 Sara Ortega-Luengo1,†María Nieves Ábalos-Sanfrutos1María Isabel Calama-Fraile1Verónica Carballo-Tejeda1María Trinidad García-Vázquez1
Sara Ortega-Luengo1,†María Nieves Ábalos-Sanfrutos1María Isabel Calama-Fraile1Verónica Carballo-Tejeda1María Trinidad García-Vázquez1 Antonia M. Caleya-Zambrano1,2*†
Antonia M. Caleya-Zambrano1,2*†
- 1Madrid Health Service (SERMAS), Madrid, Spain
- 2Department of Dental Clinical Specialties, Faculty of Dentistry, Complutense University of Madrid, Madrid, Spain
Purpose: The main objective of this study was to evaluate the relationship between Molar Incisor Hypomineralisation (MIH) and socioeconomic factors in a sample of children in the Community of Madrid.
Methods: An observational, descriptive, cross-sectional, and multicentre study was designed. After a previous calibration of all the examiners and following the diagnostic criteria of the European Academy of Paediatric Dentistry (EAPD), children between 8 and 16 years old were included from among the users of the dental services of eight primary care oral health units of the Madrid Health Service. The children underwent a dental examination, and the parents were asked to complete a questionnaire on possible socioeconomic factors related to the appearance of MIH. Factors such as sex, race, parental education, area of residence, exposure to tobacco and diet in the first two years of life were analysed. With MIH (yes/no) as the dependent variable, the χ2 test was used to compare categorical variables between MIH and non-MIH children. A logistic regression model was made with MIH (yes/no) as the dependent variable and the independent variables being those that were clinically relevant or significant in the bivariate analysis. Their associations are expressed as odds ratios (ORs).
Results: Females were significantly more likely to have MIH. The prevalence of MIH decreased with age. Residents in Parla had MIH more often than residents of other municipalities of the Community of Madrid. No other socioeconomic factor studied was associated with MIH.
Conclusions: Residents in the municipality of Parla had a higher frequency of MIH, which was a municipality with a low per capita income. When comparing the presence of MIH in breastfed children, statistically significant differences were observed. Logistic regression, however, did not suggest that breastfeeding could influence the presence of MIH. Further study is warranted on possible socioeconomic risk factors for MIH, such as household income, to lower the incidence of this pathology.
Introduction
Molar Incisor Hypomineralisation (MIH) is an enamel alteration that was described for the first time in Sweden at the end of the 1970s, when paediatric dentists began to detect alterations in the dental enamel of the first molars and permanent incisors of unknown aetiology, not related to tooth decay (1). Although the term MIH was suggested in year 2000 by the European Academy of Paediatric Dentistry (EAPD) and was defined as “hypomineralisation of systemic origin, which affects between one and four permanent molars and is frequently associated with the involvement of the permanent incisors” (2), the problem of these defects in tooth enamel development has been known for over 100 years (3). Later, the term “molar hypomineralisation” was used to refer to cases in which there was no involvement of the incisors and only the first permanent molars were affected (4, 5), and “hypomineralisation primary second molars” referred to hypomineraliation present in the second primary molars (6).
MIH is a highly prevalent disorder. Worldwide, two recent revisions estimate it to be 13.1% and 14.2% (7, 8). In Spain, the prevalence of MIH is estimated to be 21.1% (8). Prevalence estimates in some areas include 21.8% in Valencia (9), 7.94% in Barcelona (10) or 28.63% in Madrid (11).
The aetiology of this enamel alteration is still completely unknown. The enamel becomes hypomineralised when there are alterations during the maturation phase of amelogenesis. Gene-mediated enamel mineralization is a sensitive process that can be altered by environmental factors (12). Although the aetiopathogenic mechanisms for MIH are unknown, it appears to be an acquired disease at some point in dental development rather than a genetic alteration (13). Nevertheless, recent research indicates that a genetic predisposition to MIH may exist in some individuals when certain environmental factors co-exist (14–17).
Possible ethiological factors related to enamel development defects are usually divided into three groups: prenatal, perinatal, and postnatal factors, according to the timing of their action (18). A large number of aetiological causes have been studied, including drug use, childhood illnesses, problems during pregnancy and maternal illnesses, environmental pollutants or contact with toxins (12, 19–32). Recently, several systematic reviews have been conducted with the objective of clarifying the possible causes of this alteration. However, it is not straightforward to obtain conclusive results, due to the fact that there are very few longitudinal studies available (33, 34).
Last years, some authors have proposed that there is a trend towards an increase in the number of cases of MIH (7). In the latest EAPD Clinical Guidelines 2022, epidemiological data show prevalence data between 2.9%–44% (17).In 2007 the prevalence of MIH in Madrid was estimated at 12.4% (35), though in a recently published study, the prevalence of MIH in this community was 28.63% (11). In light of the findings from previous studies, which were conducted in a similar population, and the absence of any other research in Madrid that has analysed the potential aetiological factors affecting individuals diagnosed with MIH, this study was designed to investigate whether socioeconomic and environmental factors might influence the aetiology of MIH.
Material and methods
An observational, descriptive, cross-sectional, multicentre study was designed to determine which socioeconomic factors are related to the occurrence of MIH in boys and girls aged 8–16 years in different Oral Health Units (OHUs) of the Community of Madrid, Spain. This study was approved by the Ethics Committee for Drug Research of Hospital Clínico San Carlos (Internal Code: 21/162-E_Tesis).
Study population and sample selection
The study population was boys and girls between the ages of 8 and 16 who attended the SERMAS oral health program and who met the inclusion criteria of the study: (1) Children who attended the OHUs during the study data collection period. (2) Children who had complete eruption of at least 1/3 of the occlusal surface of the first four permanent molars. (3) Children whose parents or guardians signed the informed consent form. Participation was voluntary. The following were excluded: (1) Children who presented any type of fixed attachment (tubes, bands, brackets, buttons, or attachments) that did not allow direct observation of the first permanent molars. (2) Children who were under who presented any medical, congenital, or acquired pathology related to the appearance of defects in enamel development. (3) Children who did not participate in the clinical inspection.
This publication is part of a research project carried out in the Public Health System of Madrid, where it first estimated the prevalence of MIH in a multicentre study (11). For the calculation of the sample size, EPIDAT 4.2 software was used. We assumed an incidence of MIH of 12%, according to the study by Comes (35) carried out in a population similar to ours. Setting a precision of 3% and a confidence level of 95%, we obtained a sample size of at least 451 children.
Given the interest in studying the possible relationship between some socioeconomic factors and the presence of MIH, we decided to select the OHUs according to the per capita income of the place where they were located. The number and location of all the SERMAS OHUs were determined by dividing them into two groups to facilitate randomization:
• Forty metropolitan OHUs located in Madrid city.
• Forty-six OHUs located in other municipalities of the Community of Madrid. Those located in towns with fewer than 20,000 inhabitants were considered rural OHUs.
The OHUs were ordered according to the per capita income of the place where they were located and were ordered from lowest to highest income, and the quartiles were calculated to select the OHUs that were in the first quartile and the fourth quartile. Those in the first quartile were classified as low income, and those in the fourth quartile were classified as high income.
We conducted two-stage sampling. In the first phase, by means of stratified random sampling, eight OHUs were selected—four from the metropolitan area and four from the rest of the municipalities—and in each of these groups, two from high-income areas and the other two from low-income areas. In the second phase, by means of consecutive sampling, 60 children were selected from each of the selected centres.
Examiners: training and calibration
In each of the selected centres, a researcher was in charge of collecting dental data from each of the children who made up the sample. Before starting the data collection, the eight participating researchers participated in a training session on the EAPD diagnostic criteria for MIH. To ensure that all of them were calibrated, a questionnaire was designed with 29 photographs of teeth with different degrees of MIH. Each researcher answered the questionnaire twice. Once all the investigators had submitted their answers, Cohen's kappa was calculated for each of the dentists, and their answers were compared with the correct responses. The values obtained were between 0.74 and 0.94. This was an adequate degree of agreement, so the data collection phase started.
Data collection
The data collection process consisted of two phases, an oral examination and a questionnaire with questions related to socioeconomic factors and habits of the children during their first two years of life that were completed by the parents. This questionnaire has not been validated but was developed by the researchers based on the available scientific evidence on socio-economic factors related to MIH (7, 12, 19, 23–32, 36) (Figure 1).
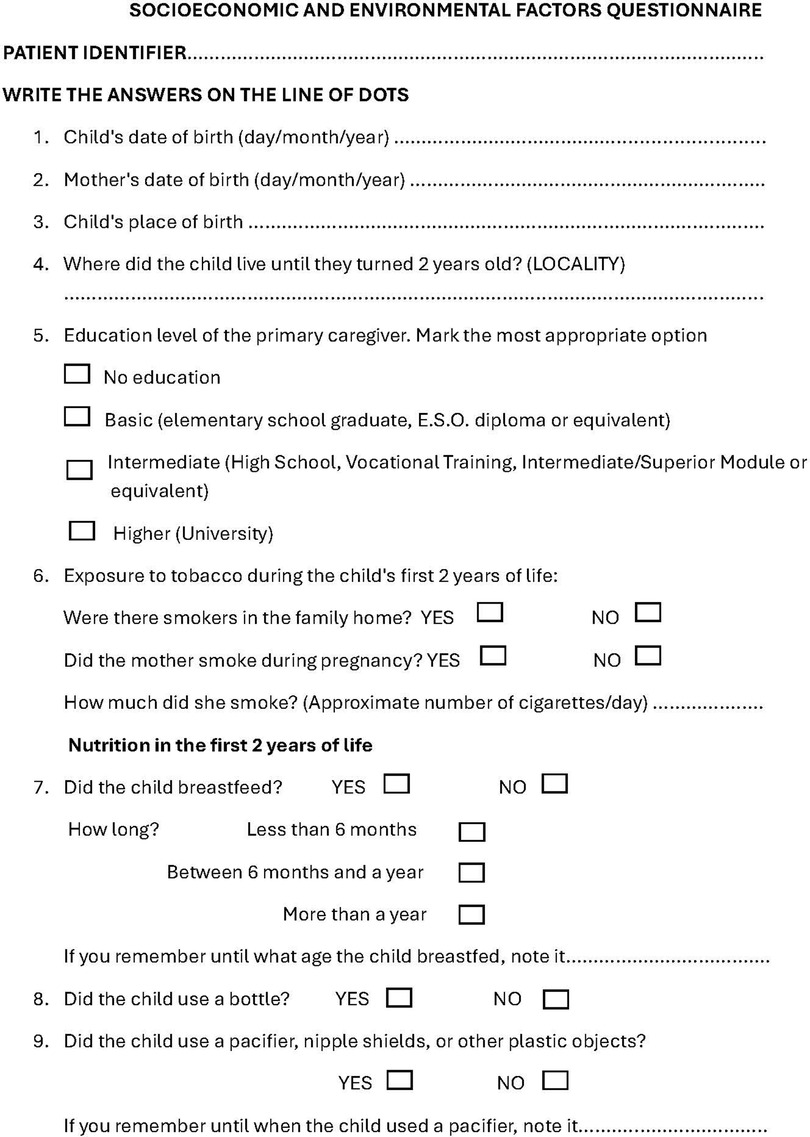
Figure 1. Questionnaire on socio-economic, environmental and nutritional factors during the first two years of life.
The oral examination was performed in the dental chairs of the OHU, from July 2022 to September 2023. Light from the dental equipment and examination mirror was used. Ball-ended probes were used to explore irregularities. If it was necessary to dry the mouth, gauze or cotton rolls were used. The diagnosis of MIH was made following the EAPD criteria (37).
Statistical analysis
SPSS version 27 software was used to carry out the statistical analysis. The quantitative variables are described as mean ± standard deviation. Categorical variables are described as n (%). With MIH (yes/no) as the dependent variable, the χ2 test was used to compare categorical variables between MIH and non-MIH children. A logistic regression model was made with MIH (yes/no) as the dependent variable and the independent variables being those that were clinically relevant or significant in the bivariate analysis. Their associations are expressed as odds ratios (ORs). Differences were considered statistically significant if p < 0.05.
Results
The sample comprised 489 boys and girls between 8 and 16 years old. A total of 258 (52.76%) were girls and 231 were boys (47.23%). A total of 140 children were affected by MIH. Of those affected, 55 were boys (39.28%), and 85 were girls (60.71%).
Most of the participants (76.7%) were Caucasian, 44.6% of their parents had a higher education level or university equivalency, and 87.85% had resided in urban areas in their first years of life. The different socioeconomic characteristics of the children who participated in the study are shown in Table 1.
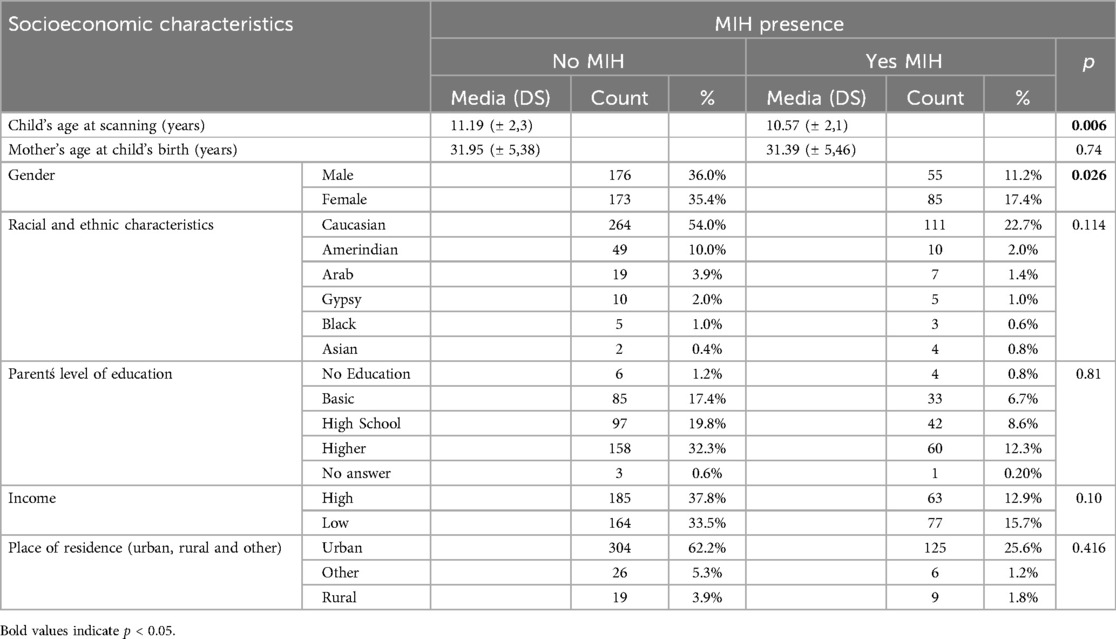
Table 1. Socioeconomic characteristics of the children in the sample.
The presence of MIH was analysed according to the location and income level of the health centre. When the presence of MIH was analysed in high- and low-income health centres, the χ2 test did not show statistically significant differences. The oral health units were in the municipalities of Madrid, Alcobendas, Parla and Algete.
When the presence of MIH according to the municipality in which the OHU was located was studied (Figure 2), residing in the OHU of Parla, one of the low-income municipalities, was associated with having MIH (χ2 test, p = 0.003). No significant differences were found between other OHU locations in the rate of MIH.
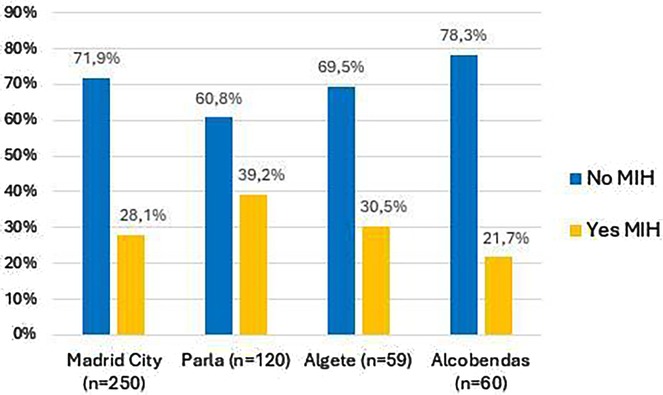
Figure 2. Bar chart comparing “No MIH” and “Yes MIH” percentages across four locations: Madrid City, Parla, Algete, and Alcobendas.
We next analysed some environmental factors and eating habits that the participants in this study had during their first 2 years of life and their possible relationship with the appearance of MIH were analysed (Table 2). Breastfeeding was associated with a higher prevalence of MIH (χ2 test, p = 0.003). However, the duration of breastfeeding (less than 6 months, 6–12 months, or more than 12 months) was not associated with the presence of MIH. The other factors studied had no effect on the presence or absence of MIH.
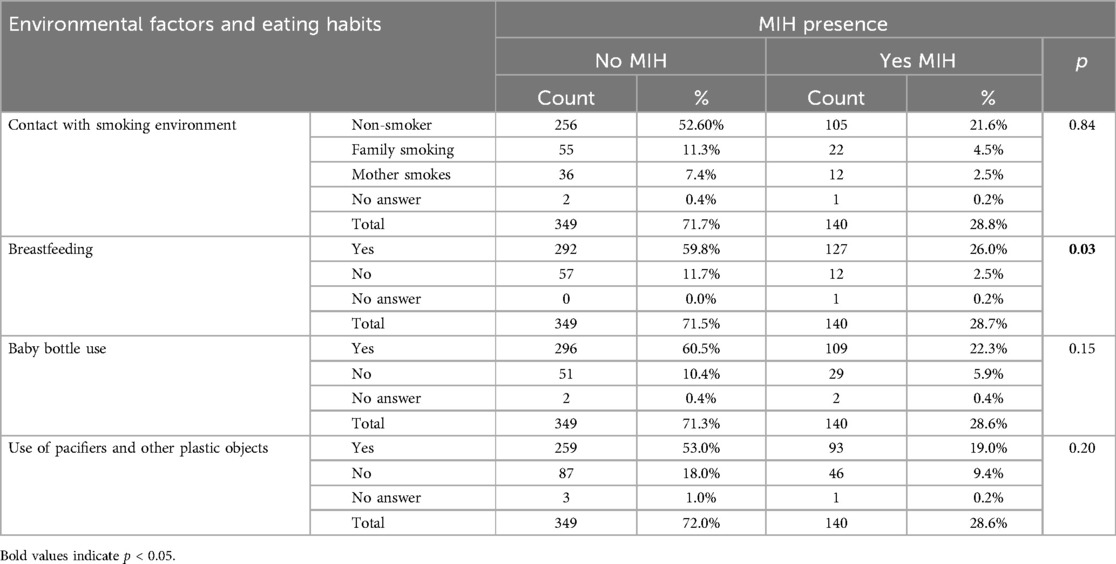
Table 2. Environmental factors and eating habits during early childhood.
To understand how each variable influenced the presence of MIH, logistic regression was carried out, in which the following variables were included: sex, age of the children at the time of the examination, age of the mothers at the birth of the children, location of the OHU, racial and ethnic characteristics, educational level of the main caregiver, residential area during the first 2 years of life, income in the area of location of the OHU, having had contact with smoking environments during the first 2 years of life, having breastfed, having used a bottle, and having had contact with other elements with plastic content. The results are shown in Table 3. Girls were significantly more likely than boys to have MIH (OR 1.546, CI 1.009–2.369) (p = 0.045); that is, the girls in this study had 1.54 times the likelihood of experiencing MIH than did the children. Older age at the time of the study made MIH less likely (OR 0.89, CI 0.814–0.942) (p = 0.019). In the rest of the variables studied, no significant results were found, so they do not seem to influence the presence of the disease.
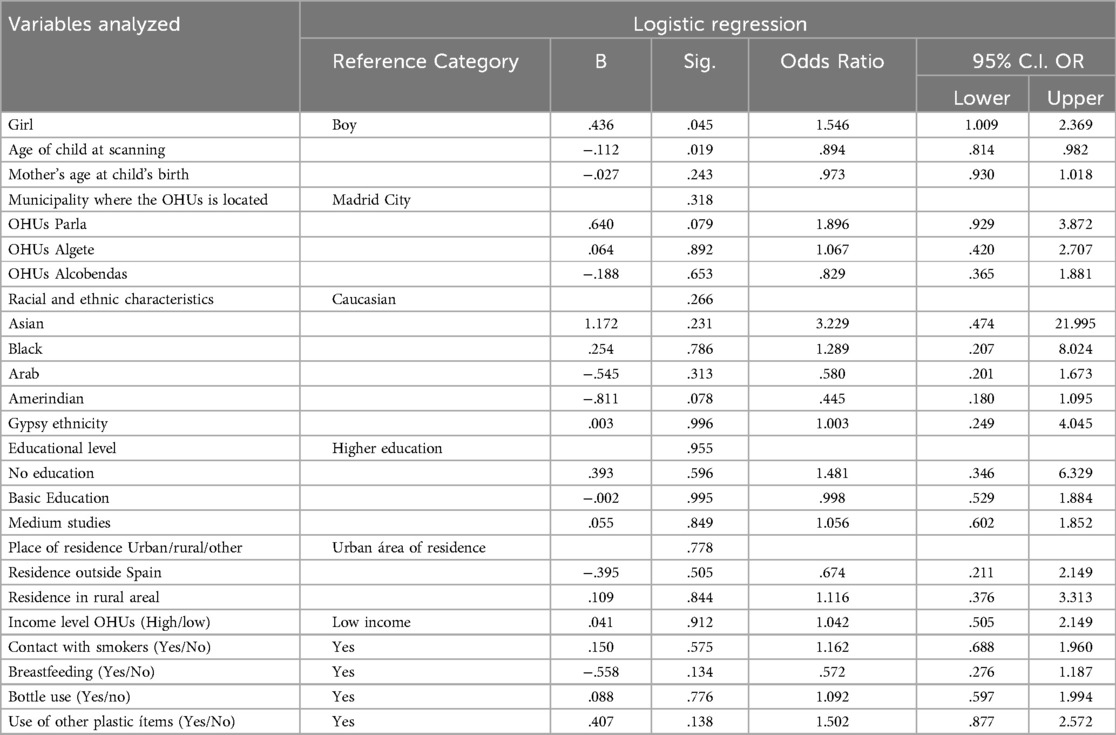
Table 3. Logistic regression model (dependent variable presents MIH Yes/No).
Discussion
This study is part of a research project on MIH carried out in the Madrid public health system. In the first part, the prevalence and clinical characteristics of affected teeth were studied. Subsequently, we studied the presence of MIH and its association with environmental factors in patients who used public dental care, which Madrid provided through the Madrid Health Service (SERMAS). Few investigations have been carried out in the field of public health on MIH (38–40), and of these, only the one carried out by Haque Afzal has studied environmental factors (40). We analysed whether the age of the mother at the time the child was born could have any influence on the presence of MIH. On this topic, Balmer (19) suggested that this could influence the presence of MIH since pregnancies in older women tend to have more complications and show a greater association with the presence of MIH. In our study, no significant differences were found when studying this factor, in line with Ghanim (41). Although some authors have found differences between the presence of MIH and the ethnic origin of children (18, 28, 41, 42), we did not, in line with at least two other studies (16, 27, 35).
Other socioeconomic factors suggested in relation to MIH are the parents' level of education, family income level, or area of residence (23, 25–30). In the case of parental education, although Yi (28) related a higher maternal education with a lower incidence of MIH and Villanueva-Gutiérrez (30) associated a greater severity of MIH injuries with a lower educational level, since a low educational level is related to lower brushing frequencies, we did not find a link between the presence of MIH and the educational level of the parents. Moreover, we did not find differences between the presence of MIH and household income, unlike some studies that concluded that they do exist, such as that of Schwendicke (7). We believe that the differences observed between the presence of MIH and economic or educational level may be due to the association between income and cultural, since individuals with higher income and higher cultural level can more easily access dental care, so that preventive treatments could be carried out and try to maintain the integrity of the affected teeth, while in families with a lower income and lower cultural level, the difficulty in accessing dental treatments would favour the deterioration of the affected teeth before the disease is diagnosed. The fact that all the children in our study had access to oral care as a result of the existence of the Children's Dental Care Program (43), regardless of the income or cultural level of the parents, could explain why we did not find an influence of these variables. This feature of our research, which leads us to believe that families with a higher level of education could be underrepresented due to the easy access to private care and that the OHUs in high-income areas would go to people with fewer resources in the area. Dental examinations were carried out in the municipalities of Madrid Capital Area, Algete, Alcobendas and Parla.
When analysing the results of our sample, we observed that in the OHUs of the Madrid Capital area, there was a high prevalence of parents with university degrees, especially in high-income neighbourhoods. The above phenomenon was detected in Alcobendas, a municipality in northern Madrid. Although it is a municipality with a very high per capita (44) the majority of parents who attended the service recognized a basic level of education. In Parla, a municipality of more than 50,000 inhabitants in southern Madrid with the lowest income per capita, the most frequent parental educational level was medium, and in Algete, a municipality in northern Madrid with high income, the most frequent level of education was university. For this reason, although we studied users of a public health service, we believe the representation at the socioeconomic level was not skewed.
When analysing the presence of MIH in the children of the sample according to the municipality where the OHUs was located, we found statistically significant differences between the children of the municipality of Parla and those of the other municipalities. The children of Parla presented MIH at a rate of 39.2%, almost double that of the children of Alcobendas, who were the ones who presented the lowest rate of MIH in this study (21.7%). The municipality of Parla is one of the municipalities with the lowest income per capita in the Community of Madrid, while Alcobendas has one of the highest incomes. By also relating the level of education of the parents of the children in these municipalities, we observed that, in Parla, many of parents had higher education, while in Alcobendas, they reported basic-level studies. We believe that the differences found in the children of Parla may be due to this disparity in educational level, since parents with a higher education level may demand more health care and therefore bring their children to a higher proportion of dental check-ups at the OHU than those with a lower education level. It would be desirable for health officials to encourage oral health programs for families with fewer resources since they may be unaware of their existence. On the other hand, the sample of the municipality of Alcobendas may be underrepresented, and parents with higher educational levels with children affected by MIH do not use public health and go directly to private dentists, so these children will not have been counted. This would mean we found a lower rate of MIH in Alcobendas not because it is rarer there but because they do not attend public consultations and were not included in the study.
Drugs, early childhood diseases, and environmental pollutants have been identified as possible causes of MIH due to their influence on the mineralization of dental enamel (12, 21–24). Some authors suggest that living in urban areas may favour the diagnosis of MIH because of the ease of access to dental consultations and medical treatment (22, 23), although other researchers have found a higher prevalence of MIH in rural areas (24). In our study, we did not find a significant effect of the urban or rural environment, though the sample of children who lived in rural areas in the first 2 years of life was small. Geographical distribution of the population in Madrid shows a concentration in urban areas, with a smaller proportion of inhabitants in rural zones. This can affect the ability to recruit a representative sample of rural patients, as most participants come from urban areas. It is recommended that future studies consider strategies to increase the representation of rural patients, such as collaborating with health centres in small towns or implementing more inclusive sampling methods.
In addition, we studied the associations between MIH and exposure to tobacco, plastic elements, and breastfeeding (due to the possible presence of toxins in breast milk) in the children in our sample since these factors are related to the aetiological mechanism of MIH (12, 31–33). Our findings agree with others (23, 38, 45, 46) in that there was no significant effect of any of those variables. Non-halogenated polycyclic aromatic hydrocarbons (PAHs) present in tobacco have been described as a possible etiological mechanism of MIH (31). Garot (33), in a systematic review, found no differences in the presence of MIH in children who had been exposed to smokers during their early years of life. Ilczuk-Rypula (45) in Poland and Wuollet (23) in Finland also found no differences in their studies. Lim, in a study conducted in the United Kingdom (46), was unable to find firm evidence of an association between MIH and maternal smoking habits. Our sample was not influenced by contact with smokers, whether the smoker was the mother or a partner or the number of cigarettes smoked, unlike Lee (47), who reported an OR of 2.37 for MIH in children whose mothers smoked during pregnancy. The presence of dioxins in breast milk has been suggested to be a factor associated with the appearance of MIH (31, 48). The existing studies on this topic are controversial. While the studies by Koruyucu (49) and Ghanim (41) revealed significant differences in the presence of MIH as a function of breastfeeding time, other researchers have not found this (7, 50–52).
In our study, statistically significant differences were found in the presence of MIH between children who breastfed and those who did not (χ2 test, p = 0.026), but the logistic regression analysis, which included breastfeeding and other confounding factors, did not reveal statistically significant differences between being breastfed or not and the presence of MIH. We also did not find a relationship between the duration of breastfeeding and the presence of MIH.
Jedeon (32) suggested in different publications that endocrine disruptors, such as bisphenol A (BPA), can interfere with enamel mineralization, favouring the appearance of MIH (32, 33). BPA is present in food containers and other utensils for babies and young children (53, 54). Several investigations have studied the relationship between the use of bottles and the presence of MIH (9, 55), without finding statistically significant effects.
Elzein (55), in Lebanon, studied the relationship between MIH and its possible association with various pre- and post-natal factors and found no difference in the presence of MIH in children who breastfed for more than 6 months compared to those who did not. However, he did detect differences in children breastfed by mothers who consumed canned foods, linking it to the possible transfer of bisphenol A from the canned foods through breast milk. In our study, we did not find an effect of feeding from a bottle or other plastic devices on the presence of MIH.
Our study has some limitations, such as memory bias. We also considered sample representativeness as a potential limitation, that could influence the external validity of our results. In this study, all participants were users of the public health system. Predominantly, dentistry in the Community of Madrid has been provided privately, so the studied population may not be entirely representative. Often, public health patients are those with fewer economic resources and/or more health issues. To counteract this, medical centres from areas with both high and low income levels were selected. We cannot rule out the possibility of confounding bias when analysing the influence of socioeconomic variables on the presence of MIH. Another possible limitation is that we used a global income indicator of the municipality or the neighbourhood instead of asking about the individual household income because we have found, in our previous experiences, that these questions tend to cause rejection and are not answered truthfully. Perhaps the ideal would have been to ask each family unit about their income level individually. On the other hand, the fact that patients were users of the public health system can also be seen as a strength of this research, as the ethnic and racial variability, as well as the socioeconomic status of the participants, is likely to have been greater than if the sample had been obtained from private clinics. Another limitation of the present study is the lack of validation of the questionnaire passed on to the parents of the patients, although it is based on the available scientific evidence and the literature found. We consider it interesting to carry out future studies to validate these questionnaires.
Conclusions
Among the users of public dentistry services in Madrid, girls were more likely than boys to have MIH. The prevalence of MIH decreased with increasing age of the children in the study. Statistically significant differences were observed when comparing the presence or absence of MIH in children living in Parla and children who had been breastfed. Given the results found in this municipality, we believe that in future research, it would be beneficial to factor in the individual (household) income level of the participants.
When comparing the presence of MIH in breastfed children, statistically significant differences were observed. Logistic regression, however, did not suggest that breastfeeding could influence the presence of MIH. No other socioeconomic factor studied was associated with MIH.
We believe it is very important to continue studying possible etiological factors in order to prevent this dental alteration that affects the quality of life of pediatric patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Hospital Clínico San Carlos. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SO-L: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MÁ-S: Investigation, Writing – original draft, Writing – review & editing. MC-F: Investigation,Writing – original draft, Writing – review & editing. VC-T: Investigation, Writing – original draft, Writing – review & editing. MG-V: Investigation, Writing – original draft, Writing – review & editing. AC-Z: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. “This project received a grant for the publication of this paper from the Foundation for Biosanitary Research and Innovation in Primary Care (FIIBAP)”.
Acknowledgments
We are grateful for the patients and their legal guardians for their participation in this study and their contribution to science. As well as Madrid Health Service for promoting research and always giving us their unconditional support. To the dentist and dental hygienists who participated in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
EAPD, European academy of paediatric; MIH, molar incisor hypomineralisation; OHUs, oral health units.
References
1. Weerheijm KL, Jalevik B, Alaluusua S. Molar-incisor hypomineralisation. Caries Res. (2001) 35:390–1. doi: 10.1159/000047479
2. Weerheijm KL. Molar incisor hypomineralisation (MIH). Eur J Paediatr Dent. (2003) 4(3):114–20.14529330
3. Hubbard MJ, Perez VA, Ganss B. 100 years of chalky teeth research: from pioneering histopathology to social good. Front Dent Med. (2021) 1:632534. doi: 10.3389/fdmed.2020.632534)
4. Chawla N, Messer LB, Silva M. Clinical studies on molar-incisor-hypomineralisation part 1: distribution and putative associations. Eur Arch Paediatr Dent. (2008) 9(4):180–90. doi: 10.1007/BF03262634
5. Mangum JE, Crombie FA, Kilpatrick N, Manton DJ, Hubbard MJ. Surface integrity governs the proteome of hypomineralized enamel. J Dent Res. (2010) 89(10):1160–5. doi: 10.1177/0022034510375824
6. Elfrink MEC, Schuller AA, Weerheijm KL, Veerkamp JSJ. Hypomineralized second primary molars: prevalence data in Dutch 5-year-olds. Caries Res. (2008) 42(4):282–5. doi: 10.1159/000135674
7. Schwendicke F, Elhennawy K, Reda S, Bekes K, Manton DJ, Krois J. Global burden of molar incisor hypomineralization. J Dent. (2018) 68:10–8. doi: 10.1016/j.jdent.2017.12.002
8. Zhao D, Dong B, Yu D, Ren Q, Sun Y. The prevalence of molar incisor hypomineralization: evidence from 70 studies. Int J Paediatr Dent. (2018) 28(2):170–9. doi: 10.1111/ipd.12323
9. Garcia-Margarit M, Catalá-Pizarro M, Montiel-Company JM, Almerich-Silla JM. Epidemiologic study of molar-incisor hypomineralization in 8-year-old Spanish children. Int J Paediatr Dent. (2014) 24(1):14–22. doi: 10.1111/ipd.12020
10. Hernández M, Boj JR, Espasa E, Peretz B. First permanent molars and permanent incisors teeth by tooth prevalence of molar–incisor–hypomineralisation in a group of Spanish schoolchildren. Acta Stomatol Croat. (2018) 52(1):4–11. doi: 10.15644/asc52/1/1
11. Ortega-Luengo S, Feijóo-Garcia G, Miegimolle-Herrero M, Gallardo-López NE, Caleya-Zambrano AM. Prevalence and clinical presentation of molar incisor hypomineralisation among a population of children in the community of Madrid. BMC Oral Health. (2024) 24(1):229. doi: 10.1186/s12903-024-04003-4
12. Alaluusua S. Aetiology of molar-incisor hypomineralisation: a systematic review. Eur Arch Paediatr Dent. (2010) 11(2):53–8. doi: 10.1007/BF03262713
13. Williams R, Perez VA, Mangum JE, Hubbard MJ. Pathogenesis of molar hypomineralisation: hypomineralised 6-year molars contain traces of fetal serum albumin. Front Physiol. (2020) 11:619. doi: 10.3389/fphys.2020.00619
14. Jeremias F, Koruyucu M, Küchler EC, Bayram M, Tuna EB, Deeley K, et al. Genes expressed in dental enamel development are associated with molar-incisor hypomineralization. Arch Oral Biol. (2013) 58(10):1434–42. doi: 10.1016/j.archoralbio.2013.05.005
15. Jeremias F, Pierri RAG, Souza JF, Fragelli CMB, Restrepo M, Finoti LS, et al. Family-based genetic association for molar-incisor hypomineralization. Caries Res. (2016) 50(3):310–8. doi: 10.1159/000445726
16. Hočevar L, Kovač J, Podkrajšek KT, Battelino S, Pavlič A. The possible influence of genetic aetiological factors on molar-incisor hypomineralisation. Arch Oral Biol. (2020) 118:104848. doi: 10.1016/j.archoralbio.2020.104848
17. Lygidakis NA, Garot E, Somani C, Taylor G, Rouas P, Wong FSL. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): an updated European academy of paediatric dentistry policy document. Eur Arch Paediatr Dent. (2022) 23:3–21. doi: 10.1007/s40368-021-00668-5
18. Alvarado-Gaytán J, Saavedra-Marbán G, Velayos-Galán L, Gallardo-López NE, de Nova-García MJ, Caleya AM. Dental developmental defects: a pilot study to examine the prevalence and etiology in a population of children between 2 and 15 years of age. Dent J. (2004) 12(4):84. doi: 10.3390/dj12040084
19. Balmer R, Toumba J, Godson J, Duggal M. The prevalence of molar incisor hypomineralisation in Northern England and its relationship to socioeconomic status and water fluoridation. Int J Paediatr Dent. (2012) 22(4):250–7. doi: 10.1111/j.1365-263X.2011.01189.x
20. Ghanim A, Silva MJ, Elfrink MEC, Lygidakis NA, Mariño RJ, Weerheijm KL, et al. Molar incisor hypomineralisation (MIH) training manual for clinical field surveys and practice. Eur Arch Paediatr Dent. (2017) 18(4):225–42. doi: 10.1007/s40368-017-0293-9
21. Amend S, Nossol C, Bausback-Schomakers S, Wleklinski C, Scheibelhut C, Pons-Kühnemann J, et al. Prevalence of molar-incisor-hypomineralisation (MIH) among 6–12-year-old children in central Hesse (Germany). Clin Oral Invest. (2021) 25:2093–100. doi: 10.1007/s00784-020-03519-7
22. Quispe DM, de Priego GP, Manco RA, Portaro CP. Molar incisor hypomineralization: prevalence and severity in schoolchildren of Puno, Peru. J Indian Soc Pedod Prev Dent. (2021) 39(3):246–50. doi: 10.4103/jisppd.jisppd_460_20
23. Wuollet E, Laisi S, Salmela E, Ess A, Alaluusua S. Background factors of molar-incisor hypomineralization in a group of Finnish children. Acta Odontol Scand. (2014) 72(8):963–9. doi: 10.3109/00016357.2014.931459
24. Souza JF, Costa-Silva CM, Jeremias F, Santos-Pinto L, Zuanon ACC, Cordeiro RCL. Molar incisor hypomineralisation: possible aetiological factors in children from urban and rural areas. Eur Arch Paediatr Dent. (2012) 13(4):164–70. doi: 10.1007/BF03262865
25. Reis PP, Jorge RC, Americano GC, Thiago Pontes ND, Peres AM, Soviero VM. Prevalence and severity of molar incisor hypomineralization in Brazilian children. Pediatr Dent. (2021) 43(4):270–5.34467841
26. Tourino LFPG, Correa-Faria P, Ferreira RC, Bendo CB, Zarzar PM, Vale MP. Association between molar incisor hypomineralization in schoolchildren and both prenatal and postnatal factors: a population-based study. PLoS One. (2016) 11(6):e0156332. doi: 10.1371/journal.pone.0156332
27. Davenport M, Welles AD, Angelopoulou MV, Gonzalez C, Okunseri C, Barbeau L, et al. Prevalence of molar-incisor hypomineralization in Milwaukee, Wisconsin, USA: a pilot study. Clin Cosmet Investig Dent. (2019) 11:109–17. doi: 10.2147/CCIDE.S172736
28. Yi X, Chen W, Liu M, Zhang H, Hou W, Wang Y. Prevalence of MIH in children aged 12 to 15 years in Beijing, China. Clin Oral Investig. (2020) 25(1):355–61. doi: 10.1007/s00784-020-03546-4
29. Wuollet E, Laisi S, Alaluusua S, Waltimo-Sirén J. The association between molar-incisor hypomineralization and dental caries with socioeconomic status as an explanatory variable in a group of finnish children. Int J Environ Res Public Health. (2018) 15(7):1324. doi: 10.3390/ijerph15071324
30. Villanueva-Gutiérrez T, Irigoyen-Camacho M, Castaño-Seiquier A, Zepeda-Zepeda M, Sanchez-Pérez L, Frechero N. Prevalence and severity of molar–incisor hypomineralization, maternal education, and dental caries: a cross-sectional study of Mexican schoolchildren with low socioeconomic status. J Int Soc Prevent Communit Den. (2019) 9:513–21. doi: 10.4103/jispcd.JISPCD_130_19
31. Alaluusua S, Lukinmaa PL. Developmental dental toxicity of dioxin and related compounds–a review. Int Dent J. (2006) 56(6):323–31. doi: 10.1111/j.1875-595X.2006.tb00336.x
32. Jedeon K, Marciano C, Loiodice S, Boudalia S, Canivenc Lavier MC, Berdal A, et al. Enamel hypomineralization due to endocrine disruptors. Connect Tissue Res. (2014) 55(sup1):43–7. doi: 10.3109/03008207.2014.923857
33. Garot E, Rouas P, Somani C, Taylor GD, Wong F, Lygidakis NA. An update of the aetiological factors involved in molar incisor hypomineralisation (MIH): a systematic review and meta-analysis. Eur Arch Paediatr Dent. (2022) 23(1):23–38. doi: 10.1007/s40368-021-00646-x
34. Fatturi AL, Wambier LM, Chibinski AC, Assunção LR, Brancher JA, Reis A, et al. A systematic review and meta-analysis of systemic exposure associated with molar incisor hypomineralization. Community Dent Oral Epidemiol. (2019) 47(5):407–15. doi: 10.1111/cdoe.12467
35. Comes Martínez Á, Puente Ruiz CD, Rodríguez Salvanés F. Prevalencia de hipomineralización en primeros molares permanentes (MIH) en población infantil del Área 2 de Madrid. RCoE. (2007) 12(3):129–34.
36. Weerheijm KL. Molar incisor hypomineralization (MIH): clinical presentation, aetiology and management. Dent Update. (2004) 31(1):9–12. doi: 10.12968/denu.2004.31.1.9
37. Weerheijm KL, Duggal M, Mejàre I, Papagiannoulis L, Koch G, Martens LC, et al. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: a summary of the European meeting on MIH held in Athens, 2003. Eur J Paediatr Dent. (2003) 4(3):110–3.14529329
38. Rodríguez-Rodríguez M, Carrasco-Colmenares W, Ghanim A, Natera A, Acosta-Camargo MG. Prevalence and distribution of molar incisor hypomineralization in children receiving dental care in caracas metropolitan area, Venezuela. Acta Odontol Latinoam. (2021) 34(2):104–1112. doi: 10.54589/aol.34/2/104
39. López Jordi MD, Cortese SG, Alvarez L, Salveraglio I, Ortolani AM, Biondi AM. Comparison of the prevalence of molar incisor hypomineralization among children with different health care coverage in the cities of Buenos Aires (Argentina) and Montevideo (Uruguay). Salud Colect. (2014) 10(2):243–51. doi: 10.18294/sc.2014.225
40. Haque Afzal S, Wigen TI, Skaare AB, Brusevold IJ. Molar–incisor hypomineralisation in Norwegian children: prevalence and associated factors. Eur J Oral Sci. (2023) 131(3):1–9. doi: 10.1111/eos.12930
41. Ghanim A, Manton D, Bailey D, Mariño R, Morgan M. Risk factors in the occurrence of molar-incisor hypomineralization amongst a group of Iraqi children. Int J Paediatr Dent. (2013) 23(3):197–206. doi: 10.1111/j.1365-263X.2012.01244.x
42. Lopes LB, Machado V, Mascarenhas P, Mendes JJ, Botelho J. The prevalence of molar-incisor hypomineralization: a systematic review and meta-analysis. Sci Rep. (2021) 11(1):22405. doi: 10.1038/s41598-021-01541-7
43. Madrid Cd. Ley 7/2018, de 26 de diciembre, de atención a la salud bucodental y de creación del programa de atencion dental infantil. BOCM. (2018):31190–202.
44. Instituto Nacional de Estadística. Atlas de Distribución de Renta de los Hogares (ADRH)—iNE. Madrid: Ayuntamiento de Madrid (2017).
45. Ilczuk-Rypuła D, Zalewska M, Pietraszewska D, Dybek A, Nitecka-Buchta A, Postek-Stefańska L. Prevalence and possible etiological factors of molar-incisor hypomineralization (MIH) in population of silesian children in Poland: a pilot retrospective cohort study. Int J Environ Res Public Health. (2022) 19(14):8697. doi: 10.3390/ijerph19148697
46. Lim QY, Taylor K, Dudding T. The effects of modifiable maternal pregnancy exposures on offspring molar-incisor hypomineralisation: a negative control study. Community Dent Health. (2022) 39(4):231–9. doi: 10.1922/CDH_00067Lim09
47. Lee DW, Kim YJ, Oh Kim S, Choi SC, Kim J, Lee JH, et al. Factors associated with molar-incisor hypomineralization: a population-based case-control study. Pediatr Dent. (2020) 42(2):134–40.32276681
48. Alaluusua S, Lukinmaa PL, Vartiainen T, Partanen M, Torppa J, Tuomisto J. Polychlorinated dibenzo-p-dioxins and dibenzofurans via mother’s milk may cause developmental defects in the child’s teeth. Environ Toxicol Pharmacol. (1996) 1(3):193–7. doi: 10.1016/1382-6689(96)00007-5
49. Koruyucu M, Özel S, Tuna EB. Prevalence and etiology of molar-incisor hypomineralization (MIH) in the city of Istanbul. J Dent Sci. (2018) 13(4):318–28. doi: 10.1016/j.jds.2018.05.002
50. Laisi S, Kiviranta H, Lukinmaa PL, Vartiainen T, Alaluusua S. Molar-incisor-hypomineralisation and dioxins: new findings. Eur Arch Paediatr Dent. (2008) 9(4):224–7. doi: 10.1007/BF03262639
51. Khazaei Y, Harris CP, Heinrich J, Standl M, Kühnisch J. Association study on nutrition in the first year of life and molar-incisor hypomineralization (MIH)-results from the GINIplus and LISA birth cohort studies. Int J Environ Res Public Health. (2021) 18(21):11411. doi: 10.3390/ijerph182111411
52. Mejía J, Restrepo M, González S, Álvarez L, Santos-Pinto L, Escobar A. Molar incisor hypomineralization in Colombia: prevalence, severity and associated risk factors. J Clin Pediatr Dent. (2019) 43(3):185–9. doi: 10.17796/1053-4625-43.3.7
53. Quitmeyer A, Roberts R. Babies, bottles, and bisphenol A: the story of a scientist-mother. PLoS Biol. (2007) 5(7):e200. doi: 10.1371/journal.pbio.0050200
54. Groff T. Bisphenol A: invisible pollution. Curr Opin Pediatr. (2010) 22(4):524–9. doi: 10.1097/MOP.0b013e32833b03f8
55. Elzein R, Chouery E, Abdel-Sater F, Bacho R, Ayoub F. Molar–incisor hypomineralisation in Lebanon: association with prenatal, natal and postnatal factors. Eur Arch Paediatr Dent. (2021) 22(2):283–90. doi: 10.1007/s40368-020-00555-5
56. Lanford MW, Yu Q, Ballard RW, Johnson JT, Armbruster PC. Prevalence of molar-incisor hypomineralization within an orthodontic department in the United States. Pediatr Dent. (2021) 43(5):51E–7E.34654503
57. Fatturi AL, Menoncin BL, Reyes MT, Meger M, Scariot R, Brancher JA, et al. The relationship between molar incisor hypomineralization, dental caries, socioeconomic factors, and polymorphisms in the vitamin D receptor gene: a population-based study. Clin Oral Investig. (2020) 24(11):3971–80. doi: 10.1007/s00784-020-03263-y
Keywords: molar incisor hypomineralization, enamel, pediatric dentistry, molar incisor, dental defects, dental enamel hypoplasia
Citation: Ortega-Luengo S, Ábalos-Sanfrutos MN, Calama-Fraile MI, Carballo-Tejeda V, García-Vázquez MT and Caleya-Zambrano AM (2025) Socioeconomic factors and feeding in the first two years of life associated with molar incisor hypomineralisation. Front. Dent. Med. 6:1573208. doi: 10.3389/fdmed.2025.1573208
Received: 8 February 2025; Accepted: 3 June 2025;
Published: 18 June 2025.
Edited by:
Sherry Shiqian Gao, Xiamen University, ChinaReviewed by:
Florence Carrouel, Université Claude Bernard Lyon 1, FranceRamiro J. Castro, Universidad de Talca, Chile
Copyright: © 2025 Ortega-Luengo, Ábalos-Sanfrutos, Calama-Fraile, Carballo-Tejeda, García-Vázquez and Caleya-Zambrano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonia M. Caleya-Zambrano, YW1jYWxleWEgQHVjbS5lcw==
†These authors have contributed equally to this work and share first authorship