 Hong Yang1,†
Hong Yang1,† Hong-Chao Feng
Hong-Chao Feng- 1Department of Prosthodontics, Guiyang Hospital of Stomatology, Guiyang, China
- 2ZBH-Center for Bioinformatics, Universität Hamburg, Hamburg, Germany
- 3Department of Oral and Maxillofacial Surgery, Division of Regenerative Orofacial Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Background/aim: Early childhood caries (ECC) is one of the most prevalent global oral health issues in children under five years old, significantly impacting their overall health and quality of life. This study aimed to analyze the global, regional, and national burden of ECC from 1990 to 2021, identify associated risk factors, and predict trends through 2040. It further examined the influence of socio-demographic factors, sex, and age on ECC incidence and prevalence.
Patients and methods: Data from the Global Burden of Disease (GBD) 2021 database were analyzed using Bayesian Meta-Regression models to estimate ECC incidence, prevalence, and years lived with disability (YLDs) across 204 countries and regions. Socio-Demographic Index (SDI) levels, sex, and age-specific trends were assessed. Age-standardized rates and estimated annual percentage changes (EAPCs) were calculated. Predictive models, including ARIMA, were developed to forecast future trends.
Results: Between 1990 and 2021, ECC incidence and prevalence showed modest declines globally, with significant variations across SDI regions. High SDI regions exhibited the lowest burden due to effective public health measures, while medium and low SDI regions faced persistent challenges. Sex disparities were observed, with males showing slightly higher rates than females. Children aged 5–9 years bore the highest burden of ECC. Predictions for 2040 indicate a potential rebound in ECC incidence in low and medium SDI regions without targeted interventions.
Conclusion: This study highlights the substantial burden of ECC, particularly in under-resourced regions, and underscores the need for tailored public health strategies. Effective prevention, improved healthcare access, and education are critical to reducing ECC burden globally, ensuring better oral health outcomes for children, and addressing disparities across socio-economic, sex, and age groups.
Introduction
Early childhood caries (ECC), or early childhood tooth decay, is one of the most prevalent oral diseases in children under the age of five worldwide. ECC has complex etiologies linked to multiple factors, including oral hygiene practices, dietary habits, socioeconomic status, and parental health awareness (1). Typical characteristics of ECC include enamel and dentin demineralization and softening, which can lead to tooth breakage and even loss, impacting chewing function, language development, nutrient absorption, and children's quality of life (2). If left untreated, ECC can progress to severe pulp infections and periradicular lesions, resulting in pain and potentially leading to systemic illnesses (3). Thus, ECC is not only an oral health issue but also a significant public health concern affecting children's overall health.
Data from the 2019 and 2021 Global Burden of Disease (GBD) studies indicate a continued increase in the global burden of ECC, especially in low- and middle-income countries (LMICs) (4). More than 500 million children are estimated to be affected by ECC worldwide, with prevalence significantly higher in developing countries and impoverished regions than in high-income nations (5). Research also suggests that childhood oral health is closely related to overall health status in adulthood (6). Therefore, ECC prevention and treatment are not only vital for childhood health but may also have long-term implications for adult health. Despite this, awareness and prevention of ECC remain insufficient globally, particularly in low- and lower-middle-income countries, where children's oral health is often overlooked, and resources for health services and education are severely lacking (7).
The pathogenesis of ECC involves multiple factors, including bacteria (such as Streptococcus mutans), dietary influences (such as frequent intake of sugary foods and drinks) (8), poor oral hygiene (such as irregular tooth brushing), socioeconomic factors (such as household income and parental education), and cultural practices (9–11). Additionally, studies have demonstrated correlations between ECC and children's nutritional status, body mass index (BMI), and cognitive development (12). The severity of ECC can negatively impact children's physical and mental development, potentially leading to malnutrition, stunted growth, and attention deficits (13). Therefore, developing effective public health policies, raising health awareness among parents and children, and improving access to oral health services—especially in LMICs—are crucial strategies for controlling ECC burden (14, 15).
Although many studies have explored the causes and control strategies of ECC, there remains a lack of systematic research on the epidemiological characteristics and burden trends of ECC globally (16). Studies based on the GBD database provide crucial data for analyzing ECC burden at global and regional levels; however, data on ECC burden distribution and trend changes across different Socio-Demographic Index (SDI) regions, sexes, and age groups remain unclear. Thus, a comprehensive global study is urgently needed to address this gap (17).
This study, based on the GBD 2021 database, aimed to systematically assess ECC burden worldwide and across regions with varying SDI levels from 1990 to 2021, examine temporal trends, and analyze the relationship between ECC burden, SDI, sex, and age distribution. By analyzing long-term dynamic changes in the global ECC burden, this study seeks to provide scientific evidence for formulating targeted public health policies and oral health interventions across regions. Additionally, the study uses predictive models to project ECC burden trends for the coming decades, offering guidance for public health policymakers to effectively control ECC burden, improve global children's oral health, and enhance overall quality of life.
Materials and methods
This study assessed the burden of early childhood caries (ECC) globally and across regions with different SDI levels from 1990 to 2021 using data from the GBD database. A systematic approach was applied to data collection, model estimation, and statistical analysis, as follows:
Data source
Data were sourced from the GBD 2021 database on the Global Health Data Exchange platform (GHDx), covering ECC epidemiological data from 1990 to 2021 for 204 countries and territories (18). ECC burden was evaluated using metrics such as prevalence, incidence, and years lived with disability (YLDs) across global and SDI regions. Data were stratified by sex (male and female) and age groups (<1 year, 2–4 years, 5–9 years, 10–14 years) and categorized according to SDI levels of different regions and countries.
Case definition and disease model
The case definition for ECC was based on the International Classification of Diseases, 10th Revision (ICD−10) standard, using code K02.3. The study population included children under five years of age (including those in the 2–4 and 5–9 age groups) with ECC from 1990 to 2021. All disease modeling was conducted using the Bayesian Meta-Regression tool, DisMod-MR, developed under the GBD framework. DisMod-MR is a Bayesian stratified model that synthesizes and estimates data across studies in the absence of direct observational data. This model integrates prevalence, incidence, and burden data from multiple sources, using Monte Carlo simulations to estimate global and regional disease burden, providing 95% uncertainty intervals (UI).
Data analysis and processing
Calculation of epidemiological metrics
The age-standardized prevalence rate, incidence rate, and disability-adjusted life years (DALYs) for ECC were calculated following GBD standardized methods. Descriptive and trend analysis assessed long-term changes in ECC burden at global and regional levels. All analyses used the age-standardized rate (ASR) and EAPC to represent the yearly trends of epidemiological metrics. Countries and regions were divided into five categories by SDI level: low SDI (<0.46), low-middle SDI (0.46–0.60), middle SDI (0.61–0.69), high-middle SDI (0.70–0.81), and high SDI (>0.81), allowing comparisons of ECC burden across development levels.
Analysis of regional disparities and SDI correlation
Regression models were used to examine the relationship between SDI and ECC burden. By calculating the EAPC for each country and region, trends in ECC burden across various SDI levels were analyzed. To further explore the SDI-ECC burden relationship, a generalized additive model (GAM) was used to evaluate ECC burden relative to SDI, with a scatter plot generated for EAPC and SDI.
Prediction model development
An Autoregressive Integrated Moving Average (ARIMA) model was used to estimate ECC burden trends through 2040 at global and SDI-specific levels. Age-standardized prevalence, incidence rates, and YLDs from 1990 to 2021 were used as independent variables, with SDI level as a key covariate. Model estimates were based on 1,000 Monte Carlo simulations, with the 95%UI defined between the 25th and 975th simulations.
Statistical methods
All data analyses were conducted using R software (v4.3.3) following the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER). Descriptive statistics were used to assess sample characteristics, and EAPC for all epidemiological indicators was calculated using a linear regression model, with statistical significance set at p < 0.05. Sensitivity analyses ensured the robustness and reliability of estimates, and ECC burden trends were visualized with line graphs, heatmaps, and scatter plots for global, regional, and country-specific data.
Ethical considerations
The data used in this study were obtained from the publicly available GBD database, with all data anonymized, thus exempting this study from ethical approval. Additionally, the study adhered to the GBD Study Framework and GATHER guidelines to ensure transparency in data usage, accuracy of results, and reproducibility of methods.
Results
Global incidence and prevalence of dental caries in primary teeth
In 2021, the global incidence and prevalence of dental caries in primary teeth showed slight differences between males and females, with males having a slightly higher incidence rate. Specifically, the age-standardized incidence rate (ASR) for males was 17,921.72 per 100,000 population (95% uncertainty interval: 14,075.56–23,235.69), compared to 17,631.42 per 100,000 for females (95% uncertainty interval=13,833.09–22,759.74). The age-standardized years lived with disability rate (ASYR) was similar between males and females, at 2.90 and 2.87, respectively (Table 1).
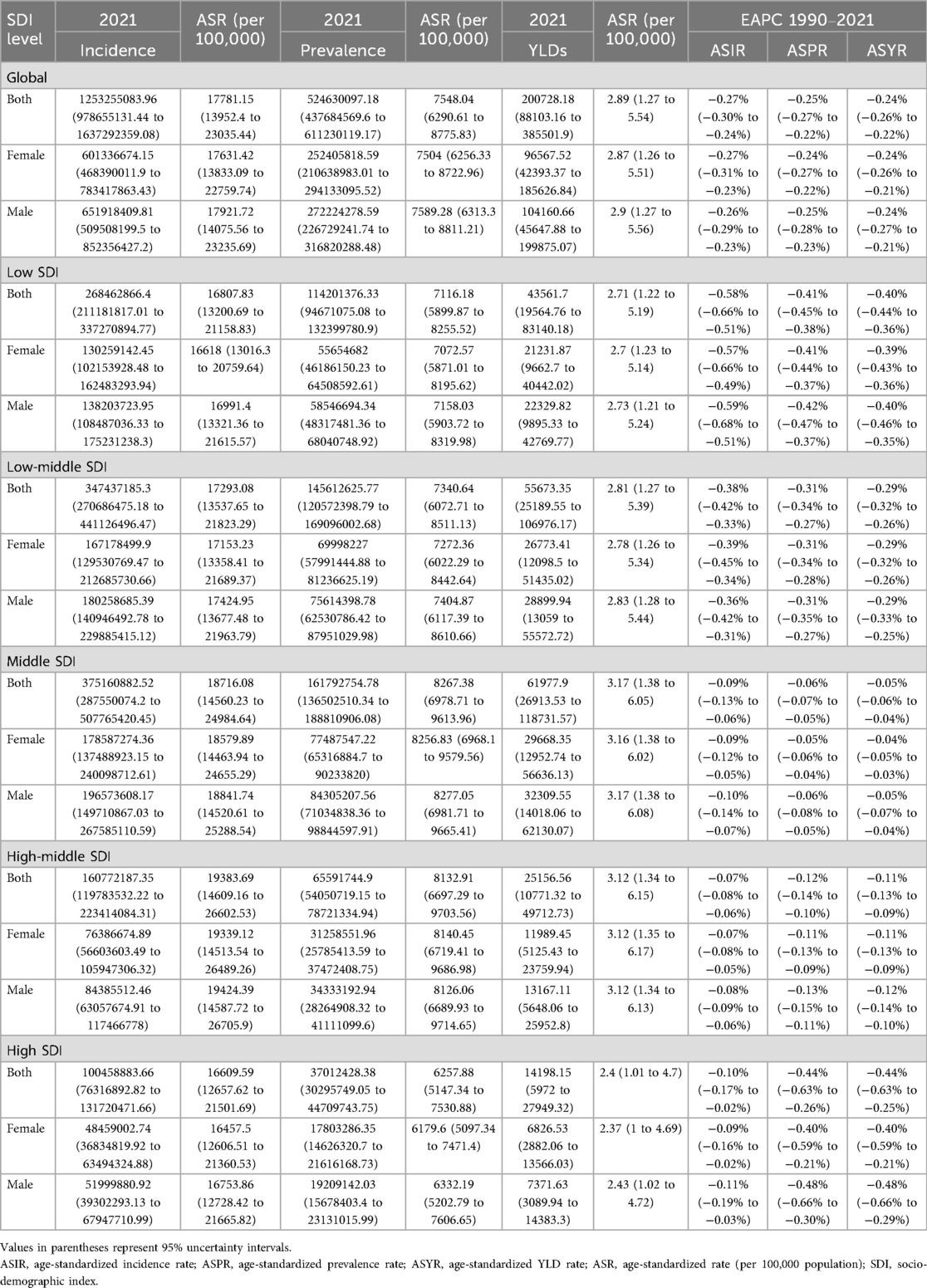
Table 1. Overview of the incidence, prevalence, and years lived with disability (YLD) rates for deciduous caries by sex globally and in SDI regions in 2021, along with the corresponding age-standardized rates and estimated annual percentage change (EAPC) values.
EAPC data indicate a declining trend in the incidence, prevalence, and ASYR of dental caries in primary teeth from 1990 to 2021. The EAPC for incidence was −0.27% (males −0.26%, females −0.27%), for prevalence it was −0.25% (males −0.25%, females −0.24%), and for ASYR it was −0.24% for both males and females. These data suggest that, although the global burden of dental caries in primary teeth has decreased, the reduction has been modest.
Differences in dental caries in primary teeth across SDI regions
Significant differences were observed in the epidemiology of dental caries in primary teeth across different SDI regions:
Low SDI region
The incidence rate and ASYR were relatively low in low SDI regions, but the EAPC showed a significant decline, particularly in males, whose incidence rate declined by −0.59%. This suggests that, despite limited resources, some effective interventions were implemented to control dental caries in primary teeth in these regions.
Medium SDI region
Medium SDI regions (including low-middle and medium SDI) showed higher incidence and prevalence rates, with relatively stable EAPC changes. In the low-middle SDI region, the ASR for males was 17,424.95 per 100,000, compared to 17,153.23 per 100,000 for females. This indicates a continued challenge in managing dental caries effectively in medium SDI regions.
High SDI region
High SDI regions had the lowest burden of dental caries in primary teeth, with both incidence and prevalence rates significantly lower than those in other regions. The EAPC for ASYR was −0.44%, indicating significant success in controlling dental caries in these regions through effective public health interventions.
Sex differences
The incidence and prevalence rates of dental caries in primary teeth were generally higher in males compared to females, although the ASYR showed no significant sex difference. This disparity may be attributed to differences in caries pathogenesis, dietary habits, and oral hygiene practices between males and females, which require further investigation to elucidate potential mechanisms.
Age and sex characteristics of dental caries in primary teeth
Incidence
The incidence of dental caries in primary teeth increased markedly among children aged 2–9 years, peaking at ages 5–9. This peak may be associated with the complete eruption of primary teeth and challenges in maintaining oral hygiene during this period. Data showed that the incidence rate was slightly higher in males than in females, suggesting subtle sex-related differences in oral health behaviors or exposure to risk factors (Figure 1A).
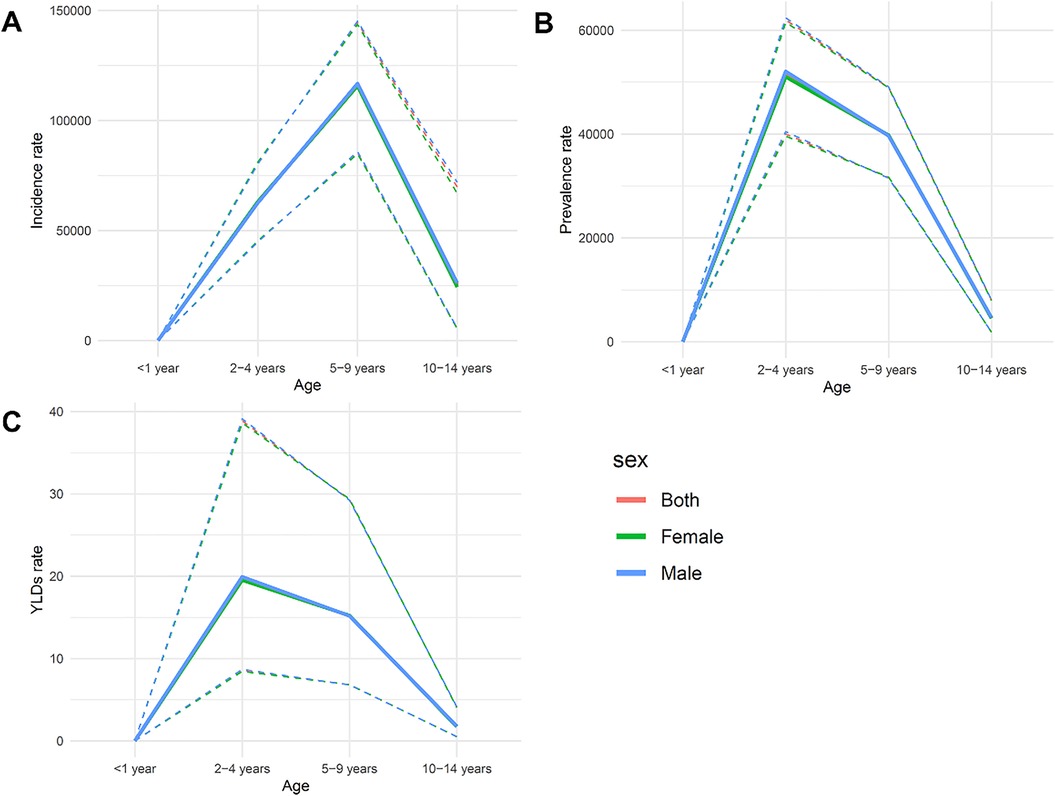
Figure 1. The incidence (A), prevalence (B), and ASYR (C) of dental caries in primary teeth according to age and sex in 2021.
Prevalence
The prevalence of dental caries followed a similar pattern to incidence, increasing significantly between ages 2 and 9 and peaking at ages 5–9, then declining in the 10–14 age group. This indicates that the peak burden of dental caries occurs during the preschool and early school years, likely influenced by changing dietary habits and lower compliance with oral hygiene practices. Additionally, the prevalence was consistently higher in males, reinforcing the trend observed in incidence (Figure 1B).
ASYR
The ASYR peaked among children aged 2–4 years and gradually declined between ages 5 and 14. Notably, ASYR was higher in males across all age groups, with the greatest difference seen in the 5–9 age group. This difference may be attributed to male behavioral factors, such as less frequent oral hygiene practices or poorer dietary choices (Figure 1C).
The incidence, prevalence, and ASYR of dental caries in primary teeth showed significant differences across age groups and sex. Ages 2–9 were the most burdened, particularly the 5–9 age group, which should be a focal point for public health interventions aimed at reducing the burden of dental caries in this population. Sex differences should also be taken into consideration when formulating policies, including health education and preventive measures specifically targeting boys to improve oral health behaviors.
Trends in dental caries in primary teeth across SDI regions
Age-standardized incidence rate
The incidence rate showed significant variation across SDI levels, with an initial increase followed by a decrease. As the SDI increased, the incidence rate peaked in medium SDI regions and then slightly declined, reflecting greater susceptibility to dental caries in medium SDI regions due to socio-economic conditions. High SDI regions benefited from improved oral health measures and awareness, resulting in lower incidence rates (Figure 2A).
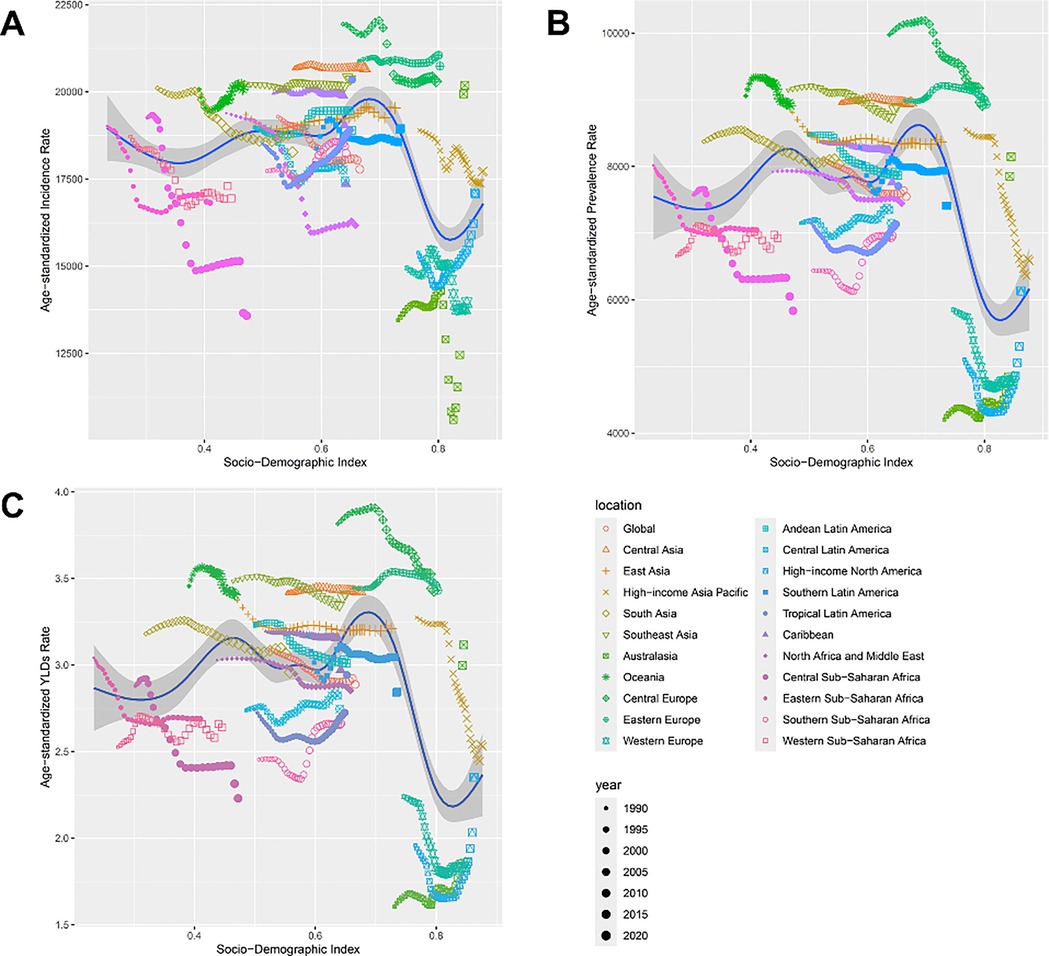
Figure 2. Illustrates that high-income Asia-Pacific and Western Europe generally have lower rates, whereas central and east Asia display higher rates. (A) Age-standardized incidence, (B) prevalence, and (C) YLD rates of oral disorders across the socio-demographic index (SDI).
Age-standardized prevalence rate
The prevalence rate followed a similar trend to the incidence rate, peaking in medium SDI regions before declining. Medium SDI regions still face challenges in caries prevention, highlighting gaps in public health infrastructure (Figure 2B).
Age-standardized YLD rate
The ASYR was higher in low and medium SDI regions and gradually decreased in high SDI regions, indicating that socio-economic development helps reduce the long-term disease burden of dental caries (Figure 2C).
Epidemiological differences across regions and sex
Central Asia and East Asia
Both regions had relatively high incidence and prevalence rates. The ASR for Central Asia was 20,660.8 per 100,000, while in East Asia it was 19,535.58 per 100,000. However, East Asia showed a slightly lower ASYR, indicating some progress in disease management. Notably, East Asia exhibited a slight increase in incidence (EAPC of 0.09%) but a decline in prevalence (EAPC of −0.09%), reflecting mixed progress (Table 2).
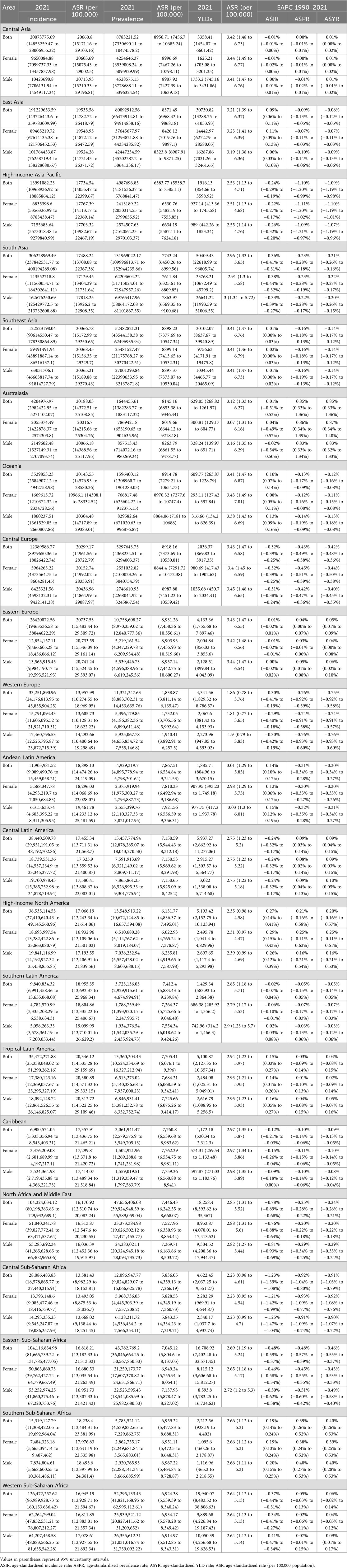
Table 2. An overview of the incidence, prevalence, and years lived with disability (YLD) rates for deciduous caries by sex in regions in 2021, along with the corresponding age-standardized rates and estimated annual percentage change (EAPC) values.
High-income Asia-Pacific and Western Europe
These regions showed the lowest burden of dental caries, with incidence and prevalence rates significantly lower than in other regions. The declining EAPC for these regions indicates effective and sustained public health measures.
South Asia and sub-Saharan Africa
South Asia and Sub-Saharan Africa had high incidence and ASYR, reflecting deficiencies in oral health services and weak public health infrastructure that hinder effective caries prevention. For example, East Sub-Saharan Africa had a prevalence ASR of 7,045.12 per 100,000, with an ASYR of 2.69.
Sex differences
Across most regions, the incidence and prevalence rates of dental caries in males were consistently slightly higher than those in females. For example, in East Asia, the ASR for males was 19,524.28 per 100,000, compared to 19,548.95 per 100,000 for females, indicating a slight sex disparity. Some regions, such as South Asia and Western Europe, showed a more pronounced decline in EAPC for females, suggesting these areas may focus more on oral health education for female children.
Trends in dental caries in primary teeth from 1990 to 2040
Incidence trend
The global incidence of dental caries in primary teeth decreased from 1990 to 2020. However, predictions beyond 2020 indicate that incidence may rebound, especially in low, medium, and low-middle SDI regions. These regions had large uncertainty intervals, indicating unpredictability in future trends (Figure 3A).
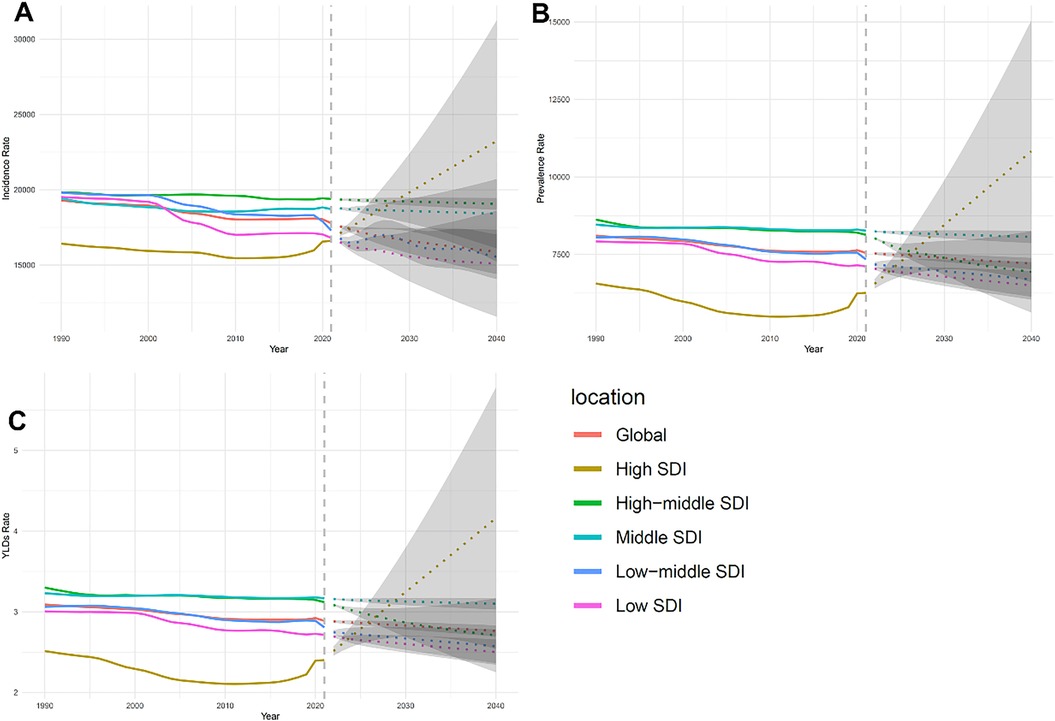
Figure 3. Trends in incidence (A), prevalence (B), and age-standardized years lived with disability (YLD) rate (ASYR) (C) of dental caries in primary teeth from 1990 to 2040, highlighting variations across different socio-demographic index (SDI) regions.
ASYR trend
The ASYR showed a decreasing trend globally, suggesting improvements in treatment and management over the past three decades. However, differences between SDI regions remained, with high SDI regions showing significantly lower ASYR compared to low SDI regions (Figure 3B).
Prevalence trend
The prevalence rate showed a similar decline, especially in high SDI regions. However, the prevalence rate in low, medium, and low-middle SDI regions showed considerable potential fluctuations, possibly related to limited healthcare access and poor oral health infrastructure (Figure 3C).
Overall trends and regional disparities
The results from Figure 3 indicate significant regional disparities in the burden of dental caries in primary teeth. High SDI regions showed significant reductions and lower predicted variations in incidence, prevalence, and ASYR, suggesting that interventions have been effective. In contrast, low and medium SDI regions are predicted to experience more variability and challenges in controlling caries rates.
Discussion
The findings of this study provide important insights into the global burden of dental caries in primary teeth, highlighting significant variations in incidence, prevalence, and ASYR across different SDI regions, age groups, and sexes. These disparities underscore the need for targeted public health strategies to address dental caries in specific populations.
The declining trend in the incidence, prevalence, and ASYR of dental caries in primary teeth from 1990 to 2021, as indicated by the EAPC, suggests a modest improvement in the global burden of this condition. However, the limited reduction highlights the ongoing challenges in preventing and managing dental caries worldwide. The reduction was particularly modest in low and medium SDI regions, where socio-economic factors, inadequate healthcare infrastructure, and limited access to oral health services may hinder effective prevention and treatment (19). These findings suggest that despite global efforts to improve oral health, the existing interventions are insufficient to address the needs of under-resourced populations (20).
Differences across SDI regions were prominent, with high SDI regions exhibiting the lowest burden of dental caries, both in terms of incidence and prevalence. This can likely be attributed to better access to healthcare, improved oral hygiene practices, and greater awareness of preventive measures in these regions (21). In contrast, medium and low SDI regions showed higher incidence and prevalence rates, with medium SDI regions experiencing a peak in both metrics (19). The higher burden in these regions may be related to the transitional socio-economic conditions that increase susceptibility to dental caries, such as changing diets high in sugar and inadequate public health measures to counteract these risks. The findings also suggest that high SDI regions have benefited from sustained public health interventions, while medium and low SDI regions require more focused efforts to bridge the gap in oral health outcomes (22).
Sex differences in dental caries were also evident, with males consistently showing slightly higher incidence and prevalence rates compared to females, although ASYR showed no significant sex difference. This disparity may be linked to differences in dietary habits, oral hygiene practices, and health-seeking behaviors between males and females (23). For example, males may be less likely to engage in preventive oral health behaviors, such as regular brushing and dental visits, which could contribute to the observed higher rates of dental caries (24). These findings indicate a need for sex-specific health education and interventions that address the unique behaviors and risks associated with dental caries in males.
Age-specific analysis revealed that children aged 2–9 years were the most burdened by dental caries, particularly those aged 5–9 years. The high incidence and prevalence in this age group are likely due to the complete eruption of primary teeth and the challenges associated with maintaining proper oral hygiene during early childhood. The findings emphasize the importance of focusing public health interventions on younger children to reduce the burden of dental caries. Effective strategies could include early education for parents and caregivers on the importance of oral hygiene, reducing sugar intake, and increasing access to preventive dental care (25). Moreover, public health policies should prioritize integrating oral health into broader child health programs to ensure that preventive measures are accessible to all children, particularly in vulnerable communities (26).
The trends observed from 1990 to 2040 indicate that, while progress has been made in reducing the burden of dental caries in high SDI regions, challenges remain in low and medium SDI regions. The predicted rebound in incidence rates in these regions after 2020 underscores the importance of continuous and adaptable public health efforts. Factors such as limited healthcare access, socio-economic instability, and lack of awareness about oral health are likely contributing to the uncertainty and potential increase in caries incidence. These findings suggest that sustained investment in healthcare infrastructure, community-based oral health initiatives, and school-based preventive programs are crucial for mitigating the burden of dental caries in these populations (21).
The results of this study illustrate the importance of focusing public health interventions on younger children to reduce the burden of dental caries. Preventive oral health programmes in schools have been shown to be very effective in instilling proper oral hygiene practices and dietary awareness at an early age (8, 10, 11). Collaboration between schools, dental hospitals and public health organisations can enhance regular dental check-ups, supervised brushing and interactive health education to reduce the risk of dental caries. In addition, educating parents and caregivers, especially in communities with limited awareness of caries risk, about reducing children's sugar intake, balanced nutrition and proper oral hygiene practices can significantly enhance the effectiveness of prevention programmes (10, 11, 15). These approaches not only address immediate risk factors, but also help to develop long-term healthy behaviours in children.
Overall, this study highlights the complex interplay between socio-economic factors, healthcare access, sex, and age in influencing the burden of dental caries in primary teeth. To achieve significant reductions in dental caries globally, particularly in under-resourced regions, public health strategies must be multifaceted and tailored to address the specific needs of different populations. Key recommendations include improving access to dental care, enhancing community-level oral health education, and implementing targeted interventions for high-risk groups such as young children and males. By focusing on these areas, it is possible to make meaningful progress in reducing the global burden of dental caries in primary teeth and improving children's oral health outcomes overall.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
HY: Writing – original draft, Writing – review & editing, Funding acquisition, Software, Project administration, Methodology. YF: Formal analysis, Writing – original draft, Methodology. L-YX: Formal analysis, Writing – original draft, Methodology. K-MW: Project administration, Writing – original draft, Investigation. H-CF: Conceptualization, Writing – review & editing, Data curation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Key Project of Science and Technology of Guiyang Health Commission under Grant number 41.
Acknowledgments
The Authors thank all the individuals who contributed to the Global Burden of Disease Study 2021 for their extensive support in finding, cataloguing, and analyzing data and facilitating communication between and among team members.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. This manuscript was polished for language clarity and style with the assistance of ChatGPT (OpenAI). The authors critically reviewed, edited, and finalized the manuscript to ensure the accuracy, integrity, and scientific rigor of the content. All intellectual contributions, study design, data analysis, and interpretation are entirely the work of the authors.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Peres MA, Macpherson LMD, Weyant RJ, Daly B, Venturelli R, Mathur MR, et al. Oral diseases: a global public health challenge. Lancet. (2019) 394:249–60. doi: 10.1016/S0140-6736(19)31146-8
2. Colak H, Dülgergil CT, Dalli M, Hamidi MM. Early childhood caries update: a review of causes, diagnoses, and treatments. J Nat Sci Biol Med. (2013) 4:29–38. doi: 10.4103/0976-9668.107257
3. Pitts NB, Baez RJ, Diaz-Guillory C, Donly KJ, Alberto Feldens C, McGrath C, et al. Early childhood caries: IAPD Bangkok declaration. J Dent Child (Chic. (2019) 86:72.31395110
4. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
5. Wagner Y, Heinrich-Weltzien R. Pediatricians’ oral health recommendations for 0- to 3-year-old children: results of a survey in Thuringia, Germany. BMC Oral Health. (2014) 14:44. doi: 10.1186/1472-6831-14-44
6. Petersen PE. World health organization global policy for improvement of oral health—world health assembly 2007. Int Dent J. (2008) 58:115–21. doi: 10.1111/j.1875-595X.2008.tb00185.x
7. Maklennan A, Borg-Bartolo R, Wierichs RJ, Esteves-Oliveira M, Campus G. A systematic review and meta-analysis on early-childhood-caries global data. BMC Oral Health. (2024) 24:835. doi: 10.1186/s12903-024-04605-y
8. Vozza I, Capasso F, Calcagnile F, Anelli A, Corridore D, Ferrara C, et al. School-age dental screening: oral health and eating habits. Clin Ter. (2019) 170:e36–40. doi: 10.7417/CT.2019.2105
9. Kassebaum NJ, Smith AGC, Bernabé E, Fleming TD, Reynolds AE, Vos T, et al. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. (2017) 96:380–7. doi: 10.1177/0022034517693566
10. Calcagnile F, Pietrunti D, Pranno N, Di Giorgio G, Ottolenghi L, Vozza I. Oral health knowledge in pre-school children: a survey among parents in central Italy. J Clin Exp Dent. (2019) 11:e327–33. doi: 10.4317/jced.55378
11. Fioravanti M, Di Giorgio G, Amato R, Bossu M, Luzzi V, Ierardo G, et al. Baby food and oral health: knowledge of the existing interaction. Int J Environ Res Public Health. (2022) 19:5799–809. doi: 10.3390/ijerph19105799
12. Lee GHM, Mcgrath CP, Yiu CKY, King N. A comparison of a generic and oral health-specific measure in assessing the impact of early childhood caries on quality of life. Community Dent Oral Epidemiol. (2010) 38(4):333–9. doi: 10.1111/j.1600-0528.2010.00543.x
13. Vadiakas G. Case definition, aetiology and risk assessment of early childhood caries (ECC): a revisited review. Eur Arch Paediatr Dent. (2008) 9:114–25. doi: 10.1007/BF03262622
14. Chen KJ, Gao SS, Duangthip D, Lo ECM, Chu CH. Prevalence of early childhood caries among 5-year-old children: a systematic review. J Investig Clin Dent. (2019) 10:e12376. doi: 10.1111/jicd.12376
15. Guerra F, Zumbo G, Straccamore L, Sansotta L, Stamegna C, Iacono R, et al. Parental knowledge and its impact on nutrition and oral health habits in children: a cognitive investigation. J Clin Med. (2024) 13:5631–45. doi: 10.3390/jcm13185631
16. Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. (2009) 22:3–8.19281105
17. Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, Alipour V, et al. And national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. (2020) 99:362–73. doi: 10.1177/0022034520908533
18. Hirohata T, Kitano T, Saeki C, Baba K, Yoshida F, Kurihara T, et al. Quantitative behavioral evaluation of a non-human primate stroke model using a new monitoring system. Front Neurosci. (2022) 16:964928. doi: 10.3389/fnins.2022.964928
19. Mathur MR, Williams DM, Reddy KS, Watt RG. Universal health coverage: a unique policy opportunity for oral health. J Dent Res. (2015) 94:3s–5. doi: 10.1177/0022034514565648
20. Listl S, Galloway J, Mossey PA, Marcenes W. Global economic impact of dental diseases. J Dent Res. (2015) 94:1355–61. doi: 10.1177/0022034515602879
21. Petersen PE, Ogawa H. The global burden of periodontal disease: towards integration with chronic disease prevention and control. Periodontol 2000. (2012) 60:15–39. doi: 10.1111/j.1600-0757.2011.00425.x
22. Watt RG, Daly B, Allison P, Macpherson LMD, Venturelli R, Listl S, et al. Ending the neglect of global oral health: time for radical action. Lancet. (2019) 394:261–72. doi: 10.1016/S0140-6736(19)31133-X
23. Lukacs JR. Sex differences in dental caries experience: clinical evidence, complex etiology. Clin Oral Investig. (2011) 15:649–56. doi: 10.1007/s00784-010-0445-3
24. Vaidya V, Partha G, Karmakar M. Gender differences in utilization of preventive care services in the United States. J Womens Health (Larchmt). (2012) 21:140–5. doi: 10.1089/jwh.2011.2876
25. Douglass JM, Clark MB. Integrating oral health into overall health care to prevent early childhood caries: need, evidence, and solutions. Pediatr Dent. (2015) 37:266–74.26063555
Keywords: deciduous dental caries, global burden of disease, socio-demographic index, ARIMA model, public health
Citation: Yang H, Feng Y, Xiao L-Y, Wang K-M and Feng H-C (2025) Global, regional and national burden of deciduous dental caries from 1990 to 2021: analysis of risk factors and prediction of trends in 2035. Front. Dent. Med. 6:1624571. doi: 10.3389/fdmed.2025.1624571
Received: 9 May 2025; Accepted: 4 September 2025;
Published: 7 October 2025.
Edited by:
Kitty Jieyi Chen, Sun Yat-sen University, ChinaReviewed by:
Iole Vozza, Sapienza University of Rome, ItalyDilek Öztaş, Yildirim Beyazit University Yenimahalle Training and Research Hospital, Türkiye
Copyright: © 2025 Yang, Feng, Xiao, Wang and Feng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li-Yuan Xiao, Y25saXl1YW4ueGlhb0Bob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work