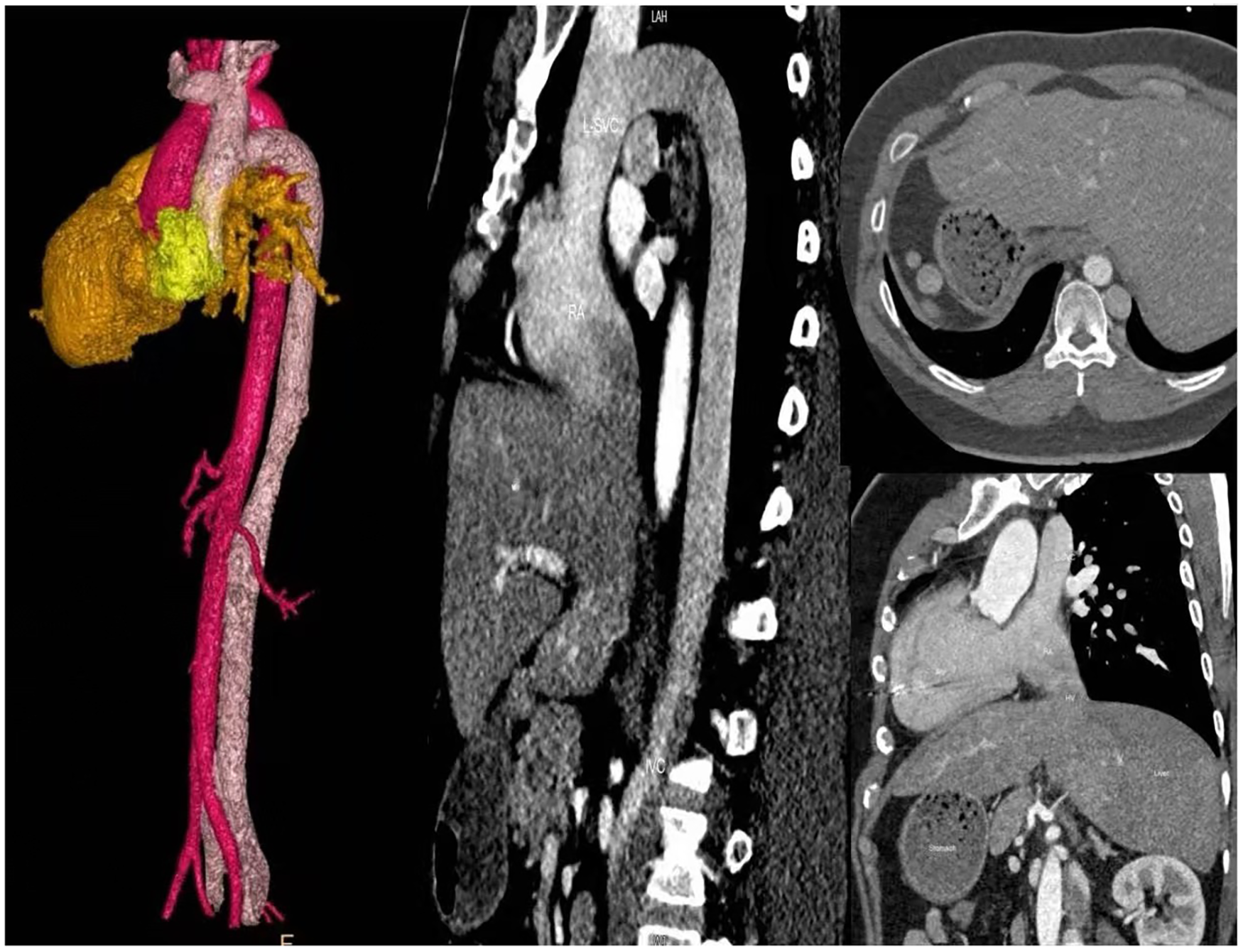
Chest and abdominal large vessel CTA: Absence of the hepatic segment of the inferior vena cava (IVC); the left-sided azygos vein is thickened and extends to the right superior vena cava (SVC); hepatic veins drain directly into the right atrium.
A routine surgical procedure was carried out, including disinfection and draping. Fluoroscopy was utilized to verify the mirror-image positioning of the heart (Figure 3A). To align the operator's field of view with the conventional anatomical orientation, the x-ray image was horizontally mirrored using computer adjustments (Figure 3B).
Figure 3
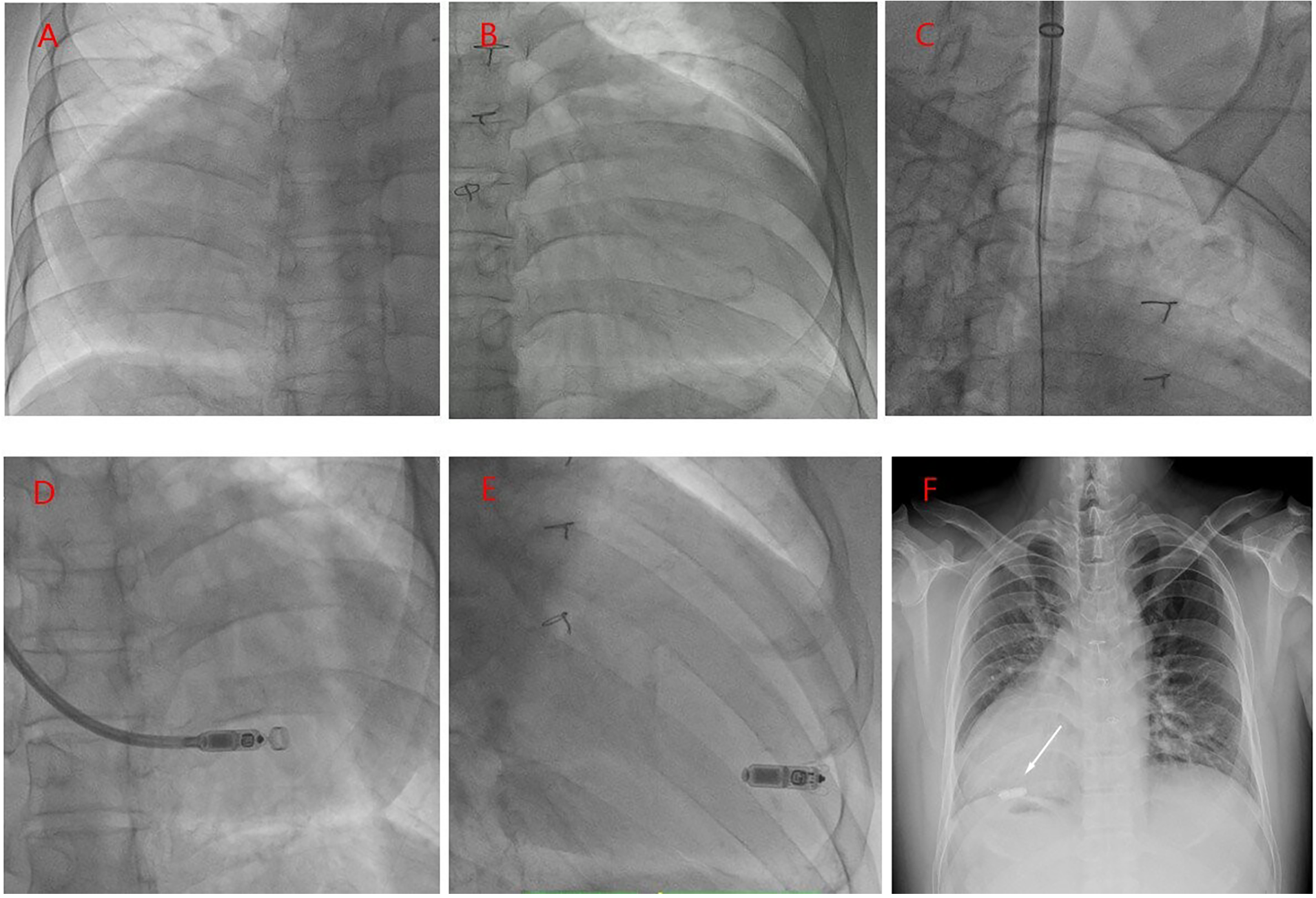
(A) RAO 30° fluoroscopy: Confirms a right-sided heart. (B) RAO 30° digital mirror view. (C) A 25 F delivery sheath was inserted via the left internal jugular vein, with its tip positioned in the right atrium. (D) A pre-loaded Micra AV controllable curved delivery system was advanced through the sheath, traversing the tricuspid valve and entering the anatomical right ventricle. (E) The leadless pacemaker was gradually deployed, with its distal tip anchored in the mid to lower ventricular septum. (F) Postoperative chest x-ray: The leadless pacemaker (white arrow) is correctly positioned against the mid-low ventricular septum without evidence of displacement.
A 6F sheath was introduced into the left femoral vein, and a temporary pacing electrode was placed. However, attempts to maneuver the electrode through the tortuous and angulated azygos vein to the superior vena cava (SVC) were unsuccessful. Subsequently, a 9F sheath was inserted into the right femoral vein, and angiography of the IVC and azygos vein was performed using a pigtail catheter. The imaging revealed that the azygos vein extended to the level of the tracheal bifurcation before turning and connecting to the right atrium. Despite repeated adjustments, positioning the temporary pacemaker into the right ventricle remained challenging. Given the long and angulated delivery path, it was anticipated that the MI2355A delivery sheath would not navigate safely through the route. As a result, the femoral approach was abandoned. Instead, the left internal jugular vein was punctured, and a guidewire was successfully advanced into the right atrium. After sequential dilation, the MI2355A delivery sheath was inserted (
Figure 3C).
The pre-loaded Micra AV leadless pacemaker (model MC1AVR1), equipped with a steerable delivery system, was introduced through the sheath and advanced through the tricuspid valve into the right ventricle. Angiography performed via the sheath confirmed that the pacemaker tip was securely positioned against the mid-lower portion of the ventricular septum (Figure 3D). The device was then gradually deployed (Figure 3E). Programmed parameters included a sensing amplitude of 12.5 mV, a pacing threshold of 0.5 V at 0.24 ms pulse duration, and an impedance of 750 Ω. Following wire traction and severance, reprogramming confirmed stable and consistent parameters. Subsequently, the delivery system and sheath were removed, the puncture site was sutured, and a compression dressing was applied, marking the completion of the procedure. Postoperative chest radiography revealed no signs of device displacement (Figure 3F), and Post-implant pacemaker programming demonstrated stable parameters. One month after implantation, the patient reported no symptoms.
Discussion
The incidence of mirror-image dextrocardia is approximately 0.01%, and 23%–70% of cases are associated with other cardiovascular malformations (1). The absence of the hepatic segment of the IVC, with continuation via the azygos vein, occurs in about 0.6% of individuals. Although this anomaly is typically asymptomatic, it can lead to significant elongation and sharp angulation along the femoral vein access path, making it challenging for the leadless pacemaker delivery system to navigate (4, 5). For preoperative evaluation of complex congenital heart diseases, high-resolution CTA is widely recommended by clinical guidelines (2, 3).
Published literature suggests that the success rate of LP implantation in patients with IVC anomalies is closely related to the angle between the azygos vein and the SVC, as well as the support provided by the delivery sheath. When this angle exceeds 90°, the failure rate of the femoral venous approach can reach up to 57%, whereas the SVC approach achieves a success rate of nearly 100% (4, 5, 7–9). When the femoral approach is not feasible, the internal jugular vein serves as a viable alternative access route. Oliveira et al. (4) first described LP implantation via the azygos vein; however, this technique required a stiff guidewire, which increased procedural risk. Guo et al. (5) later demonstrated successful implantation through the right internal jugular vein, confirming its safety. In this case, we used computer imaging technology: through the “Patient Orientation”function, we displayed the images in a prone position.the patient underwent image mirroring to align catheter manipulation with the operator's field of vision, thereby improving procedural safety and reducing fluoroscopy time. Furthermore, the anatomical right ventricle (systemic ventricle) contains abundant trabeculae that provide favorable conditions for wing anchor fixation. However, care should be taken to avoid the moderator band to prevent an elevated pacing threshold (10). Performing intra-sheath angiography during the procedure allows for real-time assessment and timely detection of potential myocardial perforation.Limitations: The lack of long-term follow-up in this single case highlights the need for larger studies to validate fixation reliability and parameter stability.
This case is exceptionally rare. It represents the first successful implantation of a Micra AV pacemaker in a patient with a mirror-image right-sided heart and absence of the hepatic segment of the inferior vena cava, performed via the left internal jugular vein. During the procedure, the use of image mirroring technology reduced fluoroscopy time and ensured accurate device deployment, demonstrating a safe and viable alternative for patients with complex anatomical variations.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by Ethics Committee of Wuhan Asia Heart Hospital (no. 2025-B041). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
YB: Data curation, Formal analysis, Software, Writing – original draft, Writing – review & editing. HY: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. HH: Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Gu M Hua W Niu H Chen X Chen K Dai Y et al Transvenous permanent pacemaker implantation in 13 patients with dextrocardia. Chin Circ J. (2021) 36(1):43–7.
2.
Bontempi L Fundaliotis A Moretti M Sammartino AM Saino AT Arabia G et al Leadless pacemaker implantation in dextrocardia with situs viscerum inversus: a case report and literature review. Pacing Clin Electrophysiol. (2023) 46(1):39–43. 10.1111/pace.14579
3.
Glikson M Nielsen JC Kronborg MB Michowitz Y Auricchio A Barbash IM et al 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Europace. (2022) 24(1):71–164. 10.1093/europace/euab232
4.
Oliveira M Mesquita D Cunha PS Delgado AS Ferreira RC . Leadless pacemaker implantation via azygos vein in a patient with absence of the hepatic segment of the inferior vena cava. Europace. (2019) 21(4):547. 10.1093/europace/euy274
5.
Guo L Zhang M Zhao Y Yan Q Feng X Tao L . Leadless pacemaker implantation in a patient with congenital azygos continuation of the inferior vena cava. BMC Cardiovasc Disord. (2025) 25(1):63. 10.1186/s12872-025-04511-3
6.
Kusumoto FM Schoenfeld MH Barrett C Edgerton JR Ellenbogen KA Gold MR et al 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart rhythm society. Circulation. (2019) 140(8):e382–482.
7.
De Regibus V Pardeo A Artale P Petretta A Filannino P Iacopino S . Leadless pacemaker implantation after transcatheter lead extraction in complex anatomy patient. Clin Case Rep. (2018) 6(6):1106–8. 10.1002/ccr3.1532
8.
Sanhoury M Fassini G Tundo F Moltrasio M Ribatti V Lumia G et al Rescue leadless pacemaker implantation in a pacemaker-dependent patient with congenital heart disease and no alternative routes for pacing. J Atr Fibrillation. (2017) 9(5):1542. 10.4022/jafib.1542
9.
Wilson DG Morgan JM Roberts PR . “Leadless” pacing of the left ventricle in adult congenital heart disease. Int J Cardiol. (2016) 209:96–7. 10.1016/j.ijcard.2016.01.099
10.
Sheehan F Redington A . The right ventricle: anatomy, physiology and clinical imaging. Heart. (2008) 94(11):1510–5. 10.1136/hrt.2007.132779
Summary
Keywords
leadless pacemaker, mirror-image dextrocardia, hepatic segment interruption of theinferior vena cava, azygos continuation, internal jugular approach
Citation
Bao Y, Yi H and Han H (2026) A case report of successful implantation of a leadless pacemaker via the left internal jugular vein in a patient with mirror-image dextrocardia and absence of the inferior vena cava’s hepatic segment. Front. Cardiovasc. Med. 12:1701484. doi: 10.3389/fcvm.2025.1701484
Received
08 September 2025
Accepted
27 October 2025
Published
05 January 2026
Volume
12 - 2025
Edited by
Marta Belmonte, Cardiovascular Center, OLV Aalst, Belgium
Reviewed by
Abdalhakim Shubietah, Advocate Illinois Masonic Medical Center, United States
Carlo Barsali, Sapienza University of Rome, Italy
Updates
Copyright
© 2025 Bao, Yi and Han.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Hongwei Yi 11354968@qq.com Hongwei Han 15327298622@189.cn
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.