 Michelle Nakatsuka1*†
Michelle Nakatsuka1*† Kekoa Taparra2,3,4†
Kekoa Taparra2,3,4† Benjamin Renton5Alexander Junxiang Chen6
Benjamin Renton5Alexander Junxiang Chen6 Ji Chen7Harlan M. Krumholz7Jeremy Samuel Faust8,9
Ji Chen7Harlan M. Krumholz7Jeremy Samuel Faust8,9- 1NYU Grossman School of Medicine, New York, NY, United States
- 2Department of Radiation Oncology, Stanford Medicine, Stanford, CA, United States
- 3Department of Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, United States
- 4Department of Health Policy and Management, University of California, Los Angeles, Los Angeles, CA, United States
- 5Ontos Analytics, Cambridge, MA, United States
- 6Global Health and Health Policy, Harvard University, Cambridge, MA, United States
- 7Yale New Haven Hospital Center for Outcomes Research and Evaluation, New Haven, CT, United States
- 8Department of Emergency Medicine, Mass General Brigham, Boston, MA, United States
- 9Division of Health Services Research, Harvard Medical School, Boston, MA, United States
Objectives: To quantify all-cause excess mortality, defined as the number of deaths exceeding the expected baseline, associated with the 2023 Lāhainā wildfire in Maui County, Hawai‘i, and highlight public health implications.
Methods: Excess mortality was estimated using seasonal autoregressive integrated moving average models trained on data from August 2018–July 2023. Projections were generated via 5,000 bootstrapped simulations, with a sensitivity analysis excluding COVID-19-attributed deaths.
Results: August 2023 reported 82 (95% CI: 55–100) excess deaths, with all-cause mortality 67% higher than expected (observed-to-expected mortality rate: 1.67; 95% CI: 1.38–2.00). Mortality peaked the week of August 19, with a 367% increase (67 excess deaths: 3.67; 2.65–5.96). Non-medical deaths increased from 68 to 80%.
Conclusion: The Lāhainā wildfire caused substantial excess mortality, likely making wildfires a leading cause of death in Maui County during this period. Findings highlight the need for improved disaster preparedness. Policy Implications. Rebuilding must incorporate Native Hawaiian ecological knowledge. Policies should focus on restoring Indigenous wetlands, removing flammable invasive grasses, and ensuring environmental justice for Native Hawaiians.
Introduction
The 2023 Lāhainā wildfire on Maui, Hawaiʻi, the deadliest wildfire in modern US history, was not an isolated catastrophe, but part of a growing trend of climate-driven wildfires in the Hawaiian Islands. These fires are fueled by the spread of flammable invasive grasses, drought exacerbated by climate change, and the displacement of Indigenous land management systems. The erosion of Native Hawaiian ecological practices, including wetland stewardship and culturally-informed firebreaks, has weakened the resilience of both ecosystems and communities, contributing to catastrophic consequences for human and environmental health (Taparra et al., 2023; Taparra and Apana, 2023; Pacific Fire Exchange, 2024; Smith and Tunison, 1992; Farrant et al., 2024).
All-cause excess mortality, a well-established metric to quantify the impact of natural or human-influenced disasters, is vital to assess population-level effects, gage disaster response efforts, and provide context for future disaster prevention (Msemburi et al., 2023). Despite the growing frequency and severity of climate-driven disasters, empirical data on their population-level health impacts remain sparse, particularly in Hawai‘i and other Indigenous territories. This study addresses that gap by quantifying all-cause excess mortality associated with the 2023 Lāhainā wildfire, capturing both direct and indirect effects beyond official fatality counts.
Methods
All-cause excess mortality (observed minus expected deaths) was determined by training seasonal autoregressive integrated moving average models on 5 years of pre-study period data (August 2018–July 2023), accessed from CDC WONDER (updated December 3, 2023). Annual estimated populations were included as covariates to account for changes in underlying population size over time, which helps stabilize the time series and satisfy the assumption of stationarity, that is, that the statistical properties of the data do not change over time. Monthly and weekly projections were determined using SARIMA models, which were designed to account for seasonality and trends in time-series data. To quantify uncertainty around these estimates, we conducted Monte Carlo simulations generating 5,000 future values from the fitted model, and calculated 95% confidence intervals (95% CI) using the percentile method (2.5th-97.5th percentiles of the simulated distribution). A sensitivity analysis excluding COVID-19-attributed mortality from the baseline period overlapping with the COVID-19 pandemic (March 2020–July 2023) was also conducted. This adjustment resulted in a slightly higher estimate of excess deaths (86; 95% CI: 60–103) but did not change the overall interpretation of wildfire-associated excess mortality. Demographic information on all-cause deaths, including age, gender, race, and place of death, was accessed and tested for changes during the study period versus baseline period ratios with significance determined using Pearson chi-squares. Analyses were performed in R (v4.2.2). Institutional review board approval was not required, as all data are public.
Results
In August 2023, there were 82 (95% CI: 55–100) all-cause excess deaths in Maui County (205 observed, 123 expected), corresponding to an excess mortality rate of 47 deaths per 100,000 person-months (95% CI: 33–61), and an observed-to-expected all-cause mortality rate of 1.67 (95% CI: 1.38–2.00). Among the 200 deaths observed during the study period (August 2023), 60 (30%) occurred in individuals under age 65 and 140 (70%) in those aged 65 and older (Table 1). A total of 125 deaths (62.5%) occurred in males and 75 (37.5%) in females. By race, 70 decedents (35%) were identified as White, and 130 (65%) were Asian, Black, Native Hawaiian or Pacific Islander, or multiracial. Most deaths (160; 80%) occurred in non-medical settings, such as homes or public locations, with only 40 (20%) occurring in medical settings.
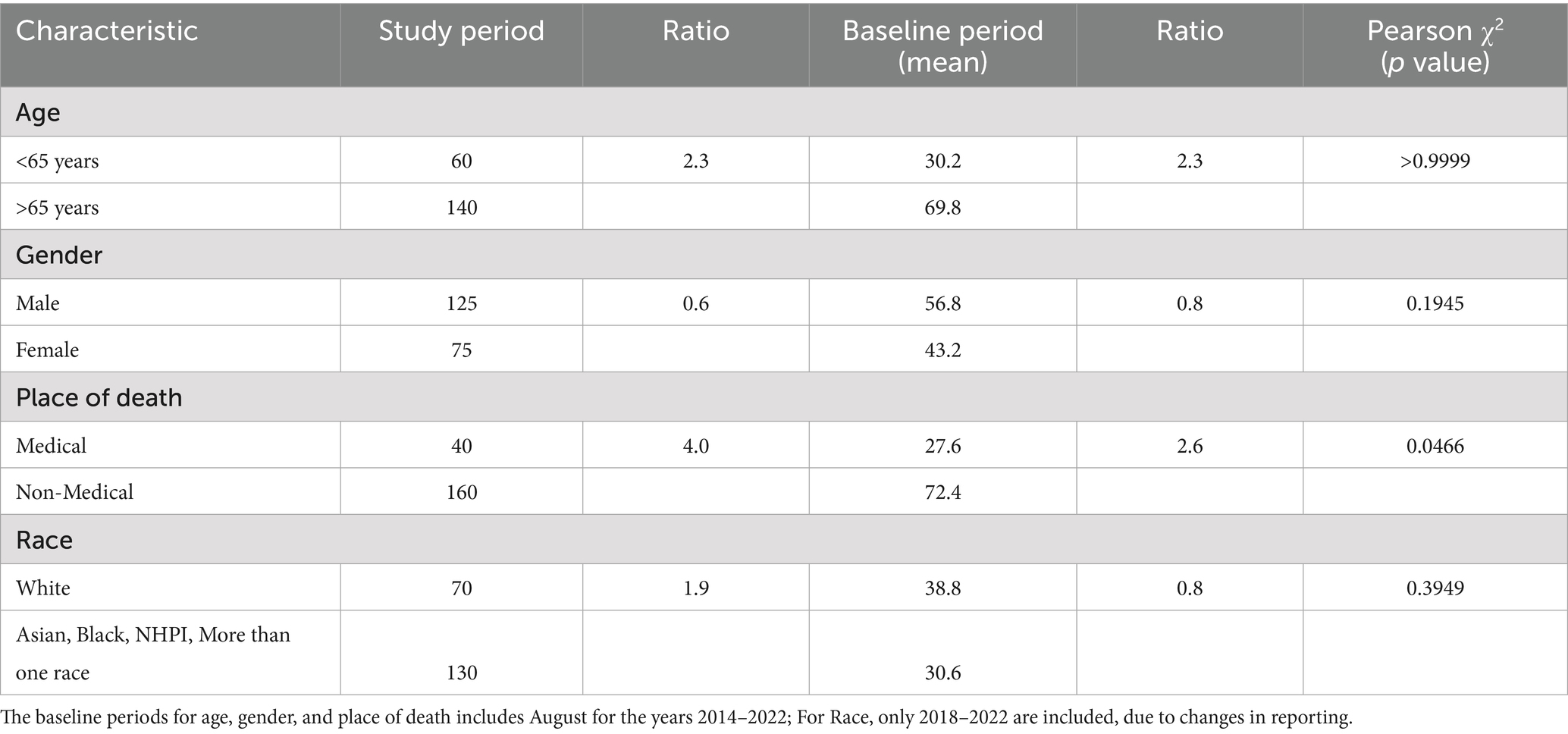
Table 1. Demographic information on all-cause mortality.
In a sensitivity analysis model removing COVID-19-attributed deaths from the baseline period, estimated excess deaths increased to 86 (95% CI: 60–103). Excess mortality peaked the week ending August 19, 2023, when 67 all-cause excess deaths were recorded, corresponding to an excess mortality rate of 41 deaths per 100,000 person-months (95% CI: 35–47), and an observed-to-expected ratio of 3.67 (95% CI: 2.65–5.96) (Figure 1). Rates returned to expected values the week ending August 26, 2023.
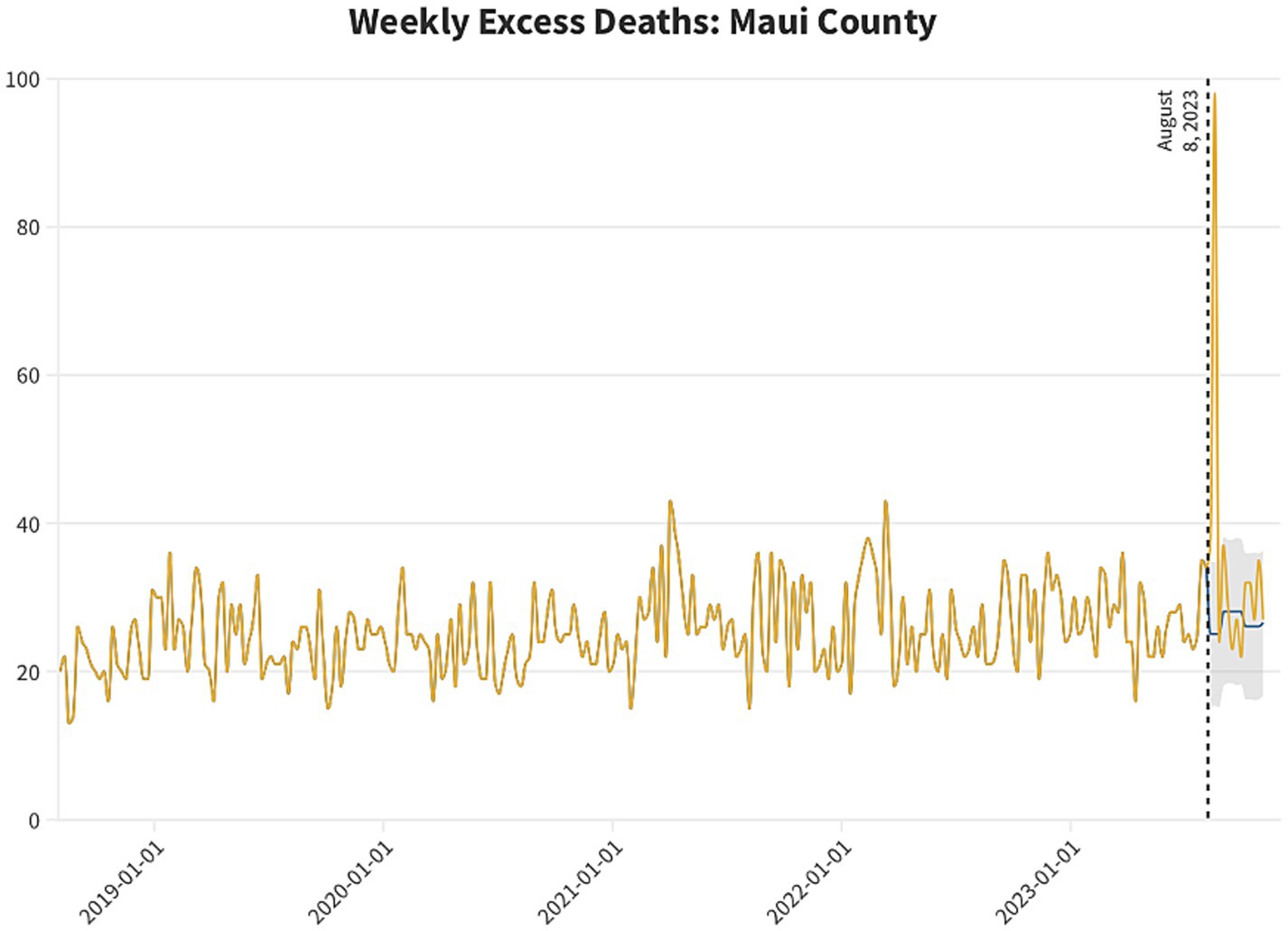
Figure 1. Weekly observed and expected raw all-cause deaths for Maui County, HI for the week ending August 4, 2018, through the week ending October 23, 2023. Observed deaths are shown in yellow. Modeled expected deaths (for the weeks ending August 5, 2023, through October 23 2023) are shown in blue. 95% confidence intervals are shown in gray.
The share of deaths occurring outside of medical settings (e.g., homes or public places) increased during August from 68% (64/94) to 80% (156/196), suggesting potential disruptions in access to emergency medical care or evacuation during the wildfire period. Although not statistically significant, the proportion of deaths in individuals aged <65 years, males, and persons of non-White race was numerically elevated compared to baseline periods (August 2018–July 2023).
Discussion
The 2023 Lāhainā wildfire was associated with increased all-cause mortality, peaking at 367% of expected rates (week ending August 19, 2023). This sudden and localized spike in mortality suggests that the wildfire was a dominant contributor to deaths on Maui during August 2023. Despite 100–102 officially reported fire-related deaths per public and government sources (CDC/NCHS, 2023), we estimated 82–86 all-cause excess deaths, which includes both directly and indirectly attributable mortality during the wildfire period. Notably, temporary decreases in other causes of death may have occurred following the wildfire (e.g., motor vehicle fatalities).
This estimate of all-cause excess mortality, 82 deaths in the primary model and 86 in the sensitivity model, closely aligns with the 88 fire-related deaths officially reported for August 2023 in CDC WONDER, 86 of which had autopsies performed. Media and government sources have cited a total of 100–102 deaths from the Lāhainā fire (CDC/NCHS, 2023), with some fatalities likely occurring in September or later and others potentially classified under different cause-of-death codes. Notably, this level of fire-related mortality is unprecedented in recent history: annual fire deaths were suppressed in all other years from 2018 to 2024, indicating counts below 10 and underscoring the exceptional mortality toll of the wildfire. While the official count reflects confirmed fire-related fatalities, our model-based estimate captures broader mortality impacts during the same period, including potentially unclassified or indirectly related deaths.
Although cause-specific data were not available, prior studies of wildfire events suggest several plausible medical and environmental pathways that may have contributed to excess mortality. These include direct injuries such as burns and asphyxiation (Stefanidou et al., 2008), smoke-related respiratory complications (Shusterman et al., 1993), and heat-related illness, particularly among older adults and individuals with pre-existing pulmonary or cardiovascular conditions (White, 2024; Hancock and Vasmatzidis, 2003). Disasters of this scale may also exacerbate mortality indirectly by delaying access to emergency care or interrupting management of chronic illnesses (Bell et al., 2019). In addition, social vulnerability, including crowded housing, limited transportation, and language barriers, may have disproportionately affected the ability to evacuate or receive timely care for certain groups (Ermagun and Janatabadi, 2024). These pathways align with observed patterns during other large-scale wildfire and heat events and may help explain the demographic patterns seen in Maui (McBrien et al., 2023).
Although not statistically significant, we also observed a numerically higher share of deaths among individuals under age 65, males, and persons of non-White race compared to prior Augusts. These demographic patterns are consistent with previous research showing that structurally vulnerable populations, particularly those with limited mobility, access to care, or pre-existing health inequities, are at higher risk of mortality during climate-related disasters. While small sample sizes may limit statistical power, these trends highlight the need for improved data collection and demographic disaggregation to better understand and address disparities in disaster impacts.
This study has several limitations. First, the analysis relies on provisional mortality data, which are subject to future updates and reclassification. Second, the data lack geographic granularity, limiting our ability to isolate trends at the city or neighborhood level (e.g., Lāhainā-specific patterns). Third, demographic fields, particularly race and ethnicity, were incomplete or inconsistently reported, constraining our ability to examine disparities with precision. Additionally, there are limitations inherent to the use of all-cause excess mortality models. While they are powerful tools for detecting population-level mortality shifts, they cannot attribute causality or identify specific causes of death. Furthermore, this study did not include toxicology, forensic, or cause-of-death certificate data, which would be necessary to directly attribute specific deaths to fire, heat, or smoke exposure. These models are also not well-suited to capturing the intergenerational health consequences of land dispossession, cultural displacement, or the erosion of Indigenous ecological knowledge. These social and historical forces may shape who is most at risk during disasters, yet remain invisible within conventional public health metrics.
It is unusual for natural or human-made disasters to be the driving force behind such a large increase in all-cause mortality, likely the temporary leading cause of death in affected regions. Whether the findings reported here are unprecedented is difficult to determine, in part because the ICD-10 classification system does not include codes for climate-related events; for example, deaths related to ecosystem collapse are often categorized under general causes such as respiratory failure or cardiac arrest. This limits the visibility of climate and ecological impacts in mortality data and highlights the need for updates to current classification systems (or the creation of new systems) to add climate and ecological conditions as factors underlying deaths from natural disasters (e.g., tornadoes and hurricanes, in addition to fires) (Taparra et al., 2024). This would allow more nuanced analyses of the impact of ecological change over time in different geographic areas.
Public health implications
The tragic and unprecedented loss of life reported here, alongside other recent high-fatality wildfire events, underscores the urgent need for disaster preparedness and prevention efforts that are responsive to local ecological and cultural conditions. Given the Indigenous people of Hawaiʻi, Native Hawaiians, experience disproportionate mortality burdens both locally and nationally, efforts to promote health equity in climate adaptation must include investment in Native Hawaiian-led environmental stewardship, climate health research, and policy reform grounded in Indigenous perspectives (Taparra et al., 2023; Taparra and Apana, 2023; Taparra and Pellegrin, 2022; Antonio et al., 2023; Keaulana et al., 2021).
While not derived directly from our mortality analysis, several forward-looking strategies, rooted in Native Hawaiian ecological knowledge, may hold promise for mitigating future wildfire risk. These include:
1. Restoring Native Hawaiian agroecological systems, such as ‘ulu (breadfruit), loko i‘a (fishponds), and lo‘i kalo (taro terraces), which support soil moisture retention and reduce erosion. Some Indigenous plants may also act as “green firebreaks” due to their lower flammability (Pacific Fire Exchange, 2024; Smith and Tunison, 1992; Farrant et al., 2024). A systematic assessment of plant flammability in Hawai‘i remains an important research need.
2. Managing dry non-native grasses, which contribute significantly to wildfire fuel loads, through approaches such as targeted grazing, controlled burns, and conversion to compost or fertilizer (Farrant et al., 2024; Maly and Wilcox, 2000). These grasses, though covering only 24% of Hawai‘i’s land, are linked to a majority of large fires (Trauernicht, 2019).
3. Restoring pre-colonial water systems and improving fire risk modeling. A high-resolution, dynamically updated wildfire risk tool for Hawai‘i, based on rainfall, wind, vegetation, and other climate data, could guide water allocation and inform state mitigation planning.
These ideas are not evaluated in this study but reflect calls within Native Hawaiian and broader Indigenous communities to design place-based strategies for ecological resilience. Incorporating these frameworks into recovery and preparedness planning may help reduce the disproportionate impact of climate disasters on Native Hawaiian communities.
Conclusion
The 2023 Lāhainā wildfire was associated with substantial excess mortality, with an observed all-cause death rate 67% higher than expected in August 2023. While official records cite 100–102 wildfire-related fatalities, our analysis identified 82–86 excess deaths, underscoring the broader health impact of the disaster, including both direct and indirect mortality. These findings highlight the importance of timely, population-level mortality monitoring during ecological crises. As climate-driven disasters grow in frequency and severity, particularly in historically marginalized communities, equitable disaster response and public health surveillance systems must evolve to better capture and mitigate their full human toll.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
MN: Writing – original draft, Writing – review & editing. KT: Writing – original draft, Writing – review & editing. BR: Writing – review & editing. AC: Writing – review & editing. JC: Writing – review & editing. HK: Writing – review & editing. JF: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Antonio, M. C., Keaulana, S., Keli‘iholokai, L., Felipe, K., and Vegas, J. K.Waimānalo Pono Research Hui, et al. (2023). A report on the Ke Ola O Ka ‘Āina: ‘āina connectedness scale. Int. J. Environ. Res. Public Health 20:3302. doi: 10.3390/ijerph20043302
Bell, S. A., Horowitz, J., and Iwashyna, T. J. (2019). Health outcomes after disaster for older adults with chronic disease: a systematic review. Gerontologist 60, 535–547. doi: 10.1093/geront/gnz123
CDC/NCHS. (2023) CDC WONDER: Provisional mortality statistics, 2018 through last week, D367F834. Available online at: https://wonder.cdc.gov/controller/saved/D176/D367F834. [Accessed November 30, 2023]
Ermagun, A., and Janatabadi, F. (2024). Compound risk of wildfire and inaccessible shelters is disproportionately impacting disadvantaged communities. Prog. Disaster Sci. 23:358. doi: 10.1016/j.pdisas.2024.100358
Farrant, N., Trauernicht, C., Kagawa-Viviani, A., Giambelluca, T. W., and D’Antonio, C. M. (2024). On the anniversary of the Maui fires, a call for indigenous land care to mitigate future disasters. Proc. Natl. Acad. Sci. USA 121:45121. doi: 10.1073/pnas.2401045121
Hancock, P. A., and Vasmatzidis, I. (2003). Effects of heat stress on cognitive performance: the current state of knowledge. Int. J. Hyperth. 19, 355–372. doi: 10.1080/0265673021000054630
Keaulana, S., Kahili-Heede, M., Riley, L., Park, M. L., Makua, K. L., Vegas, J. K., et al. (2021). A scoping review of nature, land, and environmental connectedness and relatedness. Int. J. Environ. Res. Public Health 18:5897. doi: 10.3390/ijerph18115897
Maly, K., and Wilcox, B. A. (2000). A short history of cattle and range management in Hawaii. Rangelands 22, 21–23. doi: 10.2458/azu_rangelands_v22i5_maly
McBrien, H., Rowland, S. T., Benmarhnia, T., Tartof, S. Y., Steiger, B., and Casey, J. A. (2023). Wildfire exposure and health care use among people who use durable medical equipment in Southern California. Epidemiology 34, 700–711. doi: 10.1097/ede.0000000000001634
Msemburi, W., Karlinsky, A., Knutson, V., Aleshin-Guendel, S., Chatterji, S., and Wakefield, J. (2023). The WHO estimates of excess mortality associated with the Covid-19 pandemic. Nature 613, 130–137. doi: 10.1038/s41586-022-05522-2
Pacific Fire Exchange. (2024). Coastal plants for creating green breaks. Available online at: https://pacificfireexchange.org/resource/coastal-plants-for-creating-greenbreaks/. [Accessed March 27, 2024]
Shusterman, D., Kaplan, J. Z., and Canabarro, C. (1993). Immediate health effects of an urban wildfire. West. J. Med. 158, 133–138.
Smith, C. W., and Tunison, J. T. (1992). Fire and alien plants in Hawaii: research and management implications for native ecosystems. Hilo, Hawaii: UH Hilo Center for Maunakea Stewardship - Research Library.
Stefanidou, M., Athanaselis, S., and Spiliopoulou, C. (2008). Health impacts of fire smoke inhalation. Inhal. Toxicol. 20, 761–766. doi: 10.1080/08958370801975311
Taparra, K., and Apana, N. K. (2023). Rising from ruin––revitalizing native Hawaiian health. JAMA 330, 2051–2052. doi: 10.1001/jama.2023.21427
Taparra, K., Faust, J. S., and Batangan, K. (2024). The Lāhainā wildfires and ‘Āina connectedness in the face of climate disasters. JAMA Intern. Med. 184, 1403–1405. doi: 10.1016/S0140-6736(22)01100-X
Taparra, K., and Pellegrin, K. (2022). Data aggregation hides Pacific islander health disparities. Lancet 400, 2–3. doi: 10.1016/S0140-6736(22)01273-0
Taparra, K., Purdy, M., and Raphael, K. L. (2023). From ashes to action – indigenous health perspectives on the Lāhainā fires. N. Engl. J. Med. 389, 1543–1546. doi: 10.1056/NEJMp2309966
Trauernicht, C. (2019). Vegetation-rainfall interactions reveal how climate variability and climate change alter spatial patterns of wildland fire probability on big island, Hawaii. Sci. Total Environ. 650, 459–469. doi: 10.1016/j.scitotenv.2018.08.347
Keywords: Lāhainā Maui, wildfire, excess mortality estimation, Indigenous health, environmental health
Citation: Nakatsuka M, Taparra K, Renton B, Chen AJ, Chen J, Krumholz HM and Faust JS (2025) All-cause excess mortality associated with the Lāhainā, Maui fires. Front. Clim. 7:1611198. doi: 10.3389/fclim.2025.1611198
Edited by:
Hanadi Rifai, University of Houston, United StatesReviewed by:
German Velez, New York Presbyterian Hospital, United StatesVictoria Lerma-Arce, Universitat Politècnica de València, Spain
Copyright © 2025 Nakatsuka, Taparra, Renton, Chen, Chen, Krumholz and Faust. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michelle Nakatsuka, bWljaGVsbGUubXVyYXRhQG55dWxhbmdvbmUub3Jn
†These authors have contributed equally to this work