 Madeline Jun-yu Yon
Madeline Jun-yu Yon Mark Ho-yeung Tang
Mark Ho-yeung Tang Gary Shun-pan Cheung
Gary Shun-pan Cheung- 1Division of Restorative Dental Sciences, Prince Philip Dental Hospital (PPDH), Faculty of Dentistry, University of Hong Kong, Hong Kong, Hong Kong, SAR China
- 2Department of Health, The Government of Hong Kong Special Administrative Region (HKSAR), Hong Kong, Hong Kong, SAR China
- 3Department of Dentistry, The University of Hong Kong Shenzhen Hospital, Shenzhen, China
Aim: To review the reported defect and fracture rates of various NiTi instrumentation systems and identify factors that may influence the chance of NiTi file separation clinically.
Data Sources: PubMed, EMBASE, and SCOPUS with controlled vocabulary and keywords in various combinations to identify articles that reported on the defects and/or fracture of NiTi instrument used clinically (Jan 1980 till Aug 2021), with additional search manually by going through the list of references of the initially screened articles. Those satisfying the inclusion and exclusion criteria were entered into the analysis.
Study Eligibility Criteria, Participants, and Interventions: All studies from the said databases reporting on NiTi root canal instruments that were deformed or separated during normal clinical use.
Study Appraisal and Synthesis Methods: Studies with data available and suitable for meta-analysis were grouped according to the general design of the NiTi instruments for comparison. Safety quotient value was calculated based on the rate of instrument distortion and fracture.
Results: Various instrument designs exhibited different incidences of distortion and fracture, hence a different “safety quotient” (ratio of the amount of deformed instruments to that of fractures in use). Heat-treated files showed the highest safety quotient value. All brands of NiTi file demonstrated a statistically significantly lower incidence of fracture, if treated as disposable instruments after clinical use in a patient.
Limitations: Inclusion of articles written in English only, and grouping of file systems into general design types in the analysis.
Conclusions and Implications of Key Findings: NiTi endodontic files should be scrutinized for defects before being used in the root canal. Disposing the NiTi instruments after clinical use in a patient (so-called “single use”) is recommended for minimizing fracture clinically. Certain instrument designs tend to show discernible deformation before they should fracture in the next use.
Introduction
Nickel-titanium (NiTi) instruments have revolutionized the process of root canal shaping for non-surgical endodontic treatment since its commercial introduction in early 1990's. The early brands were made of austenitic NiTi alloy that exhibits superelastic property (1). Compared with conventional stainless steel files, they are able to enlarge the root canals expeditiously while respecting the root canal curvature (2). The prepared canals, typically, have a smooth taper, with little canal transportation (2, 3). NiTi files are available in many different designs, including different (non-ISO) size convention, increased body taper, and both regular and irregular cross sections. Most, if not all current brands, however, come with a non-cutting tip design (1). In the past few years, instruments made of martensitic NiTi were introduced by many manufacturers, with some actually making use of the shape memory property of the NiTi alloy. These heat-treated variants have been promulgated with claims for improved efficiency and greater instrument safety (4).
Instrument separation is a well-recognized complication of root canal therapy, especially for NiTi rotary instruments. Engine-driven NiTi files can fail or break, as a result of torsional overload and/or cyclic fatigue (5, 6). Fatigue breakage of NiTi files typically occurs more readily in severely curvatures, and affects those overused instruments (6, 7). Ways of preventing this complication have been published (8, 9), which include the use of “crown down” approach, having a straight-line access, single use of the files, avoiding their use in severely curved canals and discarding the instruments once they show signs of deformation.
When a NiTi instrument is noticed to have been distorted (i.e., plastically deformed), either before or after clinical use, the clinician would most likely discard and will not use it anymore. This is especially true for practitioners who might be re-using the instrument (after proper infection control measures) for whatever reason. Those instruments that were reported to have fractured probably had not shown any visible defects prior to that final use. Thus, instruments that tend to deform, rather than fracture, would provide a higher degree of “clinical safety” than those which separate without warning. A safety quotient (SQ), in the context of NiTi engine-files, may be defined as the ratio of the amount of files showing plastic deformation (e.g., distorted flutes) to the amount of fractures either for a particular brand of instrument or, collectively, for instruments of similar design. The higher the SQ value, the more likely that any material defects are noticed upon visual examination, before or after clinical use, hence avoiding the mishap of file separation. The SQ value could serve as a reference to aid the selection of a relatively “safe” file type, especially for new users who need to build their confidence while familiarizing with any brand of NiTi engine-file.
The purpose of this study was to review systematically the defect and fracture rates of various brands of NiTi instrumentation system and to identify any designs or factors that may influence the chance of NiTi files separation during clinical use.
Materials and Methods
Literature Search
A comprehensive electronic search of published articles was conducted using 3 electronic databases (PubMed, EMBASE, and SCOPUS) to identify all studies that reported on distortion or breakage of NiTi instruments in clinical practice. The keywords and Boolean operators used in search are the same with each database: (breakage OR fracture OR separation OR separated OR permanent deformation OR distortion OR defect) AND (NiTi OR Ni-Ti OR nickel titanium OR nickel-titanium) AND clinical AND (root canal OR endodontic OR pulpal). The search covered all articles published from 1980 to June 2019, both in Chinese and in English language. Citations of all resultant articles were imported into EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA), and duplicate records were eliminated in that software.
Articles from the electronic search were then screened for relevance by first reading the published title and abstract. Only clinical studies were included while applying the inclusion and exclusion criteria below. Thereafter, the articles were identified, and their reference lists screened to look for any other potentially relevant studies that might have been missed out during the initial search. An update search was performed in September 2021. The process was summarized in Figure 1.

Figure 1. Flowchart of the study selection process.
Inclusion Criteria
• Instruments concerned were either noticed to have deformed, or fractured during clinical use
• Publications, including case reports, with full text available in either soft or hard copy
• Root canal treatment performed by dentists or dental students
Exclusion Criteria
• Not a clinical study, i.e., one involving using extracted teeth or artificial canals, or as a laboratory study of fatigue or torsional failure
• Publications in the form of letters, commentaries or narratives
• Animal studies
Data Extraction and Statistical Analysis
Two reviewers (MJY and MHT) independently screened all titles and abstracts, according to the inclusion and exclusion criteria. Reasons for exclusion were documented for all stages of review. In cases of disagreement, the reviewers would meet for discussion to resolve any disagreements. If that should fail to reach an agreement, a third reviewer (GSC) was recruited. The studies that remained after the screening were then submitted for data extraction. A standard, specifically designed, data collection form was used to record the relevant information systematically, which data were then entered into a spreadsheet (Microsoft Excel, Redmond, WA, USA). Information collected included year of study, method of examination for defects, type of practice (specialist vs. general practice), brand(s) of instrument, sample size, amount of defects and fractures. The two reviewers performed the appraisal and information collection independently, and any disagreement was reconciled by discussion and consensus.
Studies with similar characteristics (brand, type and cross section of instrument) and data set that allowed pooling of data were submitted for meta-analysis. A statistician was consulted for pooling of the data and to assist with the analyses. The independent variables considered were: (i) design of the file, and (ii) single vs. multiple use. In this study, for avoidance of confusion, the sub-group “single use” included all those files that were reported explicitly as having been used on a single tooth, or discarded after a single visit. The dependent variables were the amounts of defect and instrument fracture.
The pooled overall rates of defect or fracture were estimated by separate meta-analyses of the relevant proportions, using a random effect model with the Freeman-tukey double arcsine transformation (10). Heterogeneity tests were performed for each meta-analysis for the reference. Meta regressions were then performed for comparison with dummy variables if necessary. Safety quotient value and its corresponding 95% confidence interval were computed by linearization based variance estimator. Comparison between subgroups was performed by a Wald test. Statistical analysis was done using the Stata 13.1 software (StataCorp LLC, College Station, TX, USA). Results were presented in forest plots, with the computing of the study-specific confidence intervals using exact method and the comparisons made as two-tailed tests at α = 0.05.
Results
During the initial search, the three electronic databases (PubMed, EMBASE, and SCOPUS) yielded 123, 88, and 40 articles, respectively. From the lists of references, another 5 articles were included via hand search. Altogether, 257 articles were included before de-duplication, which process eliminated 112 duplicates. After applying the inclusion and exclusion criteria to the then 145 articles, 34 studies remained (Figure 1). During the process of data extraction, 10 articles had to be excluded, because they only studied files with defects and the total quantity of (each brand of) instruments consumed was not specified, thus making the calculation of defect rates impossible. Two sets of data had been reported twice each (giving rise to 4 articles). For these 4 articles, only the original sets of data were extracted for entry into meta-analysis.
Characteristics of Studies
A total of 34 studies (11–44) were identified, the characteristics of which were summarized in Table 1. All studies were published after the millennium, with 24 reports published in 2000–2009 (11–26, 35–42) and the rest after 2010 (27–34, 43, 44). Thirteen studies were conducted in Asia (15, 16, 16–22, 28, 31, 33, 34, 36, 43); 12 in North America (11, 12, 14, 17, 23, 25, 27, 29, 37, 38, 40, 42); 3 in Europe (30, 39, 41) and 2 in South America (24, 44). One study (32) did not specify the study location but the authors were from Europe. The authors of another study (13) were from Australia with the used instruments collected from several countries. For the examination methods, scanning electron microscope (n = 13 studies) (11, 14–16, 18, 20–22, 24, 31, 33, 36, 39) and/or optical microscope (n = 22 studies) (11–13, 19–32, 34, 35, 39, 42, 43) were used to examine the files in majority of studies. Six articles did not specify the visualization aids (17, 37, 38, 40, 41, 44). The overall safety quotient (SQ) value for collectively for those instruments reported in each study, where computable, was calculated (Table 1). Meta-analysis was performed on 22 sets of study data with a collective defect rate estimated for instruments of similar design (Figures 2, 3).
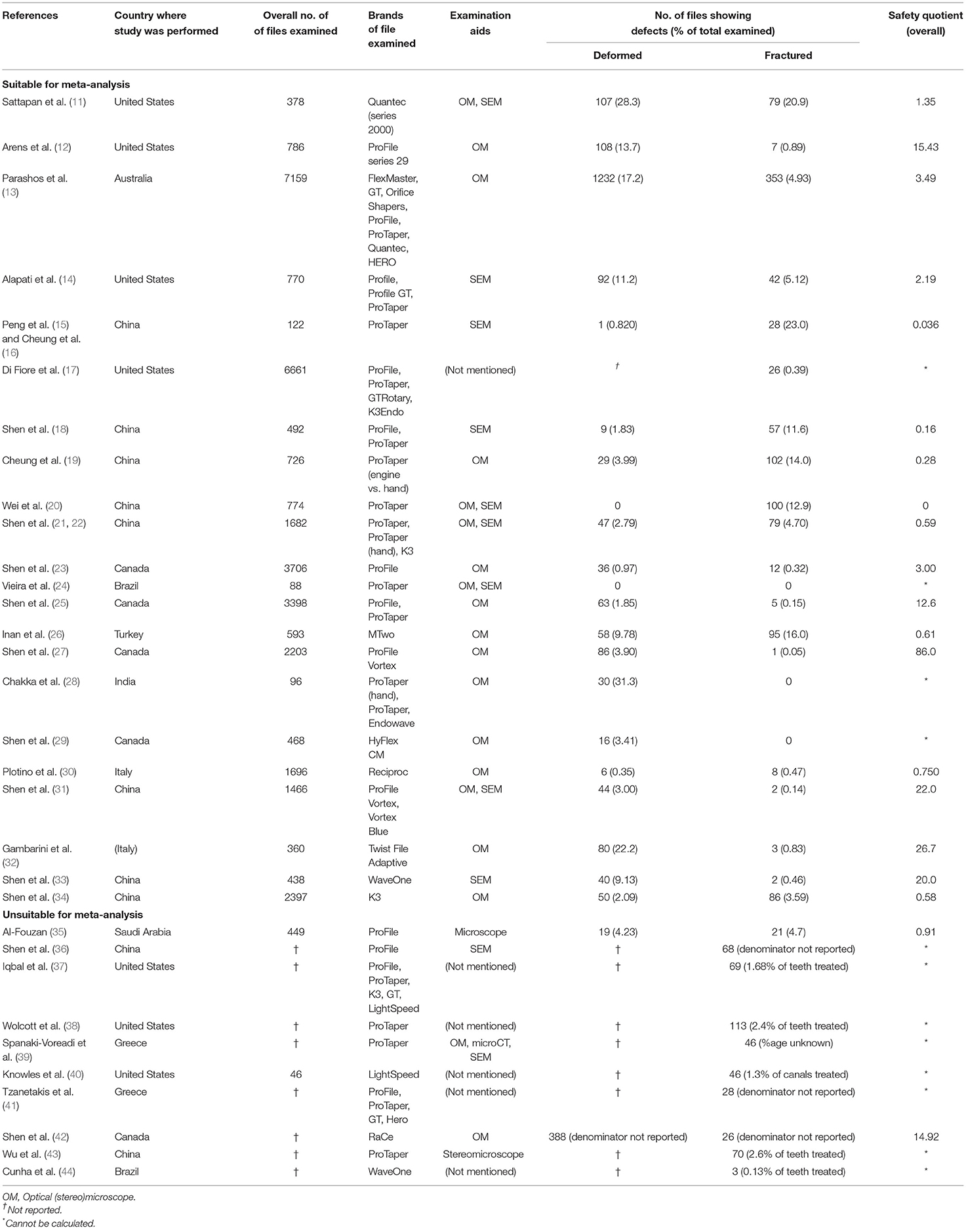
Table 1. Characteristics of studies qualified for the review.
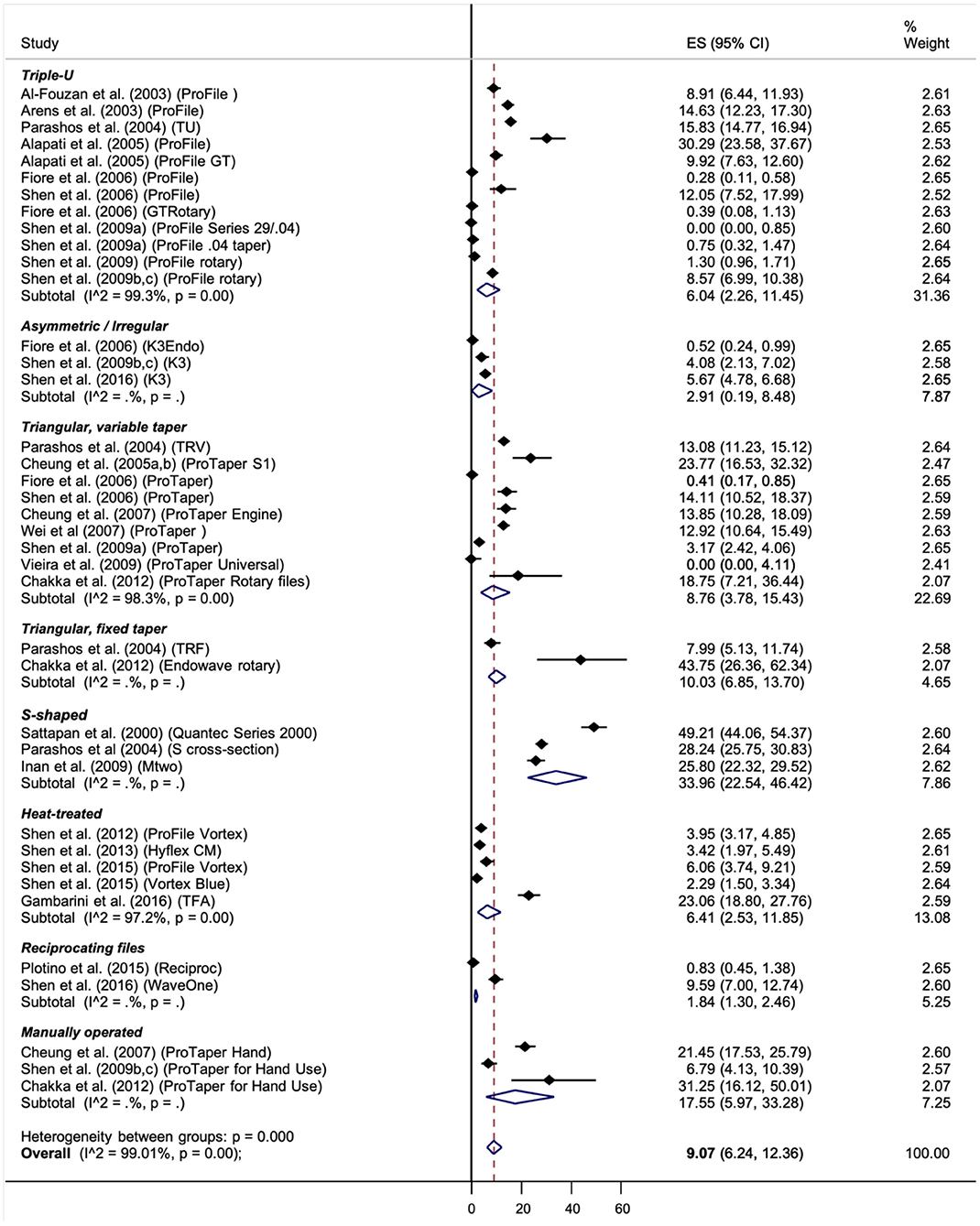
Figure 2. Forest plot for all kinds of defect, inclusive of plastic deformations and instrument separations, from reports included in the meta-analysis. [NB: X-axis represented the percentage of the total number of files reported].
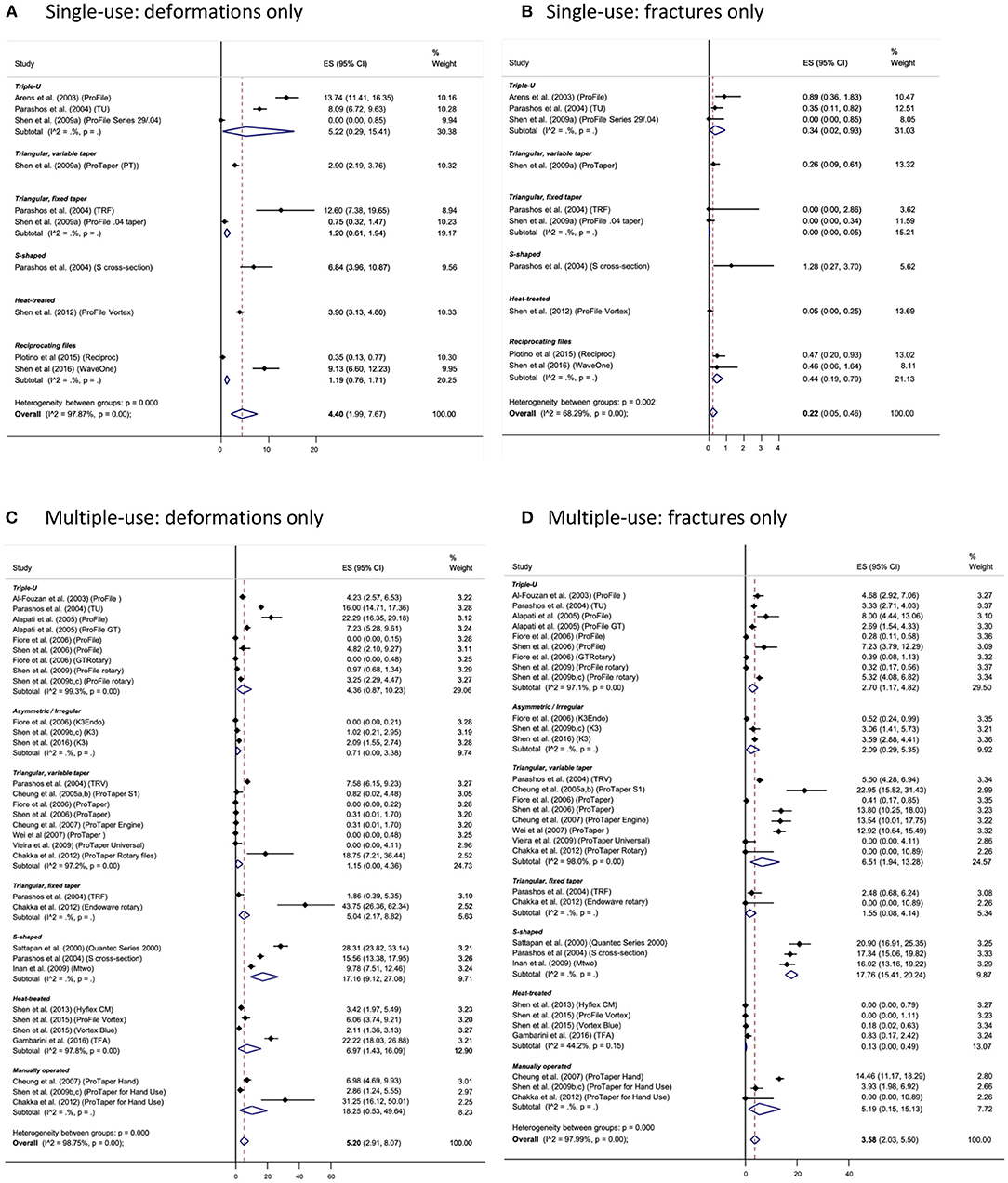
Figure 3. Forest plots of computed defect rate for NiTi instruments that were reported as being single use (A,B) vs. multiple uses (C,D). [Note different scale for the x-axis in different charts].
Overall Rate of Defects
The overall rate of defects, inclusive of fracture and plastic deformation, for all brands ranged from 0 to 49.2% (Table 1). The overall defect rate was significantly >0 (p < 0.05), for all instrument types combined, with notable differences between instruments that were subject to single use vs. multiple uses (Figure 2). In general, defects were frequently seen in S-shaped section (“S-files”), manually operated NiTi files (ProTaper for Hand Use), triangular variable taper, triple-U, triangular fixed taper, and files with irregular cross-section, in that order. Pairwise comparison indicated that S-files had a statistically significant higher defect rate than Triple-U files (p < 0.05). Heat-treated triangular files also showed an overall defect rate significantly >0 (p < 0.05).
The incidence of fracture was generally below 10% for all instruments reported (Table 1). Nearly all instrument types, regardless of whether the files were for single use (Figure 3B) or multiple uses (Figure 3D), showed a fracture rate of >0 (p < 0.05). With meta-analysis, only those heat-treated instruments seemed to enjoy a fracture rate close to zero (p > 0.05), based on the very small number of publications that included this type of instrument. S-shaped files had a statistically significant higher fracture rate than triple-U files (p < 0.01) and triangular fixed-tapered files (p < 0.05). ProTaper Hand files had a statistically significant higher fracture rate than triangular fixed-tapered files (p = 0.05).
The ratio of the amount of deformed-only to that of separated instruments, i.e., the safety quotient (SQ), was calculated for each general instrument type. The SQ value was the highest for heat-treated triangular files (SQ = 37.7), followed by triangular instrument with fixed taper (SQ = 14.0), and triple-U files (SQ = 3.5) (Figure 4).
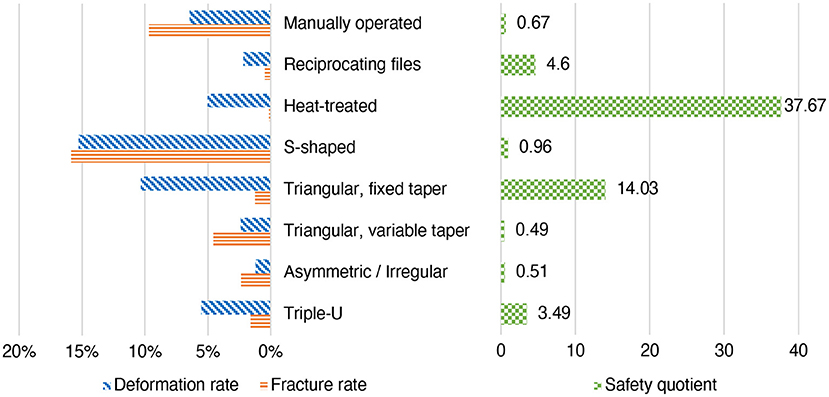
Figure 4. Proportion of single- vs. multiple use instruments showing plastic deformation or distorted flutes only (i.e., deformation rate) and those reported to have separated (i.e., fracture rate); and the calculated safety quotient values for various instrument types.
Single vs. Multiple Use
For purpose of this comparison, instruments which had been reported explicitly as being single use were identified, whereas those that were not so reported were assumed to have been used for more than once. Of all studies examined, data for single-use instruments could only be found for 4 general designs: triple-U, triangular variable taper, S-shaped and heat-treated triangular fixed taper. There were also one brand of heat-treated instrument and 2 brands of reciprocating files reported. No statistically significant difference in the rate of plastic deformations (only) was noted among the 4 general designs (p > 0.05) (Figure 3A). For instrument separation, a rate of 0.22% (C.I. 0.05–0.46%) was estimated for all NiTi files that were subject to single use (Figure 3B). Minimal amounts of fracture were reported for heat-treated files (with the collective fracture rate not significantly different from zero; p > 0.05), which file type was excluded from any pairwise comparisons for the incidence of separation. The differences between the various instrument types were not statistically significant (p > 0.05), when the “single use” strategy was employed (Figure 3B).
For those multiple-use instruments, no significant difference was found between various instruments for the rate of defects, both plastic deformation and instrument separation included, except for S-shaped instruments that appeared the most susceptible both for the amount of plastic deformation (Figure 3C) and of fracture when compared with other design types (p < 0.05) (Figure 3D). Collectively for all studies included in the meta-analysis, an overall fracture rate of about 3.6% (C.I. 2.0–5.5%) was estimated for multiple-use instruments, which was a significant rise from the figure of 0.22% for single-use files (p < 0.05). When plastic deformations only or distorted flutes of the instrument are concerned, a similar rate was observed for single-use (4.4%; C.I. 1.9–7.7%) and multiple-use instruments (5.2%; C.I. 2.9–8.1%); the heat-treated files exhibited a similar figure of 3.9% (single use) to 7% (multiple use). The calculated SQ values showed a wide range for various file types, from about 0.5 (triangular variable taper and asymmetric cross section) to over 37 (heat-treated files) (Figure 4).
Discussion
NiTi instrument has revolutionized the process of root canal preparation since its introduction. Not only are NiTi instruments able to enlarge the root canals expeditiously while respecting the root canal curvature (45, 46), but they also enable inexperienced users to achieve an improved success rate for molar endodontic treatment, compared with manual instrumentation (46). Despite all these advantages, widespread acceptance of NiTi instruments is hampered by the fear of their “unexpected” separation in the root canal. Improvements of the material have been achieved by way of surface treatment (chemical or electro-polishing) and/or heat treatment (4). Yet, they are not immune from separation during use.
Reports of instrument separation indicated a fracture rate of some 0–23% for different brands of NiTi instrument under the specific set of conditions in each study (see Table 1). Typically, only one or two brands of instruments were reported in one paper, as it is unusual for any practice or hospital to be keeping stock of all the various brands of instrument (indeed, the number of brands is ever-increasing in the last 2 decades), and because clinicians tend to favor one brand over another as a matter of personal preference. By grouping the data for instruments of the same general design for meta-analysis, it allows the estimation of an overall rate of fracture and/or defects pertaining to a certain design type. The authors recognized that many factors can affect an operator's choice for a particular type or brand of NiTi file—ability of the instrument to conform to the root canal curvature, cutting efficiency, torsional strength, fatigue resistance, and cost are but a few examples. It is likely that clinicians would attach a certain (but unequal) importance to each and every factor in their mind. Breakage of an endodontic instrument within the root canal can be a devastating incident to the operator. Although a tooth bearing a broken segment of an endodontic file within its root canal is not always doomed to failure (47), very few patients would gracefully accept the presence of a metallic fragment embedded within their tooth without any doubt.
Treating the NiTi rotary file as a disposable instrument, i.e., designating it for single use only, will reduce its chance of fracture during clinical use. That concept is corroborated by the results of this meta-analysis, with the “single use” strategy being able to significantly reduce the overall incidence of instrument fracture by over 15-fold. But then, even when single-use strategy is adopted, NiTi engine-files still showed a risk of fracture significantly >0 (see Figure 3B). Those single-use, heated treated instruments seemed to be minimally affected by separation; however, the amount of reports was very small to allow any meaningful comparison with their non-heat-treated counterparts. For clinicians who opted to sterilize the instrument for re-use, the operator has to accept a higher probability (about 3.6%) of instrument separation, that is, a significant increase from the single-use ones (about 0.22%).
It seems that there was an apparent correlation between the publication date and the reported incidence of instrument separation (see Table 1)—the earlier the article was published, the higher the rate reported. Over the years, as we understand more about the material, the mechanism and reasons of fracture, the better the chance for its prevention. There have been many recommended ways to avoid instrument breakage during use (5, 6, 8, 9), of which visual examination of the instrument, with or without magnification, is proposed almost universally. Deformed NiTi instruments are mechanically weakened and will only require a smaller load, or a lower number of revolutions to bring about fracture, compared with their intact undamaged counterparts (48, 49). Invariably, all manufacturers propose that distorted instruments should be discarded for good.
The recommendation of examining the NiTi file before use would help, but only if that distortion or the extent of plastic deformation should be visible in the clinical setting (with or without magnifying aids). Hence, the SQ value of a particular type of NiTi file might become a meaningful figure, as it indicates how likely the operator may notice any material distortions or plastic deformation that could predispose the instrument to failure upon further use in the root canal. Once a deformed file is discerned, the operator would discard and replace it with a new one, thus preventing the clinical mishap of instrument separation. The results of this study indicated that NiTi instruments of different design might demonstrate rather different SQ values (Figure 4). By definition, the higher the SQ value, the greater the chance for deformed instruments to be visually discernible. In other words, those instruments with a higher SQ value might be construed as “clinically safer,” with all other factors being equal and when instrument breakage only is concerned. With that in mind, it appears that the triangular fixed-taper and the triple-U design is likely to provide for the “safest” instrument (SQ = 37.7 and 14.0, respectively), as a great number of deformed files could be noticed (and so reported in the literature) before they should fracture in the canal. Heat-treated files have the highest safety quotient, due to the presence of martensitic phase (which has a lower modulus of elasticity) in the material brought about by the heat treatment.
Except for martensitic NiTi with shape memory property that would stay deformed upon pre-curving, permanent deformation of superelastic (austenitic) NiTi instruments, e.g., in the form of over screwing or unwinding, is a manifestation of structural defect or mechanical failure of the material (6, 9, 11). That over screwing or unwinding is a result of torsional load in excess of the (super)elastic limit. Finite elemental analysis (FEA) studies have reported on the reaction stresses and susceptibility of NiTi instruments to damages due to torsion or bending forces. There, it is noteworthy that the internal stresses developed within instruments of different cross-sectional design due to the torsional loads differed rather dramatically in their values, but that the internal stresses varied insignificantly upon different amounts of bending (50). In fact, it has also been demonstrated that the fatigue life is similar for instruments of different cross section when a proper strain-life analysis was employed, both by FEA (51) and actual experimentation (52).
There are many factors that can affect the chance of instrument fracture in use (9, 53, 54). The manufacturing process (raw material, fabrication method, heat, and/or surface treatment), root canal curvature (both radius and degrees), and presence of straight-line access which affect the curvature imposed on the instrument and/or glide path are some often-reported variables (53, 54). Manufacturers have been diligent in devising ways to produce instruments with improved torsional and fatigue resistance, compared to the first NiTi product that was introduced over 20 years ago. Heat treatment has been a promising and frequently employed method in recently introductions by nearly all manufacturers. This is reflected by the very low fracture rate that were seen in the heat-treated instruments, even when they were subject to multiple uses (see Figure 3D). On the other hand, designating the NiTi files as disposable, single-use instruments should cut down the influence of the inherent deficiency of material properties, if any, because the instrument would have been discarded before its mechanical limit (due to fatigue or torsion) is reached.
A limitation of the present study is related to the relatively small number of reports and the quality of data that were published in the literature. Although there were more than 30 reports qualified for this systematic review, almost one-third of them had not provided the complete data to permit further statistical analysis. In fact, it probably is becoming rather difficult nowadays to publish articles that purely present descriptive statistics of any phenomena, such as instrument separation. Indeed, no further such report was noted in the literature written in English since our search. That might also explain the scarcity of reports on the fracture incidence in the clinical setting for heat-treated (martensitic or shape memory) files that are rather new to the market. On the other hand, with the current mandate in some countries, as well as promotion by manufacturers, for treating the NiTi files as disposable instruments for reason of infection control, there is bound to be a reduction in the amount of instrument separation and of such reports in the literature. Another limitation might be related to the grouping instrument brands into general design categories. The authors recognized that file separation is multi-factorial and that it may not simply explained by the cross-sectional shape or body taper of the file system. The grouping was aimed to reduce the number of groups to enhance the power of the meta-analysis. Regarding the heat-treated instruments, from a metallurgical point of view, martensitic NiTi alloy demonstrates a higher resistance to crack initiation, compared with its superelastic counterpart (55). The fatigue life of martensitic NiTi has been shown to be superior to superelastic (austenitic) NiTi under strain-controlled condition (56), which condition is represented by a rotating NiTi wire being constrained into a constant curvature. Hence, theoretically, if a martensitic NiTi file should be used in mild-to-moderate curve that generate an alternating stress intensity below the crack initiation threshold of that martensitic NiTi material, crack initiation could be totally suppressed and, even if a microcrack should have been initiated, the effect of flexural fatigue would be attenuated to a clinically insignificant level. For the evaluation of effective strain imposed on the root canal instrument, careful assessment of the root canal curvature is essential (57, 58). But then, all these might become irrelevant for single-use instruments.
Within the limitations of this study, it may be concluded that different instrument designs would present an unequal risk of fracture for those instruments designated for multiple use. When NiTi files are subject to single uses, the fracture rate is similar for all brands. But then, certain design types may demonstrate visually discernible deformations (after use) more often than others. A “safety quotient” value is defined to inform the chance of spotting a deformed instrument before it might separate in the canal in the next use.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: in the articles included in the list of references.
Author Contributions
GC: conceptualization, methodology, writing—review and editing, and funding acquisition. MY and MT: methodology, formal analysis and investigation, and writing original draft preparation. All authors contributed to the article and approved the submitted version.
Funding
This study was partly funded by an Endodontic Research Fund of the University of Hong Kong (Account No. 200004107.12058.08008.001).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors MY and MT would like to acknowledge the support from the Undergraduate Research Programme at the Faculty of Dentistry, The University of Hong Kong. Thanks are due to Ms. Samantha K. Y. Li for her statistical support.
References
1. Haapasalo M, Shen Y. Evolution of nickel-titanium instruments: from past to future. Endod Topics. (2013) 29:3–17. doi: 10.1111/etp.12049
2. Del Fabbro M, Afrashtehfar KI, Corbella S, El-Kabbaney A, Perondi I, Taschieri S. In vivo and in vitro effectiveness of rotary nickel-titanium vs manual stainless steel instruments for root canal therapy: systematic review and meta-analysis. J Evid Based Dent Pract. (2018) 18:59–69. doi: 10.1016/j.jebdp.2017.08.001
3. Schäfer E, Schulz-Bongert U, Tulus G. Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study. J Endod. (2004) 30:432–5. doi: 10.1097/00004770-200406000-00014
4. Zupanc J, Vahdat-Pajouh N, Schafer E. New thermomechanically treated NiTi alloys - a review. Int Endod J. (2018) 51:1088–3. doi: 10.1111/iej.12924
5. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. (2006) 32:1031–43. doi: 10.1016/j.joen.2006.06.008
6. Cheung GSP. Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endod Topics. (2009) 16:1–26. doi: 10.1111/j.1601-1546.2009.00239.x
7. Bahia MG, Buono VT. Decrease in the fatigue resistance of nickel-titanium rotary instruments after clinical use in curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2005) 100:249–55. doi: 10.1016/j.tripleo.2004.10.013
8. Di Fiore PM. A dozen ways to prevent nickel-titanium rotary instrument fracture. J Am Dent Assoc. (2007) 138:196–201. doi: 10.14219/jada.archive.2007.0136
9. McGuigan M, Louca C, Duncan HF. Endodontic instrument fracture: causes and prevention. Br Dent J. (2013) 214:341–8. doi: 10.1038/sj.bdj.2013.324
10. Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. (2014) 72:39. doi: 10.1186/2049-3258-72-39
11. Sattapan B, Nervo GJ, Palamara JE, Messer HH. Defects in rotary nickel-titanium files after clinical use. J Endod. (2000) 26:161–5. doi: 10.1097/00004770-200003000-00008
12. Arens FC, Hoen MM, Steiman HR, Dietz GC Jr. Evaluation of single-use rotary nickel-titanium instruments. J Endod. (2003) 29:664–6. doi: 10.1097/00004770-200310000-00013
13. Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod. (2004) 30:722–5. doi: 10.1097/01.DON.0000129963.42882.C9
14. Alapati SB, Brantley WA, Svec TA, Powers JM, Nusstein JM, Daehn GS. SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical use. J Endod. (2005) 31:40–3. doi: 10.1097/01.DON.0000132301.87637.4A
15. Peng B, Shen Y, Cheung GSP, Xia TJ. Defects in ProTaper S1 instruments after clinical use: Longitudinal examination. Int Endod J. (2005) 38:550–7. doi: 10.1111/j.1365-2591.2005.00991.x
16. Cheung GSP, Peng B, Bian Z, Shen Y, Darvell BW. Defects in ProTaper S1 instruments after clinical use: fractographic examination. Int Endod J. (2005) 38:802–9. doi: 10.1111/j.1365-2591.2005.01020.x
17. Di Fiore PM, Genov KA, Komaroff E, Li Y, Lin L. Nickel-titanium rotary instrument fracture: a clinical practice assessment. Int Endod J. (2006) 39:700–8. doi: 10.1111/j.1365-2591.2006.01137.x
18. Shen Y, Cheung GSP, Bian Z, Peng B. Comparison of defects in ProFile and ProTaper systems after clinical use. J Endod. (2006) 32:61–5. doi: 10.1016/j.joen.2005.10.017
19. Cheung GSP, Bian Z, Shen Y, Peng B, Darvell BW. Comparison of defects in ProTaper hand-operated and engine-driven instruments after clinical use. Int Endod J. (2007) 40:169–78. doi: 10.1111/j.1365-2591.2006.01200.x
20. Wei X, Ling J, Jiang J, Huang X, Liu L. Modes of failure of ProTaper nickel-titanium rotary instruments after clinical use. J Endod. (2007) 33:276–9. doi: 10.1016/j.joen.2006.10.012
21. Shen Y, Haapasalo M, Cheung GS, Peng B. Defects in nickel-titanium instruments after clinical use. Part 1: relationship between observed imperfections and factors leading to such defects in a cohort study. J Endod. (2009) 35:129–32. doi: 10.1016/j.joen.2008.10.014
22. Shen Y, Cheung GS, Peng B, Haapasalo M. Defects in nickel-titanium instruments after clinical use. Part 2: fractographic analysis of fractured surface in a cohort study. J Endod. (2009) 35:133–6. doi: 10.1016/j.joen.2008.10.013
23. Shen Y, Coil JM, Haapasalo M. Defects in nickel-titanium instruments after clinical use. Part 3: a 4-year retrospective study from an undergraduate clinic. J Endod. (2009) 35:193–6. doi: 10.1016/j.joen.2008.11.003
24. Vieira EP, Nakagawa RK, Buono VT, Bahia MG. Torsional behaviour of rotary NiTi ProTaper Universal instruments after multiple clinical use. Int Endod J. (2009) 42:947–53. doi: 10.1111/j.1365-2591.2009.01602.x
25. Shen Y, Coil JM, McLean AGR, Hemerling DL, Haapasalo M. Defects in nickel-titanium instruments after clinical use. Part 5: single use from endodontic specialty practices. J Endod. (2009) 35:1363–7. doi: 10.1016/j.joen.2009.07.004
26. Inan U, Gonulol N. Deformation and fracture of Mtwo rotary nickel-titanium instruments after clinical use. J Endod. (2009) 35:1396–9. doi: 10.1016/j.joen.2009.06.014
27. Shen Y, Coil JM, Zhou HM, Tam E, Zheng YF, Haapasalo M. Profile Vortex instruments after clinical use: a metallurgical properties study. J Endod. (2012) 38:1613–7. doi: 10.1016/j.joen.2012.09.018
28. Chakka NV, Ratnakar P, Das S, Bagchi A, Kumar S, Anumula L. Do NiTi instruments show defects before separation? Defects caused by torsional fatigue in hand and rotary nickel-titanium. (NiTi) instruments which lead to failure during clinical use. J Contemp Dent Pract. (2012) 13:867–72. doi: 10.5005/jp-journals-10024-1243
29. Shen Y, Coil JM, Zhou H, Zheng Y, Haapasalo M. HyFlex nickel-titanium rotary instruments after clinical use: metallurgical properties. Int Endod J. (2013) 46:720–9. doi: 10.1111/iej.12049
30. Plotino G, Grande NM, Porciani PF. Deformation and fracture incidence of Reciproc instruments: a clinical evaluation. Int Endod J. (2015) 48:199–205. doi: 10.1111/iej.12302
31. Shen Y, Zhou H, Coil JM, Aljazaeri B, Buttar R, Wang Z, Zheng Y-F, Haapasalo M. ProFile Vortex and Vortex Blue nickel-titanium rotary instruments after clinical use. J Endod. (2015) 41:937–42. doi: 10.1016/j.joen.2015.02.003
32. Gambarini G, Piasecki L, Di Nardo D, Miccoli G, Di Giorgio G, Carneiro E, Al-Sudani D, Testarelli L. Incidence of deformation and fracture of Twisted File Adaptive instruments after repeated clinical use. J Oral Maxillofac Res. (2016) 7:e5. doi: 10.5037/jomr.2016.7405
33. Shen Y, Coil JM, Mo AJ, Wang Z, Hieawy A, Yang Y, Haapasalo M. WaveOne rotary instruments after clinical use. J Endod. (2016) 42:186–9. doi: 10.1016/j.joen.2015.10.008
34. Shen SM, Deng M, Wang PP, Chen XM, Zheng LW, Li HL. Deformation and fracture of K3 rotary nickel-titanium endodontic instruments after clinical use. Int Endod J. (2016) 49:1088–94. doi: 10.1111/iej.12561
35. Al-Fouzan KS. Incidence of rotary ProFile instrument fracture and the potential for bypassing in vivo. Int Endod J. (2003) 36:864–7. doi: 10.1111/j.1365-2591.2003.00733.x
36. Shen Y, Peng B, Fan B, Bian Z, Fan MW. Clinical analysis of the fracture of nickel-titanium instruments during root canal therapy. Zhonghua Kou Qiang Yi Xue Za Zhi. (2004) 39:38–41. doi: 10.1111/j.1365-2591.2006.01123.x
37. Iqbal MK, Kohli MR, Kim JS. A Retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod. (2006) 32:1048–52. doi: 10.1016/j.joen.2006.03.001
38. Wolcott S, Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S, Meyers J. Separation incidence of ProTaper rotary instruments: a large cohort clinical evaluation. J Endod. (2006) 32:1139–41. doi: 10.1016/j.joen.2006.05.015
39. Spanaki-Voreadi AP, Kerezoudis NP, Zinelis S. Failure mechanism of ProTaper Ni-Ti rotary instruments during clinical use: fractographic analysis. Int Endod J. (2006) 39:171–8. doi: 10.1111/j.1365-2591.2006.01065.x
40. Knowles KI, Hammond NB, Biggs SG, Ibarrola JL. Incidence of instrument separation using LightSpeed rotary instruments. J Endod. (2006) 32:14–6. doi: 10.1016/j.joen.2005.10.008
41. Tzanetakis GN, Kontakiotis EG, Maurikou DV, Marzelou MP. Prevalence and management of instrument fracture in the postgraduate endodontic program at the Dental School of Athens: a five-year retrospective clinical study. J Endod. (2008) 34:675–8. doi: 10.1016/j.joen.2008.02.039
42. Shen Y, Winestock E, Cheung GSP, Haapasalo M. Defects in nickel-titanium instruments after clinical use. Part 4: an electropolished instrument. J Endod. (2009) 35:197–201. doi: 10.1016/j.joen.2008.11.012
43. Wu J, Lei G, Yan M, Yu Y, Yu J, Zhang G. Instrument separation analysis of multi-used ProTaper Universal rotary system during root canal therapy. J Endod. (2011) 37:758–63. doi: 10.1016/j.joen.2011.02.021
44. Cunha RS, Junaid A, Ensinas P, Nudera W, Bueno CE. Assessment of the separation incidence of reciprocating WaveOne files: a prospective clinical study. J Endod. (2014) 40:922–4. doi: 10.1016/j.joen.2014.03.016
45. Wei X, Cheung GS. Performance of three nickel-titanium instruments for preparing curved root canals to two different apical dimensions. Chin J Dent Res. (2002) 5:32–42.
46. Cheung GSP, Liu CSY. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J Endod. (2009) 35:938–43. doi: 10.1016/j.joen.2009.04.016
47. Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. (2005) 31:845–50. doi: 10.1097/01.don.0000164127.62864.7c
48. Gambarini G. Cyclic fatigue of ProFile rotary instruments after prolonged clinical use. Int Endod J. (2001) 34:386–9. doi: 10.1046/j.1365-2591.2001.00259.x
49. Kim JY, Cheung GS, Park SH, Ko DC, Kim JW, Kim HC. Effect from cyclic fatigue of nickel-titanium rotary files on torsional resistance. J Endod. (2012) 38:527–30. doi: 10.1016/j.joen.2011.12.018
50. Zhang EW, Cheung GS, Zheng YF. Influence of cross-sectional design and dimension on mechanical behavior of nickel-titanium instruments under torsion and bending: a numerical analysis. J Endod. (2010) 36:1394–8. doi: 10.1016/j.joen.2010.04.017
51. Cheung GSP, Zhang EW, Zheng YF. A numerical method for predicting the bending fatigue life of NiTi and stainless steel root canal instruments. Int Endod J. (2011) 44:357–61. doi: 10.1111/j.1365-2591.2010.01838.x
52. Cheung GSP, Darvell BW. Fatigue testing of a NiTi rotary instrument. Part 1: strain-life relationship. Int Endod J. (2007) 40:612–8. doi: 10.1111/j.1365-2591.2007.01262.x
53. Jonker C, van der Vyver PJ. Factors influencing the life span of modern root canal instruments–a literature review. South Afr Dent J. (2013) 68:14–23.
54. Tang W-R, Smales RJ, Chen H-F, Guo X-Y, Si H-Y, Gao L-M, et al. Prevention and management of fractured instruments in endodontic treatment. World J Surg Proced. (2015) 5:82–98. doi: 10.5412/wjsp.v5.i1.82
55. McKelvey AL, Ritchie RO. Fatigue-crack growth behavior in the superelastic and shape-memory alloy nitinol. Metall Mater Trans A. (2001) 32:731–43. doi: 10.1007/s11661-001-0089-7
56. Robertson SW, Pelton AR, Ritchie RO. Mechanical fatigue and fracture of Nitinol. Int Mater Rev. (2012) 57:1–37. doi: 10.1179/1743280411Y.0000000009
57. Cheung GSP, Darvell W. Fatigue testing of a NiTi rotary instrument. Part 1: strain-life relationship. Int Endod J. (2007) 40:612–8.
Keywords: nickel-titanium (NiTi), engine-file, instrument separation, fracture, deform, endodontic, instrumentation
Citation: Yon MJ-y, Tang MH-y and Cheung GS-p (2021) Defects and Safety of NiTi Root Canal Instruments: A Systematic Review and Meta-Analysis. Front. Dent. Med. 2:747071. doi: 10.3389/fdmed.2021.747071
Received: 25 July 2021; Accepted: 15 September 2021;
Published: 12 October 2021.
Edited by:
Ya Shen, University of British Columbia, CanadaReviewed by:
Sangwon Kwak, Pusan National University, South KoreaSyed Saad Bin Qasim, University of Oslo, Norway
Copyright © 2021 Yon, Tang and Cheung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gary Shun-pan Cheung, c3BjaGV1bmdAaGt1Lmhr