 Jayakumar Jayaraman
Jayakumar Jayaraman- Department of Pediatric Dentistry, Virginia Commonwealth University School of Dentistry, Richmond, VA, United States
Aim: The first comprehensive chart on dental development was published 75 years ago based on Caucasian children and this has been used as a standard dental chart to date. Few population specific charts have been developed recently and updated dental charts on modern subjects can provide more information on dental development patterns. This study aims to construct a comprehensive dental atlas for modern Chinese children and young adults to assist in clinical, forensic, and public health applications.
Methods: The study sample comprised of 2,306 subjects, age ranging from 2 to 24 years belonging to Chinese ethnicity. Dental formation and eruption of permanent teeth and resorption of primary teeth were analyzed separately for females and males. For each age range, the number of teeth (n), and the stage of development was calculated for first (Q1), second (Q2) and third quartiles (Q3). Similar analysis was performed for the position of permanent teeth and the resorption of primary teeth. To determine the variations between the sex, Mann-Whitney U-test was conducted by comparing the median (Q2) stages.
Results: Variations in dental formation and eruption of permanent teeth and resorption of primary teeth were observed between maxillary and mandibular dentitions and between the sex, however the difference was not statistically significant (p = 0.535 to p = 1.000). The dental atlas was presented separately for Chinese females and males.
Conclusion: This atlas on modern Chinese population serves as a practical tool to assist in clinical diagnosis and treatment planning, in forensic investigations as well as indicators of developments in public health.
1 Introduction
Dental development is a sequential process that passes through several stages of formation to erupt to its final position in the arch. The primary teeth and first permanent molars start to develop in-utero and skeletal specimens serve as an ideal tool to evaluate early stages of dental development. This is usually conducted by direct vision of the skeletal remains; however, radiological and histological evaluation can also be of some assistance. For permanent teeth, radiographs provide an excellent platform to record dental development. Different methods of staging dental development have been proposed in the literature that varies between 4 and 32 stages (1–3); the most accepted being the eight-stage Anglo-Canadian classification system (1). Similarly, the stages of resorption of roots of primary teeth have been analyzed that classified into 4 and 5 stages respectively (3, 4). The eruption of teeth has been evaluated and a five-stage classification system was proposed to relate the position of the tooth in the arch (5). This original system has been modified into a four-stage system in the London Atlas study (4).
The first comprehensive chart on dental development was published in 1941 based on Caucasian children in the United States and this has been commonly used as a standard dental atlas chart for several decades (6). The reliability of using this chart has been questioned due to the smaller number of samples in each age group. This chart was based on histological specimens of only 25 children out of which only seven were in the age range of 2 to 15 years (7). Several investigators have shown the presence of population differences in dental development (8, 9). Considering this, population specific charts has been developed and this includes London Atlas based on Caucasian and Bangladeshi populations in London (4), Australian Atlas (10, 11), and most recently, WITS Atlas based on southern African population (12).
Chinese constitute one of the major population and occupies one fifth of the total human population in the world and about 94% of people living in Hong Kong are of Chinese, predominantly of Cantonese origin but there was some admixture of other subgroups (13). The data on eruption of permanent teeth in Chinese was first presented 50 years ago and was not updated since then (14). Moreover, their study did not analyze the entire picture of dental development namely dental formation, eruption and resorption. To our understanding, there was no comprehensive dental atlas for Chinese population. This study was aimed to evaluate dental development pattern and subsequently construct dental atlas for Chinese children and young adults.
2 Materials and methods
2.1 Study population
The study comprised of 2,306 subjects, age ranging from 2 to 24 years with equal number of males and females, refer to Table 1. All the subjects were of southern Chinese ethnicity belonging to middle socioeconomic status and the Dental Panoramic Tomographs (DPT) were obtained from the archives of a teaching hospital in Hong Kong, Special Administrative Region of China. The radiographs were previously scored for a Dental Age Estimation study and have been re-used in the current study (15). The study was approved by the Institutional Review Board (Reference No: UW 12-280). The author retains ownership of the collected dataset and subsequent secondary analysis of the de-identified data presented in this manuscript. Only healthy subjects are included and those with severe anomalies that might affect dental development were excluded from the study. All the radiographs were scored by a single trained and calibrated examiner (JJ) with intra-examiner reliability Kappa score of 0.85. These scores correspond to “almost perfect” correlation (16). The radiographs were digitized at 300 dpi in gray scale format using a flatbed scanner and viewed in a dark room on a wide screen monitor at a magnification rate of 160% (Philips 271E, Philips Industries, Taiwan). When in doubt, the digitized images were enlarged up to 300% for better evaluation. Each tooth was designated by an alphabet followed by a number, for example, UL1 refers to Upper Left Central Incisor, UL2 refers to Upper Left Lateral Incisor and so on. The median (Q2), lower (Q1) and upper (Q3) interquartile ranges for each tooth was calculated separately for males and females. This analysis was conducted for formation and eruption of permanent dentition and resorption of primary dentition at different age ranges. The median stages are compared in this study due to the assumption that the data is not normally distributed. To determine the variations in dental development in males and females, Mann-Whitney U-test was conducted by comparing the median (Q2) stages of dental formation, eruption stages and resorption stages (SPSS Version 20.0, IBM Corp, Armonk, NY).
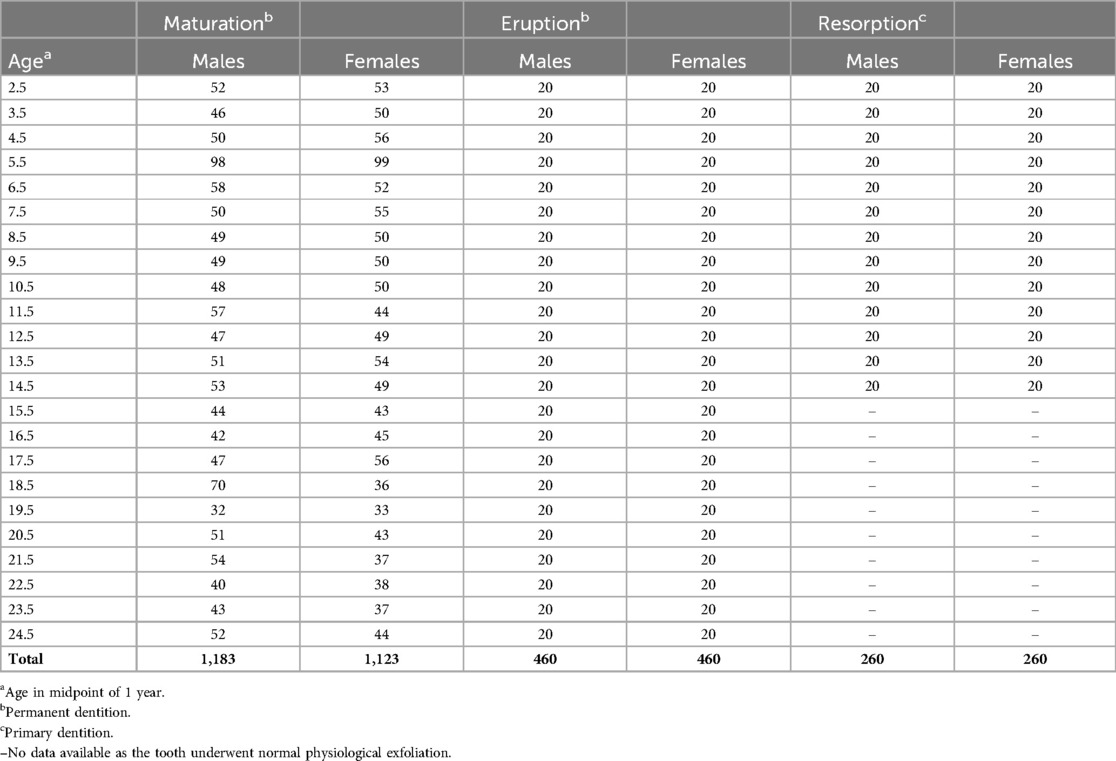
Table 1. Distribution of Chinese subjects used to analyse the formation and eruption of permanent teeth and resorption of primary teeth.
2.2 Formation of permanent teeth
Formation of permanent tooth was evaluated from 2,306 subjects based on Anglo-Canadian standards of dental formation designated in alphabets stages A to H, starting with initial calcification of tooth (stage A) up to completion of the root development (stage H), see Figure 1. All the teeth on the left side of the arch were evaluated for the stage of development (1). When a tooth in the left side is missing, the corresponding tooth on the right side was scored. The stages were recorded on a score card including the details of sex, ethnicity, date of birth and the date of exposure of the radiograph. The data was entered in the Microsoft Access database to calculate the average age for each corresponding stage of development (TDS) for each tooth morphology type (TMT). The details were then transferred to Microsoft Excel spreadsheet separately for males and females aged 2 to 24 years. For each age range, the number of teeth (n) and the corresponding stage of development were calculated for lower quartile (Q1), second quartile (Q2) and upper quartile (Q3) ranges. The stage corresponding to median (Q2) was used to develop dental formation charts for each age range, and separately for males and females.
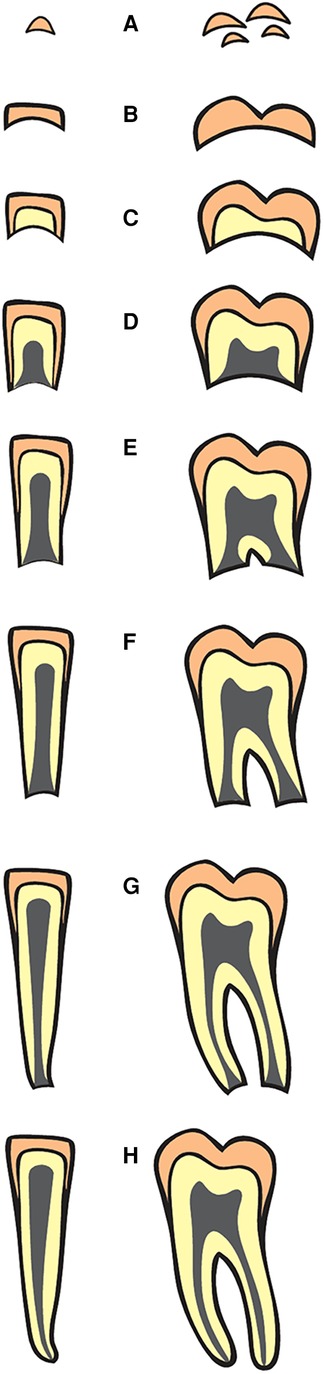
Figure 1. Classification of staging of dental formation (Stages A to H) in single and multi-rooted teeth (Data source: reference (1)).
2.3 Eruption of permanent teeth
To evaluate the position of permanent teeth in the arch, a total of 920 radiographs were randomly chosen from the total dataset partitioned by age and sex. This comprised twenty radiographs per age and sex of subjects aged 2 to 24 years. The most used classification stages of eruption of teeth follows five stages designated by P-I to P-V. Position P-I corresponds to tooth in full occlusion and P-V signifies the position of the tooth below the apical third of the primary root or more than 2 mm below the bone when the predecessor is absent. This observation was based on the permanent molars (5). However, this classification system did not consider of position of permanent teeth at subsequent categorical stages of development. In this study, a new classification system for staging dental eruption was adopted designated as E1 to E6, where E1 to E3 infers intra-osseous and E4 to E6 corresponds to extra-osseous positioning of permanent teeth. Stage E4 refers to radiographic position of tooth just above the alveolar bone level. A detailed description of this classification system was presented in Figure 2.
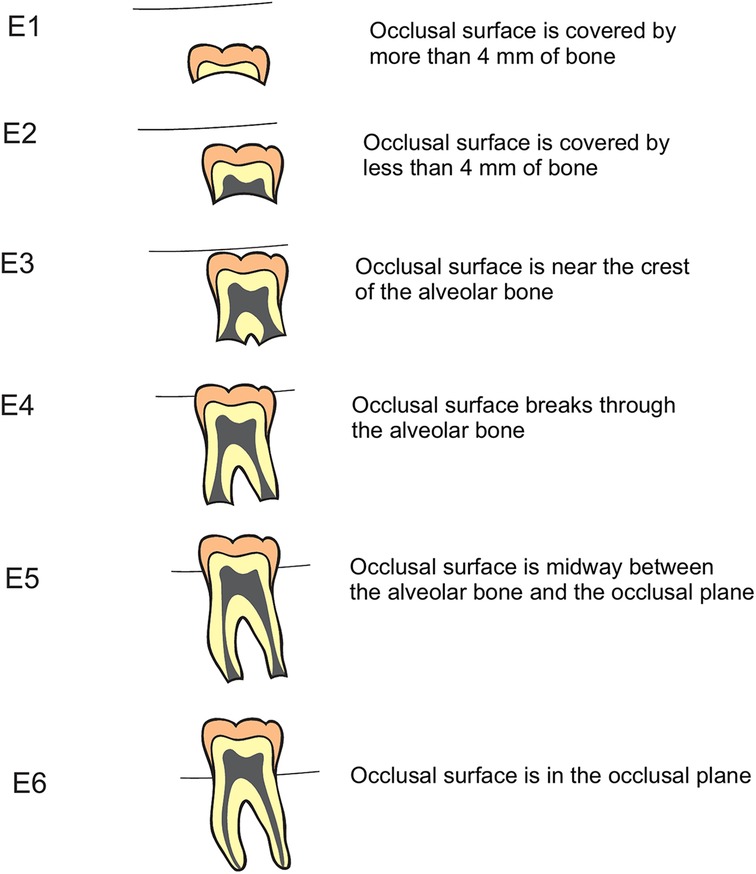
Figure 2. Classification of staging of eruption of teeth (Stages E1 to E6) in relation to alveolar bone level (Data source modified from: reference (5)).
2.4 Resorption of primary teeth
A total of 520 radiographs, comprising of 20 radiographs for each sex and age between ages 2 and 14 were chosen to evaluate the resorption pattern of primary teeth (3). This sample was randomly obtained from the same data used to analyze eruption pattern of permanent teeth. Resorption of maxillary and mandibular primary teeth was analyzed by stages defined by Moorrees and co-workers; Ac corresponds to tooth with complete root development without radiological signs of resorption, Res1/4 showing one quarter root resorption, Res1/2 and Res3/4 corresponding to half and three quarters of resorption respectively, see Figure 3.
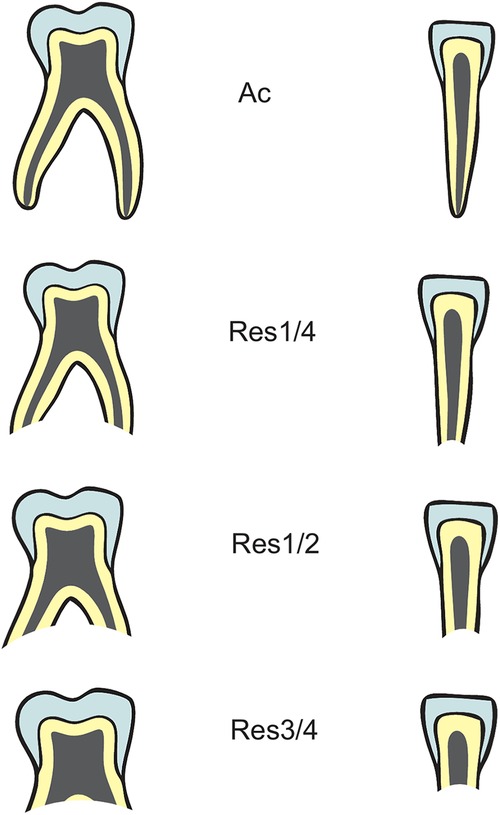
Figure 3. Classification of resorption patterns (Stages Ac, Res1/4, Res1/2, Res3/4) of single and multi-rooted primary teeth (Data source: reference (3)).
3 Results
3.1 Assessment of dental development
Mann-Whitney U-test was used to compare the median stage (Q2) of formation between males and females in the maxillary and mandibular dentitions at each age range from 2 to 24 years. One or two stage difference was observed in the median stages of dental formation of permanent teeth between maxillary and mandibular dentitions and between the sex. Between sexes, stage difference in formation of teeth was observed in all the age ranges except 3 and 7 years in the maxillary dentition and 4, 7, and 14 years in the mandibular dentition. The difference was not statistically significant between the sexes across all the age ranges (p = 0.535 to p = 1.000), see Table 2.
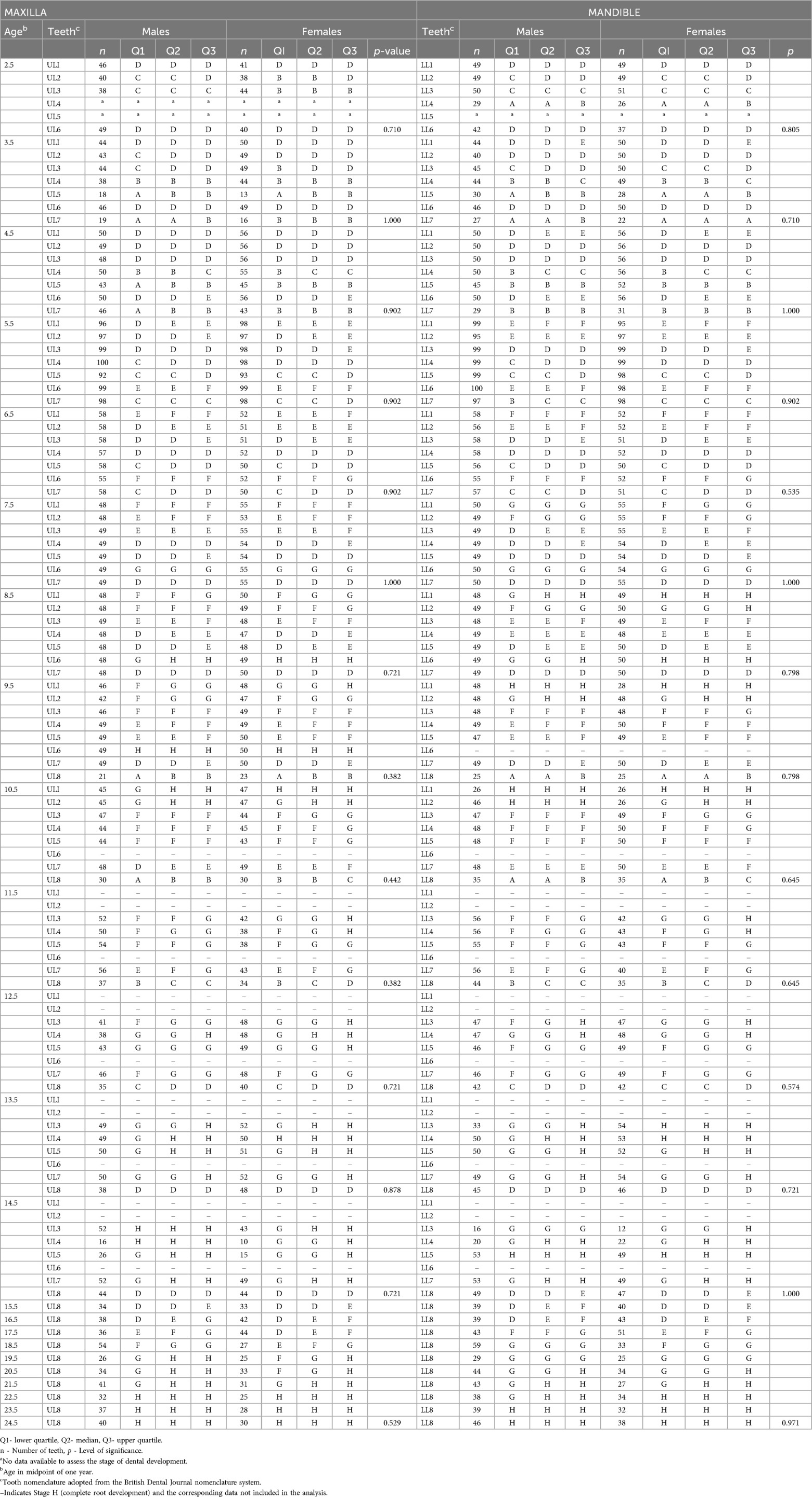
Table 2. Formation of maxillary and mandibular permanent teeth of 2 to 24 years old Chinese females and males.
The median positioning of the permanent teeth as indicated by the rate of eruption varied between males and females and between the dentitions. In both maxillary dentition, and mandibular dentitions, difference in eruption pattern between the sexes was observed more in the younger age ranges and the most varying presentation in the eruption was observed in the third molars in both maxillary dentitions. Mann-Whitney U-test no statistically significant difference between the sexes in all the age groups (p = 0.721 to p = 1.000), see Table 3.
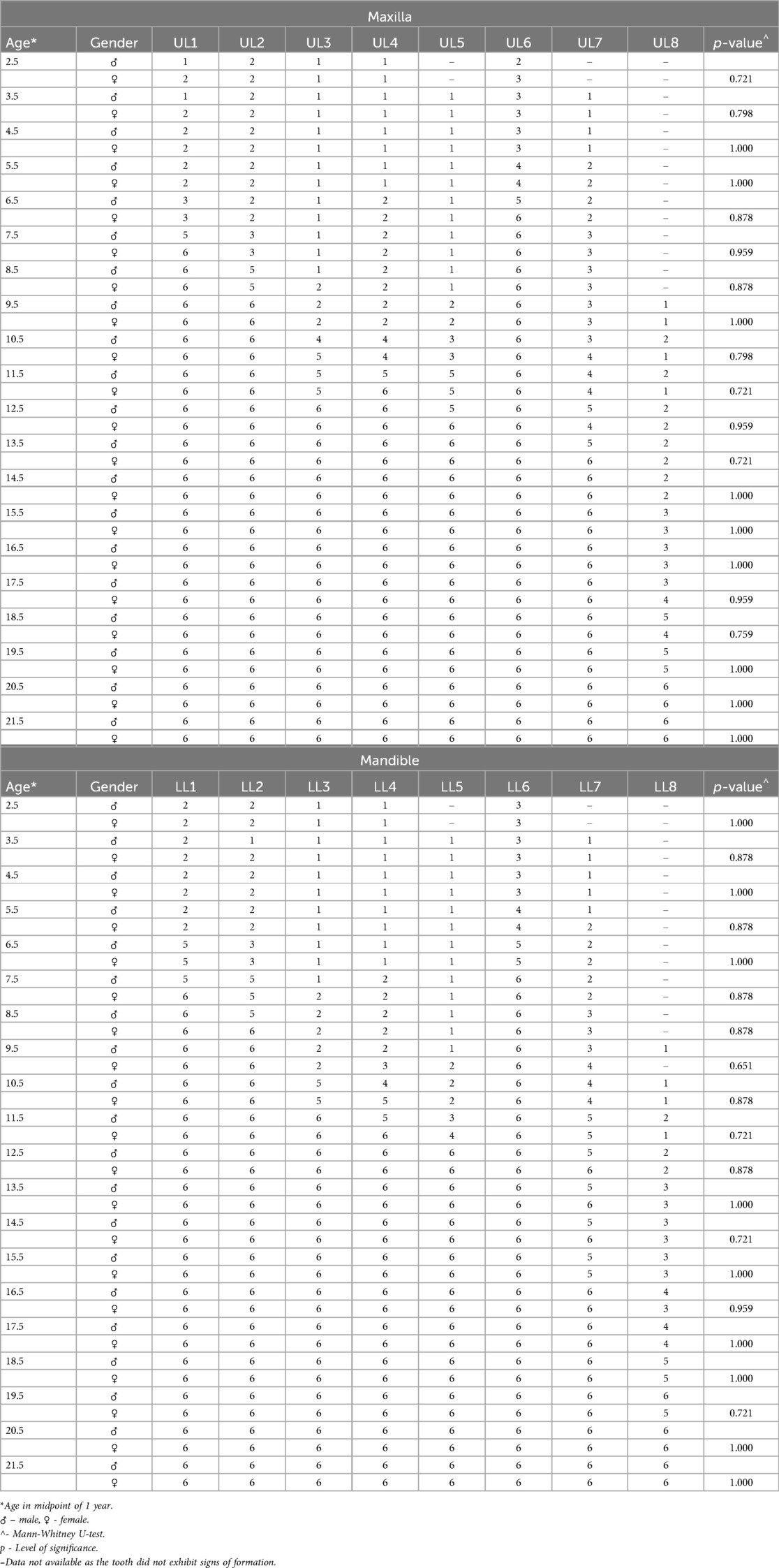
Table 3. Position of maxillary and mandibular permanent teeth in the arches of 2 to 21 years old Chinese females and males.
For the children aged 2 to 14 years, the resorption pattern of primary teeth was more pronounced in the maxillary dentition compared to the mandibular dentition. At 2 years, all the primary teeth showed complete root development in males and except maxillary and mandibular canines that had an open apex. Both canines underwent root closure in the subsequent year. Difference in resorption between males and females was observed in 2, 4, 5, 8, 9, and 10 year-old children in the maxillary dentition and 2, 5, 6, and 10-year-old children in the mandibular dentition. However, Mann-Whitney U-test showed no statistically significant difference in the resorption pattern of primary teeth in males and females in all age ranges (p = 0.690 to p = 1.000), see Table 4.
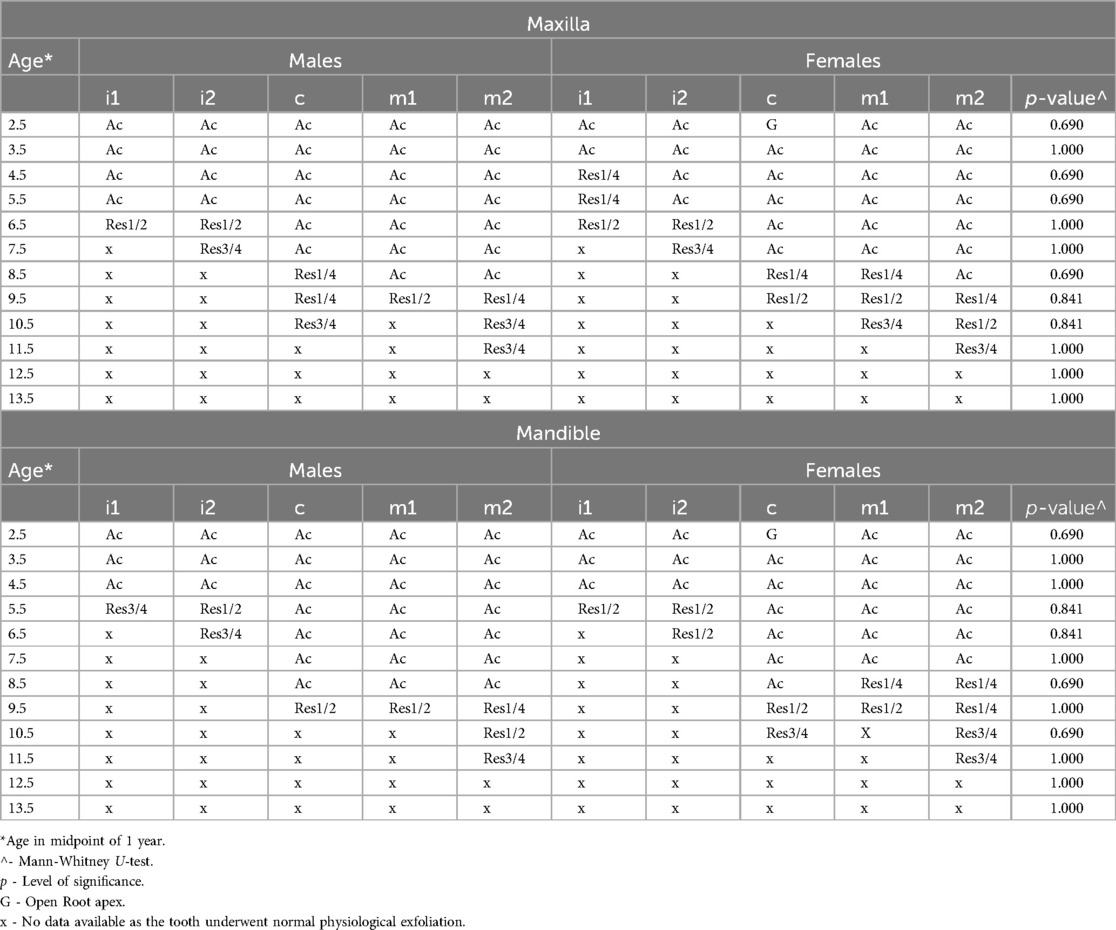
Table 4. Resorption of maxillary and mandibular primary teeth of 2 to 13 years old Chinese females and males.
3.2 Construction of dental charts
The formation and eruption patterns of permanent teeth and resorption pattern of primary teeth were different between males and females by one or two stages difference in most age ranges. Since dental development was different between the males and females, the data were presented as gender specific charts for females (Figure 4) and males (Figure 5). Templates of ten primary and sixteen permanent tooth morphology type (TMT) on the right side were obtained from a dental anatomy textbook (17). The images of teeth were carefully hand drawn and digitized using Adobe Photoshop software (Version CS6, Adobe Systems Ltd, Ireland). Internal tooth structures including enamel, dentin and pulp were colored appropriately to differentiate primary and permanent teeth. To illustrate different stages of dental formation, single tooth diagrams were prepared to exhibit eight stages of development resulting in a total of 128 images (16 TMT x 8 stages). For tooth resorption stages for primary tooth, three root resorption stages were incorporated yielding 30 images (10 TMT×3 stages). To construct dental charts, for each age range, images relating to the data for formation, and resorption were obtained. Individual images were then compiled to produce dental atlas charts for males and females aged 2 to 14 years. Since all permanent teeth except third molars completed development by 14 years, for ages 15 to 22 years, charts were constructed only for third molars. The images and charts were constructed by the first author (JJ) using Corel Draw Graphics software (CorelDRAW Graphics Suite X8, ON, Canada).
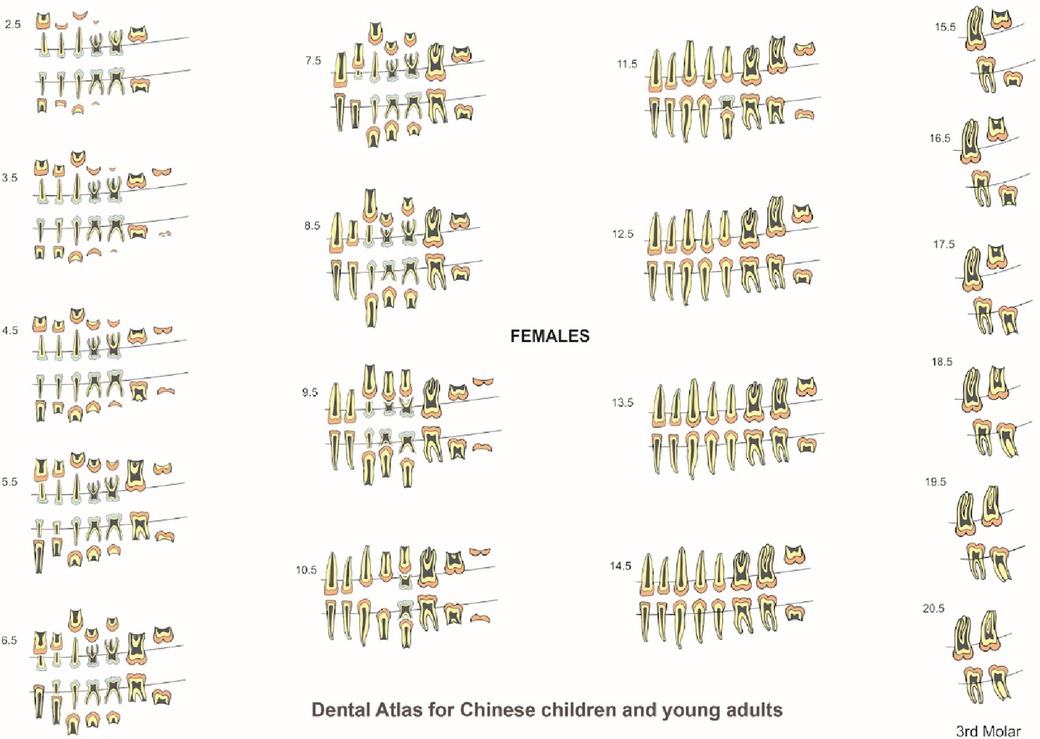
Figure 4. Dental atlas for Chinese females based on the formation and eruption of permanent teeth and resorption of primary teeth.
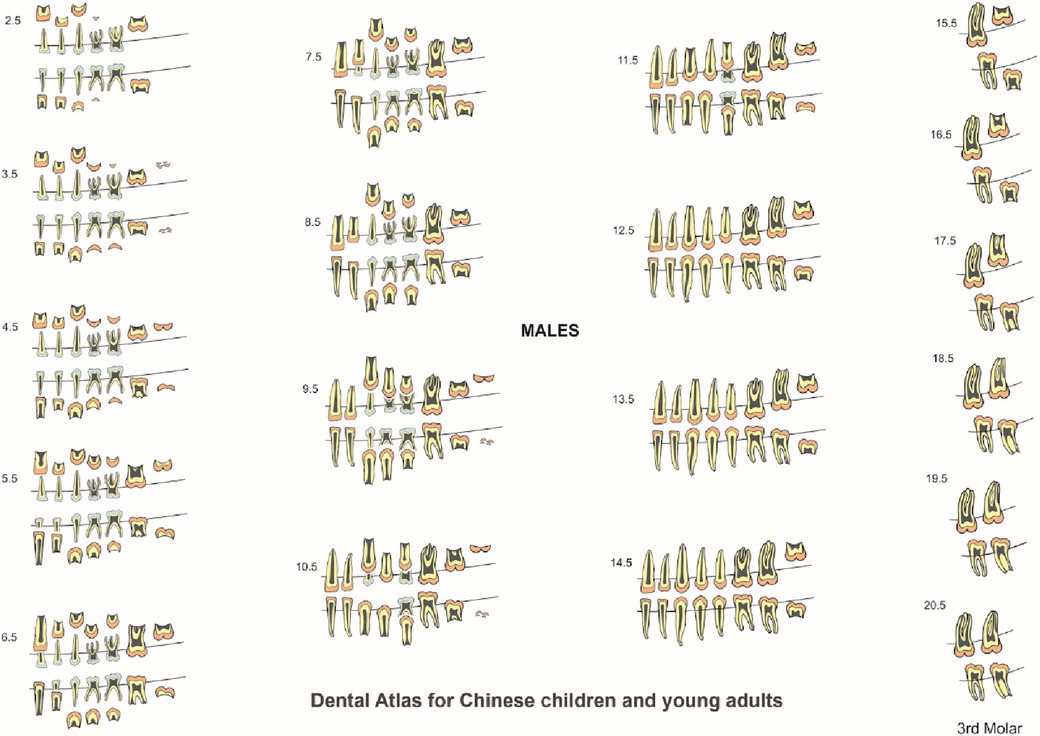
Figure 5. Dental atlas for Chinese males based on the formation and eruption of permanent teeth and resorption of primary teeth.
4 Discussion
Differences in dental emergence have been reported in different population groups. For example, advanced dental formation and emergence was reported in the WITS Atlas (12) based on black southern Africans compared to London Atlas that was based on Bangladeshi and Caucasian children (4). Dental age estimation was conducted using the London Atlas on mixed ethnic population in London and found to be accurate compared to Schour & Massler and Ubelaker charts (18). A similar finding was observed when the London Atlas was tested in Hispanic (19) as well as Iranian populations (20). In contrast, a study that tested the applicability of three dental charts including the London Atlas in New Zealand population found that all the charts demonstrated low accuracy and precision. This study further emphasized the need for population specific dental charts for accurate age estimation (21). Like population variations, sex difference in dental maturation was also an established phenomenon. Advanced dental emergence has been reported in girls compared to boys (22–24). However, a study that tested the accuracy of London Atlas in Portuguese population found difference between sexes and indicated the need for separate dental charts for each sex (25). In the present study, some difference was observed between the sexes; in females, both maxillary and mandibular first molars attained median stage of root closure at 8.5 years, one year earlier than in males. Similarly, canines and maxillary first pre-molars completed root development much earlier in females. In contrast, males showed advancement in the formation of maxillary third molar as the root apex closed at 19.5 years compared to 21.5 years in females. This trend was not observed in the mandibular third molar development, where root closure occurred around 21.5 years in both sex. Since the difference was not statistically significant, the data for males and females were combined and reported as a single dental atlas.
Eruption of permanent teeth is influenced by many other factors; socio-economic status, with their implicit connection with nutritional and health status (26), fluoride ingestion (27), and climate (28) have all been analyzed to possibly affect eruption timings. In contrast, a study conducted in southern Chinese children reported no significant difference in the eruption of teeth among children of low, medium and high socio-economic status (14). A similar finding was also observed in African Black children (29). Esan & Schepartz performed sample size calculation and found that a minimum sample size of 40 per age cohort was required to develop population specific dental atlas (12). In the present study, the data on dental maturation of permanent teeth from 2,306 subjects was re-used from the previous dental age study, accounting to over 80 subjects in each age cohort between 2 and 24 years of age (15). However, to analyze eruption of permanent teeth and resorption of primary teeth, we utilized only 40 samples per age cohort from the total sample. This sample size was relatively higher or equivalent to previous studies on dental atlas (4, 12).
The Chinese children in this study demonstrated advanced dental eruption in so much that all permanent teeth had erupted at 11.5 years whilst the London Atlas children had retained primary maxillary canines and both maxillary and mandibular second molars at this age. When the sex data were combined to compare the timing of eruption of the permanent teeth between the London Atlas and Chinese subjects in the current study, it was found that except for maxillary canines, all maxillary and mandibular incisors erupted earlier in subjects in the London Atlas. In contrast, pre-molars erupted earlier in Chinese children; however, first and second molars were similar between these groups. Both London Atlas and Chinese subjects had half of the roots of third molars formed at 16.5 years, whilst the Black African children demonstrated similar stage at 14.5 years. The root closure of third molars occurred at 17.5 years in Black African subjects whilst it happened at 21.5 years in Chinese and London Atlas subjects. These findings suggest the possibility of population variations in dental formation in third molars between the London Atlas, African Black and the Chinese subjects (4, 12). Comparison of dental development between the London Atlas and the WITS Atlas for each age cohort had been already reported (12). Another area of discussion is influence of secular trends in dental development. It has been shown that children born in different centuries (30) and between few decades (31, 32) have different patterns of dental development. This trend has also been observed in 5–6 years old Chinese children (33). To address this issue, in the current study, we utilized only radiographs belonging to modern samples. This study was conducted in 2012 and the search criteria was restricted to include only the most recent samples to represent modern day children, adolescents and young adults. The age of subjects ranged from 2 to 24 years and the date of birth of the subjects were between 1985 and 2010. For example, for 5-year old children, those who were born around 2005 alone were obtained and a similar search strategy was extended to all other age ranges.
Standards for emergence of permanent teeth in southern Chinese children were first reported in 1965 (12). This study was based on clinical observation and hence did not include other aspects of dental development including the resorption of primary teeth and formation pattern of permanent teeth at subsequent years. In our study, all the parameters of tooth formation and eruption were assessed from radiographs. It has been reported that early loss of primary molars delays the eruption of the premolars and conversely, delayed exfoliation results in earlier eruption of the premolars (34). Accelerated eruption of premolars beneath the pulpotomized primary molars have also been reported (35). In addition, trauma (36), odontogenic cysts (37), odontogenic tumors (38), gingival enlargements (39), and supernumerary tooth (40) has been reported to influence dental formation and emergence. Consequently, subjects with severe dental anomalies and other forms of development disorders were excluded from the analysis. It is evident that pathologically affected primary teeth influences the eruption of permanent teeth; however, the relationship between the pathologically involved primary teeth and the stage of formation of permanent teeth has not been established yet (34).
The method in which median stages of dental development analyzed in this study was like a study conducted in the London Atlas study (4). For subjects aged 2 to 14 years, the entire complement of maxillary and mandibular dentition was displayed in the atlas. Since all the teeth had attained complete development by 14 years, for age range of 15 to 20 years, we have presented only maxillary and mandibular third molars. This is like the London Atlas that had full dentition until 15 years followed by third molars in the 16 to 23 years range. Radiographs of subjects used in this study represent a sample population of Chinese ethnic group living in Hong Kong. They are identified by the uniqueness of their name and the family details recorded in the patient files. All the radiographs were primarily taken to assist in clinical diagnosis and were hence re-used in the current study. It is to be noted that panoramic radiographs for young patients below 5 years of age were obtained only following strong indication to assist in diagnosis and treatment planning. Occasionally, they were also taken on uncooperative children who resist to taking conventional intraoral radiographs.
Demirjian’s 8 stage method was used in our study considering the reliability and ease in identification of stages. This staging method was like the WITS Atlas study (12), however, The London Atlas study utilized 13 stage method (4). To evaluate initial stages of development of primary teeth, investigators must rely on skeletonized or preserved human remains with known details of birth and death. The London Atlas study comprised of skeletal samples as young as 30 weeks in-utero that were obtained from Maurice Stack collection at the Royal College of Surgeons of England (4). In current study, archived samples of modern Chinese subjects aged 4 months to 2 years old could not be found and so, it was impossible to present data corresponding to this age. Moreover, it has been shown that the London dental atlas tends to overestimate the age (41). Following this, a recent review questioned the logic of using dental atlas for age estimation. It reviewed five dental atlases and found inconsistency I the study design, statistical procedures and presentation styles (42). This dental atlas should be used with caution for the purpose of dental age estimation as the age is segregated by the mid-point of one year. Moreover, this atlas has not been subjected to blind validation analysis. For accurate estimation of age, it is recommended to use simple average method (SAM) as described in the author’s previous article (15).
5 Conclusions
We have presented evidence based dental chart developed from a large sample of children and young adults of Chinese ethnicity. This dental atlas serves as a practical tool for age estimation in forensic investigations, assist in clinical diagnosis and treatment planning as well as indicators of developments in public health. Future research should focus on generating population specific data on dental development as well as integrating newer imaging technologies.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the study was approved by the University of Hong Kong West Cluster Institutional Review Board (Reference No: UW 12-280). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JJ: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The author would like to thank Dr. Nigel King, former Professor of Pediatric Dentistry at the University of Hong Kong for reviewing the original draft of the manuscript.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author declares that he is an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdmed.2024.1434417/full#supplementary-material.
References
1. Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. (1973) 45:211–27.4714564
2. Haavikko K. Tooth formation age estimated on a few selected teeth. A simple method for clinical use. Proc Finn Dent Soc. (1974) 70:15–9.4821943
3. Moorrees CF, Fanning EA, Hunt EE Jr. Formation and resorption of three deciduous teeth in children. Am J Physical Anthropol. (1963) 21:205–13. doi: 10.1002/ajpa.1330210212
4. AlQahtani SJ, Hector MP, Liversidge HM. Brief communication: the London atlas of human tooth development and eruption. Am J Physical Anthropol. (2010) 142:481–90. doi: 10.1002/ajpa.21258
5. Bengston RG. A study of the time of eruption and root development of the permanent teeth between six and thirteen years. Northwest Univ Bull. (1935) 35:3–9.
7. Logan WH, Kronfeld R. Development of the human jaws and surrounding structures from birth to the age of fifteen years. J Am Dent Assoc. (1933) 20:379–428.
8. Al-Tuwirqi A, Holcombe T, Seow WK. A study of dental development in a Caucasian population compared with a non-Caucasian population. Eur Arch Paediatr Dent. (2011) 12:26–30. doi: 10.1007/BF03262775
9. Jayaraman J, Roberts GJ. Comparison of dental maturation in Hong Kong Chinese and United Kingdom Caucasian populations. Forensic Sci Int. (2018) 292:61–70. doi: 10.1016/j.forsciint.2018.09.005
10. McKenna CJ, James H, Taylor JA, Townsend GC. Tooth development standards for South Australia. Aust Dent J. (2002) 47:223–7. doi: 10.1111/j.1834-7819.2002.tb00333.x
11. Blenkin M, Taylor J. Age estimation charts for a modern Australian population. Forensic Sci Int. (2012) 221:106–12. doi: 10.1016/j.forsciint.2012.04.013
12. Esan TA, Schepartz LA. The WITS atlas: a black southern African dental atlas for permanent tooth formation and emergence. Am J Physical Anthropol. (2018) 166:208–18. doi: 10.1002/ajpa.23424
13. Chen J, Zheng H, Bei JX, Sun L, Jia WH, Li T, et al. Genetic structure of the Han Chinese population revealed by genome-wide SNP variation. Am J Hum Genet. (2009) 85:775–85. doi: 10.1016/j.ajhg.2009.10.016
14. Lee MM, Low WD, Chang KS. Eruption of the permanent dentition of Southern Chinese children in Hong Kong. Arch Oral Biol. (1965) 10:849–61. doi: 10.1016/0003-9969(65)90078-6
15. Jayaraman J, Wong HM, King NM, Roberts GJ. Development of a reference data set (RDS) for dental age estimation DAE) and testing of this with a separate validation set (VS) in a southern Chinese population. J Forensic Leg Med. (2016) 43:26–33. doi: 10.1016/j.jflm.2016.07.007
16. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33:159–74. doi: 10.2307/2529310
17. Nelson SJ, Ash MM. Wheeler’s Dental Anatomy, Physiology and Occlusion. 9th ed Missouri: Elsevier Inc (2010). p. 92–205.
18. AlQahtani SJ, Hector MP, Liversidge HM. Accuracy of dental age estimation charts: schour and massler, ubelaker and the London atlas. Am J Physical Anthropol. (2014) 154:70–8. doi: 10.1002/ajpa.22473
19. McCloe D, Marion I, da Fonseca MA, Colvard M, AlQahtani S. Age estimation of hispanic children using the London atlas. Forensic Sci Int. (2018) 288:332.e1–e6. doi: 10.1016/j.forsciint.2018.04.013
20. Ghafari R, Ghodousi A, Poordavar E. Comparison of the accuracy of the London atlas and smith method in dental age estimation in 5–15.99-year-old iranians using the panoramic view. Int J Legal Med. (2019) 133:189–95. doi: 10.1007/s00414-018-1808-6
21. Baylis S, Bassed R. Precision and accuracy of commonly used dental age estimation charts for the New Zealand population. Forensic Sci Int. (2017) 277:223–8. doi: 10.1016/j.forsciint.2017.06.011
22. Parner ET, Heidmann JM, Veth M, Poulsen S. A longitudinal study of time trends in the eruption of permanent teeth in Danish children. Arch Oral Biol. (2001) 46:425–31. doi: 10.1016/S0003-9969(01)00002-4
23. Leroy R, Bogaerts K, Lesaffre E, Declerck D. The emergence of permanent teeth in flemish children. Community Dent Oral Epidemiol. (2013) 31:30–9. doi: 10.1034/j.1600-0528.2003.00023.x
24. Elmes A, Dykes E, Cookson MJ. A cross-sectional survey to determine the ages of emergence of permanent teeth of Caucasian children of the Colchester area of the UK. Br Dent J. (2010) 209:E10. doi: 10.1038/sj.bdj.2010.672
25. Pavlovic S, Pereira CP, de Sousa Santos RFV. Age estimation in Portuguese population: the application of the London atlas of tooth development and eruption. Forensic Sci Int. (2017) 272:97–103. doi: 10.1016/j.forsciint.2017.01.011
26. Kaul S, Saini S, Saxena B. Emergence of permanent teeth in school-children in Chandigarh, India. Arch Oral Biol. (1975) 20:587–93. doi: 10.1016/0003-9969(75)90079-5
27. Short EM. Domestic water and dental caries: vI. The relation of fluoride domestic waters to permanent tooth eruption. J Dent Res. (1944) 23:247–55. doi: 10.1177/00220345440230040301
28. Friedlaender JS, Bailit HL. Eruption times of the deciduous and permanent teeth of natives on Bougainville Island, Territory of New Guinea: a study of racial variation. Hum Biol. (1969) 41:51–65.5785339
29. Maki K, Morimoto A, Nishioka T, Kimura M, Braham RL. The impact of race on tooth formation. ASDC J Dent Child. (1999) 66:353–6.10631893
30. Liversidge HM. Dental maturation of 18th and 19th century British children using Demirjian’s method. Int J Paediatr Dent. (1999) 9:111–5. doi: 10.1046/j.1365-263x.1999.00113.x
31. Nadler GL. Earlier dental maturation: fact or fiction? Angle Orthod. (1998) 68:535–8. doi: 10.1043/0003-3219(1998)068%3C0535:EDMFOF%3E2.3.CO;2
32. Cardoso HF, Heuzé Y, Júlio P. Secular change in the timing of dental root maturation in Portuguese boys and girls. Am J Human Biol. (2010) 22:791–800. doi: 10.1002/ajhb.21084
33. Jayaraman J, Wong HM, King N, Roberts G. Secular trends in the maturation of permanent teeth in 5 to 6 years old children. Am J Human Biol. (2013) 25:329–34. doi: 10.1002/ajhb.22370
34. Fanning EA. Effect of extraction of deciduous molars on the formation and eruption of their successors. Angle Orthod. (1962) 32:44–53.
35. Lauterstein AM, Pruzansky S, Barber TK. Effect of deciduous mandibular molar pulpotomy on the eruption of succedaneous premolar. J Dent Res. (1962) 41:1367–72. doi: 10.1177/00220345620410061301
36. Gungor H, Pusman E, Uysal S. Eruption delay and sequelae in permanent incisors following intrusive luxation in primary dentition: a case report. Dent Traumatol. (2011) 27:156–8. doi: 10.1111/j.1600-9657.2011.00981.x
37. Aleman Navas RM, Martinez Mendoza MG. Congenital eruption cyst. Pediatr Dermatol. (2010) 27:671–2. doi: 10.1111/j.1525-1470.2010.01335.x
38. Savage NW, Daly CG. Gingival enlargements and localized gingival overgrowths. Aust Dent J. (2010) 55:55–60. doi: 10.1111/j.1834-7819.2010.01199.x
39. Varkhede A, Tupkari JV, Sardar M. (Odontogenic tumors: a study of 120 cases in an Indian teaching hospital. Med Oral Path Oral Cir Bucal. (2011) 16:e895–9. doi: 10.4317/medoral.17251
40. Omer RS, Anthonappa RP, King NM. Determination of the optimum time for surgical removal of unerupted anterior supernumerary teeth. Pediatr Dent. (2010) 32:14–20.20298648
41. Jacometti V, Sato CM, Meireles DA, Silva RHAD. Age estimation using London atlas methodology: a systematic review and meta-analysis. Forensic Sci Int. (2023) 342:111532. doi: 10.1016/j.forsciint.2022.111532
Keywords: dental atlas, Chinese, dental development, dental chart, primary teeth, permanent teeth, human dentition, forensics age estimation
Citation: Jayaraman J (2024) Development and eruption of human teeth in the Chinese population: a comprehensive dental atlas. Front. Dent. Med 5:1434417. doi: 10.3389/fdmed.2024.1434417
Received: 17 May 2024; Accepted: 31 July 2024;
Published: 27 August 2024.
Edited by:
Thantrira Porntaveetus, Chulalongkorn University, ThailandReviewed by:
Shihai Jia, The University of Utah, United StatesInes Morais Caldas, Universidade do Porto, Portugal
Copyright: © 2024 Jayaraman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jayakumar Jayaraman, amF5YWt1bWFyODNAaG90bWFpbC5jb20=
†ORCID:
Jayakumar Jayaraman
orcid.org/0000-0003-1737-6891